publisher and€¢ wha t are the risks of sedati ng pati ents i n the gi endoscopy unit? • how...
TRANSCRIPT

PublisherAnd
Editor-in-ChiefFRANK MOYA, MD
Coral Gables, Florida
EDITORIAL BOARDJohn Aker, CRNA, DNAPCoralville, IA
Chuck Biddle, CRNA, PhDRichmond, Virginia
Linda Callahan, CRNA, PhDKlamath Falls, Oregon
Nancy Gaskey-Spears, CRNA, PhDGastonbury, Connecticut
Joseph A. Joyce, CRNA, BSWinston-Salem, North Carolina
Monte Lichtiger, MDCoral Gables, Florida
Mary Jeanette Mannino, CRNA, JDLaguna Niguel, California
Maria Garcia-Otero, CRNA, PhDCoral Gables, Florida
Sandra Ouellette, CRNAWinston-Salem, North Carolina
ADVISORY BOARD
Charles Barton, MSN, MEdAkron, Ohio
Carol G. Elliott, CRNA, MPA, PhDKansas City, Kansas
Linda J. Kovitch, CRNA, MSNBedford, Massachusetts
David Lott, CRNAHollywood, Florida
Frank T. Maziarski, CRNASeattle, Washington
Charles Moss, CRNA, MSWestcliffe, Colorado
Laura Wild, CRNA, MSNPennington, New Jersey
Associate PublishersJoan McNulty Elizabeth Moya, JD
Assistant EditorLinda G. Williams
Assistant PublishersBarbara McNulty Donna Scott
Circulation AssistantsCarrie Scott Tiffany Lazarich
Myriam Montes Kimberly Gutierrez
Sponsor -Frank Moya Continuing Education Programs, LLC
Subscription Office - Editorial Office –Current Reviews® Frank Moya, M.D. 1828 S.E. First Avenue 1450 Madruga Ave Ft. Lauderdale, FL 33316 Suite 207Phone: (954) 763-8003 Coral Gables, FL 33146Fax: (800) 425-1995Email: [email protected]
AccreditationThis program has been prior approved by the American Association of Nurse Anesthetists for 26 Class A CE credits; Code Number 33803; Expiration Date May 31, 2018. Approved by Frank Moya Continuing Education Programs, LLC. Provider approved by the California Board of Registered Nursing, Provider Number CEP 1754, for 26 contact hours and Florida Board of Nursing, Provider Number FBN 2210 for 26 contact hours. In Accordance with AANA directives, you must get 80% of the answers correct to receive one credit for each lesson and if there is a failure, there is no retaking.
Disclosure PolicyFrank Moya Continuing Education Programs, LLC, in accordance with the Accreditation Council for the Continuing Medical Education’s (ACCME) Standards for Commercial Support, will disclose the existence of any relevant financial relationship a faculty member, the sponsor or anyone else who may be in a position to control the content of this Activity has with any commercial interest. BEFORE STARTING, PLEASE SEE LAST PAGE OF LESSON TO READ WHETHER THERE ARE ANY RELEVANT RELATIONSHIPS TO DISCLOSE AND, IF SO, THE DETAILS OF THOSE RELATIONSHIPS.
Current Reviews® is intended to provide it’s subscribers with information that is relevant to anesthesia providers. However, the information published herein reflects the opinions of it’s authors and does not represent the views of Current Reviews in Clinical Anesthesia®, Current Reviews for Nurse Anesthetists®, or Frank Moya Continuing Education Programs, LLC. Anesthesia practitioners must utilize their knowledge, training and experience in their clinical practice of anesthesiology. No single publication should be relied upon as the proper way to care for patients. The information presented herein does not guarantee competency or proficiency in the performance of procedures discussed.
Copyright 2016 by Current Reviews®. Reproduction in whole or in part prohibited except by written permission. All rights reserved. Information has been obtained from sources believed to be reliable, but it’s accuracy and completeness, and that of the opinions based therein are not guaranteed. Printed in U.S.A. Current Reviews® is published biweekly by Current Reviews®, 1828 S.E. First Avenue, Ft. Lauderdale, FL 33316. POSTMASTER: Send address changes to Current Reviews®, 1828 S.E. First Avenue, Ft. Lauderdale, FL 33316 or email [email protected].

Curr Rev Nurs Anesth 39(17):221-232, 2016 223
LESSON OBJECTIVES
Upon completion of this lesson, the reader
should be able to:
1. Discuss factors that contribute to the
growth of anesthesia support in endo-
scopy units.
2. List new endoscopic procedures.
3. Define “split-dose prep” and its NPO impli-
cations.
4. Describe comorbidities that increase anes-
thesia risk during endoscopy.
5. Discuss the results of the 2011 closed
claims study on MAC anesthesia.
6. List factors that may make endotracheal
intubation safer than MAC during endo-
scopic procedures.
7. Explain how a venous air embolism can
occur during an endoscopic retrograde
cholangiopancreatography (ERCP).
8. Describe post-ERCP pancreatitis and pos-
sible interventions to reduce this compli-
cation.
9. Discuss elements of a computer-assisted
personalized sedation (CAPS) device.
