recognition and management of bradyarrhythmias and tachyarrhythmias ms lalith sivanathan
TRANSCRIPT
Recognition and management of Bradyarrhythmias and Tachyarrhythmias
Ms Lalith Sivanathan
OBJECTIVES
• Recognize unstable conditions requiring urgent intervention
• Differentiate supraventricular tachycardia (SVT) from sinus tachycardia
• Differentiate initial steps to stabilize the child who is unstable as a result of arrhythmias
• Describe indications for vagal maneuvers used for treatment of SVT with adequate perfusion
• Describe when and how to provide electrical therapy for arrhythmias with a pulse synchronized cardioversion attempts or pacing
BRADYARRHYTHMIAS
• Bradycardia is defined as a heart rate that is slow compared with the normal heart rates for the patient’s age.• Primary bradycardia
• Is a result of congenital and acquired heart conditions that directly slow the spontaneous depolarisation rate of the normal pacemaker cells
• Secondary bradycardia• Is the result of conditions that alter the
normal function of the heart (causes – hypoxia, acidosis, hypotension, hypothermia and drug effects)
SYMPTOMS• Change in the level of consciousness• Dizziness• Syncope• fatigue• Cardinal signs
• Shock with hypotension• Poor end-organ perfusion• Sudden collapse
• A very slow heart rate can cause shock from inadequate cardiac output. The child is potentially unstable if deterioration to shock or cardiac arrest is likely
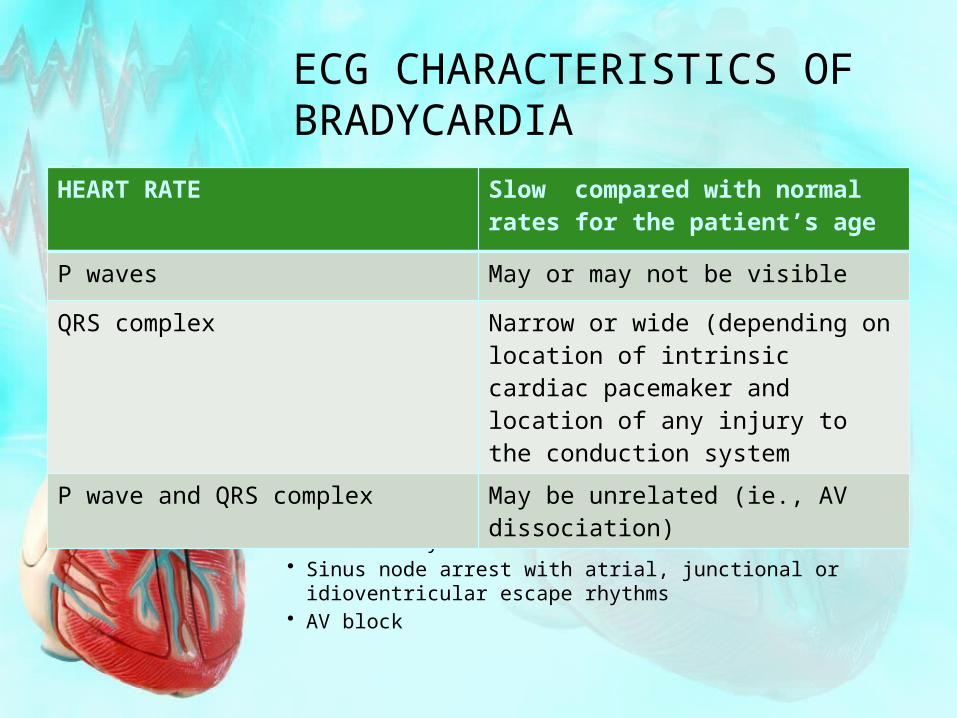
ECG CHARACTERISTICS OF BRADYCARDIA
• Examples of bradyarrythmias• Sinus bradycardia• Sinus node arrest with atrial, junctional or idioventricular
escape rhythms• AV block
HEART RATE Slow compared with normal rates for the patient’s age
P waves May or may not be visible
QRS complex Narrow or wide (depending on location of intrinsic cardiac pacemaker and location of any injury to the conduction system
P wave and QRS complex May be unrelated (ie., AV dissociation)
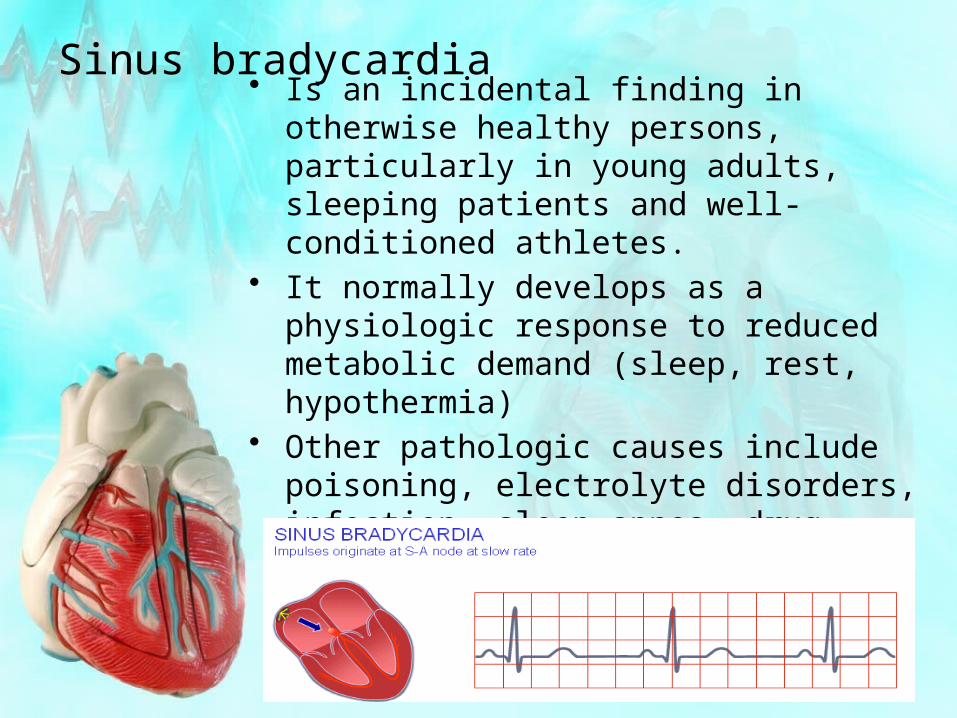
Sinus bradycardia• Is an incidental finding in otherwise healthy
persons, particularly in young adults, sleeping patients and well-conditioned athletes.
• It normally develops as a physiologic response to reduced metabolic demand (sleep, rest, hypothermia)
• Other pathologic causes include poisoning, electrolyte disorders, infection, sleep apnea, drug effects, hypoglycemia, hypothyroidism and increased ICP
