recent advances and trends in the management of locally
TRANSCRIPT

Recent Advances and Trends in the Management of Locally Advanced
Pancrea9c Cancer Incremental Progress
JillLacy,MDFeb2018
Disclosures
CelgeneAstraZenecaNavigantKeyquest
JillLacy,MD
Teaching points
• DefiniAonsand“staging”evaluaAon• Management
• improvingoutcomes• consensusguidelines• unresolvedissues
• ResponseassessmentinpaAentselecAonforsurgery• ChallengesandfuturedirecAons

Locally Advanced Pancrea9c Cancer (LAPC)
• 30-40%ofpaAentswithnewlydiagnosedpancreaAccancerpresentwithnon-metastaAclocallyadvancedunresectabledisease(LAPC)
• Historically,survivalmarginallybeTerthanmetastaAcPC,<12mo• Historically,negligible%ofpaAentswereabletoundergosurgery,<5%• PaAentssuffersignificantmorbidityreferabletolocaltumorburden• PaTernsoffailureandbiologynotwellunderstood*
• <30%non-metastaAc(5/18)• >70%metastaAc(13/18)
*JClinOncol2009Apr10;27(11):1806-13

LAPC:DefiniAon
• Non-metastaAcPCcomprisedofconAnuumfromresectabletounresectablebasedoninvolvementofadjacentvascularstructures
• ConsensusorganizaAonshavedefinedanatomiccriteriawhichdelineatethreecategoriesofnon-metastaAcPC:– resectable– borderlineresectable– locallyadvancedunresectable
• DefiniAonsprovideguidanceformanagementandneededforclinicaltrials• BUTarenotuniformandsubjecttointer-observervariability
LocallyAdvancedUnresectablePancreaAcCancer:Weknowitwhenweseeit
EncasementofSMAorceliacaxis* OR
ExtensiveinvolvementofSMVand/orPVthatprecludesresecAonand/orreconstrucAon
AND
NoevidenceofmetastaAcdiseaseincludingmetastaAcnon-regionalLNs*Encasement:>180ocontact
DefiniAonofLAPCNCCNVersion3.2017
• Nodistantmetastases• Head/uncinateprocess
– SolidtumorcontactwithSMAorCA>180o(encasement)– SolidtumorcontactwithfirstjejunalbranchofSMA– UnreconstructableSMV/PVduetotumorinvolvementorocclusion(tumororblandthrombus)– ContactwithmostproximaldrainingjejunalbranchintoSMV
• Body/tail– SolidtumorcontactwithSMAorCA>180o(encasement)– UnreconstructableSMV/PVduetotumorinvolvementorocclusion(tumororblandthrombus)– ContactwithCAandaorAcinvolvement
BorderlineResectablePancreaAcCancerontheconAnuumofvascularinvolvement
MorelimitedvascularinvolvementthanLAPCandtechnicallymayberesectableBUT:• HighriskforaposiAvemarginofresecAon(R1resecAon)• RequiresmorecomplexoperaAonw/vascularresecAonandreconstrucAon,withhighermorbidity
• MulApleanatomicdefiniAonshavebeenproposedandused• DefiniAonsareomeninsAtuAonand/oroperatordependent.

Borderline Resectable: Lack of Uniform Criteria
Criteriadiffer:-ExtenttowhichtumorinvolvementofSMV-PVdiscriminatesborderlineresectablefromresectable-ExtenttowhichinvolvementofceliactrunkdiscriminatesborderlineresectablefromLAPC

WhatisBorderlineResectablePancreaAcCancer?ASCOGuidelinesPanelApproach:“punt”
• CategorizesiniAaldiagnosesasthoseforwhomupfrontsurgeryisrecommendedversusthoseforwhompreoperaAvetherapyisrecommendedbeforeresecAon.
• ThiscategorizaAoncapturestheoncologyprovider’sintentinreducingtherateofincompleteresecAon
• Haschosennottousetheterms“resectable”and“borderlineresectable.”• ConAnuestosupporttheuseofthesetermsinthecontextofclinicaltrials,where
cleardefiniAonsofeligibilityarenecessary.
Khorana,etal.JClinOncol2016Jul20;34(21):2541-56
AJCC Staging vs Prac9cal Clinical Staging
• AJCCstagingsystemdoesnotaddressresectability
• NCCN:Forclinicalstagingpurposes,useafour-AerclinicalclassificaAonsystembasedimagingstudies:(1)Resectable(2)Borderlineresectable(3)Locallyadvancedunresectable(4)Disseminated

• CTscanchest/abd/pelvis- ProvidesstagingintermsofmetastaAcvsnon-metastaAc
• Ifnomets:repeatCTwithbiphasic“pancreaAcprotocolCT”toassessvascularinvolvement/resectability- FindingsonpancreaAcprotocolmaychangemanagementin>50%ofpts
• EUS- ComplementsCTinassessingvascularinvolvement,espportalvein- Biopsy(required)
• DiagnosAclaparoscopywithperitonealwashingsinselectedpaAents- ConsiderinpaAentswithhighCA19-9inwhomsurgerymaybeconsidered
DiagnosisandEvaluaAon:Imagingiskey
DiagnosisandEvaluaAon:MulAdisciplinaryDiscussionisKey
NCCNGuidelines:BlackBoxWarning!
ManagementofLocallyAdvancedPancreaAcCancer

LAPCManagement:CurrentStateofAffairs
• OpAmalmanagementiscontroversial• NointernaAonally-embracedstandardapproach.• IniAalchemotherapywithacombinaAonregimeninfitpaAentsisthecurrentrecommendaAonofNCCNandASCO*
• Butnoclearevidencetosupportoneregimenoveranother• LimitedprospecAvedatawith“modern”chemotherapy
*JClinOncol2016Aug1;34(22):2654-68

LAPCManagement:ManyUnresolvedQuesAons• WhatisopAmuminiAalchemotherapyregimen?
– FOLFIRINOXvsGem/Abraxanevsotherdilemma?
• WhatisopAmumduraAonofchemotherapy?– Roleofmaintenancechemotherapy?
• Whatisroleofpost-chemotherapyradiaAon?– Doesitconferasurvivalbenefit?– DoesitconferaPFSorQOLbenefit?– WhichRTtechniqueanddoseisbest?

LAPCManagement:ManyUnresolvedQuesAons
• Whatistheroleofsurgery?– WhoshouldundergosurgicalexploraAon(local-onlybiology)?– Canwepredictresectablediseaseamer”neoadjuvant”therapy?– Doessurgeryconferasurvival,PFS,orQOLbenefit?– Doessurgerycureanyone?

