radiation sources: lessons from goiania · pdf fileradiation sources: lessons from goiania ......
TRANSCRIPT

Features
Radiation sources:Lessons from Goiania
An impressive co-operative responsehelped limit the accident's consequences
and document the lessons learned
On 13 September 1987, a shielded, stronglyradioactive caesium-137 medical source wasremoved from its housing in a teletherapy machine.Tne machine had been left in a clinic abandoned bythe Instituto Goiano de Radioterapia in Goiania,the capital of the State of Goias in Central Brazil.
By 18 September, the source assembly had beenbroken out of its protective shielding and sold to ascrap metal dealer. On 21 September, the sourcecapsule, previously damaged, was broken open.Fragments of the source were distributed to otherareas of the city. Many people were directly irradi-ated by the source and were externally and inter-nally contaminated by caesium-137. Severalpersons became ill and sought medical attention.
Finally, on 28 September, a medical physician inGoiania recognized the characteristic symptoms ofradiation overexposure. A physicist who was con-sulted the next day detected high radiation levelsand promptly notified Goias health authorities, whothen contacted Brazil's National Nuclear EnergyCommission (CNEN). The Goias officials thenevacuated the affected areas and began to identifythose persons who had been seriously exposed.
CNEN immediately sent an advance team toGoiania to help treat affected persons and to con-trol contaminated areas. CNEN mobilized substan-tial additional resources and an emergencyresponse centre was set up to co-ordinate activities.
(Brazil informed the IAEA of the emergency andrequested assistance under the new Convention onAssistance in the Case of a Nuclear Accident orRadiological Emergency. The IAEA arranged forassistance by US medical experts, for assistancefrom IAEA technical co-operation experts and theprovision of dosimeters, and for the provision ofmonitoring equipment from France, the FederalRepublic of Germany, Hungary, Israel, the Nether-lands, and the United Kingdom. Separately,
Argentina, France, the Federal Republic ofGermany, the Soviet Union, the United Kingdom,and the United States provided other experts andequipment directly to Brazil.)
Twenty persons in all were hospitalized. Despiteintensive medical care, four of them died. Twenty-eight had been seriously contaminated. Over thenext two months, a contamination monitoringstation set up in a stadium screened more than112 000 people. Hundreds had to be decon-taminated.
Once the seriousness of the accident had beenrecognized, the most severely contaminated areaswere identified and closed off within a day. Thehighest radiation levels were reduced substantiallyby shielding the areas affected. Within two weeks,all the contaminated areas had been identified andisolated and the cleanup had begun.
By late October, waste from the major decon-tamination work began to be moved to a site desig-nated by Goias State 20 kilometres from Goiania.By mid-December, restrictions on the main con-taminated areas of Goiania had been lifted. Morethan 3000 cubic metres of waste were removed andstored at the new repository.
In all, more than 700 workers participated in theresponse, including CNEN staff and personnel fromthe Brazilian army, NUCLEBRAS, FURNAS, theState of Goias, and private companies. Workerdoses during the operation were held to an averageof about 20% of annual occupational limits.
Details of the accident, the response to it, andlessons learned have recently been published by theIAEA in the report The Radiological Accident inGoiania. * The report is based on a review meetingof experts held in July 1988 in Rio de Janeiro underthe joint organization of CNEN and the IAEA. Thefollowing summation is drawn from that report.
* The report is available from the IAEA Division of Publications. See the Keep abreast section for ordering information.
10 IAEA BULLETIN, 4/1988

Features
In Goiania, authorities desig-nated a nearby Olympic Stadiumas a staging area for isolatingpatients and screening othersfor contamination. Shown hereare some people being moni-tored. (Credit: CNEN)
!
