rapid response to vedolizumab therapy in biologic-naïve
TRANSCRIPT

Accepted Manuscript
Rapid response to vedolizumab therapy in biologic-naïve patients with inflammatorybowel diseases
Brian G. Feagan, MD, Karen Lasch, MD, Trevor Lissoos, MBBCh, Charlie Cao,PhD, Abigail M. Wojtowicz, PhD, Javaria Mona Khalid, PhD, Jean-FrédéricColombel, MD
PII: S1542-3565(18)30558-5DOI: 10.1016/j.cgh.2018.05.026Reference: YJCGH 55868
To appear in: Clinical Gastroenterology and HepatologyAccepted Date: 13 May 2018
Please cite this article as: Feagan BG, Lasch K, Lissoos T, Cao C, Wojtowicz AM, Khalid JM, ColombelJ-F, Rapid response to vedolizumab therapy in biologic-naïve patients with inflammatory boweldiseases, Clinical Gastroenterology and Hepatology (2018), doi: 10.1016/j.cgh.2018.05.026.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
• Rapid response to vedolizumab therapy in biologic-n aïve patients with inflammatory
bowel diseases
Short title: Rapid response to vedolizumab in IBD
Brian G. Feagan, MD,1 Karen Lasch, MD,2 Trevor Lissoos, MBBCh,2 Charlie Cao, PhD,2 Abigail
M. Wojtowicz, PhD,2 Javaria Mona Khalid, PhD,3 Jean-Frédéric Colombel, MD4
1 Robarts Research Institute, University of Western Ontario, London, Ontario, Canada
2 Takeda Pharmaceuticals U.S.A., Inc., Deerfield, IL, USA
3 Takeda Development Centre Europe, Ltd., London, UK
4 Department of Gastroenterology, Icahn School of Medicine at Mount Sinai, New York, NY, USA
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Grant support: This study is supported by Takeda Pharmaceuticals U.S.A., Inc.
Abbreviations:
ANCOVA, analysis of covariance
AP, abdominal pain
BL, baseline
BMI, body mass index
CD, Crohn’s disease
CDAI, Crohn’s disease activity index
CI, confidence interval
CRF, case report form
CrI, credible interval
CRP, C-reactive protein
CS, corticosteroid
Diff, difference
EIM, extraintestinal manifestation
HBI, Harvey-Bradshaw index
IBD, inflammatory bowel disease
IFX, infliximab
IMM, immunomodulators
IQR, interquartile range
ITT, intent-to-treat
IVRS, interactive voice response system
LSF, loose stool frequency
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MAdCAM-1, mucosal addressin cell adhesion molecule 1
MCS, Mayo Clinic score
N/A, not applicable
Non-Est, non-estimated
OR, odds ratio
PBO, placebo
PK, pharmacokinetics
PRO, patient-reported outcome
RB, rectal bleeding
RBS, rectal bleeding score
SD, standard deviation
SF, stool frequency
SFS, stool frequency score
SONIC, Study of Biologic and Immunomodulator Naïve Patients in CD
TNF, tumor necrosis factor alpha
UC, ulcerative colitis
VDZ, vedolizumab
VICTORY, VedolIzumab for Health OuTComes in InflammatORY Bowel Diseases
Correspondence:
Jean-Frédéric Colombel, MD
Department of Gastroenterology, Icahn School of Medicine at Mount Sinai, New York, NY, USA
Email: [email protected]
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Phone: +1-212-824-8944
Fax: +1-646-537-8921
Disclosures:
Brian G Feagan has received grant support from AbbVie, Amgen, AstraZeneca, Bristol-Myers Squibb, Roche, Genentech, J&J, Janssen, Millennium, Pfizer, Receptos, Tillotts, and UCB; and has served as a consultant or advisory board member for AbbVie, ActoGeniX, Akros, Albireo, Amgen, AstraZeneca, Avaxia Biologics, Avir Pharma, Baxter Healthcare Corp, Biogen Idec, Boehringer Ingelheim, Bristol-Myers Squibb, Calypso Biotech, Celgene, Elan/Biogen, enGene, Ferring Pharmaceuticals, Galapagos, Genentech/Roche, GiCare Pharma, Gilead, Given Imaging, GSK, Inception IBD Inc, Ironwood Pharmaceuticals, J&J, Janssen, Japan Tobacco, Kyowa Hakko Kirin Co Ltd, Lexicon, Lilly, Lycera Biotech, Merck, Mesoblast Ltd, Millennium, Nektar, Nestlé, Novartis, Novo Nordisk, Pfizer, Prometheus Therapeutics & Diagnostics, Protagonist, Receptos, Salix, Shire, Sigmoid Pharma, Synergy Pharmaceuticals Inc, Takeda, Teva Pharmaceutical Industries Ltd, TiGenix, Tillotts, UCB, Vertex Pharmaceuticals, VHsquared Ltd, Warner Chilcott, Wyeth, Zealand Pharma, and Zyngenia. Jean-Frederic Colombel has received grant support from AbbVie, Janssen Pharmaceuticals, and Takeda; has served as a speaker for AbbVie, Amgen, and Ferring Pharmaceuticals; has served as a consultant for AbbVie, Amgen, Boehringer Ingelheim, Celgene Corporation, Celltrion, Eli Lilly, Enterome, Ferring Pharmaceuticals, Genentech, Janssen Pharmaceuticals, Medimmune, Merck & Co., Pfizer, Protagonist, Second Genome, Seres Therapeutics, Shire, Takeda, and Theradiag; and is shareholder of Genfit and Intestinal Biotech Development. Karen Lasch, Trevor Lissoos, Charlie Cao, and Abiga il M. Wojtowicz are employees of Takeda Pharmaceuticals U.S.A., Inc. Javaria Mona Khalid is an employee of Takeda Development Centre Europe, Ltd.
Writing assistance: Medical writing assistance was provided by Reem Berro, PhD, of Syneos Health and supported by Takeda Pharmaceuticals U.S.A., Inc.
Author contributions:
1. Acquisition of data (BGF, KL, TL, JMK, JFC) 2. Statistical analysis (CC) 3. Interpretation of data (all authors) 4. Critical revision of the manuscript for important intellectual content and final approval (all
authors)
Acknowledgments:
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
The authors thank Alexandra James, an employee of Takeda Development Centre Europe, Ltd., London, UK, for her assistance with statistical analysis and data interpretation.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Abstract:
Background & Aims: Vedolizumab, a humanized monoclonal antibody against α4β7 integrin, is
used to treat adults with moderately to severely active ulcerative colitis (UC) and Crohn’s disease
(CD). We investigated the time course of clinical response to vedolizumab in patients who were
and were not previously treated with tumor necrosis factor (TNF) antagonists.
Methods: We performed a post-hoc analysis of data from phase 3, randomized, controlled trials
of vedolizumab vs placebo in adult patients with UC (n=374) or CD (n=784). We collected data
on patient-reported symptoms (rectal bleeding and stool frequency for patients with UC,
abdominal pain and loose stool frequency for patients with CD) reported at weeks 2, 4, and 6 of
treatment. We reported mean percentage score changes from baseline and proportions of
patients who achieved predefined scores. We performed multivariate logistic regression analysis
to identify factors associated with an early response (at week 2).
Results: In patients with UC (overall or naïve to TNF antagonist therapy), a significantly greater
percentage of patients given vedolizumab achieved the predefined composite symptom score at
weeks 2, 4, and 6 compared to those given placebo. In patients with CD who were naïve to TNF
antagonists, a significantly greater percentage of patients given vedolizumab achieved the
predefined score at weeks 2 and 4 compared to those given placebo. Among patients with UC
given vedolizumab, 19.1% (overall) and 22.3% (TNF antagonist naïve) achieved a composite
score of rectal bleeding of 0 and stool frequency ≤1 at week 2 compared to 10% (overall) and
6.6% (TNF antagonist naïve) of those receiving placebo. Among TNF antagonist-naïve patients
with CD, 15.0% of those given vedolizumab achieved an average daily composite score of
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
abdominal pain ≤1 and loose stool frequency ≤3 at week 2 (compared to 7.9% given placebo),
and 23.8% of those given vedolizumab achieved these by week 4 (compared to 10.3% given
placebo).
Conclusion: In a post-hoc analysis of data from phase 3 clinical trials, vedolizumab significantly
improved patient-reported symptoms of UC and CD as early as week 2 of treatment, continuing
through the first 6 weeks—especially when given as first-line biologic therapy.
KEY WORDS: GEMINI trials, IBD, time to response, patient-reported outcomes
Summary: Vedolizumab is an antibody against α4β7 integrin that is used to treat patients with
ulcerative colitis or Crohn’s disease. In an analysis of data from 3 clinical trials, we found that
vedolizumab rapidly (within 2 weeks) improved some patient-reported symptoms, through the first
6 weeks of treatment.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Introduction
Inflammatory bowel disease (IBD) is a chronic inflammatory disease of the gastrointestinal
tract with a significant burden on patients’ quality of life. Diarrhea is a common symptom in both
ulcerative colitis (UC) and Crohn’s disease (CD). In addition, patients with UC often present with
rectal bleeding (RB) and report abdominal pain (AP) in CD.1, 2 Consequently, these important
symptoms are regularly used as endpoints in clinical trials as a part of disease activity indices
and to monitor disease activity in clinical practice.3
Current therapy aims to resolve both relevant symptoms and underlying mucosal
inflammation.4 Patient-reported outcomes (PROs) have an increasingly important role in
capturing symptomatic burden and have become required by regulatory agencies in assessing
response to treatment and evaluation of claims for future product labeling.4-6 Several studies
have identified the resolution of RB and the normalization of bowel habit as primary PRO targets
for UC therapy.4, 5 In CD, Khanna et al recommended the resolution of AP and the normalization
of bowel habit as the primary PROs for the evaluation of CD treatment efficacy in clinical trials.7
Vedolizumab is a gut-selective humanized immunoglobulin (Ig) G1 monoclonal antibody
that binds to α4β7 integrin expressed on the surface of lymphocytes, thereby blocking the binding
of α4β7 to its ligand MAdCAM-1 (mucosal addressin cell adhesion molecule-1) expressed on the
endothelial surface of venules in lymphoid tissue in the GI tract. The binding of vedolizumab to
α4β7 prevents the α4β7-expressing T lymphocytes from entering gut tissue, thus reducing
inflammation.8, 9 In the GEMINI trials, vedolizumab’s efficacy as induction and maintenance
therapy was demonstrated in moderately to severely active UC or CD patients who were naïve
to, or had prior exposure to, tumor necrosis factor alpha (TNF) antagonists.10-12 Clinical benefits
of vedolizumab in UC patients were evident at week 6, with greater differences in efficacy
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
between vedolizumab and placebo observed in patients who were TNF antagonist-naïve
compared with those who failed TNF antagonist treatment.10, 13 Subgroup analyses of CD
patients indicated that significantly higher remission and response rates were achieved in TNF
antagonist-naïve patients treated with vedolizumab than those assigned to placebo at weeks 6
and 10. In patients who failed TNF antagonist treatment, a significant effect of vedolizumab
induction on clinical remission was observed at week 10.12 These data add to the growing
evidence that second-generation biologics such as vedolizumab and ustekinumab have higher
efficacy in TNF antagonist-naïve patients in both clinical trials and real-world settings.12, 14, 15
Recent trends in clinical practice are moving toward incorporating disease-modifying therapy
earlier in the treatment of IBD to prevent disease progression and cumulative bowel damage;
hence the importance of evaluating the treatment effects of vedolizumab in biologic-naïve
patients.16, 17
It has been debated whether agents affecting lymphocyte trafficking may have a relatively
slower onset of action, especially in CD. However, there are no published studies comparing the
rapidity of onset of various classes of IBD drugs. The objective of this study was to investigate
the time course of clinical response with vedolizumab, particularly when used as a first-line
biologic. Therefore, we performed exploratory analyses of the GEMINI trial data to assess
rapidity of onset and identify predictors of patient-reported symptom improvements with
vedolizumab in patients with UC or CD.
Methods
Study Design
The results are based on post hoc exploratory analyses of the phase 3, randomized,
placebo-controlled trials GEMINI 1, GEMINI 2, and GEMINI 3. The design of the trials is reported
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
in detail elsewhere10, 11, 18 and summarized in Figure S1 . To summarize, eligible patients were
aged 18 to 80 years and had UC for ≥6 months with a Mayo Clinic Score (MCS) of 6 to 12 points
and endoscopic subscore of ≥2 in GEMINI 1, or had CD for ≥3 months and a Crohn’s disease
activity index (CDAI) score of 220 to 450 in GEMINI 2 and 3. Patients were randomized to
induction treatment for 6 weeks (GEMINI 1 and 2) or 10 weeks (GEMINI 3) and received 300-mg
intravenous vedolizumab or placebo at weeks 0 and 2 (GEMINI 1 and 2) or weeks 0, 2, and 6
(GEMINI 3). These patients are referred to as the induction intent-to-treat (ITT) population and
are the focus of these analyses.
