rectal cancer contouring guide · – note: this was created for both anal and rectal cancer, which...
TRANSCRIPT

RectalCancerContouringGuide
eContourTeam

Youwanttocontour:RectalCancerWhatnow?
• Findyourreferences– RTOGcontouringatlasforanorectal:
• h<ps://www.rtog.org/CoreLab/ContouringAtlases/Anorectal.aspx• NOTE:thiswascreatedforBOTHanalandrectalcancer,whicharetreatedquite
differently,sopaya<enIon!• PublicaIonvalidaIngtheaboveatlas:Myersonetal.IJROBP2009:
h<p://www.ncbi.nlm.nih.gov/pubmed/19117696– RTOGprotocols?
• RTOG0822actuallyshowednodifferencebetweenIMRTand3D-CRT.WhilethiscouldsIllbeareferencetoguidecontouringfor3Dblockplacementperthe3D-CRTarm,let’ssIckwiththepublishedatlas.
– ARROContour:CAUTION!notpeer-reviewed,butaresidentpresentaIoncreatedbyARRO(ASTRO’sResidentCommi<ee)• h<ps://www.astro.org/uploadedFiles/_MAIN_SITE/Affiliate/ARRO/Resident_Resources/
EducaIonal_Resources/ARROcase/Content_Pieces/ARROContourRectal.pdf
*eContour.orgaimstobeyourone-stopshopforcontouringguidelines,withhyperlinkstoabovehigh-yieldreferences!

LeteContour.orghelpyou!
1. SelectCASES
2. Fromdropdowncaselist:GIàRectalàpre-op
3. DrawtheGTV
4. Reviewpelvicanatomy
5. DrawCTV
6. Addmargin/expansiontocreatefinalPTVfortreatmentplanning
7. BONUS:Draw“blocks”

Step1:ContourtheGTV
Grosstumor
IneContour:1. TurncontoursOFF2. Toggleoverlayto
MRI3. Scrollthrough
slicestoviewextentoftumor
4. Startyourcontourwherethetumorisobvious

ContourGTVinferiorly
ALWAYScheckyourvolumeagainstexam/colonoscopyfindingssinceimagingislesssensiIve
TogglebetweenMRIandCT
Assessmentà

MeasuredistanceGTVtoanalverge(OpIon1)
Lookinlowerlekofyourscreenforthe“Z”coordinateonlastGTVslice(-6.98cmhere).ScrolldownunIlyouseetheanalvergeandagainnotethecoordinate(-12.98cmhere).Thedifferenceis~6cm,whichwasthedistancenotedonexam(whichisbe<erthanimaging!).

MeasuredistanceGTVtoanalverge(OpIon2)
Orientyourselfin3DusingtheCROSSHAIRSin…green(coronal),blue(axial),red(sagi<al)