The accident
It is now known that at about the end of 1985, aprivate radiotherapy institute, the Instituto Goiano deRadioterapia in Goiania, Brazil, moved to newpremises, taking with it a cobalt-60 teletherapy unit andleaving in place a caesium-137 teletherapy unit withoutnotifying the licensing authority as required under theterms of the institute's license. The former premiseswere subsequently partly demolished. As a result, thecaesium-137 teletherapy unit became totally insecure.Some time later, in September 1987, two people enteredthe premises and, not knowing what the unit was butthinking it might have some scrap value, removed thesource assembly from the radiation head of the machine.This they took home and tried to dismantle.
In the attempt, the source capsule was ruptured. Theradioactive source was in the form of caesium chloridesalt, which is highly soluble and readily dispersible.Contamination of the environment ensued, with oneresult being the external irradiation and internal con-tamination of several persons. Thus began one of themost serious radiological accidents ever to haveoccurred.
After the source capsule was ruptured, the remnantsof the source assembly were sold for scrap to a junkyardowner. He noticed that the source material glowed bluein the dark. Several persons were fascinated by this andover a period of days friends and relatives came and sawthe phenomenon. Fragments of the source the size ofrice grains were distributed to several families. Thisproceeded for five days, by which time a number ofpeople were showing gastrointestinal symptoms arisingfrom their exposure to radiation from the source.
The symptoms were not initially recognized as beingdue to irradiation. However, one of the persons irradi-
IAEA BULLETIN, 4/1988
ated connected the illnesses with the source capsule andtook the remnants to the public health department in thecity. This action began a chain of events which led to th£discovery of the accident.
A local physicist was the first to assess, by monitor-ing, the scale of the accident and took actions on his owninitiative to evacuate two areas. At the same time, theauthorities were informed, upon which the speed and thescale of the response was impressive. Several other sitesof significant contamination were quickly identified andresidents evacuated.
The human consequences
Shortly after it had been recognized that a seriousradiological accident had occurred, specialists — includ-ing physicists and physicians — were dispatched fromRio de Janeiro and Sao Paulo to Goiania. On arrival,they found that a stadium had been designated as a tem-porary holding area where contaminated and/or injuredpersons could be identified. Medical triage was carriedout, from which 20 persons were identified as needinghospital treatment.
Fourteen of these people were subsequently admittedto the Marcilio Dias Naval Hospital in Rio de Janeiro.The remaining six patients were cared for in the GoianiaGeneral Hospital. A whole-body counter was set up toassist in the bioassay programme and to monitor theefficacy of the drug Prussian Blue, which was given topatients in both hospitals to promote the decorporationof caesium. Cytogenetic analysis was very helpful in dis-tinguishing the severely irradiated persons from thoseless exposed who did not require intensive medical care.
Decontamination of the patients' skin and dealingwith desquamation from radiation injuries and contami-nated excreta posed major problems of care. Daily hae-
11

Features
The accident in Goiania in perspective
Considerable information has been documentedabout accidents since 1945 with significant overexposureto radiation. Most of the accidents at nuclear facilitiesoccurred early in the development of the applications ofnuclear energy. Some were criticality accidents andseveral were at experimental reactors. Although the inci-dence of radiation accidents in nuclear facilities hasdecreased considerably over the years, the number ofsuch accidents elsewhere has risen. Several accidentshave affected members of the public. Some resulted indeaths when control was lost over high strength sources,which, unrecognized for what they were, ended up in thepublic domain.
The general picture seems clear and well documen-ted, even though some serious radiation accidents (forexample, hand exposures of industrial radiographers)may not have been reported and, to that extent, informa-tion that would be useful for preventing similar accidentsis unavailable, in comparison with the number of deathscaused by other types of industrial accidents every year,those due to accidental radiation exposure reportedworldwide over 40 years are not many. However, the rela-tively good safety record for applications of radiationgives no grounds for complacency, especially wherepracticable, effective steps can be taken to reduce therisks of such accidents.