Disease activity at entry into GEMINI and efficacy assessments throughout the studies
were measured by MCS for UC and CDAI for CD. Patient-reported components of MCS were RB
and stool frequency (SF) and those of CDAI were AP and loose SF (LSF).
Patient-Reported Outcomes
Mean percentage changes from baseline in patient-reported subscores were calculated for
the overall population, TNF antagonist-naïve, and TNF antagonist-exposed patients at 2, 4, and 6
weeks. Percentages of UC patients who reached RB subscore=0 (elimination of bleeding) and
SF subscore ≤1 (no more than 1 to 2 stools above normal) and of CD patients who achieved
average daily composite score of AP ≤1 and LSF ≤3 (revised PRO-219) were determined at each
timepoint (weeks 2, 4, and 6).
Statistical Analyses
The difference in adjusted percentage score change from baseline between vedolizumab and
placebo was determined using an analysis of covariance (ANCOVA) model with treatment as a
factor and baseline score as a covariate, and study as an additional factor for GEMINI 2 and 3.
95% confidence intervals (CIs) were calculated, and upper limit of 95% CI <0 was considered
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
statistically significant at a nominal significance level of 0.05, unless otherwise indicated. For the
pooled GEMINI 2 and 3 analyses, the Cochran-Mantel-Haenszel method with “study” as a
stratum was used to adjust for treatment differences in the proportion of CD patients who
achieved average daily composite score of AP ≤1 and LSF ≤3.
Univariate logistic regression analyses were performed to identify predictors of outcomes at
week 2 (composite subscores of RB=0 and SF ≤1 for UC and AP ≤1 and LSF ≤3 for CD). P
values ≤0.05 were considered statistically significant. A multivariate analysis was performed by
fitting baseline variables from the univariate analyses with a P value of <0.05 using stepwise
backward regression. For CD, “study” as a factor was included at each step of model building to
adjust for potential study differences between GEMINI 2 and 3.
Results
Patient Baseline Characteristics
A total of 374 UC (GEMINI 1) and 784 CD patients (GEMINI 2 and 3) were randomized for
induction to receive vedolizumab or placebo, and these constituted the induction ITT population.
TNF antagonist-naïve patients constituted 55% (n=206) and 36.5% (n=286) of the UC and CD
populations, respectively. No statistical comparisons were made between subpopulations.
However, a descriptive summary of baseline characteristics showed a few notable differences
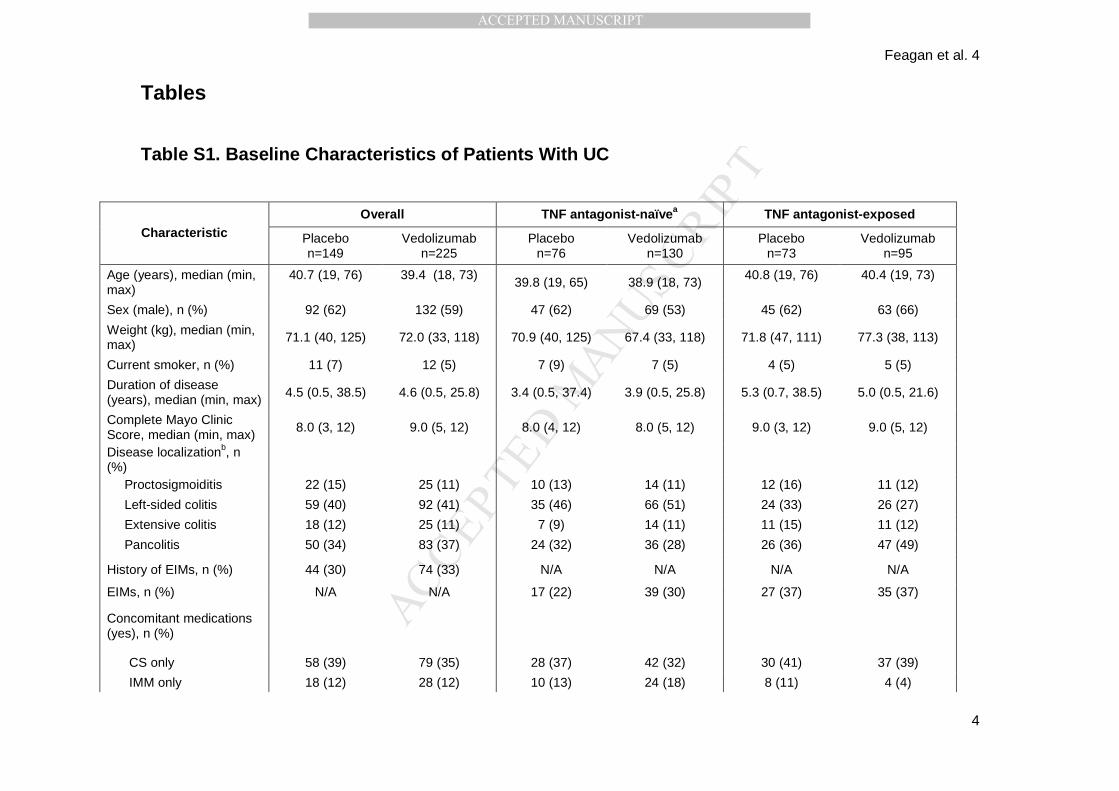
within the UC population (Table S1) . Disease activity at baseline was similar across treatment
groups with median MCS of 8.0 for vedolizumab vs 9.0 for placebo in the overall UC population,
8.0 for both vedolizumab and placebo in the TNF antagonist-naïve, and 9.0 for both vedolizumab
and placebo in the TNF antagonist-exposed patients. Median disease duration was shorter in
TNF antagonist-naïve (placebo: 3.4 years [y]; vedolizumab: 3.9 y) than TNF antagonist-exposed
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
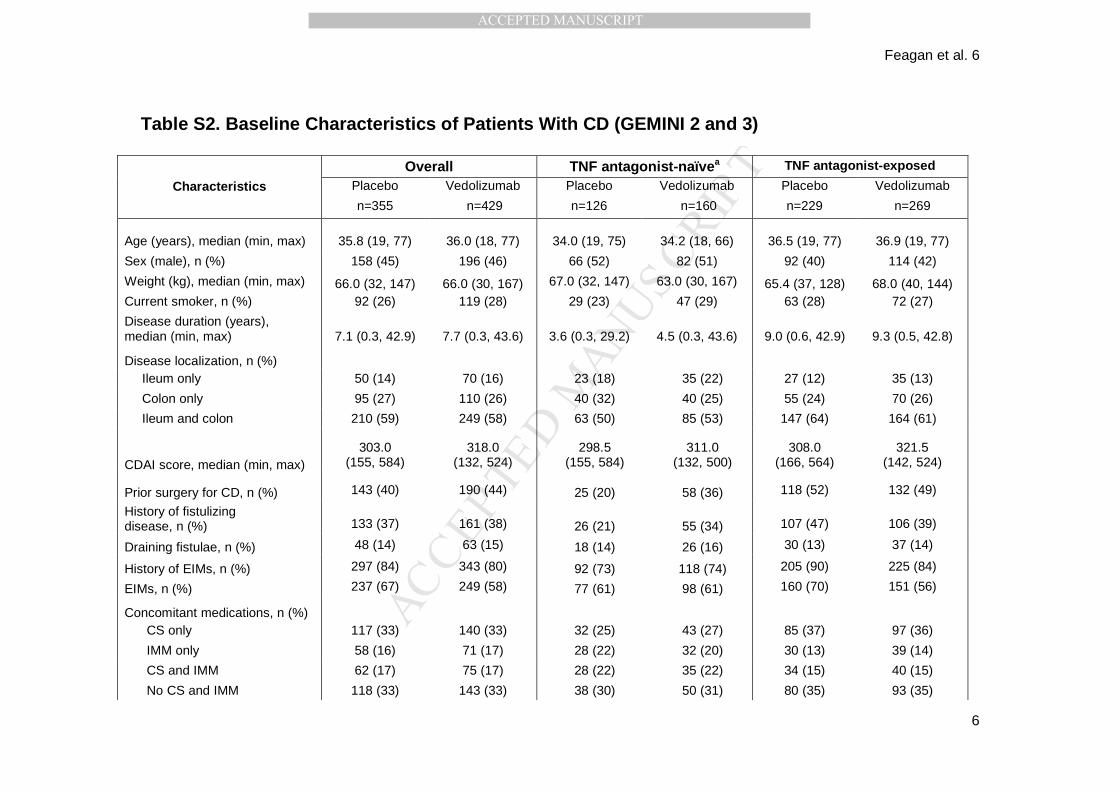
patients (placebo: 5.3 y; vedolizumab: 5.0 y) (Table S1) . In CD, median disease duration was
shorter in TNF antagonist-naïve (placebo: 3.6 y; vedolizumab: 4.5 y) than the overall (placebo:
7.1 y; vedolizumab: 7.7 y) and TNF antagonist-exposed populations (placebo: 9.0; vedolizumab:
9.3). (Table S2) .
Symptom Improvement With Vedolizumab in UC Patients
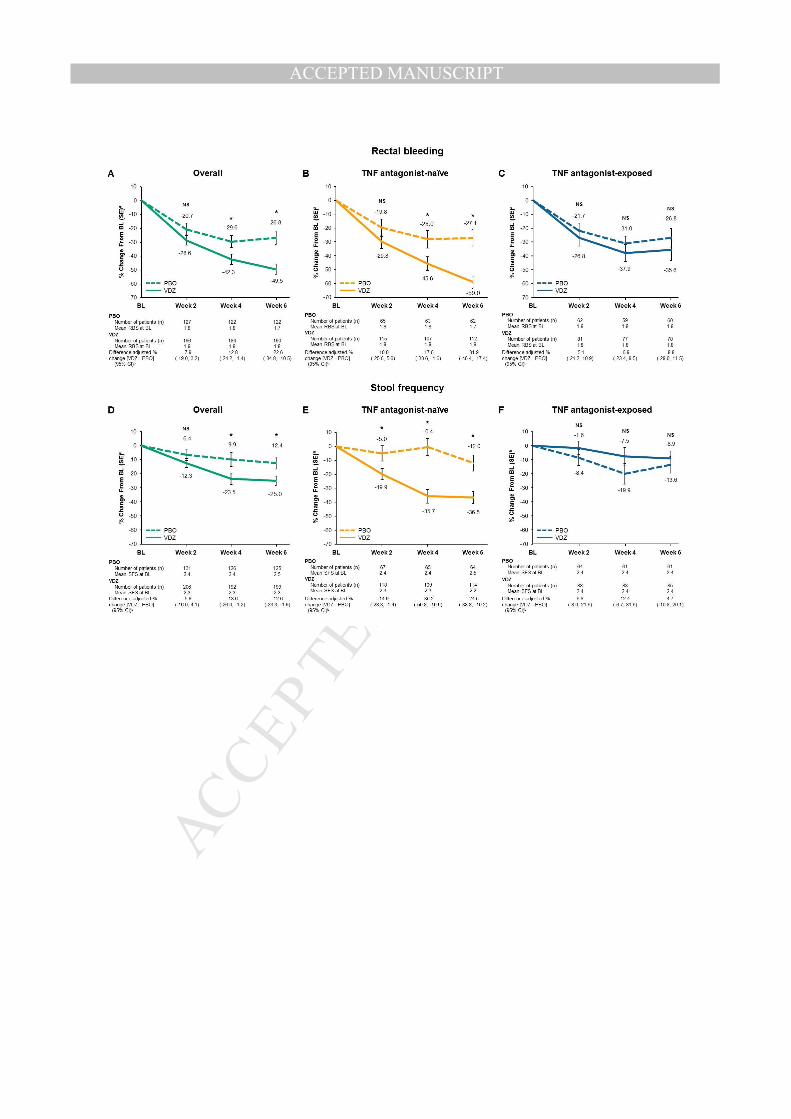
Numerically greater percentage decreases from baseline in RB subscore were observed
with vedolizumab treatment than with placebo, reaching statistical significance at weeks 4 and 6
in both overall and TNF antagonist-naïve. No significant differences between vedolizumab and
placebo were observed in TNF antagonist-exposed patients (Figure 1 A-C ).
In the overall population, statistically significant percentage decreases in SF subscore
from baseline were observed with vedolizumab than with placebo at weeks 4 and 6 and at all
timepoints in TNF antagonist-naïve patients (Figure 1 D, E ). No significant differences between
vedolizumab and placebo were observed in the TNF antagonist-exposed population (Figure 1 F) .