LAPCManagement:MeaningfulProgress
• Priorto2010,survival<11monthswithgemcitabine-basedchemo• FOLFIRINOX*hashadmeaningfulimpactonoutcomesofLAPC• MulApleretrospecAveseries,oneprospecAvetrial2andonemeta-analysis3havedemonstratedmediansurvival>24monthswithupfrontFOLFIRINOX
• 25to>40%abletoundergoresecAonamerFOLFIRINOX• Emergingexperiencewithgemcitabine/nab-paclitaxelencouraging
1Steinetal.BrJCancer.2016Mar29;114(7):737-432Sukeretal.LancetOncol.2016Jun;17(6):801-10
*Folinicacid,Flourouracil,Irinotecan,OxaliplaAn.FOLFIRINOXvGemformetastaAcPC.NEJM.2011;364:1817-25
FOLFIRINOXforlocallyadvancedpancreaAccancer:asystemaAcreviewandpaAent-levelmeta-analysis
Sukeretal.Lancet Oncol 2016; 17: 801–10 .• 13studiesw/315ptswithLAPCwhoreceivedFOLFIRINOX
• 63%alsoreceivedradiotherapy• 26%underwentsurgery(74%R0resecAons)• Medianoverallsurvival24.2mo• SurvivalsubstanAallybeTerthanhistoricalcontrolswithLAPC• SurvivalcomparesfavorablywithsurvivalofresectedpaAents


FOLFIRINOXinLAPC:YaleTrialDesignStein.BrJCancer2016
LocallyAdvancedandBorderlinePC(NCCNcriteria)
ConAnueFOLFIRINOX*
RadiaAonwithconcurrent
chemotherapy*SurgicalResecAon
mFOLFIRINOXx8cyclesCTscanamercycle4and8*
Ifstableorrespondingamer8cycles,addiAonaltreatmentperinvesAgator’sdiscreAon
*SurgeryallowedifdeemedresectablebeforecompleAonofinducAonFOLFIRINOXorameraddiAonaltherapy
Primaryendpoint:PFSSecondaryendpoints:• RR• OS• ResecAonrate

FOLFIRINOXinLAPC:YaleResultsStein.BrJCancer2016
DisconAnuedFOLFIRINOXpriortocompleAng8cycles CompletedFOLFIRINOXinducAon
ReasonsforFOLFIRINOXdisconAnuaAon:-Withdrew,2paAents-OptedforchemoRT(stabledisease),4pts-Treatmentdelays,5ptsUnresolvedinfecAon,2ptsAdverseevents,3pts
11pts35%
20pts*65%
PaAentDisposiAonDuringFOLFIRINOXInducAon
*Includes4ptsdeemedresectablepriorto8cycles

FOLFIRINOXinLAPC:YaleResults
• 31paAentsinlocallyadvancedcohort• ResponsetoinducAonFOLFIRINOX(RECIST):
– 17.2%parAalresponse;82.7%stabledisease– NopaAentsprogressed
• Surgery:41.9%(13)underwentsurgery(allR0resecAons)– 6of13hadchemoRTpriortosurgery– 9hadnode-negaAvedisease(stage0,I,IIAin1,2,and6pts)
• Medianprogressionfreesurvival17.8mo• Mediansurvival26.6mo
Stein.BrJCancer2016

ABSTRACT204
Phase2LAPACTTrialofnab®-PaclitaxelPlusGemcitabineforPa9entsWithLocallyAdvanced
Pancrea9cCancerPascalHammel,1JillLacy,2FabiennePortales,3AlbertSobrero,4RobertoPazo-Cid,5JoseL.ManzanoMozo,6EricTerrebonne,7ScotDowden,8Jack
ShiansongLi,9TengJinOng,9ThomasNydam,9PhilipA.Philip10
1HôpitalBeaujon,Clichy,France;2YaleCancerCenter,NewHaven,CT;3InsAtutrégionalduCancerdeMontpellier(ICM),Montpellier,France;4AziendaOspedalieraUniversitariaSanMarAno,Genova,Italy;5HospitalMiguelServet,Zaragoza,Spain;
6HospitalUniversitariGermansTriasiPujol,Barcelona,Spain;7HospitalHautLeveque,Giround,France;8TomBakerCancerCenter,Calgary,Canada;9Celgene
CorporaAon,Summit,NJ;10KarmanosCancerInsAtute,Detroit,MI
nab®isaregisteredtrademarkofCelgeneCorporaAon.
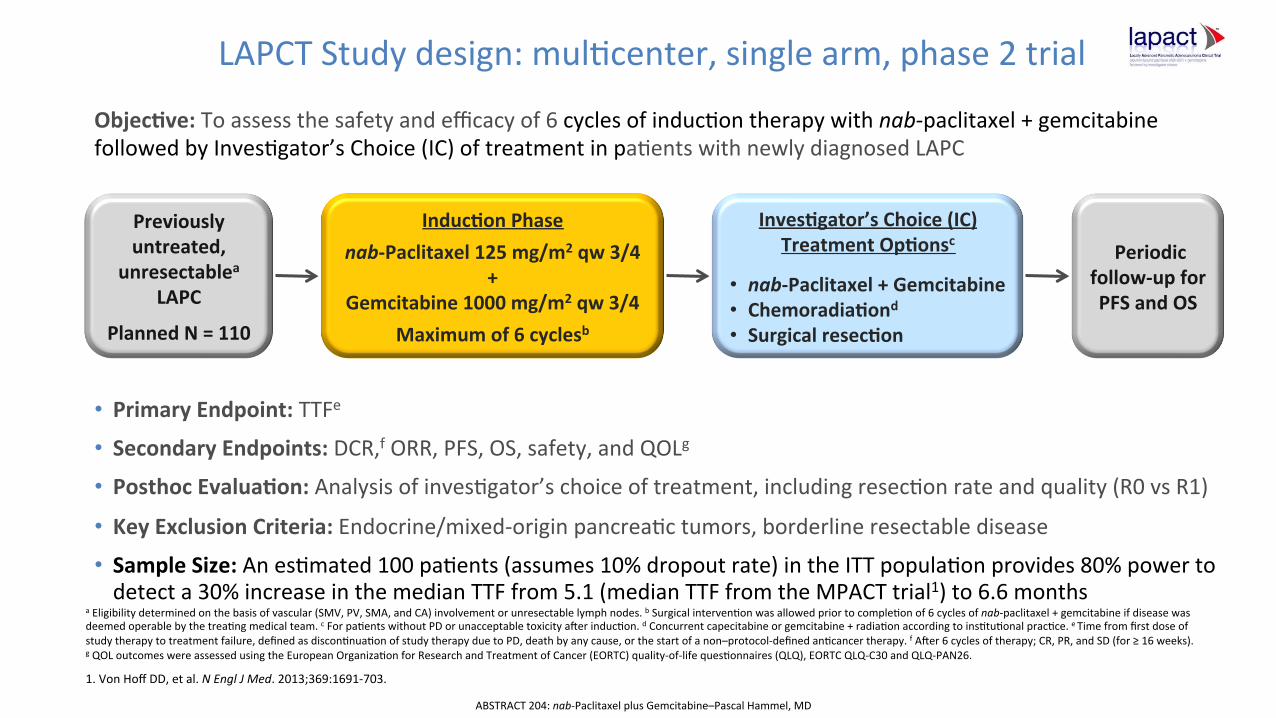
LAPCTStudydesign:mulAcenter,singlearm,phase2trial
aEligibilitydeterminedonthebasisofvascular(SMV,PV,SMA,andCA)involvementorunresectablelymphnodes.bSurgicalintervenAonwasallowedpriortocompleAonof6cyclesofnab-paclitaxel+gemcitabineifdiseasewasdeemedoperablebythetreaAngmedicalteam.cForpaAentswithoutPDorunacceptabletoxicityamerinducAon.dConcurrentcapecitabineorgemcitabine+radiaAonaccordingtoinsAtuAonalpracAce.eTimefromfirstdoseofstudytherapytotreatmentfailure,definedasdisconAnuaAonofstudytherapyduetoPD,deathbyanycause,orthestartofanon–protocol-definedanAcancertherapy.fAmer6cyclesoftherapy;CR,PR,andSD(for≥16weeks).gQOLoutcomeswereassessedusingtheEuropeanOrganizaAonforResearchandTreatmentofCancer(EORTC)quality-of-lifequesAonnaires(QLQ),EORTCQLQ-C30andQLQ-PAN26.
1.VonHoffDD,etal.NEnglJMed.2013;369:1691-703.
Objec9ve:Toassessthesafetyandefficacyof6cyclesofinducAontherapywithnab-paclitaxel+gemcitabinefollowedbyInvesAgator’sChoice(IC)oftreatmentinpaAentswithnewlydiagnosedLAPC
Previouslyuntreated,
unresectableaLAPC
PlannedN=110
Induc9onPhase
nab-Paclitaxel125mg/m2qw3/4+
Gemcitabine1000mg/m2qw3/4
Maximumof6cyclesb
Inves9gator’sChoice(IC)TreatmentOp9onsc
• nab-Paclitaxel+Gemcitabine• Chemoradia9ond• Surgicalresec9on
Periodicfollow-upforPFSandOS
• PrimaryEndpoint:TTFe
• SecondaryEndpoints:DCR,fORR,PFS,OS,safety,andQOLg• PosthocEvalua9on:AnalysisofinvesAgator’schoiceoftreatment,includingresecAonrateandquality(R0vsR1)
• KeyExclusionCriteria:Endocrine/mixed-originpancreaActumors,borderlineresectabledisease
• SampleSize:AnesAmated100paAents(assumes10%dropoutrate)intheITTpopulaAonprovides80%powertodetecta30%increaseinthemedianTTFfrom5.1(medianTTFfromtheMPACTtrial1)to6.6months
ABSTRACT204:nab-PaclitaxelplusGemcitabine–PascalHammel,MD

