red eye; recognition and management - london eye...
TRANSCRIPT
Red eye; Recognition and management
Mr. Usman Saeed
MBBS, MRCOphth, FRCOphth, MRCS (Ed), FRCS (Ed)
Consultant Ophthalmologist
Epsom & St Helier NHS Trust
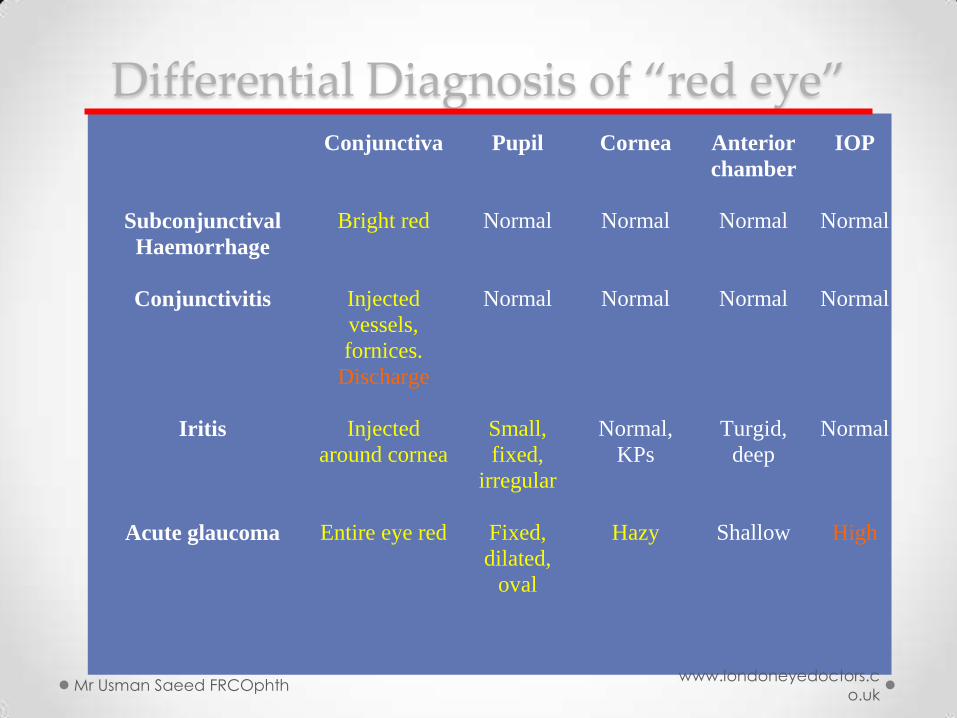
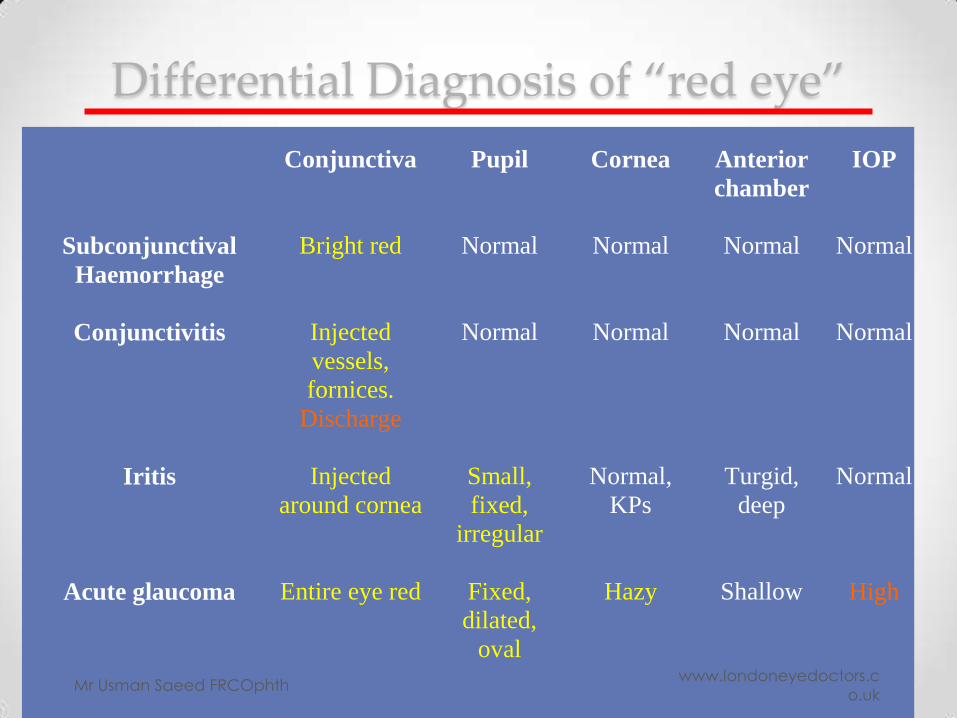
Differential Diagnosis of “red eye”
Conjunctiva
Pupil Cornea Anterior
chamber
IOP
Subconjunctival
Haemorrhage
Bright red Normal Normal Normal Normal
Conjunctivitis Injected
vessels,
fornices.
Discharge
Normal Normal Normal Normal
Iritis Injected
around cornea
Small,
fixed,
irregular
Normal,
KPs
Turgid,
deep
Normal
Acute glaucoma Entire eye red Fixed,
dilated,
oval
Hazy Shallow High
Mr Usman Saeed FRCOphth
www.londoneyedoctors.c
o.uk

CASE A 34 yr old man comes into A&E with a 3 day
history of red right eye.
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
HISTORY Gives you valuable
pointers towards
possible diagnosis
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
History How long ?
