randall g.trudell, m.d. steven p.rider, m.d. brian f ... · steven p.rider, m.d. brian f.wiseman,...
TRANSCRIPT
KNC Randall G. Trudell, M.D.Steven P. Rider, M.D.Brian F. Wiseman, M.D.Karen A. Mullins, D.O.Ronald E. Leppanen, Ph.D., FASNM
NeurophysiologistJennifer K. Sparks N.P.-C.KNOXVILLE
NEUROLOGYCLINIC
Dear New Patient:
Welcome to Knoxville Neurology Clinic. Wewould like tomake your visit as pleasant and productive as possible and inorder to do that we need your help with the following:
• Please bring any and all medical records with you to yourappointment. It is especially important that your neurologisthave the results of any test that you have taken because .of your current medical problem, such as MRI's,CATScans,EEG's,EMG's,bloodwork, etc.
• Please bring your recent CATScan and MRIfilms/CDso your neurologist can personally review them. MostRadiology departments are willing to provide you with CDs.Please make sure you bring awritten report.
• Please take a few minutes to fill out the enclosed four pagehistory and bring to your visit.
• If a referral is needed from your insurance company, makesure it has been obtained and we have the referral beforeyour appointment.
Having the above completed before your visit will helpensure that your KNC physician has all the information needed.to help you with your problem. We look forward to serving you.
appointment date / time
Knoxville Neurology Clinic2200 Sutherland Avenue
Cherokee MillsKnoxville,TN 37919
Telephone: 865-521-6174Fax: 865-546-4065
KNOXVILLE NEUROLOGY CLINIC2200 SUTHERLAND AVENUE
CHEROKEE MILLSKNOXVILLE, TN 37919
865-521-6174From 1-40 GOING EAST
• TAKE EXIT 386B ALCOA HWY (HWY 129)• TAKE THE KINGSTON PIKE EXIT (ROUTE 70)• TURN RIGHT (WEST) ON TO KINGSTON PIKE• THE NEXT RED LIGHT IS THE INTERSECTION OF KINGSTON PIKE,
CONCORD STREET AND NEYLAND DRIVE, TAKE A RIGHT ON TOCONCORD STREET
• THE NEXT RED LIGHT IS THE INTERSECTION OF CONCORDSTREET AND SUTHERLAND AVENUE
OUR BUILDING IS ON THE LEFT, YOU MAY ENTER THE PARKING LOT FROMCONCORD STREET OR SUTHERLAND AVENUE
From 275 SOUTH OR 1-40 GOING WEST• TAKE EXIT 386B ALCOA HIGHWAY (HWY 129)• TAKE THE KINGSTON PIKE EXIT (ROUTE 70)• TURN RIGHT (WEST) ON TO KINGSTON PIKE• THE NEXT RED LIGHT IS THE INTERSECTION OF KINGSTON PIKE,
CONCORD STREET AND NEYLAND DRIVE, TAKE A RIGHT ON TOCONCORD STREET
• THE NEXT RED LIGHT IS THE INTERSECTION OF CONCORD STREETAND SUTHERLAND AVENUE
OUR BUILDING IS ON THE LEFT, YOU MAY ENTER THE PARKING LOT FROMCONCORD STREET OR SUTHERLAND AVENUE
From MARYVILLE• TAKE ALCOA HIGHWAY (HWY 129) NORTH• TAKE THE KINGSTON PIKE EXIT (ROUTE 70)• TURN LEFT (WEST) ON TO KINGSTON PIKE• THE NEXT RED LIGHT IS THE INTERSECTION OF KINGSTON PIKE,
CONCORD STREET AND NEYLAND DRIVE, TAKE A RIGHT ON TOCONCORD STREET
• THE NEXT RED LIGHT IS THE INTERSECTION OF CONCORD STREETAND SUTHERLAND AVENUE
OUR BUILDING IS ON THE LEFT, YOU MAY ENTER THE PARKING LOT FROMCONCORD STREET OR SUTHERLAND AVENUE
Last
Please PrintDr. you will see today _
First MiddleStreetAddress _Mailing Address _City State Zip _Home phone # Cell phone # _Birthdate Social Security #
Male 0 Female 0 Divorced 0I Married 0 Single 0 Widowed 0
Raceo Asiano Black or African Americano Native Hawaiian or Pacific Islandero Other Raceo Patient Declinedo America Indian or Alaskan Nativeo Unknowno White