LAPACT:PaAentdisposiAonDuringNab/GemInducAona
aPercentagesarebasedonthe107enrolledpaAents;1paAentenrolledbutdisconAnuedpriortotheinducAonphase.bPaAentsdesignatedforsurgerypriortocompleAng6cyclesofinducAonwereconsideredtohavecompletedtheinducAonphase.
57.0% 42.1%
ReasonsforDiscon9nua9onofInduc9on
Adverseevent(n=20;18.7%)Progressivedisease(n=8;7.5%)Physiciandecision(n=6;5.6%)WithdrawalbypaAent(n=3;2.8%)ProtocolviolaAon(n=4;3.7%)Nonadherencetostudydrug(n=1;0.9%)Death(n=2;1.9%)Other(n=1;0.9%)
CompletedinducAontreatment(n=61)bDisconAnuedinducAontreatment(n=45)
N=107
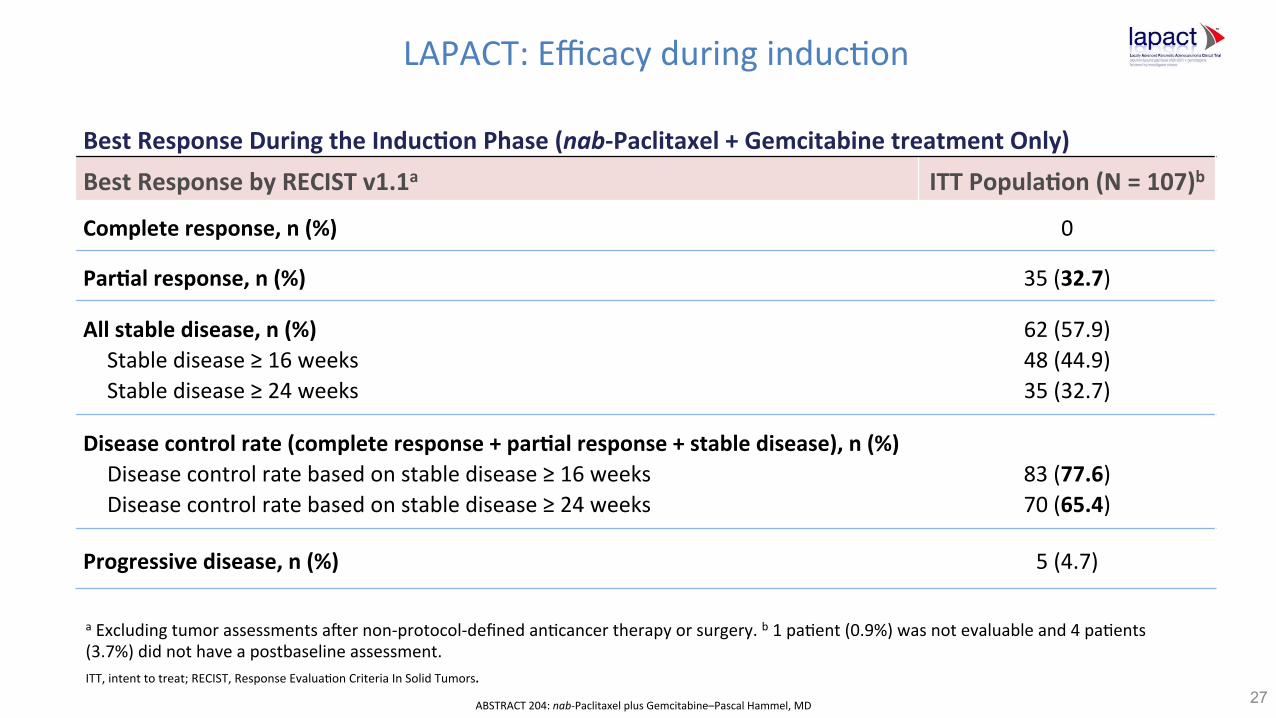
LAPACT:EfficacyduringinducAonBestResponseDuringtheInduc9onPhase(nab-Paclitaxel+GemcitabinetreatmentOnly)BestResponsebyRECISTv1.1a ITTPopula9on(N=107)b
Completeresponse,n(%) 0
Par9alresponse,n(%) 35(32.7)
Allstabledisease,n(%)Stabledisease≥16weeksStabledisease≥24weeks
62(57.9)48(44.9)35(32.7)
Diseasecontrolrate(completeresponse+par9alresponse+stabledisease),n(%)Diseasecontrolratebasedonstabledisease≥16weeksDiseasecontrolratebasedonstabledisease≥24weeks
83(77.6)70(65.4)
Progressivedisease,n(%) 5(4.7)
27
aExcludingtumorassessmentsamernon-protocol-definedanAcancertherapyorsurgery.b1paAent(0.9%)wasnotevaluableand4paAents(3.7%)didnothaveapostbaselineassessment.ITT,intenttotreat;RECIST,ResponseEvaluaAonCriteriaInSolidTumors.
ABSTRACT204:nab-PaclitaxelplusGemcitabine–PascalHammel,MD
28
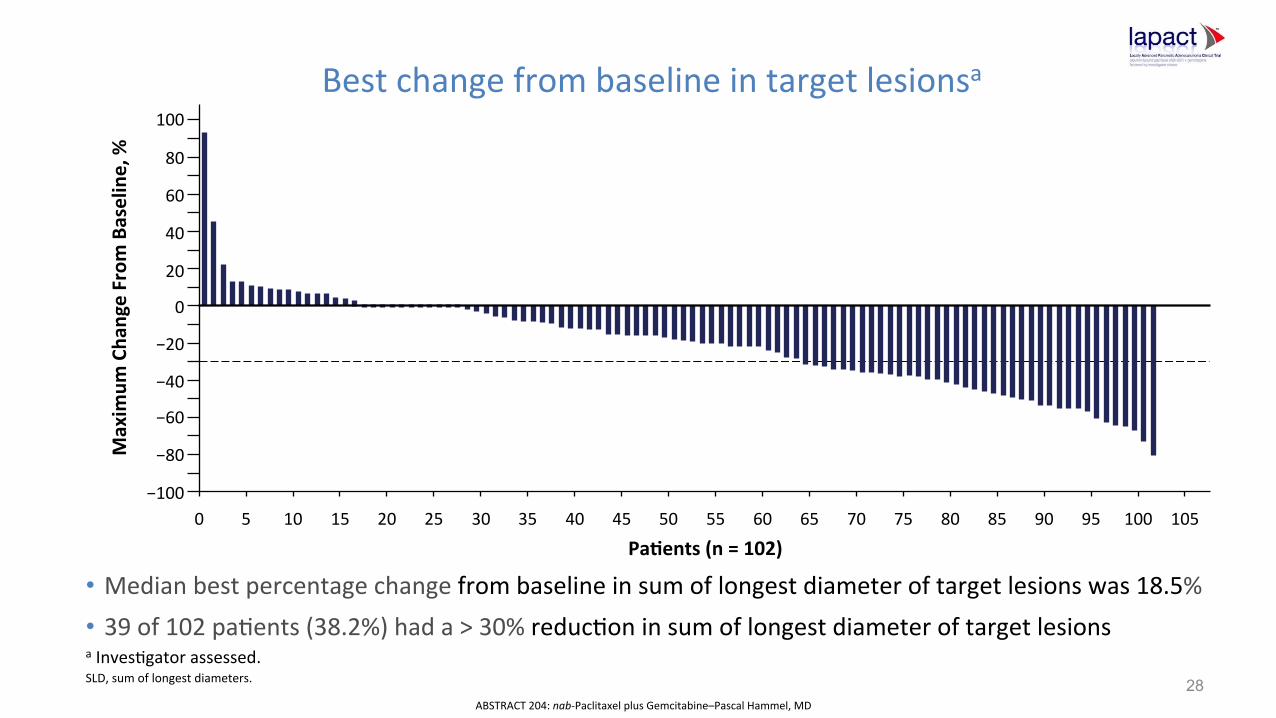
Bestchangefrombaselineintargetlesionsa
aInvesAgatorassessed.SLD,sumoflongestdiameters.
• Medianbestpercentagechangefrombaselineinsumoflongestdiameteroftargetlesionswas18.5%• 39of102paAents(38.2%)hada>30%reducAoninsumoflongestdiameteroftargetlesions
Maxim
umCha
ngeFrom
Baseline,%
Pa9ents(n=102)
100
80
60
40
20
0
−20
−40
−60
−80
−1000 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95 100 105
ABSTRACT204:nab-PaclitaxelplusGemcitabine–PascalHammel,MD

