r heumatoid a rthritis bmj 2011;342: 39-44 ra is a systemic inflammatory autoimmune disease with...
TRANSCRIPT

RHEUMATOID ARTHRITIS BMJ 2011;342: 39-44
RA is a systemic inflammatory autoimmune disease with localised and general manifestations. It is characterised by polyarticular inflammation of synovial tissue, which causes pain, swelling and stiffness of the joints of the hands, wrists, and feet in particular. It results in functional limitations and may progress to joint destruction and extra-articular disease (e.g. Nodules, osteoporosis, vasculitis, lung fibrosis, peripheral neuropathy).
SYNOVIAL TISSUE – the inside layer of the external fibrous joint capsule. It secretes a thick lubricating fluid

RHEUMATOID ARTHRITIS BMJ 2011;342: 39-44
It is diagnosed through a combination of the amount of joint involvement, and serology (rheumatoid factor, anti-citrullinated protein antibodies, C reactive protein, ESR)
More than a 12 week delay in referral to a rheumatologist is associated with a reduced chance of drug-free remission and increased risk for progressive joint damage
The ultimate goal of therapy is a “cure” i.e. Clinical remission
RA can have a gradual onset but damage still starts early

RHEUMATOID ARTHRITIS AMH 2011
Rationale for drug use – relieve symptoms and prevent damage to bones, joints and other organs
Before starting treatment – baseline assessment, CVD risk, consequences of suppressing immune function, physical and occupational therapy requirements, education, referral to a rheumatologist
Drug treatment* No evidence for clinical superiority of any
individual or class of antirheumatic

RHEUMATOID ARTHRITIS THERAPEUTIC GUIDELINES
Between 15-70% of the risk of developing RA may be due to genetic factors
RA is best characterised as a lymphocyte-mediated inflammatory disease
The stimulating antigens are unknown
Pro-inflammatory mediators
RHEUMATOID ARTHRITIS AMH 2011
Drug treatment
• Choice is based on disease severity and relative efficacy and toxicity of drugs
• Combinations of antirheumatics are used to improve efficacy but there is little evidence to inform appropriate choice
• Mild disease – sulfasalazine and hydroxychloroquine

RA – DRUG TREATMENT AMH 2011
Moderate – severe disease • low dose methotrexate – appears less toxic than other
immunosuppressants (azathioprine, cyclosporin, leflunomide), gold or penicillamine
• Methotrexate may need to be combined with cytokine modulators (also known as biological agents) or leflunomide to slow progression of joint damage
• Oral corticosteroids are well tolerated and work quickly but long-term use is undesirable. They reduce joint destruction and improve symptoms

RA – DRUG TREATMENT AMH 2011
The optimal dose of glucocorticoids in combination treatment is unknown (BMJ 2011; 342)
Withdrawal in remission often results in relapse – consider limiting the use of more toxic agents at this time
Daily supplements of omega-3 fatty acids may reduce severity of symptoms (at the correct dose)

TNFα ANTAGONISTS
NAME ACTS ON USE
Adalimumab TNFα
RA, psoriasis, psoriatic arthritis,
ankylosing spondylitis, IBD
Certolizumab TNFα
Etanercept TNFα
Golimumab TNFα
Infliximab TNFα
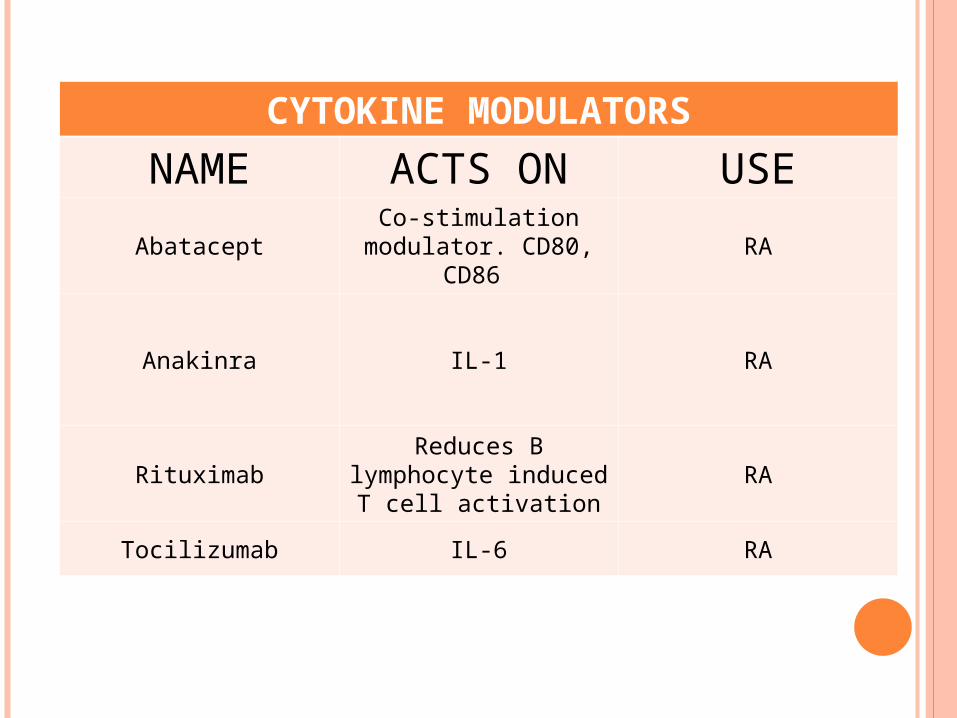
CYTOKINE MODULATORS
NAME ACTS ON USE
AbataceptCo-stimulation
modulator. CD80, CD86
RA
Anakinra IL-1 RA
RituximabReduces B
lymphocyte induced T cell activation
RA
Tocilizumab IL-6 RA