10. Identify the administrative and practice
recommendations from the ASA if the
SEDASYS System is to be used in a facil-®
ity.
Anesthesia forEndoscopic Procedures
Terrence L. Trentman, MDDepartment of Anesthesiology
Mayo Clinic ArizonaPhoenix, Arizona
Current Reviews for Nurse Anesthetists designates this lesson ®
for 1 CE contact hour in pharmacology/therapeutics.
IntroductionAnesthesia providers are increasingly being asked toprovide services for endoscopic procedures performedby gastroenterologists. The majority of these pro-cedures are performed in an outpatient setting,although many hospitals have an endoscopy unitthat serves both in- and outpatients. Across thecountry, non-operating room anesthesia (NORA)cases have grown substantially in recent years. Atthe author’s institution, NORA cases now constituteapproximately 30% of the anesthesia department’swork by case volume (although not necessarily byminutes of anesthesia time). The gastrointestinal(GI) endoscopy unit is the largest driver of thisNORA case growth, with significant growth also seenin interventional radiology and the cardiology/elec-trophysiology lab.
The growth in anesthesia endoscopy practice hasbeen driven by many factors, including the develop-ment of new and lengthy endoscopic procedures thatrequire more than moderate sedation, the desire andexpectation of many patients that they will be com-pletely “out” and unaware during their endoscopicprocedure, and the increasingly common opiate toler-ant/difficult to sedate patient. Furthermore, the useof propofol sedation by anesthesia providers haspotential advantages for patients and proceduralists,including rapid onset of and efficient recovery fromsedation, rapid discharge from the unit, and providerand patient satisfaction.
Endoscopists may be (appropriately) reluctant touse propofol due to reports of adverse outcomes andthe Food and Drug Administration’s warning thatpropofol should be used only by those trained in theadministration of general anesthesia (with the excep-

224 Current Reviews for Nurse Anesthetists®
tion of the SEDASYS System, see below). There-®
fore, anesthesia providers will find themselves calledto the endoscopy unit with regularity, often to facedifficult to sedate, medically complex patients.
Based upon a review of current literature andguidelines, the discussion points in this lesson willinclude:• What are the common and newest GI endoscopic
procedures?• Should GI endoscopy patients undergo a formal
pre-anesthetic medical evaluation?• What are the risks of sedating patients in the GI
endoscopy unit?• How does the endoscopy physical facility con-
tribute to anesthesia challenges?• What are anesthesia technique considerations
for endoscopic procedures?• Is sedation with propofol always preferable to
general endotracheal anesthesia (GETA)?• What is a computer-assisted personalized seda-
tion (CAPS) device?
There is the risk that medically complex
patients will appear for endoscopic pro-
cedures with very little warning for the
anesthesia team.
Old and NewEndoscopic Procedures
Screening colonoscopy is the most common procedurecarried out in endoscopy units. This procedure,which is now recommended for patients over 50 yearsof age, is frequently performed under minimal ormoderate sedation directed by the endoscopist,without the need for an anesthesia provider’s assis-tance. Colonoscopy is performed to screen for pre-cancerous polyps, ulcers, diverticuli, and areas ofbleeding or inflammation. Upper endoscopy (EGD,esophagogastroduodenoscopy) is also commonly per-formed under moderate sedation and is used toscreen for upper GI/esophageal scarring (Barrett’sesophagus) from gastroesophageal reflux disease(GERD), strictures, hiatal hernias, and stomach andduodenal abnormalities including bleeding sources.
Endoscopic technical advances now allow com-plex procedures (Table 1) to be carried out in theendoscopy suite, including radiofrequency or cryo-ablation of Barrett’s esophagus, ultrasound examina-tions and fine needle aspiration (biopsies), stentplacement, dilation of strictures and endomucosalresections of lesions or polyps (EMR). Other recentdevelopments include closure of tracheo-esophagealfistula, drainage of pancreatic pseudocysts and per-cutaneous endoscopic gastrostomy tube placement.In some instances, endoscopic procedures haveobviated the need for open surgical proce-dures.
Endoscopic retrograde cholangiopancreatography(ERCP) is performed in the semi-prone or lateralposition and includes visualizing the bile ducts,pancreatic duct and gallbladder. Patients with bileduct stones, liver failure/previous liver transplant,cholangiocarcinoma, pancreatic cancer or cholestaticliver disease (e.g., primary sclerosis cholangitis)undergo ERCP with frequent repeat exams for re-evaluation and stent changes. Although these pro-cedures can theoretically be performed with moder-ate or deep sedation, at the author’s institution theyare almost always done with GETA due to the lengthof the procedure and positioning.
Double balloon enteroscopy (DBE, or “push-pullenteroscopy”) is a technique used to extend thelength of bowel that can be visualized during anendoscopic procedure. It can be performed via anantegrade (through the mouth to small bowel) orretrograde (large bowel to ileum) approach. Thetechnique involves using a balloon at the end of theenteroscope plus a proximal overtube, also fittedwith a balloon. The overtube fits outside (over) theenteroscope. The bowel is examined for lesions suchas GI bleed sites with the distal enteroscope camera.Then, the distal balloon is inflated and the scope(and bowel) is pulled back to the overtube, at whichtime the overtube balloon is inflated and the distalballoon is deflated. The distal scope is then ad-vanced and the process is repeated. In essence, thebowel is progressively pleated over the endo-scope. General anesthesia is usually considered forantegrade procedures due to the shared airway andduration of the process; shorter retrograde proce-dures may be accomplished with moderate or deepsedation.