29
Progression-freesurvivala
Events/N Median,mo(90%CI)
Allpa9ents 80/107 10.8(9.26–11.63)
No.atRisk
100
80
60
40
20
00 3 6 9 12 15 18 21 24
97 85 68 40 23 14 7AllPaAents 107
Months
Percen
tageofP
a9en
ts
With
outD
iseaseProgression
,%
aAsofmonth12,27paAentshavenotprogressedordied.ABSTRACT204:nab-PaclitaxelplusGemcitabine–PascalHammel,MD
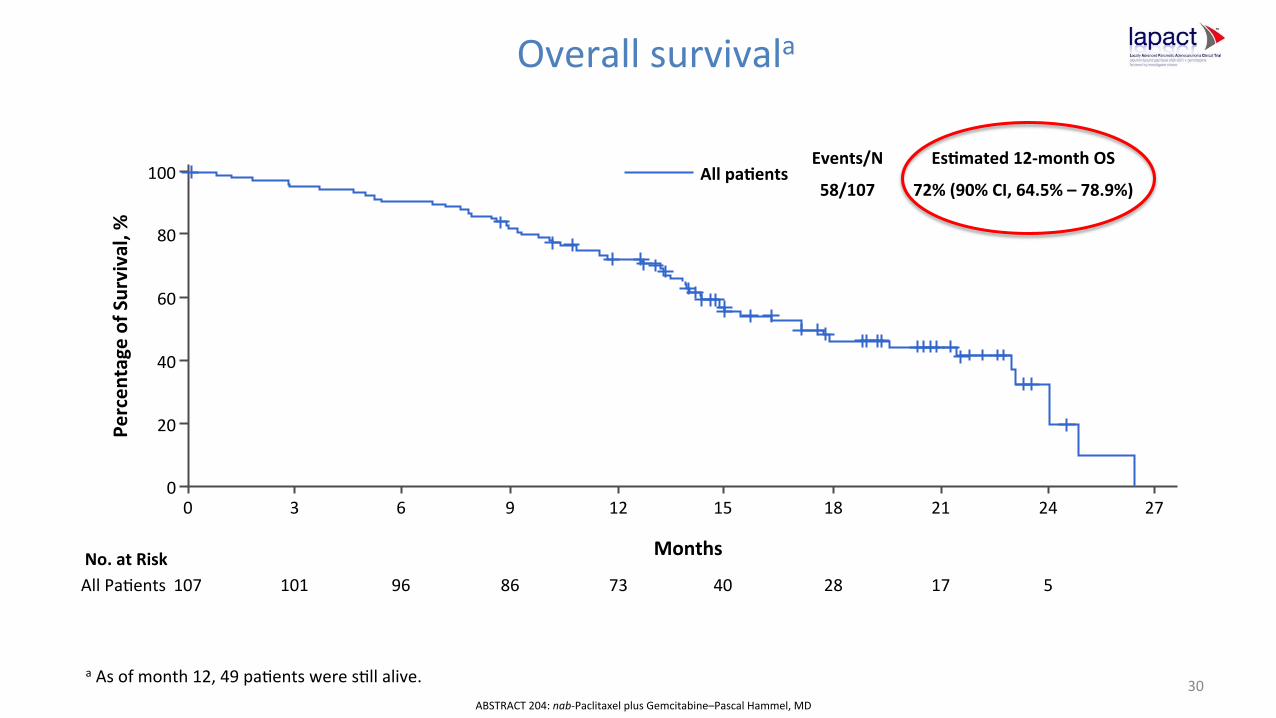
Allpa9entsEvents/N Es9mated12-monthOS
58/107 72%(90%CI,64.5%–78.9%)
30
Overallsurvivala
aAsofmonth12,49paAentsweresAllalive.
No.atRisk
100
80
60
40
20
00 3 6 9 12 15 18 21 24 27
101 96 86 73 40 28 17 5AllPaAents 107
Percen
tageofS
urvival,%
Months
ABSTRACT204:nab-PaclitaxelplusGemcitabine–PascalHammel,MD

