radioactivity -...
TRANSCRIPT

RADIOACTIVITY OVERTHE SPLEENANDLIVER FOLLOWINGTHE TRANSFUSIONOF CHROMIUM51-LABELLEDERYTH-
ROCYTESIN HEMOLYTICANEMIA'
By LEE L. SCHLOESSER,2DONALDR. KORST,s DALLAS V. CLATANOFF,2 ANDROBERTF. SCHILLING
(From the Department of Medicine, University of Wisconsin Medical School, Madison, Wisc.)
(Submitted for publication April 17, 1957; accepted June 24, 1957)
The beneficial effect of splenectomy in heredi-tary spherocytosis is well recognized. Selectiveretention of spherocytes in the spleens of patientswith congenital hemolytic anemia was reported byEmerson, Shen, and Castle in 1946 (1). Sub-sequently, spherocyte "trapping" was demon-strated in spleens removed from patients withoutthis disorder (2, 3). In addition, these abnormalred cells in the spleen have greater osmotic fragil-ity than those in the peripheral blood (1). Hamand Castle first postulated that the spleen increasedthe osmotic fragility of red cells by intravascularstasis in a manner similar to that produced bysterile incubation of blood (47). Recently ithas been suggested that the spleen "conditions"spherocytes for early osmotic hemolysis or in-creases their susceptibility to destruction by themechanical forces of the circulation (8, 9). Al-though exact mechanisms of spherocyte destruc-tion remain obscure, splenectomy in congenitalhemolytic anemia alleviates the hemolytic process.
The role of the spleen in red cell destruction inacquired hemolytic anemia is less thoroughly un-derstood. Splenic hemosiderosis, erythrophago-cytosis, and congestion with red cells suggest theimportance of red cell sequestration by this organin the pathogenesis of many of the acquired hemo-lytic anemias. The first good response to splenec-tomy was reported by Micheli in 1911 (10). Thisoperation has since been performed with unpre-dictable results in diseases having little in com-
1 Supported by research grants from the National In-stitutes of Health; the Office of the Surgeon General,United States Army; and the Graduate School of theUniversity of Wisconsin from funds supplied by the Wis-consin Alumni Research Foundation.
2Trainee, National Cancer Institute, during part ofthis study.
3 Present address: Department of Medicine, Universityof Michigan and Veterans Administration Hospital, AnnArbor.
mon other than hemolytic anemia. Criteria forpredicting a favorable result from splenectomy inacquired, or autoimmune, hemolytic anemia havenot been provided by conventional laboratory aids.
Determination of relative organ distribution ofradioactive erythrocytes is feasible by externalscintillation counting (11). Jandl, Greenberg,Yonemoto, and Castle have reported a method fordetermining organ sites of red cell sequestrationusing Cr5l-labelled erythrocytes (12, 13). Theyreported splenectomy was beneficial in one pa-tient who had splenic accumulation of labelled redcells.
A method of determining organ localization ofCr51-labelled red cells utilizing the ratio spleen:liver radioactivity as estimated by external scintil-lation counting was reported from this laboratoryin 1955 (14). It was assumed that a high splenicuptake of radioactivity concomitant with an in-creased rate of Crp5 red cell disappearance from theperipheral blood was evidence for abnormal redcell accumulation in the spleen. The present re-port of red cell survivals and organ counting datawas derived from 27 labelled red cell infusions.Splenic uptake of radioactivity in hemolytic ane-mia was correlated with response to splenectomy.
MATERIALS AND METHODS
Conventional laboratory data
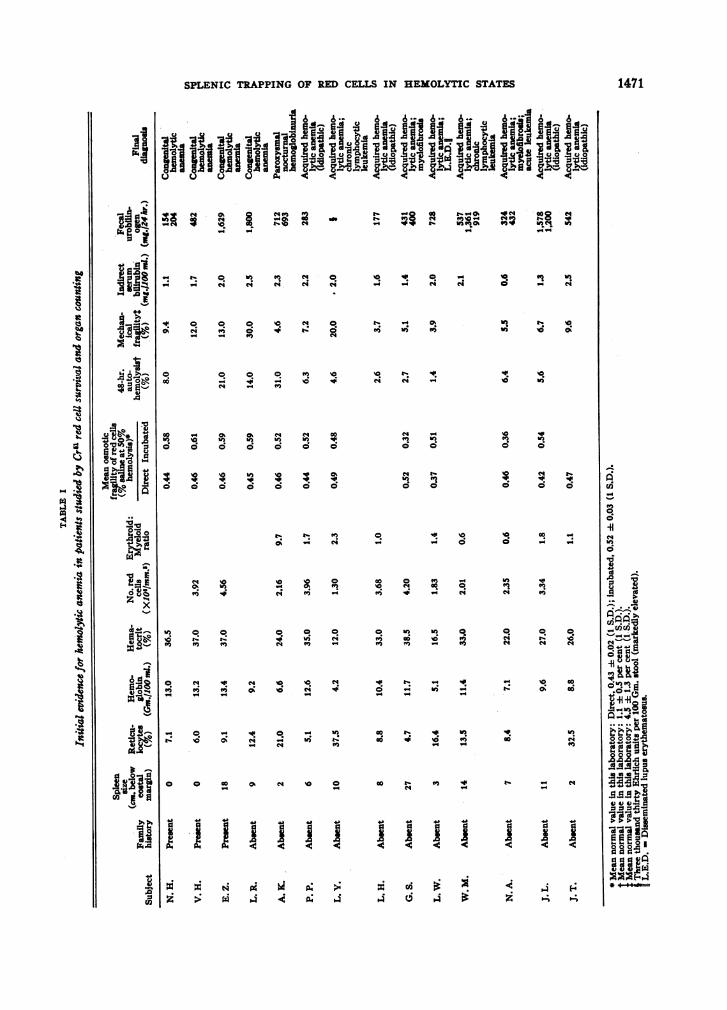
In patients suspected of hemolytic anemia, determina-tions of hemoglobin, reticulocytes, hematocrit, red bloodcell count, red cell fragilities (15), and serum bilirubin(16, 17) were performed by established techniques. Themethod of Dacie was used for the determination of auto-hemolysis of red cells (18). Erythroid: myeloid ratioswere computed after counting 1,000 nucleated cells in thebone marrow smear. Average fecal urobilinogen in afour-day stool collection was determined by the methodof Watson (19), using a Coleman junior colorimeter. Onestool urobilinogen determination was semiquantitative(20). When these data showed evidence for hemolytic
1470
SPLENIC TRAPPING OF RED CELLS IN HEMOLYTIC STATES
~~~~~~~~~~1 luo lo "e2 IN_o0b
KoX W 8 bS " _ b B (4 _ ,7_44 t-5
4 ( C; 4
C
0) eq~~~~0
o to. o4o o0
Wi ) in )b o;_; C; c
o. oW e s_Itoc; _ c;
N '00%,
0 0
r r4
t'.4
0 a0
10N
'R~
0.0
WI.
Iq It C!
o o40 0
0 0
O.
0,
4;
0.
0
0,
Go0
45
*0 .
. 4
'4 -45
I
,uF0 I0
A .
(0 0
o
3 N
'0.
0
O.
N
t4
0
Go
L-
0
0s0,
NR
'0.
wo
O.
0
0.'0
°̂.~~~~~~̂O. ~~~~~ w 0. tv ^ va >Le~~~~~~~~45N 0a 0 '0 0
45 N404A4 45
C4 i 2!3 > PAz~ ~i X X X o;3
1471
I
it
41
3
I
1*w
.1
k*.
ob
ialf
.0
WZX
W.0!
031
XS
U)e
0O0
0
dao
0
3
0,
0
Pi
O"
N
.0;4 4
41
045
4114..
-
* -4.
I
11
I
I
II
I

L. L. SCHLOESSER, D. R. KOIST, D. V. CLATANOFF, AND R. F. SCHILLING
anemia, Cr" red cell survival studies with organ countingwere performed.
Technique of Cr" red cell survival studies
A. Labelling and administration of erythrocytes. Steriletechnique was used throughout. Seventy-five to 90 ml.of venous blood were collected by gravity flow into a
100-ml. siliconized bottle containing 10 ml. acid-citrate-dextrose4 solution. Seventy-five to 100 microcuries Cr"(specific activity range, 0.7 to 26.0 mc. per mg.) as so-
dium chromate diluted in 0.85 per cent NaCl were addedat once. The mixture was incubated at 37°C. for 45minutes with frequent gentle agitation. Following in-cubation, 200 mg. ascorbic acid were added to prevent
4Abbott Laboratories, North Chicago, Illinois. TheACDsolution had the following composition per 100 ml.:Dextrose, USP 132 mg.; sodium citrate, USP 250 mg.;citric acid, USP80 mg.
further uptake of Cr" by red cells (21). A single wash-ing procedure, using cold sterile saline, was done as fol-lows: The mixture was centrifuged and the supernatantplasma was removed. The red cells were washed once
with saline and finally diluted with saline to a volume ap-proximating that of the whole blood withdrawn. Theseinfusions were designated "washed." The washing pro-
cedure removed Cr" which was not bound to erythro-cytes so that more than 97 per cent of Cr" infused was
red-cell bound. In some instances the blood was notwashed and such infusions were designated "non-washed."Cr"-labelled red cells were given intravenously throughan 18-gauge needle by gravity drip from the collectingbottle or in 50-ml. volumes by calibrated syringe.