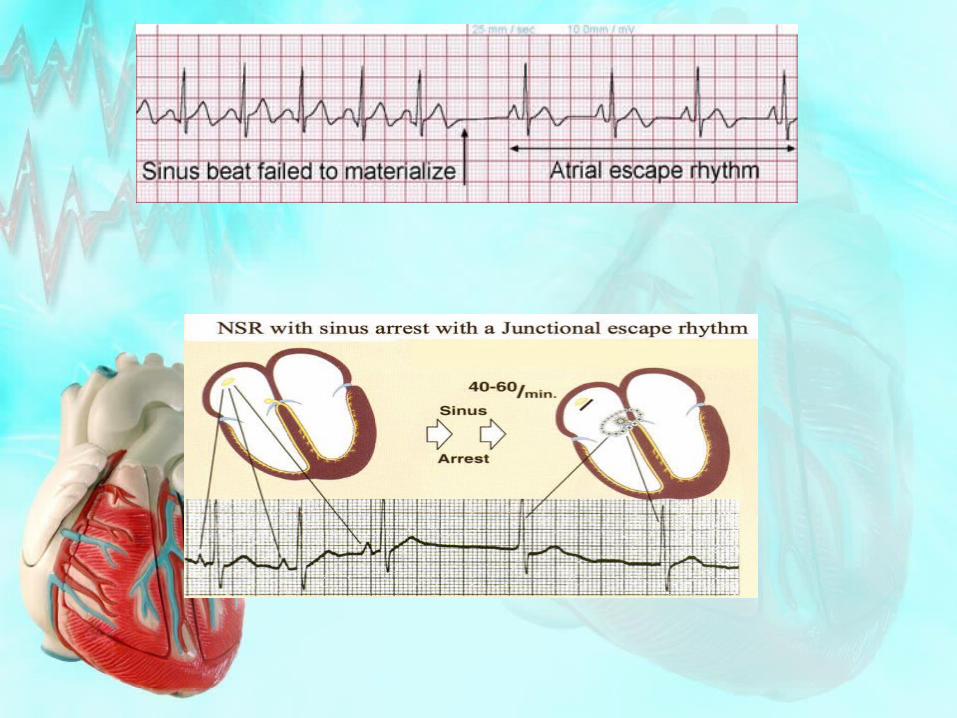
Sinus node arrest
• It is characterized by absent pacemaker activity in the sinus node, In such care a subsidiary pacemaker in the atrium, AV junction or ventricles may initiate cardiac depolarization, resulting in• Atrial escape rhythm
• Impulse arise from subsidiary non sinus atrial pacemaker (late P wave)
• Junctional escape rhythm• The rhythm originates in the AV node
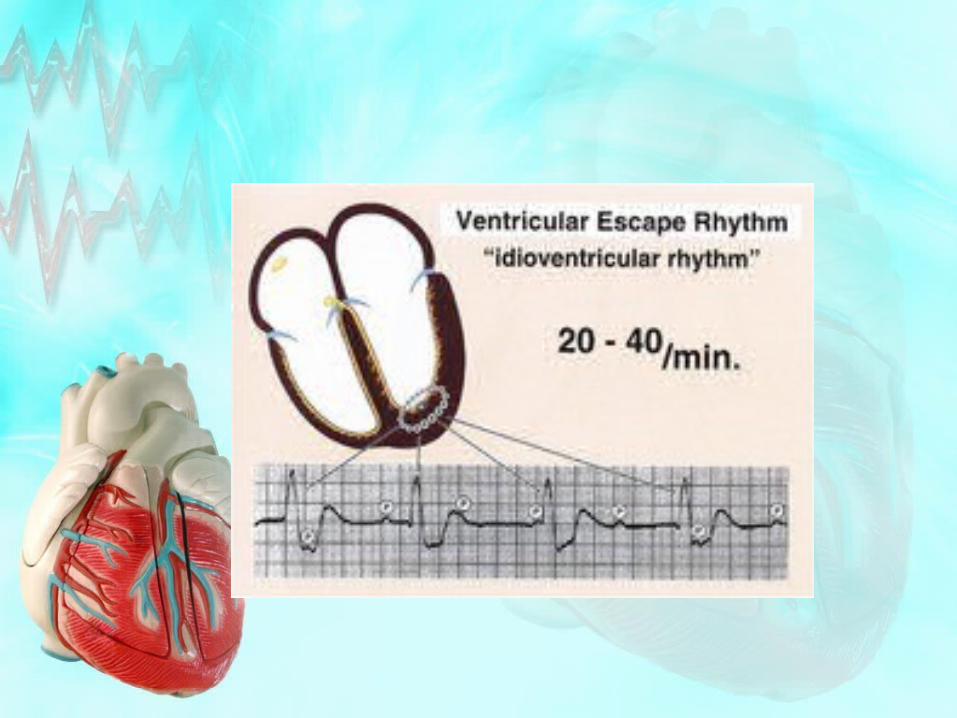
(narrow QRS complex)• Idioventricular rhythm
• The rhythm originates in the ventricles
AV Block• AV block is a disturbance of electrical conduction through
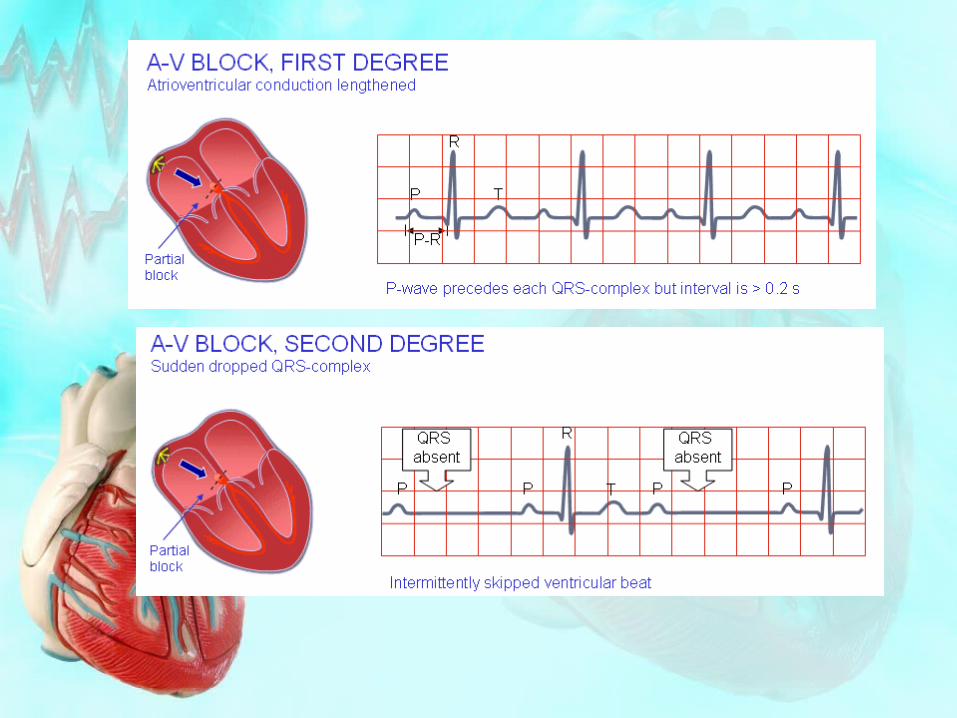
the AV node. AV block is classified as• First degree
• Prolonged PR interval representing slowed conduction through AV node
• Second degree• Some but not all atrial impulses are conducted to
the ventricles• Mobitz I (Wenckebach) – occurs at the AV
node, One P is not followed by QRS• Mobitz II – occurs below the level of AV node
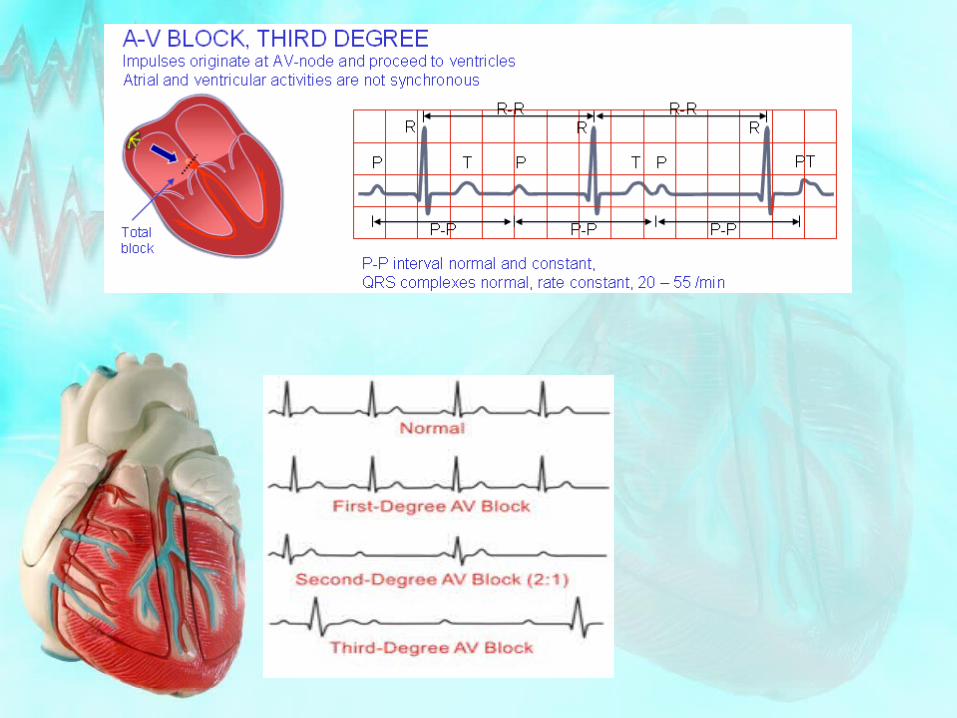
• Third degree• None of the atrial impulses is conducted to the
ventricle. Complete heart block or complete AV block
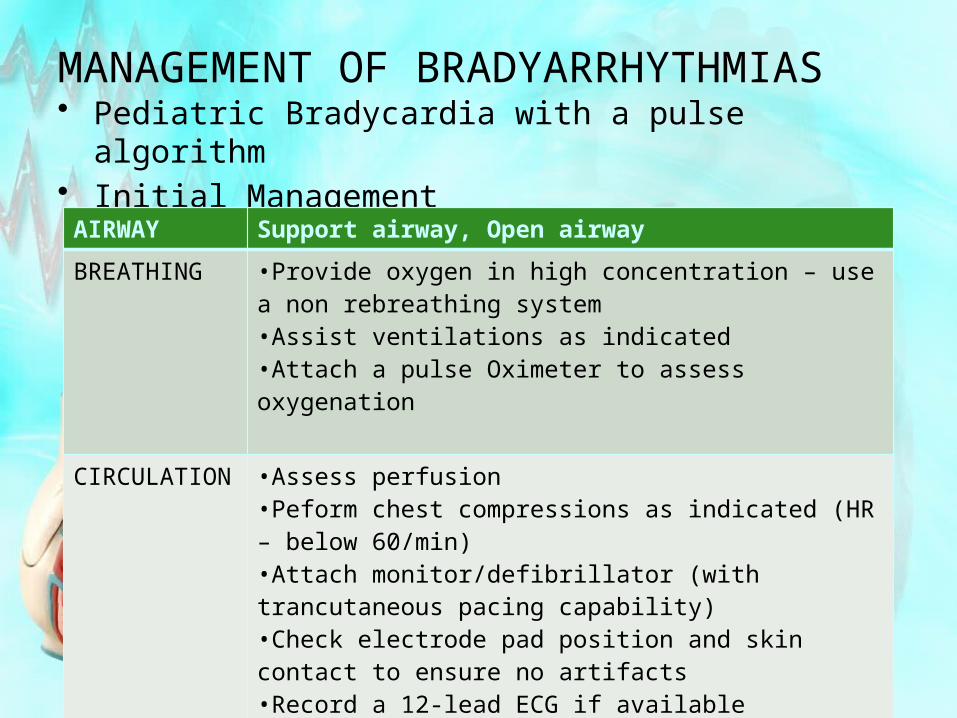
