relatively high estrogen and low progesterone relatively high estrogen and low progesterone
TRANSCRIPT

Relatively High estrogen and
Low progesterone
Relatively High estrogen and
Low progesterone

Development of excess fibrous tissue
Hyperplasia of the epithelial lining of the mammary ducts
Proliferation of mammary ducts
Cyst formation
Palpable lumps that are round, well-delineated and freely movable
Lumps increase in size premenstrual
Tenderness
Pain
Nipple discharge

Does having a fibrocystic breastcondition increase a woman’s risk for development of breast cancer ?

Ultrasound
Biopsy◊Fine needle Aspiration◊Excisional
Why is a fine needle aspiration biopsy preferred over an excisional biopsy?

Patient Teaching◊Wear good support bra
◊Diet Therapy Low salt No chocolate or caffeine
◊Medications Vitamin E Antiestrogen - Danazol Diuretics Analgesics
◊Remind Patient to have a Yearly follow-up
◊Continue to perform monthly BSE
In teaching the patient with painful fibrocystic breast changes about the condition, the nurse explains thata. All breast lumps must be biopsied to rule out
malignant changesb. The symptoms will probably subside after
menopause unless you use HRTc. Restrictions of coffee and chocolate and
supplements of vitamin E may relieve the discomforts
d. The lumps will become progressively larger and more painful, eventually necessitating surgical removal

Breast Cancer

•Significant health concern for women
•1 in 7 chance of being diagnosed with Breast Cancer
•Intense feelings of shock, fear, denial
•One of the most common malignancies in American women
•Significant health concern for women
•1 in 7 chance of being diagnosed with Breast Cancer
•Intense feelings of shock, fear, denial
•One of the most common malignancies in American women

◊Female gender; ≥50 years of age◊Personal History
Family history Personal history of cancer (breast, colon,
endometrial, ovarian) ◊Hormonal factors
Early menarche or late menopause No pregnancies First child after 30 years of age
◊Weight gain and obesity after menopause
◊High fat diet, alcohol intake◊Exposure to ionizing radiation
BRCA1 and BRCA2 are human genes that belong to a class of genes known as tumor suppressors.
In normal cells, BRCA1 and BRCA2 help ensure the stability of the cell’s genetic material (DNA) and help prevent uncontrolled cell growth.
Mutation of these genes has been linked to the development of hereditary breast and ovarian cancer.
A woman’s lifetime risk of developing breast and/or ovarian cancer is greatly increased if she inherits a harmful mutation in BRCA1 or BRCA2.

HER-2 receptors are found on the inside and outside of the Cancer cell. Receptors join together to send messages
telling cancer cells to grow and divide

Detected as a lump
Abnormality on mammography
If palpable, irregular shaped, poorly delineated, nonmobile (usually attached to chest wall), and nontender
May have nipple discharge – bloody
Nipple retraction
Dimpling

One of the best ways for a woman to become self-aware of how their breasts normally look and feel and to detect when something changes.
Should be done monthly when the breasts are non tender, right after the end of menses
If no longer have menses – use the first day of each month

Step 1: Begin by looking at your breasts in the mirror with your shoulders straight and your arms on your hips.
Here's what you should look for:Breasts that are their usual size, shape, and colorBreasts that are evenly shaped without visible distortion or swelling
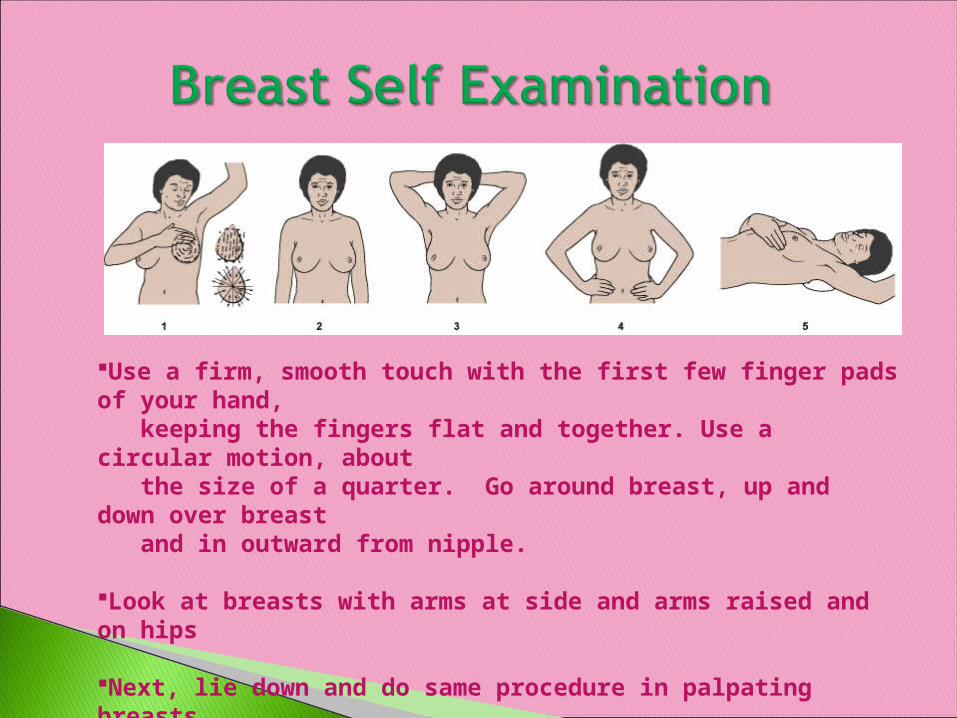
Use a firm, smooth touch with the first few finger pads of your hand, keeping the fingers flat and together. Use a circular motion, about the size of a quarter. Go around breast, up and down over breast and in outward from nipple.
Look at breasts with arms at side and arms raised and on hips
Next, lie down and do same procedure in palpating breasts.