B. Determination of Cr" red cell surival. Al samplesof peripheral blood were collected in balanced oxalate
(15) in approximately 6-ml. quantities. Packed cellvolumes were determined. Exactly 4 ml. were pipettedinto counting tubes calibrated at 4 ml. Plasma was re-
LE II
Donors and recipients of Cru-kabelled red ceUs
Recipient of Cra red cellsSpleen
size Cr" AverageDonor of Cru red cells (cm. below red-celi ratio
Study costal half-life spleen Cry:No. Subject Diagnosis Subject Diags margin) (days) liver Cra
1 D. D. Normal D. D. Normal 0 34 1.62 D. D. Normal J. H. Normal 0 38 1.83 T. M. Normal T. M. Normal 0 42 1.14 M. M. Normal M. M. Normal 0 30 1.35 D. H. Normal D. H. Normal 0 32 0.9
6 D. H. Normal L. R. Congenital 9 30 1.9hemolyticanemia
7 J.K. Polycythemia J.K. Polycythemia 8 27 2.88 L.K. Myelofibrosis L.K. Myelofibrosis 17 27 1.8
9 L. R. Congenital D. H. Normal 0 6 3.4hemolyticanemia
10 L. R. Congenital L. R. Congenital 9 10 3.4-hemolytic hemolyticanemia anemia
11 Normal E. Z. Congenital 18 22 2.4hemolyticanemi
12 E. Z. Congenital E. Z. Congenital 18 11 3.3hemolytic hemolyticanemia anemia
13 V. H. Congenital V. H. Congenital 0 11 1.4hemolytic hemolyticanemia anemia
14 V. H. Congenital V. H. Congenital 0 29 (post-hemolytic hemolytic splenec-anemia anemia tomy)
15 N. H. Congenital N. H. Congenital 0 17 2.4hemolytic hemolyticanemia anemia
1472
SPLENIC TRAPPING OF RED CELLS IN HEMOLYTIC STATES
TABLE I-Continued
Recipient of Cru red cellsSpleen
size Cra AxerDonor of Cru red cells (cm. below red-cell ratioStudy costal half-life spleen Cru:
No. Subject Di s Subject Diagnosis margin) (days) liver Cr"
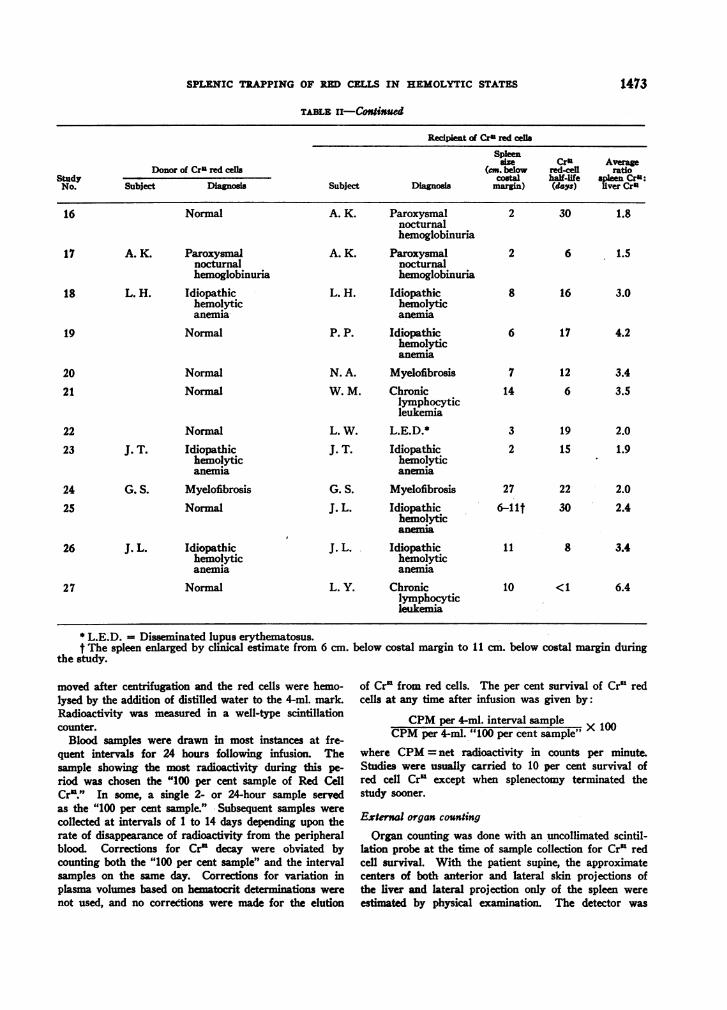
16 Normal A. K. Paroxysmal 2 30 1.8nocturnalhemoglobinuria
17 A. K. Paroxysmal A. K. Paroxysmal 2 6 1.5nocturnal nocturnalhemoglobinuria hemoglobinuria
18 L. H. Idiopathic L. H. Idiopathic 8 16 3.0hemolytic hemolyticanemia anemia
19 Normal P. P. Idiopathic 6 17 4.2hemolyticanemia
20 Normal N. A. Myelofibrosis 7 12 3.4
21 Normal W. M. Chronic 14 6 3.5lymphocyticleukemia
22 Normal L. W. L.E.D.* 3 19 2.0
23 J. T. Idiopathic J. T. Idiopathic 2 15 1.9hemolytic hemolyticanemia anemia
24 G. S. Myelofibrosis G. S. Myelofibrosis 27 22 2.0
25 Normal J. L. Idiopathic 6-lit 30 2.4hemolyticanemia
26 J. L. Idiopathic J. L. Idiopathic 11 8 3.4hemolytic hemolyticanemia anemia
27 Normal L. Y. Chronic 10 <1 6.4lymphocyticleukemia
* L.E.D. = Disseminated lupus erythematosus.t The spleen enlarged by clinical estimate from 6 cm. below costal margin to 11 cm. below costal margin during
the study.
moved after centrifugation and the red cells were hemo-lysed by the addition of distilled water to the 4-ml. mark.Radioactivity was measured in a well-type scintillationcounter.
Blood samples were drawn in most instances at fre-quent intervals for 24 hours following infusion. Thesample showing the most radioactivity during this pe-riod was chosen the "100 per cent sample of Red CellCr"." In some, a single 2- or 24-hour sample servedas the "100 per cent sample." -Subsequent samples werecollected at intervals of 1 to 14 days depending upon therate of disappearance of radioactivity from the peripheralblood. Corrections for Cr" decay were obviated bycounting both the "100 per cent sample" and the intervalsamples on the same day. Corrections for variation inplasma volumes based on heiatocrit detminations were
not used, and no corrections were made for the elution
of Cr" from red cells. The per cent survival of Cr" redcells at any time after infusion was given by:
CPMper 4-ml. interval sampleCPMper 4-ml. "100 per cent sample" X 1
where CPM= net radioactivity in counts per minute.Studies were usually carried to 10 per cent survival ofred cell Cr" except when splenectomy terminated thestudy sooner.
External organ counting
Organ counting was done with an uncollimated scintil-lation probe at the time of sample collection for Cr" redcell survival. With the patient supine, the approximatecenters of both anterior and lateral skdn projections ofthe liver and lateral projection only of the spleen wereestimated by physical eamnation. The detector was
1473

L. L. SCHLOESSER, D. R. KORST, D. V. CLATANOFF, AND R. F. SCHILLING
placed on the skin at these sites so the face of the crystalwas approximately parallel to the body surface. Whenmultiple determinations of radioactivity were made froma single organ at the same time, the results were aver-aged. A minimum of 5,000 counts over each organ sitewas obtained. Radioactivity values over either organless than 1.5 times background were not used. The ra-tio net spleen counts: net liver counts was determined.
Selection of subjects for Cr' studies
Twenty-one subjects were studied by Cr'-labelled redcell survival and organ counting techniques. Five werehealthy young men without splenomegaly. Studies weremade on two patients who had splenomegaly withouthemolytic anemia. Radioactivity studies were made in14 patients who had classical evidence of hemolytic anemia.
With the exception of Patient N. A., all subjects withacquired hemolytic anemia were given adrenal steroidsprior to splenectomy without significant benefit. Wehave hesitated to advise splenectomy for acquired hemo-lytic anemia when the process was controlled by steroids.
RESULTS
Initial data on patients with hemolytic anemia
Pertinent clinical features and laboratory dataon the 14 patients showing evidence for hemolyticanemia are presented in Table I. The final diag-nosis for each subject is entered in Table I forcompletion, but was not made in all patients priorto labelled erythrocyte studies. All subjects butN. H. and L. H. had increased (> 280 mg. per
day) fecal urobilinogen. The osmotic fragility ofred cells after incubation was abnormally increasedin patients with hereditary spherocytosis. In-creases in mean fragility upon incubation were notseen consistently in patients with acquired hemo-lytic anemia. Autohemolysis after 48 hours ofsterile incubation was strikingly increased in he-reditary spherocytosis and in the one subject(A. K.) with paroxysmal nocturnal hemoglobi-nuria. In acquired hemolytic anemia the degreeof autohemolysis varied within wide limits fromnormal to abnormal. Mechanical fragility wasregularly increased only in the hereditary sphero-cytosis group.
Cr5l red cell survival and organ counting
There were 26 simultaneous determinations ofCr5l red cell survival and spleen Cr51: liver Cr5'ratios in the 21 subjects. Five of these subjectsreceived labelled red cells from a suitable donor(homologous), and at another time an infusion oftheir own labelled red cells (autologous). An ad-ditional survival study was done in one subject(V. H.) after splenectomy. Pertinent data ondonor red cells and recipients are shown in TableII.
In Figures 1 to 9 data on Cr5' red cell survivaland organ counting for each recipient are plotted
Cr5 LABELLED (WASHEDAUTOLOGOUSNORMALRED CELLS
50 % SURVIVAL' 42 DAYS aa
zj
SPLEEN' NOT PALPABLEAVERAGERATIO SrENOr"' 1-1
- S t
51'2 '4& ' 36 ' 4:8 ' 10' 7'2 '
DAYS
RECIPIENT T. M. NORMAL
100
80
60
40
20i
6-
08 5.
i 4.| 34a -3 3.
r-2 2
a I
Cr5G LABELLED (WASHED)AUTOLOGOUSNORMALRED CELLS
50 % SURVIVAL 30 DAYS
SPLEEN' NOT PALPABLE
AVERAGE RATIO SLVER Cr5 ' 1*5
'2 24' 36 4*8 6'0DAYS
RECIPIENT M. M. NORMAL
72
FIG. 1. NoRMALRDCULLs INFUSED rNTo NORMALRECIPIENTSRecipients T. M. and M. M. (Studies No. 3 and 4-Table II).
100
0
j 80
o 60cca-z3 400
X 20
a8 h 6-
3.0P 2.9I I
1474
L.