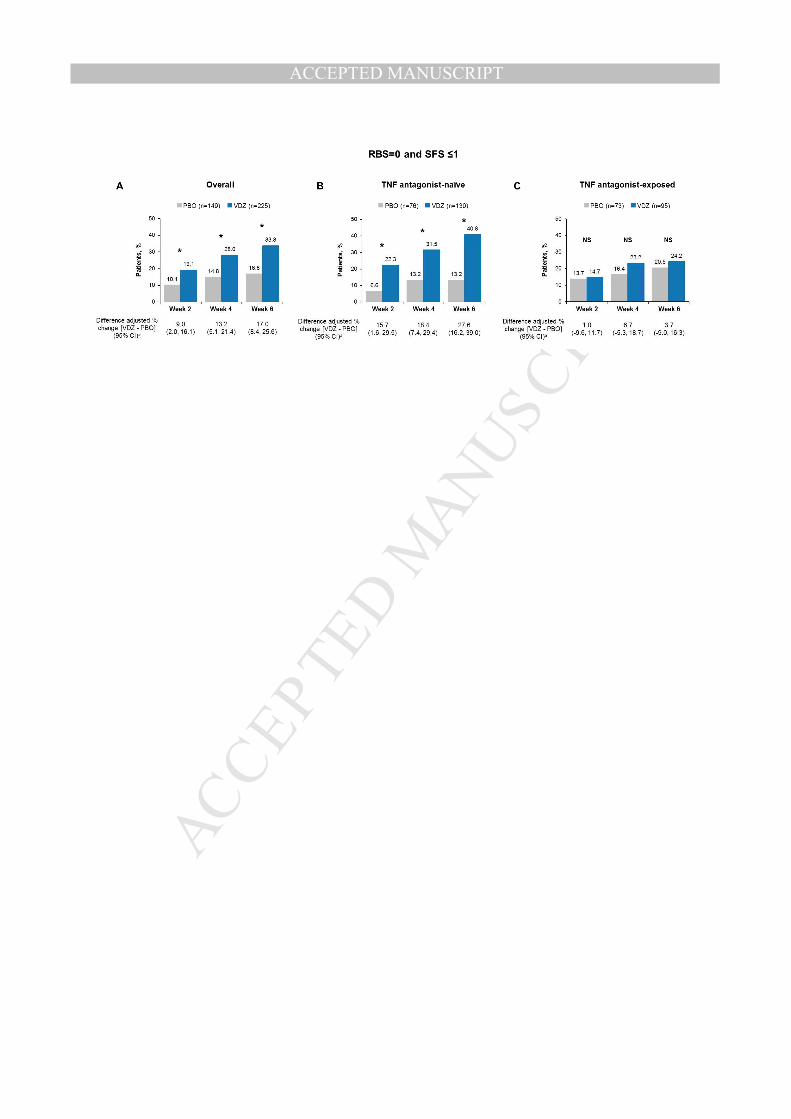
Significantly larger percentages of patients achieved a composite score of RB=0 and SF
≤1 with vedolizumab than placebo at all timepoints in the overall and TNF antagonist-naïve
populations (Figure 2 A, B ). No significant differences between vedolizumab and placebo were
observed in the TNF antagonist-exposed population (Figure 2 C) .
Symptom Improvement With Vedolizumab in CD Patients
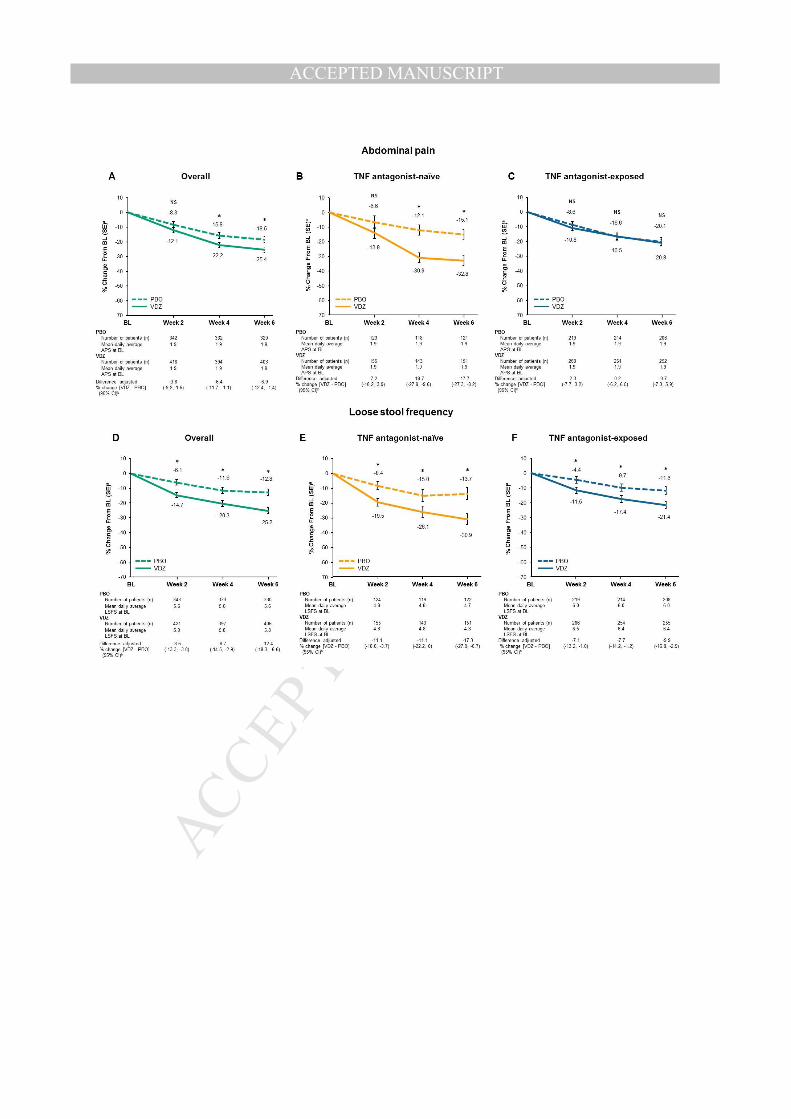
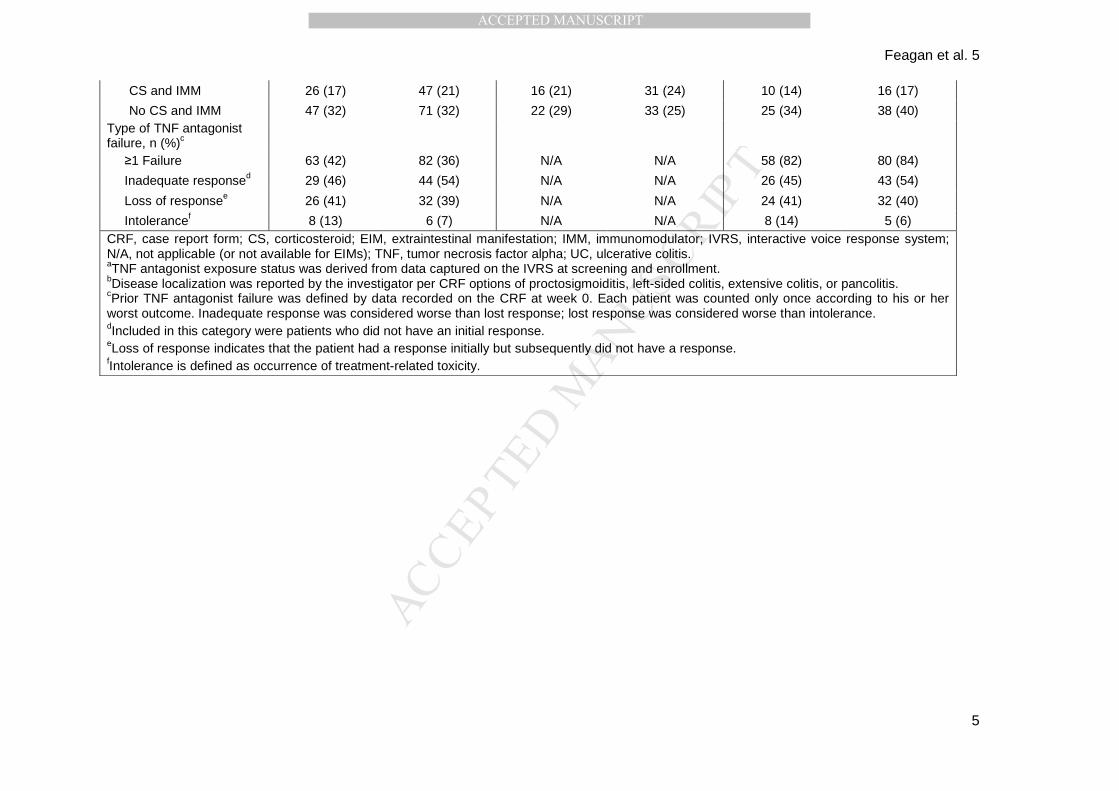
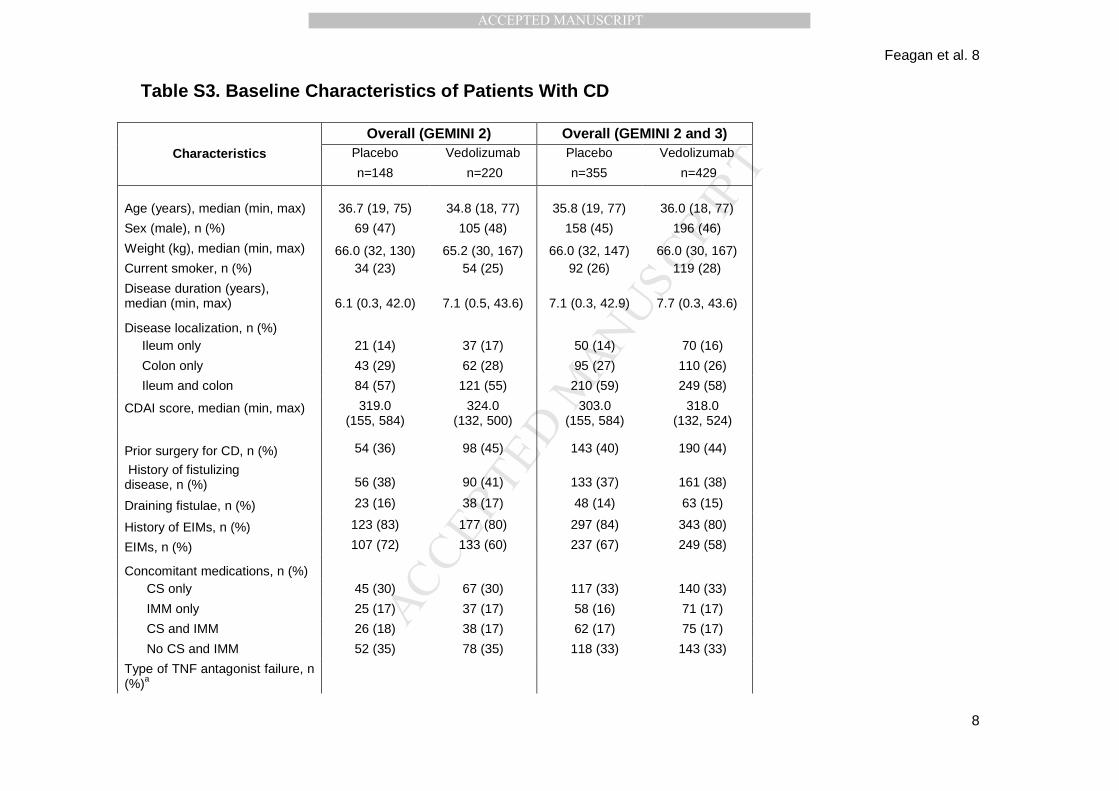
Percentage score decrease from baseline was evaluated in the pooled GEMINI 2 and 3
populations. GEMINI 2 was composed of 50% TNF antagonist-naïve patients while GEMINI 3
consisted of predominantly TNF antagonist-failure population (failure: 76%; naïve: 24%) (Table
S3). Significantly greater percentage decreases in AP subscore from baseline were observed
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
with vedolizumab than placebo as of week 4 in the overall GEMINI 2 and 3 combined (Figure 3
A). In TNF antagonist-naïve patients, there was a significantly greater decrease in the AP
subscore with vedolizumab than placebo as of week 4 (Figure 3B) . No significant differences
were observed in the TNF antagonist-exposed population (Figure 3C) .