Serious radiation accidents reported,1945-1987
Type offacility
No. of events Overexposures Deaths
Nuclearfacilities
Non-nuclearfacilities
IndustryResearchMedical
27 (34%) 272 (64%) 35 (59%)
42 (52<>/o) 84 (20%) 20 (34%)7(9%) 10(2%) - ( - )4 (5%) 62 (14%) 4 (1%)
80 (100%) 428 (100%) 59 (100%)
An overexposure is taken here as exposure of the wholebody, blood-forming organs, or other critical organs to0.25 Sv or more; of skin to 6 Sv or more; other externalexposure of 0.75 Sv or more; and internal contaminationof half or more of the "maximum permissible organ bur-den". (The concept of the "maximum permissible organburden" has now been superseded by the concept of the"annual limit of intake".) The table excludes patient-related events and off-site exposures at Chernobyl.
Fatal
Year
radiation accidents reported,
Location
1945-1987
Radiationsource
Fatalities
Worker Public
19451946195819581961196219631964196419751978198119821983198419861987
Los Alamos, USALos Alamos, USAVinca, YugoslaviaLos Alamos, USASwitzerlandMexico City, MexicoChinaFed. Rep. of GermanyRhode Island, USABrescia, ItalyAlgeriaOklahoma, USANorwayConstituyentes, ArgentinaMoroccoChernobyl, USSRGoiania, Brazil
Critical assemblyCritical assemblyExperimental reactorCritical assemblyTritiated paintLost radiography sourceSeed irradiatorTritiated paintUranium* recovery plantFood irradiatorLost radiography sourceIndustrial radiographyInstrument sterilizerResearch reactorLost radiography sourceNuclear power plantStolen teletherapy source
111
111
29
Total: 17 events with 59 fatalities 40 19
Note: The table refers to reported accidents in nuclear facilities and non-nuclear facilities in industry, research, and medi-cine (excluding patient-related events).
Sources: "The Medical Basis for Radiation Accident Preparedness" (Proc. REAC/TS Int. Conf. Oak Ridge, TN, 1979)(Hiibner, K.F., Fry, S.A., Eds), Elsevier North Holland, New York (1980); United Nations Scientific Committee on theEffects of Atomic Radiation, Ionizing Radiations: Sources and Biological Effects, 1982 Report to the General Assembly,United Nations, New York (1982).
— Information and tables are excerpted from the IAEA's Nuclear Safety Review for 1987, copies of which are availablefrom the IAEA Division of Publications. See the Keep Abreast section for ordering information.
12 IAEA BULLETIN, 4/1988
Features
•
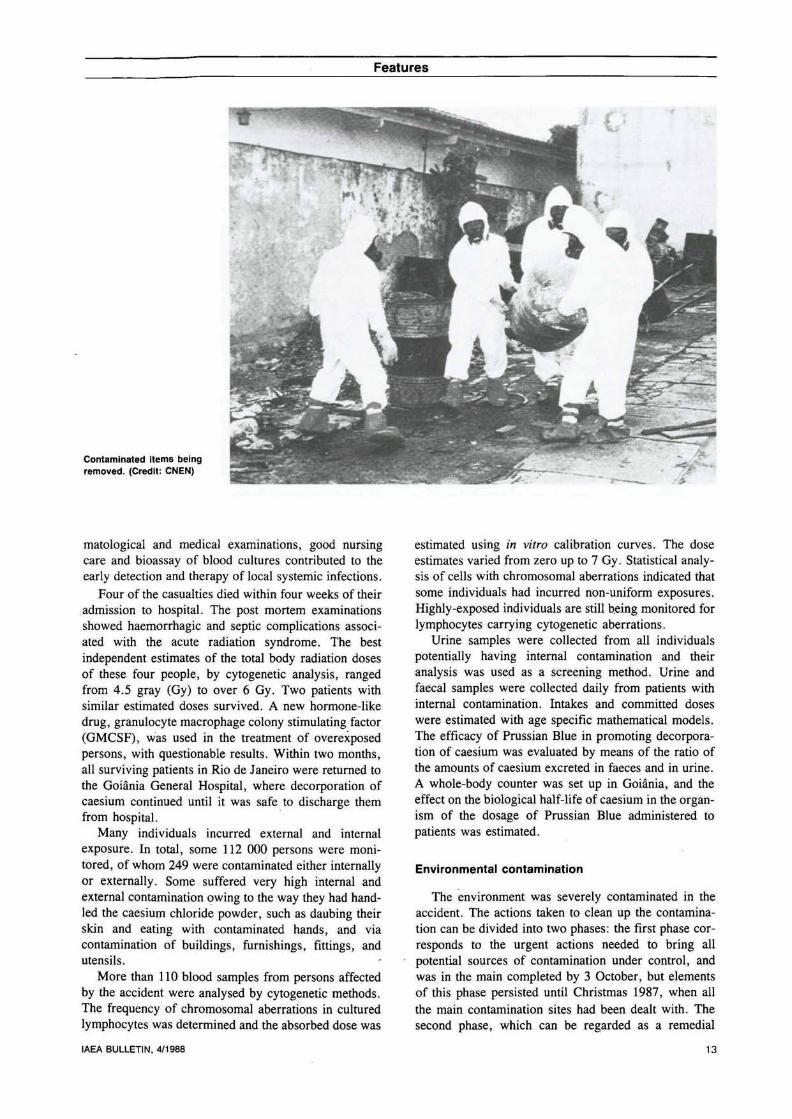
Contaminated items beingremoved. (Credit: CNEN)
matological and medical examinations, good nursingcare and bioassay of blood cultures contributed to theearly detection and therapy of local systemic infections.