SPLENIC TRAPPINOG OF RMCELLS IN HEMOLYTIC STATES
Cr LABELHOMOLOGOIJ
(FRO50% SUR
._._._._*_
:ED (WASHED)JS SPHEROCYTESHI L R.)VVAL' 6 DAYS
I100~loo.a
ao
Aus
2C 60-
4-~0
1 _2o
AVERAGE RATIO WWO a' 3.4 t a 6SPLEEN' NOT PALPOGLE 5
: I122436 48~~~~~Oa72
12' 24 36 48 60 72DAYS
RECIPIENT 0. H.
elm LABELLED (NON-WASHED)AUTOLOGOUSNORMALRED CELLS
50% SURVIVAL, 32 DAYS
SPLEEN' NOT PALPABLESPLEEN
o
AVERAGE RATIO LIVER W0r .
_ _* 12 ' & ' S ' 48 ' 60
4'DLAYS
NORMAL
I
8~~~~~Oro LAELA.ED (WASNECO ~8AUTaLOGOU5 rPNEROCYTESI i50% SURVIVALs 10 DAYS aaTo
II-
. 6.
G. J 3.
° 2.ml I'-
SPLEEN' 9en BELOWCOSTaALMARGIN
AVERAGERATIO SPL'EEN%-$I 3.4LIVER Cr
12 24 36 48 6072DAYS
RECIPIENT L. R.
100
80
60
40
20
Crc LABELLED (NON-WASHEWNOlOOKL0US NORMALRED CELLS
(FROM D. N)50% SURVIVAL' 30 DAYS
SPLEEN S9 a BELOWCOSTAL MARGIN
AVERAG RATIO SPLEENC ,s
- 0
2 24 '376W '
DAYS
CONGENITAL HEMOLYTIC ANEMIA
60 72
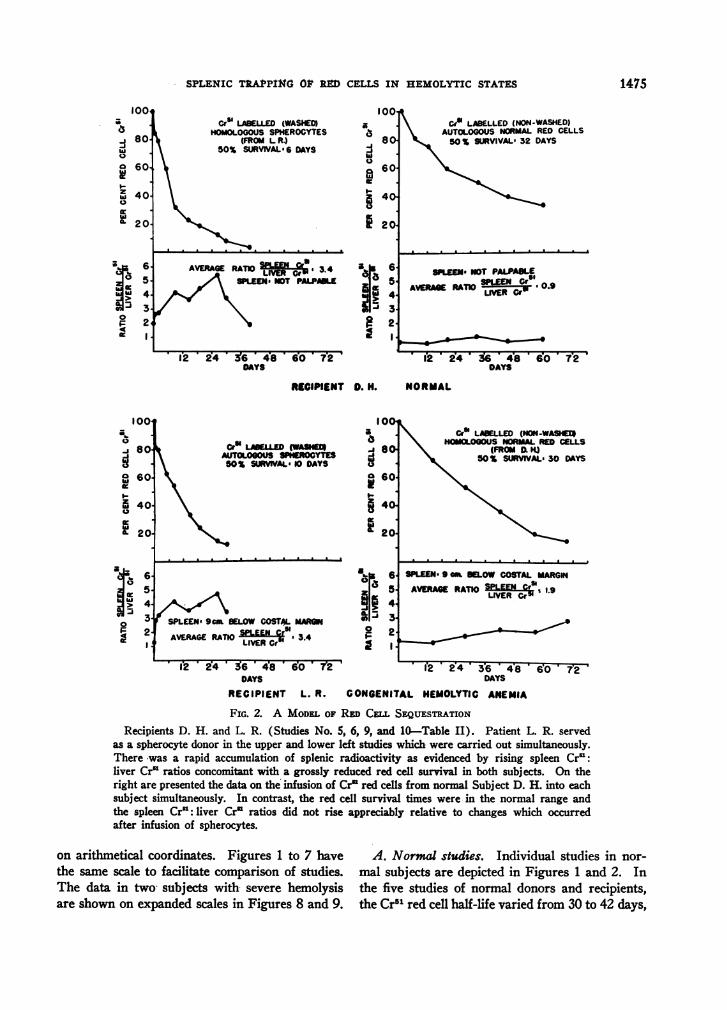
FIG. 2. A MODELOF RED CELL SEQUESTRATIONRecipients D. H. and L. R. (Studies No. 5, 6, 9, and 10-Table II). Patient L. R. served
as a spherocyte donor in the upper and lower left studies which were carried out simultaneously.There was a rapid accumulation of splenic radioactivity as evidenced by rising spleen Cr':liver Cr' ratios concomitant with a grossly reduced red cell survival in both subjects. On theright are presented the data on the' infusion of Cr' red cells from normal Subject D. H. into eachsubject simultaneously. In contrast, the red cell survival times were in the normal range andthe spleen Cr': liver Cr' ratios did not rise appreciably relative to changes which occurredafter infusion of spherocytes.
on arithmetical coordinates. Figures 1 to 7 have A. Normal studies. Individual studies in nor-the same scale to facilitate comparison of studies. mal subjects are depicted in Figures 1 and 2. InThe data in two subjects with severe hemolysis the five studies of normal donors and recipients,are shown on expanded scales in Figres 8 and 9. the Cr51 red cell half-life varied from 30 to 42 days,
1475
1004
-I 80-a
0 7o 60-t-
zw 40.40a- 20-
*C6
0
3.F 24a1 I
72
loot
0
808hi
Da 60-e
5f 40-40
A 20.
i,4-
F 2-II
1-0
L. L. SCHLORSSER, D. R. KORST, D. V. CLATANOFF, AND R. P. SCHILLING
Cr' LABELLED (WASHEDHOMOLOGOUSNORMALRED CELLS
50SUOWAs22DAYS
SPLEEN 18 cm BELOWCOSTAL MARGIN
AVERAGE RATIO C 2.4
10I
0
.j 80a
8 60
I-
40
it 20
a0
hih
0
4c
Ea:
65432
12 24 36 48 * 60 * 72DAYS
CrO LABELLED (WASHED)AUTOLOGOUSSPHEROCYTES50 % SURVIVAL: II DAYS
SPLEEN- 18 cm BELOW COSTAL MARGIN
AVERAGE RATIO LVEEN Gr 3,3
?Y%~~~IVRC
12 2w4 * 36 * 478DAYS
RECIPIENT E. Z.CONGENITAL HEMOLYTIC ANEMIA
60 72
6-
5,
4.
3'i
2.
I.1
Ce1 LABELLED (NON -WASHED)AUTOLOGOUSSPHEROCYTES50 % SURVIVAL. II DAYS
100'1a-i 80-
0
X 60
L 40
a- 20
SPLEENANOT PALPABLE as6-
SPLEENSCap 14 5aAVERAGE RATIO ru- I5.Joi 4-
&. J 3.ai~
* 1'2 '4 3'6 ' 48 ' d0 ' 7'2'
DAYS
\Cr' LABELLED (NON -WASHED)AUTOLOGOUSSPHEROCYTES50% SURVIVAL, 29 DAYS
POST- SPLENECTOMY
12 36 48DAYS
60 T2
RECiENT V.H
CONGENITAL HEMOLYTIC ANEMIA
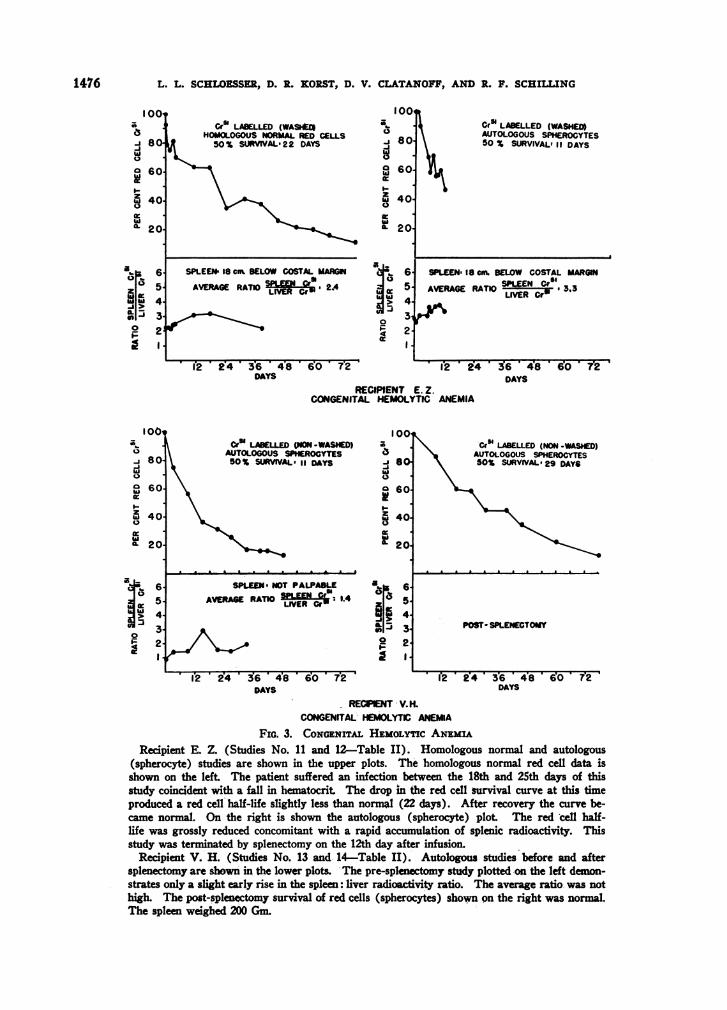
FIG. 3. CONGENITALHEMOLYCANinuRecipient E. Z. (Studies No. 11 and 12-Table II). Homologous normal and autologous
(spherocyte) studies are shown in the upper plots. The homologous normal red cell data isshown on the left. The patient suffered an infection between the 18th and 25th days of thisstudy coincident with a fall in hematocrit. The drop in the red cell survival curve at this timeproduced a red cell half-life slightly less than normal (22 days). After recovery the curve be-came normal. On the right is shown the autologous (spherocyte) plot. The red cell half-life was grossly reduced concomitant with a rapid accumulation of splenic radioactivity. Thisstudy was terminated by splenectomy on the 12th day after infusion.