Ethnicityo African Americano Hispanic or Latinoo Asiano Not Hispanic or Latinoo Caucasiano Unknowno Hispanico Patient Declinedo Native Americano Other
Dr. that referred you here:Drs.Lastname _
Drs. First name, _
Drs. Address, _
Drs.Phone# _
Languageo Englisho Spanisho Chinese Mandarino Chinese Cantoneseo Frencho Germano Russiano Japaneseo Italiano Portugese
o Unknowno Patient Declined
Your Primary Care Physician:Dr. Lastname _
Dr. First name _Dr. Address _
D~Phone# _
Your Employer name _
Employer address _Spouse name Birthdate _Employer _
Employer address, _
Employer phone # Employer phone _
In case of emergency list someone that does not live with you.
Name Relationship Phone _
Patient em ail
Primary insurance companyPrimary policy or ID # _
Primary group numberPrimary policy holder name, D.O.B. _
Relationship to patient
Secondary insurance company _Secondary policy or ID # _
Secondary groupSecondary policy holder name D.O.B _
Relationship to patient
Is this a work related injury? yes 0If yes, date of accident _
Name of Worker's Comp insurancej _
Worker's Comp address _
no 0
Worker's Comp phone # _
Worker's Comp contact person
yes 0 no 0Is this an auto accident related injury?
Attention: We do not file auto insurance claims! You will beresponsible for balance at time of service and wewill provide you with a list of your charges to fileyour own claim.
PLEASE ALLOW US TO MAKE A COPY OF YOUR INSURANCE IDENTIFICATION CARD.PLEASE READ: The patient (or guardian) is responsible for all fees, regardless of insurance coverage or pending litigation. Payment is expected at the time service is rendered unless other arrangements havebeen made in advance with our patient accounts manager. Hospitalization charges will be filed with your insurance carrier; however. payment is expected within 60 days regardless of pending insurance payment.AUTHORIZATION AND ASSIGNMENT: I hereby authorize Knoxville Neurology Clinic to furnish information to insurance carriers concerning my illness and treatment and to request additionalmedical information from any hospital or physician who has cared for me, including medication history from pharmacy.] hereby assign to Knoxville Neurology Clinic all payments for medical services rendered to myself or my dependents. I understand that I am responsible for all fees and agreeto stated payment policies. (Any overpayment by insurance carriers will be refunded appropriately).
Signallire, Date. _
Date: / /
KNOXVILLE NEUROLOGY CLINICHEALTH HISTORY QUESTIONNAIRE
All questions contained in this questionnaire are strictly confidential and will become part of your medical record.
DOB ------AGE
/ /Name: 0 M(Last, First, M./.) 0 F
Please list your doctors (starting with the doctor who referred you here):Doctor: Specialty:
Childhood Illness: 0 Measles 0 Mumps 0 Rubella 0 Chickenpox 0 Rheumatic Fever 0 PolioList Any Medical Problems That Other Doctors Have Diagnosed:
Surgeries:Operation: Age or Year:
Other Hospitalizations:Year Reason
List Your Prescribed Drugs and Over-the-Counter Drugs, Such as Vitamins and Inhalers:
Name the Drug How much? When? Name the drug How much? When?1.) 6.)
2.) 7.)
3.) 8.)
4.) 9.)
