recognition of primary immunodeficiency dr. andy gennery clinical reader/honorary consultant...
TRANSCRIPT

Recognition of Primary Immunodeficiency
Dr. Andy GenneryClinical Reader/Honorary Consultant
Paediatric Immunology + HSCT
Sept 2010

Joseph Priestly:
The more elaborate our means of communication, the less we communicate.

Immunodeficiency
‘a failure to achieve immune function to provide efficient, self-limited host defence against the biotic and abiotic environment while preserving tolerance to self.’
Casanova et al. J Allergy Clin Immunol 2005

Infection
Allergy
MalignancyAutoinflammatory disorders
Autoimmunity
• Infancy + early childhood - immune system encounters antigens for first time, mounting immune responses and acquiring memory.
The Problem

• Infancy + early childhood - immune system encounters antigens for first time, mounting immune responses and acquiring memory.
• Young children mix with other children in families or nursery
The Problem

• Infancy + early childhood - immune system encounters antigens for first time, mounting immune responses and acquiring memory.
• Young children mix with other children in families or nursery
• Exposed to many pathogens.
The Problem

• Infancy + early childhood - immune system encounters antigens for first time, mounting immune responses and acquiring memory.
• Young children mix with other children in families or nursery
• Exposed to many pathogens.
• Young children vulnerable to infection - recurrent infection is common.
The Problem
• Recurrent or persistent infection is major manifestation of primary immunodeficiency (PID).
The Problem

• Significant treatment advances make it important to recognize children with PID early, before significant end organ damage occurs to maximize opportunity for successful treatment.
The Problem

• Maternal IgG transferred to fetus during 3rd trimester via the placenta
• As maternal IgG decays intrinsic IgG responses develop
• As maternal IgG decays there is a physiological nadir between 3 - 6 months, which may be prolonged
Physiological immunodeficiency of immaturity

• Maternal IgG passed to foetus in last trimester
0
200
400
600
800
1000
1200
-8 -6 -4 -2 0 2 4 6 8 10 12
Months from birth
Immunoglobulin level (mg/100 ml)
Total
IgG
IgM
IgA

• Production of IgG2 (anti-polysaccharide responses) delayed in young children, explaining infant susceptibility to polysaccharide encapsulated organisms such as pneumococcus
Physiological immunodeficiency of immaturity
• Production of IgG2 (anti-polysaccharide responses) delayed in young children, explaining infant susceptibility to polysaccharide encapsulated organisms such as pneumococcus
• These responses mature between about 2–5 years of age, (may be delayed beyond this).
Physiological immunodeficiency of immaturity