Four of the casualties died within four weeks of theiradmission to hospital. The post mortem examinationsshowed haemorrhagic and septic complications associ-ated with the acute radiation syndrome. The bestindependent estimates of the total body radiation dosesof these four people, by cytogenetic analysis, rangedfrom 4.5 gray (Gy) to over 6 Gy. Two patients withsimilar estimated doses survived. A new hormone-likedrug, granulocyte macrophage colony stimulating factor(GMCSF), was used in the treatment of overexposedpersons, with questionable results. Within two months,all surviving patients in Rio de Janeiro were returned tothe Goiania General Hospital, where decorporation ofcaesium continued until it was safe to discharge themfrom hospital.
Many individuals incurred external and internalexposure. In total, some 112 000 persons were moni-tored, of whom 249 were contaminated either internallyor externally. Some suffered very high internal andexternal contamination owing to the way they had hand-led the caesium chloride powder, such as daubing theirskin and eating with contaminated hands, and viacontamination of buildings, furnishings, fittings, andutensils.
More than 110 blood samples from persons affectedby the accident were analysed by cytogenetic methods.The frequency of chromosomal aberrations in culturedlymphocytes was determined and the absorbed dose was
estimated using in vitro calibration curves. The doseestimates varied from zero up to 7 Gy. Statistical analy-sis of cells with chromosomal aberrations indicated thatsome individuals had incurred non-uniform exposures.Highly-exposed individuals are still being monitored forlymphocytes carrying cytogenetic aberrations.
Urine samples were collected from all individualspotentially having internal contamination and theiranalysis was used as a screening method. Urine andfaecal samples were collected daily from patients withinternal contamination. Intakes and committed doseswere estimated with age specific mathematical models.The efficacy of Prussian Blue in promoting decorpora-tion of caesium was evaluated by means of the ratio ofthe amounts of caesium excreted in faeces and in urine.A whole-body counter was set up in Goiania, and theeffect on the biological half-life of caesium in the organ-ism of the dosage of Prussian Blue administered topatients was estimated.
Environmental contamination
The environment was severely contaminated in theaccident. The actions taken to clean up the contamina-tion can be divided into two phases: the first phase cor-responds to the urgent actions needed to bring allpotential sources of contamination under control, andwas in the main completed by 3 October, but elementsof this phase persisted until Christmas 1987, when allthe main contamination sites had been dealt with. Thesecond phase, which can be regarded as a remedial
IAEA BULLETIN, 4/1988 13
Features
phase aiming to restore normal living conditions, lasteduntil March 1988.