MANAGEMENT OF BRADYARRHYTHMIAS• Pediatric Bradycardia with a pulse algorithm• Initial Management
AIRWAY Support airway, Open airway
BREATHING •Provide oxygen in high concentration – use a non rebreathing system•Assist ventilations as indicated•Attach a pulse Oximeter to assess oxygenation
CIRCULATION •Assess perfusion•Peform chest compressions as indicated (HR – below 60/min)•Attach monitor/defibrillator (with trancutaneous pacing capability)•Check electrode pad position and skin contact to ensure no artifacts•Record a 12-lead ECG if available•Establish vascular access•Obtain appropriate lab studies (K, Ca, Mg, Blood gas PH)
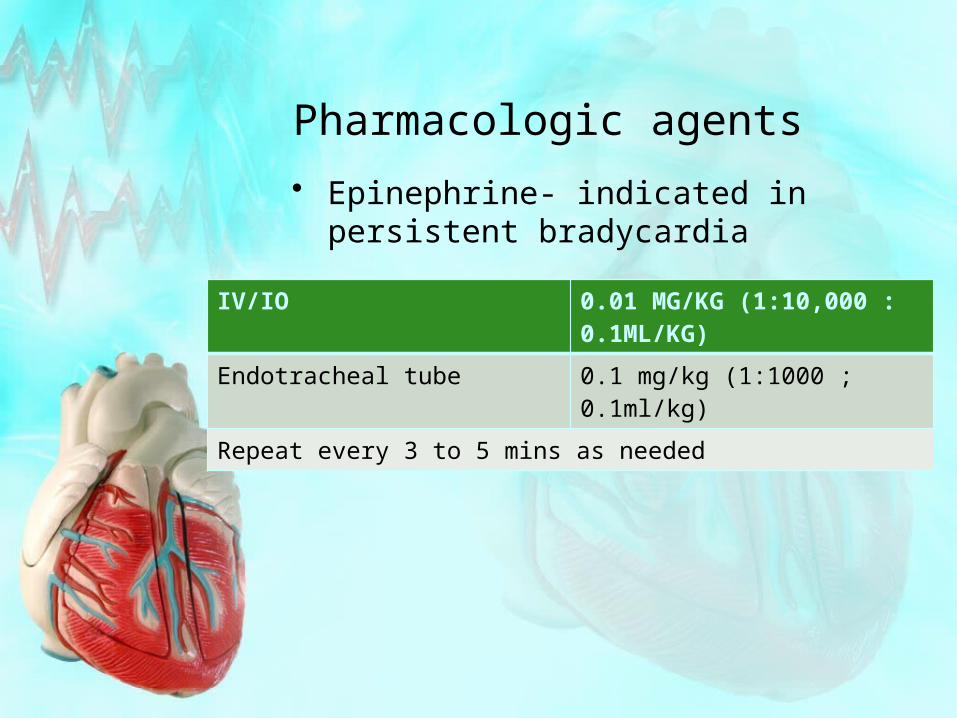
Pharmacologic agents
• Epinephrine- indicated in persistent bradycardia
IV/IO 0.01 MG/KG (1:10,000 : 0.1ML/KG)
Endotracheal tube 0.1 mg/kg (1:1000 ; 0.1ml/kg)
Repeat every 3 to 5 mins as needed
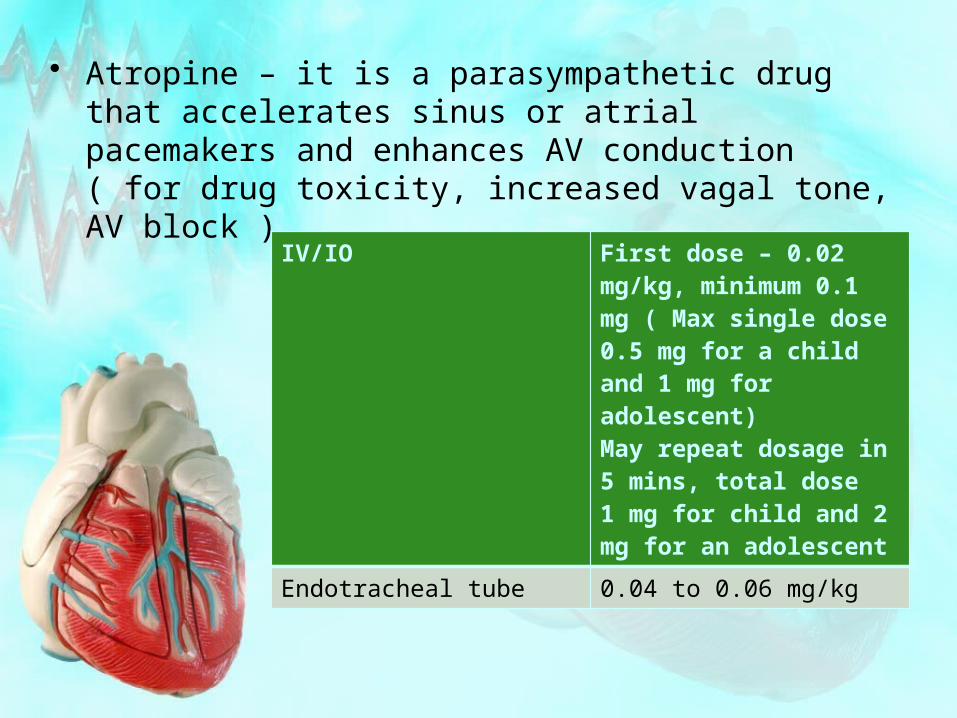
• Atropine – it is a parasympathetic drug that accelerates sinus or atrial pacemakers and enhances AV conduction ( for drug toxicity, increased vagal tone, AV block )
IV/IO First dose – 0.02 mg/kg, minimum 0.1 mg ( Max single dose 0.5 mg for a child and 1 mg for adolescent)May repeat dosage in 5 mins, total dose 1 mg for child and 2 mg for an adolescent