Pain/irritation/gritty/ache/dry
Change in vision
Photophobia
Discharge/watering
Previous history of similar problem
Past ophthalmic history
Contact lens wear ?
Any other member of the family affected ?
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
History How long ? Chlymidia, blepharitis
Pain/irritation/gritty/ache/dry dry eye
Change in vision possible uveitis , glaucoma
Photophobia uveitis, corneal ulcer
Discharge/watering conjunctivitis, infection, allergy
Previous history of similar problem uveitis
Past ophthalmic history uveitis
Contact lens wear ? Corneal ulcer
Any other member of the family affected ? infection
Mr Usman Saeed FRCOphth www.londoneyedoctors.co.uk
Drug History Anticholinergics/ dry eyes
Oral contraceptives -dry eyes
Amiodarone – vortex keratopathy
Mr Usman Saeed FRCOphth www.londoneyedoctors.co.uk
PMH/ROS HT/IHD – subconjunctival haemorrhage
Rheumatoid arthritis – scleritis, corneal problems
Ankylosing spondylitis HLA 27 + Uveitis
Steroid use uveitis
Rosacea Blepharitis
Ask specifically for any recent eye
surgery / injection / procedure
Mr Usman Saeed FRCOphth www.londoneyedoctors.co.uk
EXAMINATION

What you need to know • Visual acuity Use a Snellen chart at 6 meters or
newer electronic charts @ various distances
• Are the lids OK
• Is the Conjunctiva OK
• Is the cornea OK
• Is the iris OK
• Is the lens OK
Mr Usman Saeed FRCOphth www.londoneyedoctors.co.uk
What you need
www.londoneyedoctors.c
o.uk Mr Usman Saeed FRCOphth
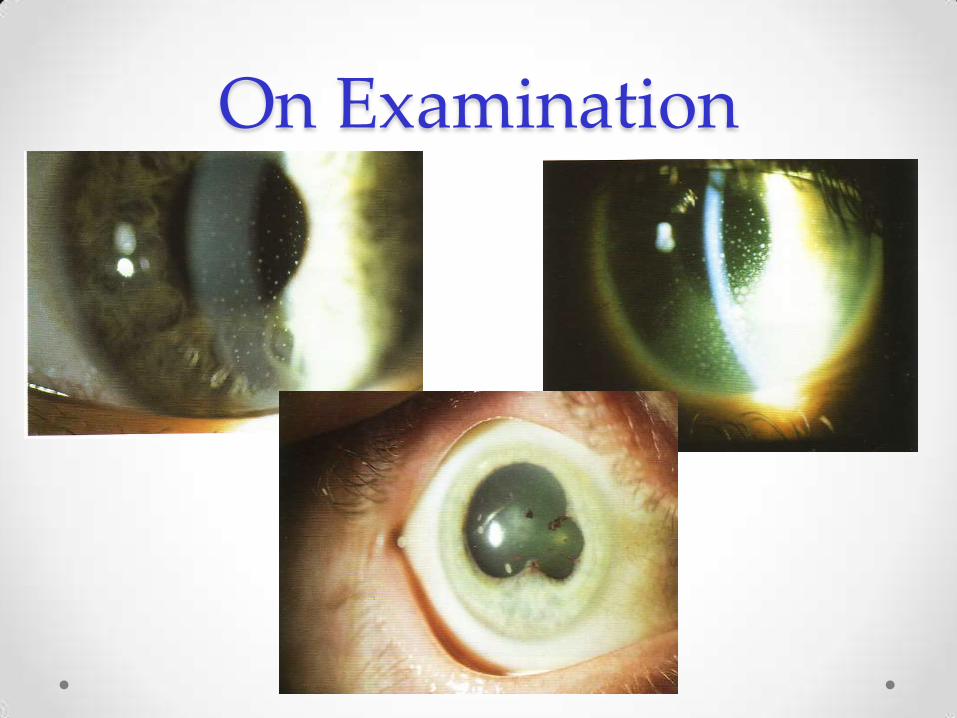
On Examination
Differential Diagnosis of “red eye”
Conjunctiva
Pupil Cornea Anterior
chamber
IOP
Subconjunctival
Haemorrhage
Bright red Normal Normal Normal Normal
Conjunctivitis Injected
vessels,
fornices.