Age

Organism
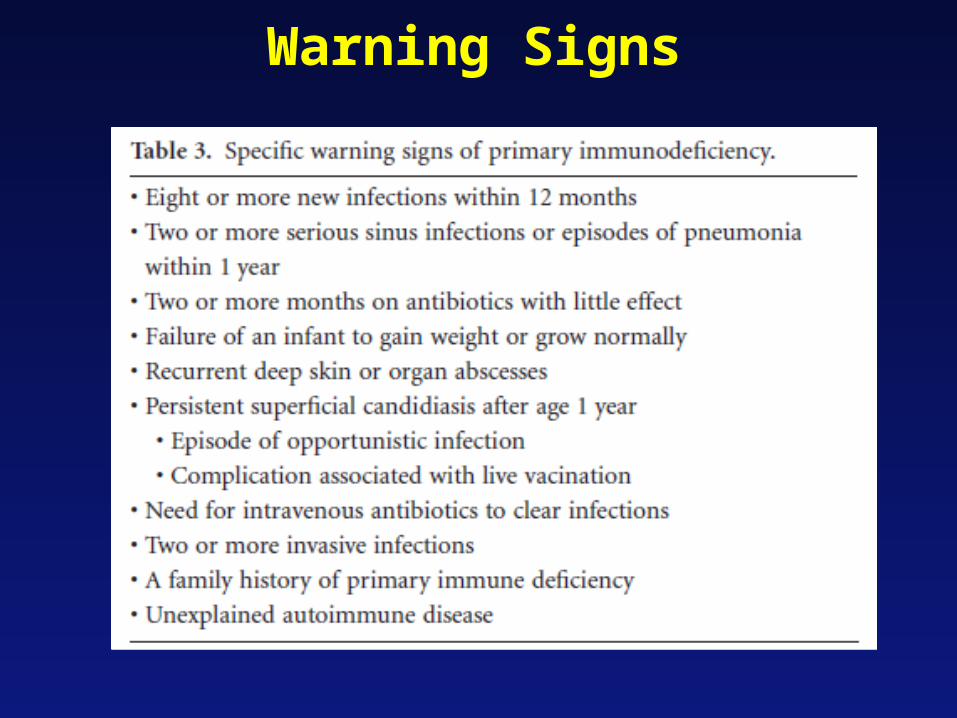
Warning Signs

RC., dob 03/2001
Referred Nov 2006 (prev. phone/advice):
• 2 episodes of Pneumococcal sepsis• Little response to single dose Prevenar• Good response to Pneumovax• ? Falling HiB specific antibody levels
For further investigation

Local hospital notes review
• Dec 2001– ? Meningitis
• CRP <1; ESR 21 mm/h• WCC 22x10e9/l (Ne 14.6); PLT 424x10e9/l• B/C; CSF; urine: -ve cultures • Urine: +ve Pneumococcal Ag
• March, May, Nov 2002- fitting episodes
• Dec 2003– Lethargic, fever
• CRP 212• WCC 32x10e9/l (Ne 29)• B/C – Strep. Pneumoniae (strain 18C)

Investigations(on Penicillin prophylaxis => Trimethoprim)
• Jan 2004– Normal IgG, A, M; IgG subclasses– Tet 0.05 (>0.1 IU/ml)– HiB <0.1 (>1 mg/l)– Pneumo 23 (>20 mg/l)
• Aug 2004 (after Tet/HiB boost)– Tet 0.24– HiB >9– Pneumo 10
• Oct 2004 – Prevenar (conj. Pneumococcal vacc.)
• July 2005– Tet 0.19– HiB 1.1– Pneumo 13– Measles, Rubella +ve – Mumps equivocal
• July 2006 - Pneumovax (polysaccharide-only Pn. vacc.)
• Oct 2006– Tet 0.27– HiB 0.2– Pneumo 100
• Abdominal US – present spleen
• Complement function (C+A) normal
• Serum sample before Prevenar sent to Manchester for Pneumococcal strain-specific antibody responses
• ? Serum to Manchester post-Prevenar
Lakshman R et al. ADC, 2003
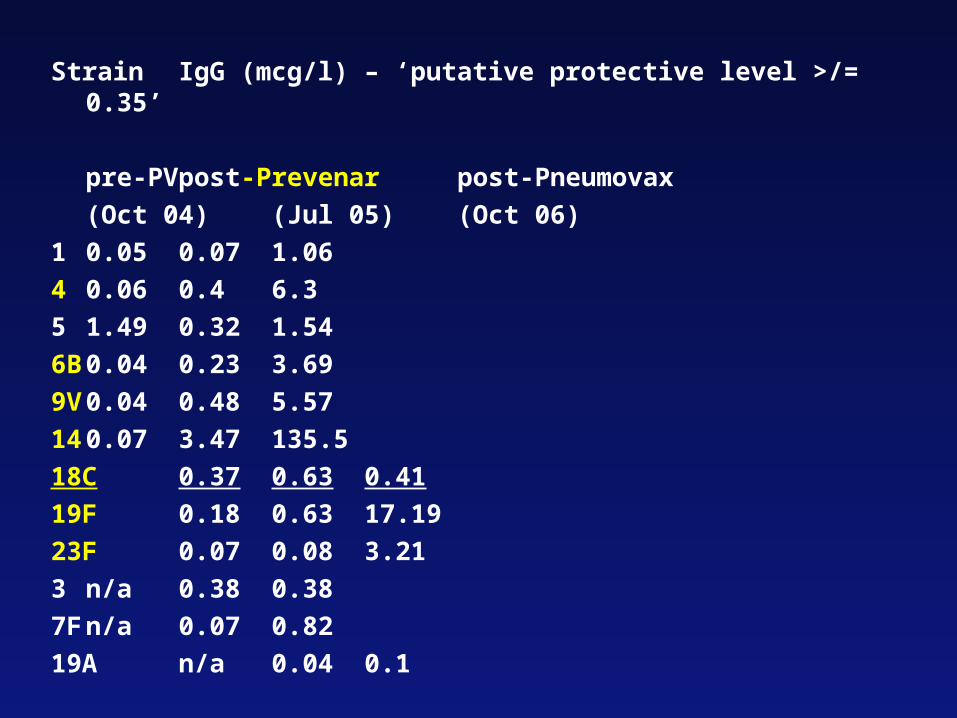
Strain IgG (mcg/l) – ‘putative protective level >/= 0.35’
pre-PV post-Prevenar post-Pneumovax
(Oct 04) (Jul 05) (Oct 06)
1 0.05 0.07 1.06
4 0.06 0.4 6.3
5 1.49 0.32 1.54
6B 0.04 0.23 3.69
9V 0.04 0.48 5.57
14 0.07 3.47 135.5
18C 0.37 0.63 0.41
19F 0.18 0.63 17.19
23F 0.07 0.08 3.21
3 n/a 0.38 0.38
7F n/a 0.07 0.82
19A n/a 0.04 0.1