Endotracheal tube 0.04 to 0.06 mg/kg
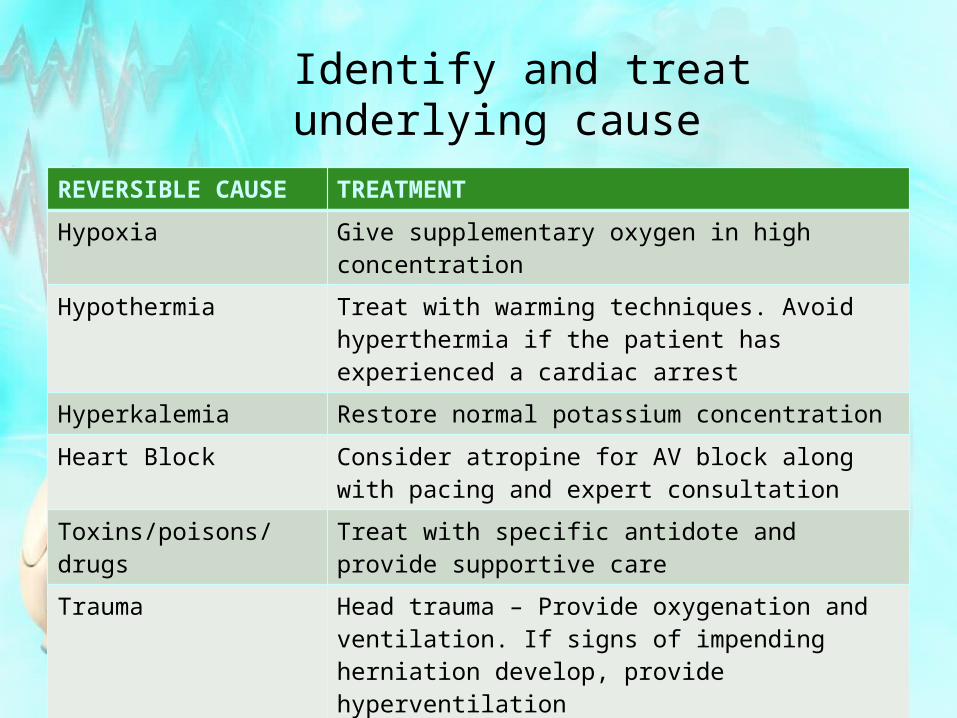
Identify and treat underlying cause
REVERSIBLE CAUSE TREATMENT
Hypoxia Give supplementary oxygen in high concentration
Hypothermia Treat with warming techniques. Avoid hyperthermia if the patient has experienced a cardiac arrest
Hyperkalemia Restore normal potassium concentration
Heart Block Consider atropine for AV block along with pacing and expert consultation
Toxins/poisons/drugs Treat with specific antidote and provide supportive care
Trauma Head trauma – Provide oxygenation and ventilation. If signs of impending herniation develop, provide hyperventilation
TACHYARRHTHMIAS
• It is defined as a heart rate that is fast compared with normal heart rates for the patient’s age
• Cardinal signs:• Respiratory distress/failure often due to
pulmonary edema (lung tissue disease)• Shock with hypotension or poor end –
organ perfusion• Altered consciouness• Sudden collapse with rapid detectable
pulses
Tachycardic rhythmsIt may be classified according to the width of the QRS complex
NARROW COMPLEX WIDE COMPLEX
•Sinus tachycardia•Supraventricular tachycardia•Atrial flutter