A related topic is NPO guidelines for endoscopicprocedures. While standard guidelines regardingNPO for solids apply, liquid bowel prep is often pre-
Table 1
Complex Endoscopic Procedures
# Ablation of Barrett’s esophagus
# Endoscopic retrograde cholangio-
pancreatography (ERCP)
# Endoscopic ultrasound with
biopsies
# Double balloon enteroscopy (DBE,
or “push-pull enteroscopy”)
# Dilation of strictures; stent
placement
# Endomucosal resection of lesions
# Closure of tracheo-esophageal
fistula
# Drainage of pancreatic pseudocysts
# Percutaneous endoscopic
gastrostomy tube placement

Curr Rev Nurs Anesth 39(17):221-232, 2016 225
scribed for patients undergoing lower endoscopy.The prep may consist of 4 liters of clear liquid con-sumed the night before the planned procedure. How-ever, there is data to show improved bowel cleansingwhen a “split-dose prep” is used, meaning that thepatient drinks 2-3 liters of prep the night before andthe remaining prep solution the morning of the pro-cedure. This may create a scenario where an anes-thesia sedation patient has consumed a large volumeof liquid 1-2 hours before the planned procedure.
It is noteworthy that in a study of 712 EGD/colonoscopy patients with otherwise normal GImotility (no bowel obstruction or gastric resection, nogastroparesis history), there were no increasedgastric volumes seen in those who received a split-dose prep technique (Huffman et al., 2010). None-theless, at the author’s institution we advise that thepatients complete their split-dose at least 4 hoursbefore the planned sedation, and that patients atrisk for slowed gastric emptying follow standardNPO guidelines (e.g., NPO after midnight).
An analysis suggested that inadequate
monitoring and unrecognized over seda-
tion were significant contributors to ad-
verse events.
Pre-anesthesia Evaluationfor Endoscopic Procedures
Although GI endoscopic procedures are not typicallyassociated with significant blood loss or fluid shifts,the required anesthetic is associated with risk andsome patients will benefit from a pre-anestheticevaluation. Furthermore, in contrast to surgicalprocedures where the surgeon has almost alwaysseen the patient before the day of surgery and per-formed a history and physical, endoscopy patientsmay present for their procedure having never prev-iously met the endoscopist.
Although there is no simple answer to this pro-blem, anesthesia providers can be proactive andshare concerns and criteria with endoscopists andreferring physicians. Patients with significanthistories of ischemic heart disease, heart fail-ure, obstructive/reactive lung disease, renalfailure, diabetes and morbid obesity shouldbe identified before the day of the procedure.Some of these patients may not be good candidatesfor endoscopy at a free-standing, ambulatory center;but rather, they should be cared for at a hospital-based unit.
At a minimum, an anesthesia provider can con-tact the patient before the day of the procedure toscreen for significant co-morbidities and anesthesiarisks. Each organization must develop work flows toaddress the pre-anesthetic evaluation, with patientsafety as the focus. At the author’s institution, endo-
scopy nurses screen the histories along with theendoscopist, and sicker patients are sent to ourPreoperative Evaluation Clinic.
Risks of Sedation in Endoscopy
A 2011 review of the Closed Claims Databasehighlighted some of the risks associated with moni-tored anesthesia care (MAC), including NORA/endo-scopic procedures. The authors noted that after the2000s, MAC anesthesia cases represented 10% of theclosed claims, with 21% of the MAC claims related torespiratory depression, and 38% of the MAC claimsdue to death. Further, patient factors of concernincluded obesity, advanced age, and ASA classifi-cation 3-4.
A later population-based study by Cooper et al(2013) reviewed over 35,000 patients who underwentcolonoscopy with anesthesia assistance. The authorssearched for complications including aspirationpneumonia, bowel perforation and splenic injury.They found an overall low rate of complications(0.17%), but adverse events were more commonwith anesthesia assistance. For instance, aspirationoccurred in 173 of the anesthesia patients (0.14%) vs.0.10% of non-anesthesia cases, p=0.02. Althoughthese percentages are small, they suggest thatairway impairment associated with anesthesiadrugs (notably deep sedation with propofol)can contribute to adverse respiratory events.Similar to the closed claims analysis, the authorsfound that older patients (> 70 years) and the pre-sence of comorbidities increased the risk of compli-cations (Table 2).
Microaspiration may also occur during endo-scopic procedures, which may manifest as coughing.El Chafic et al (2012) showed that cough was morecommon during endoscopic procedures performedwith propofol sedation. In this study, cough was alsomore common in upper endoscopy (P < 0.0001), non-smokers (P = 0.05), and longer procedures (P =0.0001). Oxygen desaturation was uncommon (4%)but only occurred during deep sedation (P = 0.02).Finally, other notable complications include oxygen
Table 2
Comorbidities that Contribute
to Risk in Endoscopy
# Morbid obesity
# Advanced age
# ASA physical status of 3-4
# Ischemic heart disease
# Heart failure
# COPD
# Renal failure
# Diabetes
226 Current Reviews for Nurse Anesthetists®
desaturation, hypotension and hypertension, andvenous air embolism (VAE). The likely mechanismof VAE in this context is dissection of air from theendoscope via the bile ducts into a hepatic vein, andfrom there into the central circulation.