Discharge
Normal Normal Normal Normal
Iritis Injected
around cornea
Small,
fixed,
irregular
Normal,
KPs
Turgid,
deep
Normal
Acute glaucoma Entire eye red Fixed,
dilated,
oval
Hazy Shallow High
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Diagnosis? Offer a diagnosis based on your history and examination
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Common causes of red eye
• Conjunctivitis
• Keratitis
• Iritis
• Scleritis
• Acute glaucoma
• Trauma
• other
Mr Usman Saeed FRCOphth www.londoneyedoctors.co.uk
LIDS
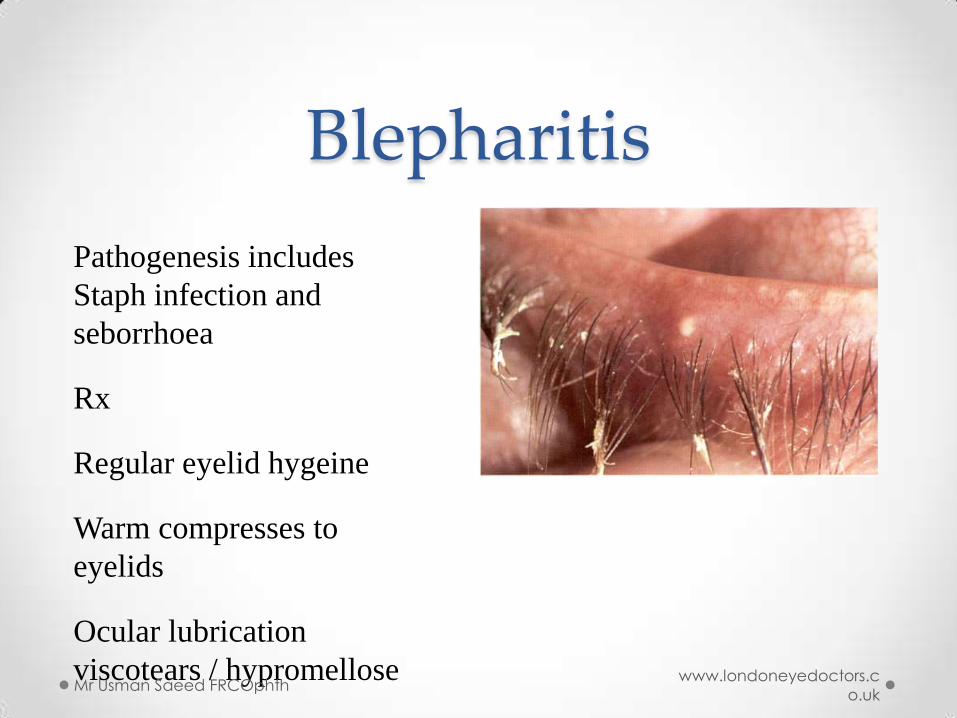
Blepharitis
Pathogenesis includes
Staph infection and
seborrhoea
Rx
Regular eyelid hygeine
Warm compresses to
eyelids
Ocular lubrication
viscotears / hypromellose Mr Usman Saeed FRCOphth
www.londoneyedoctors.c
o.uk

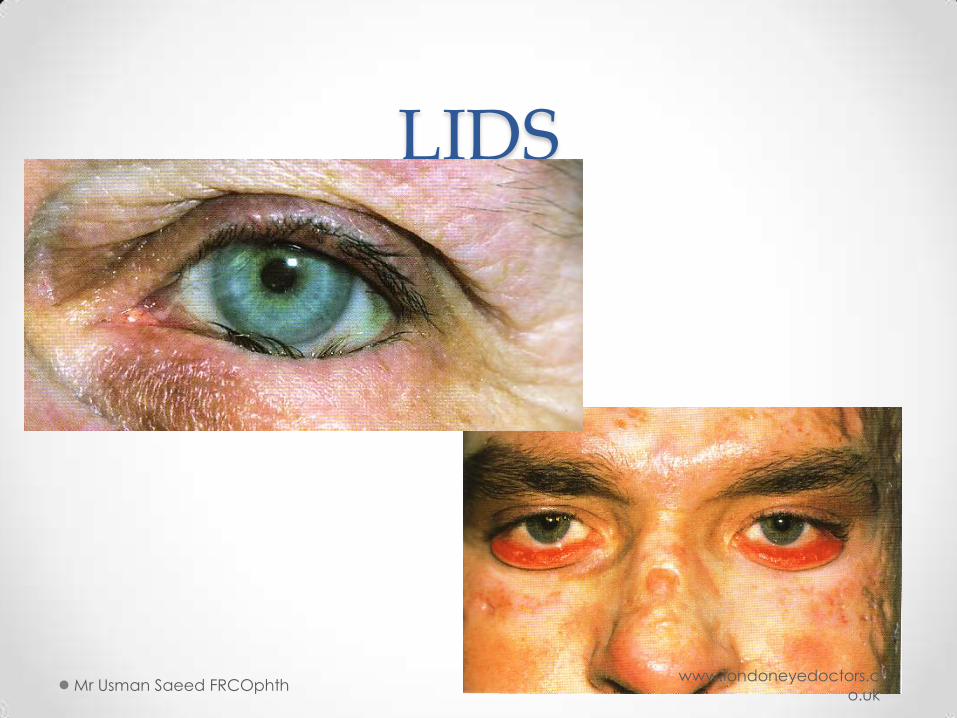
LIDS
Mr Usman Saeed FRCOphth www.londoneyedoctors.co.uk
LIDS
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
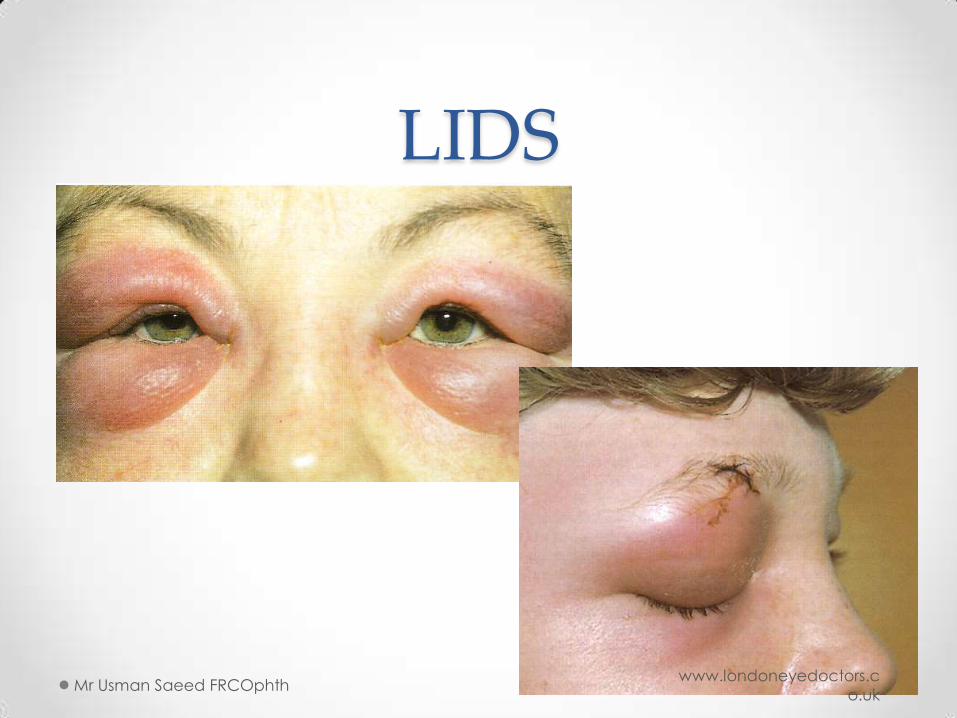
LIDS
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
PRESEPTAL CELLULITIS
Risk factors include 1. Trauma
2. Skin infection
3. Age <6years
4. URTI/Otitis media
S.aureus, H.influenza, S.pneumonia and
S.pyogenes responsible for >95%
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk

Shingles • Treat with anti virals
• Aciclovir 800 mg 5 times a day for 2 weeks
• Remember post neuralgic pain
• Amytryptaline or capcasin
www.londoneyedoctors.c
o.uk Mr Usman Saeed FRCOphth
Conjunctiva
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
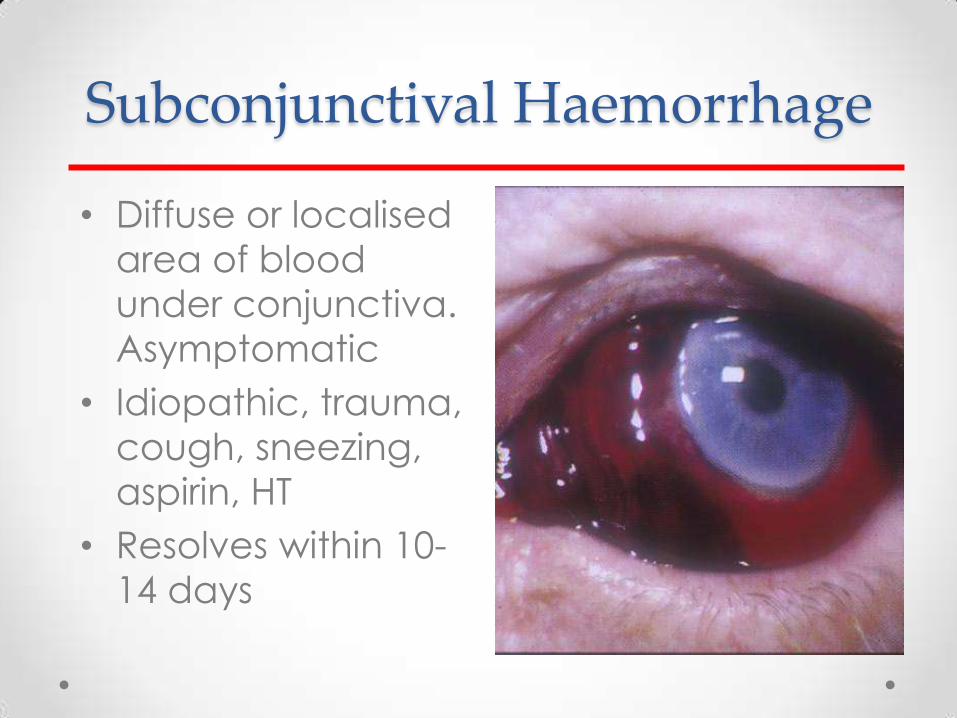
Subconjunctival Haemorrhage
• Diffuse or localised
area of blood
under conjunctiva.
Asymptomatic
• Idiopathic, trauma,
cough, sneezing,
aspirin, HT
• Resolves within 10-
14 days
Conjunctiva
•N.Gonorrhoeae
•Aerobic gram neg cocci
•Can get corneal involvement
•Rx gent drops