The primary objectives of the urgent response wereto prevent high individual radiation doses that mightbring about non-stochastic effects; to identify the mainsites of contamination; and to establish control overthese sites. In the initial response, all actions were aimedat bringing sources of actual exposure under control,and this took three days.
Initial radiation surveys were conducted on foot overthe contaminated areas. Seven main foci of contamina-tion were identified around the junkyards concerned,some of them with dose levels of up to 1 sievert per hourat one meter.
An aerial survey by a suitably equipped helicopterconfirmed that no major areas of contamination had beenoverlooked. Over a period of two days, all of the morethan 67 square kilometers of urban areas of Goianiawere monitored. The extents of the seven known prin-cipal foci were confirmed and only one previouslyunknown site, giving rise to a dose rate of about20 millisievert (mSv) per hour at one metre, wasdiscovered.
It was possible for lesser areas of contamination tohave been missed, especially in the vicinity of the heav-ily contaminated areas around the main foci. A com-plementary system of monitoring covering large areas,although limited to roads, was put into practice. Thissystem used detectors mounted on and in cars, and 80%of the Goiania road network, over 2000 kilometres, wasthus covered. The main foci of contamination were thejunkyards and residences where the integrity of the
source capsule was breached; these covered an area ofabout one square kilometre.
Action levels in this initial response were set for con-trol of access (10 mSv per hour); for evacuation andprohibited access (2.5 mSv per hour and later 10 mSvper hour for houses, and 150 mSv per hour for unoc-cupied areas); and for workers participating in accidentmanagement (dose limits and corresponding dose ratesper day, week, and month). In total, 85 houses werefound to have significant contamination, and200 individuals were evacuated from 41 of them. Aftertwo weeks, 30 houses were free for reoccupation. Itshould be emphasized that these, levels, whichcorrespond roughly to the lowest values of the interven-tion levels recommended by the International Commis-sion on Radiological Protection and the IAEA(non-action levels), were extremely restrictive, owing topolitical and social pressures.
Subsequently, the dissemination of contaminationthroughout the area and the hydrographic basin wasassessed. A laboratory was set up in Goiania for measur-ing the caesium content of soils, ground water, sedimentand river water, drinking water, air, and foodstuffs.Countermeasures were only necessary, however, forsoil and fruit within a 50-metre radius of the main foci.
The subsequent response, consisting mainly ofactions undertaken for recovery, faced various difficul-ties in surveying the urban area and the river basin.These were compounded by the heavy rain that hadfallen between 21 and 28 September, which had furtherdispersed caesium into the environment. Instead of beingwashed out as expected, radioactivity materials were
Control, safe use, and disposal of radiation sources
The use of radiation sources of various types andactivities is widespread in industry, medicine, research,and teaching in virtually all Member States of theAgency. Loss of control of radiation sources can give riseto unplanned exposures to workers, patients, and mem-bers of the public, sometimes with fatal results. Exam-ples are the events in Mexico in 1983-1984, Morocco in1984, and the recent accident in Brazil in 1987.
Agency programmes aimed at reducing the likelihoodof such events have been ongoing for some time; forexample the Waste Management Advisory Programme(WAMAP) missions and the Radiation Protection Advi-sory Teams (RAPAT). However, the events of 1987 haveprompted renewed efforts towards improving the controlover sealed sources in Agency Member States.