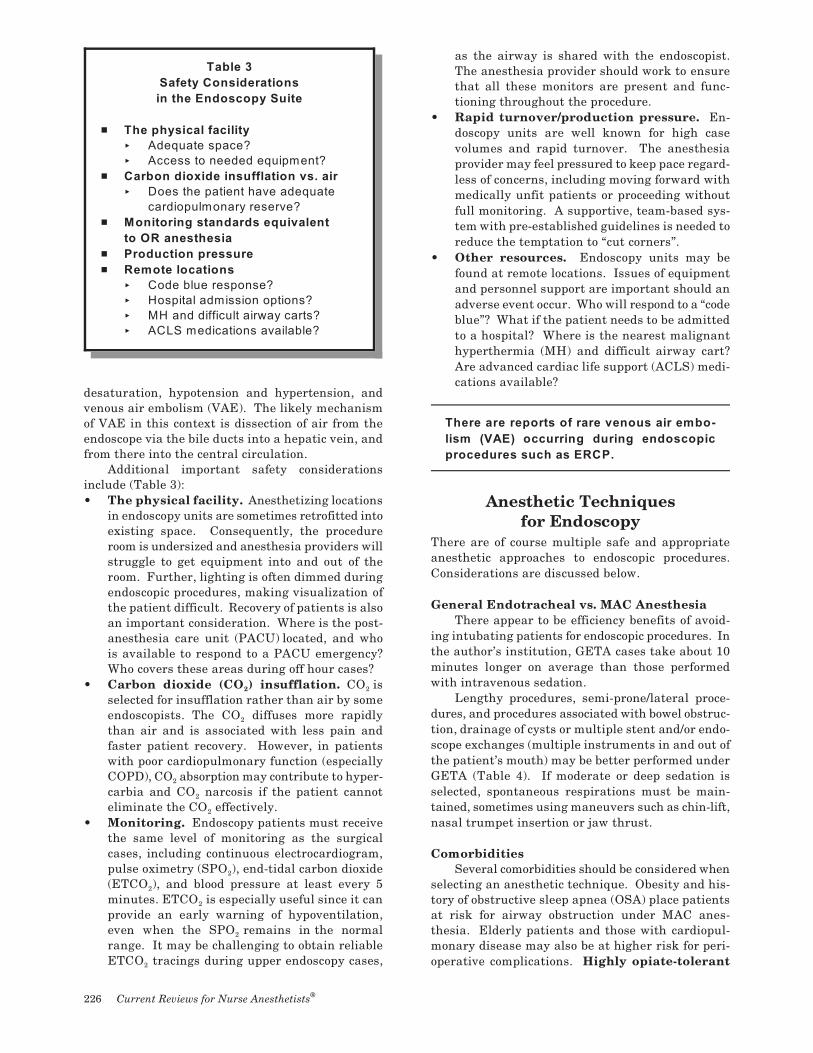
Additional important safety considerationsinclude (Table 3):• The physical facility. Anesthetizing locations
in endoscopy units are sometimes retrofitted intoexisting space. Consequently, the procedureroom is undersized and anesthesia providers willstruggle to get equipment into and out of theroom. Further, lighting is often dimmed duringendoscopic procedures, making visualization ofthe patient difficult. Recovery of patients is alsoan important consideration. Where is the post-anesthesia care unit (PACU) located, and whois available to respond to a PACU emergency?Who covers these areas during off hour cases?
2 2• Carbon dioxide (CO ) insufflation. CO isselected for insufflation rather than air by some
2endoscopists. The CO diffuses more rapidlythan air and is associated with less pain andfaster patient recovery. However, in patientswith poor cardiopulmonary function (especially
2COPD), CO absorption may contribute to hyper-2carbia and CO narcosis if the patient cannot
2eliminate the CO effectively.• Monitoring. Endoscopy patients must receive
the same level of monitoring as the surgicalcases, including continuous electrocardiogram,
2pulse oximetry (SPO ), end-tidal carbon dioxide2(ETCO ), and blood pressure at least every 5
2minutes. ETCO is especially useful since it canprovide an early warning of hypoventilation,
2even when the SPO remains in the normalrange. It may be challenging to obtain reliable
2ETCO tracings during upper endoscopy cases,
as the airway is shared with the endoscopist.The anesthesia provider should work to ensurethat all these monitors are present and func-tioning throughout the procedure.
• Rapid turnover/production pressure. En-doscopy units are well known for high casevolumes and rapid turnover. The anesthesiaprovider may feel pressured to keep pace regard-less of concerns, including moving forward withmedically unfit patients or proceeding withoutfull monitoring. A supportive, team-based sys-tem with pre-established guidelines is needed toreduce the temptation to “cut corners”.
