pt ii dr. johnson summer 2001 marty jo caceres normal
TRANSCRIPT
PT II Dr. Johnson Summer 2001 Marty Jo Caceres
1
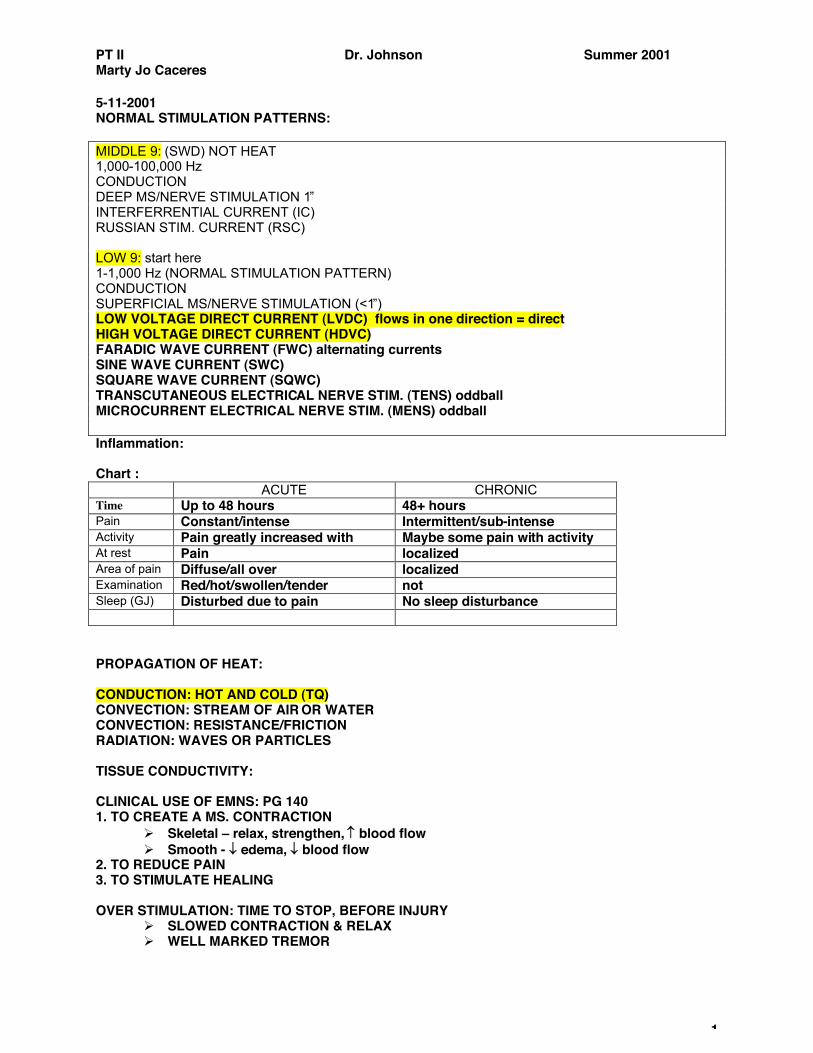
5-11-2001 NORMAL STIMULATION PATTERNS: MIDDLE 9: (SWD) NOT HEAT 1,000-100,000 Hz CONDUCTION DEEP MS/NERVE STIMULATION 1! INTERFERRENTIAL CURRENT (IC) RUSSIAN STIM. CURRENT (RSC) LOW 9: start here 1-1,000 Hz (NORMAL STIMULATION PATTERN) CONDUCTION SUPERFICIAL MS/NERVE STIMULATION (<1!) LOW VOLTAGE DIRECT CURRENT (LVDC) flows in one direction = direct HIGH VOLTAGE DIRECT CURRENT (HDVC) FARADIC WAVE CURRENT (FWC) alternating currents SINE WAVE CURRENT (SWC) SQUARE WAVE CURRENT (SQWC) TRANSCUTANEOUS ELECTRICAL NERVE STIM. (TENS) oddball MICROCURRENT ELECTRICAL NERVE STIM. (MENS) oddball Inflammation: Chart :
ACUTE CHRONIC Time Up to 48 hours 48+ hours Pain Constant/intense Intermittent/sub-intense Activity Pain greatly increased with Maybe some pain with activity At rest Pain localized Area of pain Diffuse/all over localized Examination Red/hot/swollen/tender not Sleep (GJ) Disturbed due to pain No sleep disturbance PROPAGATION OF HEAT: CONDUCTION: HOT AND COLD (TQ) CONVECTION: STREAM OF AIR OR WATER CONVECTION: RESISTANCE/FRICTION RADIATION: WAVES OR PARTICLES TISSUE CONDUCTIVITY: CLINICAL USE OF EMNS: PG 140 1. TO CREATE A MS. CONTRACTION
! Skeletal ! relax, strengthen, ! blood flow ! Smooth - " edema, " blood flow
2. TO REDUCE PAIN 3. TO STIMULATE HEALING OVER STIMULATION: TIME TO STOP, BEFORE INJURY
! SLOWED CONTRACTION & RELAX ! WELL MARKED TREMOR
PT II Dr. Johnson Summer 2001 Marty Jo Caceres
2
! PAIN, STIFFNESS, SORENESS ! "High volt DC for muscle stimulation and parlors#
FREQUENCY$S:
1-10 Hz: VASOCONSTRICTION (SMOOTH MUSCLE) 20-40 Hz: VASODILATION 40-80 Hz: MUSCLE STIMULATION (skeletal) 80+ Hz: ANALGESIA (ENKEPHALINS) (for pain) *ENDORPHINS 2-5 Hz Oddball***** 5 Hz can cause endorphins (CNS) myoneural jx tissue**** Called the "4 basic food groups of frequency# by Johnson
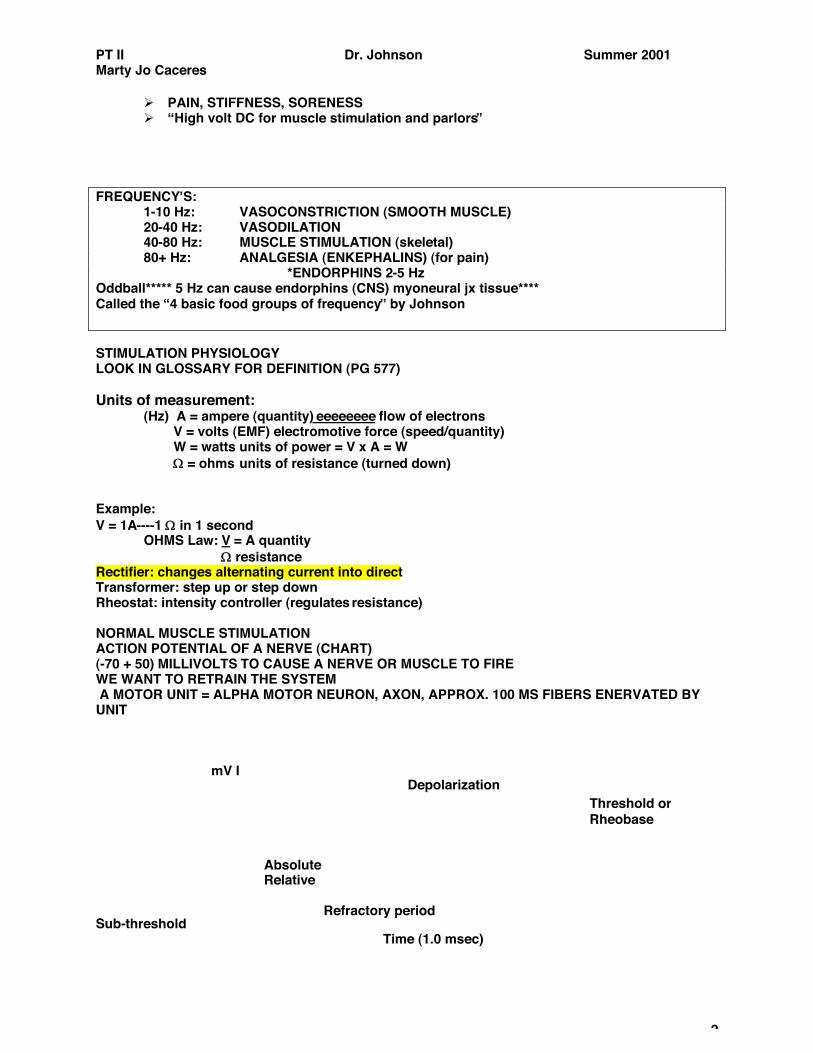
STIMULATION PHYSIOLOGY LOOK IN GLOSSARY FOR DEFINITION (PG 577) Units of measurement: (Hz) A = ampere (quantity) eeeeeeee flow of electrons V = volts (EMF) electromotive force (speed/quantity) W = watts units of power = V x A = W # = ohms units of resistance (turned down) Example: V = 1A----1 # in 1 second OHMS Law: V = A quantity # resistance Rectifier: changes alternating current into direct Transformer: step up or step down Rheostat: intensity controller (regulates resistance) NORMAL MUSCLE STIMULATION ACTION POTENTIAL OF A NERVE (CHART) (-70 + 50) MILLIVOLTS TO CAUSE A NERVE OR MUSCLE TO FIRE WE WANT TO RETRAIN THE SYSTEM A MOTOR UNIT = ALPHA MOTOR NEURON, AXON, APPROX. 100 MS FIBERS ENERVATED BY UNIT mV I Sub-threshold Time (1.0 msec)
Threshold or Rheobase
Depolarization
Absolute Relative Refractory period Repolarization time
PT II Dr. Johnson Summer 2001 Marty Jo Caceres
3