In late 1987, the Agency introduced new programmesto enhance its efforts towards providing practical help toMember States in the control of sources while in use andin the management of the sources at the end of their use-ful lives. Assistance in this latter area will be given in twomain ways:
• Short-term assistance in waste disposal. In the shortterm, prompt action may be justified in a few MemberStates which have no capability at present for the safemanagement and disposal of radiation sources. Thesespecial cases are considered to be identified throughWAMAP or RAPAT missions reports. The Agency is plan-ning to institute discussions on this and other relatedsubjects with Member States, including countries whichare supplying radiation sources.• Promotion of national waste management capabili-ties. The Agency will provide guidance on procedures forthe collection and immobilization of sources and, asnecessary, safe storage and eventual disposal. Empha-sis is placed on standardization of designs and proce-dures, as for example in the provision of plans anddesigns for immobilization and storage facilities. A pilotdemonstration of many of these techniques has beendesigned; this will be conducted in late 1988 in conjunc-tion with a WAMAP mission. Preparations were made tomake a video film to illustrate the techniques for use aspart of the guidance material and also for use in trainingcourses.
14 IAEA BULLETIN, 4/1988

Features
As part of decontamination efforts, an excavator removes a radiation "hot spot" in a house before demolition. (Credit: CNEN)
deposited on roofs, and this was the major contributorto dose rates in houses.
Levels of contamination in drinking water were verylow. The groundwater was also found to be free of con-tamination, except for a few wells near the main foci ofcontamination with concentrations of caesium just abovethe detection level.
The main countermeasures undertaken during thisremedial phase were the decontamination of the mainsites of contamination (including areas outside the mainfoci), of houses, of public places, of vehicles, and so on.For decontamination at the main foci, heavy machinerywas necessary to remove large amounts of soil and fordemolishing houses. Large numbers of various types ofreceptacles for the waste also had to be constructed. Inaddition, a temporary waste storage site had to beplanned and built. This was done by the middle ofNovember, and decontamination of the main foci andremaining areas was carried out from mid-November upuntil the end of December 1987.
The investigation levels selected for considering thevarious actions corresponded to a projected dose of5 mSv in the first year and a long-term projected doseof 1 mSv per year in subsequent years. The workincluded the demolition (and removal) of seven housesand the removal of soil. Areas from which soil wasremoved were covered with concrete or a soil pad. Inless contaminated places, the main source of exposure
was contaminated dust deposited on the soil; afterremoval of the soil layers where necessary, surfaceswere covered with clean soil. Of 159 houses monitored,42 required decontamination. This decontamination wasachieved by vacuum cleaning inside and by washingwith high pressure water jets outside. Various proce-dures for chemical decontamination proved to be effec-tive, each adapted to the circumstances, the materialconcerned, and the level of radioactivity.
The action levels for these remedial actions wereselected under strong political and public pressures. Thelevels were set substantially lower than would haveresulted from an optimization process. In most cases,they could be regarded as more applicable to normalsituations than to an accident recovery phase.
After the Christmas holidays in December 1987, theareas of lower dose rate surrounding the main fociwere decontaminated. There was no need for heavymachinery, and optimization procedures were developedand adopted. This stage lasted until March 1988.
From its inception, the response generated largequantities of radioactive wastes. A temporary wastestorage site was chosen 20 kilometres from Goiania.Wastes were classified into non-radioactive (below74 kilobecquerels per kilogram), low level (below2 mSv per hour) and medium level (between 2 and20 mSv per hour). Various types of packaging wereused, according to the levels of contamination. The
IAEA BULLETIN, 4/1988 15
Features
packaging of wastes required 3800 metal drums (200litres), 1400 metal boxes (5 tonnes), 10 shipping con-tainers (32 cubic metres) and six sets of concrete packag-ing. The temporary storage site was designed for avolume of waste of 4000—5000 cubic metres, encapsu-lated in about 12 500 drums and 1470 boxes.
The final total volume of wastes stored was 3500cubic metres, or more than 275 lorry loads. This largevolume is directly attributable to the restrictive actionlevels chosen, both in the emergency period and in therecovery phase. The economic burden of such levels,especially in the latter phase, is far from insignificant.