• Other resources. Endoscopy units may befound at remote locations. Issues of equipmentand personnel support are important should anadverse event occur. Who will respond to a “codeblue”? What if the patient needs to be admittedto a hospital? Where is the nearest malignanthyperthermia (MH) and difficult airway cart?Are advanced cardiac life support (ACLS) medi-cations available?
There are reports of rare venous air embo-
lism (VAE) occurring during endoscopic
procedures such as ERCP.
Anesthetic Techniquesfor Endoscopy
There are of course multiple safe and appropriateanesthetic approaches to endoscopic procedures.Considerations are discussed below.
General Endotracheal vs. MAC AnesthesiaThere appear to be efficiency benefits of avoid-
ing intubating patients for endoscopic procedures. Inthe author’s institution, GETA cases take about 10minutes longer on average than those performedwith intravenous sedation.
Lengthy procedures, semi-prone/lateral proce-dures, and procedures associated with bowel obstruc-tion, drainage of cysts or multiple stent and/or endo-scope exchanges (multiple instruments in and out ofthe patient’s mouth) may be better performed underGETA (Table 4). If moderate or deep sedation isselected, spontaneous respirations must be main-tained, sometimes using maneuvers such as chin-lift,nasal trumpet insertion or jaw thrust.
ComorbiditiesSeveral comorbidities should be considered when
selecting an anesthetic technique. Obesity and his-tory of obstructive sleep apnea (OSA) place patientsat risk for airway obstruction under MAC anes-thesia. Elderly patients and those with cardiopul-monary disease may also be at higher risk for peri-operative complications. Highly opiate-tolerant
Table 3
Safety Considerations
in the Endoscopy Suite
# The physical facility
< Adequate space?
< Access to needed equipment?
# Carbon dioxide insufflation vs. air
< Does the patient have adequate
cardiopulmonary reserve?
# Monitoring standards equivalent
to OR anesthesia
# Production pressure
# Remote locations
< Code blue response?
< Hospital admission options?
< MH and difficult airway carts?
< ACLS medications available?

Curr Rev Nurs Anesth 39(17):221-232, 2016 227
patients may be difficult to sedate, while simul-taneously suffering from GI dysmotility (the“narcotic bowel syndrome”). Patients for EGDare likely to have reflux symptoms; cancer patientsmay suffer from bowel obstruction with associatedfood retention. If an esophageal stent is planned, theanesthesia provider should assume the patient hasretained food proximal to the obstruction; there isalso the risk of reflux when the stricture is opened.
Painful InterventionsWhile most endoscopic procedures are not pain-
ful, including post-procedure pain, there are a fewnoteworthy exceptions. Ablation of Barrett’s esoph-agus can be uncomfortable, including post-proceduresubsternal burning. Biliary stent placement is some-times associated with post-procedure right upperquadrant pain, and air insufflation can cause abdom-inal distension and discomfort.
Single vs. Multi-drug AnesthesiaPropofol can be used as a single drug for mod-
erate or deep sedation or for general anesthesia forendoscopic procedures. It has advantages of rapidonset of sedation, rapid recovery and easy titration inmost patients. Further, it has anti-emetic effects.Arguably, propofol is an ideal agent for short, mini-mally painful outpatient endoscopic procedures. Ifthe patient is opiate tolerant and/or undergoinga painful procedure, such as ablation of Barrett’sesophagus, small doses of fentanyl, remifentanil orketamine can be added to the propofol.
Other Anesthesia ConsiderationsTopical anesthesia can be used on the upper
airway to ease insertion of the endoscope. Althoughnot routine because of the risk of tachycardia,glycopyrrolate can be used to reduce secretions andimprove the effectiveness of topical anesthetics.Midazolam can be used to reduce pre-procedureanxiety as well as a part of a multi-drug anesthetictechnique. Dexmedetomidine has been used duringendoscopic procedures; while this centrally actingalpha-2 agonist provides sedation, improved patient
acceptance of the endoscope and some analgesia, it isnot rapidly titratable and usually requires othermedications (e.g., midazolam) to increase amnesia.Acetaminophen (PO or IV) and anti-inflammatories(such as ketorolac) can be considered for painfulprocedures, and 5-HT3 antagonists for their anti-emetic effect.
Balanced against efficiency are concernsover patient positioning and a sharedairway.
Post-procedure Considerations
After endoscopic procedures, patients may have com-mon complaints like nausea, esophageal or abdom-inal discomfort. Less common but more seriousevents include perforation of bowel, bleeding orsepsis. Excellent communication with the procedur-alist is needed to identify and preempt these com-plications if possible. Some patients may require anextended observation period in recovery or evenadmission to a hospital (Table 5).
ERCP can result in acute pancreatitis or sepsis.Post-ERCP pancreatitis occurs in 1-10% of cases,although some reports note an even higher incidence.Pancreatitis is identified by post-procedure painand elevated serum amylase requiring hospitaladmission. A number of endoscopic techniques havebeen employed to reduce this complication; medi-cal therapy that the anesthesia team can use in-cludes prophylactic administration of antibiotics andanti-inflammatory drugs (indomethacin, diclofenacsodium).