Rheostat intensity reaches max = depolarization Rheobase = minimum voltage required amount to stimulate (ALL OR NON LAW) = MS OR NERVE WILL REACT 100% IF THRESHOLD IS MET OR NOT AT ALL Johnson$s Law AKA (PREGNANCY LAW) Raymond Dubois Law: modulation of frequency ! modulation prevents accommodation Wave Train: Different pulses , Biphasic pulse continued = accommodate 1 (ms) TO DEPOLARIZE THE UNIT (Actin and Myosin to react) ABSOLUTE RP = NOT ENOUGH TO REACH DEPOLARIZATION "tapped out# (-50 to -70 mV) RELATIVE RP = Grothus & Draper: Arndt and Schultz:
! weak stimuli excite physiologic activity. Moderately ! Strong ones favor it ! Strong ones retard it ! And very strong ones retard it
Phluegers Law: CCC> ACC > AOC > COC 1000 S/S MINIMUM = once in a milli-second 1000 C/S 1000 Hz WEDENSKY INHIBITION = TOO FAST TO RECOVER FROM REFRACTORY PERIOD Applies to Middle, High and Ultra High Freq. modalities Questions to ANSWER: 1. Middle frequency$s are above 1000 ms ! INTERFERRENTIAL, RUSSIAN STIM. = NERVE AND MS STIMULATORS. 2. UV, MWD, IR, BELOW 1000 ms ! HIGH FREQUENCY$S AND ULTRA HIGH FREQUENCY$S Thursday, May 24, 2001 PT II Lecture LOW VOLT DIRECT CURRENT:
! the most difficult modality ! "the first one# ! LVDC
! LVG = low voltage group, low amperage group, low frequency (the triple lows) ! Low voltage direct current
! <150 Volts, [speed, push ,power, force] ! Galvanic [Giovanni] ! Monopolar current, one pole is ! in physiological effects and concentration then the
other, the other pole is diluted ! Monophasic [ one phase per pulse] ! 1 second ! pulse duration [criteria] to cause effect ! Make and Break ! pg. 276 fig. 7.7
! Make = open the circuit [phluegers law] spike, rush of current, then response ! Chemical and Polar properties ! pg. 293 table 7.5
! Germicidal effect ! positive anode list [correction]
PT II Dr. Johnson Summer 2001 Marty Jo Caceres
4
! "Positive pole is acidic# ! "Negative is Basic# ! Positive pole rusts metal [oxidizes] ! Positive pole = hardens, retards, dehydrates ! Negative pole = softens
! Chronic ! Cathode [negative, active] ! Anode ! Acute
Experimentation: ! Water bubble test ! Litmus paper test ! Phenolphthalein test
Anode and Cathode: Active vs. Inactive: important
! Active electrodes actively treat Pt. With physiologic effects in concentration ! Dispursive, Dilute, Inactive = will not treat Pt. [completes circuit], collects electricity,
disburse electricity, ! Polarity = the choice for the tissue needing treatment
! Electrode over pain area [positive] to ease pain, low, other end is nearby at least 18 inches within site [dispursive] negative to positive flow
! Electricity enters in through the negative pole
! Muscle atrophy ! negative pole over site to increase nerve irritability [inters negative to positive]
! ischemia ! negative pole, to inhance vasodilation
Current Density:
! How do you know you are using the correct type? ! Formula is in range: 0.5 ! 1.0 mA/square inch [Inch$] ! Peal and stick electrodes; 2x2= 4, 1x1 = 1, 3x3 = 9 ! ! Examples: ! 2x2 electrode + 2x2 electrode + 5 mA of amperage = 5 mA through patient and back
into the machine ! Active electrode 2x2 + 3x3 inactive electrode = 3 mA will only treat 2x2 site [active]