5.) 10.)More on next page
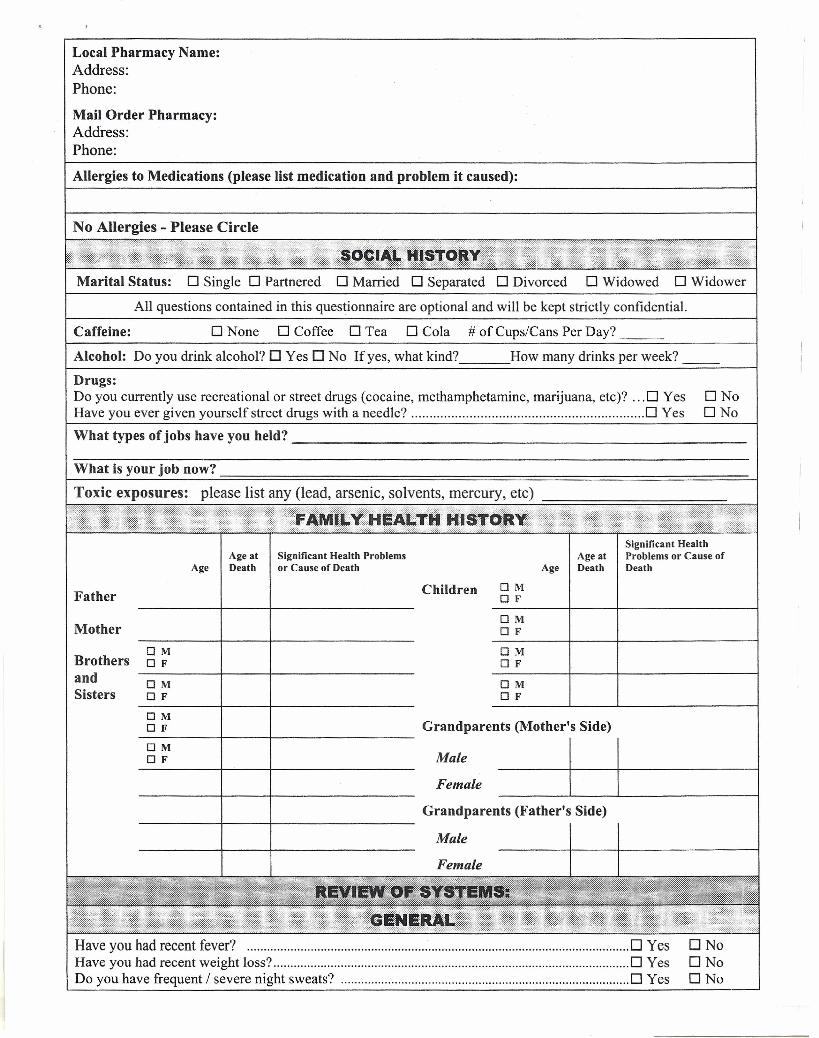
Local Pharmacy Name:Address:Phone:Mail Order Pharmacy:Address:Phone:Allergies to Medications (please list medication and problem it caused):
No Allergies - Please Circle
Marital Status: 0 Single 0 Partnered 0 Married 0 Separated 0 Divorced 0 Widowed 0 Widower
All questions contained in this questionnaire are optional and will be kept strictly confidential.
o None 0 Coffee 0 Tea 0 Cola # of Cups/Cans Per Day?
How many drinks per week? __
Caffeine:
Alcohol: Do you drink alcohol? 0 Yes 0 No If yes, what kind?
Drugs:Do you currently use recreational or street drugs (cocaine, methamphetamine, marijuana, etc)? 0 YesHave you ever given yourself street drugs with a needle? 0 Yes
ONoONo
What types of jobs have you held? _
What is your job now?