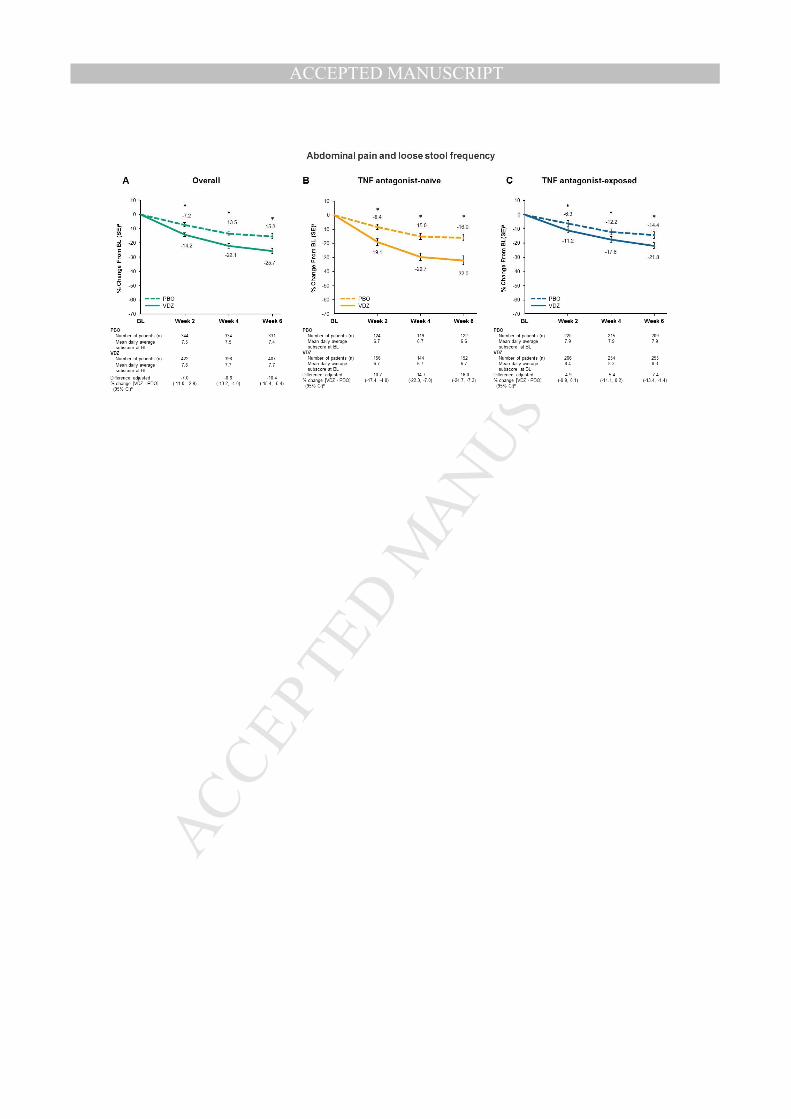
Greater percentage decreases in LSF were observed with vedolizumab than placebo,
reaching statistical significance as of week 2 in all populations (Figure 3 D-F ). A combined score,
calculated by adding the AP and LSF subscores, showed a similar trend with significantly greater
percentage decreases with vedolizumab than placebo at all timepoints in all populations (Figure
4 A-C).
Overall, differences in percentage subscore reduction between vedolizumab and placebo
were greater in the TNF antagonist-naïve patients than in the overall and TNF antagonist-
exposed populations. Notably, differences in the percentage decrease from baseline in the AP
subscore among the TNF antagonist-naïve patients at week 2 (-7.2), week 4 (-18.7), and week 6
(-17.7) were about 2 times as high as in the overall population (-3.8, -6.4, and -6.9, respectively)
(Figure 3 A, B ).
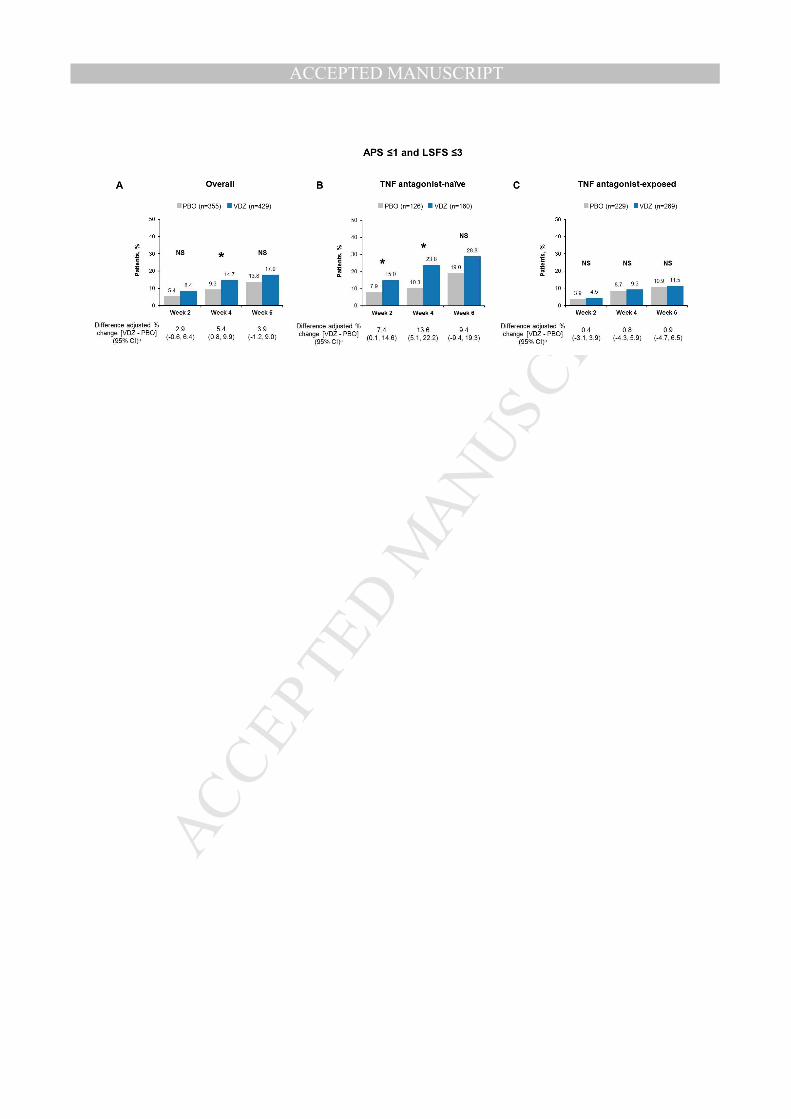
Significantly larger percentages of patients achieved an average daily composite score of
AP ≤1 and LSF ≤3 with vedolizumab than placebo at weeks 2 and 4 in the TNF antagonist-naïve
group and only at week 4 in the overall population, but not in the TNF antagonist-exposed group
(Figure 5) .
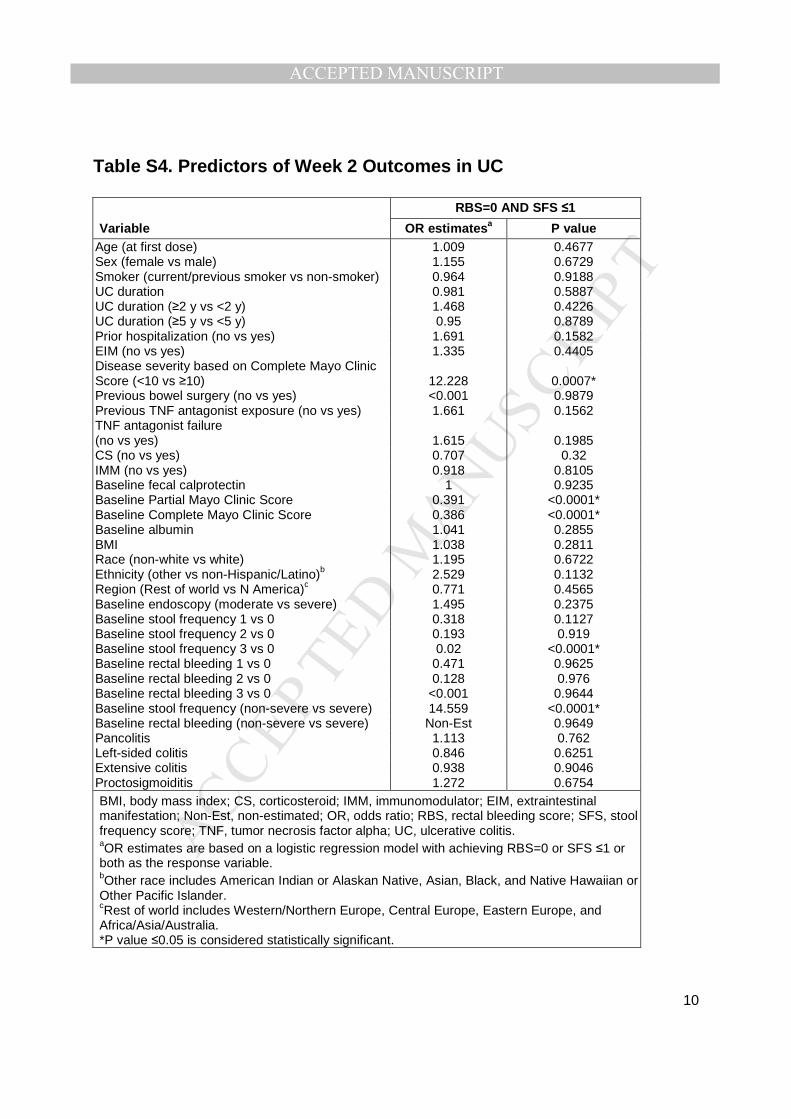
Predictors of Symptomatic Improvement in UC and CD at Week 2
Univariate analyses of UC outcome predictors identified disease severity, baseline partial and
complete MCS, and baseline SF subscore as significant variables (P≤0.05) for achieving the
composite score of RB subscore=0 and SF subscore ≤1 (Table S4). In multivariate analyses,
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
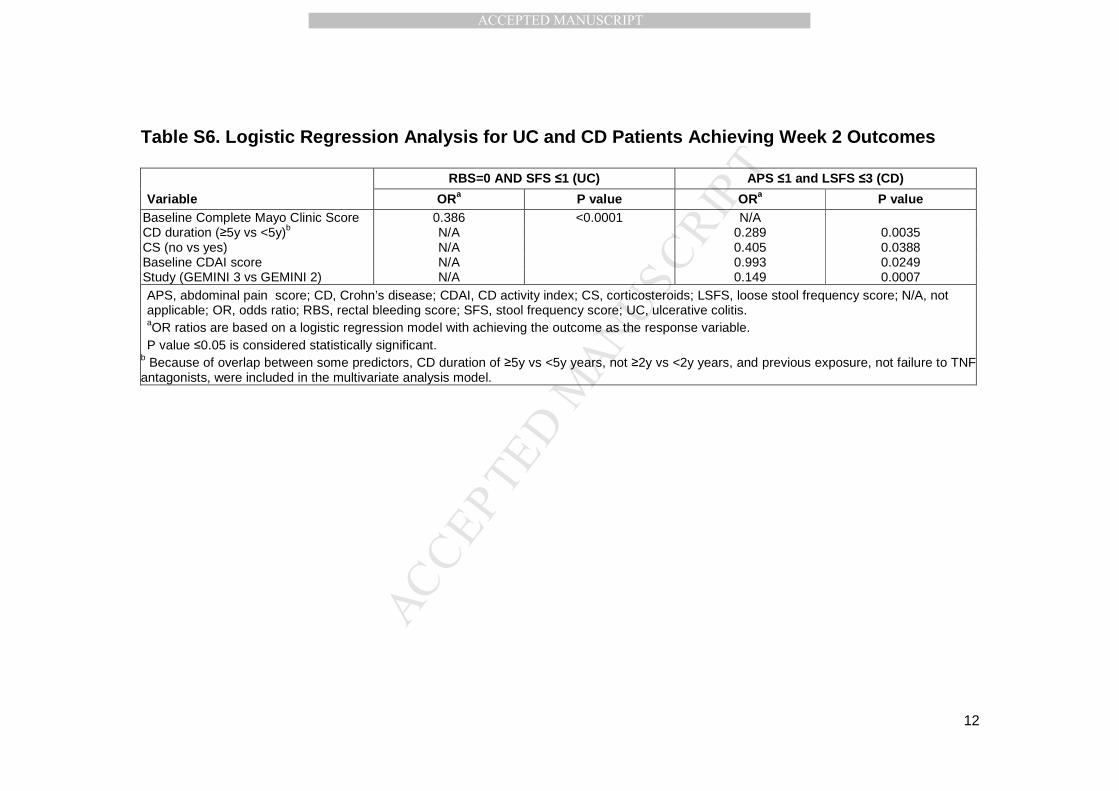
baseline complete MCS remained significant and lower baseline MCS was associated with
achieving RB subscore=0 and SF subscore ≤1 (Table S6) .