but not the inactive electrode ! Higher then the pad$s expectations will destroy the pad
LVDC comes in two currents, Continuous Mode (electrophoresis): polarity [two flavors]:
! Hydrophoresis [through water] catophoresis (-), Anaphoresis (+) ! Iontophoresis [through ions] catophoresis(-), anophoresis(+)
Use product either Na+, Ca+, Niacin as examples into tissue = zero Hz [not completed within 1 second of time, it took 20 minutes to complete.
PT II Dr. Johnson Summer 2001 Marty Jo Caceres
5
Pulse Mode: frequency [1-10 Hz, 20-40 Hz, 40-80 Hz, 80+Hz]
! Vasodilation by catophoretic ion$s, anophoretic ion$s, 4 ways with LVDC
Electrophoresis: ! Iontophoresis ! Catophoresis ! Anaphoresis ! Ions (300,301,302)
! Source, action, ! Hydrophoresis ! Penetration depth: 1-2 mm ! Current strength: 5 mA is necessary [ need correct pad 2x2 or 3x3] to drive ions for
Iontophoresis End for 5-24-01 Electrophoresis continued:
! Ions = active electrode, repels active electrode, acetate (white vinegar) acid radical production in a alkaline condition
! Scler-o-lytic = hard break, digestive enzyme ! Fibrosis, adhesive conditions, calcific conditions
! Table salt: also scerolytic, antiseptic, bactericidal
! Iodine: ludal solution, analgesics, scerolytic
Precautions: ! Allergies to ions ! Iodine-shellfish, ! Niacin- vasodilator, niacin-amide ! derivative ! Paba- rare use Pg. 302 Proteolytic enzymes ! Adolph$s meat tenderizer, scar tissue, fascia ! Solisolate, methyl-solysolate, anti-inflammatory, anti pyretic, ! DMSO ! don$t use any more
+ Ions: ! Ca+
! chloride liquid, vasodilator, chronic spasms, ! Copper +
! - indication is fungus infection*, copper sulfate, ! Magnesium + - Magnesium sulfate
! Epson salts ! Anti spasmodic analgesic, GI (runs) ! Vasodilator, ! Pg. 302 ! Zinc+ - zinc oxide ! Caustic antiseptic for fungus*
PT II Dr. Johnson Summer 2001 Marty Jo Caceres
6
Reverse Polarity: ! Treatment time: 15-20 min ! Treatment Range: up to MCL ! up to 30 mA (20-30)
! Minimum amount ! 5 mA to drive in Ions (Iontophoresis)
Indications & Contraindications ! pg. 298 (193)(140) ! use common sense
Thursday, June 07, 2001 Pg. 269-286 Pg. 287 pad placement HIGH VOLTAGE DIRECT CURRENT Definitions:
! Aka.: High voltage galvanic current ! Twin-peaked, symmetrical, Monophasic Fig.B Pg. 352
= Burning, painful, redness, itching effects that are negative SPECIFICATIONS:
! FREQUENCIES: ! %: 4 groups (Hz)
! 0-1, 1-10, 10-20,20-40, 40-60, 80+ ! V: 150+ V (adjustable to control effects)
! A: 1-1/5 mA
! &: < 100 'sec
! Polarity: (30%
! Need at least 5 mA to achieve therapy
PHYSIOLOGICAL EFFECTS:
! General effects of EMNS = (pg. 140) ! Higher penetration ! deeper then LVDC, less resistance, ! Less vasodilation ! less heat, less burn, pain, itching, redness ! Denervation (1 ms "rule#) sensor, motor, autonomic changes occur
! Human body needs "1 ms rule# need at least 1 ms artificially to keep it functional till repairs
APPLICATIONS TO HVDC:
! Bipolar (Monopolar) pad placement ! Polarity is less significant
! Pad switching rate: ! Switches pads with intensity Pg. 329 ! For active electrodes only.