Recipient V. H. (Studies No. 13 and- 14-Table II). Autologous studies before and aftersplenectomy are shown in the lower plots. The pre-splenectomy study plotted on the left demon-strates only a slight early rise in the spleen: liver radioactivity ratio. The average ratio was nothigh. The post-splenectomy survival of red cells (spherocytes) shown on the right was normal.The spleen weighed 200 Gm.
1476
00,
8o
601-Jw0
I-z0
i*
w
I-
a :12or.
10z
-10,-_>0
40.
20
65,4,3.2.I,1
100a0-J 80hi0
O 60I-3 400
0.20-
ahi h
0IF4
)I
I
1.
0
k
SPLENIC TRAPPING OF RED CELLS IN HEMOLYTIC STATES
and average spleen: liver radioactivity ratios from0.9 to 1.8 (Table II-Studies 1 to 5).
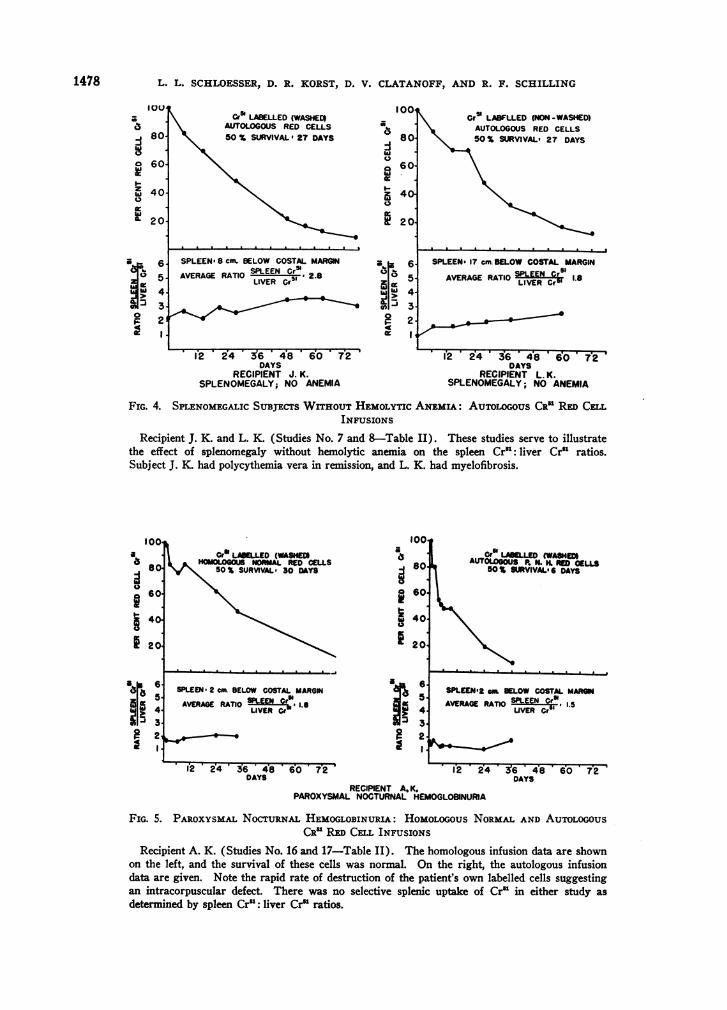
B. Splenomegaly without hemolytic anemia.These studies are illustrated in Figure 4. In re-cipient J. K. (polycythemia vera in remission), theCrl red cell half-life was 27 days, and the averagespleen: liver radioactivity ratio was 2.8. PatientL. K. had myelofibrosis without anemia. TheCrl1 red cell half-life was 27 days, and the averagespleen: liver radioactivity ratio was 1.8. A veryslight increase in ratios occurred concomitantwith the disappearance of labelled red cells fromthe peripheral blood in both of these subjects.
C. Congenital hemolytic anemia. For the ob-servations shown in Figure 2, Subjects L. R.(congenital hemolytic anemia) and D. H. (nor-mal) served a dual role, i.e., as autologous andreciprocal homologous recipients of Cr"l red cells(Table II-Studies 5, 6, 9, 10). Labelled sphero-cytes infused into a normal person or back intothe donor were rapidly eliminated from the periph-eral circulation, and the spleen Crl1: liver Crl ra-tios increased to abnormally high levels. In con-trast were the normal survival of normal red cellsin the same subjects.
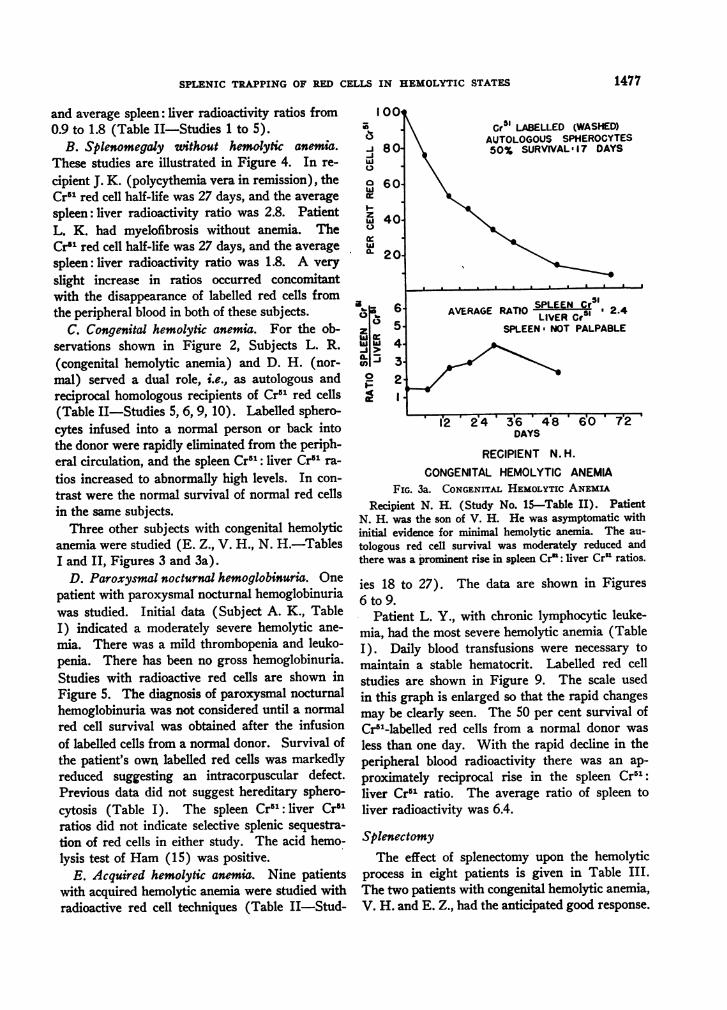
Three other subjects with congenital hemolyticanemia were studied (E. Z., V. H., N. H.-TablesI and II, Figures 3 and 3a).
D. Paroxysmal nocturnal hemoglobinuria. Onepatient with paroxysmal nocturnal hemoglobinuriawas studied. Initial data (Subject A. K., TableI) indicated a moderately severe hemolytic ane-mia. There was a mild thrombopenia and leuko-penia. There has been no gross hemoglobinuria.Studies with radioactive red cells are shown inFigure 5. The diagnosis of paroxysmal nocturnalhemoglobinuria was not considered until a normalred cell survival was obtained after the infusionof labelled cells from a normal donor. Survival ofthe patient's own labelled red cells was markedlyreduced suggesting an intracorpuscular defect.Previous data did not suggest hereditary sphero-cytosis (Table I). The spleen Cr'l: liver Cr'1ratios did not indicate selective splenic sequestra-tion of red cells in either study. The acid hemo-lysis test of Ham (15) was positive.
E. Acquired hemolytic anemia. Nine patientswith acquired hemolytic anemia were studied withradioactive red cell techniques (Table II-Stud-
100OroU
-80-J0
O 60.wI-
z 40.
0C nru'U.
a
or0Z C
A >z hiwI
0I-91
6'5,14'i3.
2
'Cr51 LABELLED (WASHED)AUTOLOGOUSSPHEROCY150% SURVIVALa17 DAY'
TESIs
AVERAGE RATIO SPLEEN Cr 51AVERAGERATIO LIVER Cr5' ' 2.4
SPLEEN: NOT PALPABLE
I2 ' 2'4D'3 S6' 4'8DAYS
6'0 7@2
RECIPIENT N. H.
CONGENITAL HEMOLYTIC ANEMIAFIG. 3a. CONGENITALHEMOLYTICANEMIA
Recipient N. H. (Study No. 15-Table II). PatientN. H. was the son of V. H. He was asymptomatic withinitial evidence for minimal hemolytic anemia. The au-tologous red cell survival was moderately reduced andthere was a prominent rise in spleen Cr": liver Cr" ratios.
ies 18 to 27). The data are shown in Figures6 to 9.
Patient L. Y., with chronic lymphocytic leuke-mia, had the most severe hemolytic anemia (TableI). Daily blood transfusions were necessary tomaintain a stable hematocrit. Labelled red cellstudies are shown in Figure 9. The scale usedin this graph is enlarged so that the rapid changesmay be clearly seen. The 50 per cent survival ofCrl-labelled red cells from a normal donor wasless than one day. With the rapid decline in theperipheral blood radioactivity there was an ap-proximately reciprocal rise in the spleen Cr1:liver Cr"5 ratio. The average ratio of spleen toliver radioactivity was 6.4.