Computer-assisted PersonalizedSedation (CAPS) Devices
In 2013, the FDA approved for use the SEDASYS®
System (Ethicon Endo-Surgery, Inc.). The SEDASYSis a CAPS device approved to deliver propofol seda-tion to healthy (ASA 1-2) adults during upper (esoph-ageal) and lower (colon) cancer screenings. Themanufacturer states the device should not be used(and has not been studied) in patients < 18 years old,
Table 4
Frequent Indications
for Endotracheal Intubation
# Lengthy procedure
# Semi-prone/lateral position
# Bowel/esophageal obstruction
# Drainage of cysts
# Multiple stent exchanges
# Comorbidities
< Morbid obesity
< Obstructive sleep apnea (OSA)
Table 5
Post-endoscopy Considerations
# Nausea and vomiting
# Abdominal pain from insufflated
gases
# Bowel perforation
# Splenic rupture
# Sepsis
# Acute pancreatitis
228 Current Reviews for Nurse Anesthetists®
patients wearing a fentanyl patch, patients with anabnormal airway or sleep apnea, gastroparesis, bodymass index > 35, patients undergoing both colon-oscopy and EGD during the same visit, or emergentprocedures.
The device uses patient sensors, including blood2 2pressure, EKG, SPO , exhaled CO and response to
verbal commands to control the rate of propofol andoxygen delivery to achieve moderate (not deep) seda-tion. The system calculates a bolus dose of propofolthat is delivered over 3 minutes, and then delivers amaintenance infusion, usually between 25-75 mcg/kg/min. The clinician can administer additionalboluses of propofol via the device, and an initial bolusof fentanyl three minutes before initiating propofol.SEDASYS does not increase the propofol infu-sion rate; this can only be determined by theclinician. SEDASYS will decrease or suspend theinfusion based upon patient response and physiologicparameters.
As shown in the pivotal study (see Pambianco etal, 2011), the use of the SEDASYS system wasassociated with unintentional episodes of deep seda-tion or general anesthesia (i.e., no response ornon-purposeful response to painful stimulation). Ifevents like this occurred during a well-controlled(pivotal) trial, it is reasonable to assume that suchevents would happen in daily clinical practice aswell.
The American Society of Anesthesiologists (ASA)and American Association of Nurse Anesthetists(AANA) have commented on CAPS devices includingSEDASYS. They point out that machines cannotreplace skilled clinicians, and that emergencies canand do occur during routine endoscopy cases, even inhealthy patients.
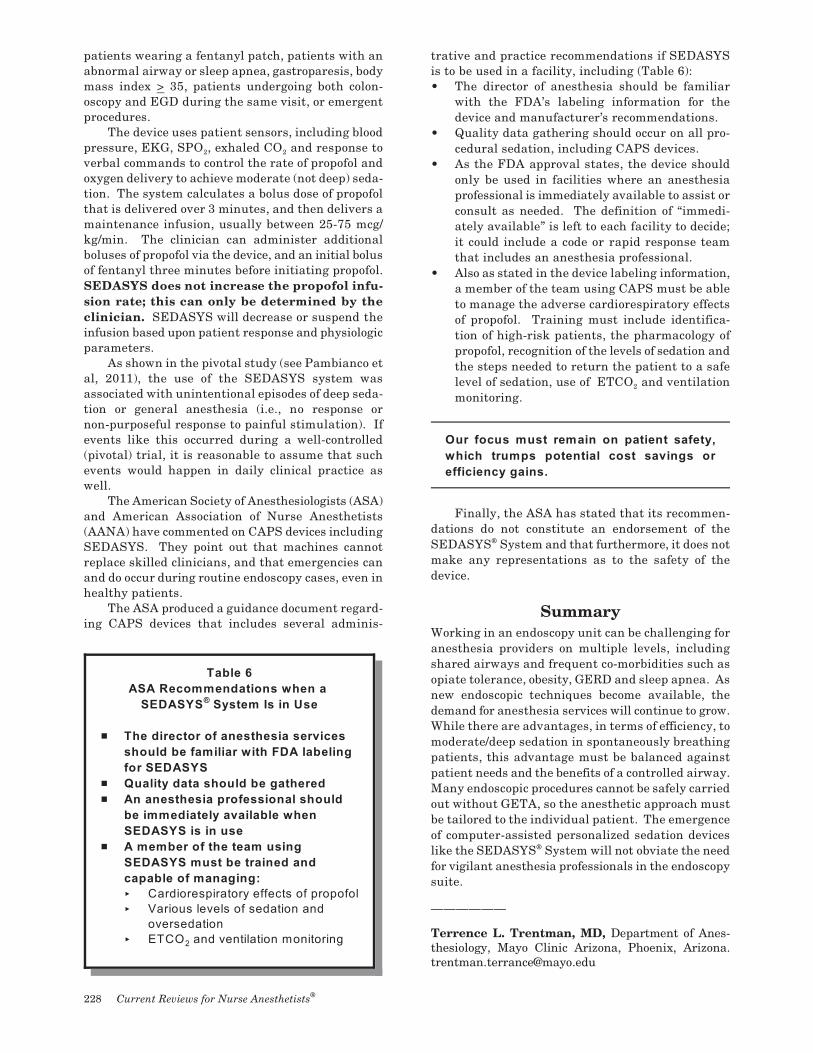
The ASA produced a guidance document regard-ing CAPS devices that includes several adminis-
trative and practice recommendations if SEDASYSis to be used in a facility, including (Table 6):• The director of anesthesia should be familiar
with the FDA’s labeling information for thedevice and manufacturer’s recommendations.