! 2.5 sec.! no effectiveness ! 5.0 sec.- acute conditions ! 10.0 sec. ! chronic conditions ! 0 sec. ! cond.
! Pg. 329 fig.8.6 (bipolar) A+B= entire surface area = active = inactive
PT II Dr. Johnson Summer 2001 Marty Jo Caceres
7
! Bounces between the A and B pads = duty cycle, dispursive electrode is always on ! Frequency rate:
! 4BFG Voltage intensity:
! Patient comfort, objective stimulation ! Higher: chronic conditions ! Lower: acute conditions
Micro-interval space:
! MSI / MIS ! Similar to interpulse interval ! Range: < pulse width micro seconds ! Higher: less irritating ! Lower: more irritating
Indications / contraindications: Pg. 193-194 Read this before lab next week Thursday, June 14, 2001 Lab practical ! June 29. 2001 Class midterm ! next week-------! Chapter 8 page 323, 325, 327,328, 329, 330, 331 frequency, endorphins = 1-10 hz Pg 330 ! Tx with HVDC ! pad placement 2+ disbursement, with ice bag (not good) Pg 336 ! pad placement is Monopolar, Modality combination: USD and electrical stimulation
! HVDC most often ! Linked internally ! 316 has both USD/HVDC ! USD has sound waves to benefit the Pt. Also becomes a "fifth active electrode#
+ +
+ +
HDVC - Neg.
USD
With Gel, at same time as HVDC treatment= 5 electrodes

PT II Dr. Johnson Summer 2001 Marty Jo Caceres
8
SINE WAVE CURRENT (AC) = SWC ! Pg. 287
Definition: ! Symmetrical, biphasic pulse ! No polarity
Specifications: ! Frequency: standard groups, variable function ! Current: 1-60 mA (20-30 mA) variable by Pt. mcl ! Pulse width: 1 ms (milliseconds) fixed ! Voltage: </= 110V fixed
Types of current:
! pulsed, four different ways to use it ! Regular (pulsed) ! Surged ! a feature of modulation, changes mA: =+/- 10-15% range
= 9 mA! 10 mA! 11 mA! MIMICS THE MUSCLE UNIT Physiological effects: pg. 140
! General EMS ! Stimulates innervated, denervated ! You can make a cadaver jump
Indications/contraindications: GML (where applicable) Pg. 287 ! techniques of electrical stimulation, rules of applications END OF MATERIAL FOR 1st Test SQUARE WAVE CURRENT = SQWC DEFINITIONS:
! asymmetrical, biphasic pulse ! no polarity
Specifications:
! frequency: standard groups ! Current: 1- 60 mA ! Pulse width: microseconds ! Voltage: </= 110 Volts
Types of current:
! Pulse: 4 food groups ! Square wave current ! 1-10 ! 20-40 ! 40-80 ! 80+Hz
>Narrow wave form: ! 100 microseconds/400 microseconds
PT II Dr. Johnson Summer 2001 Marty Jo Caceres
9
+4 -1
400 ms Rule of 25% Amplitude counteracts the duration of the frequency
! Acute Tx ! Small muscles Tx
! Wide wave form:
! 300 microseconds/1200 microseconds
! Chronic case
! Large muscles cases
AC wave form: alternating current
! 400 microseconds/400 microseconds ! Immediate rise and fall ! Rehabilitation
Physiological effects;
! general EMS Indications/Contraindications: GML (where applicable) FARADIC WAVE CURRENT (AC) pg. 288
DEFINITION: ! Asymmetrical, biphasic pulse ! No polarity ! Aka,: tetanic
(door) Deinnervated / Innervated (door) SINE WAVE LVDC FARADIC WAVE SQUARE WAVE HVDC
! Electrodiagnosis (pg. 303) ED = pg. 303 ! EMG ! needle placed within nerve pathway, to Dx nerve induction ! ED ! "poor mans EMG# (a procedure with 5 digit code) ! ED will determine the RD (TQ)
! Equipment needed = pg. 304 ! LVDC and FARADIC units ! Dx after testing muscles, +3 or +4 ! Patient are in acute state due to sensory problems, after a long time of non
tx, the DTR are +1 or 0 ! Late stage is atrophy or wasting can take as little as 0-14 days later ! Refer out for an EMG or perform an ED yourself
PT II Dr. Johnson Summer 2001 Marty Jo Caceres
10
Ex: LVDC AE = - IE = + Volts = 60 Hz I = "muscle contraction# Set up on patient on belly of muscle and on muscle spindle jx As you increase the intensity you must palpate muscle for simple ms contraction. FARADIC WAVE CURRENT AE = X (0 polarity)
IE = X (Two pads of equal size) V = 60 Hz I = "muscle contraction# L R
LVDC 16 mA 11 mA FARADIC 22 mA 15 mA determines a full or partial RD
! "Reduction of muscle spasm# ! Adjust patient accordingly using modality that effected the muscle best !