A sampling system was built to monitor the run-off(including rainwater) from the platform on which thewastes were placed. The best estimate of the radio-activity accounted for in contamination is around44 terabecquerels (1200 curies), compared with theknown radioactivity of the caesium chloride sourcebefore the accident of 50.9 terabecquereis (1375 curies).No decision has yet been made on the final disposal sitefor the waste.
Observations and recommendations
Very often reviews of radiological accidents serveonly to call attention to what is already well known.Many observations and recommendations emerged fromthe review of the accident in Goiania. However, obser-vations made here do not necessarily refer to the specificcircumstances of the accident.
On the subject of the potential occurrence of suchaccidents, one major observation is that nothing candiminish the responsibility of the person designated asliable for the security of a radioactive source. Radio-active sources that are removed from the locationdefined in the process of notification, registration, andlicensing can present a major hazard. Means to precludesuch breaches of care should therefore be ensured by theperson liable for a radioactive source, and these shouldinclude verification procedures and appropriate securityarrangements. Although the regulatory system is a checkon the effectiveness of the professional and managementsystem, it should be emphasized that regulatory andlegal control cannot and must not detract frommanagerial responsibility.
In order to facilitate the discharging of responsibilityby the person liable for a radioactive source, suitableways of complying with regulatory requirements shouldbe specific, simple, and enforceable. In particular, goodcommunication is required among all concerned inimplementing and enforcing radiological protectionrequirements.
Recognition by the general public of the potentialdanger of radiation sources is an important factor in les-sening the likelihood of radiological accidents. Due con-sideration should be given to a system of markings forradiation hazards that would be recognizable to thewider public.
The physical and chemical properties of radioactivesources are very important in relation to radiologicalaccidents. They should be taken into account in thelicensing for manufacture of such sources, in view of thepotential influence of these properties on the conse-quences of accidents with, and in the misuse of, sources.
If, all precautions notwithstanding, an accident doesoccur and a radiological hazard is foreseen, there shouldbe a well understood chain of information and com-mand. In this regard, it is worth mentioning that prepa-rations to respond to radiological emergencies shouldcover not only nuclear accidents but the entire range ofpossible accidents entailing radiation exposure.
Medically, experience in Goiania confirmed ingeneral the' adequacy of presently available diagnostictechniques, antibiotics, and methods for platelet separa-tion and transfusion. In addition, it demonstrated theusefulness of cytogenetic dose estimates and the remark-able efficacy of Prussian Blue in eliminating internalcontamination by caesium-137.
The treatment of casualties of radiological accidentsis extremely varied and complex. They must be caredfor in hospitals by staff who are engaged on a daily basisin the haematological, chemotherapeutic, radiotherapeu-tic, and surgical treatment of patients at risk fromcancer, immunosuppression, and blood dyscrasias.Generally, medical personnel and facilities are not pre-pared for dealing with radiation injuries and radiologicalemergencies. Provision should be made in radiologicalemergency plans for immediate assistance from medicalspecialists trained to handle such patients. Recognitionof the nature of radiation injury, however, depends onthe education of non-nuclear workers as well as ontrained health professionals, all of whom are dependentupon widely disseminated educational programmes.
On the subject of dealing with the environmental con-tamination due to an accident, it is worth noting the issueof decisions on intervention levels. There is usually atemptation to impose extremely restrictive criteria forremedial actions, generally prompted by political andsocial considerations. Such criteria, however, impose asubstantial economic and social burden in addition tothat caused by the accident itself, and this is not alwayswarranted.
Finally, it is worth mentioning that an accident shouldbe documented as soon as possible, since the facts tendto become blurred with the passage of time. Dissemina-tion of information to the communications media, thepublic and, indeed, the response force is especiallyimportant. In particular, the response teams shouldreceive support in administration and public informationappropriate to the scale of the emergency. Major emer-gencies require prompt on-site administrative and publicinformational support. All individuals who are likelyresponders to radiological emergencies should undergotraining, both formal and in drills, appropriate to theirlikely functions.