In CD, univariate analyses of outcome predictors identified male sex, CD duration of <2 or
<5 years, no prior bowel surgery, no previous exposure or failure to TNF antagonists,
corticosteroid use, lower baseline CDAI, HBI, and LSF scores as significant predictors for
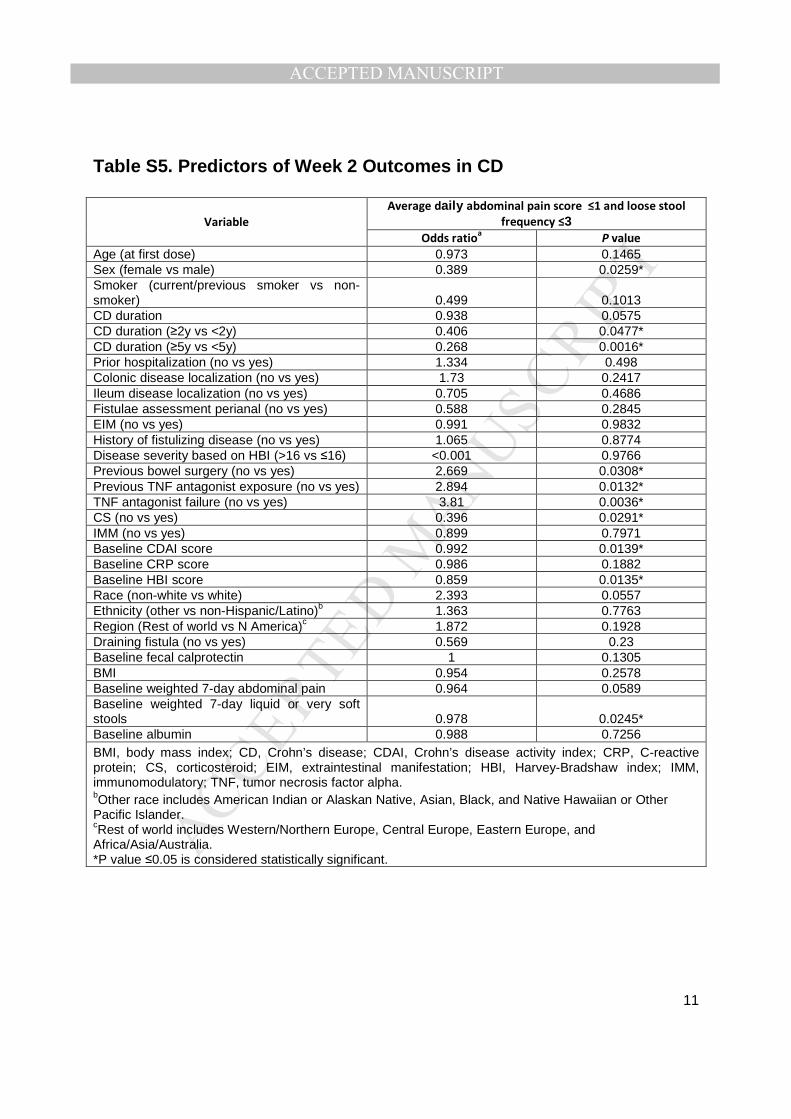
achieving the composite score of AP ≤1 and LSF ≤3 (Table S5) . A multivariate analysis
confirmed a CD duration of <5 years, corticosteroid use, and lower baseline CDAI score as
significant predictors of week 2 outcome (Table S6) .
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Discussion
These exploratory, post hoc analyses indicated that vedolizumab was effective at reducing
patient-reported symptoms as of week 2 in patients with UC or CD, with continued improvement
throughout the first 6 weeks of treatment. More specifically, 40.8% of TNF antagonist-naïve UC
patients achieved both elimination of RB (RB subscore=0) and reduction in SF (SF subscore ≤1)
at week 6 with vedolizumab compared with 13.2% with placebo. In CD, greater percentage
decreases from baseline in combined AP and LSF score were observed with vedolizumab
(32.0%) than placebo (16.0%) in the TNF antagonist-naïve patients after 6 weeks. The efficacy of
vedolizumab for inducing response and remission was demonstrated in the GEMINI trials,
whereby clinical benefits were more likely to be achieved at week 6 in patients treated with
vedolizumab than those assigned to placebo. The rapid onset of vedolizumab’s action reported
here suggests that symptomatic improvements may precede observed benefits by objective
measures of disease activity.
To assist with clinical interpretation of these data, we explored changes in complete MCS and
CDAI that corresponded with the percentage change from baseline in the individual symptomatic
improvements. At week 6, the change in RB subscore (overall: ~50%; TNF antagonist-naïve:
~60%) and SF subscore (overall: 25%; TNF antagonist-naïve: ~37%) were associated with an
approximate reduction of 2.7-2.9 and 3.3-3.5 points in complete MCS in the overall and TNF
antagonist-naïve GEMINI 1 populations, respectively. In GEMINI 2 and 3, a change in AP
subscore of 25.4%% and LSF subscore of 25.2% corresponded to an approximate 80-point
reduction in CDAI score in the overall population. In TNF antagonist-naïve populations, changes
of 32.8% and 30.9% in AP and LSF subscores, respectively, corresponded to an approximate
98.6-point reduction in CDAI score.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Although there is no published evidence to establish a correlation between early patient-
reported symptomatic improvement and long-term treatment benefits, several studies have
demonstrated that PROs are responsive to treatment effects. Specifically, in a post hoc analysis
of two independent studies in UC, the combination score of RB=0 and SF ≤1 (defined as PRO2)
was able to differentiate a treatment effect between active drug and placebo and was significantly
associated, alone or in combination with endoscopy, with clinical response.5 In addition, symptom
scores generally correlated well with endoscopic scores in UC, but some patients still exhibited
persistent symptoms even after endoscopic healing.16 Similarly in CD, 2- or 3-item PROs
consisting of SF and RB, or SF, RB, and general well-being, respectively, were responsive to
change in disease activity and indicated similar treatment effects as CDAI-based outcomes.7 On
the other hand, in a post hoc analysis of the Study of Biologic and Immunomodulator Naïve
Patients in CD (SONIC) trial, clinical symptoms as scored by CDAI did not correlate with
objective measures of inflammation such as mucosal lesions and CRP levels20, highlighting the
need to further assess the relationship between symptoms and disease activity, particularly in
CD. In a real-world setting, symptom-based clinical response to vedolizumab at week 4 was
found to be an independent predictor of long-term mucosal healing (up to 12 months) for UC and
CD.21
In general, reductions from baseline in symptom scores with vedolizumab versus placebo
were observed in the overall ITT UC or CD population, but were greater in TNF antagonist-naïve
patients. These observations are consistent with published clinical trial and real-world data
supporting the efficacy of vedolizumab in TNF antagonist-naïve patients at week 6 and beyond.
In a post hoc analysis of GEMINI 1 and GEMINI 2 data, TNF antagonist-naïve vedolizumab-
treated UC and CD patients had greater differences versus placebo at week 6 than patients who
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
had previous TNF antagonist failure, specifically in clinical response and remission in UC and CD
and mucosal healing in UC.13, 18 A German real-world study observed that vedolizumab was
significantly more effective at inducing clinical remission (partial MCS ≤1 with RB=0) at week 54
in TNF-naïve than in TNF-exposed patients with UC (55% vs 18%, P=0.02).22 A network meta-
analysis of 5 studies provides further evidence for the benefits of vedolizumab maintenance
therapy over other biologics among TNF antagonist-naïve UC patients23, including significantly
greater odds for achieving durable clinical response, clinical remission, and mucosal healing.
Specifically, vedolizumab was associated with higher odds of achieving durable clinical response
than adalimumab (OR: 3.96; 95% credible interval [CrI]: 1.67–9.84), infliximab (IFX) (OR: 3.18;
95% CrI: 1.14–9.20), and golimumab (OR: 2.33; 95% CrI: 1.04–5.41). Data from the VICTORY
consortium, the largest cohort of IBD patients on vedolizumab in a real-world clinical setting,
reported a reduction in vedolizumab effectiveness when used after TNF antagonists, with an
incremental reduction in effectiveness based on the number of prior TNF antagonists used. 14, 24
Vedolizumab’s benefits on corticosteroid use and IBD-related hospitalization in TNF antagonist-
naïve patients were also demonstrated in a real-world setting.25 Overall, our results in addition to
published evidence indicate that vedolizumab could be considered as a viable first-line biologic
option for UC and CD patients who are TNF antagonist treatment naïve.
Previous studies have evaluated the predictors of response to vedolizumab at later time
points (54 weeks and beyond)14, 26; however, this is the first evaluation of predictors of early
symptomatic response. In fact, multivariate regression analyses in this study indicated that
baseline disease activity (MCS and CDAI scores in UC and CD patients, respectively) was a
significant predictor of symptomatic improvements at week 2. In addition, CD duration and CS
use were significant predictors of CD outcome.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Overall, our observations here are inconsistent with the current notion that anti-integrin
therapies have a relatively slow onset of action. In fact, etrolizumab, an anti-integrin therapy still
in development, has recently been shown induce symptom improvement as of week 4 in a phase
3 study in UC.27 Our study demonstrated early symptomatic improvement with vedolizumab,
achieved as of week 2, particularly in patients naïve to anti-TNF therapies, and thus has
important implications on the optimal positioning of vedolizumab in treatment algorithms.
However, for patients who show a modest initial improvement, continued treatment and
assessment through week 14 is recommended.28
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Figure legends
Figure 1. Rectal bleeding and stool frequency subsc ores in patients with UC. aAdjusted % change from BL mean, where adjustment is for BL subscore and treatment bUpper limit of 95% CI <0 indicates statistical significance at a nominal significance level of 0.05. Asterisk (*)
indicates statistical significance and NS non-significance.
BL, baseline; CI, confidence interval; ITT, intent-to-treat; PBO, placebo; RBS, rectal bleeding subscore; SE, standard
error; SFS, stool frequency subscore; TNF, tumor necrosis factor alpha; UC, ulcerative colitis; VDZ, vedolizumab.
Figure 2. Proportion of patients with UC who achiev ed the composite score RBS=0 and SFS ≤1. aLower 95% CI limits >0 indicate statistical significance at a nominal significance level of 0.05. Asterisk (*) indicates
statistical significance and NS non-significance.
CI, confidence interval; PBO, placebo; RBS, rectal bleeding subscore; SFS, stool frequency subscore; TNF, tumor
necrosis factor alpha; UC, ulcerative colitis; VDZ, vedolizumab.
Figure 3. Abdominal pain and loose stool frequency subscores in patients with CD. aAdjusted % change from BL mean, where adjustment is for BL subscore and treatment. bUpper limit of 95% CI <0 indicates statistical significance at a nominal significance level of 0.05. Asterisk (*)
indicates statistical significance and NS non-significance.
APS, abdominal pain subscore; BL, baseline; CD, Crohn’s disease; CI, confidence interval; ITT, intent-to-treat;
LSFS, loose stool frequency subscore; PBO, placebo; SE, standard error; tumor necrosis factor alpha; VDZ,
vedolizumab.
Figure 4: Combined score of abdominal pain and loos e stool frequency in patients with CD . aAdjusted % change from BL mean, where adjustment is for BL subscore and treatment. bUpper limit of 95% CI <0 indicates statistical significance at a nominal significance level of 0.05. Asterisk (*)
indicates statistical significance and NS non-significance.
APS, abdominal pain subscore; BL, baseline; CD, Crohn’s disease; CI, confidence interval; LSFS, loose stool
frequency subscore; PBO, placebo; SE, standard error; TNF, tumor necrosis factor alpha; VDZ, vedolizumab.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Figure 5. Proportion of patients with CD (GEMINI 2 and 3) who achieved the average daily composite sco re
of AP ≤1 and LSF ≤3. aLower 95% CI limits >0 indicate statistical significance at a nominal significance level of 0.05. Asterisk (*) indicates
statistical significance and NS non-significance.
APS, abdominal pain subscore; CD, Crohn’s disease; CI, confidence interval; LSFS, loose stool frequency subscore;
PBO, placebo; TNF, tumor necrosis factor alpha; VDZ, vedolizumab.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
References
1. Ordas I, Eckmann L, Talamini M, et al. Ulcerative colitis. Lancet 2012;380:1606-19.
2. Torres J, Mehandru S, Colombel JF, et al. Crohn's disease. Lancet 2017;389:1741-1755.
3. El-Matary W. Patient-reported outcome measures in inflammatory bowel disease. Can J Gastroenterol
Hepatol 2014;28:536-42.
4. Peyrin-Biroulet L, Sandborn W, Sands BE, et al. Selecting Therapeutic Targets in Inflammatory Bowel
Disease (STRIDE): determining therapeutic goals for treat-to-target. Am J Gastroenterol 2015;110:1324-38.