SplenectomyThe effect of splenectomy upon the hemolytic
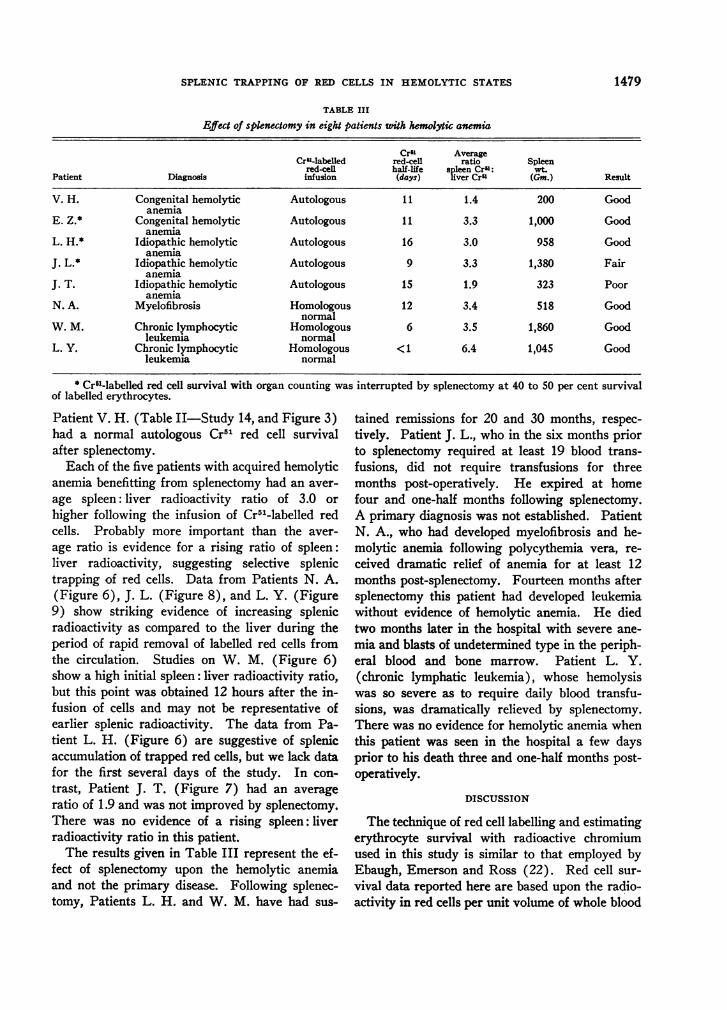
process in eight patients is given in Table III.The two patients with congenital hemolytic anemia,V. H. and E. Z., had the anticipated good response.
1477
L. L. SCHLOESSER, D. R. KORST, D. V. CLATANOFF, AND R. F. SCHILLING
100Cr5' LABELLED (WASHED)
AUTOLOGOUSRED CELLS50 % SURVIVAL: 27 DAYS
0.0
I..
0
SPLEEN8 cm BELOW COSTAL MARGINSPLEEN Cr St
AVERAGE RATIO 7*gEE ' 2.8LIVER Cr
80-
60O
40-
20.
a' 65-1Ia:z
w 4-iI. 3.F 24a I i
12 24 .6 48 60 72DAYS
RECIPIENT J. K.SPLENOMEGALY;NO ANEMIA
Cra LABFLLED (NON -WASHED)AUTOLOGOUSRED CELLS50% SURVIVAL, 27 DAYS
SPLEEN, 17 cm. BELOWCOSTAL MARGIN
AVERAGERATIO SLVEERN Cri 1.8
-~~~~~LVRC5
12 24 ' 36 ' 48 '6 7DAYS
RECIPIENT L. K.SPLENOMEGALY;NO ANEMIA
FIG. 4. SPLENOMEGALICSUBJECTSWITHOUTHEMOLYTICANEMIA: AUToLxoUs CRe RED CELIINFUSIONS
Recipient J. K. and L. K (Studies No. 7 and 8-Table II). These studies serve to illustratethe effect of splenomegaly without hemolytic anemia on the spleen Cr': liver Cr' ratios.Subject J. K. had polycythemia vera in remission, and L. K. had myelofibrosis.
100
q 80:
@ 60.
bi 40.
Cr ,LeI LD (WASHEDIHoMLGOU NORMAL RED CELLS
SO SURVVAL. 30 DAYS
SPLEEN. 2 cat BELOW COSTAL MARGI5
AVERAGE RATIO LER Goin 1.8LIVER Cr
a 6
5432
12 -2-4 S6 48 '0 * 72DAYS
Ael (WASHED)AUTNLA.. NoRED CGLLS501 SURVIVAL6 DAYS
SPLEEN2 an BELOWCOSTAL MARGI
AVERAGERATIO SLEER Go", 1. 5UVER Cr|
12 24 3'6 48DAYS
RECIPIENT A, K.PAROXYSMALNOCTURNALHEMOGLOBINURIA
60 72
FIG. 5. PAROXYSMALNocTURNAL HEMOGLOBINURIA: HOMOLOGOUSNORMALAND AUTOLOGOUSCR' RED CELL INFUSIONS
Recipient A. K. (Studies No. 16 and 17-Table II). The homologous infusion data are shownon the left, and the survival of these cells was normal. On the right, the autologous infusiondata are given. Note the rapid rate of destruction of the patient's own labelled cells suggestingan intracorpuscular defect. There was no selective splenic uptake of Cr' in either study asdetermined by spleen Cr': liver Cr' ratios.
IOUa
80:so-w0o 60
zw 400
ww 20
a 6-524
g 30 21
0: I
aa
100.
so.
60
40
20
a8a 6a
ul 4
1478
& V
SPLENIC TRAPPING OF RED CELLS IN HEMOLYTIC STATES
TABLE III
Efect of splenectomy in eight patients with hemolytic anemia
CrO AverageCru-labelled red-cell ratio Spleen
red-cell half-life spleen CrO: wt.Patient Diagnosis infusion (days) liver Cru (Gm.) Result
V. H. Congenital hemolytic Autologous 11 1.4 200 Goodanemia
E. Z.* Congenital hemolytic Autologous 11 3.3 1,000 Goodanemia
L. H.* Idiopathic hemolytic Autologous 16 3.0 958 Goodanemia
J. L.* Idiopathic hemolytic Autologous 9 3.3 1,380 Fairanemia
J. T. Idiopathic hemolytic Autologous 15 1.9 323 Pooranemia
N. A. Myelofibrosis Homologous 12 3.4 518 Goodnormal
W. M. Chronic lymphocytic Homologous 6 3.5 1,860 Goodleukemia normal
L. Y. Chronic lymphocytic Homologous <1 6.4 1,045 Goodleukemia normal
* Crl-labelled red cell survival with organ counting was interrupted by splenectomy at 40 to 50 per cent survivalof labelled erythrocytes.
Patient V. H. (Table II-Study 14, and Figure 3)had a normal autologous Cr51 red cell survivalafter splenectomy.
Each of the five patients with acquired hemolyticanemia benefitting from splenectomy had an aver-age spleen: liver radioactivity ratio of 3.0 orhigher following the infusion of Cr51-labelled redcells. Probably more important than the aver-age ratio is evidence for a rising ratio of spleen:liver radioactivity, suggesting selective splenictrapping of red cells. Data from Patients N. A.(Figure 6), J. L. (Figure 8), and L. Y. (Figure9) show striking evidence of increasing splenicradioactivity as compared to the liver during theperiod of rapid removal of labelled red cells fromthe circulation. Studies on W. M. (Figure 6)show a high initial spleen: liver radioactivity ratio,but this point was obtained 12 hours after the in-fusion of cells and may not be representative ofearlier splenic radioactivity. The data from Pa-tient L. H. (Figure 6) are suggestive of splenicaccumulation of trapped red cells, but we lack datafor the first several days of the study. In con-trast, Patient J. T. (Figure 7) had an averageratio of 1.9 and was not improved by splenectomy.There was no evidence of a rising spleen: liverradioactivity ratio in this patient.
The results given in Table III represent the ef-fect of splenectomy upon the hemolytic anemiaand not the primary disease. Following splenec-tomy, Patients L. H. and W. M. have had sus-
tained remissions for 20 and 30 months, respec-tively. Patient J. L., who in the six months priorto splenectomy required at least 19 blood trans-fusions, did not require transfusions for threemonths post-operatively. He expired at homefour and one-half months following splenectomy.A primary diagnosis was not established. PatientN. A., who had developed myelofibrosis and he-molytic anemia following polycythemia vera, re-ceived dramatic relief of anemia for at least 12months post-splenectomy. Fourteen months aftersplenectomy this patient had developed leukemiawithout evidence of hemolytic anemia. He diedtwo months later in the hospital with severe ane-mia and blasts of undetermined type in the periph-eral blood and bone marrow. Patient L. Y.(chronic lymphatic leukemia), whose hemolysiswas so severe as to require daily blood transfu-sions, was dramatically relieved by splenectomy.There was no evidence for hemolytic anemia whenthis patient was seen in the hospital a few daysprior to his death three and one-half months post-operatively.
DISCUSSION
The technique of red cell labelling and estimatingerythrocyte survival with radioactive chromiumused in this study is similar to that employed byEbaugh, Emerson and Ross (22). Red cell sur-vival data reported here are based upon the radio-activity in red cells per unit volume of whole blood
1479
L. L. SCHLOESSER, D. R. KORST, D. V. CLATANOFF, AND R. F. SCHILLING
Cro LABELLED (WASHECIAUTO US RED CELLS50% SURVIAL: DAYS
. .L
SPLEENI S L BELOW COSTAL MARGINAVERAGE RATIO -L 3.0UIVER Ct
a
80
60
1 40
1 20
a :2I
12 *4 '6 4T8'6o72_DAYS
RECIPIENT L. H.IDIOPATHIC HEMOLYTIC ANEMIA
Crt LABELLED (WASHED)NORMAL RED CELLS
50% SURVIVAL. 17 DAYS
SPLEEN. A em BELLOW COSTALE AS
AVERAGERATIOLIECrsI WWLIVER Cr'
12 24 36- 48 60 72'?P.DAYS
RECIPIENT P. P.IDIOPATHIC HEMOLYTIC ANEMIA
Cr' LABELLED (NON -WASHEDIHOMOLOGOUS-NORMALRED CELLS
50% SURVIVALI 12 DAYS
100
-I 800ma 60
§ 40
1! 20.
fi a
SPLEENs 7 eL BELOWCOSTAL MARNAVERAGE RATIO PLEEN - 54UVER Cr
. .6 .: .o
6.
5.
4.