16 IAEA BULLETIN, 4/1988

Features
Lessons learned by the Brazilian National Nuclear Energy Commission (CNEN)
• A radiological accident entailing contamination due tothe breaking up of a radioactive source can be aggra-vated if much time elapses before the discovery of theaccident.• The physical and chemical properties of a radioactivesource are important factors in an accident. The recordsof sealed sources should contain that information. It issuggested that physical and chemical properties ofsources should be taken into account in the licensing formanufacture of such sources, emphasizing the possibleconsequences of accidents or misuse.• An adequate system of information is essential toavert panic on the part of the public. In general, the pub-lic should be made aware of what radiation is and of itsapplications. A booklet explaining the special terms andunits related to radiation should be available to the com-munications media. In the event of a radiological emer-gency, a group should be set up to present informationin the legislative assembly, schools, churches, and com-munity associations, and so on, as well as to the newsmedia. Personnel working in decontamination andattending to casualties should be instructed on how toconvey information comprehensibly to the population.Their contacts with the individuals affected in the acci-dent in Goiania proved very important: people wouldgauge the seriousness of contamination by the reactionsof the workers. The people most affected by the accidentwould judge whether their houses were really free of con-tamination by whether the CNEN personnel acceptedwater or coffee from them.
• An adequate system of social and psychological sup-port should be provided following a radiological accidentcausing serious contamination. The psychological sup-port should be provided to those individuals directly andindirectly affected and the personnel working in responseto the emergency. Psychologists should be available forcounselling, joining the group responsible for makingquick decisions and planning action to be taken, andevaluating the possible stress to the casualties.• The effectiveness of international assistance follow-ing a radiological accident depends on the infrastructureof the country concerned. The emergency trainingcourses co-ordinated by the IAEA should be held indeveloping countries and not only in developed countrieswhere facilities are available and work well. In general,these programmes deal with emergencies responded toby strong organizations under a priori known conditions.In many countries, circumstances are very different,equipment is diverse, the climate is adverse, and mattersare administered differently.
• A mobile system of first aid transportable by airshould be available at all times.
• The IAEA should maintain a record of radiologicalequipment available. Customs regulations should beamended to facilitate the import and re-export of materialand/or equipment. The IAEA should have a set of radio-logical equipment at hand ready to be shipped andshould establish a regional centre for emergency atten-dance in every continent.
• Instrumentation should be capable of being adjustedto withstand field conditions, so that it can be used inhigh humidities, high temperatures, and unstableenvironmental conditions. Personnel using instrumentsshould be trained to be able to obtain a clear indicationof dose-rate response for a wide range of doses; and toknow the most suitable equipment in different conditionsand its calibration factors.
• Records of available personnel resources accordingto field of work should be kept. Experts from the IAEA, ineach area of action, should be available to be contactedin the event of an emergency to give support to the localradiological protection teams. These experts should beready to advise actively in decision making and on inter-vention measures, and to participate in all the work thatneeds to be done. The experience of the accident inGoiania indicated that supposedly 'better' reports had infact been prepared by specialists who had not partici-pated in the response.
• The provision of a temporary waste storage site nearthe area affected by a radiological accident is consideredindispensable. A delay in the decision, usually a politicalone, on where to construct a site, could permit greaterdispersion of radioactive material in the environment.
• An infrastructure of civil engineering personnelshould be available to participate in decontaminationwork.• For decision making and the organization of workingteams following a radiological accident, the hierarchyshould be well defined. The assigning of responsibilitiesin the decision process, from planning to action andevaluation of consequences, should be very clear, andeach group should be sure of its function. If possible,teams should be formed with a leader who heads thegroup in normal working conditions.
• In general, a programme of inspection of radiologicalequipment and facilities is very important; however, it isonly effective if coupled with some kind of enforcementsystem, such as assigning civil or professional liability inlicensing sources.
IAEA BULLETIN, 4/1988 17