5. Jairath V, Khanna R, Zou GY, et al. Development of interim patient-reported outcome measures for the
assessment of ulcerative colitis disease activity in clinical trials. Aliment Pharmacol Ther 2015;42:1200-10.
6. Williet N, Sandborn WJ, Peyrin-Biroulet L. Patient-reported outcomes as primary end points in clinical trials
of inflammatory bowel disease. Clin Gastroenterol Hepatol 2014;12:1246-56 e6.
7. Khanna R, Zou G, D'Haens G, et al. A retrospective analysis: the development of patient reported outcome
measures for the assessment of Crohn's disease activity. Aliment Pharmacol Ther 2015;41:77-86.
8. Soler D, Chapman T, Yang LL, et al. The binding specificity and selective antagonism of vedolizumab, an
anti-alpha4beta7 integrin therapeutic antibody in development for inflammatory bowel diseases. J
Pharmacol Exp Ther 2009;330:864-75.
9. Wyant T, Fedyk E, Abhyankar B. An overview of the mechanism of action of the monoclonal antibody
vedolizumab. J Crohns Colitis 2016;10:1437-1444.
10. Feagan BG, Rutgeerts P, Sands BE, et al. Vedolizumab as induction and maintenance therapy for ulcerative
colitis. N Engl J Med 2013;369:699-710.
11. Sandborn WJ, Feagan BG, Rutgeerts P, et al. Vedolizumab as induction and maintenance therapy for
Crohn's disease. N Engl J Med 2013;369:711-21.
12. Sands BE, Sandborn WJ, Van Assche G, et al. Vedolizumab as induction and maintenance therapy for
Crohn's disease in patients naive to or who have failed tumor necrosis factor antagonist therapy. Inflamm
Bowel Dis 2017;23:97-106.
13. Feagan BG, Rubin DT, Danese S, et al. Efficacy of vedolizumab induction and maintenance therapy in
patients With ulcerative colitis, regardless of prior exposure to tumor necrosis factor antagonists. Clin
Gastroenterol Hepatol 2017;15:229-239 e5.
14. Dulai P, Meserve JD, Hartke JG, et al. Predictors of Clinical and Endoscopic Response with Vedolizumab for
the Treatment of Moderately-Severely Active Ulcerative Colitis: Results from the us Victory Consortium.
Gastroenterology;152:S371.
15. Sandborn W, Gasink C, Blank M, et al. O-001 A Multicenter, Double-Blind, Placebo-Controlled Phase3 Study
of Ustekinumab, a Human IL-12/23P40 mAB, in Moderate-Service Crohn's Disease Refractory to Anti-TFNα:
UNITI-1. Inflammatory Bowel Diseases 2016;22:S1-S1.
16. Colombel JF, Keir ME, Scherl A, et al. Discrepancies between patient-reported outcomes, and endoscopic
and histological appearance in UC. Gut 2016.
17. Torres J, Billioud V, Sachar DB, et al. Ulcerative colitis as a progressive disease: the forgotten evidence.
Inflamm Bowel Dis 2012;18:1356-63.
18. Sands BE, Feagan BG, Rutgeerts P, et al. Effects of vedolizumab induction therapy for patients with Crohn's
disease in whom tumor necrosis factor antagonist treatment failed. Gastroenterology 2014;147:618-627
e3.
19. Gasink C, Friedman J, Gao LL, et al. Evaluation of an interim Crohn's disease outcome measure (PRO-2)
based on two patient-reported components (stool frequency, abdominal pain) of the Crohn's Disease
Activity Index (CDAI) in the ustekinumab CERTIFI Study. J Crohns Colitis 2015;9:S158.
20. Peyrin-Biroulet L, Reinisch W, Colombel JF, et al. Clinical disease activity, C-reactive protein normalisation
and mucosal healing in Crohn's disease in the SONIC trial. Gut 2014;63:88-95.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
21. Kochhar G, Parikh M, Chaudrey K, et al. Mucosal healing with vedolizumab in ulcerative colitis and Crohn’s
disease: outcomes from the VICTORY consortium, In Advances in Inflammatory Bowel Diseases, Orlando,
FL, 2016.
22. Stallmach A, Langbein C, Atreya R, et al. Vedolizumab provides clinical benefit over 1 year in patients with
active inflammatory bowel disease - a prospective multicenter observational study. Aliment Pharmacol
Ther 2016;44:1199-1212.
23. Vickers AD, Ainsworth C, Mody R, et al. Systematic review with network meta-analysis: Comparative
efficacy of biologics in the treatment of moderately to severely active ulcerative colitis. PLoS One
2016;11:e0165435.
24. Dulai PS, Singh S, Jiang X, et al. The Real-World Effectiveness and Safety of Vedolizumab for Moderate-
Severe Crohn's Disease: Results From the US VICTORY Consortium. Am J Gastroenterol 2016;111:1147-55.
25. Raluy-Callado M, N. A, Donaldson R, et al. P288. A real-world study of outcomes in biologic-naïve patients
with Crohn’s disease and ulcerative colitis initiating vedolizumab, In European Crohn's and Colitis
Organisation, Amsterdam, The Netherlands, 2016.
26. Allegretti JR, Barnes EL, Stevens B, et al. Predictors of clinical response and remission at 1 year among a
multicenter cohort of patients with inflammatory bowel disease treated with vedolizumab. Dig Dis Sci
2017;62:1590-1596.
27. Peyrin-Biroulet L, Feagan BG, Mansfield J, et al. OP011 Etrolizumab treatment leads to early improvement
in symptoms and inflammatory biomarkers in anti-TNF-refractory patients in the open-label induction
cohort of the phase 3 HICKORY study, In European Crohn's and Colitis Organisation, barcelona, Spain, 2017.
28. Takeda. Entyvio (vedolizumab) [package insert]. Deerfield, IL: Takeda Pharmaceuticals America, Inc., 2014.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Feagan et al. 1
1
Supplemental material
Detailed figure legend
Figure 1. Rectal bleeding and stool frequency subsc ores in patients with UC. Percentage change from baseline in RB subscore in the overall
ITT (A), TNF antagonist-naïve (B), and TNF antagonist-exposed (C) populations and in SF subscore in the overall ITT (D), TNF antagonist-naïve
(E), and TNF antagonist-exposed (F) populations after vedolizumab or placebo administration. aData points represent adjusted % change from BL mean, where adjustment is for subscore BL value and treatment. Error bars represent standard
error. b Difference adjusted % change [VDZ - PBO]=adjusted mean % change from BL for VDZ – adjusted mean % change from BL for PBO. Upper limit
of 95% CI <0 indicates statistical significance at a nominal significance level of 0.05. Asterisk (*) indicates statistical significance and NS non-
significance.
Patients with baseline RBS=0 or SFS=0 were excluded from this analysis. Of note, the number of patients varies per study population at weeks 2,
4, and 6 and is reported below the x-axis.
BL, baseline; CI, confidence interval; ITT, intent-to-treat; PBO, placebo; RBS, rectal bleeding subscore; SFS, stool frequency subscore; TNF,
tumor necrosis factor alpha; UC, ulcerative colitis; VDZ, vedolizumab.
Figure 2. Proportion of patients with UC who achiev ed the composite score RBS=0 and SFS ≤1 in the overall ITT (A), TNF antagonist-
naïve (B), and TNF antagonist-exposed (C) populatio ns. aDifference adjusted % change [VDZ – PBO]=% of VDZ patients who achieved the indicated subscore – % of PBO patients who achieved the
indicated subscore. Lower 95% CI limits >0 indicate statistical significance at a nominal significance level of 0.05. Asterisk (*) indicates statistical
significance and NS non-significance.
CI, confidence interval; PBO, placebo; RBS, rectal bleeding subscore; SFS, stool frequency subscore; TNF, tumor necrosis factor alpha; UC,
ulcerative colitis; VDZ, vedolizumab.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Feagan et al. 2
2
Figure 3. Abdominal pain subscores in patients with CD. Percentage change from baseline in AP subscore in overall ITT (A), TNF antagonist-
naïve (B), and TNF antagonist-exposed (C) populations and percentage change from baseline in LSF subscore in overall ITT (D), TNF antagonist-
naïve (E), and TNF antagonist-exposed (F) populations after vedolizumab or placebo administration. aData points represent adjusted % change from BL mean, where adjustment is for subscore BL value and treatment. Error bars represent standard
error. bDifference adjusted % change [VDZ – PBO]=% =adjusted mean % change from BL for VDZ – adjusted mean % change from BL for PBO. Upper
limit of 95% CI <0 indicates statistical significance at a nominal significance level of 0.05. Asterisk (*) indicates statistical significance and NS non-
significance.
Patients with baseline APS=0 or LSFS=0 were excluded from this analysis.
APS, abdominal pain subscore; BL, baseline; CD, Crohn’s disease; CI, confidence interval; ITT, intent-to-treat; LSFS, loose stool frequency
subscore; PBO, placebo; SE, standard error; tumor necrosis factor alpha; VDZ, vedolizumab.
Figure 4: Combined score of abdominal pain and loos e stool frequency in patients with CD . Percentage change from baseline in AP and
LSF subscores in the overall ITT (A), TNF antagonist-naïve (B), and TNF antagonist-exposed (C) populations after vedolizumab or placebo
administration. aData points represent adjusted % change from BL mean, where adjustment is for subscore BL value and treatment. Error bars represent standard
error. bDifference adjusted % change [VDZ – PBO]=adjusted mean % change from BL for VDZ – adjusted mean % change from BL for PBO. Upper limit
of 95% CI <0 indicates statistical significance at a nominal significance level of 0.05. Asterisk (*) indicates statistical significance and NS non-
significance.
Patients with baseline APS=0 and LSFS=0 were excluded from this analysis.
APS, abdominal pain subscore; BL, baseline; CD, Crohn’s disease; CI, confidence interval; LSFS, loose stool frequency subscore; PBO, placebo;
SE, standard error; TNF, tumor necrosis factor alpha; VDZ, vedolizumab.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Feagan et al. 3
3
Figure 5. Proportion of patients with CD (GEMINI 2 and 3) who achieved the average daily composite sco re of AP ≤1 and LSF ≤3 in the
overall ITT (A), TNF antagonist-naïve (B), and TNF antagonist-exposed (C) populations. aDifference adjusted % change [VDZ – PBO]=% of VDZ patients who achieved the indicated subscore – % of PBO patients who achieved the
indicated subscore. Lower 95% CI limits >0 indicate statistical significance at a nominal significance level of 0.05. Asterisk (*) indicates statistical
significance and NS non-significance.