•Ventricular tachycardia•Supraventricular tachycardia with aberrant intraventricular conduction
• Sinus tachycardia – is defined as a rate of sinus node discharge faster than normal for the patient’s age (causes – hypoxia, hypovolemia, fever, metabolic stress, injury, pain, anxiety, toxins, drugs, anemia)
• Supraventricular tachycardia is abnormally fast rhythm originating above the ventricles. SVT is the most common tachyarrhythmia producing cardiovascular compromise during infancy• Common signs in infants are poor feeding,
rapid breathing, irritability, unusual sleepiness, pale or blue skin, vomiting
• In older children – palpitations, shortness of breath, chest pain, dizziness, lightheadedness and fainting
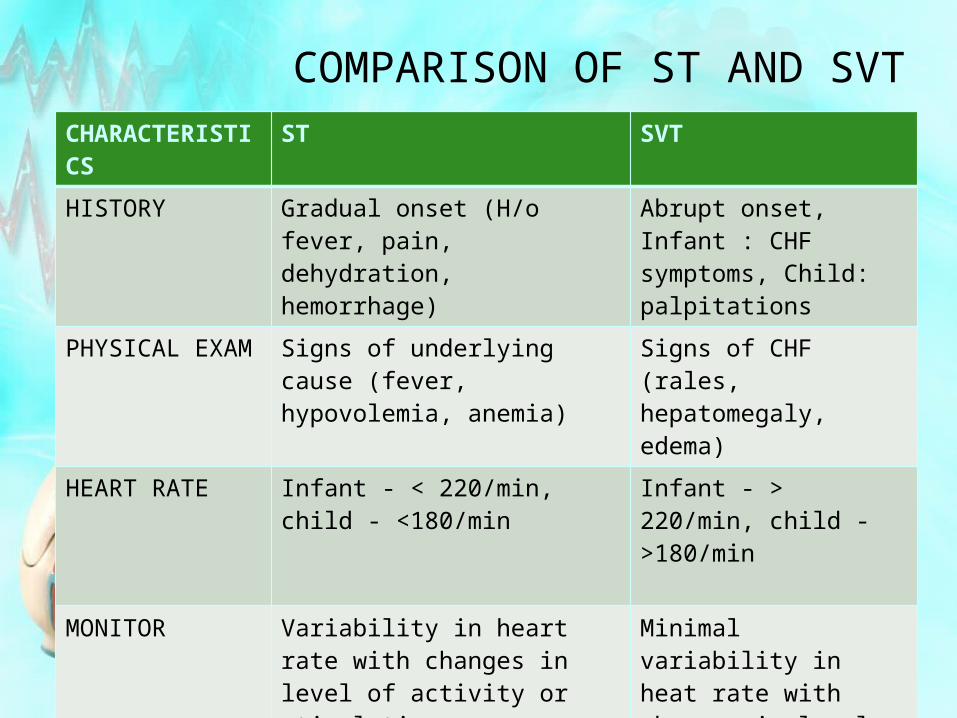
COMPARISON OF ST AND SVTCHARACTERISTICS
ST SVT
HISTORY Gradual onset (H/o fever, pain, dehydration, hemorrhage)
Abrupt onset, Infant : CHF symptoms, Child: palpitations
PHYSICAL EXAM Signs of underlying cause (fever, hypovolemia, anemia)
Signs of CHF (rales, hepatomegaly, edema)
HEART RATE Infant - < 220/min, child - <180/min
Infant - > 220/min, child - >180/min
MONITOR Variability in heart rate with changes in level of activity or stimulation