FromthispaIent’sAssessment,weknowthatonexamthetumorislocated6cmfromanalverge…let’sdoublecheckwhereweareatonSAGITTAL!
TIP:IntheSAGITTALview,usethemeasuringtooltochecktheverIcalextentofyourcontour.
Tryusingthemeasuringtool
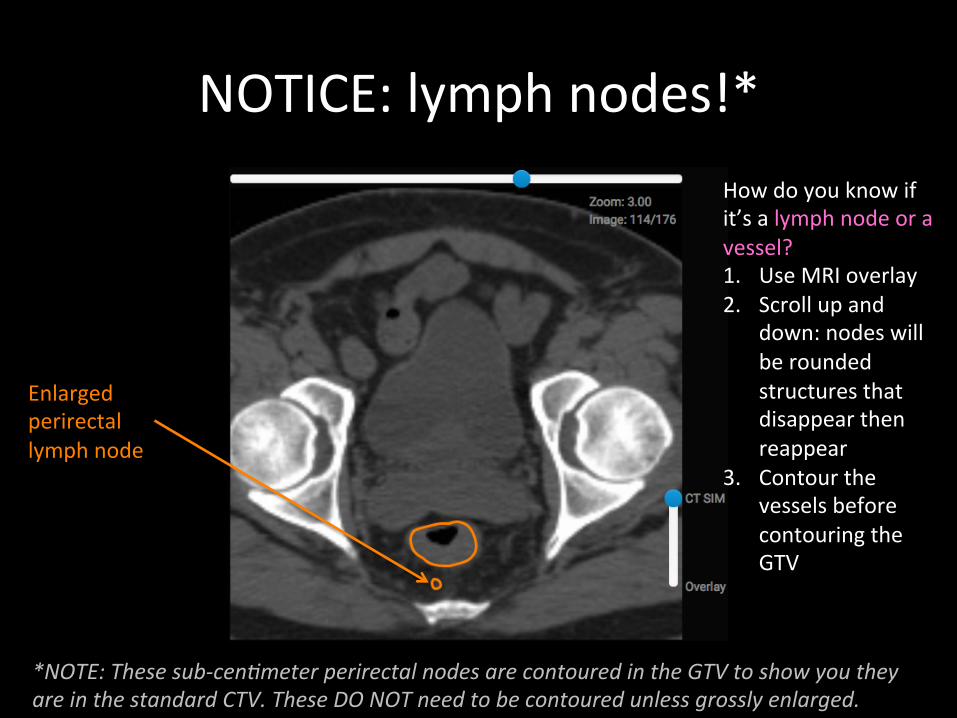
NOTICE:lymphnodes!*
Enlargedperirectallymphnode
Howdoyouknowifit’salymphnodeoravessel?1. UseMRIoverlay2. Scrollupand
down:nodeswillberoundedstructuresthatdisappearthenreappear
3. ContourthevesselsbeforecontouringtheGTV
*NOTE:Thesesub-cenEmeterperirectalnodesarecontouredintheGTVtoshowyoutheyareinthestandardCTV.TheseDONOTneedtobecontouredunlessgrosslyenlarged.

IneContour:1. Turnoffall
contoursEXCEPT“Anatomy”
2. ContoursstartwhereaortaandIVCbranch
3. Scrollinferiorly,followingbranches
Step2:Reviewanatomyofpelvicvessels(whichwilldefinelymphnodesatrisk!)

Axialviewofvessels

CanyoufollowthesevesselsonCT?
1. NowturnoffALLcontours
2. Startatabdominalaorta
3. Scrollinferiorly,followingbranches
Lymphnodessitonvessels(justcan’tseethemwhennotenlarged).ThisiswhywecontourvesselsinnodalCTV
Aorta(artery)orIVC(vein)àCommonIliacs(RandL)àInternaliliac(goposterior/infrontofsacrum)andExternalIliacs(goanterior…becomeinguinal/femoralwhenexitpelvis)

Useanatomycontours
Confirmyourfindingsbyindividuallyturningonthecontoursforeachstructure