DNA testing for BRCA – 1 and BRCA-2Mammogram / ultrasound
Mammogram showing Bilateral Invasive Ductal Carcinoma
Biopsy
Lymphatic mapping and sentinel lymph node dissection (SLND)◊Helps surgeon identify lymph nodes that drain first from tumor site
◊Radioisotope and/or blue dye is injected into tumor site
◊Lymph nodes dissected and sent to lab for analysis
◊

While discussing risk factors for breast cancer, the nurse stresses that the greatest known risk factor for breast cancer isa. Being a woman over 60 years of ageb. Experiencing menstruation for 40 years
or morec. Using estrogen replacement therapy
during menopaused. Having a paternal grandmother with
postmenopausal breast cancer




Most common options for resectable Breast Cancer
◊Breast conservation surgery with radiation therapy
◊Modified radical mastectomy with or without reconstruction

Sentinel lymph node dissection (SLND) has replaced ALND for patients who do not have malignant cells
ALND performed when one or more sentinel lymph nodes contain malignant cells
Examination of lymph nodes provides prognosis and treatment information

Involves removal of entire tumor with a margin of normal tissue
Radiation therapy is delivered to entire breast, ending with a boost to tumor bed
Evidence of systemic disease may warrant chemotherapy before radiation

Modified radical mastectomy◊Removal of breast and axillary lymph nodes with preservation of the pectoralis major muscle
◊Patient has the option of breast reconstruction

Primary radiation therapy ◊ Usually performed after local excision of breast
mass
◊ Breast is radiated daily over ~5 to 6 weeks
◊ “Boost” treatment may be given to full breast following primary dose
Intraoperative Radiation Therapy◊ Single intense dose delivered to surgery site in
the operating room

High-dose brachytherapy ◊ Internal radiation delivered via radioactive seeds into a balloon catheter
◊Balloon catheter is placed within the lumpectomy site
◊Treatment is over 4-5 days

Palliative radiation therapy◊Used to stabilize symptomatic metastatic lesions in such sites as
Bone Soft tissue organs Brain Chest
◊Relieves pain ◊Successful in controlling recurrent or metastatic disease for long periods

Radiation therapy side effects ◊Fatigue
◊Skin changes
◊Breast edema


Removes or blocks source of estrogen, promoting tumor regression
Estrogen can increase growth of BC cells if cells are estrogen receptor positive
Most common drug used in estrogen-receptor positive women is:
Tamoxifen (Nolvadex) – antiestrogen Side effects – decreased visual acuity, and
vascular changes Fulvestrant (Faslodex) - antiestrogen
Hormonal therapy (cont'd)◊2 advances have increased use in BC Hormone receptor assays developed to identify those likely to respond to treatment
Drugs have been developed that can inactivate hormone-secreting glands as effectively as surgery or radiation

How are these used in treatment?

Trastuzumab (Herceptin) is a monoclonal antibody to HER-2
Once the antibody attaches to antigen, it is taken to cells and eventually kills them
It can be used to alone or in combination with other chemotherapies
Side-effect – monitor for signs of ventricular dysfunction and congestive heart failure.

◊Use of cytotoxic drugs to destroy cancer cells
◊BC is one of the solid tumors that is most responsive to chemotherapy
◊Given preoperatively in some patients to decrease size of primary tumor


The patient will:◊ Actively participate in decision-making
process related to treatment options
◊ Fully comply with therapeutic plan
◊ Manage side effects of therapy
◊ Be satisfied with support provided by significant others and health care providers