112 * 24 * 36 * "CS * CO * 7f2 'DAYS
REPIENT NA.ACQUIRED HEMOLYTIC ANEhUA
CrS LABELLED (*HOMOLOGOUSNORMAL
50 % SURVIVALI
NASHEMRED CELLS
.6 DAYS
SPLEEN. 14 ca BELOW COSTA. mARGIAVERAGE RATIO UVER Cr *T0LIValt Iolk , 30|-5
-an?0 0' =_'---- _It 2-4 36 ' 48 *'DAYS
REGIPMENT W. M.ACQUIRED HEMOLYTIC ANEMA
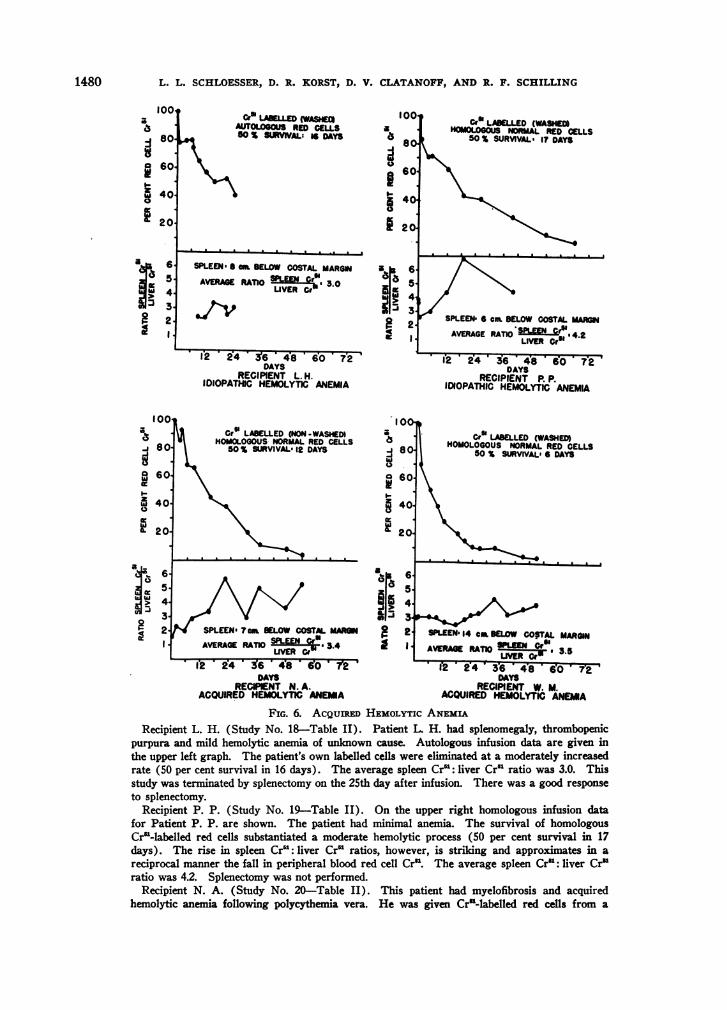
FIG. 6. ACQUIRED HEMOLYTIC ANEMIARecipient L. H. (Study No. 18-Table II). Patient L. H. had splenomegaly, thrombopenic
purpura and mild hemolytic anemia of unknown cause. Autologous infusion data are given inthe upper left graph. The patient's own labelled cells were eliminated at a moderately increasedrate (50 per cent survival in 16 days). The average spleen Cr': liver Cr' ratio was 3.0. Thisstudy was terminated by splenectomy on the 25th day after infusion. There was a good responseto splenectomy.
Recipient P. P. (Study No. 19-Table II). On the upper right homologous infusion datafor Patient P. P. are shown. The patient had minimal anemia. The survival of homologousCr'-labelled red cells substantiated a moderate hemolytic process (50 per cent survival in 17days). The rise in spleen Cr': liver Cr' ratios, however, is striking and approximates in areciprocal manner the fall in peripheral blood red cell Cr'. The average spleen Cr': liver Cr'ratio was 4.2. Splenectomy was not performed.
Recipient N. A. (Study No. 20-Table II). This patient had myelofibrosis and acquiredhemolytic anemia following polycythemia vera. He was given Cr"-labelled red cells from a
1480
100
:1 80-
a 60.
i 40.
20.
a6p
2.
100
-I 80
I-w1 6 0
z. 400
F201
6-5.
4-
3-2-l
i4>>a1
....a . .
SPLENIC TRAPPING OF RED CELLS IN HEMOLYTIC STATES
Cro LABELLED (WASpIEHOMOLOGOUSIORMAL RED CELLS
50 % SURVI' IS DAYS
. . . . . . . . . . . .
SPLEENS3mam LOW COSTAL MARG
AVERAGE RATIO IER Cry 2.0
-I
I-zi
001
s0o
60
40.
20
a a
4.*i 3.
F 22 I
* I> *2t436 -48 60 72DAYS
RECIPIENT L W.ACQUIRED HEMOLYTIC ANEMIA
Cro LABELLED (NON -WASHED)AUTOLOGOUSRED CELLS50 % SURVIVAL: I5 DAYS
SPLEEN' 2 am BELOW COSTAL MARGIN
AVERAE RATIO SPLEEN Or L9AVERGE RTIOLIVER Cra L
*2 * R4 ' 36 * 48 '60e ' 72DAYS
RECIPIENT J. T.IDIOPATHIC HEMOLYTIC ANEMA
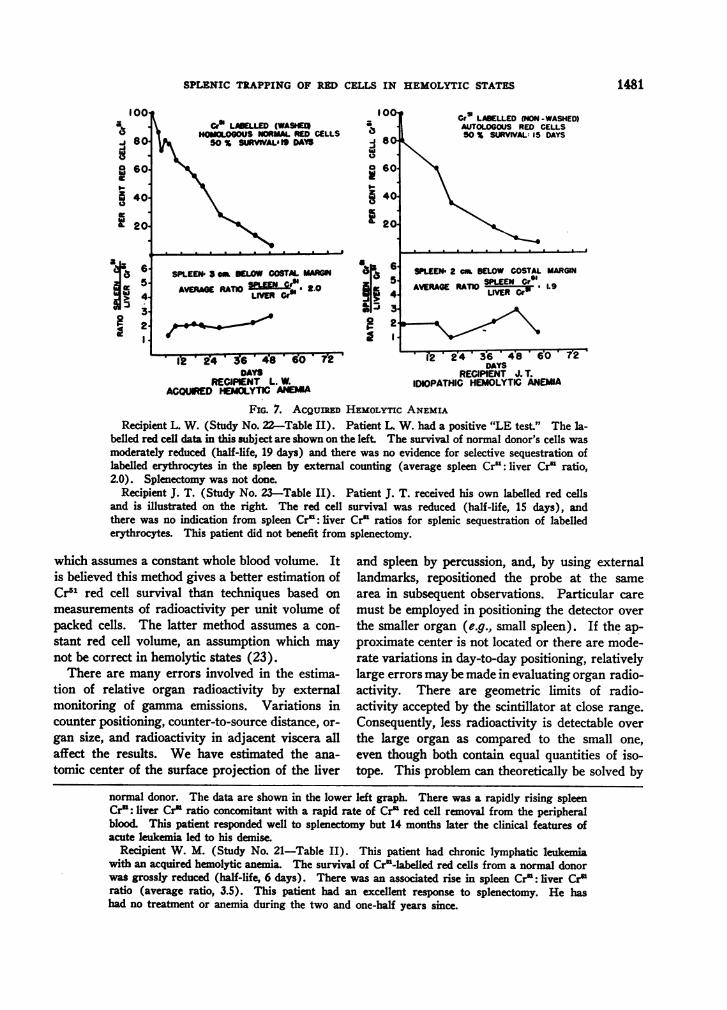
FIG. 7. ACQUIRED HEMOLYTIC ANEMIARecipient L. W. (Study No. 22-Table II). Patient L. W. had a positive "LE test." The la-
belled red cell data in this subject are shown on the left. The survival of normal donor's cells was
moderately reduced (half-life, 19 days) and there was no evidence for selective sequestration oflabelled erythrocytes in the spleen by external counting (average spleen Cr': liver Cr" ratio,2.0). Splenectomy was not done.
Recipient J. T. (Study No. 23-Table II). Patient J. T. received his own labelled red cellsand is illustrated on the right. The red cell survival was reduced (half-life, 15 days), andthere was no indication from spleen Cry: liver Cr" ratios for splenic sequestration of labellederythrocytes. This patient did not benefit from splenectomy.
which assumes a constant whole blood volume. Itis believed this method gives a better estimation ofCr51 red cell survival than techniques based onmeasurements of radioactivity per unit volume ofpacked cells. The latter method assumes a con-
stant red cell volume, an assumption which may
not be correct in hemolytic states (23).There are many errors involved in the estima-
tion of relative organ radioactivity by externalmonitoring of gamma emissions. Variations incounter positioning, counter-to-source distance, or-
gan size, and radioactivity in adjacent viscera allaffect the results. We have estimated the ana-
tomic center of the surface projection of the liver
and spleen by percussion, and, by using externallandmarks, repositioned the probe at the same
area in subsequent observations. Particular care
must be employed in positioning the detector over
the smaller organ (e.g., small spleen). If the ap-
proximate center is not located or there are mode-rate variations in day-to-day positioning, relativelylarge errors maybe made in evaluating organ radio-activity. There are geometric limits of radio-activity accepted by the scintillator at close range.
Consequently, less radioactivity is detectable over
the large organ as compared to the small one,
even though both contain equal quantities of iso-tope. This problem can theoretically be solved by
normal donor. The data are shown in the lower left graph. There was a rapidly rising spleenCry: liver Cr" ratio concomitant with a rapid rate of Cr" red cell removal from the peripheralblood. This patient responded well to splenectomy but 14 months later the clinical features ofacute leukemia led to his demise.
Recipient W. M. (Study No. 21-Table II). This patient had chronic lymphatic leukemia
with an acquired hemolytic anemia. The survival of Cr"-labelled red cells from a normal donorwas grossly reduced (half-life, 6 days). There was an associated rise in spleen Cr": liver Cr"ratio (average ratio, 3.5). This patient had an excellent response to splenectomy. He hashad no treatment or anemia during the two and one-half years since.
100
80-9 60
5 40
L 20
1481
a-I
ii
65432l
L. L. SCELOESSER, D. R. KORST, D. V. CLATANOFI, AND R. P. SCHILLING
increasing the counter to source distance; however,without elaborate shielding apparatus, specificityof organ radioactivity is lost. Organ areas havebeen counted with an unshielded probe touchingthe skin, assuming this procedure would givevalid data.