Step3:ContouryourCTVThesearetheconsensusCTVsforanorectalcancer
Inrectalcancer,externaliliacnodes(CTVB)andinguinalnodes(CTVC)arenotatriskoftumorspread*,sowewillonlycontourCTVA
(*FYITheanalcanaldrainstotheinguinalnodes,whichiswhytheyaretreatedinanalcancer)
RTOGAnorectalcontouringatlas
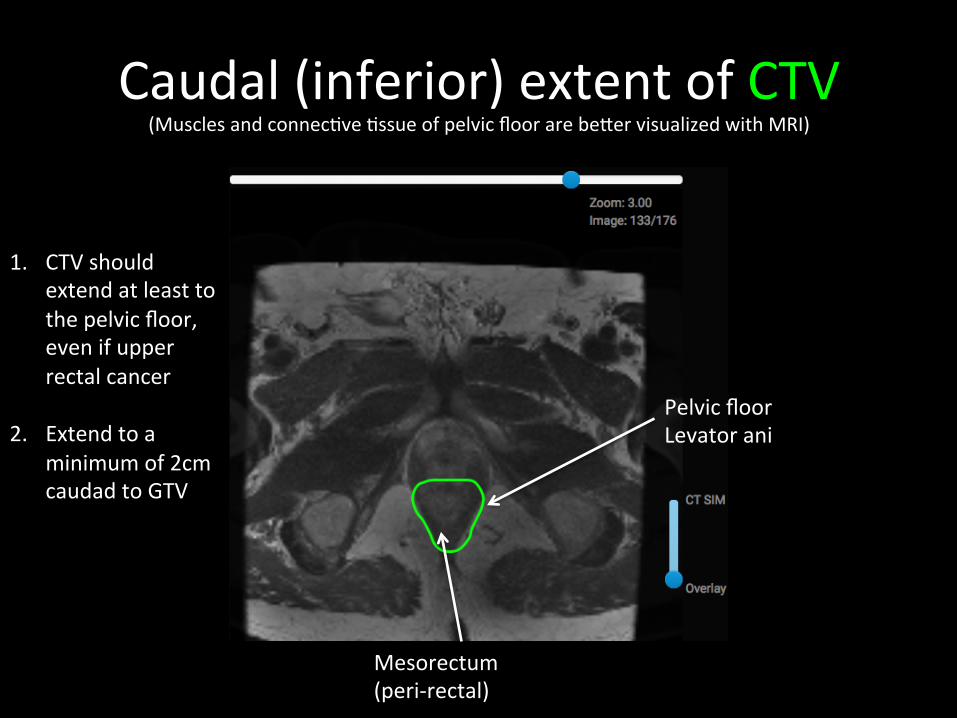
Caudal(inferior)extentofCTV(MusclesandconnecIveIssueofpelvicfloorarebe<ervisualizedwithMRI)
1. CTVshouldextendatleasttothepelvicfloor,evenifupperrectalcancer
2. Extendtoaminimumof2cmcaudadtoGTV
PelvicfloorLevatorani
Mesorectum(peri-rectal)
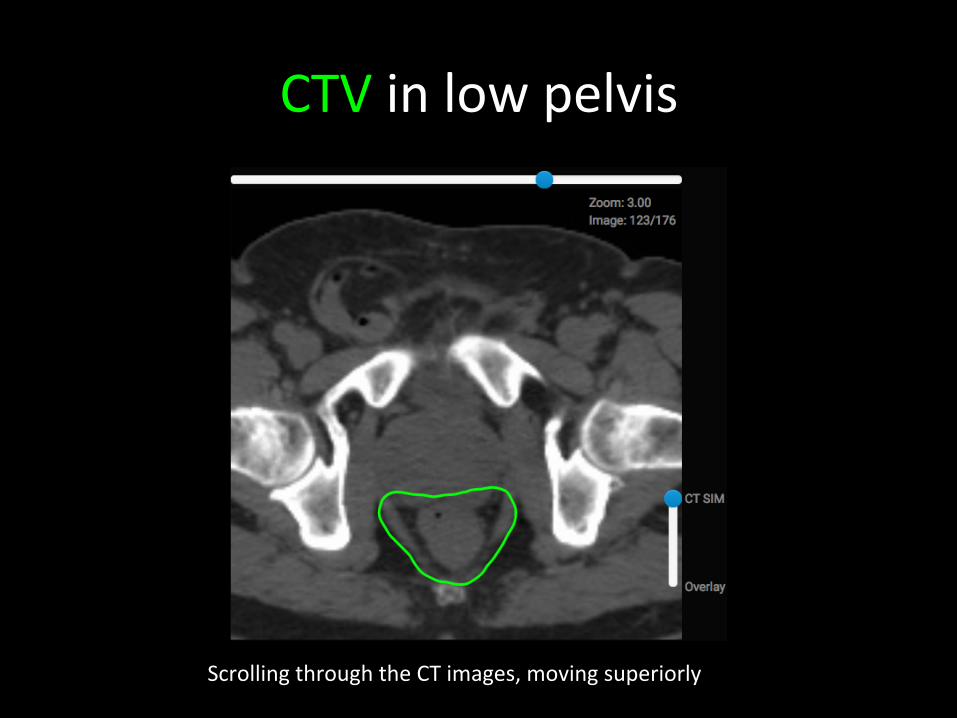
CTVinlowpelvis
ScrollingthroughtheCTimages,movingsuperiorly