•Send to GU
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Conjunctiva - CHLAMYDIA
TRACHOMATIS
•Serotypes A, B, C cause classic endemic trachoma
•Serotypes D to K cause sexually transmitted keratoconjunctivitis
•50% have concomitant genital infection
•Transmission autoinnoculation from genital secretions
•Eye to eye spread rare Mr Usman Saeed FRCOphth
www.londoneyedoctors.c
o.uk

Allergic conjunctivitis
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk

TYPES OF CONJUNCTIVITIS
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Conjunctivitis • Infective
o Viral • Adenovirus
• HSV (usually primary infection with lid vesicles)
o Bacterial • Acute- S. aureus, Str. pneumoniae, H. influenza,
chlamydia trachomatis
• Hyperacute- N. gonorrhoea
• Chronic (commonly blepharoconjunctivitis) -S. Aureus, chlamydia trachomatis
• Allergic
• Chemical/drug induced
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Conjunctivitis- clinical features
• Viral o Watery discharge, pain +/-, lid swelling
o Conj hyperaemia, follicles
o Sometimes corneal subepithelial infiltrates
o Pre-auricular lymphadenopathy
• Bacterial o Purulent discharge
o Conj hyperaemia, papillae
• Allergic o Itch, watery discharge, h/o hayfever
o Lid swelling, conj hyperaemia, papillae
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Viral conjunctivitis
Mr Usman Saeed FRCOphth www.londoneyedoctors.co.uk
Bacterial conjunctivitis
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Atopic conjunctivitis
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Primary HSV infection
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Conjunctivitis • Investigations
o Conjunctival swabs for MC&S +/- viral culture
• Treatment o Broad spectrum topical antibiotic eg chloramphenicol QDS or fucithalmic
BD
• Natural history o Self limiting in most cases within 2 weeks