EORTCQLQ-C30Measurements
31
Global Health Status/ QoL
EORTC QLQ-C30
Functional Scales Symptom Scales/Items
• How would you rate your overall health during the past week?
• How would you rate your overall quality of life during the past week?
a Scales have been revised since version 1.0
• Physical functioninga • Role functioninga • Emotional functioning • Cognitive functioning • Social functioning
• Fatigue • Nausea and vomiting • Pain • Dyspnea • Insomnia • Appetite loss • Constipation • Diarrhea • Financial difficulties
The QLQ-C30 QoL was completed by patient: screening, on day 1 of each A+G cycle, and at the 28-day follow-up visit during the induction phase

QualityoflifeduringinducAona
aPaAentswereaskedtoratetheiroverallhealthandqualityoflifeduringthepastweek.
• PaAents’overallglobalhealthstatusandoverallQOLwasmaintainedthroughday1ofcycle6
Baseline C2, D1 C3, D1 C4, D1 C5, D1 C6, D1
99 85 73 70 53 42 Cycle, Day
Mea
n C
hang
e fr
om B
asel
ine
± SE
All Patients
10
5
0
−5
−10
ABSTRACTID204(200537):nab-PaclitaxelplusGemcitabine–PascalHammel,MD

Gem+Nab-paclitaxelinLAPC:LAPACTSummary• FirstprospecAvestudytoevaluateNab/GeminLAPC
• Nonewsafetysignals• ResponsetoinducAonNab/Gemencouraging
– 32.7%parAalresponse;57.9%stabledisease– 4.7%progression
• R0orR1resecAonrate15%• QualityoflifemaintainedinmostpaAents• Medianprogressionfreesurvival10.8mo(TTF8.8mo)• Mediansurvivalunavailable(72%aliveatoneyear)
ABSTRACT204:nab-PaclitaxelplusGemcitabine–PascalHammel,MD

CrossTrialComparisonsofInducAonChemotherapyinLAPCInduc9onRegimen
Completedinduc9on
DCRduringinduc9on
RRduringinduc9on
PFS(mo)
OS(mo)
12mosurvival
Resec9onRate
SCALOPN114
Gem/Cape13mo
64.9% ? ? ? 12.7 53% ?
LAP07N442
Gem+/-ErloAnib24mo
60.9%
? ? 7.5 12.8 54% 4%
YaleN31
ModifiedFOLFIRINOX34mo
65% 100%
17.2% 17.8 26.6 86% 42%
LAPACTN106
Gem/nab-paclitaxel46mo
57% 77.6%(at4mo)
32.7% 10.8 72% 15%
1Post-inducAon:randomizedtoRTwthCapeorGem(LancetOncol2013Apr;14(4):317-26)2Post-inducAon:randomizedtoRTorconAnuedchemo(JAMA2016May3;315(17):1844-53)3Post-inducAon:invesAgatorschoicechemo,RT,orsurgery(BrJCancer2016Mar29;114(7):737-43)4Post-inducAon:invesAgatorschoicechemo,RT,orsurgery(Abs204ASCOGISymposium2018)
LAPCManagement:
• WhattodoamerinducAonchemotherapyinnon-progressors?– ConAnuechemotherapy– RadiaAonandifsowhattechnique
• LAP07trialshowednosurvivalbenefitforRTamergemcitabine+/-eroloAnibinducAoninnon-progressor1
• AdvancesinchemoandRTlimitapplicaAonofLAP07tocurrentpracAce
– Surgery(?precededbyRT)– IrreversibleelectroporaAon(?)
1Hammeletal.JAMA2016;315(17):1844-53
LAPCManagement:
• WhattodoamerinducAonchemotherapyinnon-progressors?– ConAnuechemotherapy– RadiaAonandifsowhattechnique
• LAP07trialshowednobenefitforRTamerGemcitabine1
• AdvancesinchemoandRTlimitapplicaAonofLAP07tocurrentpracAce
– Surgery(?precededbyRT)– IrreversibleelectroporaAon(?)
1Hammeletal.JAMA2016;315(17):1844-53

LAPC:WhoshouldundergosurgicalexploraAon?LimitaAonsofCTImagingAmerInducAonTherapy
• MayshowpersistentsignificantvascularinvolvementinptswhoachieveR0resecAon
• OflimitedvalueindifferenAaAngresidualtumorfromfibroinflammatoryAssueamerpre-optreatment.
• Usualsizecriteriaforresponse(RECIST)areinsufficienttoevaluate“biologic”responseofLAPC
CassinoTo.Radiology2014;273(1):108-16(Bordeaux,FR).DonahueArchSurg2011Jul;146(7):836-43(UCLA).Ferrone.AnnSurg.2015;261(1):12(MGH).Wagner.EurRadiol2017Jul;27(7):3104-3116(French).Michelakos.AnnSurg2017Dec7(MGH)