Specifications:
! Frequency: 4BFG (40- 80+) ! Current: 1-60 mA ! Pulse width: 1ms ! Voltage: </= 110 V
Types of current: ! Pulsed FARADIC ! Surged FARADIC
Physiological effects: ! General EMS ! Stimulates innervated tissue only
INTERFERRENTIAL CURRENT (IFC) (middle frequency) pg. 349
" Need some form of heat therapy or cold therapy in your practice# Definition/backround ! Hans Nemec is the creator ! Aka. Heterodyne wave or pattern ! Super-position ! same body part two poles ! 2 middle frequency sine waves (4000 Hz) ! Cross and intersect each other
PT II Dr. Johnson Summer 2001 Marty Jo Caceres
11
! Example:
! Plumber with supraspinatus muscle problem IFC
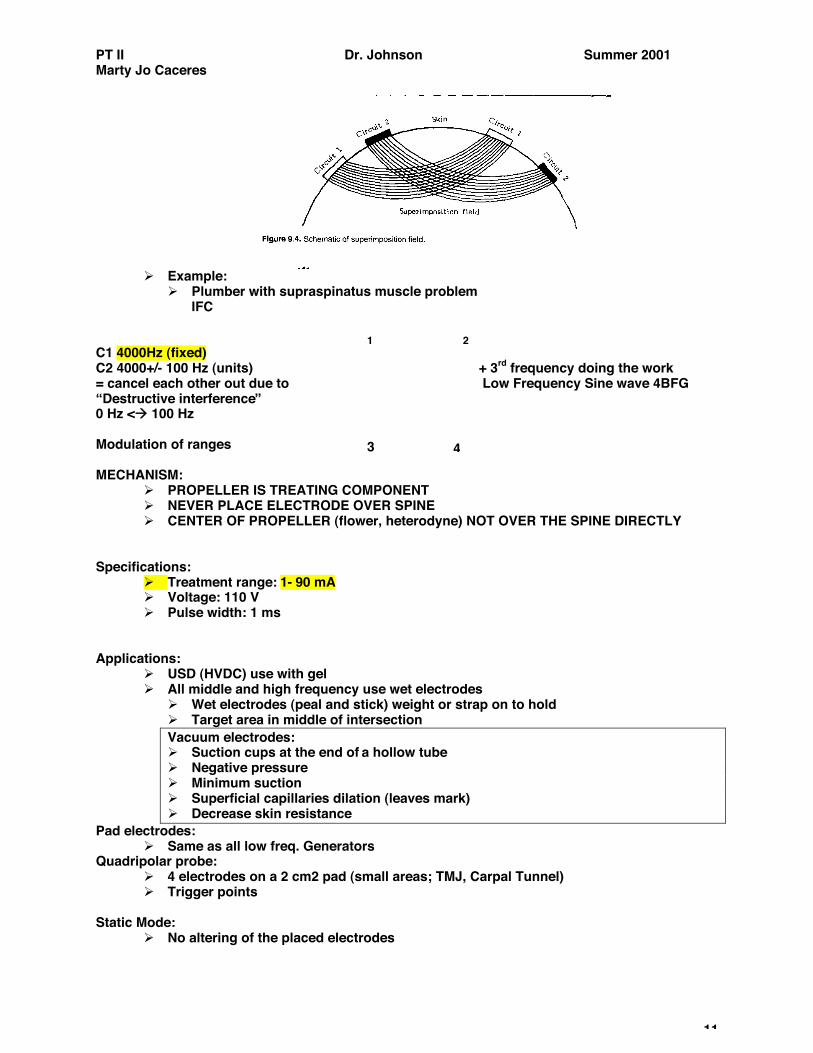
C1 4000Hz (fixed) C2 4000+/- 100 Hz (units) + 3rd frequency doing the work = cancel each other out due to Low Frequency Sine wave 4BFG "Destructive interference# 0 Hz <! 100 Hz Modulation of ranges MECHANISM:
! PROPELLER IS TREATING COMPONENT ! NEVER PLACE ELECTRODE OVER SPINE ! CENTER OF PROPELLER (flower, heterodyne) NOT OVER THE SPINE DIRECTLY
Specifications:
! Treatment range: 1- 90 mA ! Voltage: 110 V ! Pulse width: 1 ms
Applications:
! USD (HVDC) use with gel ! All middle and high frequency use wet electrodes
! Wet electrodes (peal and stick) weight or strap on to hold ! Target area in middle of intersection Vacuum electrodes: ! Suction cups at the end of a hollow tube ! Negative pressure ! Minimum suction ! Superficial capillaries dilation (leaves mark) ! Decrease skin resistance
Pad electrodes: ! Same as all low freq. Generators
Quadripolar probe: ! 4 electrodes on a 2 cm2 pad (small areas; TMJ, Carpal Tunnel) ! Trigger points
Static Mode:
! No altering of the placed electrodes
1 2
3 4
PT II Dr. Johnson Summer 2001 Marty Jo Caceres
12
! Exact tissue target area Scan Mode:
! Target tissue area is not known (buckshot tx) ! Higher volume of tissue treated ! 45 degree angle shifting (spinning on pt.)
Target mode: not all machines
! Moves central intersection target ! Dynatrone 500 machine !