Toxic exposures: please list any (lead, arsenic, solvents, mercury, etc)--============---
Age at Significant Health ProblemsAge Death or Cause of Death
Significant HealthAge at Problems or Cause of
Age Death Death
MotherOMOF
Father Children 0 MOF
OMOF
OMOF
Haveyou hadrecentfever? D YesHave you had recent weight loss? 0 YesDo you have frequent / severe night sweats? _ ; 0 Yes
BrothersandSisters
OMOF
OMOF
OMo F Grandparents (Mother's Side)
-g-~--~~--+-------------- ~:~.k I----~I~------------~Grandparents (Father's Side)
----------+-----+------------------Male
Female
DNoONoONo
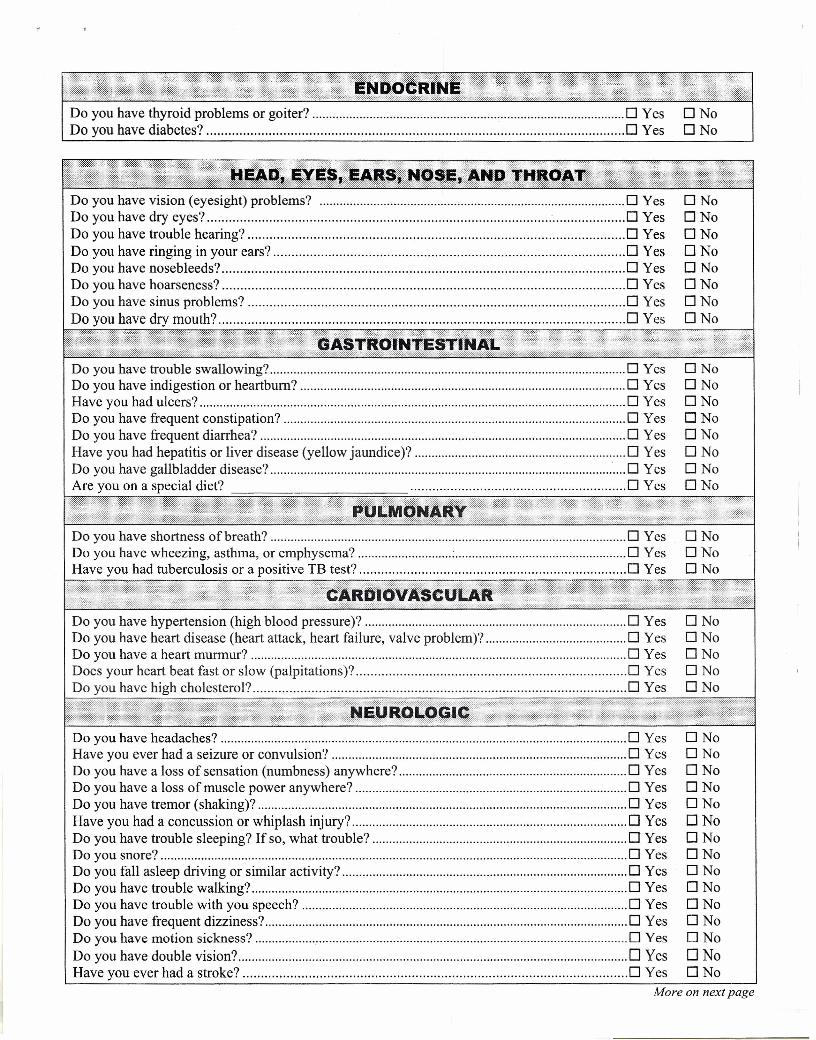
Do you have thyroid problems or goiter? 0 YesDo you have diabetes? 0 Yes
Do you have vision (eyesight) problems? 0 YesDo you have dry eyes? : 0 YesDo you have trouble hearing? 0 YesDo you have ringing in your ears? 0 YesDo you have nosebleeds? 0 YesDo you have hoarseness? 0 YesDo you have sinus problems? 0 YesDo you have dry mouth? 0 Yes
ONoONoONoONoONoONoONoONo
Do you have trouble swallowing? 0 YesDo you have indigestion or heartburn? 0 YesHave you had ulcers? 0 YesDo you have frequent constipation? 0 YesDo you have frequent diarrhea? 0 YesHave you had hepatitis or liver disease (yellow jaundice)? 0 YesDo you have gallbladder disease? 0 YesAre you on a special diet? 0 Yes
ONoDNoONoONoONoONoONoONo