Minimal variability in heat rate with changes in level of activity or stimulation
ECG P waves present/ normal P waves absent/abnormal
CHEST X-RAY Usually small heart and clear lungs
Signs of CHF (pulm edema may be present)
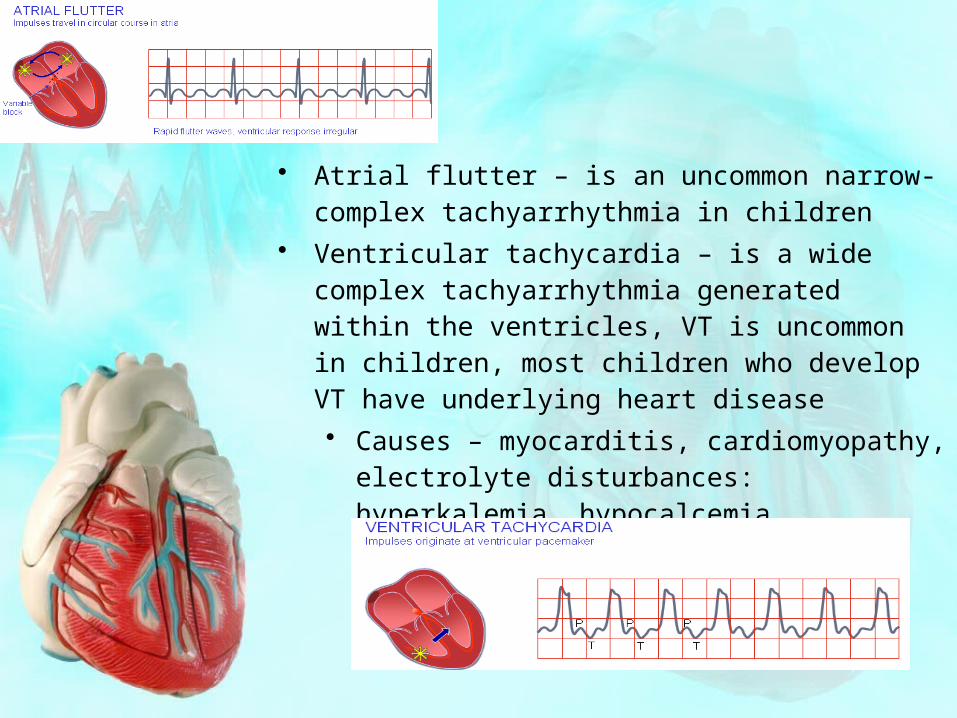
• Atrial flutter – is an uncommon narrow-complex tachyarrhythmia in children
• Ventricular tachycardia – is a wide complex tachyarrhythmia generated within the ventricles, VT is uncommon in children, most children who develop VT have underlying heart disease• Causes – myocarditis, cardiomyopathy,
electrolyte disturbances: hyperkalemia, hypocalcemia, hypomagnesemia and drug toxicity)
MANAGEMENT OF TACHYARRHYTHMIAS
• Initial Management• Support ABCs and oxygenation as
needed• Establish monitoring• Establish vascular access• Obtain lab studies (k, glucose, ca, mg,
etc)• Assess neurologic status• Treat hypothermia• Anticipate need for appropriate
medications
Vagal maneuvers
• In normal infants and children the heart rate falls when the vagus nerve is stimulated, In patients with SVT, vagal stimulation may terminate the tachycardia by slowing the conduction through the AV node
CARDIOVERSION
• Electrical cardioversion can be frightening and painful for a child, establish vascular access and provide preprocedural sedation
• For syn cardioversion – use a first dose of 0.5 to 1 J/kg for SVT or VT with pulse. Increase the dose to 2J/kg if initial dose is ineffective, then all remaining shocks at 2 J/kg
PHARMACOLOGIC THERAPY
• Adenosine (Blocks conduction through AV node temporarily)– 0.1 mg/kg (max first dose 6 mg) by rapid bolus, max second dose 12 mg
• Amiadarone(vasodilatation and Av node suppresion) – 5 mg/kg IV over 20 to 60 mins
• Procainamide (antiarrhythmic agent) 15 mg/kg IV over 30 to 60 mins
• Lidocaine (sodium channel blocker) – 1 mg/kg bolus
• Infuse loading doses slowly in a stable patient to avoid hypotension. Monitor blood pressure frequently during administration
Summary
• Recognize unstable conditions requiring urgent intervention
• Differentiate supraventricular tachycardia (SVT) from sinus tachycardia
• Differentiate initial steps to stabilize the child who is unstable as a result of arrhythmias
• Describe indications for vagal maneuvers used for treatment of SVT with adequate perfusion
• Describe when and how to provide electrical therapy for arrhythmias with a pulse synchronized cardioversion attempts or pacing
Thank you…