o Viral is highly contagious
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Cornea
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk

Keratitis • Bacterial
o Wide range of organisms o Most commonly staph and strep sp. o Risk factors: trauma, CL wear, ocular surface
disease
• Viral o HSV (dendritic ulcer) o Recurrent
• Fungal o Trauma with vegetable matter eg branch
• Acanthamoeba o Contact lens wearers with poor lens hygiene
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Dry Eyes
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk

Dry Eye Syndrome • Poor quality
o Meibomian gland disease,Acne
rosacea
o Lid related
o Vitamin A deficiency
• Poor quantity
o KCS
• Sjogren Syndrome
• Rheumatoid Arthritis
o Lacrimal disease ie, Sarcoidosis
o Paralytic ie, VII CN palsy
Mr Usman Saeed FRCOphth www.londoneyedoctors.co.uk
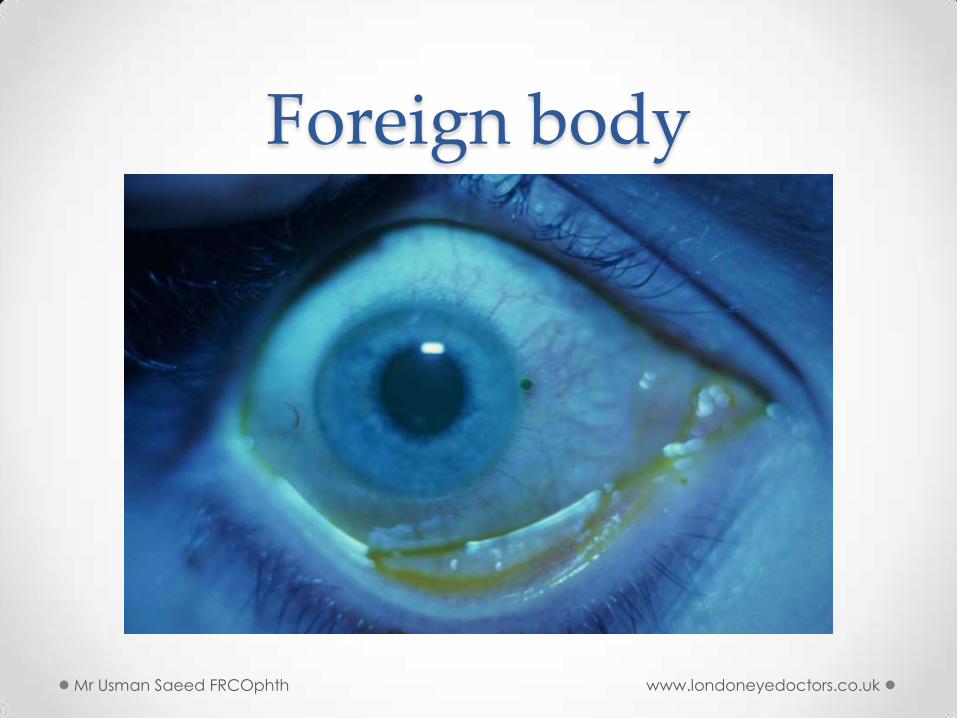
Foreign body
Mr Usman Saeed FRCOphth www.londoneyedoctors.co.uk
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Corneal Abrasion • Surface epithelium sloughed off.
• Stains with fluorescein
• Usually due to trauma
• Pain, FB sensation, tearing, red eye
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk

Marginal keratitis
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Infective keratitis • Investigations
o Corneal scrape for gram stain and culture & sensitivity and HSV culture
• Treatment o HSV- acyclovir eye ointment 5/day
o Bacterial- intensive broad spectrum antibiotic eye drops, eg ciprofloxacin
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Corneal Ulcer • Infection
o Bacterial: Adnexal infection, lid malposition, dry eye, CL
o Viral: HSV, HZO
o Fungal:
o Protozoan: Acanthamoeba in CL wearer
• Mechanical or trauma
• Chemical: Alkali injuries are worse than acid
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Bacterial corneal ulcer