CTVinlowpelvis
Posteriorandlateralmargins:Extendtolateralpelvicmusclesorbone
Anteriormargin:Extendintoprostate/seminalvesiclesinamale(vaginaforfemale)

CTVinmid-pelvis
Anteriormargin:Extend1cmintoposteriorbladderwall
Mesorectum(peri-rectal)
CTVAcovers:RectumMesorectumInternaliliacvesselsPresacralspace
Prsacral

MovingsuperiorlyinCTV
Lymphnode
IncludeinternaliliacarteriesandveinsNOTICE:posteriorborderofCTVabutsexternaliliacvessels(whichwedoNOTincludeunlessT4tumorinvadingprostateorvaginalanteriorly)
Presacral
DONOTincludemuscleorbone

Cephalad(superior)extentofCTV
ConInuecontouruptowherethecommoniliacsbifurcateORL5/S1interspace*
*RadoncisamidatransiIonawayfrombonyanatomytoguidecontours(insteadcontouringsokIssue),butitsIllpervadesinmanyways–includingpelvicnodalupperborders(ieL5/S1).

Step4:AddaCTVBoostvolume
SequenIalboostmeansaddiIonaltreatmentstogivehigherdosetosmallervolume
ButhowdoIdothis??Nextslide…
ExtendCTVtocoverenIremesorectumandpresacralregionatlevelofGTV,withaminimum2cmmarginonGTVcephaladandcaudad
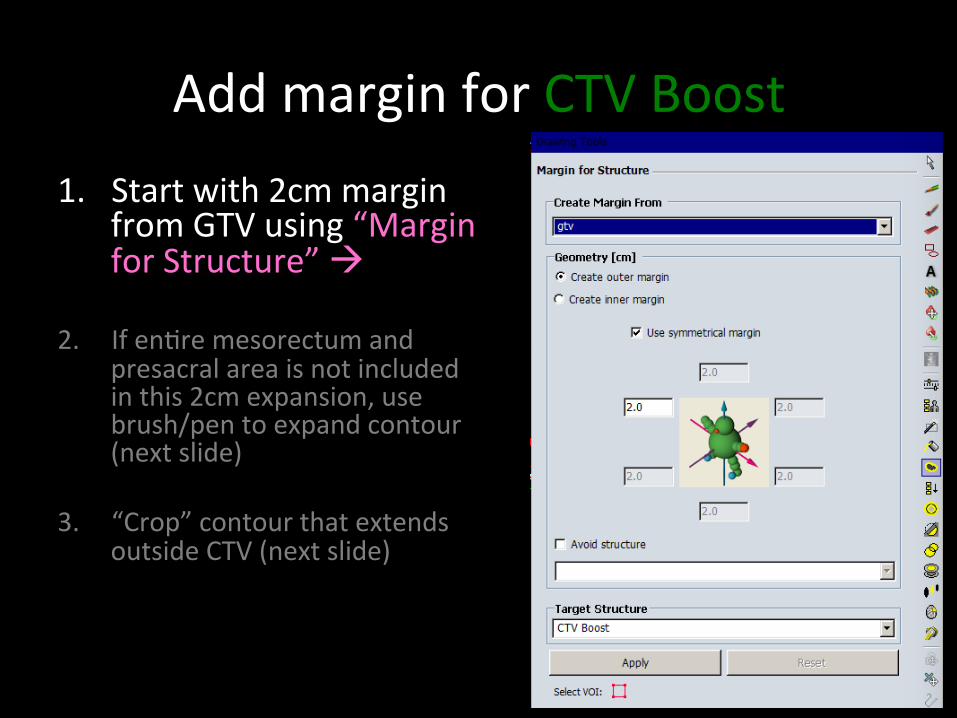
AddmarginforCTVBoost1. Startwith2cmmargin
fromGTVusing“MarginforStructure”à
2. IfenIremesorectumandpresacralareaisnotincludedinthis2cmexpansion,usebrush/pentoexpandcontour(nextslide)
3. “Crop”contourthatextendsoutsideCTV(nextslide)