Do you have hypertension (high blood pressure)? 0 YesDo you have heart disease (heart attack, heart failure, valve problem)? 0 YesDo you have a heart murmur? 0 YesDoes your heart beat fast or slow (palpitations)? 0 YesDo you have high cholesterol? 0 Yes
ONoONoONoONoONo
Do you have headaches? 0 Yes 0 NoHave you ever had a seizure or convulsion? 0 Yes 0 NoDo you have a loss of sensation (numbness) anywhere? 0 Yes 0 NoDo you have a loss of muscle power anywhere? 0 Yes 0 NoDo you have tremor (shaking)? 0 Yes 0 NoHave you had a concussion or whiplash injury? 0 Yes 0 NoDo you have trouble sleeping? If so, what trouble? 0 Yes 0 NoDo you snore? 0 Yes 0 NoDo you fall asleep driving or similar activity? 0 Yes 0 NoDo you have trouble walking? 0 Yes 0 NoDo you have trouble with you speech? 0 Yes 0 NoDo you have frequent dizziness? 0 Yes 0 NoDo you have motion sickness? 0 Yes 0 NoDo you have double vision? 0 Yes 0 NoHave you ever had a stroke? 0 Yes 0 No
More on next page
· .
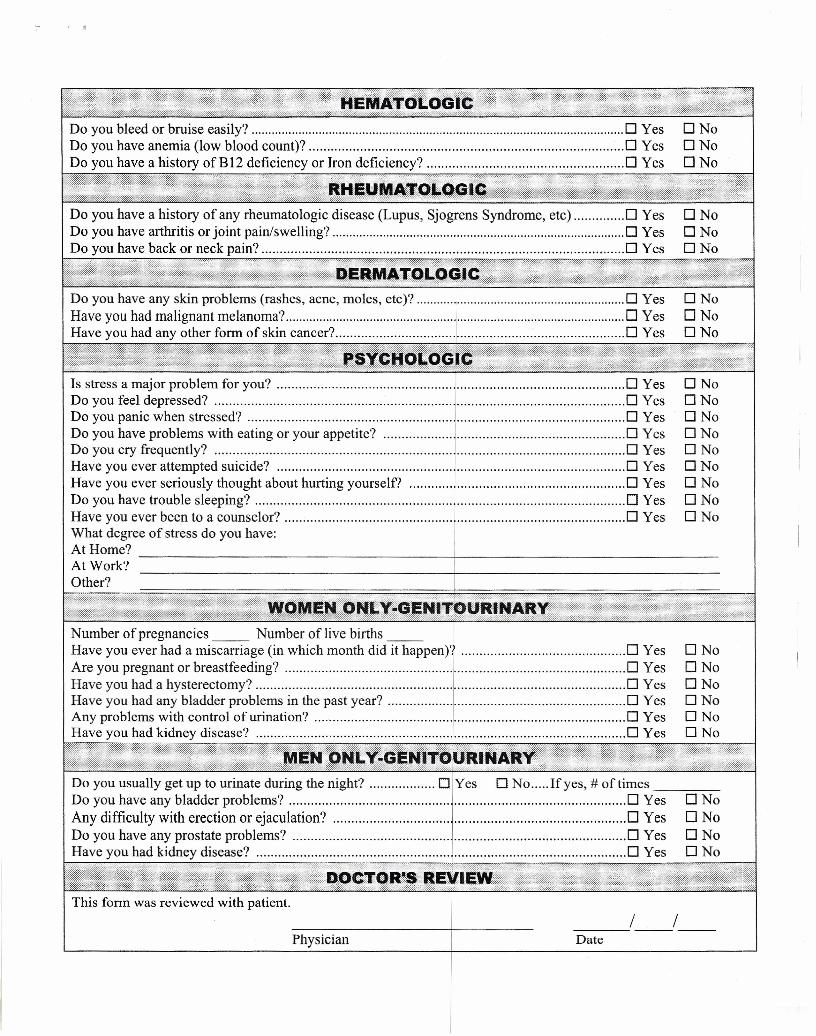
Is stress a major problem for you? ..1. 0 YesDo you feel depressed? 0 YesDo you panic when stressed? 0 YesDo you have problems with eating or your appetite? 0 YesDo you cry frequently? 0 YesHave you ever attempted suicide? 1 0 YesHave you ever seriously thought about hurting yourself? ']" 0 YesDo you have trouble sleeping? 0 YesHave you ever been to a counselor? ..1. 0 YesWhat degree of stress do you have: IAt Home? IAt Work? IW~ I