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Bacterial corneal ulcer
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Cornea
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Cornea
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Contact Lens Changes Reduced blink rate
Stagnation of tears under lens
Reduced oxygenation of tissues
Switch to more anaerobic metabolism with
more lactic acid production
Selective adhesion to contact lens
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Pseudomonas Aeruginosa
Gram neg
Aerobic
Aquatic
Doesn’t penetrate healthy epithelium well but action of proteases allow it to pass through traumatized epithelium
Thick mucopurulent discharge
Diffuse liquifactive necrosis
Ground glass appearance of adjacent stroma
ACANTHAMOEBA
Ubiquitous free-living protozoans
Found in air, soil, water
Exist as active trophozoite and dormant cyst
Signs – limbitis
- stromal infiltrates
- ring abscess
Acanthamoeba keratitis
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk

Fungal keratitis
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
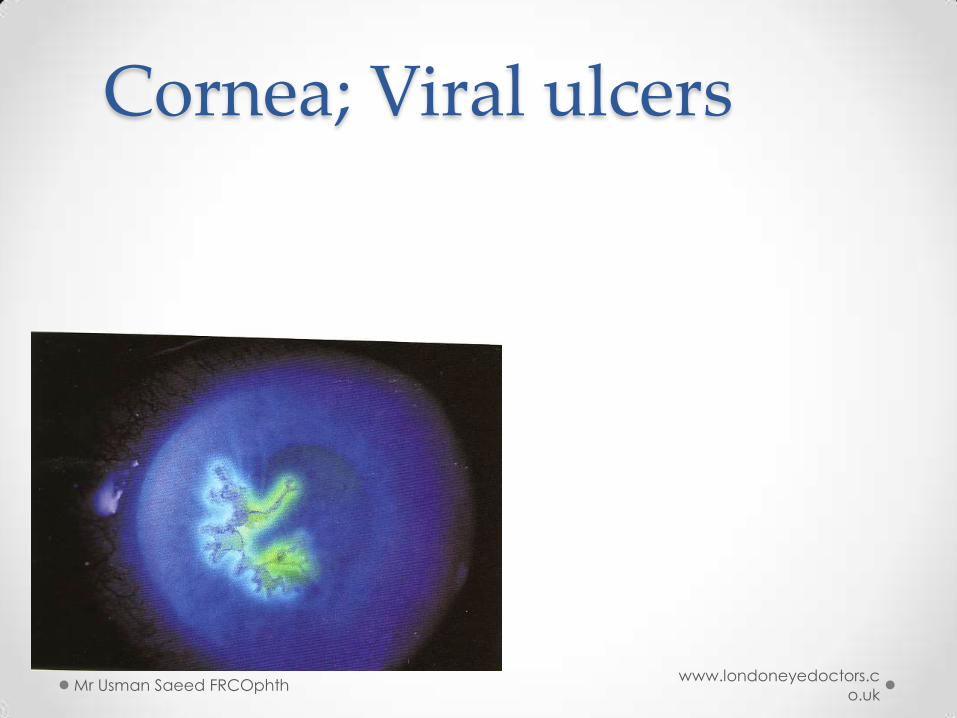
Cornea; Viral ulcers
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
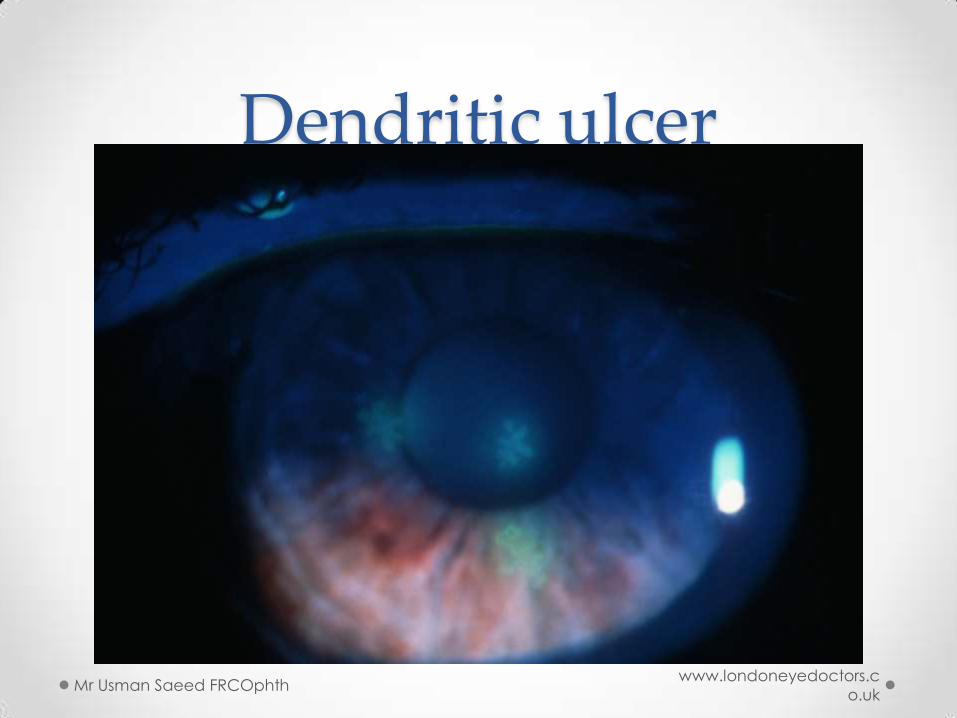
Dendritic ulcer
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
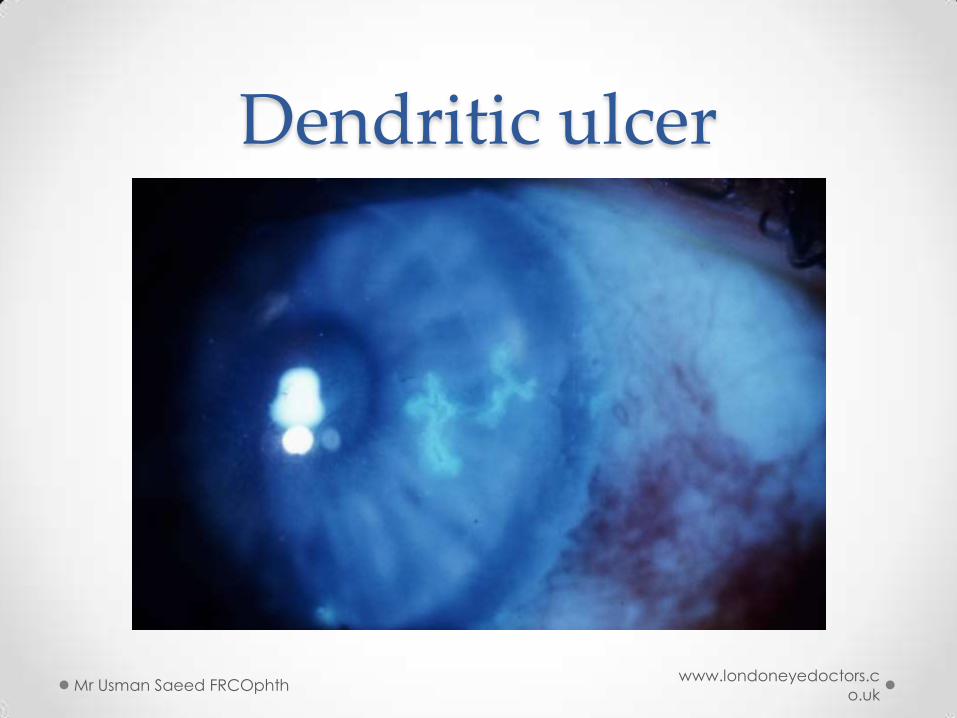
Dendritic ulcer
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Other corneal causes of red eye
• Marginal keratitis o Immune reaction to lid margin staph exotoxins
• Corneal abrasion
• Chemical injury
• Foreign body
• Dry eye
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Scleritis & episcleritis • Episcleritis
o Acute onset, often minimal pain, recurrent, sectoral redness, episcleral
nodule
o Benign but sometimes systemic autoimm dis.