APS, abdominal pain subscore; CD, Crohn’s disease; CI, confidence interval; LSFS, loose stool frequency subscore; PBO, placebo; TNF, tumor
necrosis factor alpha; VDZ, vedolizumab.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Feagan et al. 4
4
Tables
Table S1. Baseline Characteristics of Patients With U C
Characteristic Overall TNF antagonist-naïve a TNF antagonist-exposed
Placebo n=149
Vedolizumab n=225
Placebo n=76
Vedolizumab n=130
Placebo n=73
Vedolizumab n=95
Age (years), median (min, max)
40.7 (19, 76) 39.4 (18, 73) 39.8 (19, 65) 38.9 (18, 73)
40.8 (19, 76) 40.4 (19, 73)
Sex (male), n (%) 92 (62) 132 (59) 47 (62) 69 (53) 45 (62) 63 (66)
Weight (kg), median (min, max)
71.1 (40, 125) 72.0 (33, 118) 70.9 (40, 125) 67.4 (33, 118) 71.8 (47, 111) 77.3 (38, 113)
Current smoker, n (%) 11 (7) 12 (5) 7 (9) 7 (5) 4 (5) 5 (5)
Duration of disease (years), median (min, max)
4.5 (0.5, 38.5) 4.6 (0.5, 25.8) 3.4 (0.5, 37.4) 3.9 (0.5, 25.8) 5.3 (0.7, 38.5) 5.0 (0.5, 21.6)
Complete Mayo Clinic Score, median (min, max)
8.0 (3, 12) 9.0 (5, 12) 8.0 (4, 12) 8.0 (5, 12) 9.0 (3, 12) 9.0 (5, 12)
Disease localizationb, n (%)
Proctosigmoiditis 22 (15) 25 (11) 10 (13) 14 (11) 12 (16) 11 (12)
Left-sided colitis 59 (40) 92 (41) 35 (46) 66 (51) 24 (33) 26 (27)
Extensive colitis 18 (12) 25 (11) 7 (9) 14 (11) 11 (15) 11 (12)
Pancolitis 50 (34) 83 (37) 24 (32) 36 (28) 26 (36) 47 (49)
History of EIMs, n (%) 44 (30) 74 (33) N/A N/A N/A N/A
EIMs, n (%) N/A N/A 17 (22) 39 (30) 27 (37) 35 (37)
Concomitant medications (yes), n (%)
CS only 58 (39) 79 (35) 28 (37) 42 (32) 30 (41) 37 (39)
IMM only 18 (12) 28 (12) 10 (13) 24 (18) 8 (11) 4 (4)
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Feagan et al. 5
5
CS and IMM 26 (17) 47 (21) 16 (21) 31 (24) 10 (14) 16 (17)
No CS and IMM 47 (32) 71 (32) 22 (29) 33 (25) 25 (34) 38 (40) Type of TNF antagonist failure, n (%)c
≥1 Failure 63 (42) 82 (36) N/A N/A 58 (82) 80 (84)
Inadequate responsed 29 (46) 44 (54) N/A N/A 26 (45) 43 (54)
Loss of responsee 26 (41) 32 (39) N/A N/A 24 (41) 32 (40)
Intolerancef 8 (13) 6 (7) N/A N/A 8 (14) 5 (6) CRF, case report form; CS, corticosteroid; EIM, extraintestinal manifestation; IMM, immunomodulator; IVRS, interactive voice response system; N/A, not applicable (or not available for EIMs); TNF, tumor necrosis factor alpha; UC, ulcerative colitis. aTNF antagonist exposure status was derived from data captured on the IVRS at screening and enrollment. bDisease localization was reported by the investigator per CRF options of proctosigmoiditis, left-sided colitis, extensive colitis, or pancolitis. cPrior TNF antagonist failure was defined by data recorded on the CRF at week 0. Each patient was counted only once according to his or her worst outcome. Inadequate response was considered worse than lost response; lost response was considered worse than intolerance. dIncluded in this category were patients who did not have an initial response. eLoss of response indicates that the patient had a response initially but subsequently did not have a response. fIntolerance is defined as occurrence of treatment-related toxicity.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Feagan et al. 6
6
Table S2. Baseline Characteristics of Patients With C D (GEMINI 2 and 3)
Characteristics
Overall TNF antagonist-naïve a TNF antagonist-exposed Placebo
n=355
Vedolizumab
n=429
Placebo
n=126
Vedolizumab
n=160
Placebo
n=229
Vedolizumab
n=269
Age (years), median (min, max) 35.8 (19, 77) 36.0 (18, 77) 34.0 (19, 75) 34.2 (18, 66) 36.5 (19, 77) 36.9 (19, 77)
Sex (male), n (%) 158 (45) 196 (46) 66 (52) 82 (51) 92 (40) 114 (42)
Weight (kg), median (min, max) 66.0 (32, 147) 66.0 (30, 167) 67.0 (32, 147) 63.0 (30, 167) 65.4 (37, 128) 68.0 (40, 144) Current smoker, n (%) 92 (26) 119 (28) 29 (23) 47 (29) 63 (28) 72 (27)
Disease duration (years), median (min, max) 7.1 (0.3, 42.9) 7.7 (0.3, 43.6) 3.6 (0.3, 29.2) 4.5 (0.3, 43.6) 9.0 (0.6, 42.9) 9.3 (0.5, 42.8)
Disease localization, n (%)
Ileum only 50 (14) 70 (16) 23 (18) 35 (22) 27 (12) 35 (13)
Colon only 95 (27) 110 (26) 40 (32) 40 (25) 55 (24) 70 (26)
Ileum and colon 210 (59) 249 (58) 63 (50) 85 (53) 147 (64) 164 (61)
CDAI score, median (min, max) 303.0
(155, 584) 318.0
(132, 524) 298.5
(155, 584) 311.0
(132, 500) 308.0
(166, 564) 321.5
(142, 524)
Prior surgery for CD, n (%) 143 (40) 190 (44) 25 (20) 58 (36) 118 (52) 132 (49)
History of fistulizing disease, n (%) 133 (37) 161 (38) 26 (21) 55 (34) 107 (47) 106 (39)
Draining fistulae, n (%) 48 (14) 63 (15) 18 (14) 26 (16) 30 (13) 37 (14)
History of EIMs, n (%) 297 (84) 343 (80) 92 (73) 118 (74) 205 (90) 225 (84)
EIMs, n (%) 237 (67) 249 (58) 77 (61) 98 (61) 160 (70) 151 (56)
Concomitant medications, n (%)
CS only 117 (33) 140 (33) 32 (25) 43 (27) 85 (37) 97 (36)
IMM only 58 (16) 71 (17) 28 (22) 32 (20) 30 (13) 39 (14)
CS and IMM 62 (17) 75 (17) 28 (22) 35 (22) 34 (15) 40 (15)
No CS and IMM 118 (33) 143 (33) 38 (30) 50 (31) 80 (35) 93 (35)
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Feagan et al. 7
7
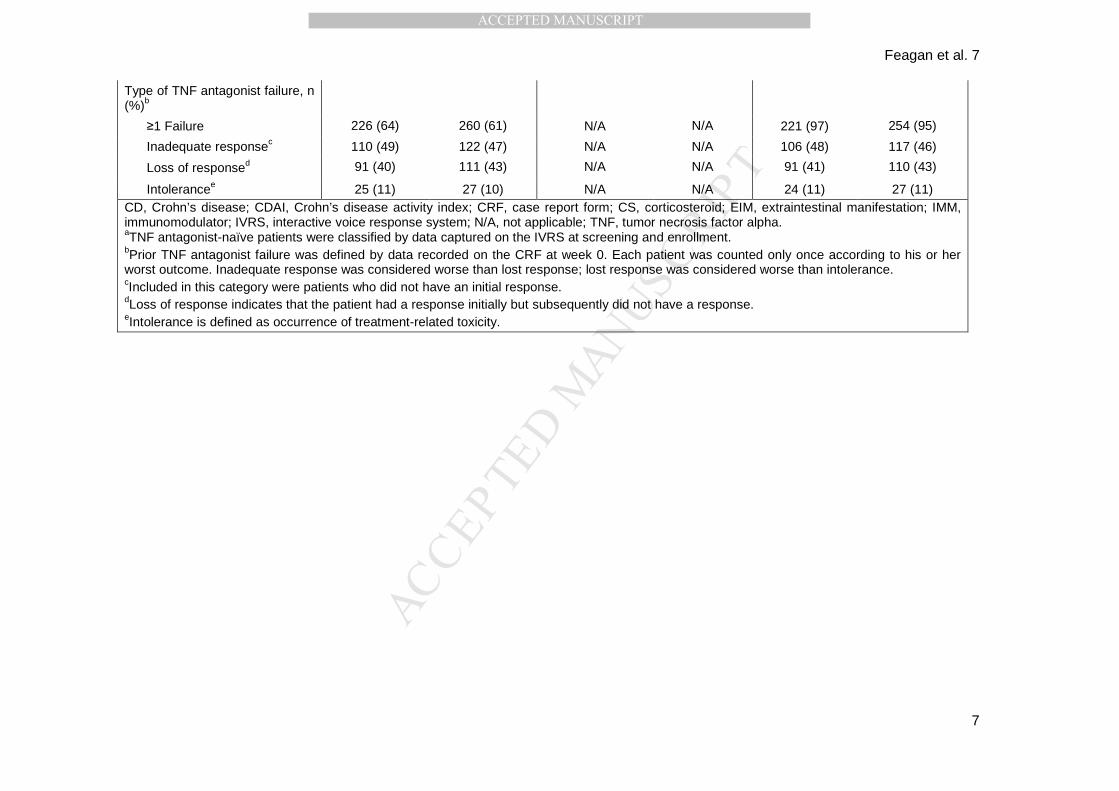
Type of TNF antagonist failure, n (%)b
≥1 Failure 226 (64) 260 (61) N/A N/A 221 (97) 254 (95)
Inadequate responsec 110 (49) 122 (47) N/A N/A 106 (48) 117 (46)
Loss of responsed 91 (40) 111 (43) N/A N/A 91 (41) 110 (43)
Intolerancee 25 (11) 27 (10) N/A N/A 24 (11) 27 (11) CD, Crohn’s disease; CDAI, Crohn’s disease activity index; CRF, case report form; CS, corticosteroid; EIM, extraintestinal manifestation; IMM, immunomodulator; IVRS, interactive voice response system; N/A, not applicable; TNF, tumor necrosis factor alpha. aTNF antagonist-naïve patients were classified by data captured on the IVRS at screening and enrollment. bPrior TNF antagonist failure was defined by data recorded on the CRF at week 0. Each patient was counted only once according to his or her worst outcome. Inadequate response was considered worse than lost response; lost response was considered worse than intolerance. cIncluded in this category were patients who did not have an initial response. dLoss of response indicates that the patient had a response initially but subsequently did not have a response. eIntolerance is defined as occurrence of treatment-related toxicity.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Feagan et al. 8
8
Table S3. Baseline Characteristics of Patients With C D
Characteristics
Overall (GEMINI 2) Overall (GEMINI 2 and 3) Placebo
n=148
Vedolizumab
n=220
Placebo
n=355
Vedolizumab
n=429
Age (years), median (min, max) 36.7 (19, 75) 34.8 (18, 77) 35.8 (19, 77) 36.0 (18, 77)
Sex (male), n (%) 69 (47) 105 (48) 158 (45) 196 (46)
Weight (kg), median (min, max) 66.0 (32, 130) 65.2 (30, 167) 66.0 (32, 147) 66.0 (30, 167) Current smoker, n (%) 34 (23) 54 (25) 92 (26) 119 (28)
Disease duration (years), median (min, max) 6.1 (0.3, 42.0) 7.1 (0.5, 43.6) 7.1 (0.3, 42.9) 7.7 (0.3, 43.6)
Disease localization, n (%)
Ileum only 21 (14) 37 (17) 50 (14) 70 (16)
Colon only 43 (29) 62 (28) 95 (27) 110 (26)
Ileum and colon 84 (57) 121 (55) 210 (59) 249 (58)
CDAI score, median (min, max)
319.0 (155, 584)
324.0 (132, 500)
303.0 (155, 584)
318.0 (132, 524)
Prior surgery for CD, n (%) 54 (36) 98 (45) 143 (40) 190 (44)
History of fistulizing disease, n (%) 56 (38) 90 (41) 133 (37) 161 (38)
Draining fistulae, n (%) 23 (16) 38 (17) 48 (14) 63 (15)
History of EIMs, n (%) 123 (83) 177 (80) 297 (84) 343 (80)
EIMs, n (%) 107 (72) 133 (60) 237 (67) 249 (58)
Concomitant medications, n (%)
CS only 45 (30) 67 (30) 117 (33) 140 (33)
IMM only 25 (17) 37 (17) 58 (16) 71 (17)
CS and IMM 26 (18) 38 (17) 62 (17) 75 (17)
No CS and IMM 52 (35) 78 (35) 118 (33) 143 (33)
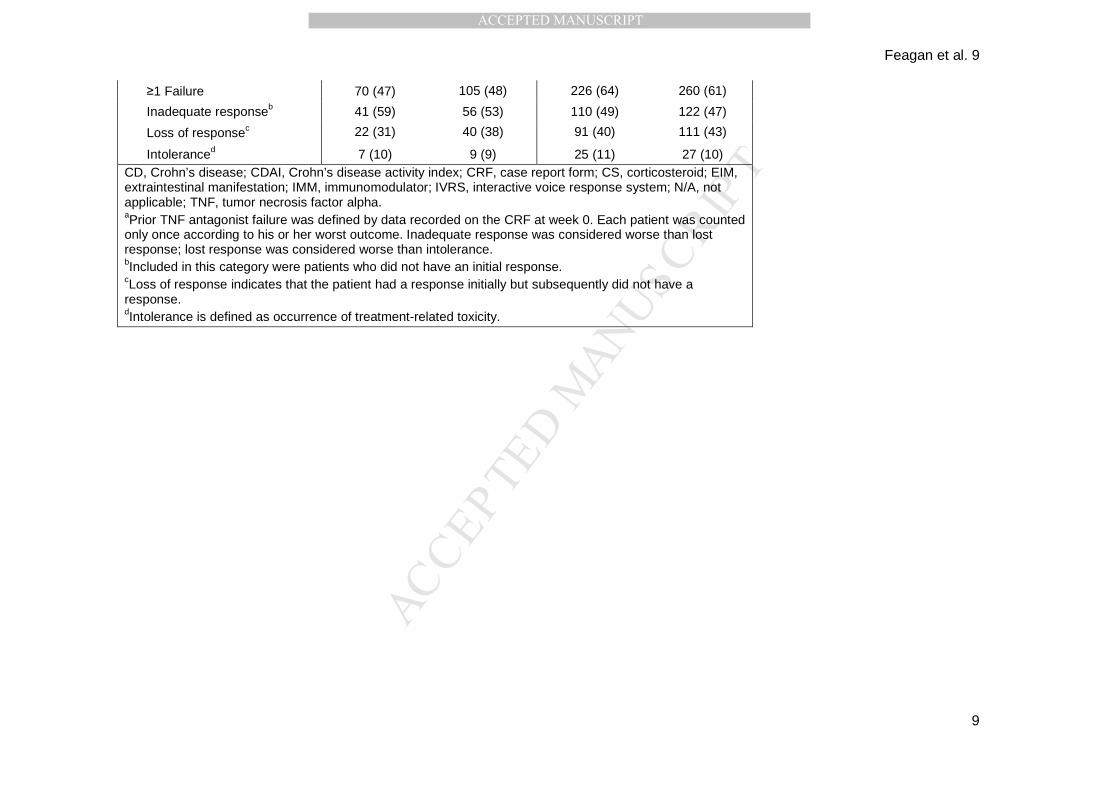
Type of TNF antagonist failure, n (%)a
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Feagan et al. 9
9
≥1 Failure 70 (47) 105 (48) 226 (64) 260 (61)
Inadequate responseb 41 (59) 56 (53) 110 (49) 122 (47)
Loss of responsec 22 (31) 40 (38) 91 (40) 111 (43)