Clinics Dec 2006/Feb 2007
• Well grown• No infections• Big tonsils, peripheral LN
• Specific Pneumococcal Ab Deficiency
• Talked to parents– Penicillin prophylaxis FOR LIFE– ? Further Ix for underlying PID
Local hospital notes review
• Dec 2001– ? Meningitis
• CRP <1; ESR 21 mm/h• WCC 22x10e9/l (Ne 14.6); PLT 424x10e9/l• B/C; CSF; urine: -ve cultures • Urine: +ve Pneumococcal Ag
• March, May, Nov 2002- fitting episodes
• Dec 2003– Lethargic, fever
• CRP 212• WCC 32x10e9/l (Ne 29)• B/C – Strep. Pneumoniae (strain 18C)

RC., dob 03/2001
2 episodes of Pneumococcal sepsis
For further investigation
AG 06/2008• 39/52, No problems
• Swelling L face + ear 5/52 - mastoiditis
• WCC 71, N 54, L 5, plt 651
• CT brain normal
• No growth
• Oral candida since 4/52

AG 06/2008• Lymph subsets normal
• Neutrophil oxidative burst normal

AG 06/2008• Leukocyte Adhesion Deficiency

AG 06/2008• Swelling L face + ear 5/52 - mastoiditis
• Oral candida since 4/52
• WCC 71, N 54
• Careful history – delay in loss of umbilical stump

JT 04/2003
• Normal birth
• Well until 6/52
• Staph aureus septicaemia 6/52
• ‘icthyotic erythroderma’
• lymphadenopathy

JT 04/2003
• Pseudomonas ear infection
• Pneumococcal meningitis
• Rotavirus enteritis
• 10/12 O/E fine hair• Thickened eczema• LN++• 3 cm liver

JT 04/2003
• Mainly OK!!
• IgG 4, IgM 0.3
• Low tet/Hib - responded to vaccine boost
• ??? Some sort of immunodeficiency???
• Start IVIG

JT 04/2003
• Defect in NEMO - NF kappa B essential modulator

JT 04/2003
• Normal birth
• Well until 6/52
• Staph aureus septicaemia 6/52
• ‘icthyotic erythroderma’
• lymphadenopathy

JT 04/2003
• Pseudomonas ear infection
• Pneumococcal meningitis
• Sometimes diagnosis becomes clear over time!!
AD 09/2008
• 2nd child, unrelated parents
• Well until 3 months - bronchiolitis (hMPV)• Admitted - no symptom resolution• Cough continued
AD 09/2008
• Re-admission 2 months later - pneumonia - hMPV• Continued chestiness, O2 requirement• Weight loss
• Referred age 7/12
• Hypogammaglobulinaemia, lymphopenia

AD 09/2008
• 2nd child, unrelated parents
• Well until 3 months - bronchiolitis (hMPV)• Lymphopenic• Admitted - no symptom resolution• Cough continued
AD 09/2008
• Re-admission 2 months later - pneumonia - hMPV• Continued chestiness, O2 requirement• Weight loss
• Referred age 7/12
• Hypogammaglobulinaemia, lymphopenia
DC 02/2010
• 3 yr boy, 2nd of 3 boys
• No FH of note
• Neonatal history unremarkable
DC 02/2010
• 48hr h/o L neck swelling, fever, rash, red tongue, cracked lips.
• ? Kawasaki disease
• Rx antibiotics, IVIG
DC 02/2010
• Fever settled
• X 3 episodes fever @ night, sweats
• Odd gait
• ? Kawasaki disease/JIA overlap