There is evidence that not all of the Cr5' foundin the spleen after the infusion of labelled red cellsis hemoglobin bound (24). It is considered un-likely, however, that such radioactivity is derivedfrom sources other than Cr5l-labelled red cellsdestroyed in the spleen. Cr5lCl3 (13, 25) andCrl-labelled hemoglobin infusions (13) showinglow flat curves of splenic radioactivity supportthis conjecture.
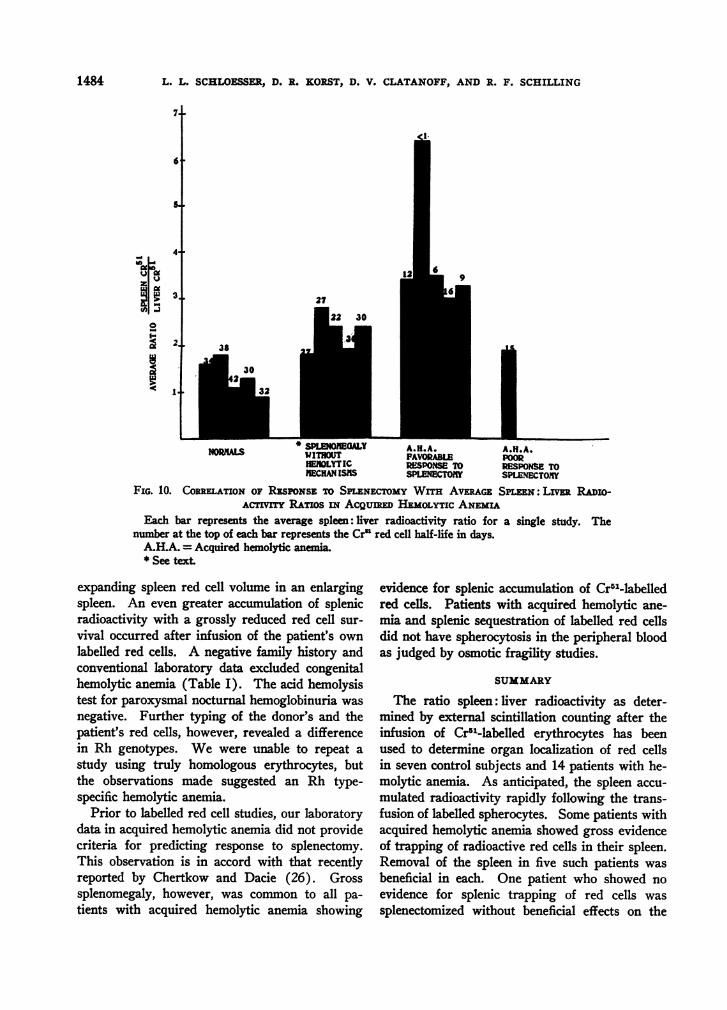
In Figure 10, average spleen to liver radioac-tivity ratios in acquired hemolytic anemia patientswere grouped according to splenectomy response
and compared with the ratios obtained in normaland splenomegalic subjects not demonstratinghemolytic mechanisms. The latter group noted byan asterisk in Figure 10 includes average organradioactivity ratios from Studies 6 to 8, 11 and 25,Table II. Average ratios of spleen: liver radio-activity in the five normal subjects receiving la-belled normal red cells ranged from 0.9 to 1.8.The higher ratios of spleen: liver radioactivity insplenomegalic subjects without hemolytic anemiaare presumptive evidence for a greater labelled redcell volume "seen" by the detector over the largerorgan. These studies provided control observa-tions. From these data it appears that patientswith reduced Cr5' red cell survival and a risingor high spleen: liver radioactivity ratio will have afavorable response to splenectomy. Obviouslymany more patients will have to be studied by
Cr1 LABEL.LED (WASHED)HOMOLOGOUSNORMALRED CELLS
50 % SURVIVAL, 30 DAYSa
a
10]
bso60
40
20
SPLEEN, 6 cm IBELOW COSTAL MARGIN
AVERAGE RATIO SPLVEERN Cr ' 2.4
-~~~~~VRC1
4 12 e8 24 30 36DAYS
a
aI
3
6-5-4.3,2.l
Crm LABELLED (WASHEDAUTOLOGOUSRED CELLS50 % SURVIVAL: 8 DAYS
SPLEEN. It cm BELOWCOSTAL MARGIN
AVERAGERATIO EELNCr .
6 It 18 24 30 36DAYS
RECIPIENT J. L.IDIOPATHIC HEMOLYTIC ANEMIA
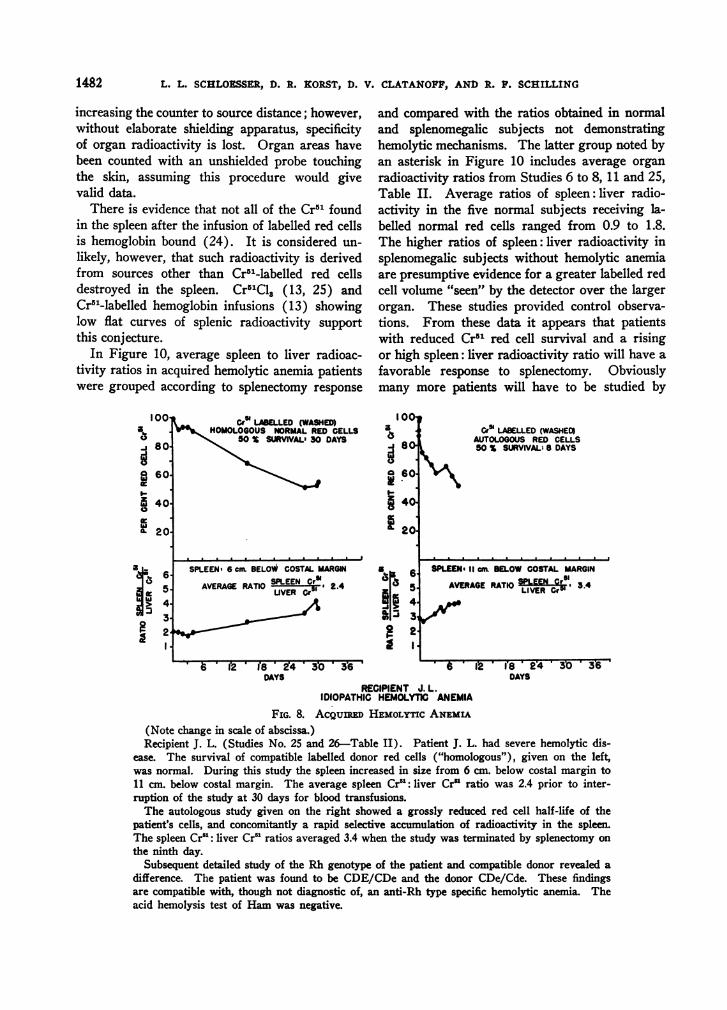
FIG. 8. ACQuIED HEMOLYTICANEMIA(Note change in scale of abscissa.)Recipient J. L. (Studies No. 25 and 26-Table II). Patient J. L. had severe hemolytic dis-
ease. The survival of compatible labelled donor red cells ("homologous"), given on the left,was normal. During this study the spleen increased in size from 6 cm. below costal margin to11 cm. below costal margin. The average spleen Cr": liver Cr' ratio was 2.4 prior to inter-ruption of the study at 30 days for blood transfusions.
The autologous study given on the right showed a grossly reduced red cell half-life of thepatient's cells, and concomitantly a rapid selective accumulation of radioactivity in the spleen.The spleen Cr': liver Cr" ratios averaged 3.4 when the study was terminated by splenectomy on
the ninth day.Subsequent detailed study of the Rh genotype of the patient and compatible donor revealed a
difference. The patient was found to be CDE/CDe and the donor CDe/Cde. These findingsare compatible with, though not diagnostic of, an anti-Rh type specific hemolytic anemia. Theacid hemolysis test of Hamwas negative.
100
9 80
g 60.
I 40.
20
ai
.13
65.4.3.2l
1482

SPLENIC TRAPPING OF RED CELLS IN HEMOLYTIC STATES
100O
o 80-J-i 6w
0
0 60-
z
0
a.
40-
201
8
in 7-
O 6-
J 4
0 3
r 2AI=
Cr5 LABELLED (WASHEDHOMOLOGOUSNORMALRED CELLS50 % SURVIVAL:.< I DAY
SPLEEN; 10 cm. BELOW COSTAL MARGIN
AVERAGE RATIO SPLEEN Cr, 6.4LIVER Crtm
2 4 6 8 10 12DAYS
RECIPIENT L. Y.AGQUIRED HEMOLYTIC ANEMIA
FIG. 9. ACQUIRED HEMOLYTICANEMIA(Note change in scale of abscissa.)Recipient L. Y. (Study No. 27-Table II). Patient
L. Y. had chronic lymphatic leukemia with severe hemo-lytic anemia. The accumulation of radioactivity in thespleen is striking and the plot of splee Crc: liver Cr'ratios is approximately reciprocal to the plot of disap-pearance of Cr'1-labelled erythrocytes from the peripheralblood. The average spleen Cry: liver Cr' ratio was 6.4.This patient had a good respnse to splenectomy.
these techniques before one can say that they pro-vide valid criteria for preoperative prediction ofthe results of splenectomy. In a correlation ofsplenic sequestration with results of splenectomythe following combinations are possible:
1)2)3)4)
Evidence forsequestration
Benefit fromsplenectomy
Our data from patients with acquired hemolyticanemia show five examples of the first combina-tion and one example of the fourth. Wehave notobserved No. 2 or 3. Thus it cannot be claimedthat the data provide evidence enabling one to
predict a failure to benefit from removal of thespleen. The data are considered evidence in favorof the theory that splenectomy will be beneficialin those patients demonstrating selective splenicsequestration of erythrocytes.
Wehave no data from patients with acquiredhemolytic anemia without detectable splenomegaly(Table II), and have studied only the one patient(J. T.-Table III) with minimal splenomegalywho had splenectomy. However, it is likely thatpatients with acquired hemolytic anemia, red cellsequestration in the spleen and normal spleen size(should these features co-exist) would showspleen: liver radioactivity ratios similar to that insubjects without splenomegaly infused with la-belled spherocytes (Figures 2 and 3a). Weareunable to explain the failure to demonstrate Cr11-lablled spherocyte accumulation in the spleen ofthe patient with hemolytic anemia without spleno-megaly (V. H.-Figure 3).