Complications;
◊Heaviness◊Pain◊ Impaired motor function in arm◊Numbness◊Paresthesia of the fingers◊Cellulitis and progressive fibrosis can result
http://www.youtube.com/watch?v=Di5E_KXbAnU&feature=related
◊Positioning Place in a semi-Fowler’s position with arm on
affected side elevated on a pillow, never dependent
◊ Exercise Flexing and extending fingers should begin in
recovery room and progressive increase in activity
Exercises are designed to prevent contractures and muscle shortening, maintain muscle tone, and improve lymph and blood circulation
Postoperative arm and shoulder exercises are instituted gradually at surgeon’s direction
◊Avoid constriction Do not take Blood pressure readings on
that arm Avoid constrictive clothing
◊Compression Wrap arm with bandages going from distal
to proximal Use intermittent pneumatic compression
sleeve or a fitted elastic pressure gradient sleeve
◊Massage Therapy
Venipunctures, and injections should not be done on affected arm
Apply insect repellantWear gloves when gardeningUse cooking mittUse electric razor for shaving axilla Avoid cutting cuticles – push back
cuticleNo heavy liftingKeep clean and dry

Relieve postmastectomy pain syndrome: ◊ Chest and upper arm pain, tingling down
arm◊ Numbness, shooting or prickling pain◊ Unbearable itching persisting beyond
3-month healing time
Treatment includes ◊Nonsteroidal antiinflammatory drugs◊Antidepressants◊Topical lidocaine patches or EMLA

Postoperative discomfort can be minimized by administering analgesics ~30 minutes prior to exercises
When showering is appropriate, warm water has a soothing effect and decreases joint stiffness
Psychologic care◊All aspects of care must include sensitivity to woman’s effort to cope
◊Nurse can help by: Assisting her to develop a positive but realistic attitude
Helping her identify sources of support and strength to her
Must be follow-up for rest of life at regular intervals
Professional examinations every 6 months for 2 years, then annually
Practice monthly breast self examinations (BSE) on both breasts or remaining breast
A patient had a radical mastectomy with lymph node dissection. Post op nursing care focused on restoring arm functioning would includea. Use of heating pads or blankets to
increase circulationb. Daily application of ice packs to minimize
the risk of lymphedemac. Compression bandaging with sleeves or
stocking for acute swellingd. Frequent and sustained exercises with the
arm in a dependent position


Chest prior to Implants
Breast implants placed in pocket under pertoralis muscle and
musculocutaneous skin flap applied

Musculocutaneous flap most often taken from abdomen or back is used in reconstruction

As part of the final stage of reconstruction, the nipple and areola are reconstructed
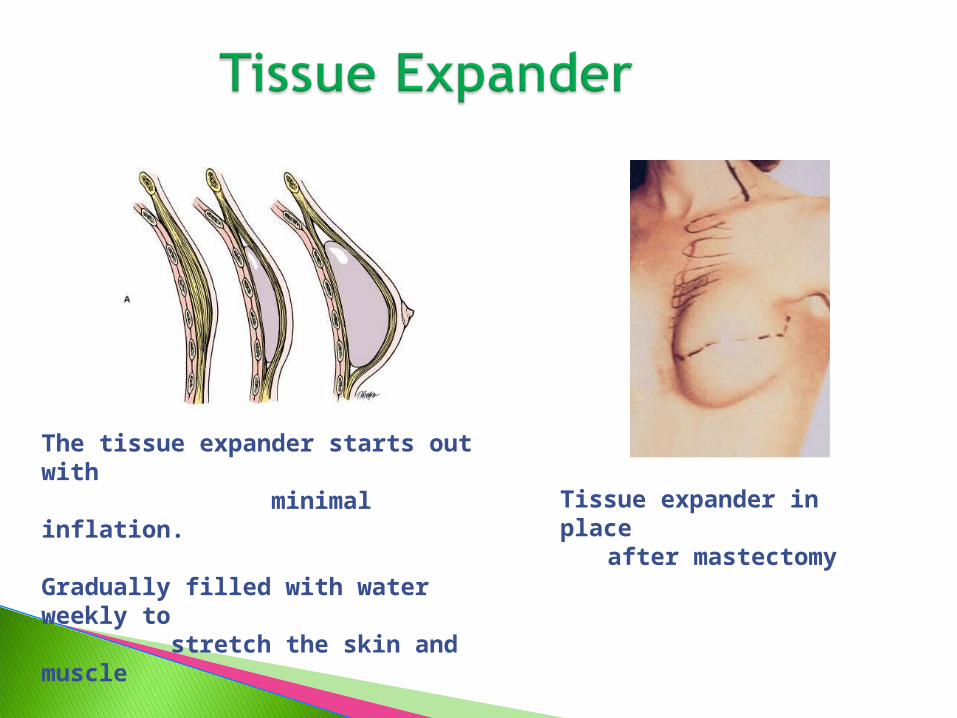
The tissue expander starts out with minimal inflation.
Gradually filled with water weekly to stretch the skin and muscle
Tissue expander in place after mastectomy

Capsular formation◊ Part of bodies natural defense mechanism to
form a fibrous capsule around the implant
Infection
Hematoma
Skin ulceration
Hypertropic scar formation
To prevent capsular formation following breast reconstruction with implants, the nurse teaches the patient toa. Gently massage the area around the
implantb. Bind the breasts tightly with elastic
bandagec. Exercise the arm on the affected side to
promote drainaged. Avoid strenuous exercise until implant
healing has occurred.