CTevaluaAonamerneoadjuvantFOLFIRINOXforborderlineandlocallyadvancedpancreaAcadenocarcinoma:FrenchExperience
• 36ptswithBR/LAPC(NCCN)resectedamerFFX(+RT,12):31R0,5R1• CriteriaforexploraAon:improvingPS,decreasingCA19-9,noprogression• SignificantresponsetoFFXbyRECISTonCT:PRin17/36(47%)• StablediseasevsresponsebyRECISTunabletopredictR0resecAon• Decreasedarterial/venousinvolvementunabletopredictR0resecAon• NCCNclassificaAonpost-inducAonFFXunabletopredictR0resecAon:R0resecAonpossibleinptswithpost-treatmentLAPCbyNCCN
Wagneretal.EurRadiol2017Jul;27(7):3104-3116.
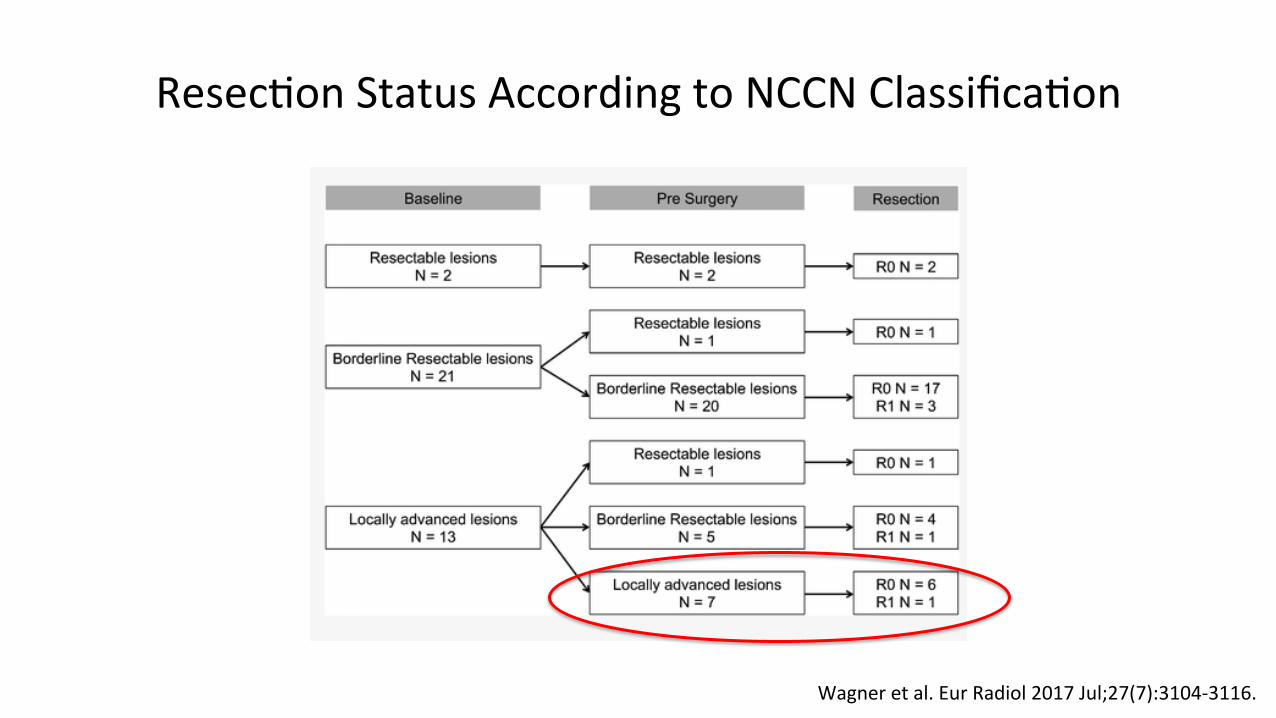
ResecAonStatusAccordingtoNCCNClassificaAon
Wagneretal.EurRadiol2017Jul;27(7):3104-3116.
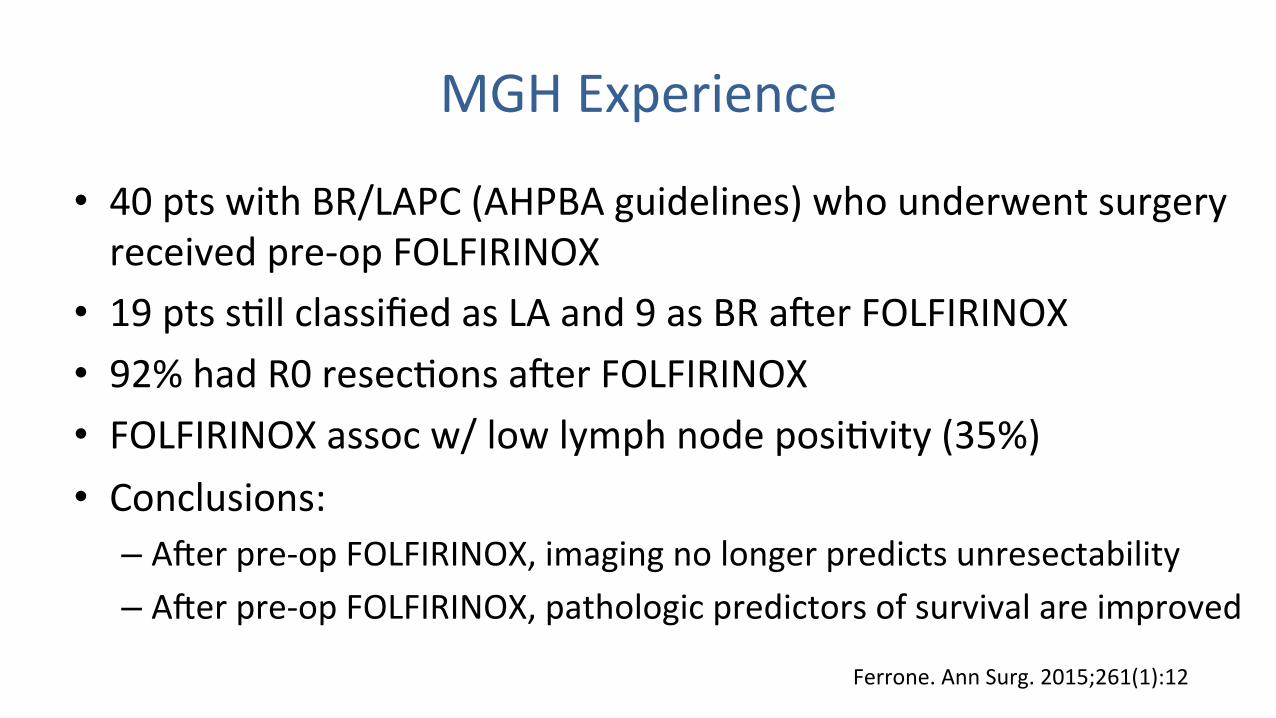
MGHExperience
• 40ptswithBR/LAPC(AHPBAguidelines)whounderwentsurgeryreceivedpre-opFOLFIRINOX
• 19ptssAllclassifiedasLAand9asBRamerFOLFIRINOX• 92%hadR0resecAonsamerFOLFIRINOX• FOLFIRINOXassocw/lowlymphnodeposiAvity(35%)• Conclusions:
– Amerpre-opFOLFIRINOX,imagingnolongerpredictsunresectability– Amerpre-opFOLFIRINOX,pathologicpredictorsofsurvivalareimproved
Ferrone.AnnSurg.2015;261(1):12