DC 02/2010
• M/P x 3 - better
• Symptoms recurred - fever, limp, sweats
• L Cx LN swelling - pointing

DC 02/2010
• I+D
• home
• Burkholderia cepacia grown from LN



DC 02/2010
• 3 yr boy, 2nd of 3 boys
• No FH of note
• Neonatal history unremarkable
DC 02/2010
• 48hr h/o L neck swelling, fever, rash, red tongue, cracked lips.
• ? Kawasaki disease
• Rx antibiotics, IVIG
DC 02/2010
• Fever settled
• X 3 episodes fever @ night, sweats
• Odd gait
• ? Kawasaki disease/JIA overlap
DC 02/2010
• M/P x 3 - better
• Symptoms recurred - fever, limp, sweats
• L Cx LN swelling - pointing

DC 02/2010
• I+D
• home
• Burkholderia cepacia grown from LN

Clues!
• Age
• FH
• Organism– Pneumocystis jerovici– Invasive S. aureus infection or Burkholderia cepacia
septicaemia– Aspergillus (fungal) pneumonia– Aspergilloma (S. aureus pneumonia)– EBV-associated lymphoma
– Disseminated atypical mycobacterial infection
– Recurrent meningococcal infection
• Organ specific features

Who to Investigate?
• difficult - infection in childhood is very common!
• High index of clinical suspicion is needed
• Compared with other children, an immunodeficient child is likely to have:– more infections that take longer to resolve or have
an atypical course– Infections with common organisms may run an
unusually severe course, e.g. haemorrhagic chickenpox, or fail to respond to standard treatments
Who to Investigate?
• Infection should be taken in context with other findings in history & examination and FH
• When evaluating the number of infections, other factors:– parental smoking, – attendance at nursery – anatomical problems
should be considered.

Predictive value of the 10 warning signs in children with primary immunodeficiency (PI)
160 (37%) of 430 children with defined PI had • less than two of 10 warning signs of PI
• Only 18 (4%) were referred by primary care physicians, remainder came via hospital specialists (? Who referred there).
• Analysing PI as a single entity, only 3/10 warning signs (family history, oral antibiotics and failure to thrive) positively predicted patients with defined PIs.
Subbarayan A, Colarusso G, Gennery AR, Hughes S, Slatter M, Cant AJ, Arkwright PD, European Society of Immunodeficiencies, Istanbul, October 2010
Compared with patients where no defined PI was found, patients with all PI types were more likely to have
• a family history
• had a prolonged course of oral antibiotics.
• T-cell PI associated with thrush and FTT but less sinus and ear infections.
• Complement PI associated with the highest prevalence of deep-seated bacterial infections
• Neutrophil PIs associated with the highest risk of recurrent abscesses and IV antibiotic use.
Predictive value of the 10 warning signs in children with primary immunodeficiency (PI)
Subbarayan A, Colarusso G, Gennery AR, Hughes S, Slatter M, Cant AJ, Arkwright PD, European Society of Immunodeficiencies, Istanbul, October 2010
Critical Messages
• Consider immunodeficiency
• Other clues?
• Don’t dismiss non-pathogenic organisms
• Treat with broad spectrum agents
• Multi-agent treatment:– Resistance
– Multiple organisms
George Bernard Shaw:
The problem with communication ... is the illusion that it has been accomplished.
Take Home Message• Talk to each other
– about the patient– about possible diagnoses– about likely microbes – is serotype important– tissue diagnosis – what tests?– ? Any special microbiological tests– ? Role of PCR (nb serology unhelpful)– about appropriate treatment– how long? (long usually)– alternative treatments

Immunodeficiency
‘a failure to achieve immune function to provide efficient, self-limited host defence against the biotic and abiotic environment while preserving tolerance to self.’
Casanova et al. J Allergy Clin Immunol 2005

Any individual
presenting with infection is immunodeficient (at that moment)

Not
‘Who should be investigated for primary immunodeficiency?’

Rather
‘What are the reasons for
not investigating this child further?’