EdiIngCTVBoost
Nowwehave2problems:1. TheenIre
mesorectumisnotincludedinourvolume– SOLUTION:Usepen/
brushtoexpandthevolume(finalCTVBoostindarkgreen)
2. ThecontourextendsoutsideCTV(andintobone!)– SOLUTION(nextslide)
CurrentCTVBooststructureshowninRED
CTVBoostCTV(inclnodes)

EdiIngCTVBoost
“Crop”contourthatextendsoutsideCTVàNOTE:SomeImesyouwillwanttocropwithanaddiIonalmargin(ie0.3cmmarginPTVtoskininH&N)

Step5:AddamarginforPTV
7-10mmmarginonCTVisusuallysufficienttoaccountforpelvicmoIonCTV+7mm=PTVà
We’vedonethisbefore…

AddamarginforPTV
“Marginforstructure”
NOTE:allmarginssame
REPEATthisstepforCTVboost

Sagi<al Coronal
Alwayscheckyourfinalvolumesinsagi<alandcoronalviewstomakesureyouhavecontouredavolumethatmakessensein3dimensions!BONUS:Youcancompareyourvolumesto“bonyanatomy”blocks(nextslide)Imagesreproducedfrom:h<ps://www.astro.org/uploadedFiles/_MAIN_SITE/Affiliate/ARRO/Resident_Resources/EducaIonal_Resources/ARROcase/Content_Pieces/ARROContourRectal.pdf

FORFUN:Drawblocks/MLCs!
Youwillneedtogoto“ExternalBeamPlanning”inyourtreatmentplanningsystemeContourà“Pearls”tabdescribesbordersfor3DconformalblocksNOTE:classicbordersfora3-fieldbeamarrangementwerebasedonBONYANATOMY.WithCTsimulaIon,wecancontourareasatrisk,anddecreaseourmargins.However,fancytreatmentplanning(withIMRT)didnotimproveoutcomesonRTOG0822(whichisDIFFERENTfromanalcancer).ThemarginfromPTVto“blockedge”(meaning,theshapeofyouMLCs)issuggestedtobeabout7mmbecausethedoseattheendofthefieldis~50%(requiressomebuild-upinIssuetogetto100%prescripIondose).

References• RTOGcontouringatlasforanorectal:
– h<ps://www.rtog.org/CoreLab/ContouringAtlases/Anorectal.aspx– NOTE:thiswascreatedforBOTHanalandrectalcancer,whicharetreated
quitedifferently,sopaya<enIon!– PublicaIonvalidaIngtheaboveatlas:Myersonetal.IJROBP2009:
h<p://www.ncbi.nlm.nih.gov/pubmed/19117696• RTOGprotocol
– RTOG0822actuallyshowednodifferencebetweenIMRTand3D-CRT.ThiscouldsIllbeareferencetoguidecontouringandplacementof3Dblocksperthe3D-CRTarm.
– h<ps://www.rtog.org/ClinicalTrials/ProtocolTable/StudyDetails.aspx?study=0822
• ARROContour:CAUTION!notpeer-reviewed,butaresidentpresentaIoncreatedbyARRO(ASTRO’sResidentCommi<ee)– h<ps://www.astro.org/uploadedFiles/_MAIN_SITE/Affiliate/ARRO/
Resident_Resources/EducaIonal_Resources/ARROcase/Content_Pieces/ARROContourRectal.pdf