• Scleritis o Severe pain and tenderness, less acute than episcleritis, no discharge, no
chemosis
o Systemic autoimmune disease common esp. rheumatoid arthritis
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Sclera
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Episcleritis • Superficial
• Idiopathic,
collagen vascular
disorder (RA)
• Asymptomatic,
mild pain
• Self-limiting or
topical treatment
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk

Scleritis • Deep
• Idiopathic
• Collagen vascular disease (RA,AS, SLE,
Wegener, PAN)
• Zoster
• Sarcoidosis
• Dull, deep pain wakes patient at night
• Systemic treatment with NSAI or
Prednisolone if severe
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Anterior chamber and Uveal tissue
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
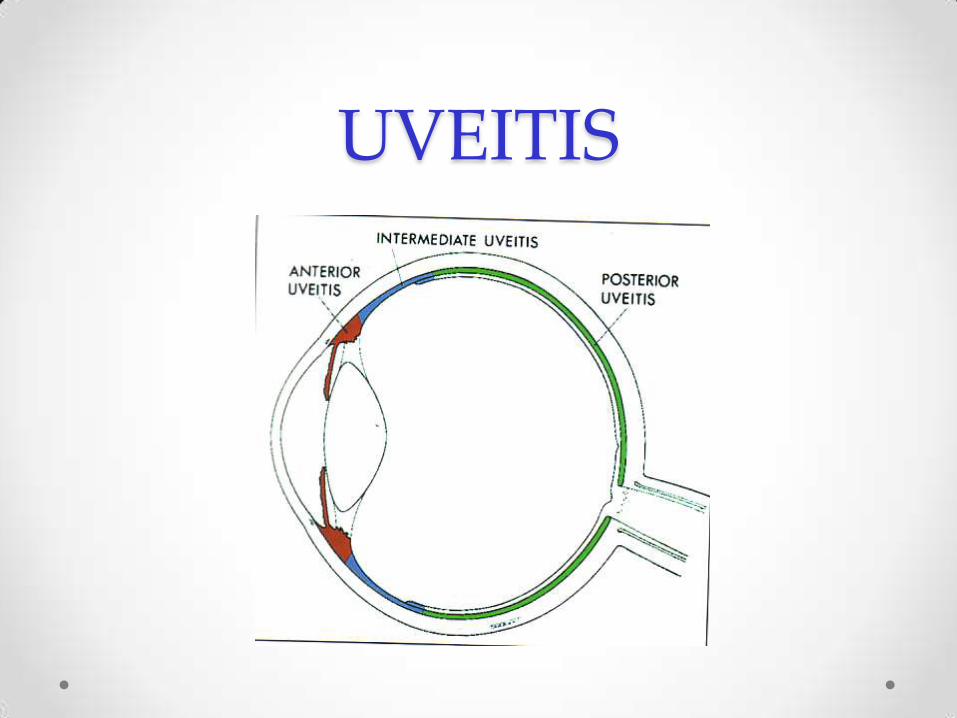
UVEITIS

UVEITIS Idiopathic
Associated with systemic disease Arthritis
Sarcoid
Inflammatory bowel disease
Infections Bacteria – TB/syphillis/leprosy
Fungi – candida
Viruses – herpes
Protozoa – toxoplasmosis
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Acute iritis • Pain, photophobia, onset over 1-3 days
• Often recurrent
• Limbal injection, posterior synechiae, AC cells & flare
• Associated with HLA-B27 o Ank spon
o Reiters o Reactive arthritis
o Inlammatory bowel disease
o Psoriatic arthritis
• Treatment o Topical corticosteroids, dilating drops (cyclopentolate) o Idiopathic in > 50%
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Uveitis Anterior: acute recurrent and chronic
Posterior: vitritis, retinal vasculitis, retinitis,
choroiditis
Panuveitis: anterior and posterior