• Quality data gathering should occur on all pro-cedural sedation, including CAPS devices.
• As the FDA approval states, the device shouldonly be used in facilities where an anesthesiaprofessional is immediately available to assist orconsult as needed. The definition of “immedi-ately available” is left to each facility to decide;it could include a code or rapid response teamthat includes an anesthesia professional.
• Also as stated in the device labeling information,a member of the team using CAPS must be ableto manage the adverse cardiorespiratory effectsof propofol. Training must include identifica-tion of high-risk patients, the pharmacology ofpropofol, recognition of the levels of sedation andthe steps needed to return the patient to a safe
2level of sedation, use of ETCO and ventilationmonitoring.
Our focus must remain on patient safety,
which trumps potential cost savings or
efficiency gains.
Finally, the ASA has stated that its recommen-
dations do not constitute an endorsement of theSEDASYS System and that furthermore, it does not®
make any representations as to the safety of thedevice.
Summary
Working in an endoscopy unit can be challenging foranesthesia providers on multiple levels, includingshared airways and frequent co-morbidities such asopiate tolerance, obesity, GERD and sleep apnea. Asnew endoscopic techniques become available, thedemand for anesthesia services will continue to grow.While there are advantages, in terms of efficiency, tomoderate/deep sedation in spontaneously breathingpatients, this advantage must be balanced againstpatient needs and the benefits of a controlled airway.Many endoscopic procedures cannot be safely carriedout without GETA, so the anesthetic approach mustbe tailored to the individual patient. The emergenceof computer-assisted personalized sedation deviceslike the SEDASYS System will not obviate the need®
for vigilant anesthesia professionals in the endoscopysuite.
——————
Terrence L. Trentman, MD, Department of Anes-thesiology, Mayo Clinic Arizona, Phoenix, [email protected]
Table 6
ASA Recommendations when a
SEDASYS System Is in Use®
# The director of anesthesia services
should be familiar with FDA labeling
for SEDASYS
# Quality data should be gathered
# An anesthesia professional should
be immediately available when
SEDASYS is in use
# A member of the team using
SEDASYS must be trained and
capable of managing:
< Cardiorespiratory effects of propofol
< Various levels of sedation and
oversedation
2< ETCO and ventilation monitoring

Curr Rev Nurs Anesth 39(17):221-232, 2016 229
References
Agostoni M et al. Adverse events during monitoredanesthesia care for GI endoscopy: an 8-year experience.Gastrointest Endosc 74:266-75, 2011.
Cooper GS et al. Complications following colonoscopywith anesthesia assistance. JAMA 173(7):551-6, 2013.
El Chafic AH, Eckert G, Rex DK. Prospective descrip-tion of coughing, hemodynamic changes, and oxygendesaturation during endoscopic sedation. Dig Dis Sci57:1899-1907, 2012.
Hauser G et al. Preventing post-endoscopic retrogradecholangiopancreatography pancreatitis: what can be
done? World Journal of Gastroenterology 21(4):1069-80, 2015.
Huffman M et al. Split-dose preparation for colon-oscopy and residual gastric fluid volume: an observa-tional study. Gastrointest Endosc 72:516-22, 2010.
Metzner J. et al. Closed claims analysis. Best Prac-tice & Research Clinical Anesthesiology 25(2):263-76,2011.
Pambianco DJ et al. Computer-assisted personalizedsedation for upper endoscopy and colonoscopy: a com-parative, multicenter randomized study. GastrointestEndosc 73(4):765-72, 2011.
Terrence L. Trentman, MD
Dr. Trentman graduated from Tulane University School of Medicine and completed an internship, anesthesiologyresidency and pain fellowship at Mayo Clinic, Rochester, Minnesota.
He now practices at Mayo Clinic in Arizona and is a member of the liver transplant team. He divides his timebetween the general operating room including ultrasound guided regional anesthesia, the endoscopy suite andthe chronic pain clinic.
Tips for your Clinical Practice: Key Points
# Medically complex patients (those with cardiac disease, lung disease, renal failure, diabetes andmorbid obesity) should be identified prior to the day of the procedure.
# Monitoring standards in the endoscopy suite must be equivalent to those utilized in the operatingroom.
# There must be procedures available for emergency situations (e.g., cardiac arrest, MH) that canarise in remote locations.
# If moderate or deep sedation is utilized, spontaneous ventilation must be maintained, even if itrequires airway access and/or instrumentation.
# There are patients and procedures that are more safely taken care of with general endotracheal
anesthesia (as compared to MAC with sedation).
# Computer-assisted personalized sedation (CAPS) devices do not eliminate the need for vigilant
anesthesia professionals in the endoscopy suite.