Intoleranced 7 (10) 9 (9) 25 (11) 27 (10) CD, Crohn’s disease; CDAI, Crohn’s disease activity index; CRF, case report form; CS, corticosteroid; EIM, extraintestinal manifestation; IMM, immunomodulator; IVRS, interactive voice response system; N/A, not applicable; TNF, tumor necrosis factor alpha. aPrior TNF antagonist failure was defined by data recorded on the CRF at week 0. Each patient was counted only once according to his or her worst outcome. Inadequate response was considered worse than lost response; lost response was considered worse than intolerance. bIncluded in this category were patients who did not have an initial response. cLoss of response indicates that the patient had a response initially but subsequently did not have a response. dIntolerance is defined as occurrence of treatment-related toxicity.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
10
Table S4. Predictors of Week 2 Outcomes in UC
RBS=0 AND SFS ≤1
Variable OR estimates a P value Age (at first dose) 1.009 0.4677 Sex (female vs male) 1.155 0.6729 Smoker (current/previous smoker vs non-smoker) 0.964 0.9188 UC duration 0.981 0.5887 UC duration (≥2 y vs <2 y) 1.468 0.4226 UC duration (≥5 y vs <5 y) 0.95 0.8789 Prior hospitalization (no vs yes) 1.691 0.1582 EIM (no vs yes) 1.335 0.4405 Disease severity based on Complete Mayo Clinic Score (<10 vs ≥10) 12.228 0.0007* Previous bowel surgery (no vs yes) <0.001 0.9879 Previous TNF antagonist exposure (no vs yes) 1.661 0.1562 TNF antagonist failure (no vs yes) 1.615 0.1985 CS (no vs yes) 0.707 0.32 IMM (no vs yes) 0.918 0.8105 Baseline fecal calprotectin 1 0.9235 Baseline Partial Mayo Clinic Score 0.391 <0.0001* Baseline Complete Mayo Clinic Score 0.386 <0.0001* Baseline albumin 1.041 0.2855 BMI 1.038 0.2811 Race (non-white vs white) 1.195 0.6722 Ethnicity (other vs non-Hispanic/Latino)b 2.529 0.1132 Region (Rest of world vs N America)c 0.771 0.4565 Baseline endoscopy (moderate vs severe) 1.495 0.2375 Baseline stool frequency 1 vs 0 0.318 0.1127 Baseline stool frequency 2 vs 0 0.193 0.919 Baseline stool frequency 3 vs 0 0.02 <0.0001* Baseline rectal bleeding 1 vs 0 0.471 0.9625 Baseline rectal bleeding 2 vs 0 0.128 0.976 Baseline rectal bleeding 3 vs 0 <0.001 0.9644 Baseline stool frequency (non-severe vs severe) 14.559 <0.0001* Baseline rectal bleeding (non-severe vs severe) Non-Est 0.9649 Pancolitis 1.113 0.762 Left-sided colitis 0.846 0.6251 Extensive colitis 0.938 0.9046 Proctosigmoiditis 1.272 0.6754 BMI, body mass index; CS, corticosteroid; IMM, immunomodulator; EIM, extraintestinal manifestation; Non-Est, non-estimated; OR, odds ratio; RBS, rectal bleeding score; SFS, stool frequency score; TNF, tumor necrosis factor alpha; UC, ulcerative colitis. aOR estimates are based on a logistic regression model with achieving RBS=0 or SFS ≤1 or both as the response variable. bOther race includes American Indian or Alaskan Native, Asian, Black, and Native Hawaiian or Other Pacific Islander. cRest of world includes Western/Northern Europe, Central Europe, Eastern Europe, and Africa/Asia/Australia. *P value ≤0.05 is considered statistically significant.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
11
Table S5. Predictors of Week 2 Outcomes in CD
Variable
Average daily abdominal pain score ≤1 and loose stool
frequency ≤3
Odds ratioa P value
Age (at first dose) 0.973 0.1465 Sex (female vs male) 0.389 0.0259* Smoker (current/previous smoker vs non-smoker) 0.499 0.1013 CD duration 0.938 0.0575 CD duration (≥2y vs <2y) 0.406 0.0477* CD duration (≥5y vs <5y) 0.268 0.0016* Prior hospitalization (no vs yes) 1.334 0.498 Colonic disease localization (no vs yes) 1.73 0.2417 Ileum disease localization (no vs yes) 0.705 0.4686 Fistulae assessment perianal (no vs yes) 0.588 0.2845 EIM (no vs yes) 0.991 0.9832 History of fistulizing disease (no vs yes) 1.065 0.8774 Disease severity based on HBI (>16 vs ≤16) <0.001 0.9766 Previous bowel surgery (no vs yes) 2.669 0.0308* Previous TNF antagonist exposure (no vs yes) 2.894 0.0132* TNF antagonist failure (no vs yes) 3.81 0.0036* CS (no vs yes) 0.396 0.0291* IMM (no vs yes) 0.899 0.7971 Baseline CDAI score 0.992 0.0139* Baseline CRP score 0.986 0.1882 Baseline HBI score 0.859 0.0135* Race (non-white vs white) 2.393 0.0557 Ethnicity (other vs non-Hispanic/Latino)b 1.363 0.7763 Region (Rest of world vs N America)c 1.872 0.1928 Draining fistula (no vs yes) 0.569 0.23 Baseline fecal calprotectin 1 0.1305 BMI 0.954 0.2578 Baseline weighted 7-day abdominal pain 0.964 0.0589 Baseline weighted 7-day liquid or very soft stools 0.978 0.0245* Baseline albumin 0.988 0.7256 BMI, body mass index; CD, Crohn’s disease; CDAI, Crohn’s disease activity index; CRP, C-reactive protein; CS, corticosteroid; EIM, extraintestinal manifestation; HBI, Harvey-Bradshaw index; IMM, immunomodulatory; TNF, tumor necrosis factor alpha. bOther race includes American Indian or Alaskan Native, Asian, Black, and Native Hawaiian or Other Pacific Islander. cRest of world includes Western/Northern Europe, Central Europe, Eastern Europe, and Africa/Asia/Australia. *P value ≤0.05 is considered statistically significant.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
12
Table S6. Logistic Regression Analysis for UC and CD Patients Achieving Week 2 Outcomes
RBS=0 AND SFS ≤1 (UC) APS ≤1 and LSFS ≤3 (CD)
Variable ORa P value ORa P value Baseline Complete Mayo Clinic Score 0.386 <0.0001 N/A CD duration (≥5y vs <5y)b N/A 0.289 0.0035 CS (no vs yes) N/A 0.405 0.0388 Baseline CDAI score N/A 0.993 0.0249 Study (GEMINI 3 vs GEMINI 2) N/A 0.149 0.0007 APS, abdominal pain score; CD, Crohn’s disease; CDAI, CD activity index; CS, corticosteroids; LSFS, loose stool frequency score; N/A, not applicable; OR, odds ratio; RBS, rectal bleeding score; SFS, stool frequency score; UC, ulcerative colitis. aOR ratios are based on a logistic regression model with achieving the outcome as the response variable. P value ≤0.05 is considered statistically significant.
b Because of overlap between some predictors, CD duration of ≥5y vs <5y years, not ≥2y vs <2y years, and previous exposure, not failure to TNF antagonists, were included in the multivariate analysis model.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
13
Figure S1.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
14
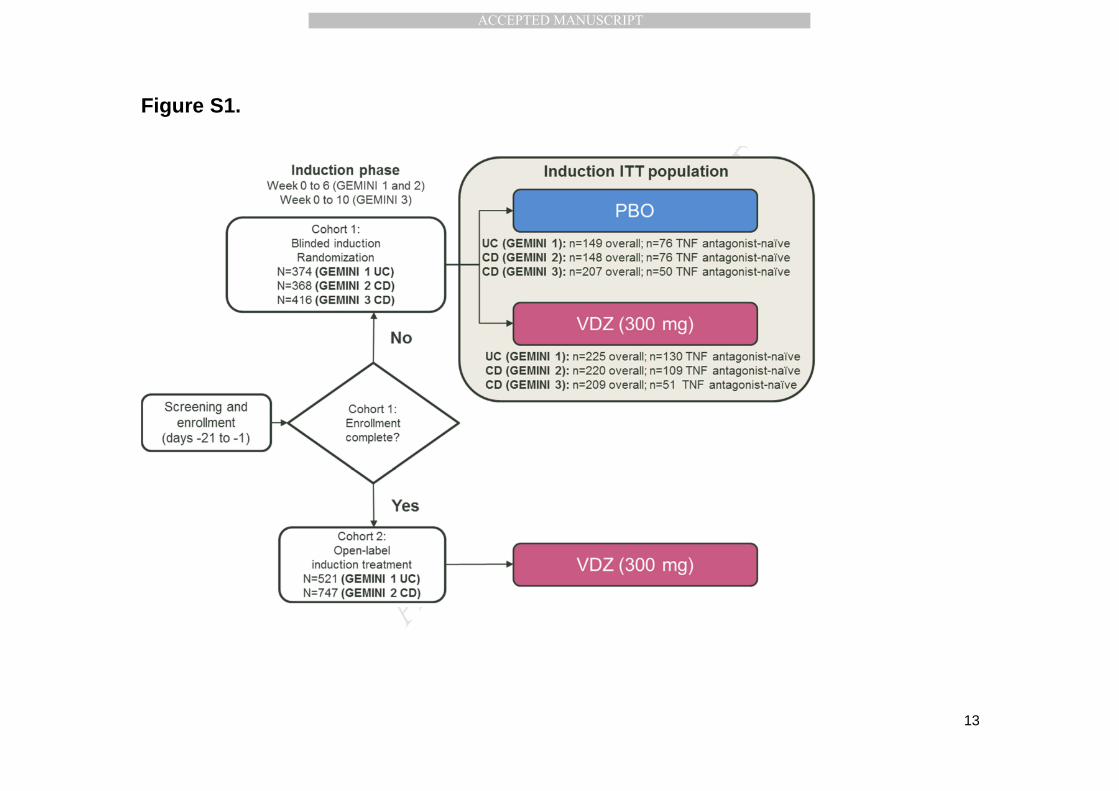
Figure S1. GEMINI study design. During the induction phase for GEMINI 1 and 2, patients with UC or CD received double-blind vedolizumab or
placebo (cohort 1) or open-label vedolizumab (cohort 2) at weeks 0 and 2. For GEMINI 3, patients with CD received double-blind vedolizumab or
placebo at weeks 0, 2, and 6. Data for prior TNF antagonist use were obtained from responses on the IVRS during screening and enrollment.
Patients with prior exposure to a TNF antagonist according to the IVRS and without prior failure according to the CRF were excluded from the
analyses.
CD, Crohn’s disease; CRF, case report form; ITT, intention-to-treat; IVRS, interactive voice response system; PBO, placebo; TNF, tumor necrosis
factor alpha; UC, ulcerative colitis; VDZ, vedolizumab.
Adapted from Feagan BG, et al. Clin Gastroenterol Hepatol. 2017;15(2):229-239 and Sands BE, et al. Inflamm Bowel Dis. 2017;23(1):97-106.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Background: Vedolizumab, an antibody against α4β7 integrin, is indicated for
ulcerative colitis (UC) and Crohn’s disease (CD). We investigated the time course of
clinical response to vedolizumab in TNF-naïve or -experienced patients.
Findings: Vedolizumab improved patient-reported symptoms of UC and CD as early as
week 2 of treatment, with continuing improvement through week 6—especially for TNF-
naïve patients.
Implications for Patient Care: These findings have implications for optimal positioning
of vedolizumab in treatment algorithms. The rapid improvement of UC and CD
symptoms in TNF-naïve patients supports vedolizumab’s use as a first-line biologic.