............" ·.w.·.·.·.····
Number of pregnancies __ Number of live births __Have you ever had a miscarriage (in which month did it happen)? 0 YesAre you pregnant or breastfeeding? 0 YesHave you had a hysterectomy? 0 YesHave you had any bladder problems in the past year? 0 YesAny problems with control of urination? 0 YesHave you had kidney disease? 0 Yes
ONoONoONoONoONoONoONoONoONo
ONoONoONoONoONoONo
Do you usually get up to urinate during the night? 0 Yes 0 No Ifyes, # of times _--,=-_Do you have any bladder problems? 0 Yes 0 NoAny difficulty with erection or ejaculation? .0 Yes 0 NoDo you have any prostate problems? 0 Yes 0 NoHave you had kidney disease? 0 Yes 0 No
Physician Date___ .1__ 1_-
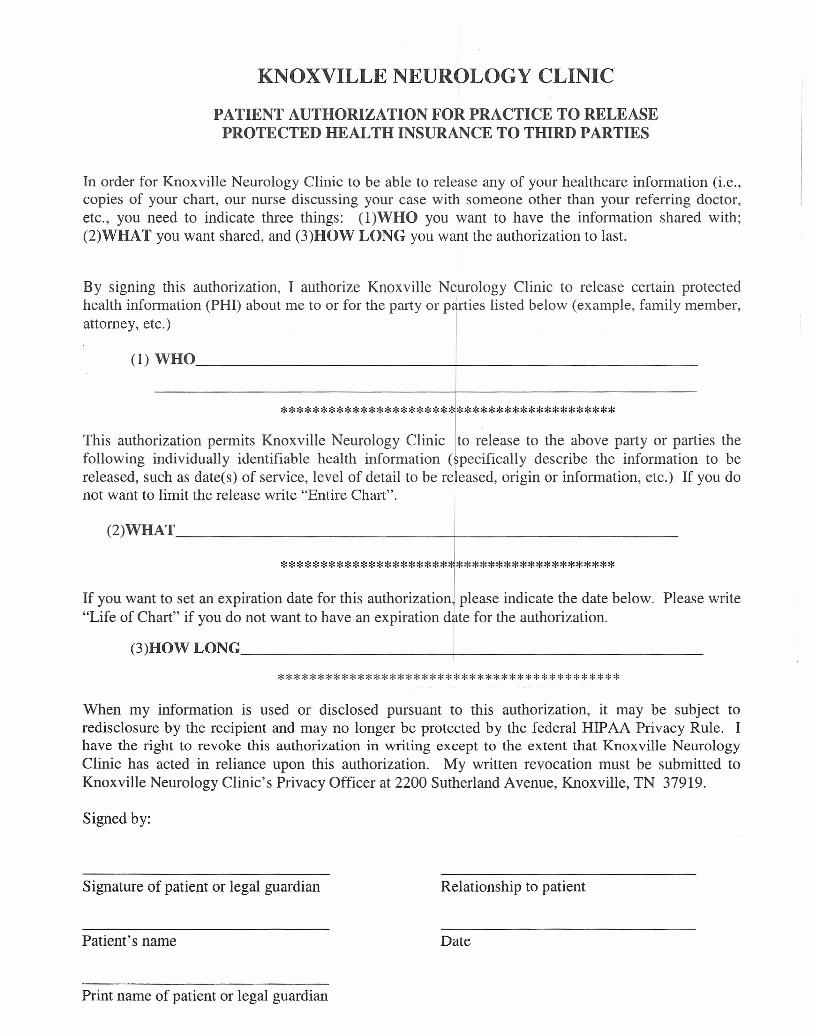
KNOXVILLE NEUROLOGY CLINIC
PATIENT AUTHORIZATION FOR PRACTICE TO RELEASEPROTECTED HEALTH INSURANCE TO THIRD PARTIES
In order for Knoxville Neurology Clinic to be able to release any of your healthcare information (i.e.,copies of your chart, our nurse discussing your case with someone other than your referring doctor,etc., you need to indicate three things: (l)WHO you want to have the information shared with;(2)WHAT you want shared, and (3)HOW LONG you want the authorization to last.