MGHExperience
• 141pts(BR/LA)surgicallyexploredamerFFX(10%)orFFXf/bRT(90%)*• 110pts(78%)resected(R080.6%,R119.4%)• Nopre-opfactorsaccuratelypredicAveofresectabilitywereidenAfied• Predictorsofshortsurvivalinresectedpts
– highpre-opCA19-9– tumorsize>3cm
• MedianOSofallFOLFIRINOX-treatedpts34.2andand37.7moforresectedpts(vs25.1moforupfrontresectedpts)
*ExcludedptswhoprogressedordiedonFOLFIRINOX Michelakos.AnnSurg2017Dec7.[Epubaheadofprint]
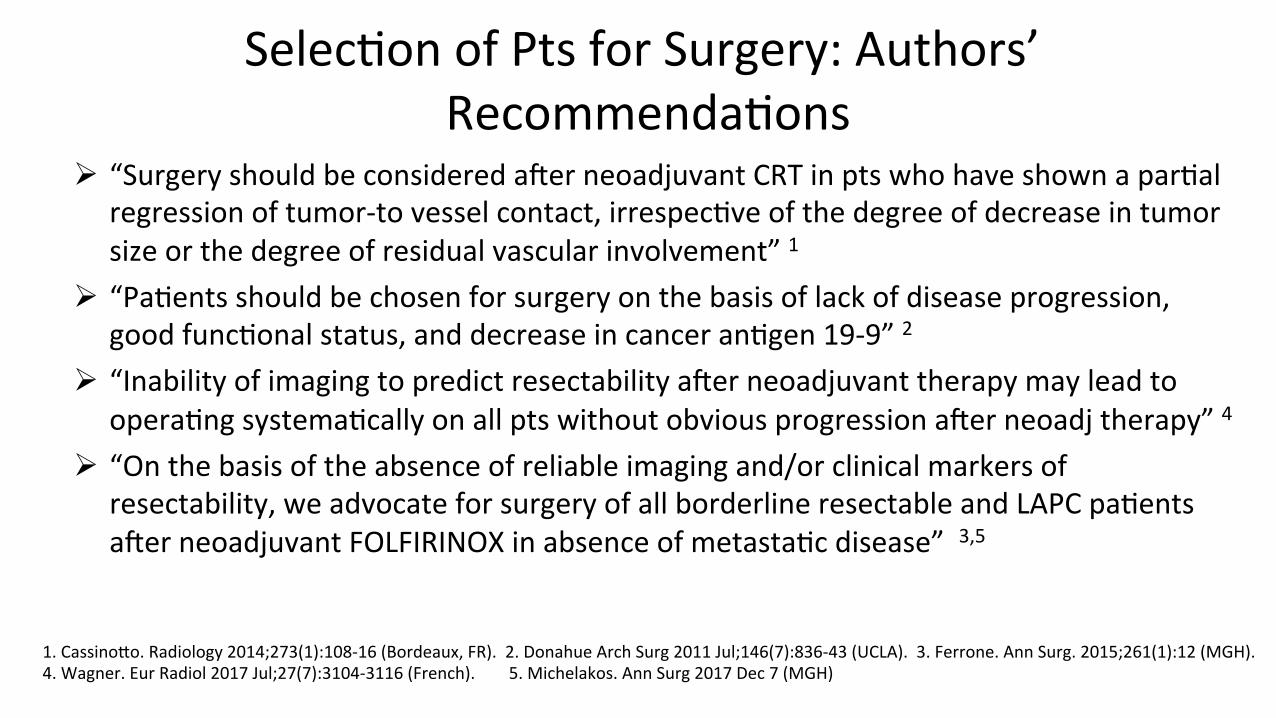
SelecAonofPtsforSurgery:Authors’RecommendaAons
Ø “SurgeryshouldbeconsideredamerneoadjuvantCRTinptswhohaveshownaparAalregressionoftumor-tovesselcontact,irrespecAveofthedegreeofdecreaseintumorsizeorthedegreeofresidualvascularinvolvement”1
Ø “PaAentsshouldbechosenforsurgeryonthebasisoflackofdiseaseprogression,goodfuncAonalstatus,anddecreaseincanceranAgen19-9”2
Ø “InabilityofimagingtopredictresectabilityamerneoadjuvanttherapymayleadtooperaAngsystemaAcallyonallptswithoutobviousprogressionamerneoadjtherapy”4
Ø “Onthebasisoftheabsenceofreliableimagingand/orclinicalmarkersofresectability,weadvocateforsurgeryofallborderlineresectableandLAPCpaAentsamerneoadjuvantFOLFIRINOXinabsenceofmetastaAcdisease”3,5
1.CassinoTo.Radiology2014;273(1):108-16(Bordeaux,FR).2.DonahueArchSurg2011Jul;146(7):836-43(UCLA).3.Ferrone.AnnSurg.2015;261(1):12(MGH).4.Wagner.EurRadiol2017Jul;27(7):3104-3116(French).5.Michelakos.AnnSurg2017Dec7(MGH)

LimitaAons• RetrospecAvestudiesofonlythoseFFX-treatedptswhowentontosurgicalexploraAon
• StrongselecAonbias• MixofLAPCandBRandlackofuniformdefiniAons• RoleofRTimpossibletoteaseout• Long-termdisease-freesurvivalrateunknown• Studiesneededto
– beTerdefinecriteriathatpredictR0vR1resecAonvunresectabledisease– toidenAfypredictorsoflong-termdisease-freesurvivalamersurgery
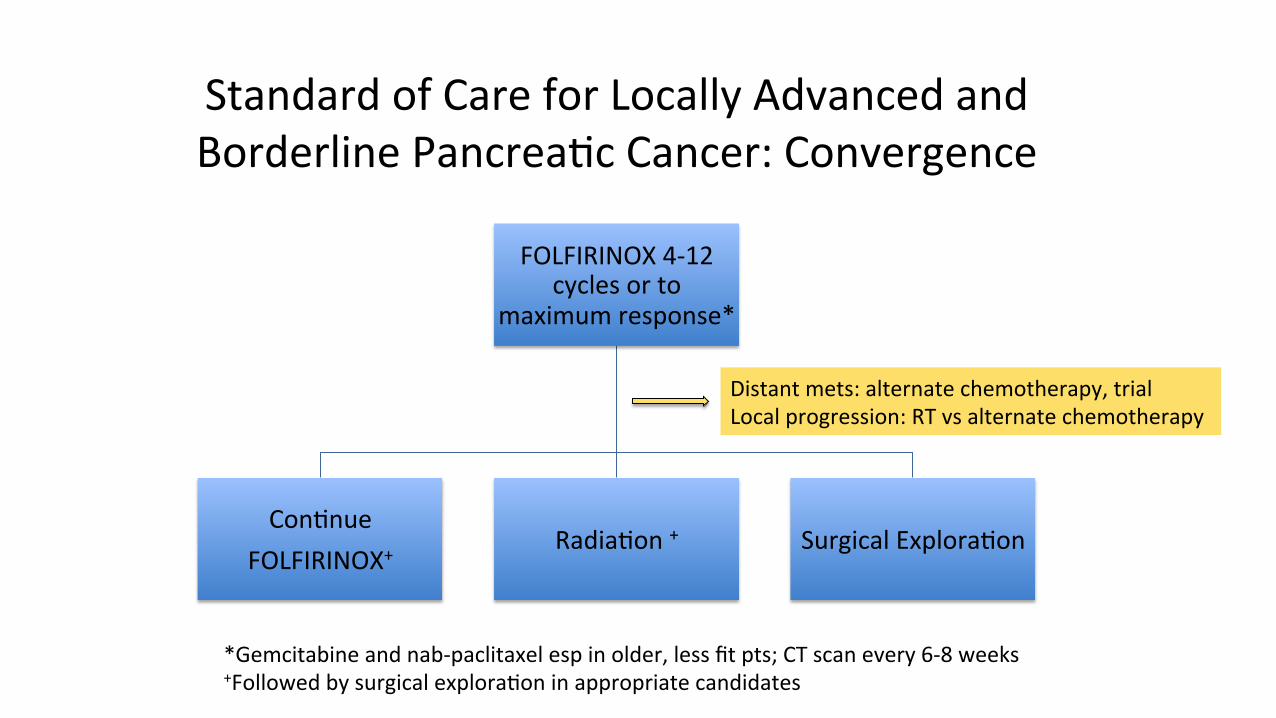
StandardofCareforLocallyAdvancedandBorderlinePancreaAcCancer:Convergence
FOLFIRINOX4-12cyclesorto
maximumresponse*
ConAnueFOLFIRINOX+
RadiaAon+ SurgicalExploraAon
*Gemcitabineandnab-paclitaxelespinolder,lessfitpts;CTscanevery6-8weeks+FollowedbysurgicalexploraAoninappropriatecandidates
Distantmets:alternatechemotherapy,trialLocalprogression:RTvsalternatechemotherapy