Cr5l-labelled erythrocyte studies, in addition tothe estimation of organ accumulation of red cells,may occasionally suggest mechanisms of hemolyticdisease previously unsuspected. Clinical evalua-tion of Patient A. K. had indicated a brisk hemo-lytic anemia, mild thrombopenia and leukopenia.Splenectomy might have been advised -for "hyper-splenism" had not erythrocyte survival studies in-dicated an intracorpuscular defect (Figure 5).There was no evidence for congenital hemolyticanemia (Table I), and the acid hemolysis testwas unequivocally positive establishing the diag-nosis of paroxysmal nocturnal hemoglobinuria.Organ radioactivity ratios in this patient did notsuggest splenic accumulation of autologous or ho-mologous erythrocytes. These studies are in ac-cord with the usual observation that patients withthis disorder are not helped by splenectomy (18).On the other hand, Jandl and his colleagues havereported that splenectomy was beneficial in a pa-tient with this disorder in whom splenic seques-tration of autologous Cr51-labelled red cells hadbeen demonstrated (13).
Studies with radioactive red cells in PatientJ. L. were of particular interest. This patient hadsevere hemolytic anemia of unknown type. Thesurvival of "homologous" normal Cr51-labelled redcells was normal. The relatively marked rise ofthe spleen: liver radioactivity ratio during thisstudy (Figure 8) was considered secondary to an
1483
L. L. SCHLOESSER, D. R. KORST, D. V. CLATANOFF, AND R. F. SCHILLING
6
I-QI
0 j
So
3
2. 38
S EOREAT A.H.A. A.H.A.NORM"L WITHOUT FAVORABLE POORHEMOLYTIC RESPONSETO RESPONSETOIECHANISS SPLENECTOKY SPLENECTOMIY
FIG. 10. CORRELATIONOF RESPONSETO SPLENECTOMYWITH AvERAcz SPUEN: LiVER RADIo-ACmTVT RATios IN AcQunw HEMOLYTICANEMIA
Each bar represents the average spleen: liver radioactivity ratio for a single study. Thenumber at the top of each bar represents the Cr' red cell half-life in days.
A.H.A. = Acquired hemolytic aneia.* See text.
expanding spleen red cell volume in an enlargingspleen. An even greater accumulation of splenicradioactivity with a grossly reduced red cell sur-vival occurred after infusion of the patient's ownlabelled red cells. A negative family history andconventional laboratory data excluded congenitalhemolytic anemia (Table I). The acid hemolysistest for paroxysmal nocturnal hemoglobinuria wasnegative. Further typing of the donor's and thepatient's red cells, however, revealed a differencein Rh genotypes. Wewere unable to repeat astudy using truly homologous erythrocytes, butthe observations made suggested an Rh type-specific hemolytic anemia.
Prior to labelled red cell studies, our laboratorydata in acquired hemolytic anemia did not providecriteria for predicting response to splenectomy.This observation is in accord with that recentlyreported by Chertkow and Dacie (26). Grosssplenomegaly, however, was common to all pa-tients with acquired hemolytic anemia showing
evidence for splenic accumulation of Cr5l-labelledred cells. Patients with acquired hemolytic ane-mia and splenic sequestration of labelled red cellsdid not have spherocytosis in the peripheral bloodas judged by osmotic fragility studies.
SUMMARY
The ratio spleen: liver radioactivity as deter-mined by external scintillation counting after theinfusion of Cr51-labelled erythrocytes has beenused to determine organ localization of red cellsin seven control subjects and 14 patients with he-molytic anemia. As anticipated, the spleen accu-mulated radioactivity rapidly following the trans-fusion of labelled spherocytes. Somepatients withacquired hemolytic anemia showed gross evidenceof trapping of radioactive red cells in their spleen.Removal of the spleen in five such patients wasbeneficial in each. One patient who showed noevidence for splenic trapping of red cells wassplenectomized without beneficial effects on the
1484
'a
SPLENIC TRAPPING OF RED CELLS IN HEMOLYTIC STATES
hemolytic process. The method described is con-sidered a useful aid in the selection of patientswhose hemolytic process will be benefitted bysplenectomy.
ACKNOWLEDGMENT
The authors appreciate the cooperation of Kay Strutz,Virginia Loy, and Francis Morris.
REFERENCES
1. Emerson, C. P., Jr., Shen, S. C., and Castle, W. B.,The osmotic fragility of the red cells of the periph-eral and splenic blood in patients with congenitalhemolytic jaundice transfused with normal redcells (abstract). J. Clin. Invest., 1946, 25, 922.
2. Young, L. E., Platzer, R. F., Ervin, D. M., and Izzo,M. J., Hereditary spherocytosis. II. Observationson the role of the spleen. Blood, 1951, 6, 1099.
3. Weisman, R., Jr., Hurley, T. H., Harris, J. W., andHam, T. H., Studies of the function of the spleenin the hemolysis of red cells in hereditary sphero-cytosis and sickle cell disorders. J. Lab. & Clin.Med., 1953, 42, 965.
4. Ham, T. H., and Castle, W. B., Studies on the de-struction of red blood cells. Relation of intra-vascular stasis and of abnormal fragility of erythro-cytes to the mechanism of hemolysis in certainhemolytic anemias. Year Book, Am. Philosoph.Soc., Philadelphia, 1939, p. 228.
5. Ham, T. H., and Castle, W. B., Studies on destructionof red blood cells. Relation of increased hypotonicfragility and of erythro-stasis to the mechanism ofhemolysis in certain anemias. Proc. Am. Philo-soph. Soc., 1940, 82, 411.
6. Ham, T. H., and Castle, W. B., Mechanism of he-molysis in certain anemias: Significance of in-creased hypotonic fragility and of erythrostasis(abstract). J. Clin. Invest, 1940, 19, 788.
7. Ham, T. H., and Castle, W. B., Relation of increasedhypotonic fragility and of erythrostasis to themechanism of hemolysis in certain anemias. Tr.A. Am. Physicians, 1940, 55, 127.
8. Weisman, R., Jr., Ham, T. H., Hinz, C. F., Jr., andHarris, J. W., Studies of the role of the spleen inthe destruction of erythrocytes. Tr. A. Am.Physicians, 1955, 68, 131.
9. Emerson, C. P., Jr., Shen, S. C., Ham, T. H., Flem-ing, E. M., and Castle, W. B., Studies on the de-struction of red blood cells. IX. Quantitative meth-ods for determining the osmotic and mechanicalfragility of red cells in the peripheral blood andspleen pulp. The mechanism of increased hemoly-sis in hereditary spherocytosis (congenital hemo-lytic jaundice) as related to the functions of thespleen. Arch. Int. Med., 1956, 97, 1.
10. Micheli, F., Unmittelbare effekte der splenektomiebei einem fall von erworbenem hiimolytischen
splenomegalischen ikterus typus nayem-Widal.Wien. klin. Wchnschr., 1911, 24, 1269.
11. Huff, R. L., Elmlinger, P. J., Garcia, J. F., Oda,J. M., Cockrell, M. C., and Lawrence, J. H., Fer-rokinetics in normal persons and in patients hav-ing various erythropoietic disorders. J. Clin. In-vest., 1951, 30, 1512.
12. Jandl, J. H., Greenberg, M. S., Yonemoto, R. H., andCastle, W. B., Clinical determination of the sitesof red cell destruction. Clin. Research Proc., 1955,3, 95.
13. Jandl, J. H., Greenberg, M. S., Yonemoto, R. H., andCastle, W. B., Clinical determination of the sites ofred cell sequestration in hemolytic anemias. J.Clin. Invest., 1956, 35, 842.
14. Korst, D. R., Clatanoff, D. V., and Schilling, R. F.,External scintillation counting over the liver andspleen after the transfusion of radioactive eryth-rocytes. Clin. Research Proc., 1955, 3, 195.
15. Ham, T. H., Ed., A syllabus of laboratory examina-tion in clinical diagnosis. Critical evaluation oflaboratory procedures in the study of the patient.Cambridge, Harvard University Press, 1950.
16. Malloy, H. T., and Evelyn, K. A., The determinationof bifirubin with the photoelectric colorimeter. J.Biol. Chem., 1937, 119, 481.
17. Ducci, H., and Watson, C. J., The quantitative de-termination of the serum bilirubin with specialreference to the prompt-reacting and the chloro-form-soluble types. J. Lab. & Clin. Med., 1945, 30,293.
18. Dacie, J. V., The Hemolytic Anemias. Congenitaland Acquired. NewYork, Grune & Stratton, 1954.
19. Watson, C. J., Studies of urobilinogen. I. An im-proved method for the quantitative estimation ofurobilinogen in urine and feces. Am. J. Clin. Path.,1936, 6, 458.
20. Watson, C. J., Schwartz, S., Sborov, V., and Bertie,E., Studies of urobilinogen. V. A simple methodfor the quantitative recording of Ehrlich reactionas carried out with urine and feces. Am. J. Clin.Path., 1944, 14, 605.
21. Read, R. C., Studies of red-cell volume and turnoverusing radiochromium. Description of a new"closed" method of red-cell-volume measurement.New England J. Med., 1954, 250, 1021.
22. Ebaugh, F. G., Jr., Emerson, C. P., and Ross, J. F.,The use of radioactive chromium 51 as an eryth-rocyte tagging agent for the determination of redcell survival in vivo. J. Clin. Invest., 1953, 32,1260.
23. Strumia, M. M., Taylor, L., Sample, A. B., Colwell,L. S., and Dugan, A., Uses and limitations ofsurvival studies of erythrocytes tagged with Cr'.Blood, 1955, 10, 429.
24. Schloesser, L. L., Unpublished data.25. Korst, D. R., Unpublished data.26. Chertkow, G., and Dacie, J. V., Results of splenec-
tomy in auto-immune haemolytic anaemia. Brit. J.Haemat., 1956, 2, 237.
1485