By signing this authorization, I authorize Knoxville Neurology Clinic to release certain protectedhealth information (PHI) about me to or for the party or parties listed below (example, family member,attorney, etc.)
(1)WHO ~----------------------
******************************************This authorization permits Knoxville Neurology Clinic to release to the above party or parties thefollowing individually identifiable health information (specifically describe the information to be
Ireleased, such as date(s) of service, level of detail to be released, origin or information, etc.) If you donot want to limit the release write "Entire Chart".
(2)WHAT -+-- _
*********************J********************
If you want to set an expiration date for this authorization I please indicate the date below."Life of Chart" if you do not want to have an expiration date for the authorization.
(3)HOW LONG 1 _
Please write
*******************************************When my information is used or disclosed pursuant to this authorization, it may be subject toredisclosure by the recipient and may no longer be protected by the federal HIPAA Privacy Rule. Ihave the right to revoke this authorization in writing except to the extent that Knoxville NeurologyClinic has acted in reliance upon this authorization. My written revocation must be submitted toKnoxville Neurology Clinic's Privacy Officer at 2200 Sutherland Avenue, Knoxville, TN 37919.
Signed by:
Signature of patient or legal guardian Relationship to patient
Patient's name Date
Print name of patient or legal guardian
KNOXVILLE NEUROLOGY CLINIC
Patient Consent for Use and Disclosureof Protected Health Information
With my consent, Knoxville Neurology Clinic may use and disclose protected health information(PHI) about me to carry out treatment, payment, and healthcare operations (TPO). Please refer toKnoxville Neurology Clinic's Notice of Privacy Practices for a more complete description of suchuses and disclosures.
I have the right to review the Notice of Privacy Practices prior to signing this consent. KnoxvilleNeurology Clinic reserves the right to revise its Notice of Privacy Practices at anytime. A revisedNotice of Privacy Practices may be obtained by forwarding a written request to KnoxvilleNeurology Clinic Privacy Officer at 2200 Sutherland Avenue, Knoxville, Tennessee 37919.
With my consent, Knoxville Neurology Clinic may call my home or other designated location andleave a message on voice mail or in person in reference to any items that assist the practice incarrying out TPO, such as appointment reminders, insurance items and any call pertaining to myclinical care, including laboratory results among others.
With my consent, Knoxville Neurology Clinic may mail to my home or other designated locationany items that assist the practice in carrying out TPO, such as appointment reminder cards andpatient statements.
I have the right to request that Knoxville Neurology Clinic restrict how it uses or discloses by PHIto carry out TPO. However, the practice is not required to agree to my requested restrictions, but ifit does, it is bound by this agreement.
By signing this form, I am consenting to Knoxville Neurology Clinic's use and disclosure of myPHI to carry out TPO.
I may revoke my consent in wntmg except to the extent that the practice has already madedisclosures in reliance upon my prior consent. If I do not sign this consent, Knoxville NeurologyClinic may decline to provide treatment to me.
Signature of Patient or Legal Guardian
Patient's Name Date
Print Name of Patient or Legal Guardian