Target mode: Display on machine Target seep mode:
! Moves central intersecting target in a specific pattern ! Two basic ways to use IFC
! 1: Quadpolar setup (4 pad IFC) (endogenous IFC) (IFC) above! ! 2: Premodulated (2 pad IFC) (exogenous) ! bilateral or crossed current inside the machine
! 1 2 exogenous, 0-100 Hz, two areas same machine, smaller areas ! 1 2 superficial
! or ! 1 2 endogenous, 0-100 Hz, deeper penetration, 99% of the time ! 2 1
! Indications: pg 193
! Contraindications: pg. 193-194 ! Precautions:
! High freq. Generators (4 foot rule) safe with some metal implants ! Electrodes:
! Further away the deeper the penetration
! Page 349 fig. 9.1 Russian Stimulation:
! Yadoo M. Kots-Russian Stim inventor in 1977 ! Associated with IFC ! Poly phasic wave form in a burst mode
Specifications: ! Frequency: "2500 Hz# at 50 burst pulses per second (2500 x 50 pulses per second) ! Pulse width: microseconds ! Current range: 0-90 mA (mc 20-30 mA)
1 2
2 1
PT II Dr. Johnson Summer 2001 Marty Jo Caceres
13
Mechanisms: ! Larger interburst interval ! Used for skeletal ms. stimulation only ! Muscle relaxes further (relax, recoup phase) ! More stimulating (more time to repolarize)
Conventional RS set-up: standard protocol ! 10 seconds of on time followed by 50 seconds of off time (elongated recoup time) ! Repeated for 10-15 minutes or cycles ! Variations ! middle frequency (! 1000)- user defined, for anti-edema effects (not vasoconstriction) ! EX: on 10 seconds off for 10 seconds allows ms stimulates to contract for
vasoconstriction (pumping mechanism) ! ! bi-polar (2 pads) ! ms stimulation 40-70 Hz ! Burst pulse (beat) (envelope) ! 2500 pulses per burst (polyphasic) ! followed by interpulsed interval equal or greater then pulse width ! followed by 50 bursts per second (50Hz to body) ! causes violent contraction
Indications: pg. 140, ms stim applies, 193, 194 193- indications = skeletal ms atrophy, fibromyalgia, spasm
! GML (where applicable) ! Rehabilitation, reduction, strengthening Set-up ! bi-polar pad placement, WVMC = workable viable muscle contraction ! Motor point placement and ms tendon jx near insertion ! 10 on/50 off seconds (duty cycle), 10-15 minutes duration ! use 4x4 electrodes for more accuracy
Book pg. 367
TENS = Transcutaneous electrical nerve stimulation ! Biphasic wave forms (most common) ! Symmetrical wave forms (most common) ! Asymmetrical wave forms ! Monophasic wave forms
Specifications:
! Frequency range: 1-600 Hz (in lab up to 300 Hz) ! Current Range: 1-150 mA (pt max 20-30 mA) ! Voltage range: 50-80 V (fixed) ! Pulse widths: 10-350 microseconds (100-150 ms) ! Treatment time: (20 mm ! 20 hours) not in bath, shower or sex
Mechanism:
! pg 17 through 24 for Pain, Gateway theory, etc. for "final exam# ! Block ,alter nociceptor transmission
PT II Dr. Johnson Summer 2001 Marty Jo Caceres
14
! Gate theory (synaptic inhibition) ! Endorphins (pituitary gland, terminals): Half-life: 4 hours ! Enkephalins (terminals): Half-life: 2 hours + 80+ Hz
Applications:
! Electrode pairs are over, (or) proximal to pain site or as close to spinal column (nerve root) (analgesia 80+) as close to 18 inches as possible
! Apply add. Electrodes along the radiation (same direction) Post surgery: close to incision site
! "Sandwiching effect# 0 }{ 0 each side of incision Acupuncture needles:
! Contraindicated with steroids (30 days) (BQ) ! Provide sensory and not motor stimulations (which aggravate) ! Afferent nerve de stimulators
Thursday, July 19, 2001
(4th question on lab test, five basic techniques of TENS) Types of Waves:
Square: better machine
! Less irritating ! Longer time needed ! Longer lasting effects (more endorphins, Enkephalins production) ! Chronic, hypersensitive
Spiked waves:
! More irritating ! Shorter time needed ! Shorter lasting effects ! Acute, resistant
Techniques: TENS ! Using Paresthesia ! Each one builds on previous techniques ! Technique is No better or nor worse then any of these techniques 1. Conventional TENS:
! Paresthesia (SMT) = Sub-Motoric Threshold (WVMC) ! WVMC then bring down to sub contractile threshold ! Scoliosis treatment (MT) ! children past history
! Frequency: 50 ! 100 Hz old scoliosis tx (80+ Hz now) ! Pulse width: 20- 60 microseconds ! Treatment time: 23 hrs (time off for bathing !SSS)
PT II Dr. Johnson Summer 2001 Marty Jo Caceres