StandardofCareforLocallyAdvancedandBorderlinePancreaAcCancer:Convergence
FOLFIRINOX4-12cyclesorto
maximumresponse*
ConAnueFOLFIRINOX+
RadiaAon+ SurgicalExploraAon
*Gemcitabineandnab-Paclitaxelespinolder,lessfitpts;CTscanevery6-8weeks+FollowedbysurgicalexploraAoninappropriatecandidates
Distantmets:alternatechemotherapy,trialLocalprogression:RTvsalternatechemotherapy
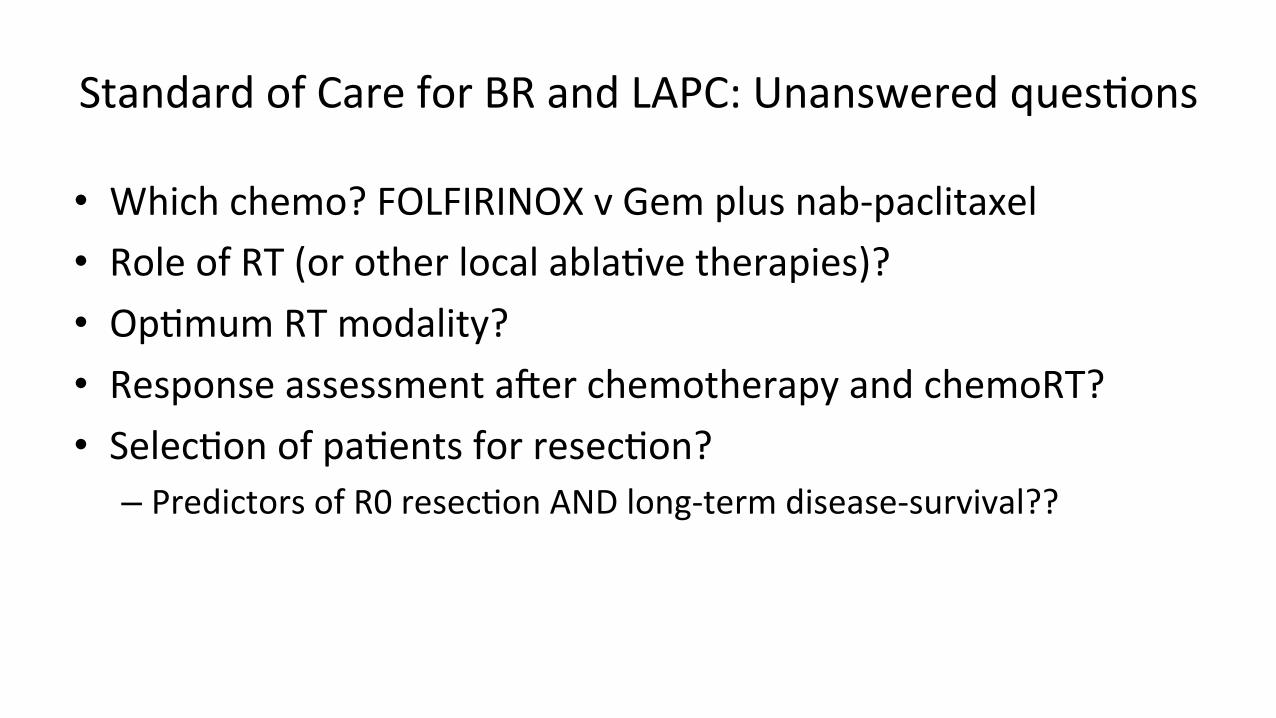
StandardofCareforBRandLAPC:UnansweredquesAons
• Whichchemo?FOLFIRINOXvGemplusnab-paclitaxel• RoleofRT(orotherlocalablaAvetherapies)?• OpAmumRTmodality?• ResponseassessmentamerchemotherapyandchemoRT?• SelecAonofpaAentsforresecAon?
– PredictorsofR0resecAonANDlong-termdisease-survival??
LAPC:Challenges
– Needforreliablebiomarkerstosortlocal-onlybiologyfrommetastaAcbiology(?SMAD4)
– NeedforwelldesignedRCTstoopAmizecurrentstandardofcare– StrongbeliefsonvalueofcomponentsoftreatmenthashamperedtrialdesigntoanswerkeyquesAons
– NeedforclinicaltrialswithnovelagentsfocusedonLAPC

ClinicalTrialsinLAPCPhaseIIIRCTs
Ø FOLFIRINOXvsFOLFIRINOXfollowedbySBRT(US)Ø Chemotherapy(FOLFIRINOXorGemmonotherapy)vsChemotherapyfollowedby
chemoradiaAon(GermanCONKO-007)Ø IrreversibleElectroporaAonvsSBRTamerFOLFIRINOX(CROSSFIRETrial)(Netherlands)Ø FOLFIRINOXvsGemcitabine(NEOPAN)Ø Gem/CapvsGem/Cap+GV1001vaccine(LAPCandmetastaAc)Ø GemcitabinevsGemcitabine+micellarcisplaAnNC-6004(LAPCandmetastaAc)

ClinicalTrialsinLAPCPhaseIandII
Ø SBRT:12studies• DoseescalaAon• Withimmunecheckpointinhibitors• Withvaccine• Withconcurrentchemotherapy
Ø IrreversibleelectroporaAon:4studiesØ StandardradiaAonwithalternaAveconcurrentchemotherapy(Abraxane,nelfinivir,S-1)
Ø Approvedchemotherapydrugs(withorwithoutRT)
ClinicalTrialsinLAPCPhaseIandII
Ø NovelagentswithorwithoutRTorchemotherapy• Theragene(ReplicaAon-competentAdenovirus-mediatedDoubleSuicideGeneTherapy)• Oregovomab(anA-CA125)• Intra-tumoralgenedeliveryofCYL-02(plasmidDNAencodingmousesomatostaAnreceptorand
fusionproteinofhumandeoxycyAdinekinaseanduridinemonophosphatekinase)• CG200745PPA(hypomethylaAngagent)• ATRA(stromalablaAonstrategy)• Intra-tumoralNanoPac(NanoparAculatePaclitaxel)• CeriAnib• Tocilizumab(targetsIL6receptor)• Nelfinavir(radiosensiAzer)

LAPC:Summary
• DisAncAons/definiAonsofborderlineresectableandLAPCaresomewhatarbitraryanddifficulttoimplementaccuratelyandconsistently
• TherapeuAcapproachforptswithvascularinvolvementhasconverged->upfrontcombinaAonchemotherapyfollowedbyphysician’sdiscreAon
• Responseassessment/paAentselecAonforsurgeryamerchemotherapy+/-RTremainsachallenge
• SurvivalandresecAonratesareincreasingwith“modern”chemotherapy• Arewecuringmoreptswith”modern”neoadjuvantapproaches??• Needforbiologicalpredictorsofdisseminateddisease• NeedforhighqualityRCTsandevaluaAonofnovelagents

ThankYou