Monte Lichtiger, MDEditor, Current Reviews
230 Current Reviews for Nurse Anesthetists®
FRANK MOYA CONTINUING EDUCATION PROGRAMS, INC. & FACULTY DISCLOSURE
THIS AUTHOR’S AND FM CEP’S SPECIFIC DISCLOSURES:
C The author / faculty has indicated that there is no relevant financial interest or relationship with any com m ercial interest.
C The author / faculty has indicated that, as appropriate, he/she has disclosed that a product is not labeled for the use under discussion, or is still
under investigation.
C As a m atter of policy, FM CEP does not have any relevant financial interest or relationship with any com m ercial interest. In addition, all m em bers
of the staff, Governing Board, Editorial Board and CM E Com m ittee who m ay have a role in planning this activity have indicated that there is no
relevant financial interest or relationship with any com m ercial interest.
C Current Reviews is intended to provide its subscribers with information that is relevant to anesthesia providers. However, the information published
herein reflects the opinions of its authors. Anesthesia practitioners m ust utilize their knowledge, training and experience in their clinical practice
of anesthesiology. No single publication should be relied upon as the proper way to care for patients.
DESIGNATON OF SPECIFIC CONTENT AREAS:
Current Reviews for Nurse Anesthetists (CRNA) is designed to m eet the standards and criteria of the Am erican Association of Nurse Anesthetists
(AANA) for the prior-approved continuing m edical education activity, Provider-Directed Independent Study, also known as hom e study. CRNA is an
approved program provider.
CRNA has designated the lessons which m eet specific content areas such as pharm acology, H IV/AIDS, etc. However, only the Board of Nursing
of an individual State is the final authority in the determ ination of whether or not these lessons meet the State’s licensure requirem ents.

1828 SE First AvenueFort Lauderdale, FL 33316Phone: 954-763-8811 Fax: 800-425-1195www.currentreviews.com
Register Early!
43rd Annual Virginia Apgar SeminarObstetric Anesthesthesia and Care of the Newborn
March 10 - 12, 2017
Hilton Resort Walt Disney World Village, Orlando, Florida
20 Class A CE Credits
17MARK ONLY THE ONE BEST ANSWER PER QUESTION ON YOUR
ANSWER CARD. MARK THIS PAGE AND KEEP FOR YOUR RECORDS.
In accordance with AANA directives, you must get 80% of the answers correctto receive one credit for each lesson, and “if there is a failure, there is no retaking”.
POST-STUDY QUESTIONS
1. The growth of anesthesia support during endo-scopic procedures is driven by:G A. Federal law—anesthesia providers are required
to be present for these cases.G B. New and lengthy procedures that require more
than moderate sedation.G C. The SEDASYS System.®
2G D. The use of CO insufflation during endoscopy.
2. During a double balloon enteroscopy (DBE):G A. The bile and pancreatic ducts are examined and
stented.G B. Ultrasound is used to biopsy pancreatic cysts.G C. The patient is always in the prone position.G D. The bowel is essentially “pleated” over the endo-
scope to extend the length of bowel that can beexamined.
3. A “split-dose prep” is used by some endoscopistsbecause:G A. It is less expensive than standard bowel prep
techniques.G B. Gastric emptying is improved in diabetics.G C. It seems to improve the quality of bowel cleans-
ing.G D. Patients prefer to drink more prep solution in the
morning.
4. All of the following comorbidities should be iden-tified before the day of an endoscopy, EXCEPT:G A. Well-controlled hypertension.G B. Heart failure.G C. Morbid obesity.G D. Renal failure.
5. The Closed Claims study identified factors thatcontribute to adverse outcomes during MAC anes-thesia, including:G A. Patients with diet-controlled diabetes.G B. Uncooperative patients between 20-30 years of
age.G C. Inadequate monitoring and unrecognized over
sedation.G D. None of the above.
6. The most likely mechanism of venous air embolism(VAE) during endoscopic retrograde cholangiopan-creatography (ERCP) is:G A. Air bubbles administered by anesthesia through
a peripheral IV.G B. Dissection of air from a bile duct into the hepatic
veins.G C. Expansion of nitrous oxide in a closed air space.
2G D. Use of CO insufflation rather than air.
7. Which factor is the strongest indication for trachealintubation during an endoscopic procedure:G A. A patient with an obstructed esophagus, recent
consumption of solid food for esophageal stentplacement.
G B. A patient with diet-controlled diabetes for abla-tion of Barrett’s esophagus.
G C. A patient with a BMI of 28 for colonoscopy.G D. A patient for colonoscopy who takes 3 oxyco-
done (5 mg) tablets per day.
8. Post-ERCP pancreatitis:G A. Occurs in 1-10% or more of patients.G B. Is associated with elevation of serum amylase.G C. May be treated with indomethacin.G D. All of the above.
9. Elements of computer-assisted personalized seda-tion (CAPS) devices include:G A. Response to verbal commands.G B. Electroencephalograms (EEG).G C. Bispectral index (BIS) monitoring.G D. Serum lactate.
10. The ASA recommends the following if a SEDASYS®
System is to be used in a facility:G A. An anesthesia provider is physically present in
the procedure room.G B. An anesthesia provider is immediately available.G C. An anesthesia provider personally controls the
SEDASYS.G D. An anesthesia provider is available for phone
consultation.