RA – BIOLOGIC AGENTS
TNF-alpha antagonists – they bind to TNF-alpha ADALIMUMAB ADA = chosen by manufacturer LIM = for immune and inflammatory diseases U = human MAB = monoclonal antibody INFLIXIMAB INF = chosen by manufacturer LI = for immune and inflammatory diseases XI = chimeric MAB = monoclonal antibody


RA - IMMUNOLOGY
“mAbs to human targets are generated either in other species – for example, in mice – or through recombinant engineering. With chimeric mAbs, the variable region of a murine-derived mAb is fused to the Fc piece of a human IgG molecule. The resulting construct is approximately one quarter murine and three quarters human.”
(Recombinant engineering – the use of viruses or yeast to create antibodies rather than mice)
J Allergy Clin Immunol 2010; 125: 814-20.

RA – IMMUNOLOGY Immune system cells originate from stem cells of the
bone marrow They differentiate into lymphocyte stem cells or
myeloid stem cells Lymphocyte stem cells produce T lymphocytes and
B lymphocytes Myeloid cells produce granulocytes (neutrophils,
eosinophils, basophils, mast cells, monocytes and macrophages – the last 2 cell types producing the cytokines TNF, IL-1 and IL-6)
T lymphcytes bind to the antigen directly, through their surface receptors (i.e. CD (“cluster of differentiation”) receptors).
Allergy. Arshad SH. Churchill Livingstone 2002

RA IMMUNOLOGY
STEM CELL
Lymphocyte stem cell Myeloid stem cell
T lymphocyte B Lymphocyte Granulocytes (Neutrophil, basophils,
eosinophils, mast cells,
monocytes, macrophages)
Bind directly cytokines
Immunoglobulins autoantibodies Cytokines (TNFα,
IL-1, IL-6)

RA - IMMUNOLOGY T lymphocytes, monocytes and macrophages
contribute to immunological responses through release of cytokines
B lymphocytes produce immunoglobulins or antibodies (i.e. IgG, IgA, IgM, IgD, IgE)
An antibody molecule is Y-shaped. The stem of the Y = Fc fragment. It binds to the cell surface receptor
The two forks = Fab ( ab = antigen binding) fragments
Allergy. Arshad SH. Churchill Livingstone 2002.

ANTIBODIES
Antigen binding
Fab light chain
heavy chain
Fc Combines with complement
Binds to macrophages
Biologic activity

RA – IMMUNOLOGY B lymphocytes are thought to play a
pathogenic role in RA by producing autoantibodies (i.e. rheumatoid factor, anticyclic citrullinated protein)
IL-6 is a multifunctional cytokine that is involved in the acute inflammatory response. It induces the development of B cells, osteoclastogenesis, and acute phase proteins production in the liver. High levels of Il-6 have been found in the synovial fluids from inflamed joints of patients with RA
J Allergy Clin Immunol 2010; 125: 814-20


RA – TNF J ALLERGY CLIN IMMUNOL 2010; 125: S314-23
TNF is a proinflammatory cytokine in RA, psoriatic arthritis, and ankylosing spondylitis
TNF activates various cell types, promotes accumulation of immunocompetent cells at sites of inflammation by activation of the vascular endothelium, and stimulates synthesis of other pro-inflammatory cytokines (e.g. IL-1, IL-6)
Both TNF and IL-1 mediate bone and cartilage destruction through activation of osteoclasts and macrophages to release destructive mediators (collagenase, prostaglandins)

CYTOKINE MODULATORS
ANAKINRA is a recombinant Il-1ra (ra = receptor antagonist).
TOCILIZUMAB is a humanised anti IL-6 receptor mAB that binds to both soluble and membrane-bound IL-6 receptor
ABATACEPT is a soluble protein consisting of the extracellular domain of CTLA-4 (cytotoxic T lymphocyte-associated antigen 4) linked to the Fc portion of IgG1
J Allergy Clin Immunol 2010; 125: S314-23