15
2. Acupuncture TENS: like but not acupuncture ! Intensity at MT (irritation) ! Analgesia by Endorphins, Enkephalins (longer lasting) ! Longer time, longer lasting (! half life) ! Frequency: 1-4 Hz (point at which products released) ! Pulse width: 150 ! 250 microseconds (max out range) ! Treatment time: 20-30 minutes
3. Brief-intense TENS: ! Intensity at SMT ! Frequency : 100 Hz ! Pulse width: 150-250 milliseconds ! Treatment time: 20-30 minutes
! Ex: Intercostal neuritis, treatment for pain, Paresthesia, 4. Burst TENS: best of last two ! Intensity at SMT ! Frequencies: 70 ! 100 Hz, 1 ! 4 Hz (two freq. Out of cycle) some at 8 Hz ! Pulse width: 150 ! 250 milliseconds ! Treatment time: 20 ! 30 minutes 5. Modulated TENS: ! Intensity at SMT ! Prevents accommodation ! Varying; pulse widths, frequency ! "Clinical gem# start with "BRIEF INTENSE# TENS, If fails then use "BURST#, if this
fails use "MODULATION# ! Treatment time: 20 - 30 minutes
100% mark-up on resale of TENS units Indications:
! Pain (for that condition) ! Labor and delivery pain relief,
Step by Step procedures: 2 pads on T8
L1 remain in contact all through process
S2
Mom
97028 Physiotherapy 72000 X-rays 99000 Office visit 98000 Adjustments
Non contractions TENS
Contraction S2$s replace T8$s increase amplitude of unit
PT II Dr. Johnson Summer 2001 Marty Jo Caceres
16
Contraindications: ! GML (where applicable) pg. 309 ! Demand pacemakers ! Carotid sinus ! knocks out patient ! Pharyngeal area ! causes choking ! Undiagnosed pain - ???? don$t know what to treat
MENS: pg 381 in the book
! "stupid modality# un-substantiated claims (Johnson) ! cannot be felt, no direct effects related ! Definitions and background: Mico current Neuromuscular Electrical Stimulation ! Non union bone fractures ! Skin wounds (lesions) ! Replace tissue current, ! Uses DC & carrier frequency externally
Specifications:
! Frequency: less than 1 Hz ! Pulse width that last two seconds ! Intensity: < 500 ms (micro amps) ! No action potential acquired ! Sub-sensory & non-contractile
Applications: Pg 389 for picture of application
! Calibrated modalities (chips) ! Reads @ 100% +
read ahead on chapter 13,14 of rehab and exercise 8- 2- 2001 Thursday Exercise packet in Book Store PURPOSE/GOALS:
! IMPROVE FUNCTION ! MAINTAIN WELL BEING ! ! STRENGTH, STRETCH, COORDINATION ! PREVENT DEFORMITY/CORRECT DEFORMITIES ! "TO DO NO HARM# ("DO SOME GOOD#) ! ACCURATE DIAGNOSIS & PROGNOSIS ! TREATING CAUSES NOT THE EFFECTS ! ADDRESS THE PAIN ADHERENCE TO LAWS OF NATURE:
! DON$T RUSH ! DON$T DELAY ! ALLOW TIME TO HEAL
REALISTIC & PRACTICAL TREATMENTS: ! COMMON SENSE ! FOLLOW THROUGH & COMPLIANCE ( 3 IS MAX)
PT II Dr. Johnson Summer 2001 Marty Jo Caceres
17
> TREATMENT IS ELECTIVE, NOT AN EMERGENCY > TREAT FOR THE PATIENT-NOT JUST TO THE PATIENT
PHASE OF TREATMENT: ! CLINICAL MEDICINE & PREVENTATIVE MEDICINE ! PREVENTATIVE MEDICINE:
! 1) - PRE-PATHOGENESIS OR OPTIMUM HEALTH ! 2) & 3) ! DURING ILLNESSES
REHABILITATION:
! ULTIMATE RESTORATION ! TO MAXIMUM CAPACITY [FOR THAT PATIENT] ! PHYSICAL, EMOTIONAL, VOCATIONAL ! START AS EARLY AS POSSIBLE [ACUTE%SUB%CHRONIC] ! IN EARLY 2) PHASE THROUGH LATE 3) PHASE EXERCISE IS A VITAL TO REHAB. FULL RESTORATION MAY NOT BE ATTAINABLE-- > ORTHO. DEVICES
METHODS OF TREATMENT:
! NEED NEXT SEMESTER FOR MIDTERM ! EXCESS REST:
! TOO MUCH: o DISUSE ATROPHY, MUSCLE SORENESS, OETEOPOROSIS ! ! Ca+ EXCRETION ! DVT [WITH OR WITHOUT EMBOLISM] ! DECUBITUS ULCER ! ADHESION FORMATION ! ! EDEMA FORMATION
! PROPER REST:
! EFFECTIVE WITH EARLY AMBULATION ! " INFLAMMATION & PAIN ! ! SPEED OF HEALING
! RELATIVE REST: ! " WEIGHT BEARING LOAD ! " USUAL DAILY STRESS LOADS LONG TERM REST= 1-2 MONTHS
CLASSIFICATIONS OF RANGE OF MOTION:
! PASSIVE ROM [DURING TIME PT. HURTS] ! ACTIVE-ASSISTED ROM ! ACTIVE ROM [EXERCISES] ! ACTIVE-RESISTED ROM
PHYSIOLOGICAL EFFECTS OF EXERCISES:
TYPE 1; RED, SLOW TWITCH ! BETTER ENDURANCE ACTIVITY: ! ! MYOGLOBIN ! ! MTIOCHONDRIA ! " ATP ! ASE ! AEROBIC ACTIVITY
PT II Dr. Johnson Summer 2001 Marty Jo Caceres
18
TYPE II: WHITE FAST TWITCH ! BETTER BRIEF, INTENSE, SPRINTING ! ANAEROBIC ACTIVITY ! I & II CAN ! WITH ENDURANCE
BLOOD FLOW: ! REST: 15-20% TO MUSCLES ! 80-85% TO VISCERA ! BRAIN REMAINS CONSTANT ! WORK; REVERSE ! CUTANEOUS ! FOR HEAT RELEASE ! CUTANEOUS " FOR SHUNTING ! CORE TEMP. WILL !