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Anterior uveitis (iritis) • Photophobia, red eye, decreased vision
• Idiopathic. Commonest
• Associated to systemic disease o Seronegative arthropathies:AS, IBD, Psoriatic arthritis, Reiter’s
o Autoimmune: Sarcoidosis, Behcets
o Infection: Shingles, Toxoplasmosis, TB, Syphillis, HIV
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Acute Glaucoma
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Acute angle closure glaucoma
• Symptoms o Pain
o Blurred vision
o Haloes
o Nausea & vomiting
• Signs o Red eye
o Corneal oedema
o Fixed mid-dilated oval pupil
o High intraocular pressure
o Shallow anterior chamber
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
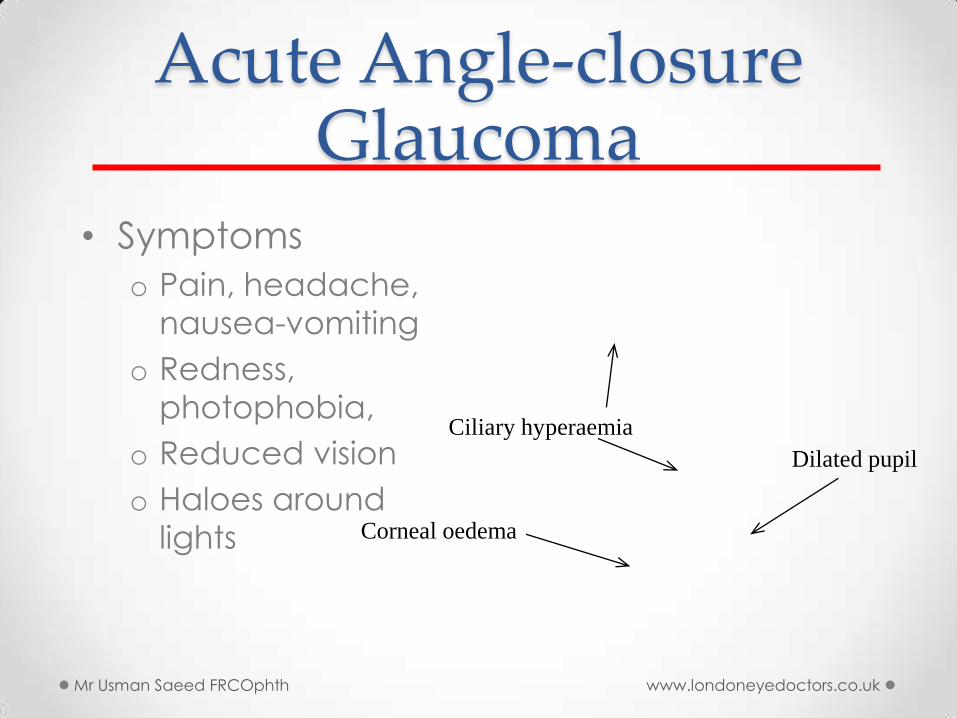
Acute Angle-closure Glaucoma
• Symptoms
o Pain, headache,
nausea-vomiting
o Redness,
photophobia,
o Reduced vision
o Haloes around
lights Corneal oedema
Ciliary hyperaemia
Dilated pupil
Mr Usman Saeed FRCOphth www.londoneyedoctors.co.uk
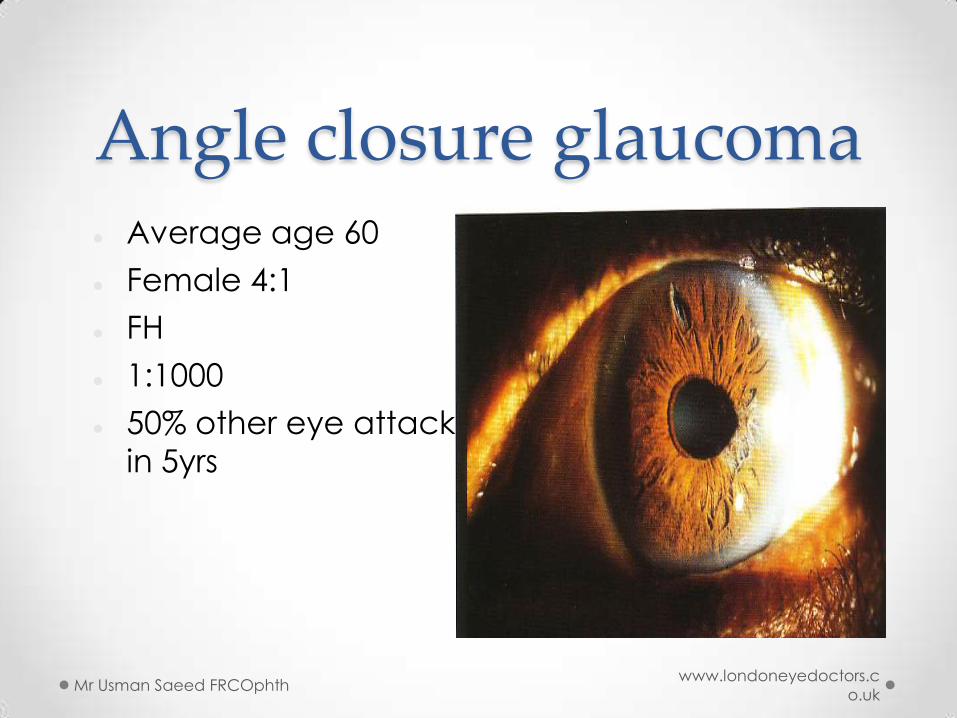
Angle closure glaucoma Average age 60
Female 4:1
FH
1:1000
50% other eye attack
in 5yrs
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk
Treatment of AACG • Immediate
o Acetazolamide (diamox) IV
o Pilocarpine drops
o Beta blocker drops
o Steroid drops
• Once pressure has decreased o YAG laser peripheral iridotomy
Cataract surgery to remove the natural lens and reduce the risk of AACG
Mr Usman Saeed FRCOphth www.londoneyedoctors.c
o.uk

Questions Useful contacts
London eye doctors website
• www.londoneyedoctors.co.uk
Mr Usman Saeed FRCOphth www.londoneyedoctors.co.uk