STROKE VOLUME:
! LINEAR WITH WORK LOAD ! SV @ REST IS 60 ML/BEAT ! SV @ MAX IS 120 ML/BEAT
CEREBRAL FLOW REMAINS CONSTANT CO2: LINEAR WITH WORK LOAD
! @ REST ! 5 I/MIN ! @ MAX ! 20 L/MIN ! DRIVING FORCE FOR RESPIRATION
BLOOD PRESSURE:
LINEAR TO WORK LOAD ! MAX. @ 190-220 MMHG (D) ! RELATIVELY STABLE SYSTOLIC ! PULSE PRESSURE LINEAR TO WL
MUSCLE SPINDLE REFLEX: read on own GOLGI TENDON ORGAN: read on own AKA REFLEX RELAXATION, AUTOGENIC INHIBITION [BQ] TYPES OF EXERCISES:
! ROM: Active or Passive ! Due to spasm, edema, swelling, weakness ! Start with conservative types of ROM ! stretches, repetitions, set = repetitions +
break in between, ! 2x sessions/day @ 3x/session ! joints through full ROM ! Active process ! ! pain/inflammation ! gentle exercises ! !! pain/inflammation ! passive first (spastic)
Re-education exercises: relearn previously known ! Stroke patient ( daily living) Pressive resistive/strength: ! = max force load for and from the muscle ! Performed 2x /day ! Contraction for 6 seconds ( to override a GTO reflex) ! Avoid Valsalva (have patient breath) ! Ball, tubes, straps as aids ! Full body! swimming best for weight load limitations of patient
PT II Dr. Johnson Summer 2001 Marty Jo Caceres
19
! Best in/after mid-morning ( not warmed up) ! Concentric (+) ! Eccentric (-) ! Isometric (static strength):
! Best for inflamed joints ! Isotonic (dynamic strength) ! Isokinetic (no greater benefit)
! 1 RM & 10 RM = repetition maximum Prescription: average mesomorphic patient
! 3-5 lbs ! higher ! Large ! small groups ! 1 set of 8-12 reps ! No more than 12 exercises at one time (3) ! Exercise until fatigue (not past that) ! ! weight by 5% if 12 reps have been reached without trouble ! No more then 3x per week per area ! Movements slow sustained concentrated ! Warm up ! stretch! exercise ! cool down period afterwards
Endurance exercises:
! Higher reps, less weight load Co-ordination exercises:
! Relearned sites
Relaxation: ! Direct visual imaging ! Meditation
Breathing:
! Alexander technique ! Specific to their sport ! Respiratory therapists
Stretching:
! Best at 43) C ! Best in/after mid morning ! 3- 4x/day
Muscles: ! If no inflammation! vigorous stretch ! ! inflammation ! Gentle stretch ! Stretch to point of pain (beyond 2 hours) ! No inflammation into the next day (properly done)
Ligaments:
! Done gently ! Short of point of pain ! Patient totally relaxed
Muscle test grading = 0,1,2,3,4,5 (Hoppenfeld) Handout: What sections:
! pg. 423 ! Frenkel$s exercise = CB dysfunction ! Exercises while supine = "not on test#

PT II Dr. Johnson Summer 2001 Marty Jo Caceres
20
! Pg. 424 ! Exercises while seated, while standing, relaxation will be on test ! Pg. 457 Equipment = 1945 De Lorme boot (quadriceps boot) 10 reps max ! Pg. 457 Oxford technique = transfer 10 reps up ! Pg. 682 Head and spinal injuries
! Neck exercises = phase 1 and 2 ! William$s Flexion Exercises (low Back)
! Abdominal crunch ! pg. 683 chair exercises ! pg. 684 Shoulder and arm exercises ! pg. 685 Advanced rehabiitation ! GHJ dislocations ! ACJ disocations ! Pg. 689 knee and thigh ! Pg. 690 post operative ! Pg. 695 home knee exercises ! Pg. 698 calf, foot, ankle, leg ! Pg. 6 modern medicine ! Pg. 30 exercise prescriptions (walking program) ! Pg. 31 running, out door cycling ! Pg. 32 swimming
Last subject: Massage:
! Mass = to touch (Arabic) ! Massein = to knead (Greek) ! Pressure and stretching ! Legal but ! liability goes with it (done by yourself) ! Can hire a masseuse (best training) CMT
Physiological effects: pg. 140
! General heat modalities ! Not a substitute for exercises ! Will not build muscle strength
Types of massage: 1. Stroking: aka.: effleurage (French) the flower
- broad surface stroking - In one direction only, - Uncorking effect (all unidirectional) for peripheral edema due to
valvular adhesions - Opposite the flow of the vessel
2. Compression: aka petrissage, kneading, grasping, lifting, pressing, squeezing, wringing
- motion in the muscle, sections at a time, concentrate, - " adhesions - Mobilize tissue deposits
3. Friction: aka friction
- Crossing against the skin - " fibrotic nodules - " muscle spasms - " trigger points - no lotion (or very little) - Doc becomes one with the patient
PT II Dr. Johnson Summer 2001 Marty Jo Caceres
21
4. Percussion: aka Tapotement, hacking, whipping, clapping (slapping), beating, Tapping (superficial), Vibration (Deep), Cupping (respiratory dz)
- Depends on the depth of penetration, closed or open hand - Usually performed last - Invigorating
5. Application:
! Preserve the patients modesty (nude) ! Steady, smooth movements ! Stay in contact ! Reduce friction ! No mentholated, camphor gels: Smell ! Robbing blood supply from deep structures (vasodilators)
EXERCISES TO DEVELOP NEUROMUSCULAR COORDINATION: