promoting action on research · pdf fileii promoting action on research implementation in...
TRANSCRIPT

PROMOTING ACTION ON RESEARCH IMPLEMENTATION IN HEALTH
SERVICES (PARIHS) FRAMEWORK:
APPLICATION TO THE FRACTURE FIGHTERS PROGRAM
by
Vinita Anjali Bansod
A thesis submitted in conformity with the requirements for the degree of
Master of Science
Graduate Department of Health Policy, Management and Evaluation
in the University of Toronto
© Copyright by Vinita Anjali Bansod 2009

ii
PROMOTING ACTION ON RESEARCH IMPLEMENTATION IN HEALTH
SERVICES (PARiHS) FRAMEWORK:
APPLICATION TO THE FRACTURE FIGHTERS PROGRAM
Vinita Anjali Bansod
Master of Science (2009)
Department of Health Policy, Management and Evaluation
University of Toronto
ABSTRACT
The purpose of this thesis is to apply the Promoting Action on Research Implementation in
Health Services (PARiHS) framework to a provincial osteoporosis management program to
describe unit level factors that may have influenced implementation among participating
inpatient rehabilitation units. A toolbox of measures was proposed to operationalize the
frameworks elements of evidence, context and facilitation. A cross-sectional survey was
completed with clinicians responsible for championing the program and their managers. Results
demonstrated that leadership behaviours, organizational climate traits and champion behaviours
varied among practice environments indicating that attention to unit level factors outlined by the
PARiHS framework could increase the uptake of research evidence in practice. The proposed
toolbox could be utilized as a diagnostic and prescriptive tool to identify potential
implementation barriers, and guide the selection of appropriate tools/strategies to overcome
them. Furthermore, it will enable future studies to provide further empirical support for the
PARiHS framework.

iii
Acknowledgements
“Feeling gratitude and not expressing it is like wrapping a present and not giving it”
~William Arthur Ward
I would not have accomplished all that I have without the encouragement and support of several
individuals.
I have been unbelievably lucky to have Dr. Susan Jaglal as my thesis supervisor and mentor.
Susan, the level of commitment and care you show to your students is unmatched – please be
assured it has not gone unnoticed and is much appreciated. I thank you for your encouragement
and belief in me over the last two years.
I am also indebted to my committee members: Dr. Gillian Hawker, Dr. Sharon Straus and Dr.
Nancy Salbach for giving up many hours to provide me with feedback and counsel. I was
fortunate to have such a highly capable support team.
To the Fracture Fighters team, Sarah Munce, Vicky Quan, and Cathy Evans, thank you for your
willingness to provide feedback and suggestions, you were instrumental in shaping my project
ideas through every stage of my research. In addition, this project would not have been possible
without the rehabilitation unit managers and clinical staff who took time out of their busy
schedules to complete my study questionnaires.
To my professors and classmates in the Department of HPME, I am proud to be in the company
of such a well respected group. Especially, Nancy Gill and Arun Radhakrishnan, thanks for
being my sounding board over last two years. It was comforting to have great friends on this ride
with me. I will miss our Pogue Mahone sessions!

iv
Most importantly, I am grateful to have had the support of my wonderful friends and family,
especially Chantelle Antao, Andrea Goveas, Angela Lalla, Nafessa Ladha Waljee and Kelly
Roche. Dad, although we may not see eye-to-eye all the time, you have always had confidence
in me – thanks for that. Mom, thank you for your everlasting kindness and care. You are a
constant reminder that brilliance is not measured by the number of degrees one obtains but by the
quality of ones character. Finally, to Dan, I thank you for your patience, understanding and
support. Most of all, thank you for your encouragement in the moments when I felt discouraged
and frustrated, you never doubted me. Thanks for always being by my side, I couldn‘t have done
this without your love and support.
Vinita Bansod
September 2009

v
TABLE OF CONTENTS
1 CHAPTER 1: INTRODUCTION........................................................................... 1
1.1 Research Goal........................................................................................................... 4
1.2 Primary Objectives.................................................................................................. 4
1.3 Secondary Objective.................................................................................................. 4
1.4 Outline of Thesis Chapters...................................................................................... 4
2 CHAPTER 2: LITERATURE REVIEW................................................................ 7
2.1 Osteoporosis & Fractures ...................................................................................... 8
2.2 The Fracture Fighters Program............................................................................. 9
2.3 Knowledge Translation Models, Frameworks and Theories............................. 13
2.3.1 The Need to Consider Context ................................................................................... 15
2.3.2 The Need for Theory ................................................................................................. 16
2.3.2.1 Diffusion Theory – Spread of Ideas........................................................................... 18
2.3.2.2 The Ottawa Model of Research Use (OMRU)........................................................... 19
2.3.2.3 The Knowledge to Action Process Framework (KTA).............................................. 21
2.3.2.4 The Quality Enhancement Research Initiative (QUERI)........................................... 22
2.3.2.5 Promoting Action on Research Implementation in Health Services (PARiHS)
Framework................................................................................................................ 23
2.3.2.6 Selection of the KT Model for Fracture Fighters Program ........................................ 26
2.4 Summary.................................................................................................................... 27
3 CHAPTER 3: MANUSCRIPT 1 – PROPOSING A TOOLBOX OF MEASURES
FOR THE PROMOTING ACTION ON RESEARCH IMPLEMENTATION IN
HEALTH SERVICES (PARIHS) FRAMEWORK: APPLICATION TO THE
FRACTURE FIGHTERS
PROGRAM.............................................................................................................. 28
3.1 Abstract..................................................................................................................... 28
3.2 Introduction............................................................................................................... 30
3.2.1 Purpose....................................................................................................................... 34
3.2.2 Description of the Fracture Fighters Program ........................................................... 35
3.3 Operationalizing the PARiHS Framework.......................................................... 35

vi
3.3.1 Evidence..................................................................................................................... 36
3.3.1.1 Evidence Toolbox: Kitson‘s Preliminary Evidence Questions.................................. 37
3.3.2 Context....................................................................................................................... 39
3.3.2.1 Leadership.................................................................................................................. 39
3.3.2.1.1 Context Toolbox: Multifactor Leadership Questionnaire (MLQ)........................ 40
3.3.2.2 Culture......................................................................................................................... 42
3.3.2.2.1 Context Toolbox: Organizational Readiness for Change – Organizational
Climate Domain.................................................................................................... 45
3.3.2.3 Evaluation.................................................................................................................. 46
3.3.2.3.1 Context Toolbox: Fracture Fighters Process Indicators ….................................. 47
3.3.3 Facilitation.................................................................................................................. 48
3.3.3.1 Facilitation Toolbox: Opinion Leadership Scale & Champion Behaviour Measure.. 49
3.4 Discussion.................................................................................................................. 52
3.4.1 Limitations.................................................................................................................. 55
3.5 Conclusion................................................................................................................ 56
4 CHAPTER 4: MANUSCRIPT 2: LEADERSHIP, ORGANIZATIONAL
CLIMATE AND FACILITATION: A SURVEY OF INPATIENT
REHABILITATION UNITS IN ONTARIO......................................................... 57
4.1 Abstract..................................................................................................................... 58
4.2 Introduction.............................................................................................................. 60
4.3 Methods..................................................................................................................... 62
4.3.1 Assumptions of Fracture Fighters Program based on the PARiHS Framework......... 62
4.3.1.1 Fracture Fighters Evidence......................................................................................... 63
4.3.1.2 Fracture Fighters Context........................................................................................... 63
4.3.1.3 Fracture Fighters Facilitation...................................................................................... 64
4.3.2 Study Design and Procedures..................................................................................... 65
4.3.3 Setting and Participants.............................................................................................. 65
4.3.4 Measures Applied to PARiHS.................................................................................... 66
4.3.4.1 Evidence: Research, Clinical Experience and Patient Experience............................. 67
4.3.4.2 Context: Leadership Sub-Element.............................................................................. 67
4.3.4.3 Context: Climate Sub-Element................................................................................... 68
4.3.4.4 Context: Evaluation Sub-Element.............................................................................. 69
4.3.4.5 Facilitation.................................................................................................................. 69
4.3.4.6 Implementation Success Indicators............................................................................ 70
4.3.5 Statistical Analysis...................................................................................................... 71

vii
4.4 Results......................................................................................................................... 73
4.4.1 Response Summary and Demographics...................................................................... 73
4.4.2 Survey Results............................................................................................................ 75
4.4.2.1 Evidence..................................................................................................................... 75
4.4.2.1.1 Evidence Overall.................................................................................................. 75
4.4.2.2 Context: Leadership.................................................................................................... 75
4.4.2.2.1 Leadership Behaviours Overall............................................................................ 75
4.4.2.2.2 Leadership Behaviours by Inpatient Rehabilitation Unit..................................... 76
4.4.2.3 Context: Organizational Climate................................................................................ 80
4.4.2.3.1 Overall Organizational Climate............................................................................ 80
4.4.2.3.2 Organizational Climate by Inpatient Rehabilitation Unit..................................... 80
4.4.2.4 Facilitation.................................................................................................................. 82
4.4.2.4.1 Facilitation Overall.............................................................................................. 82
4.4.2.4.2 Facilitation by Inpatient Rehabilitation Unit....................................................... 82
4.4.2.5 Implementation Success............................................................................................ 82
4.4.2.5.1 Relationship between Implementation Success and PARiHS Sub-Elements...... 83
4.5 Discussion ................................................................................................................. 86
4.5.1 Limitations and Suggested Toolbox Revisions.......................................................... 90
4.6 Conclusion ................................................................................................................ 93
5 CHAPTER 5: DISCUSSION................................................................................... 94
5.1 Implications for Quantitative Applications of the PARiHS Framework............ 95
5.1.1 Organizational Climate vs. Organizational Culture.................................................... 96
5.1.2 The Context Assessment Instrument (CAI)................................................................ 96
5.1.3 The Use of the Proposed PARiHS Toolbox in Implementation Planning................. 97
5.1.4 Implementation Evaluation ....................................................................................... 99
5.2 Limitation................................................................................................................. 99
5.3 Future Directions..................................................................................................... 100
5.3.1 Provide Support for the PARiHS Framework........................................................... 100
5.3.2 Prospective Application of the PARIHS Toolbox to Guide Implementation
Planning ................................................................................................................... 101
5.4 Conclusion ............................................................................................................... 103
6 REFERENCES....................................................................................................... 104
viii
LIST OF TABLES
TABLE 1: Fracture Fighters Best-Practices on Inpatient Rehabilitation Units .......................... 10
TABLE 2: Fracture Fighters Resources........................................................................................ 12
TABLE 3: Percent of Inpatient Rehabilitation Units Implementing Selected Best-Practices.... 13
TABLE 4: The QUERI 6-step framework.................................................................................... 23
TABLE 5: PARIHS Toolbox – Adapted Evidence Questionnaire............................................... 38
TABLE 6: Leadership styles, behaviours and sample questionnaire items.................................. 42
TABLE 7: Similarities and Differences between Culture and Climate........................................ 44
TABLE 8: Culture characteristics and ORC Climate Scale Items................................................ 46
TABLE 9: Opinion Leadership Scale – Adapted to Fracture Fighters ........................................ 50
TABLE 10: The Champion Behaviour Measure – Adapted to Fracture Fighters ........................ 51
TABLE 11: Percent of Inpatient Rehabilitation Units Implementing Selected Best-Practices.... 60
TABLE 12: Demographics of Respondents................................................................................ 73
TABLE 13: Percent agreement between Coach Rating and Manager Self-Rating of Leadership
Behaviours....................................................................................................................... 79
TABLE 14: Champion Behaviour Scores For N=22 Inpatient Rehabilitation Units................... 82
TABLE 15: Success Indicators: Best Practice Implementation by Site (N=20)......................... 83
TABLE 16: Coach Reported Leadership Behaviours, Organizational Climate and Facilitation.. 84
TABLE 17: Manager Reported Facilitation ................................................................................ 84
TABLE 18: Logistic Regression Models (Successful Implementation)...................................... 85

ix
LIST OF FIGURES
FIGURE 1: Promoting Action on Research Implementation in Health Services (PARiHS)
Framework…………………….……………………………………....……………….... 2
FIGURE 2: Greenhalgh‘s Spread of Innovations Conceptual Model ……................................ 19
FIGURE 3: The Ottawa Model of Research Use........................................................................ 20
FIGURE 4: The Knowledge-to-Action Process........................................................................... 22
FIGURE 5: Promoting Action on Research Implementation in Health Services (PARiHS)
Framework…………………….…………………………………………………........... 24
FIGURE 6: Promoting Action on Research Implementation in Health Services (PARiHS)
Framework…………………….……………………………………………………….... 31
FIGURE 7: The Proposed PARiHS Toolbox................................................................................ 52
FIGURE 8: Promoting Action on Research Implementation in Health Services (PARiHS)
Framework…………………….…………………………………………………........... 62
FIGURE 9: Data Collection Tools: The PARiHS Toolbox......................................................... 66
FIGURE 10: Response Rate Flow Chart..................................................................................... 74
FIGURE 11: Mean Leadership Behaviour Scores of Inpatient Rehabilitation Managers
Compared to US (N=27,285) Normal Percentiles........................................................... 76
FIGURE 12a: Transformation Leadership Behaviours Present by Inpatient Rehabilitation Unit
(Clinical Coach Respondents)......................................................................................... 78
FIGURE 12b: Transactional Leadership Behaviours Present by Inpatient Rehabilitation Unit
(Clinical Coach Respondents)........................................................................................... 78
FIGURE 13: Organizational Climate Scores Compared to ORC Score Profiles......................... 80
FIGURE 14: Organizational Climate Traits Present by Inpatient Rehabilitation Unit............... 81

x
LIST OF APPENDICES
APPENDIX A: Fracture Fighters 6 month Follow-Up Telephone Survey
(Selected Questions)....................................................................................................... 119
APPENDIX B: Overview of Knowledge Translation Theories, Models and Frameworks........ 121
APPENDIX C: Outline of PARiHS Elements........................................................................... 135
APPENDIX D: Informed Consent Materials – Information Letters and Consent Forms.......... 137
APPENDIX E: Survey Instruments – Clinical Coach and Manager Questionnaire.................. 141
APPENDIX F: Normative values: Multifactor Leadership Questionnaire (Form 5X) and
Organizational Readiness for Change (ORC) .............................................................. 153

1
CHAPTER 1: INTRODUCTION
Knowledge translation (KT) is defined as "the exchange, synthesis and ethically-sound
application of knowledge—within a complex system of interactions among researchers and
users—to accelerate the capture of the benefits of research for Canadians through improved
health, more effective services and products, and a strengthened health care system"(Canadian
Institutes of Health Research 2009). The discipline, also referred to as knowledge exchange,
knowledge to action, research utilization, knowledge utilization and knowledge transfer, has
increased in popularity since the mid-1980‘s and 1990‘s with the rise of evidence-based
medicine (Haynes 2004). Knowledge translation spans the entire research process from the
creation of knowledge to use by decision makers (Graham et al. 2006). In the past, a significant
proportion of health research dollars have been invested in clinical research, while relatively
little attention was given to ensuring these findings were incorporated into practice (Haynes and
Haines 1998). Therefore one of the central questions posed by health services researchers is how
to close the research-to-practice ―gap‖.
To date, multiple interventions and strategies have been developed in order to increase
the likelihood that clinicians will incorporate new research into their practice. The majority of
interventions have been shown to achieve moderate improvements in care (Oxman et al. 1995;
Bero et al. 1998; Grimshaw, Thomas et al. 2004), but with considerable variation in the observed
effects across interventions(Shojania and Grimshaw 2005). Although there is a widespread
agreement that evidence implementation requires strategies to meet the needs of the individual
stakeholder (or decision maker), there is an increasing acknowledgement of the importance of
organizational context. There may be differences in the context between studies that assessed
similar interventions, since few studies provide contextual data (Eccles et al. 2005). In addition,

2
leaders in the KT field have put out a call to increase the use and development of theoretically
grounded approaches to KT with hopes that this will shed light on the ―black box‖ of
implementation research (Rycroft-Malone 2007).
A promising framework to describe implementation success in health care organizations
has been developed by Kitson and colleagues (Kitson et al. 1998). The Promoting Action on
Research Implementation in Health Services (PARiHS) framework (Figure 1) states that
successful implementation is a function of three elements: 1) evidence 2) context and 3)
facilitation. Kitson and colleagues (1998) demonstrated that the most successful implementation
occurs when: 1) the evidence is scientifically robust and matches professional consensus
and
patient needs ("high" evidence); 2) the context is receptive to change with sympathetic cultures,
strong leadership, and appropriate monitoring and feedback systems ("high" context);
and 3)
there is appropriate facilitation of change with input from skilled external and internal facilitators
("high" facilitation)(Rycroft-Malone et al. 2002). F
AC
ILIT
AT
ION
CO
NT
EX
T
EV
IDE
NC
E
Implementation Success = f (Evidence, Context, Facilitation)
RESEARCH
CLINICAL
EXPERIENCE
PATIENT
EXPERIENCE
LEADERSHIP
CULTURE
EVALUATION
PURPOSE
ROLES
SKILLS &
ATTIBUTES
Figure 1: Promoting Action on Research Implementation in Health Services Framework
The aim of this thesis is to apply the PARiHS framework to a best-practice program for
post-fracture care in inpatient rehabilitation units. In 2003, a report by the Ontario Osteoporosis

3
Action Plan Committee (OAPC) of the Ministry of Health and Long-Term Care highlighted the
importance of addressing both a diagnostic and therapeutic care gap for patients with fragility
fractures (Ontario Action Plan Committee 2003). Osteoporosis guidelines have identified prior
fracture as a significant indicator of future fractures and osteoporosis, yet the majority of at-risk
individuals are under- investigated or treated (Elliot-Gibson et al. 2004; Giangregorio et al. 2006;
Bessette et al. 2008; Papaioannou et al. 2008). In response to the OAPC report, the Ontario
Ministry of Health and Long-Term Care announced a $15 million strategy to improve
osteoporosis care in Ontario (Smitherman 2005) with a priority to improve tertiary prevention of
fractures.
Fracture Fighters, in the inpatient rehabilitation setting was one of the programs funded
through the Ontario Osteoporosis Strategy to address this recommendation, since inpatient
rehabilitation protocols frequently did not make the link between fractures and osteoporosis and
therefore lacked osteoporosis assessment and management interventions (Ontario Osteoporosis
Strategy 2009). The program used a multi-component knowledge translation strategy based on
Pathman‘s Awareness-to-Adherence model of physician behaviour change (Pathman et al. 1996).
The primary strategy used trained front line clinicians (Clinical Coaches) to facilitate integration
of osteoporosis management into existing inpatient rehabilitation services provided to patients
post-fracture in order to prevent repeat fractures. Although a survey of participating
rehabilitation units at six month follow-up demonstrated improvements across all best-practice
categories, only about half of 36 participating sites provided education about osteoporosis,
supplements and referrals for osteoporosis follow-up (Jaglal et al. 2008).
In order to increase our understanding of how to design more effective knowledge
translation strategies for programs such as Fracture Fighters, we must first identify determinants

4
of change that include consideration of contextual or unit level factors. Identifying factors that
influence implementation is essential to allowing the design of more effective strategies that are
adapted to the factors that facilitate or impede actual change (Fleuren et al. 2004).
1.1 RESEARCH GOAL
The goal of this study is to apply the Promoting Action on Research Implementation in
Health Services (PARiHS) framework to the Fracture Fighters program to describe unit level
factors that may have influenced best-practice implementation.
1.2 PRIMARY OBJECTIVES
1. To propose a toolbox of measures to operationalize the PARiHS framework
2. To apply these measures to the Fracture Fighters program to describe:
a. leadership behaviours of inpatient rehabilitation managers
b. the organizational climate of participating rehabilitation units
c. the facilitation behaviours of Clinical Coaches
1.3 SECONDARY OBJECTIVE
3. To describe the relationship between leadership behaviours, organizational climate, and
facilitation traits among successful and unsuccessful units
1.4 OUTLINE OF THESIS CHAPTERS
This thesis is organized into the following five chapters:
Chapter 1: Introduction

5
This introductory chapter identifies the problem. The study goal and specific objectives
are listed.
Chapter 2: Literature Review
This chapter describes the persistent research-to-practice gap in osteoporosis
management and reviews a number of knowledge translation theories that could be applied to
explain research implementation in clinical practice. The chapter focuses on theories, models and
frameworks that are inclusive of contextual factors and describes why the Promoting Action on
Research Implementation in Health Services (PARiHS) framework was suited to examine
implementation issues of the Fracture Fighters inpatient rehabilitation best practice program.
Chapter 3: Manuscript 1 – Proposing A Toolbox of Measures for the Promoting Action on
Research Implementation in Health Services (PARiHS) Framework: Application to the
Fracture Fighters Program
This manuscript discusses the PARiHS elements of evidence, context and facilitation
with the goal of operationalizing the framework for evaluating the Fracture Fighters Program.
Each element and sub-element is discussed and appropriate measurement instruments are
selected to quantify each element and sub-element. A toolbox of measures is assembled into a
questionnaire to apply the PARiHS framework to Fracture Fighters.
Chapter 4: Manuscript 2 – Leadership, Organizational Climate and Facilitation: A Survey
of Inpatient Rehabilitation Units in Ontario
This chapter is also written in manuscript format. Based on the toolbox assembled in
Chapter 3, survey questionnaires were completed with unit managers and clinical coaches

6
participating in the Fracture Fighters program to describe implementation success, leadership,
organizational climate and facilitation. Results suggest that there are potential differences in
leadership, organizational climate and facilitators between organizations who were successful in
implementing Fracture Fighters best-practices and those who were not.
Chapter 5: Discussion
This final chapter reports a synthesis of the results presented in Chapter 3 & 4 and the
implications for quantitative applications of the PARiHS framework. Specifically, implications
for use of the proposed PARiHS toolbox as a diagnostic and prescriptive tool for barrier
identification and tailoring during implementation planning and as a tool for evaluating
implementation of evidence in organizations are discussed. The discussion also includes
commentary on the limitations of this approach and suggestions for future research.

7
CHAPTER TWO: LITERATURE REVIEW
This chapter describes the persistent knowledge-to-practice gap in osteoporosis care for patients
post-fracture and reviews a number of knowledge translation theories that could be applied to
explain research implementation in clinical practice. The chapter focuses on theories, models and
frameworks that are inclusive of contextual factors and describes why the Promoting Action on
Research Implementation in Health Services (PARiHS) framework was suited to examine
implementation issues of the Fracture Fighters inpatient rehabilitation best practice program.

8
2.1 OSTEOPOROSIS & FRACTURES
Osteoporosis is a skeletal disease that affects one in four women and one in eight men
over the age of 50 in Canada (Hanley and Josse 1996). The disease is characterized by a
reduction in bone mass, and changes to bone structure, causing a decline in bone strength,
making individuals with the disease more susceptible to fractures (Cummings and Melton 2002 ).
Fragility or low trauma fractures, most commonly in the wrist, shoulder, pelvis, spine or hip can
occur in osteoporotic individuals as a result of minimum force such as a fall from standing height
that would be insufficient to fracture normal bone (Poole and Compston 2006). The
consequences of fractures are severe as hip fractures are associated with increased morbidity
(Lorrain et al. 2003) and mortality (Cree et al. 2003) and decreased quality of life (Adachi et al.
2003) and are costly to the health system. For example, the average acute care length of stay for
hip fracture is two weeks with 25% of community dwelling individuals discharged to long-term
care (Jaglal et al. 1996). The acute care cost of caring for a person with a hip fracture is
estimated to be between $10,000-$15,000 USD, with additional costs required for community
and institutional care post-discharge (Haentjens et al. 2005; Papaioannou et al. 2008). More
importantly, only a third to one half of individuals with hip fracture will regain their pre-fracture
level of physical function and 18 to 28% of patients with hip fractures will die within one year of
their fracture (Mossey et al. 1989; Marolttoli et al. 1992; Koval 1994; Cooper 1997; Magaziner
et al. 2000; Hannan et al. 2001).
Individuals who have already had one low trauma fracture are at the greatest risk of
sustaining a subsequent fracture (Klotzbuecher et al. 2000). For this reason, the Canadian
Osteoporosis Guidelines have highlighted the importance of appropriate osteoporosis
investigation (bone mineral density testing) and appropriate treatment of patients with low

9
trauma fractures (Brown and Josse 2002; Khan et al. 2007). Despite these recommendations the
majority of patients who experience these fractures are under-investigated and under-treated
identifying both a diagnostic and therapeutic gap (Elliot-Gibson et al. 2004; Giangregorio et al.
2006; Bessette et al. 2008; Papaioannou et al. 2008).
2.2 THE FRACTURE FIGHTERS PROGRAM
Recently the Ontario Ministry of Health and Long-Term Care (MOHLTC) announced a
five-year $15 million strategy to improve osteoporosis care in the province (Smitherman 2005).
The funding was in response to a report by the Osteoporosis Action Plan Committee (OAPC)
that highlighted the care gaps in prevention and management of osteoporosis in Ontario (Ontario
Action Plan Committee 2003). One recommendation included the need to improve the
management of tertiary prevention services for individuals with low trauma fractures.
Fracture Fighters was one of the programs funded through the Ontario Osteoporosis
Strategy to address this recommendation. The purpose of the program was to integrate
osteoporosis management into existing inpatient rehabilitation services provided to patients 40
years of age and older post-fracture in order to prevent repeat fractures. Inpatient rehabilitation
units were selected because they are positioned at an ideal point in the continuum of care to
intervene with patients with fractures, as the average length of stay is 25 days (Sutherland and
Walker 2008). In addition, an environmental scan of Ontario inpatient rehabilitation units
demonstrated that osteoporosis investigation and management strategies were not part of usual
treatment protocols (Jaglal et al. 2006). The Fracture Fighters best-practices were based on the
Canadian Osteoporosis Guidelines (Brown and Josse 2002), and current literature with
expectation the rehabilitation units would provide, at minimum, education and referral for
osteoporosis investigation. The full-list of osteoporosis best-practices are listed in Table 1.

10
Table 1: Fracture Fighters Best-Practices for Inpatient Rehabilitation Units
Category Fracture Fighters Osteoporosis Best-Practices for Inpatient Rehabilitation
Education Osteoporosis and Fractures
Providing patients with fractures with osteoporosis education (verbal or
written);
Distributing a patient information booklet on osteoporosis and fractures*
Exercise
Demonstrating strength, posture, balance and weight-bearing exercise*;
Distributing an exercise tear-off sheet;
Talking to patients and their families about fractures and providing
education related to osteoporosis exercises
Diet & Supplements
Talking about the recommended intake from diet and supplements of
vitamin D and calcium*
Falls Risk
Providing education about home modifications
Assessment Completing a falls risk assessment;
Ordering Bone Mineral Density (BMD) testing as an inpatient if
available in facility+;
Ordering a BMD test as an outpatient+;
Referral Sending a recommendation to family physician to order BMD+;
Sending a letter to family physicians to follow-up for osteoporosis*;
Making a referral to the Community Care Access Centre (CCAC) for a
physical therapist to prescribe osteoporosis exercises; and
Making a referral to the CCAC occupational therapist for home safety
assessment
Management Initiating osteoporosis medications
*These were the minimal best-practice expectations; + one of three was expected
To integrate these best-practices into existing care the Fracture Fighters team developed a
multi-component knowledge translation strategy based on the Awareness-to-Adherence model of
clinician behaviour change (Pathman et al. 1996). The Awareness-to-Adherence model states
that clinicians must pass through sequential cognitive and behavioural steps as they comply with
a guideline. First, they must become aware of it, then intellectually agree to it, then decide to
follow it in their practice (adopt), and finally succeed in following it at appropriate times
(adherence). A variety of predisposing, enabling and reinforcing strategies have been suggested
based on the Awareness-to Adherence stage of the clinician, including distribution of educational

11
materials and academic detailing to increase awareness; opinion leaders and small group
sessions to promote agreement; clinical flowcharts or algorithms and audit and feedback to
facilitate adoption; and reminders to sustain adherence (Davis et al. 2003).
The Fracture Fighters primary strategy utilized trained front-line clinicians (Clinical
Coaches) to facilitate implementation. In order to increase their knowledge about osteoporosis
and their ability to implement the Fracture Fighters best practices two front-line clinicians (e.g.
nurse, physical therapist, occupational therapist) from each participating inpatient rehabilitation
unit were selected by their unit managers to be trained as Fracture Fighters Clinical Coaches.
Clinical Coaches attended one of seven one-day training workshops. The purpose of the
workshop was to provide clinicians with education about osteoporosis and best-practices. The
workshops were facilitated by two physical therapists and used evidence-based adult learning
methods such as interactive case discussions rather than didactic presentations. A short pre- post
osteoporosis knowledge questionnaire was administered and confirmed an increased knowledge
of osteoporosis and management practices post workshop. In addition, Clinical Coaches
received resources to raise awareness and facilitate the use of these practices (website, booklets,
posters, audit checklist) and strategies for implementation and integration of these practices into
standard fracture care. A number of additional resources were provided to Clinical Coaches after
the workshop specifically designed to aide them in program implementation including an
instructional video on how to discuss the Fracture Fighters program with their manager; two
PowerPoint presentations to facilitate small group teaching sessions within their unit; as well as
support and reminders from two Fracture Fighters implementation coordinators. A list of
Fracture Fighters resources are listed in Table 2. These materials were all developed by the
Fracture Fighters team based on osteoporosis best-practice guidelines and current research
evidence (www.fracturefighters.ca). Finally, throughout the implementation stage of the

12
program, the Clinical Coaches were invited by the Fracture Fighters project team to participate in
an advisory committee, to share strategies and barriers with Clinical Coaches from other
inpatient rehabilitation sites and make program modifications. Clinical Coaches were asked to
facilitate a teaching session with their unit, update their manager on the Strategy, complete
Fracture Fighters audit checklists and provide on-going support to their unit.
Table 2: Fracture Fighters Resources
Type Format Target Title
Education Booklet Patient A Guide to Osteoporosis for
Patients with Fractures
Education Booklet Inpatient
Rehabilitation –
Health Care
Professionals
A Guide to Osteoporosis for
Health Care Professionals
Education Tear Off Pad Patient Exercise Program for Persons
with Osteoporosis
Audit Tool Tear off Pad Health Care
Professionals
Inpatient Rehabilitation Best-
Practice Checklist
Referral Letter Tear off Pad Health Care
Professionals
Letters to communicate
osteoporosis risk and follow-up
recommendations
Education Electronic Health Care
Professionals
Fracture Fighters Newsletter
Education Slide Deck Health Care
Professionals
Fracture Fighters information
on Osteoporosis and Fractures
Education Slide Deck Health Care
Professionals
Fracture Fighters information
on Osteoporosis and Fracture,
and Rehabilitation Topics
Education Electronic Health Care
Professionals
www.FractureFighters.ca
To evaluate the implementation of the program, telephone surveys (see Appendix A –
copy of survey) with unit Managers were conducted at baseline (prior to implementation) and
again at 6 months with Clinical Coaches to determine which best practices were successfully
implemented. Overall the results showed improvements from baseline across many best practice
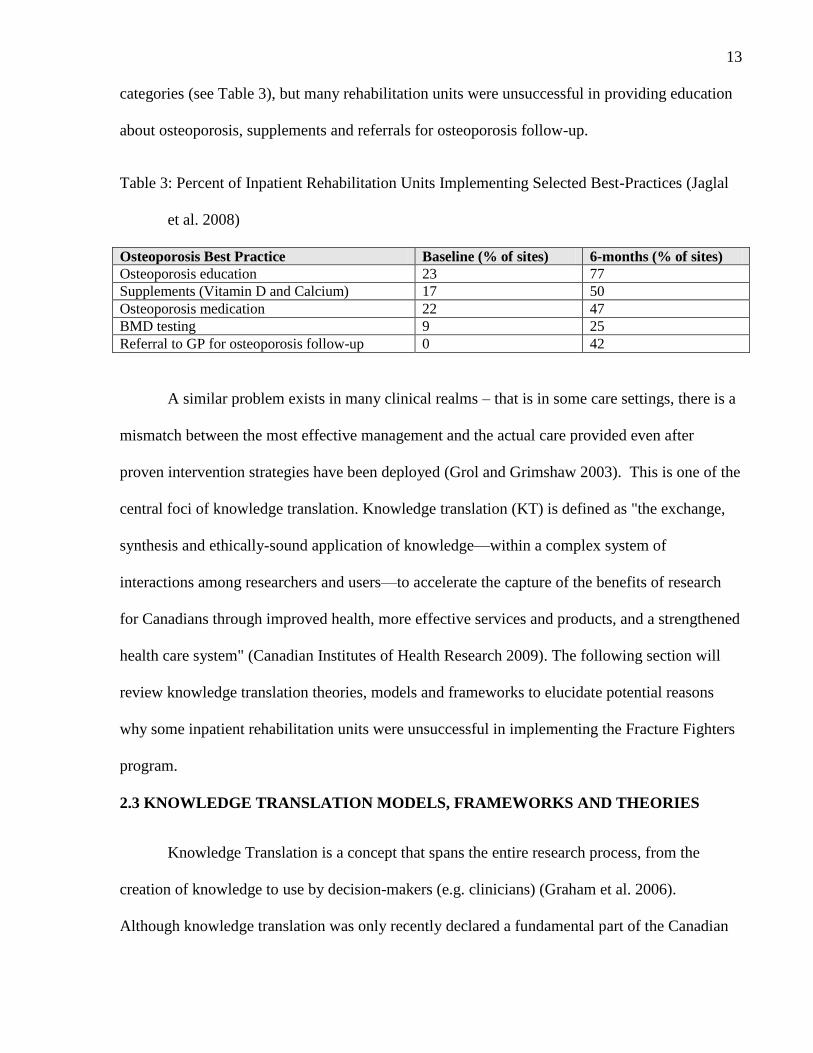
13
categories (see Table 3), but many rehabilitation units were unsuccessful in providing education
about osteoporosis, supplements and referrals for osteoporosis follow-up.
Table 3: Percent of Inpatient Rehabilitation Units Implementing Selected Best-Practices (Jaglal
et al. 2008)
Osteoporosis Best Practice Baseline (% of sites) 6-months (% of sites) Osteoporosis education 23 77 Supplements (Vitamin D and Calcium) 17 50 Osteoporosis medication 22 47 BMD testing 9 25 Referral to GP for osteoporosis follow-up 0 42
A similar problem exists in many clinical realms – that is in some care settings, there is a
mismatch between the most effective management and the actual care provided even after
proven intervention strategies have been deployed (Grol and Grimshaw 2003). This is one of the
central foci of knowledge translation. Knowledge translation (KT) is defined as "the exchange,
synthesis and ethically-sound application of knowledge—within a complex system of
interactions among researchers and users—to accelerate the capture of the benefits of research
for Canadians through improved health, more effective services and products, and a strengthened
health care system" (Canadian Institutes of Health Research 2009). The following section will
review knowledge translation theories, models and frameworks to elucidate potential reasons
why some inpatient rehabilitation units were unsuccessful in implementing the Fracture Fighters
program.
2.3 KNOWLEDGE TRANSLATION MODELS, FRAMEWORKS AND THEORIES
Knowledge Translation is a concept that spans the entire research process, from the
creation of knowledge to use by decision-makers (e.g. clinicians) (Graham et al. 2006).
Although knowledge translation was only recently declared a fundamental part of the Canadian

14
Institutes of Health Research mandate (Canadian Institutes of Health Research 2000), the study
of the use of research evidence in the health system has evolved over the last 30 or 40 years
(Estabrooks et al. 2004).
Initial studies simply attempted to measure the use of research evidence among individual
professionals. Subsequently, researchers attempted to understand the factors that predicted,
facilitated or hindered the use of research evidence by individuals, which then led to studies on
the applicability of relevant theories to explain the phenomenon (Dobbins et al. 2002). In the last
decade, researchers have sought out different interventions to improve uptake, yet no one
strategy has emerged as most effective (Grimshaw, Eccles et al. 2004). This is the focus of
implementation research, the scientific study of methods to promote the uptake of research
findings and hence reduce inappropriate care (Eccles et al. 2005).
Many of the intervention strategies or products developed to date such as best-practice
guidelines were tailored based on improving innovation features or attributes (Estabrooks et al.
2004) and most, like the Fracture Fighters program were focused on individual level factors or
barriers to research use (e.g. lack of research skills, educational preparation) (Cummings et al.
2004; Fleuren et al. 2004; Estabrooks et al. 2007). A number of literature reviews of
implementation research have consistently shown that the majority of interventions can achieve
moderate improvements in care (Oxman et al. 1995; Bero et al. 1998; Grimshaw, Eccles et al.
2004), but with considerable variation in the observed effects across interventions (Grimshaw,
Thomas et al. 2004). Several potential explanations of this variation exists, first is that the
reviews combined studies comparing the effectiveness of intervention strategies across different
intervention targets (e.g. provider, patients) (Shojania and Grimshaw 2005). In addition, a
subsequent comparison of the impact of improvement strategies from two systematic reviews for

15
diabetes and hypertension respectively revealed that any given intervention strategy may work
for diabetes but not for hypertension, emphasizing that the effectiveness of a particular approach
to quality improvement depends at least partly on the clinical context and almost certainly on
other contextual factors that have received little study (Shojania and Grimshaw 2005). Therefore,
the effectiveness of implementation strategies may be dependent on the clinical features of the
target and relevant attitudes and beliefs of providers and patients but also the organizational or
social context (Shojania and Grimshaw 2005).
2.3.1 The Need to Consider Context
In their 2008 systematic review of guideline implementation with allied health
professionals, Hakkaennes & Dodd (2008) found that all except four included studies focused on
educational interventions, assuming that the reason that allied health professionals do not use
evidence is due to lack of knowledge. Although barriers that operate at the level of the
individual health care professional are important, there is increased recognition that there exists
multiple barriers to evidence-based practice which operate at levels beyond the control of
individual practitioners (Grimshaw, Eccles et al. 2004). Increasingly, investigators have begun
to acknowledge the importance of contextual factors in achieving successful implementation in
addition to the need to involve clinicians in the knowledge creation process (Logan and Graham
1998; Cummings et al. 2007). The environment or setting in which care is provided and
proposed changes are to be implemented is defined as the context (Rycroft-Malone et al. 2002).
Since few studies provide contextual data, there may be differences in the context between
studies that assessed homogenous interventions (Eccles et al. 2005). Specifically, Cummings
(2004) notes the how and why of organizational context are important unanswered questions
(Cummings et al. 2004). Ferlie and Shortell (2001) suggest that strategies focusing on the

16
individual alone are seldom effective on their own, because the individual approach fails to
recognize that medicine is largely practiced as part of a group or team embedded within a
complex system and organizational structure. They further suggest that there are four levels
(individual health professionals; groups/teams; organizations (hospital); larger health system) of
health care at which interventions to improve quality of care could be applied. Intervention plans
do not have to address all levels simultaneously, but should consider the effect on the other
levels.
In the case of Fracture Fighters, the inpatient rehabilitation unit is the context in which
the proposed changes were to be made. Several contextual factors have been suggested to affect
implementation of evidence in practice, these include but are not limited to: staff-mix, financial
disincentives, access to resources/equipment, academic affiliation of organization, organizational
culture/climate, evaluation, provision of education, learning environment/time to read/for
research activities, stress, organizational readiness for change, uncertainty, support, leadership
style, decision-making structure, staff turnover, autonomy (Funk et al. 1991; McCormack et al.
2002; Fleuren et al. 2004; Dijkstra et al. 2006; Meijers et al. 2006; Francke et al. 2008; Koh et al.
2008; Scott et al. 2008; Yano 2008; Bostrom et al. 2009). Therefore, it is plausible that failure to
implement Fracture Fighters best practices in some inpatient rehabilitation units was due to
contextual factors not accounted for during program planning and roll-out.
2.3.2 The Need for Theory
In addition to considering contextual factors, knowledge translation researchers have
begun to advocate for the use of theory to guide implementation research (Eccles et al. 2005;
Estabrooks et al. 2006; Grol et al. 2007). The lack of theoretical underpinning and interventions

17
attempting to explicitly and prospectively modify theoretical constructs has made it difficult to
interpret why interventions have positive or negative effects (Eccles et al. 2005).
Currently, no overarching knowledge translation theory exists (Estabrooks et al. 2006).
Indeed,
―new paradigms are needed that integrate salient psychological and organizational
theories into a uniform model and make them accessible to implementation researchers,
but in the absence of such paradigms, implementation researchers should capitalize on
the contribution of organizational theories already contributed by psychology, sociology,
management science and other disciplines in order to be explicit about the anticipated
mechanisms of action at the organizational level‖ (Yano 2008).
A short scan of the literature turned up over 70 theories, models and frameworks from a variety
of disciplines that have been applied or are suggested for knowledge translation research (See
Appendix B overview of KT theories, models and frameworks). Therefore, the inclusion of a
comprehensive review of all knowledge translation theories, models and frameworks would not
be feasible. Instead, five have been selected for inclusion in this discussion based on their focus
on the implementation stage of knowledge translation; relevance to the Canadian healthcare
context or frequent citation in the literature. These include: 1) Diffusion Theory and the Spread
of Ideas (Rogers 1995; Greenhalgh et al. 2004); 2) the Knowledge-to-Action Process (Graham et
al. 2006); 3) The Ottawa Model for Research Use (OMRU) (Logan and Graham 1998; Graham
and Logan 2004); 4) The Quality Enhancement Research Initiative (QUERI)(Stetler, Mittman et
al. 2008); and 5) The Promoting Action on Research Implementation in Health Services
(PARiHS) Framework (Kitson et al. 1998; Rycroft-Malone et al. 2002). Each of these will be
briefly described followed by selection of a KT model appropriate for the Fracture Fighters
program.

18
2.3.2.1 Diffusion Theory – Spread of Ideas (Rogers 1995; Greenhalgh et al. 2004)
The Diffusion of Innovations Theory was originally developed by Rogers (1995) and has
been one of the most oft cited theories in knowledge translation research (Estabrooks 2004).
Rogers (1995) defined innovation as any idea, practice or item that is perceived to be new by an
individual or other adopting unit; and diffusion as the process by which an innovation is
communicated through certain communication channels over time. In addition he described
innovation attributes (e.g. Relative Advantage, Complexity, Trialability, Compatibility,
Observability) which are the source for much tailoring of intervention products such as clinical
guidelines.
In 2004, Greenhalgh and colleagues completed a comprehensive systematic review of
research studies in health care that applied the Diffusion of Innovation Theory. They identified
13 research areas that had provided evidence relevant to the diffusion of innovations in health
service organizations. Through their synthesis of theoretical and empirical findings Greenhalgh
and colleagues (2004) derived a conceptual model which they organized into several components
(see Figure 2):1)The innovation; 2) Adoption by Individuals; 3) Assimilation by the System; 4)
Diffusion and Dissemination; 5) System antecedents for innovation; 6) System Readiness for
innovation; 7) Interorganizational networks and collaboration; 8) Implementation and
Routination. The authors admit that components of this model do not represent a comprehensive
list of the determinants of organizational innovativeness and successful assimilation. They are
simply the areas on which research has been undertaken and findings have been published. In
addition, they noted that the model was intended merely as a ―memory aide‖ and should not be
viewed as a prescriptive formula

19
Figure 2: Greenhalgh‘s Spread of Innovations Conceptual Model (Greenhalgh et al. 2004)
2.3.2.2 The Ottawa Model of Research Use (OMRU)(Logan and Graham 1998; Graham and
Logan 2004)
The Ottawa Model of Research Use (OMRU) was developed for use by policymakers
seeking to increase the use of health research by practitioners and researchers interested in
studying the process by which research becomes integrated into practice (see Figure 3). It
features six primary elements and requires attention to a continuous assessment, monitoring, and
evaluation process. The framework is organized into three research use processes: 1) assessment
of barriers and supports; 2) monitor intervention and degree of use; and 3) evaluate outcomes.
Assessment of barriers and supports includes the evidence based innovation (development

20
process and innovation attributes); potential adopters (awareness, attitudes, knowledge/skill,
concerns, current practice); and practice environment or context (patients, culture/social,
structural, economic, uncontrolled events). The implementation plan is then selected and tailored
to overcome the identified barriers. Finally, the outcomes of the intervention are evaluated to
determine if the innovation is producing the intended effect. The feedback loops signify on-going
monitoring of barriers and supports throughout the implementation process. The model has been
used in a variety of clinical areas such as neonatal intensive care (Hogan and Logan 2004),
tertiary hospital care (Graham and Logan 2004), ulcer care (Logan, Harrison et al. 1999), and
nurse call centres (Logan et al. 1999; Stacey et al. 2006).
Figure 3: Ottawa Model of Research Use

21
2.3.2.3 The Knowledge to Action Process Framework (KTA) – (Graham et al. 2006)
The KTA is the framework endorsed by the Canadian Institutes of Health Research as it
encompasses the entire KT process from knowledge creation through to action. It was developed
based on a review of over 30 planned action models. The KTA has two main components, the
knowledge creation ―funnel‖ and the action cycle (see Figure 4). Knowledge creation consists of
three phases, knowledge inquiry, synthesis and tools/products. Through synthesis the vast
amount of knowledge is funnelled or distilled down eventually to a small number of tools or
products that can be used to facilitate knowledge implementation. ―Tailoring‖ runs throughout
the funnel to demonstrate through each phase of knowledge creation, the potential needs of
stakeholders are considered. The action part of the process can be thought of as a cycle leading
to implementation or application of knowledge. In contrast to the knowledge funnel, the action
cycle represents the activities that may be needed for knowledge application. The steps in the
cycle include problem identification; identification, review and selection of knowledge;
adaptation to local context; assessment of barriers to knowledge use; selection and tailoring of
interventions; monitoring use; evaluation; and sustained knowledge use. The action process is
similar to that described by OMRU. The KTA is a more comprehensive framework as it includes
the knowledge creation process in addition to the action cycle.

22
Figure 4: Knowledge to Action (CIHR http://www.cihr-irsc.gc.ca/e/39033.html )
2.3.2.4 Quality Enhancement Research Initiative (QUERI)
The Quality Enhancement Research Initiative (QUERI) is a planned action model,
intended to be used to engineer change. It was conceptualized within the US Veteran‘s Affairs
(VA) healthcare delivery system. A major contribution to the field is that the QUERI model
divides up the implementation process into manageable and logical steps (Graham and Tetroe
2009). One of the key elements is the 6-step framework or process that guides all implementation
activity (Stetler, Mittman et al. 2008). The QUERI research group has published numerous
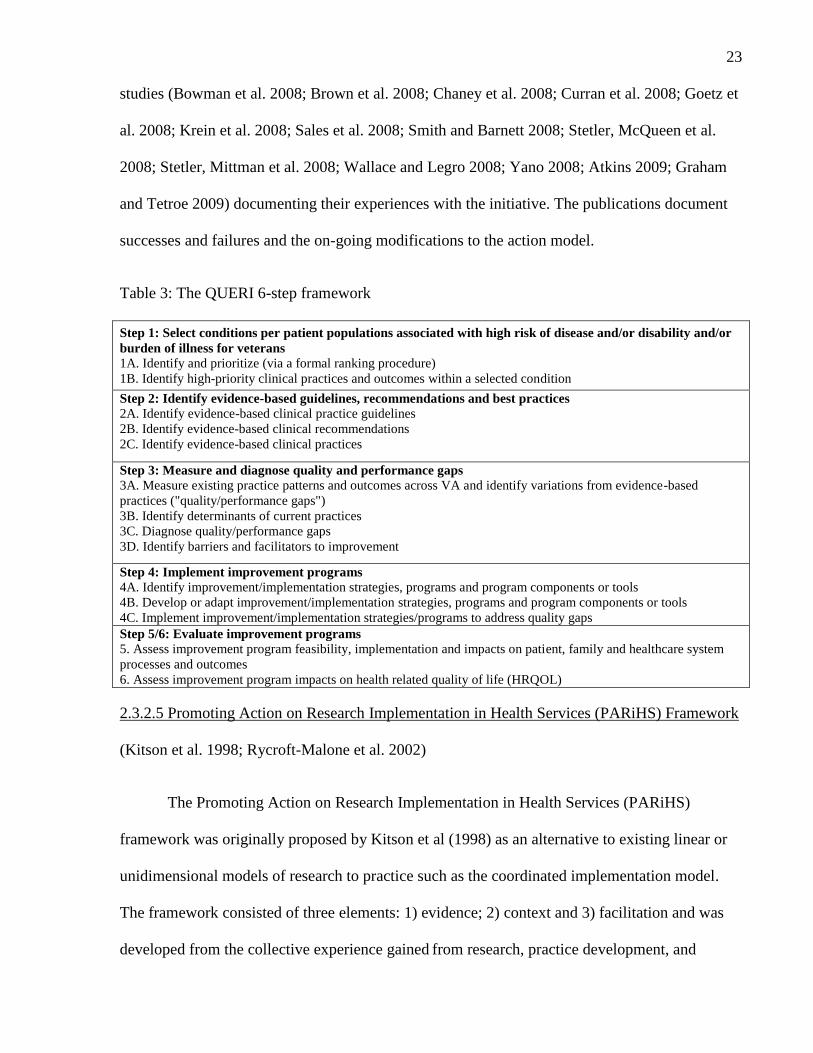
23
studies (Bowman et al. 2008; Brown et al. 2008; Chaney et al. 2008; Curran et al. 2008; Goetz et
al. 2008; Krein et al. 2008; Sales et al. 2008; Smith and Barnett 2008; Stetler, McQueen et al.
2008; Stetler, Mittman et al. 2008; Wallace and Legro 2008; Yano 2008; Atkins 2009; Graham
and Tetroe 2009) documenting their experiences with the initiative. The publications document
successes and failures and the on-going modifications to the action model.
Table 3: The QUERI 6-step framework
Step 1: Select conditions per patient populations associated with high risk of disease and/or disability and/or
burden of illness for veterans 1A. Identify and prioritize (via a formal ranking procedure)
1B. Identify high-priority clinical practices and outcomes within a selected condition
Step 2: Identify evidence-based guidelines, recommendations and best practices 2A. Identify evidence-based clinical practice guidelines
2B. Identify evidence-based clinical recommendations
2C. Identify evidence-based clinical practices
Step 3: Measure and diagnose quality and performance gaps 3A. Measure existing practice patterns and outcomes across VA and identify variations from evidence-based
practices ("quality/performance gaps")
3B. Identify determinants of current practices
3C. Diagnose quality/performance gaps
3D. Identify barriers and facilitators to improvement
Step 4: Implement improvement programs 4A. Identify improvement/implementation strategies, programs and program components or tools
4B. Develop or adapt improvement/implementation strategies, programs and program components or tools
4C. Implement improvement/implementation strategies/programs to address quality gaps
Step 5/6: Evaluate improvement programs 5. Assess improvement program feasibility, implementation and impacts on patient, family and healthcare system
processes and outcomes
6. Assess improvement program impacts on health related quality of life (HRQOL)
2.3.2.5 Promoting Action on Research Implementation in Health Services (PARiHS) Framework
(Kitson et al. 1998; Rycroft-Malone et al. 2002)
The Promoting Action on Research Implementation in Health Services (PARiHS)
framework was originally proposed by Kitson et al (1998) as an alternative to existing linear or
unidimensional models of research to practice such as the coordinated implementation model.
The framework consisted of three elements: 1) evidence; 2) context and 3) facilitation and was
developed from the collective experience gained from research, practice development, and

24
quality improvement projects. Instead of a hierarchy or linearity of cause and effect each of the
dimensions are considered simultaneously (Kitson et al. 1998).
Through the application of the model to four case studies completed by the Royal College
of Nursing Institute, Kitson and colleagues (1998) demonstrated that most successful
implementation occurred when: 1) the evidence is scientifically robust and matches professional
consensus and patient needs ("high" evidence); 2) the context is receptive
to change with
sympathetic cultures, strong leadership, and appropriate monitoring and feedback systems
("high" context); and 3) there is appropriate facilitation for change with input
from skilled
external and internal facilitators ("high" facilitation) (Rycroft-Malone et al. 2002) (Figure 5)
Figure 5: Promoting Action on Research Implementation in Health Services (PARiHS)
Framework

25
Each element in the framework (evidence, context and facilitation) included a number of
sub-elements which were revisited in 2002 by the same authors (Harvey et al. 2002; McCormack
et al. 2002; Rycroft-Malone et al. 2002). They completed a content analysis by critically
reviewing the literature to further develop the sub-elements included within the framework. The
element of evidence has three sub-elements: research, clinical experience, patient experience;
context has three sub-elements of leadership, culture and evaluation; and high facilitation
included a match between the purpose and role of facilitation with the skills and attributes of the
facilitator. Each of the elements is ranked on a scale from low to high. A full outline of the
PARiHS elements is available in Appendix C (Rycroft-Malone et al. 2002).
Several empirical studies have provided support for the PARiHS framework by
demonstrating that successful implementation is a function of evidence, context and facilitation.
However, it is still unclear if the elements or sub-elements have equal weighting in getting
evidence into practice (Kitson et al. 2008). Two studies have demonstrated a dose-response
relationship in that higher levels of culture, leadership and evaluation (context) resulted in
greater research utilization (Cummings et al. 2007; Estabrooks et al. 2007) and two studies (Ellis
et al. 2005; Wallin et al. 2005) have utilized the PARiHS framework to guide qualitative
evaluations of evidence implementation. Ellis et al (2005) explored the relative and combined
importance of context and facilitation in successful implementation of clinical practice protocols
and concluded that good facilitation appeared to be more influential than context in overcoming
the barriers to evidence-based practice. Whereas, Wallin and colleagues (2005) demonstrated
that a facilitation intervention appeared to be no more effective than an improvement focused
organizational culture for implementing guidelines in neonatal care units in Australia.

26
2.3.2.6 Selection of the KT Model for Fracture Fighters Program
Common to these theories/models is attention to identifying, describing, and assessing
the practice environment and its influences, which may facilitate and/or impede the process of
research transfer and use. Other common features of the models are monitoring the progress of
the transfer effort, and evaluating usage of the evidence-based innovation and its impact on
outcomes of interest (Kontos and Poland 2009).
Grimshaw and colleagues (2004) suggest that it is unlikely that one theory will apply
equally well to every possible intervention, and thus it is more reasonable to try to find the best
fit between theories and particular interventions(Grimshaw, Eccles et al. 2004). Of the five
models described, the PARiHS framework was selected for application to the Fracture Fighters
program due to its emphasis on the importance of facilitation. Although many of these models do
mention the need for linkages, facilitation or opinion leaders, PARiHS included facilitation as
one of three core elements required for successful implementation, fitting with the primary type
of implementation strategy employed by Fracture Fighters, facilitation via the Clinical Coach
model. What distinguishes the PARiHS conceptual framework from the others is that as well as
mapping the interrelationships, PARiHS has the potential to be used as a practical and pragmatic
tool by practitioners and researchers at the local level during implementation planning (Kitson et
al. 2008). However, to do this there is a need to clarify the definition of each element and sub-
element and to identify appropriate questionnaires to measure each of the constructs.
The framework developers have prioritized the need to develop diagnostic and evaluative
tools based on PARiHS (Kitson, 2008). In this regard, in order to use PARiHS in practice,
instruments are needed to assess barriers and facilitators during implementation planning
(diagnose) as well as to determine the effectiveness of intervention strategies (evaluation). In

27
addition, concrete guidance on how to match tools to identified barriers (prescribe) is required
(Green et al. 2007).
2.4 SUMMARY
Unit or organizational level factors such as context are increasingly being recognized as
important considerations for evidence implementation. PARiHS may be a useful framework to
examine unit level factors that influence evidence implementation in practice. However, prior to
application, the PARiHS framework must be operationalized by identifying appropriate
measures of evidence, context and facilitation and respective sub-elements.

28
CHAPTER 3: Manuscript 1
TITLE: Proposing a Toolbox of Measures for the Promoting Action on Research
Implementation in Health Services (PARiHS) Framework: Application to Fracture
Fighters Program
3.1 ABSTRACT
Background: Interventions to increase uptake of research have led to moderate success, but no
overarching intervention strategy has emerged. This may be due to differences in the
environment in which these interventions are applied thus knowledge translation models and
frameworks have begun to incorporate contextual factors. The Promoting Action on Research
Implementation in Health Services (PARiHS) is one such framework but further work is needed
to operationally define the constructs of PARiHS to enable its widespread application.
Purpose: The purpose of this paper is to propose a toolbox of measures for the PARiHS
framework by describing its potential application to a best practice program called Fracture
Fighters.
Methods: Measures were selected after a review of statements suggested by the framework
developers and additional available measures of evidence, leadership, climate, evaluation and
facilitation. Where available, standardized measures were selected, based on content validity
with the PARiHS description of elements/sub-elements and evidence of psychometric validity
and reliability.
Results: The proposed toolbox consists of the following validated scales: the Multifactor
Leadership Questionnaire (Leadership); the Organizational Climate sub-scale of the
Organizational Readiness for Change measure (Climate); the Champion Behavior Measure and

29
the Opinion Leadership Scale (Facilitation). In addition, we suggested a simple measure of
evidence based on statements suggested by the framework developers and an assessment of
project-specific process indicators be included to provide information on the evidence and
evaluation sub-elements respectively.
Conclusion: The proposed toolbox will enable measurement of the PARiHS constructs of
evidence, context and facilitation and their respective sub-elements. Future research could apply
the proposed toolbox to provide further validation that high evidence, context and facilitation are
predictors of implementation success and provide refinements to the model by determining
which elements or sub-elements are the primary drivers of implementation success.
Word Count: 289

30
3.2 INTRODUCTION
Implementation research is the scientific study of methods to promote the uptake of
research findings and hence reduce inappropriate care (Eccles et al. 2005). In recent years it has
been given much attention by knowledge translation scholars and numerous interventions, such
as guideline dissemination, continuing medical education, reminders, educational outreach and
audit and feedback, have been developed and tested in order to increase the likelihood that
clinicians will incorporate new research into their current practice. However, several systematic
reviews of implementation strategies have concluded that there is no ―magic bullet‖ or one best
approach to increasing the use of evidence in practice (Oxman et al. 1995) and that multi-
component strategies are no more effective then single interventions (Grimshaw, Eccles et al.
2004). Although there is a widespread agreement that evidence implementation requires
strategies to meet the needs of the individual clinician, there is an increasing acknowledgement
of the importance of organizational context (Logan and Graham 1998; Cummings et al. 2007;
Wallin 2009).
Context is defined as the environment or setting in which the proposed change is to be
implemented (Rycroft-Malone et al. 2002). Some examples of contextual factors include:
academic affiliation of organization, functional differentiation/staff-mix, organizational
culture/climate, evaluation, access to resources/equipment, provision of education, learning
environment/time to read/for research activities, stress, organizational readiness for change,
uncertainty, support, leadership style, decision-making structure, staff turnover, autonomy (Funk
et al. 1991; Frenk 1992; McCormack et al. 2002; Fleuren et al. 2004; Dijkstra et al. 2006;
Meijers et al. 2006; Francke et al. 2008; Koh et al. 2008; Scott et al. 2008; Yano 2008; Bostrom
et al. 2009). Several studies are available that demonstrate correlations between contextual

31
factors and research use (Meijers 2006; Estabrooks 2007; Cummings 2007). In addition, several
KT models and frameworks have been developed that attempt to include contextual or
environmental factors (e.g. Ottawa Model for Research Use (Logan and Graham 1998);
Knowledge-to-Action Process(Graham et al. 2006); PARiHS Framework(Kitson et al. 1998;
Rycroft-Malone et al. 2002); The Spread of Ideas (Greenhalgh et al. 2004); QUERI(Stetler,
Mittman et al. 2008)). One framework developed to describe implementation success in health
care organizations is the Promoting Action on Research Implementation in Health Services
(PARiHS) framework (Kitson et al. 1998). This framework (Figure 6) states that successful
implementation is a function of three elements: 1) evidence 2) context and 3) facilitation. Each
element and its respective sub-elements are rated on a continuum from low to high. In a series of
case reports, Kitson and colleagues (1998) demonstrated that the most successful implementation
occurs when: 1) the evidence is scientifically robust and matches professional consensus
and
patient needs ("high" evidence); 2) the context is receptive to change with sympathetic cultures,
strong leadership, and appropriate monitoring and feedback systems ("high" context);
and 3)
there is appropriate facilitation of change with input from skilled external and internal facilitators
("high" facilitation)(Rycroft-Malone et al. 2002).
FA
CIL
ITA
TIO
N
CO
NT
EX
T
EV
IDE
NC
E
Implementation Success = f (Evidence, Context, Facilitation)
RESEARCH
CLINICAL
EXPERIENCE
PATIENT
EXPERIENCE
LEADERSHIP
CULTURE
EVALUATION
PURPOSE
ROLES
SKILLS &
ATTIBUTES
Figure 6: Promoting Action on Research Implementation in Health Services Framework

32
Each element in the framework (evidence, context and facilitation) included a number of
sub-elements which were revisited in 2002 by the same authors (Harvey et al. 2002; McCormack
et al. 2002; Rycroft-Malone et al. 2002). They completed a content analysis by critically
reviewing the literature to further refine the sub-elements included within the framework.
Recently a number of qualitative studies have applied the PARiHS framework to inform
implementation planning (Ellis et al. 2005; Wallin et al. 2005; Doran and Sidani 2007; Conklin
and Stolee 2008) and to evaluate the relationship between the PARiHS elements of evidence,
context, and facilitation and research use (Sharp et al. 2004; Brown and McCormack 2005; Ellis
et al. 2005; Wallin et al. 2005; Meijers et al. 2006; Doran and Sidani 2007). Brown and
McCormack (2005) utilized the PARiHS framework to guide a document analysis of 58 studies
and found supporting evidence of the importance of evidence, context and facilitation in getting
evidence into practice. Whereas, Sharp and colleagues (2004) found the framework useful for
guiding a content-analysis assessing the barriers and facilitators to implementation of a pilot
intervention in 6 medical centres in the US Veteran‘s Health Administration Network. Finally,
Meijers et al (2006) focused on the element of context and identified six contextual factors in a
systematic review that influenced research utilization in nursing.
Although the PARiHS framework is well described in the original introduction (Kitson et
al. 1998) and subsequent concept reviews (Harvey et al. 2002; McCormack et al. 2002; Rycroft-
Malone et al. 2002) and there is accumulating evidence (Sharp et al. 2004; Brown and
McCormack 2005; Ellis et al. 2005; Wallin et al. 2005; Meijers et al. 2006; Cummings et al.
2007; Doran and Sidani 2007; Estabrooks et al. 2007; Estabrooks et al. 2008) on the
framework‘s usefulness and validity, there are several limitations to its application. First and
foremost, there is lack of guidance on how to determine the status of elements on the continuum

33
scales from low to high. Specifically, at the time of this study, the developers had not identified a
validated scale or questionnaire to assess the constructs. Bahtsevani et al (2008) attempted to
validate a questionnaire based on the PARiHS framework. They reported test-retest reliability of
a questionnaire designed to gather data about guidelines that had been implemented with health
care professionals in Swedish hospitals. They derived eight statements directly from the PARiHS
framework to measure the context of care. For example ―the context is characterized by
transformational leadership‖ and ―the context is characterized by traditional (command and
control) leadership‖ were placed at the opposite ends of a visual analogue scale. However, the
developers noted major limitations of the scale as the questionnaire statements were found to be
too abstract and several respondents commented that the questions were difficult to interpret due
to unfamiliarity with the concepts.
Currently, it is unclear which elements or sub-elements included in the framework are the
most influential in determining successful implementation (Kitson et al. 2008). Two qualitative
studies applying the framework found conflicting results regarding the importance of the
elements of context and facilitation. Ellis and colleagues (2005) explored the relative and
combined importance of context and facilitation in successful implementation of clinical practice
protocols and concluded that good facilitation appeared to be more influential than context in
overcoming the barriers to evidence-based practice. Conversely, Wallin et al (2005)
demonstrated that a facilitation intervention appeared to be no more effective than context (an
―improvement‖ focused organizational culture) for implementing guidelines in neonatal care
units in Australia. Dijkstra (2006) points out that despite the increasing attention to
organizational determinants in implementation; research evidence on the relevance of specific
factors is needed. This can be achieved through quantitative designs that link the sub-elements
with an outcome indicator. There have been only a few published studies (Cummings et al. 2007;

34
Estabrooks 2007; Estabrooks et al. 2008) applying the PARiHS framework using quantitative
methods, thus supporting the need for further studies to provide validation that evidence, context
and facilitation are indeed associated with and ideally predictive of implementation success
(Wallin 2009).
Finally, the terminology used to describe some of the elements and their associated
definitions are debated by different disciplines. In nursing, McCormack et al (2002) noted that
the inconsistency in the use of the term context has had an impact on claims of its importance.
Previous attempts to measure the nursing practice environment have led to the development of
numerous instruments each of which appears to measure a different construct (Meijers et al.
2006). For example, Cummings et al. (2006) examined the validity of three instruments as
measures of nursing practice and concluded that each had a theoretical and/or measurement fault.
Therefore, they suggested that the most useful advances in developing the concept of context
will result from advancing and testing robust theory about the relationships among specific
feature within the practice environment of context (Cummings et al. 2006). Thus, the PARiHS
elements require clarification in order to ensure different groups applying the framework are
indeed measuring the same constructs.
3.2.1Purpose
The purpose of this study is to operationalize the PARiHS framework by proposing a
toolbox of questionnaires to enable measurement of the three main elements and sub-elements.
An osteoporosis best-practice program called Fracture Fighters will be used as an example of
how the questionnaires could be applied.

35
3.2.2 Description of the Fracture Fighters Program
The Fracture Fighters program used a comprehensive knowledge translation approach
based on Pathman et al.‘s (1996) Awareness-to-Adherence model that centred on the use of
trained front line clinicians (Clinical Coaches) to facilitate integration of osteoporosis
management into existing inpatient rehabilitation services. The program best practices included
providing patients with fracture education about osteoporosis risk factors, supplements, and
exercise as well as ensuring the patient was scheduled or referred for follow-up osteoporosis
investigation; finally inpatient rehabilitation units were expected to notify the patients‘ primary
care provider that osteoporosis follow-up care and management was required.
3.3 OPERATIONALIZING THE PARIHS FRAMEWORK
The PARiHS framework suggests that successful implementation is a function of
evidence, context and facilitation. Recently, Kitson et al (2008) proposed a list of draft
statements to be used as diagnostic (barrier identification) and evaluation measures of the
elements of evidence and context. They suggest that these questions could be answered
individually and/or through a facilitated dialogue where each team members‘ assumptions,
prejudices, views about existing practice, and the proposed change are discussed and debated.
The strength of this tool is that the statements possessed high face validity and map directly to
the PARiHS sub-elements. However, no scaling or scoring information was provided with the
statements demonstrating the need for further development work on these measures to provide
evidence of acceptable psychometric properties (validity and reliability) as well as usability.
The measures proposed in this paper were selected after a review of Kitson et al‘s (2008)
suggested statements and available measures of evidence, leadership, climate, evaluation and

36
facilitation. Where available, standardized measures were selected, based on content validity
with the PARiHS description of elements/sub-elements and evidence of psychometric validity
and reliability. Kimberly and Cook (2008) noted several advantages to utilization of
standardized measures. First, they are easily accessible and ready to use often with little or no
modification. Second they usually have been empirically validated and thus have a certain
amount of face validity and psychometric legitimacy. Finally, they allow for ease of replicability
(Kimberly and Cook 2008). Each element and corresponding sub-elements will be discussed and
potential questionnaires will be identified to include in a toolbox to measure these framework
constructs. The Fracture Fighters program will be used as an example throughout the discussion.
3.3.1 Evidence
Evidence, one of three core elements of the PARiHS framework, is composed of the sub-
elements of research, clinical experience and patient preferences/experience (Kitson et al. 1998;
Rycroft-Malone et al. 2002) that can be evaluated on a continuum from low to high. For
example, low clinical experience is characterized by a diversity of expert opinions or several
―camps‖, whereas high clinical expertise would include consensus and consistency in opinions.
According to the PARiHS developers, for the most successful implementation to occur all three
sub-elements should be rated on the high range of the continuum. For example, even if the
research evidence shows an intervention is highly effective through a randomized controlled
trial, if it is rejected by clinicians and patients it is unlikely to be successfully implemented
despite its gold standard research evidence. The inclusion of patient experience and clinical
experience as sub-elements of evidence is a unique aspect of the PARiHS framework. For
example, evidence based medicine (EBM) is defined as ―the conscientious, explicit, and
judicious use of current best evidence in making decisions about the care of individual patients‖
(Sackett et al. 1996). Rather than include these sub-elements (patient experience and clinical

37
experience) as types of evidence, EBM advocates for the integration of individual clinical
expertise (a type of knowledge) with the best available external clinical evidence from systematic
research (Sackett et al. 1996). To highlight the importance of clinical experience and patient
experience, the PARiHS model includes these as types of evidence in addition to systematic
research. All three types of evidence should be considered, included in decisions; their
importance weighed and judged for relevance (Rycroft-Malone et al. 2002).
3.3.1.1Evidence Toolbox: Kitson‘s Preliminary Evidence Questions
Kitson et al (2008) recently published a set of ―draft‖ questions to be used for evaluating
the elements in the PARiHS framework. The process for establishing these questions was not
described. Although the items have not been tested psychometrically for ―evidence‖, the items
map directly to the sub-elements and have high face validity. Since no scoring for the statements
were included, we suggest a standard 5-point Likert scale (<1>strongly disagree; <5> strongly
agree). An example of how the statements were modified for the Fracture Fighters program is
shown in Table 5.

38
Table 5: PARiHS Toolbox – Adapted Evidence Questionnaire
Strongly Disagree Disagree Neutral Agree Strongly Agree
<1> <2> <3> <4> <5>
Research
1. I value the research evidence
I value the research evidence provided by Fracture Fighters 1 2 3 4 5
2. The research evidence fits with my understanding of the issue
The Fracture Fighters research evidence fits with my understanding of fractures and
osteoporosis management
1 2 3 4 5
3. The research evidence is useful in thinking about the issue
The Fracture Fighters research evidence is useful in thinking about the issue of
osteoporosis management for fracture patients
1 2 3 4 5
4. I am clear about what the key messages for the planned intervention are
I am clear about what the key messages for the Fracture Fighters intervention are 1 2 3 4 5
5. There is consensus amongst my colleagues about the usefulness of this research to this issue
There is consensus amongst my colleagues about the usefulness of Fracture Fighters
research to the issue of osteoporosis management in fracture patients
1 2 3 4 5
Clinical Experience
6. I have reflected on my own clinical experience in relation to this issue
I have reflected on my own clinical experience in relation to fractures and osteoporosis 1 2 3 4 5
7. I have shared and critically reviewed my clinical experience in relation to this issue
I have shared and critically reviewed my clinical experience in relation fractures and
osteoporosis
1 2 3 4 5
8. I have shared and critically reviewed my clinical experience with knowledgeable colleagues
outside of my (clinical) workplace
I have shared and critically reviewed my clinical experience with knowledgeable colleagues
outside of my (clinical) workplace
1 2 3 4 5
9. There is a consensus of (clinical) experience about this issue
There is a consensus of (clinical) experience about the Fracture Fighters osteoporosis best-
practices
1 2 3 4 5
10. Clinical experience will be used as one part of the evidence
Clinical experience will be used as one part of the evidence for implementing the program 1 2 3 4 5
11. The consensus of clinical experience fits with my understanding of the issue
The consensus of clinical experience fits with my understanding of fractures and
osteoporosis
1 2 3 4 5
Patient Experience
12. We routinely (and systematically) collect users/patients‘ experiences about this particular
issue
We routinely (and systematically) collect patients’ experiences about fractures and
osteoporosis follow-up
1 2 3 4 5
13. Users/patients experiences will be used as one part of the evidence
Patients experiences will be used as one part of the evidence 1 2 3 4 5
14. I value patient experiences evidence
I value patient experiences as evidence 1 2 3 4 5
15. The evidence of patients experiences fits my understanding of the issue(s)
The evidence of patients experiences fits my understanding of the issue(s) 1 2 3 4 5
16. Patient experiences are useful in thinking about the issue
Patient experiences are useful in thinking about the osteoporosis best-practices 1 2 3 4 5
17. There is a consensus amongst my colleagues about the usefulness of patient experiences to
this issue
There is a consensus amongst my colleagues about the usefulness of patient experiences to
osteoporosis management in fracture patients
1 2 3 4 5
Italicized items are adapted for the Fracture Fighters program (Kitson et al. 2008)

39
3.3.2 Context
The second element of the PARiHS framework is context. Context is defined as the
environment or setting in which people receive healthcare services or the context of getting
research evidence into practice (Rycroft-Malone et al. 2002). Context in the PARiHS framework
is comprised of three sub-elements: leadership, organizational culture and
evaluation/measurement that are also judged on a continuum from low to high. A ―strong‖
context is defined as having clear physical, social, structural and cultural boundaries; appropriate
resources available; uses appropriate and transparent decision making processes; power and
authority are understood; information and feedback systems are in place; and is receptive to
change (McCormack et al. 2002).
3.3.2.1Leadership
Leadership is one of three sub-elements of context. Kitson et al (1998) claimed that
―high‖ leadership included: Role clarity, effective teamwork, effective organizational structures
and clear leadership. This sub-element was expanded in the concept review of PARiHS elements
by McCormack (2002) to include transformational leadership a concept derived from Bass‘s
transactional theory on leadership, which recently has begun to dominate the leadership literature
in nursing management (Marchionni and Ritchie 2008). The PARiHS developers argue that
transformational leaders have the ability to transform cultures to create a context more conducive
to the integration of evidence into practice as opposed to transactional leaders who ―command
and control‖(McCormack et al. 2002).
However, upon further exploration, transformational leadership is not a one-dimensional
category as implied by the PARiHS description but includes four interrelated components:

40
charismatic, inspirational, intellectually stimulating, and individually considerate leaders (Bass et
al. 1996). Charismatic leaders are highly esteemed; they are role models that strive to let
followers emulate their actions towards a vision, common purpose or goal. Inspirational leaders
provide meaning and optimism about the mission and its attainability. However, inspirational
leaders are distinct from charismatic leaders in that followers may not necessarily seek to
emulate the leader. Intellectually stimulating leaders encourage followers to question basic
assumptions and to consider problems from new perspectives. Finally, individually considerate
leaders work with followers to define their needs and subsequently help them to achieve higher
levels based on these needs (Vroom and Jago 2007). A transformational leader may have all or
some of these traits. A closer look at Avolio and Bass‘s Full-Range Leadership Theory (FRLT)
revealed the identification of nine single-order factors (Avolio and Bass 2004). Five of the
factors are categorized as transformational, three are transactional and one is a non-transactional
‗laissez-faire‘ style that reflects the absence of leadership as opposed to the simplified
transformational vs. transactional description included by PARiHS. As a result we suggest that
leadership measures other than those suggested by Kitson et al (2008) be considered.
3.3.2.1.1Context Toolbox: Multifactor Leadership Questionnaire (MLQ)
A review of questionnaires to measure leadership indicated that the Multifactor
Leadership Questionnaire (MLQ Form 5X) is one of the most widely used instruments to
measure transactional and transformational behaviours in the organizational sciences (Tejeda et
al. 2001). The MLQ (Form 5X) contains 45 items in total, 36 which correspond to the nine
leadership factors. These nine leadership factors are derived from the Full-Range Leadership
Theory (Avolio and Bass 1991 ) and includes: 1) idealized influence attributed (perceived
socialized charisma); 2) Idealised influence behaviour (charismatic actions of the leader); 3)

41
Inspirational motivation (the ways leaders energize their followers); 4) Intellectual stimulation
(the way leaders challenge followers to think and problem solve); 5) Individualized consideration
(extent that advice is individualised to needs of the follower); 6) Contingent reward leadership
(constructive transactions); 7) Management-by-exception active (leaders goal is to ensure
standards are met); 8) Management-by-exception passive (leaders intervene only after mistakes
have already happened). The final factor is nontransactional laissez-faire leadership which
represents a leader who avoids decisions, relinquishes responsibility and does not use their
authority (Antonakis et al. 2003). Each of the 36 MLQ items are scored on a Likert scale from 1
to 5 (<1> not at all; <5> frequently if not always). Mean composite scores are computed for each
of the nine leadership factors. These individual leadership scores can subsequently be compared
to a normative score profile which is based on a US database of approximately 27,000 MLQ
respondents (See Appendix F for Percentiles of Individual Scores) (Avolio and Bass 2004). The
score profiles are reflective of a variety of industries (military, government, educational,
manufacturing, high technology, church, correctional, hospital, and volunteer organizations) and
a wide variety of rater groups (self-report, lower level rating, same level rating, higher level
rating) (Avolio and Bass 2004).
The MLQ (Form 5X) was developed and revised based on results from previous versions
of the MLQ and a confirmatory factor analysis (Antonakis et al. 2003). The developers of the
MLQ used a sample from their global database (United States n=27,000; Europe n=15,000;
Australia n =13,000; South Africa n =500) to complete a confirmatory factor analysis to test the
expanded nine factor model (MLQ Form 5X) whereas previous models included a six factor
model. In all instances there was clear support for the nine factor model regardless of rater
source or geographic variation (Bass and Avolio 1994). More importantly, the MLQ has been
validated in a health care setting, a group of Finnish nurses and nurse leaders (n=601) (Kanste et

42
al. 2007). Cronbach‘s alpha for the leadership subscales ranged from 0.78 to 0.94 in this group.
Inter-item correlations ranged from 0.30 to 0.70. Thus the MLQ would be suitable for evaluating
leadership in the clinical setting. Sample items are listed in Table 6.
Table 6: Leadership styles, behaviours and sample questionnaire items
Leadership
Style
Leadership Behaviour Sample MLQ Form 5X Question*
Transformational Charismatic (Idealized
Influence – attributed)
Instills pride in me for being associated with him/her
Charismatic (Idealized
Influence – behaviours)
Inspirational Motivation Talks optimistically about the future Intellectual Stimulation Suggests new ways of how to complete assignments Individualized Consideration
Transactional Contingent Rewards Management-by-Exception
(active) Directs my attention towards failures to meet
standards Management-by-Exception
(passive) Fails to interfere until problems become serious
Laissez-Faire Laissez-Faire *Note, due to copyright restrictions, only 5 items are permitted for inclusion
3.3.2.2 Culture
Organizational culture is the second sub-element of context included in PARiHS. Kitson
et al. (1998) describe culture as the ―forces at work that give the physical environment a
character and feel‖, suggesting a direct relationship between culture and context (McCormack et
al. 2002). Organizational culture has been argued to be the dominant factor in clinical
effectiveness, practice development and successful outcome achievement (McCormack et al.
2002). The characteristics of ―strong‖ culture include: 1) the organizations ability to define
values and beliefs; 2) valuing individual staff and clients; 3) promotion of learning in the
organization; and 4) consistency in relationships with others, including teamwork, power and
authority as well as a rewards and recognition system. A focus on systems, process and

43
structures can describe the context where a practice takes place, however, it does little to
articulate the culture in the context (McCormack et al. 2002).
It is possible that several diverse and at times conflicting cultures can operate under one
organization or institution, reflecting variability in cultural norms, different values and
worldviews (Kennedy 2001). Clashes of cultures within an organization often lead to
dysfunctional or suboptimal relationships thereby reducing the ability to implement change. For
example, other factors that may restrict interdisciplinary working include: differences in
priorities, aims, and objectives, confusion over accountability, lack of understanding of the team
process and the team members' role and responsibility within it, as well as interpersonal skills
(Barr 1997) or staff turnover and lack of team learning (Gibbon 1999).
Although McCormack et al. (2002) attempted to clarify the PARiHS definition of culture
in their concept analysis of context, they failed to appropriately distinguish organizational culture
from organizational climate, thereby missing the crucial implications of the distinction.
Organizational culture was recently defined as ―the way things are done in the organization‖ and
organizational climate as ―the way people perceive their work environment‖ (Glisson et al.
2008). Previously, Denison (1996) undertook an extensive comparison of organizational culture
and organizational climate literature to highlight differences and areas of convergence (See Table
7). The biggest difference stemmed from their theoretical foundations. The climate literature
evolved from the work of Lewin (Sansone et al. 2003) who stated that behaviour was a function
of the environment and the person [B=f(E, P)]. By stating the environment and person discretely
it is possible to conceptualize, dimensionalize and compare these across different social
environments. In contrast, culture literature stems from anthropology/ethnography, symbolic
interactionism and social construction; therefore individuals cannot be separated from their
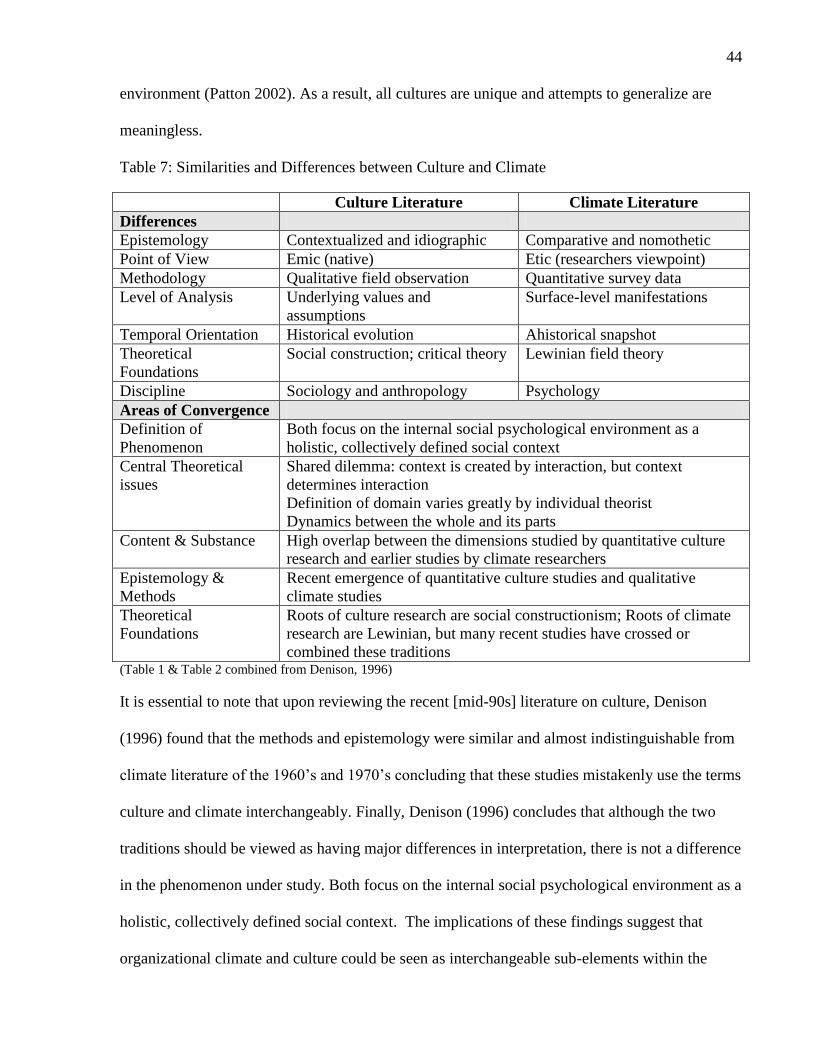
44
environment (Patton 2002). As a result, all cultures are unique and attempts to generalize are
meaningless.
Table 7: Similarities and Differences between Culture and Climate
Culture Literature Climate Literature
Differences
Epistemology Contextualized and idiographic Comparative and nomothetic
Point of View Emic (native) Etic (researchers viewpoint)
Methodology Qualitative field observation Quantitative survey data
Level of Analysis Underlying values and
assumptions
Surface-level manifestations
Temporal Orientation Historical evolution Ahistorical snapshot
Theoretical
Foundations
Social construction; critical theory Lewinian field theory
Discipline Sociology and anthropology Psychology
Areas of Convergence
Definition of
Phenomenon
Both focus on the internal social psychological environment as a
holistic, collectively defined social context
Central Theoretical
issues
Shared dilemma: context is created by interaction, but context
determines interaction
Definition of domain varies greatly by individual theorist
Dynamics between the whole and its parts
Content & Substance High overlap between the dimensions studied by quantitative culture
research and earlier studies by climate researchers
Epistemology &
Methods
Recent emergence of quantitative culture studies and qualitative
climate studies
Theoretical
Foundations
Roots of culture research are social constructionism; Roots of climate
research are Lewinian, but many recent studies have crossed or
combined these traditions (Table 1 & Table 2 combined from Denison, 1996)
It is essential to note that upon reviewing the recent [mid-90s] literature on culture, Denison
(1996) found that the methods and epistemology were similar and almost indistinguishable from
climate literature of the 1960‘s and 1970‘s concluding that these studies mistakenly use the terms
culture and climate interchangeably. Finally, Denison (1996) concludes that although the two
traditions should be viewed as having major differences in interpretation, there is not a difference
in the phenomenon under study. Both focus on the internal social psychological environment as a
holistic, collectively defined social context. The implications of these findings suggest that
organizational climate and culture could be seen as interchangeable sub-elements within the

45
PARiHS framework. In essence, if context is being studied through observational methods with a
symbolic interactionist perspective the element under study should be culture. If context is being
evaluated through the use of an interview or survey that relies on the perspective of individuals,
the concept of organizational climate should be used.
3.3.2.2.1Context Toolbox: Organizational Readiness for Change - Organizational Climate
Domain
An example of a climate questionnaire that could be used is the Organizational Readiness
for Change (ORC) assessment which focuses on organizational traits that predict program
change. In a recent review of 43 instruments measuring organizational readiness for change
Weiner et al (2008) found that the ORC met all six measures of validity (content, predictive,
concurrent, convergent, discriminant) and reliability. The ORC includes scales for four major
domains—motivation readiness, institutional resources, staff attributes, and climate. The
organizational climate domain includes six sub-scales rated using 5-point response categories
(disagree strongly, disagree, uncertain, agree, agree strongly). These scales include: 1) Mission,
which captures staff awareness of agency mission and clarity of its goals; 2) Cohesion, which
focuses on workgroup trust and cooperation; 3) Autonomy addresses the freedom and latitude
staff members have in doing their jobs ; 4) Communication focuses on the adequacy of
information networks to keep staff informed and having bidirectional interactions with
leadership; 5) Stress measures perceived strain, stress, and role overload; and 6) Change
represents staff attitudes about agency openness and efforts in keeping up with changes that are
needed. A comparison between PARiHS‘s defining characteristics of culture (McCormack et al.
2002) and items included in the ORC Climate Sub-scale(Lehman et al. 2002) (Table 8)
demonstrates a clear convergence on constructs.
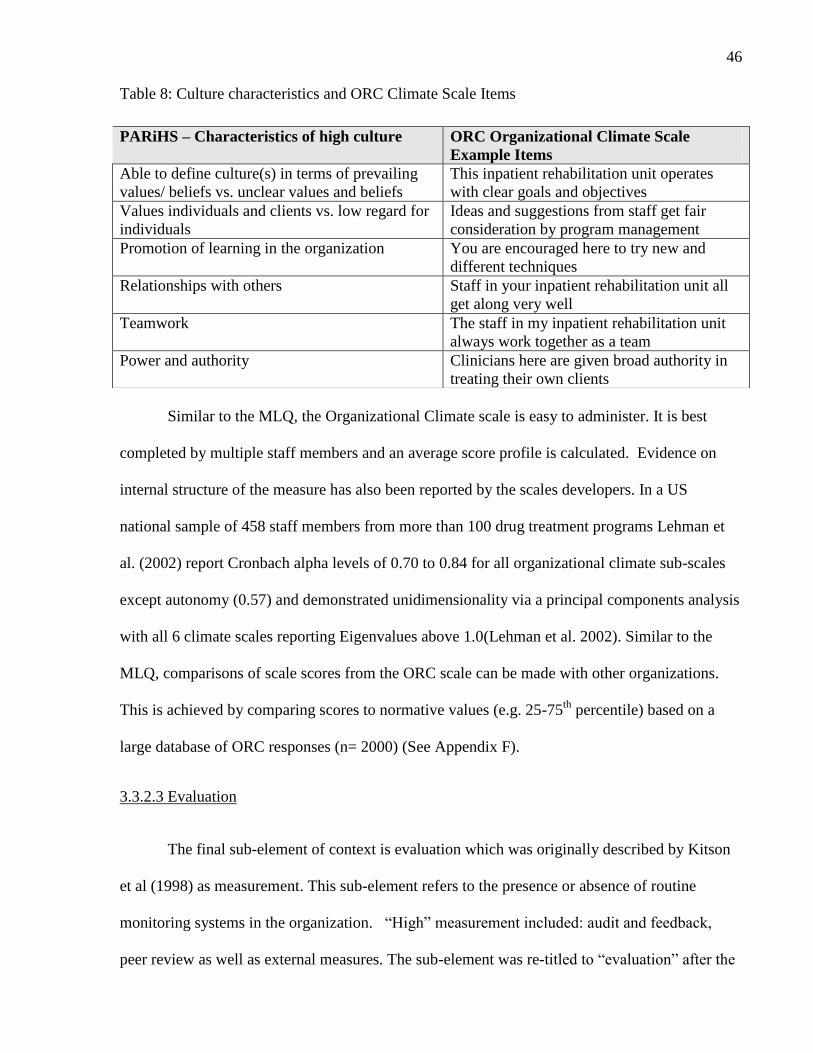
46
Table 8: Culture characteristics and ORC Climate Scale Items
Similar to the MLQ, the Organizational Climate scale is easy to administer. It is best
completed by multiple staff members and an average score profile is calculated. Evidence on
internal structure of the measure has also been reported by the scales developers. In a US
national sample of 458 staff members from more than 100 drug treatment programs Lehman et
al. (2002) report Cronbach alpha levels of 0.70 to 0.84 for all organizational climate sub-scales
except autonomy (0.57) and demonstrated unidimensionality via a principal components analysis
with all 6 climate scales reporting Eigenvalues above 1.0(Lehman et al. 2002). Similar to the
MLQ, comparisons of scale scores from the ORC scale can be made with other organizations.
This is achieved by comparing scores to normative values (e.g. 25-75th
percentile) based on a
large database of ORC responses (n= 2000) (See Appendix F).
3.3.2.3 Evaluation
The final sub-element of context is evaluation which was originally described by Kitson
et al (1998) as measurement. This sub-element refers to the presence or absence of routine
monitoring systems in the organization. ―High‖ measurement included: audit and feedback,
peer review as well as external measures. The sub-element was re-titled to ―evaluation‖ after the
PARiHS – Characteristics of high culture ORC Organizational Climate Scale
Example Items
Able to define culture(s) in terms of prevailing
values/ beliefs vs. unclear values and beliefs
This inpatient rehabilitation unit operates
with clear goals and objectives
Values individuals and clients vs. low regard for
individuals
Ideas and suggestions from staff get fair
consideration by program management
Promotion of learning in the organization You are encouraged here to try new and
different techniques
Relationships with others Staff in your inpatient rehabilitation unit all
get along very well
Teamwork The staff in my inpatient rehabilitation unit
always work together as a team
Power and authority Clinicians here are given broad authority in
treating their own clients

47
concept review by Rycroft-Malone and colleagues (2002) and expanded to include feedback on
multiple levels (individual, team and system); multiple sources for performance and finally
multiple methods (clinical, performance, economic, experience).
Kitson‘s (2008) diagnostic and evaluative tool included statements such as ―we have
routine mechanisms in place to collect data on: individual performance, team performance, and
system performance‖. A similar item was included in Bahtsevani et al (2008) test-retest
evaluation of their instrument to assess implementation of clinical practice guidelines, ―There is
feedback on individual, team, and system performance‖ but this item demonstrated only
moderate agreement (kappa = 0.459) and 73 percent concordance. Furthermore, respondents
reported difficulty with the terminology of these items. Therefore, we suggest a simpler measure
of evaluation should be included in the proposed toolbox.
3.3.2.3.1 Context Toolbox: Fracture Fighters Process Indicators
The Fracture Fighters initiative included a number of evaluation phases and feedback
activities including: an environmental scan at baseline to determine current osteoporosis best
practices, an advisory committee, audit checklists, distribution of newsletters, updating their unit
manager; and patient survey phase. To assess the sub-element of evaluation, process indicators
for participation in these phases and completion of specific activities could be assessed through a
series of simple dichotomous (yes/no) questions to describe evaluation across participating
inpatient rehabilitation units. Alternatively, audit documentation could be used to determine the
evaluation activities completed by each organization. These measures are primarily related to
team performance and do not focus on individual or system level process indicators nor are they
inclusive of structural or outcome indicators.

48
3.3.3 Facilitation
Facilitation is the final element of the PARiHS framework and is defined as a technique
by which one person makes things easier for others (Kitson et al. 1998). Further, facilitators are
described as individuals who help others towards achieving particular goals, provide
encouragement to others and promote action (Harvey et al. 2002). In 2002, Harvey et al revisited
the PARiHS framework to further define the concept of facilitation. They identified three
models of facilitation: 1) co-creation of knowledge through critical reflection and dialogue
between practitioner (learner) and the experienced facilitator; 2) achievement of specific goals
(implementing standards and audits in practice); and 3) a hybrid model where the purpose of
facilitation is to achieve specific goals and the development of processes to enable effective
teamwork, leading them to conclude that there is a facilitation continuum which ranged from
task specific to holistic (Harvey et al. 2002). Harvey (2002) also suggested that the roles as well
as skills and attributes of a facilitator are related to the purpose of facilitation.
There are a variety of terms in the literature used to describe these individuals who have a
role in facilitating the use of research in practice: opinion leaders, champions, change agents,
educational outreach workers, linking agents and facilitators. Opinion leaders (Rogers 1995),
1995) are influential individuals as others in the social system usually follow their example.
Titler (2007) elaborated that opinion leaders are people from the local peer group, viewed by
their associates as respected sources of influence and who are technically competent and have a
broader span of influence across units or clinics. Thompson et al. (2006) agreed that in all cases
opinion leaders have the ability to persuade others but also distinguished expert opinion leaders
in addition to peer leaders. Expert opinion leaders exert their influence through authority and
status, whereas peer opinion leaders exert their influence through their representativeness and
credibility (Greenhalgh et al. 2004).

49
Titler (2007) distinguished opinion leaders from ―change champions‖ who are
practitioners within the local group setting. They are expert clinicians, passionate about the
innovation and committed to improving the quality of care. Champions are individuals who are
internal to an organization who emerge unsolicited from any level in the organization. They
advocate for new ideas and projects and have the ability to influence others to support projects.
Their distinguishing characteristic is their overwhelming enthusiasm and visionary qualities.
Educational outreach workers, are ―topic experts‖ that are external to the practice setting and
knowledgeable about the research. This person meets with practitioners in their setting to provide
information about the research and may also provide feedback on provider or team performance
(Titler 2007). Change agents can be internal or external to an organization. To be effective they
must have strong interpersonal and communication skills as well as be able to earn the trust and
respect of the individuals they are trying to influence (Thompson et al. 2006). Shirley (2006)
describes that nurses could potentially play multiple roles as champions, change agents or
opinion leaders. Although the terms to describe these individuals seem to be conceptually
unique, there are two underlying similarities. The first is the assumption that through facilitation,
increasing knowledge will lead to behaviour change and second that each role is a form or type
of change agent (Thompson et al. 2006).
3.3.3.1 Facilitation Toolbox: Opinion Leadership Scale and Champion Behavior Measure
For the Fracture Fighters program, two scales were selected for inclusion in the PARiHS
toolbox, one is a self-rated measure that identifies Opinion Leaders and the second identifies
three champion behaviours associated with increased innovation success. These scales were
selected based on the purpose and roles that were expected of Clinical Coaches, someone who
influences others and whom others follow their example (opinion leader) and expert clinicians
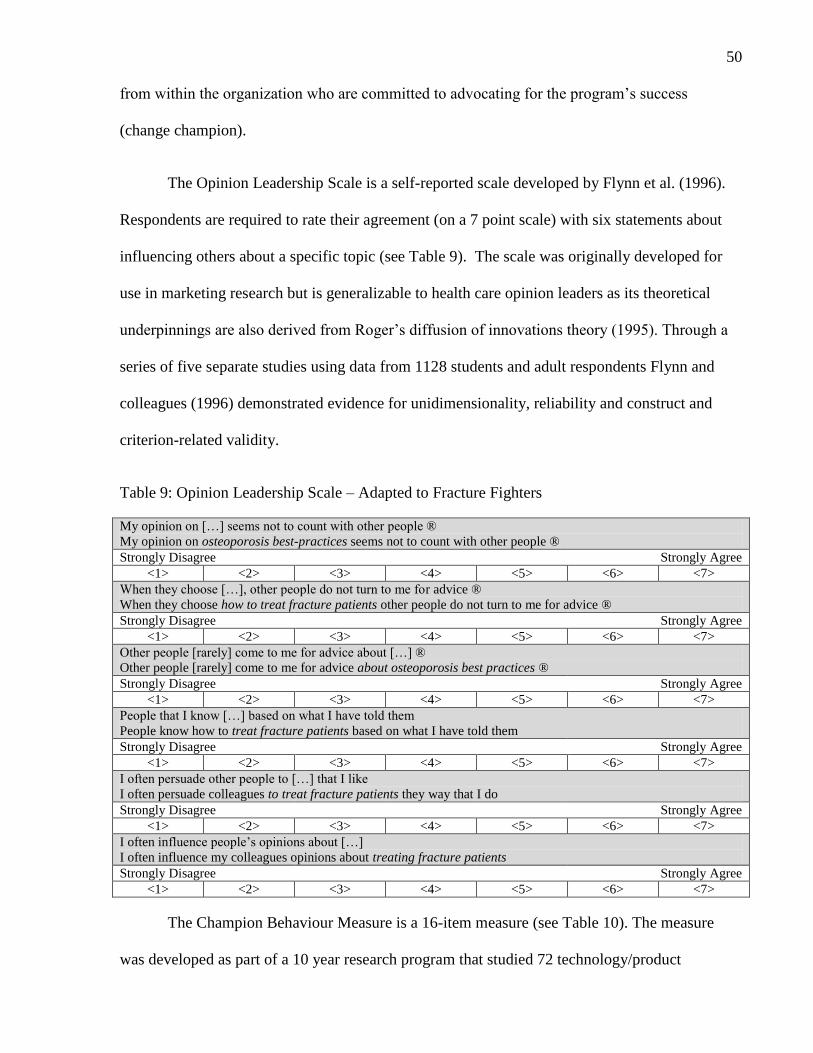
50
from within the organization who are committed to advocating for the program‘s success
(change champion).
The Opinion Leadership Scale is a self-reported scale developed by Flynn et al. (1996).
Respondents are required to rate their agreement (on a 7 point scale) with six statements about
influencing others about a specific topic (see Table 9). The scale was originally developed for
use in marketing research but is generalizable to health care opinion leaders as its theoretical
underpinnings are also derived from Roger‘s diffusion of innovations theory (1995). Through a
series of five separate studies using data from 1128 students and adult respondents Flynn and
colleagues (1996) demonstrated evidence for unidimensionality, reliability and construct and
criterion-related validity.
Table 9: Opinion Leadership Scale – Adapted to Fracture Fighters
My opinion on […] seems not to count with other people ®
My opinion on osteoporosis best-practices seems not to count with other people ®
Strongly Disagree Strongly Agree
<1> <2> <3> <4> <5> <6> <7>
When they choose […], other people do not turn to me for advice ®
When they choose how to treat fracture patients other people do not turn to me for advice ®
Strongly Disagree Strongly Agree
<1> <2> <3> <4> <5> <6> <7>
Other people [rarely] come to me for advice about […] ®
Other people [rarely] come to me for advice about osteoporosis best practices ®
Strongly Disagree Strongly Agree
<1> <2> <3> <4> <5> <6> <7>
People that I know […] based on what I have told them
People know how to treat fracture patients based on what I have told them
Strongly Disagree Strongly Agree
<1> <2> <3> <4> <5> <6> <7>
I often persuade other people to […] that I like
I often persuade colleagues to treat fracture patients they way that I do
Strongly Disagree Strongly Agree
<1> <2> <3> <4> <5> <6> <7>
I often influence people‘s opinions about […]
I often influence my colleagues opinions about treating fracture patients
Strongly Disagree Strongly Agree
<1> <2> <3> <4> <5> <6> <7>
The Champion Behaviour Measure is a 16-item measure (see Table 10). The measure
was developed as part of a 10 year research program that studied 72 technology/product

51
innovations in 38 companies (Howell 2005). In an analysis by Howell et al (2005) this measure
showed acceptable reliability (Cronbach alpha 0.83 – 0.91) as well as convergent (moderate
average correlation of 0.56) and discriminant validity (low correlations with risk taking and
innovativeness, ranging from 0.03 to 0.14). The measure can be completed by sub-ordinates,
same level or superiors. It can also be re-worded to obtain self-report. Mean scores are calculated
for the following behaviours: 1) demonstrating conviction in the innovation; 2) Building
involvement and support; and 3) Persisting under adversity.
Table 10: The Champion Behaviour Measure – Adapted to Fracture Fighters
(Name of Coach) Demonstrates conviction in the Fracture Fighters Program
1. Expresses confidence in what the innovation can do
Expresses confidence in what the Fracture Fighters program can do 0 1 2 3 4
2. Point out reasons why the innovation will success
Points out reasons why the Fracture Fighters program will succeed 0 1 2 3 4
3. Enthusiastically promotes the innovation‘s advantages
Enthusiastically promotes the Fracture Fighters program‘s advantages 0 1 2 3 4
4. Expresses strong conviction about the innovation
Expresses strong conviction about the Fracture Fighters program 0 1 2 3 4
5. Keeps pushing enthusiastically
Keeps pushing enthusiastically for the Fracture Fighters program 0 1 2 3 4
6. Shows optimism about the success of the innovation
Shows optimism about the success of the Fracture Fighters program 0 1 2 3 4
(Name of Coach) Builds involvement and support
7. Gets the key decision makers involved
Gets the key decision makers involved 0 1 2 3 4
8. Secures the top level support required
Secures the top level support required 0 1 2 3 4
9. Gets problems into the hands of those who can solve them
Gets problems into the hands of those who can solve them 0 1 2 3 4
10. Gets the right people involved in the innovation
Gets the right people involved in the program 0 1 2 3 4
11. Makes improvements based on feedback received
Makes improvements based on feedback received 0 1 2 3 4
(Name of Coach) Persists under adversity
12. Persists in the face of adversity
Persists in the face of adversity 0 1 2 3 4
13. Does not give up when others say it cannot be done
Does not give up when others say it cannot be done 0 1 2 3 4
14. Sticks with it
Sticks with it 0 1 2 3 4
15. Knocks down barriers to the innovation
Knocks down barriers to implementing the Fracture Fighters program 0 1 2 3 4
16. Shows tenacity in overcoming obstacles
Shows tenacity in overcoming obstacles 0 1 2 3 4
Not at All Frequently, if not always
<0> <1> <2> <3> <4>

52
Figure 7 presents a summary of the proposed PARiHS toolbox.
Figure 7: The Proposed PARiHS Toolbox
3.4 DISCUSSION
The assembly of the PARiHS toolbox is a first step towards providing further validation
of the framework. Through the application of the toolbox measures, investigators will be able to
examine associations between the PARiHS elements and successful implementation. The
advantage of utilizing the PARiHS toolbox is not only the inclusion of organizational level
factors in the analysis, but that the scales included to measure contextual factors (leadership,
climate) also identify areas that can be modified. The inclusion of these measures allows the
proposed toolbox to be used in implementation planning as well. For example, the MLQ Form
5X, provides scores on nine leadership behaviours which can be compared to a standardized
score profile (See Appendix F). Leaders can identify their deficiencies or perceived deficiencies
and identify the specific areas that require improvement. For example, a leader who scores low
on individual consideration behaviour may need to actively work towards treating staff members
IMPLEMENTATION SUCCESS
Fracture Fighters Best Practices
EVIDENCE
CONTEXT
FACILITATION
RESEARCH
Kitson et al 2008: q 1-5
CLINICAL
EXPERIENCE
Kitson et al 2008: q 6-12
PATIENT
EXPERIENCE
Kitson et al 2008: q 13-13
LEADERSHIP
Multifactor Leadership
Questionnaire
CLIMATE
Organizational Readiness
for Change Climate Scale
EVALUATION
Fracture Fighters
Process Indicators
Champion Behavior
Measure
Opinion Leadership Scale

53
as individuals rather than just a member of the group (Bass and Avolio 1994). This includes
providing more time for one-on-one mentoring, delegating work to individual staff members
based on their interests and strengths (Bass and Avolio 1994) and verbalizing thankfulness and
gratitude for individual contributions, suggestions and input (Bally 2007). Another example is
the ORC Climate scale‘s ―mapping‖ tool (Dansereau and Simpson 2006) which can be used to
match barriers with implementation strategies. The ORC is intended for use by teams planning to
implement new programs. The maps enable identification of potential problems, and suggest
discussion activities for teams and managers to work through to ensure organizational climate
barriers are addressed prior to implementation (Dansereau and Simpson 2006). Courtney et al.
(2007) demonstrated that providing program directors and clinical supervisors ORC scores
during a feedback session was predictive of engagement in strategies to improve low rated
climate indicators. The inclusion of specific tools and strategies to address the contextual barriers
identified by this proposed PARiHS toolbox fills a need that has not been addressed in prior
studies. Dijkstra (2006) completed a meta-analysis of organizational characteristics to describe
their effect on clinical guidelines and discovered there was limited advice on tailoring strategies
to address organizational level barriers, despite the increased importance given to tailoring in the
literature.
An additional benefit of the proposed PARiHS toolbox, is it will allow future studies to
provide quantitative validation of the framework. To date, only two other investigators have
published quantitative findings based on the PARiHS framework. In two studies, Estabrooks
(2007) and Cummings (2007) used single items measures of culture (freedom to make important
patients care and work decisions), leadership (a nurse manager or immediate supervisor who is a
good manager and leader), evaluation (praise and recognition for a job well done), and
facilitation (opportunity for staff nurses to consult with clinical nurse specialist or expert

54
nurse/clinician experts) to determine the association of context and facilitation with research use
in nursing. Although both studies provided evidence that there is a dose-response relationship
between context and research use their usefulness to inform implementation planning is limited
due to narrowly defined context measures. Similarly, a subsequent study Estabrooks (2008),
used the Nursing Unit Culture assessment tool (co-worker support, questioning behaviour,
continuing education, work creativity, work efficiency) to study the relationship between context
and research use in seven patient care units, but once again this only linked a composite score to
outcomes.
Although all three quantitative studies demonstrated support for the PARiHS framework,
the measures of context were specifically designed for and administered with nurses. Thomas
and colleagues (1999), in their search for primary studies to conduct a systematic review to
evaluate the effectiveness of practice guidelines in professions allied to medicine, could not
locate such studies in rehabilitation. Sudsawad (2007) also cautions about the applicability of
findings from other healthcare fields, such as nursing and medicine, because of the differences in
practice focus, culture, methods and contexts. Currently, the proposed PARiHS toolbox is non-
specific for any health professional discipline and could be applied and tested in a variety of
health care settings with a mix of health professionals. However, knowledge translation
interventions may have different effectiveness based on the intervention target (Shojania and
Grimshaw 2005). Most likely, the toolbox would be useful in settings where there are teams of
health professionals rather than primary care settings, however, further exploration in this area is
warranted.
In summary, the application of the proposed PARiHS toolbox is two-fold. First, the
toolbox could be utilized to provide further evidence to validate the PARiHS framework, by

55
demonstrating a relationship between implementation success and the framework elements.
Second, the proposed PARiHS toolbox could be used by organizations or teams planning to
implement new programs or change. By completing the PARiHS toolbox organizations can
identify specific strengths or weakness of the organizational context that can be targeted as part
of the implementation plan. A strength of our approach is that the toolbox scales provide specific
information on strategies for addressing weaknesses in leadership, climate and facilitation.
3.4.1 Limitations
The majority of the measures selected for inclusion in the proposed toolbox have
evidence of good psychometric validity. However, there are potential limitations of the items
included for evaluation and evidence. The evaluation questions were selected based on the
project-specific process indicators put in place by the Fracture Fighters program and only
captured team performance. The PARiHS definition of the evaluation sub-element also suggests
that assessment is required at the individual and system level. The statements proposed by Kitson
et al (2008) are more inclusive of evaluation at multiple levels but require further validation and
feasibility testing prior to application. A potential improvement could include a chart audit as a
method to assess evaluation. Similarly, the statements included for the element ‗evidence‘ will
require psychometric testing to ensure item and scale validity. Future improvements to the
proposed toolbox could include a more comprehensive measure of evaluation and evidence of
the validity to assess these constructs.
Since the completion of this study, McCormack and colleagues (2009) have published the
Context Assessment Index (CAI). The CAI was developed and validated through a 5-step
process with continence nurse specialists based on the PARiHS framework. To the author‘s
knowledge, no studies have been published utilizing the CAI instrument. The purpose of the tool

56
is to enable nurses to understand their context prior to program implementation and is intended
for implementation planning (McCormack et al. 2009). However, unlike the proposed PARiHS
toolbox, the CAI reports global measures (e.g. context, leadership, culture and evaluation) and
identifiable traits (e.g. specific leadership behaviour) are not linked to specific strategies for
addressing the contextual barriers identified. This is a limitation of the CAI in that it will be
unclear which of the context specific or organizational components of the intervention (e.g.
leadership, climate) are contributing to a difference. Furthermore, the CAI neglects the elements
of evidence and facilitation leaving it as an incomplete measurement tool for the full PARIHS
framework.
Our next steps include applying the PARiHS toolbox to the Fracture Fighters program to
determine the relationship between implementation success and ratings on the evidence, context
and facilitation scales. This will potentially provide further evidence for the validity of the
PARiHS framework in addition to the qualitative applications already published. In addition, it
will enable further refinements to the PARiHS model in terms of which aspects of the elements
(e.g. specific leadership behaviours) are driving successful implementation.
3.5 CONCLUSION
The trend in implementation research is moving towards the inclusion of contextual
factors to explain the ability to increase research use in clinical practice. The toolbox presented
in this discussion will enable further steps to be taken to validate the PARiHS framework which
claims that implementation success is a function of strong evidence, context and facilitation.
Furthermore, the toolbox proposed could be utilized to assess organizational level barriers and
facilitators during the implementation planning stage.

57
Chapter 4: Leadership, Organizational Climate and Facilitation: A Survey of Inpatient
Rehabilitation Units in Ontario
In Chapter 3, the Promoting Action on Research Implementation in Health Services
Framework was operationalized for application to the Fracture Fighters program. The PARiHS
elements and sub-elements were re-defined for application in this quantitative study. A toolbox
of measures was assembled to enable quantification of each sub-element within the framework.
Chapter 4 will report the results of the questionnaire administered in inpatient rehabilitation units
participating in the Fracture Fighters program in manuscript form.

58
CHAPTER 4: MANUSCRIPT 2
TITLE: Leadership, Organizational Climate and Facilitation: A Survey of Inpatient
Rehabilitation Units in Ontario
4.1 ABSTRACT
Background: Thirty-six inpatient rehabilitation units in Ontario enrolled in a best-practice
program to integrate osteoporosis management into fracture care protocols. Program evaluation
indicated a variable level of success implementing the program across units.
Objective: To apply the Promoting Action on Research Implementation in Health Services
(PARiHS) Framework toolbox to the Fracture Fighters program to describe context (leadership
behaviours and organizational climate traits) and facilitation (championship behaviours and
opinion leadership) factors that may have influenced implementation success.
Method: Cross-sectional surveys with clinicians responsible for championing program
implementation (Clinical Coaches) and their unit managers.
Results: Questionnaires were completed by Clinical Coaches (n=20) and managers (n=22)
representing 76% of enrolled units. Forty-five percent of units successfully implemented five
minimally required osteoporosis best-practices. Leadership behaviours of managers varied across
units, with clinical coaches reporting the presence of 5 (30%); 1-4 (45%); and no (25%)
transformational leadership behaviors. Indicators for organizational climate also ranged across
units: 10% of units received positive scores on all 6 climate traits (mission, autonomy, cohesion,
communication, change and stress), 20% on 4-5 traits, 40% on 1-3 traits and 30% rated poorly
on all traits. Finally, the mean opinion leadership score was 3.9+ 1.2 and 59% of Clinical
Coaches exhibited all three championship behaviours, while 36% displayed none. Inpatient

59
rehabilitation units that successfully implemented all best-practices had higher mean scores on
all measures of transformational leadership behaviour, climate and facilitation. Odds ratios
indicated an increased effect of intellectual stimulation leadership behaviour (2.1); mission (3.5),
cohesion (2.4) and change (3.6) organizational climate scores; and opinion leadership (1.7) on
successful implementation. The odds of implementation failure doubled with laissez-faire
behaviour.
Conclusion: Application of the PARiHS toolbox demonstrated that contextual factors such as
leadership and organizational climate were dissimilar across inpatient rehabilitation units. This
indicates the importance of considering contextual factors along with individual level factors
prior to implementation.
(Words: 305)
Key Words: PARiHS framework, leadership, organizational climate, champion, osteoporosis,
fracture, survey, inpatient rehabilitation, implementation

60
4.2 INTRODUCTION
Clinical practice guidelines have stressed the importance of osteoporosis assessment and
management following a fracture since prior fracture is a major risk factor for future fracture and
osteoporosis (Brown and Josse 2002; Khan et al. 2007). In spite of these recommendations, the
majority of at-risk individuals continue to be under-investigated and treated (Elliot-Gibson et al.
2004; Giangregorio et al. 2006; Bessette et al. 2008; Papaioannou et al. 2008). Recently, the
Ontario Ministry of Health and Long-Term care funded a provincial wide strategy to improve
osteoporosis prevention and management. Fracture Fighters was one of the programs funded in
the inpatient rehabilitation setting to improve post-fracture osteoporosis investigation and
management. The Fracture Fighters program used a multi-component approach that centred on
the use of trained front-line clinicians (clinical coaches) to facilitate integration of osteoporosis
management into existing inpatient rehabilitation services. Other components of the program
included patient and provider educational materials, audit checklists, program newsletters and a
clinical coach advisory panel.
Table 11: Percent of Inpatient Rehabilitation Units Implementing Selected Best Practices (Jaglal
et al. 2008)
Osteoporosis Best Practice Baseline (% of sites) 6-months (% of sites)
Osteoporosis education 23 77
Supplements (Vitamin D and Calcium) 17 50
Osteoporosis medication 22 47
BMD testing 9 25
Referral to GP for osteoporosis follow-up 0 42
Although a survey of participating sites at six months demonstrated positive
improvements across a number of best-practice categories (see Table 11), not all participating
sites were providing education about osteoporosis and supplement use and referring patients for

61
osteoporosis follow-up demonstrating less than optimal care in some inpatient rehabilitation
units. This situation is not unique to the Fracture Fighters program. A number of reviews of
implementation research have consistently shown the majority of interventions can achieve
moderate improvements in care (Oxman et al. 1995; Bero et al. 1998; Grimshaw, Thomas et al.
2004), but with considerable variation in the observed effects across studies. Eccles et al (2005),
suggest that a possible explanation may be differences in the context. Increasingly, investigators
have begun to acknowledge the importance of contextual factors in achieving successful
implementation (Cummings et al. 2004). However, since few studies provide contextual data the
contribution of these factors is not known.
One framework describing implementation success in health care organizations that takes
into account the influence of context has been developed by Kitson and colleagues (1998). The
Promoting Action on Research Implementation in Health Services (PARiHS) framework (Figure
8) indicates that successful implementation is a function of three elements: 1) evidence 2)
context and 3) facilitation. Through a series of case studies, Kitson et al (1998) demonstrated
that the most successful implementation occurs when: 1) the evidence is scientifically robust and
matches professional consensus and patient needs ("high" evidence) 2) the context is receptive
to
change with sympathetic cultures, strong leadership, and appropriate monitoring and feedback
systems ("high" context) and 3) there is appropriate facilitation of change with input
from skilled
external and internal facilitators ("high" facilitation) (Rycroft-Malone et al. 2002). To date
several qualitative studies have used the PARiHS framework to inform the development of
knowledge translation interventions (Ellis et al. 2005; Wallin et al. 2005; Doran and Sidani 2007)
and to refine implementation models and guiding frameworks (Doran and Sidani 2007; Conklin
and Stolee 2008). Several have also used the framework to guide descriptions of research use and
implementation (Sharp et al. 2004; Brown and McCormack 2005; Ellis et al. 2005; Meijers et al.

62
2006; Doran and Sidani 2007) compared to few quantitative studies that examined research use
(Cummings et al. 2007; Estabrooks 2007; Estabrooks et al. 2008).
FA
CIL
ITA
TIO
N
CO
NT
EX
T
EV
IDE
NC
E
Implementation Success = f (Evidence, Context, Facilitation)
RESEARCH
CLINICAL
EXPERIENCE
PATIENT
EXPERIENCE
LEADERSHIP
CULTURE
EVALUATION
PURPOSE
ROLES
SKILLS &
ATTIBUTES
Figure 8: Promoting Action on Research Implementation in Health Services Framework
This study aims to apply the Promoting Action on Research Implementation in Health
Services (PARiHS) Framework using a toolbox of measures proposed by us to describe inpatient
rehabilitation units participating in the Fracture Fighters program. The primary objective of this
study is to describe leadership behaviours of inpatient rehabilitation unit managers,
organizational climate traits of inpatient rehabilitation units and championship behaviours of
clinician facilitators. The secondary objective is to identify potential elements that could have
contributed to implementation success of the Fracture Fighters Program.
4.3 METHODS
4.3.1 Assumptions of Fracture Fighters Program based on the PARiHS Framework
Based on the design of the Fracture Fighters program and specific implementation
strategies utilized, the author assumes that several of the PARiHS sub-elements were high: the
research, clinical experience and patient experience sub-elements of evidence and evaluation, a

63
sub-element of context. However, the other sub-elements of context (leadership, organizational
culture) and facilitator skills and attributes were not considered during the program design and
could potentially be the source of variation in implementation success between inpatient
rehabilitation units. These assumptions are briefly described below.
4.3.1.1 Fracture Fighters Evidence
The author assumes the strength of the evidence for Fracture Fighters is high because the
program considered all three sub-elements of research, clinical expertise and patient experience.
All components of the model are based on the Canadian Osteoporosis guidelines (Brown and
Josse 2002) and up-to-date peer-reviewed literature (―high‖ research). The osteoporosis best-
practices are non- invasive or prescriptive to patients (e.g. hand out educational materials) and
patient preference was considered. For example, one best-practice included sending a letter to the
patients‘ family physician to inform them of the fracture. If the patient was uncomfortable with
this notification, clinicians were instructed not to proceed with notification (―high‖ patient
experience). Finally, clinical opinion was considered in each inpatient unit, if clinicians‘
expectations were not in agreement with Fracture Fighters best-practices, expectations for
congruence with these items were modified. For example, the Fracture Fighters advisory group
felt the one-leg balance exercise for patients with hip fractures (a Fracture Fighters exercise best-
practice) was unsafe for some patients, therefore clinicians modified the exercises to include only
sitting or prone exercises (―high‖ clinician experience).
4.3.1.2 Fracture Fighters Context
Leadership in the inpatient rehabilitation units is represented by the unit managers. These
managers had the authority to enrol their inpatient rehabilitation unit in the Fracture Fighters

64
program as well as to decide which clinicians from the unit would be trained as Clinical
Coaches. However the characteristics and leadership behaviours of each manager is currently
unknown and could be a potential source of variability of implementation success across
inpatient rehabilitation units.
The 36 inpatient rehabilitation units are staffed by multidisciplinary teams, however these
team structures vary across the participating organizations in both size and composition.
Disciplines that may have been included in the Fracture Fighters program include: nursing,
physical therapy, occupational therapy, speech-language pathology, general medicine,
orthopaedic surgery and physiatry. The existence of common values and beliefs, collaborative
teamwork and communication among each unit should be examined to determine the impact of
culture or climate variability on Fracture Fighters implementation.
The Fracture Fighters program has built in several mechanisms for measurement and
evaluation which are reported about and to multiple levels. These measurements included a
telephone survey with Clinical Coaches and audit checklists that were faxed back to the
implementation coordinators; and patient surveys to determine outcomes 6 months post-
discharge. The sub-element of evaluation is considered as ‗high‘ for the Fracture Fighters
program and not considered a source of variability for best-practice implementation.
4.3.1.3 Fracture Fighters Facilitation
Facilitation in the Fracture Fighters program was provided by Clinical Coaches.
Conceptually, Clinical Coaches could be viewed as facilitators, change champions, internal
change agents or opinion leaders (Thompson et al. 2006). However, Fracture Fighters did not
provide specific criteria (skills and attributes) for the selection of practitioners who were trained

65
as Clinical Coaches. The only requirement was that they were a health care professional working
in the participating inpatient rehabilitation unit. These individuals were selected by their unit
managers to be trained as Clinical Coaches. The skills and attributes of individual Clinical
Coaches are assumed to be variable across the participating units.
4.3.2 Study Design and Procedures
A cross-sectional survey design was used. Questionnaires and informed consent
packages were mailed to eligible subjects between October 27, 2008 and November 14, 2008.
Non-responders received follow-up phone calls and reminder e-mails 2- and 4- weeks after the
initial mailing with the additional option to complete the survey via telephone as these methods
are expected to increase response rate (Dillman 1978). A second copy of the questionnaire was
mailed eight weeks after the initial mailing. This study received approval from the University of
Toronto Research Ethics Board for Research with Human Subjects (protocol reference #:
23260)(See Appendix D for Informed Consent Materials).
4.3.3 Setting and Participants
At the time of the survey, 36 inpatient rehabilitation units were enrolled in the
provincially sponsored osteoporosis best-practice program called Fracture Fighters. Eligible
participants included clinicians responsible for championing the Fracture Fighters program
implementation and their rehabilitation unit managers. Program champions (known as Clinical
Coaches) were front-line clinicians selected by their unit manager to attend one of seven Fracture
Fighters training workshops (between March – August 2007). They also acted as the primary
contact for the Fracture Fighters program coordinators throughout all stages of implementation
and program evaluation. Individuals who had retired, left their position at the hospital or
transferred to another department or position at the time of data collection were excluded from

66
the study. In total, 30 Clinical Coaches and 35 Managers were mailed an invitation to complete
the questionnaire.
Figure 9: Data Collection Tools: The Proposed PARiHS Toolbox
4.3.4 Measures Applied To PARiHS
Data were collected in the form of two questionnaires (see Figure 9) based on the
Promoting Action on Research Implementation in Health Services framework toolbox (see
Chapter 3). Clinical coaches were surveyed to describe the strength of the Fracture Fighters
evidence, the context of their inpatient rehabilitation unit (leadership, organizational climate,
evaluation) and implementation facilitation. In addition, Clinical Coaches were asked to report
which Fracture Fighters best-practices were routinely incorporated in fracture care in their unit.
The manager questionnaire included self-report scales about their leadership behaviour and
champion behaviours of the Clinical Coach.
IMPLEMENTATION SUCCESS
Fracture Fighters Best Practices
EVIDENCE
CONTEXT
FACILITATION
RESEARCH
Kitson 2008: q 1-5
CLINICAL
EXPERIENCE
Kitson 2008: q 6-12
PATIENT
EXPERIENCE
Kitson 2008: q 13-13
LEADERSHIP
Multifactor Leadership
Questionnaire
CLIMATE
Organizational Readiness
for Change Climate Scale
EVALUATION
Fracture Fighters
Process Indicators
Champion Behavior
Measure
Opinion Leadership Scale

67
4.3.4.1 Evidence: Research, Clinical Experience and Patient Experience
Kitson et al (2008) recently published a set of questions to evaluate the concepts of the
PARiHS framework. No description of how these statements were developed was included.
Although the items have not been tested psychometrically, the items map directly to sub-
elements of research, clinical experience and patient experience and have high face validity. No
scoring for the items was provided with the statements, therefore a standard 5-point Likert scale
was employed (<1> strongly disagree, <2> disagree, <3> neutral, <4> agree, <5> strongly
agree).
4.3.4.2 Context: Leadership Sub-element
The Multifactor Leadership Questionnaire (MLQ Form 5X) is one of the most widely
used instruments to measure transactional and transformational behaviours in the organizational
sciences with proven reliability and validity (Tejeda et al. 2001; Avolio and Bass 2004).
Transformational leaders have the ability to transform cultures to create a context more
conducive to the integration of evidence into practice as opposed to transactional leaders who
―command and control‖ (McCormack et al. 2002). The MLQ (Form 5X) contains 45 items in
total, 36 which correspond to nine leadership factors and includes 1) idealized influence
attributed (IIA) (perceived socialized charisma); 2) Idealized influence behaviour (IIB)
(charismatic actions of the leader); 3) Inspirational motivation (IM) (the ways leaders energize
their followers); 4) Intellectual stimulation (IS) (the way leaders challenge followers to think
and problem solve); 5) Individualized consideration (IC) (extent that advice is individualised to
needs of the follower); 6) Contingent reward (CR) leadership (constructive transactions); 7)
Management-by-exception active (MBEA) (leaders goal is to ensure standards are met); and 8)

68
Management-by-exception passive (MBEP) (leaders intervene only after mistakes have already
happened). Transformational leadership behaviours correspond to factors 1 to 5 and
transactional behaviours with factors 6-8. The ninth factor is nontransactional laissez-faire (LF)
leadership which represents a leader who avoids decisions, relinquishes responsibility and does
not use their authority (Antonakis et al. 2003). Each of the 36 MLQ (Form 5X) items are scored
on a Likert scale from 0 to 4 (<0> not at all; <1> once in awhile; <2> sometimes; <3> fairly
often; <4> frequently if not always). A score was calculated for each of the nine leadership
factors by computing the mean score of the 4 items corresponding to each behaviour. The MLQ
is not intended as a ―classification‖ of leadership type, rather, it describes specific behaviours of
leaders. Scores on individual leadership behaviours can be compared to standardized score
profiles. The score profiles are based on a US database of approximately 27,000 MLQ
respondents (See Appendix F for Percentiles of Individual Scores).
4.3.4.3 Context: Climate Sub-Element
The Organizational Readiness for Change (ORC) assessment focuses on organizational
traits that predict program change (Lehman et al. 2002). The ORC includes scales for four major
domains—motivation, resources, staff attributes, and climate. This study only used the
organizational climate domain which includes six sub-scales rated using 5-point response
categories ranging from 1 disagree strongly to 5 agree strongly. These scales include: 1) Mission,
which captures staff awareness of agency mission and clarity of its goals; 2) Cohesion, which
focuses on workgroup trust and cooperation; 3) Autonomy addresses the freedom and latitude
staff members have in doing their jobs; 4) Communication focuses on the adequacy of
information networks to keep staff informed and having bidirectional interactions with
leadership; 5) Stress measures perceived strain, stress, and role overload; and 6) Change

69
represents staff attitudes about agency openness and efforts in keeping up with changes that are
needed. The climate domain has been shown to have good internal consistency(Lehman et al.
2002). A composite score was computed for each of the six ORC climate traits by taking the
mean of the corresponding sub-scale items. Individual climate trait scores were compared to
normative values (Appendix F).
4.3.4.4 Context: Evaluation Sub-Element
To assess the construct of evaluation, Clinical Coaches were asked to report which
Fracture Fighters evaluation activities each inpatient rehabilitation unit participated in. These
included process indicators for: Completing an environmental scan at baseline to determine
current osteoporosis best practices; Participating in the Fracture Fighters advisory committee;
Completing a minimum of 10 audit checklists; Circulating the Fracture Fighters newsletter;
Providing regular updates to their unit manager; and Participating in the patient survey phase. A
series of dichotomous (yes/no) questions were used to determine which Fracture Fighters
evaluation activities each unit participated in.
4.3.4.5 Facilitation
Two measures were included to measure facilitation in the participating inpatient
rehabilitation units, the Opinion Leadership Scale (Flynn et al. 1996) and the Champion
Behaviour Measure (Howell et al. 2005). The Opinion Leadership Scale is a self-reported scale
developed by Flynn et al. (1996). Respondents are required to rate their agreement (on a 7 point
scale) with 6 statements about influencing others about a specific topic. The scale was originally
developed for use in marketing research but is generalizable to health care opinion leaders as its
theoretical underpinnings are also derived from Roger‘s diffusion of innovations theory

70
(1995)(Rogers 1995). After a correction for reverse coding, scores for each item are summed and
divided by 6 to determine a mean score for opinion leadership.
The Champion Behaviour Measure was completed by the unit managers to assess the
facilitation attributes of the clinical coaches. It is composed of 16-items that correspond to three
sub-scores: 1) Demonstrating conviction in the innovation (items 1 -6); 2) Building involvement
and support (items 7-11); and 3) Persisting under adversity (items 12-16) (Howell et al. 2005).
Each item is scored from 0 <not at all> to 4 <frequently, if not always>. Items corresponding to
each sub-score are tallied and a mean score calculated. This measure has been shown to have
acceptable reliability as well as convergent and discriminant validity (Howell et al. 2005).
4.3.4.6 Implementation Success Indicators
The Fracture Fighters program promoted five best-practices as ―minimal implementation
requirements‖ for successful Fracture Fighters implementation. These included: 1) Providing
osteoporosis education to patients post-fracture; 2) Demonstrating strength, posture, balance and
weight-bearing exercises; 3) Providing nutritional recommendations for vitamin D and calcium;
4) Initiating follow-up for osteoporosis investigation; and 5) Sending a letter to the patients‘
primary care provider for osteoporosis follow-up. Initiation of osteoporosis follow-up
investigation included one or more of: ordering a bone mineral density (BMD) test during the
inpatient stay, ordering a BMD as an outpatient, or sending a recommendation to the patients‘
primary care physician to order a BMD test. Implementation success was defined as the
proportion of units implementing all five best-practice requirements.
Items were included at the end of both questionnaires to evaluate respondent
demographics. See Appendix E for copy of questionnaires.
71
4.3.5 Statistical Analysis
The aim of the analysis plan for this project was three-fold. First, we set out to describe
evidence, context and facilitation across all participating inpatient rehabilitation units. Second,
individual unit scores for each leadership behaviour, climate trait and champion behaviour were
dichotomized to compare contextual and facilitation factors among inpatient rehabilitation units.
Third, we aimed to examine the relationship between leadership behaviours, climate traits and
facilitator behaviours with successful implementation of the Fracture Fighters program. All
statistical analyses were performed using the statistical software package SPSS version 16.0
(Chicago, IL, USA).
1. Overall Description of Inpatient Rehabilitation Units: The mean score and standard
deviation for evidence sub-elements (research, clinical experience, patient experience),
leadership behaviours, organizational climate traits, champion behaviours and opinion
leadership were calculated for inpatient rehabilitation units. Both Clinical Coach and
Manager self-reported scores for leadership behaviours were reported and compared to a
standardized US score profile (see Appendix F) (Avolio and Bass 2004). Organizational
climate trait scores were adjusted (multiplied by a factor of 10) to compare results to
standard score profiles. Frequency distributions were reported for participation in
Fracture Fighters evaluation activities.
2. Comparison Among Inpatient Rehabilitation Units: Dichotomous categories were
assigned for each leadership behaviour score, organizational climate trait and champion
behaviour to generate indicators representing the presence or absence of strong
leadership, organizational climate and facilitation respectively.
a. Leadership behaviour scores ranging from 0 – 2.99 and scores ranging from 3.0 –
4.0 were coded as absent and present respectively for each leadership behaviour.

72
This procedure was carried out for both Clinical Coach and Manager Self-rated
leadership scores. Proportion of overall agreement for leadership behaviours and
attributes was calculated to compare leadership indicators generated from Clinical
Coaches questionnaires and those self-reported by Managers.
b. Indicators for the organizational climate traits of mission, autonomy, cohesion,
communication and change were defined as ―high‖ according to the 75th
percentile of the Organizational Readiness for Change Standardized Score Value
(Lehman, 2002), whereas a cut point of below the 25th
percentile was used for
stress.
c. Finally, indicators for strong implementation facilitation were created by
dichotomizing the three championship behaviour scores (0-2.99 and 3.0-4.0), with
the latter indicating ―strong‖.
3. Association with Implementation Success: The frequency distribution was reported for
individual best practices and implementation success.
a. Mean score and standard deviation was reported for continuous variables (nine
leadership behaviours; six organizational climate traits; and three champion
behaviours) stratified by implementation success.
b. Binary logistic regression was used to explore associations between
implementation success with individual leadership behaviours, climate traits and
champion behaviour scores. The Homer & Lemeshow chi-square test of goodness
of fit was examined to ensure each model adequately fit the data. The regression
analysis was bivariate and unadjusted. Odds ratios and associated 95% confidence
intervals were reported to generate hypothesis regarding the relationship between
these covariates and implementation success.

73
4.4 RESULTS
4.4.1 Response Summary and Demographics
Surveys were administered between October 27, 2008 and January 17, 2009. One
hospital site was excluded prior to survey distribution as both Clinical Coach and Manager had
left their positions in the rehabilitation unit. In four units surveys were completed by Clinical
Coaches only and in six units by Managers only. Data were collected from both the Clinical
Coach and Manager for 16 sites. In total 42 staff members (n=20 Clinical Coaches; n=22
Managers) from 26 units participated in this cross-sectional study, representing 72% of sites
enrolled in the Fracture Fighters program (see Figure 10: response rate flow chart).
Table 12 displays the demographics of Clinical Coach and Manager responders. The
study participants were almost all female (95%) and most had completed some post-secondary
education (90%). Clinical Coach respondents were practicing as physical therapists (65%) and
nurses (30%) and the majority of Managers were trained as nurses (73%).
Table 12: Demographics of Respondents
Clinical Coach Manager
N 20 22
Age (years) 43 + 8.6 51 + 9.0
Gender
Female
Male
20 (100%)
0
20 (91%)
2 (9%)
Profession
Physical Therapist
Nurse (RN/RPN)
Occupational Therapist
Other
13 (65%)
6 (30%)
1 (5%)
-
4 (18%)
16 (73%)
1 (4.5%)
1 (4.5%)
Highest Education
Certificate/Diploma
Bachelors
Masters
4 (20%)
13 (65%)
3 (15%)
0
10 (45%)
12 (55%)
Number of Years in Position
< 5
5-10
11 +
8 (40%)
7 (35%)
5 (25%)
14 (64%)
5 (23%)
3 (14%)

74
Figure 10: Response Rate Flow Chart
Units Enrolled in
Fracture Fighters
(n=36)
Units Eligible for
Survey (n=35)
Excluded Units
(n=1)
Surveys Mailed
to Clinical
Coach (n=30)
Excluded
Clinical
Coaches (n=5)
Surveys Mailed
to Managers
(n=35)
Excluded (n=5)
Declined (n=2)
Unable to Reach
(n=2)
Non-responders
(n=4)
Completed
Manager Survey
(n=22)
Excluded (n=4)
Declined (n=1)
Unable to Reach
(n=2)
Non-responders
(n=3)
Completed
Clinical Coach
Survey (n=20)

75
4.4.2 Survey Results
4.4.2.1Evidence
4.4.2.1.1 Evidence Overall
The mean evidence scores were 4.4 + 0.4, 3.7 +0.7 and 3.7 +0.9 for research, clinical
experience and patient experience respectively for all inpatient rehabilitation units (n=20).
4.4.2.2Context: Leadership
4.4.2.2.1 Leadership Behaviour Overall
The mean leadership behaviour scores as reported by Clinical Coaches (Coach Rating)
and self-reported by Managers (Manager Rating) are displayed in Figure 11. Overall, compared
to standardized percentiles (Appendix F) based on a US sample of approx. 27,000 (Figure 11)
Clinical Coaches rated the transformational behaviours of their managers close to the 50th
percentile for Idealized Influence Attributed (IIA) (2.9), Idealized Influence Behaviour (IIB)(2.8)
and Inspirational Motivation (IM)(3.0) and slightly lower for Intellectual Stimulation (IS)(2.6)
and Individualized Consideration (IC)(2.6) as well as Contingent Rewards (CR) (2.7). However,
Clinical Coaches rated their managers at or above the 70th
percentile for two of the three
transactional behaviours: Management-by-Exception-Active (MBEA) (2.1) and Management-
by-Exception Passive (MBEP)(1.3). Laissez-Faire (LF)(1.0) behaviour was also rated above the
70th
percentile.
Conversely, Managers self-reported their transformational behaviours well above the
standardized mid-point. IIA (3.3) and IIB (3.5) were rated close to the 70th
percentile and IM
(3.6), IS (3.5) and IC (3.5) were rated between the 80-90th
percentile. Contingent reward

76
behaviour (3.3.) was also rated close to the 80th
percentile, but the other two transactional
behaviours (MBEA (2.0); MBEP (0.7)) dropped closer to the normal average. Laissez-faire
behaviour (0.6) was similar to the 50th
percentile score.
Figure 11: Mean Leadership Behaviour Scores of Inpatient Rehabilitation Managers Rated by
Managers and Coaches Compared to US (N=27,285) Normal Percentiles
4.4.2.2.2. Leadership Behaviour by Inpatient Rehabilitation Unit
Leadership behaviour profiles of managers were dissimilar across inpatient rehabilitation
units (Figure 12a and 12b). Thirty percent (6/20) of Clinical Coaches reported their managers
exhibited all five transformational leadership behaviours, another 30% (6/20) reported 3-4
IIA = Idealized influence attributed; IIB = Idealized influence behaviour; IM = Inspirational motivation; IS = Intellectual stimulation; IC = Individualized consideration; CR = Contingent rewards; MBEA = Management-by-exception active; MBEP = Management-by-exception passive; LF = Laissez-faire

77
behaviours, 15% (3/20) reported 2 behaviours and 25% (5/20) said their managers did not exhibit
any transformational behaviours. Idealized influence attributed (IIA) and behaviour (IIB) were
most frequently reported (13/20), while intellectual stimulation (IS) was the lowest (9/20). Of
transactional leadership behaviours, 55% (11/20) of Clinical Coaches reported their manager
used contingent rewards (CR), while three of these also use Management-by-Exception Active
(MBEA). Only 10% (2/20) reported Management-by-Exception Passive (MBEP) behaviour and
30% (6/20) reported no transactional behaviours. No Clinical Coaches reported the presence of
laissez-faire behaviour.

78
Figure 12a: Transformational Leadership Behaviours Present
by Inpatient Rehabilitation Unit (Clinical Coach Respondents)
Figure 12b: Transactional Leadership Behaviours Present by
Inpatient Rehabilitation Unit (Clinical Coach Respondents)
IIA = Idealized influence attributed; IIB = Idealized influence behaviour; IM = Inspirational motivation; IS = Intellectual stimulation; IC = Individualized consideration
CR = Contingent rewards; MBEA = Management-by-exception active; MBEP = Management-by-exception passive

79
It was evident that Managers self-reported a high frequency of transformational
leadership behaviours but their staff (Clinical Coaches) did not concur. Table 13 displays the
percent agreement in rating the presence of leadership behaviours between Clinical Coaches and
Managers from 16 hospital sites. Overall agreement ranged from 44-69% for transformational
behaviours. Contingent rewards and management-by-exception-active were around 50%. The
highest rates of agreement were observed for management-by-exception-passive (94%) and
laissez-faire leadership behaviour (100%).
Table 13: Percent agreement between Coach Rating and Manager Self-Rating of Leadership
Behaviours (N=16)
Leadership
Behaviours
A
Freq. agree
behaviour
absent
B
Disagree
C
Disagree
D
Freq. agree
behaviour
present
%
Agree-
ment
Idealized
Influence
Attributed
1 1 4 10 69%
Idealized
Influence
Behaviour
0 1 5 10 62%
Inspirational
Motivation
0 1 8 7 44%
Intellectual
Stimulation
0 0 8 8 50%
Individualized
Consideration
0 0 8 8 50%
Contingent
Reward
1 2 6 7 50%
Management by
Exception Active
9 4 3 0 56%
Management by
Exception Passive
15 1 0 0 94%
Laissez-faire
Leadership
16 0 0 0 100%

80
4.4.2.3 Context: Organizational Climate
4.4.2.3.1Overall Organizational Climate
The adjusted organizational climate score values were compared to Organizational
Readiness for Change Score Profiles (See Figure 13) (N=2,031; TCU, 2004). Overall Clinical
Coaches reported Organizational Climate scores for Mission (37.8), Cohesion (35.6) and
Communication (34.1) slightly above the normal average, and Stress (30.8) and Change (33.3)
scores slightly below. The mean Autonomy score was the highest (39.9 + 5.3) among all climate
scores and notably above the 75th
percentile of the ORC score profile
Figure 13: Organizational Climate Scores Compared to ORC Score Profiles
4.4.2.3.2 Organizational Climate by Inpatient Rehabilitation Unit
When dichotomous scores were created, individual inpatient rehabilitation units revealed
variation on ratings of six Organizational Climate categories (Figure 14). The presence of an

81
indicator signified a positive organizational climate trait. Only 10% (2/20) of Clinical Coaches
rated their inpatient rehabilitation units highly on all six Organizational Climate traits, an
additional 20% (4/ 20) rated high on 4 or 5 traits and 40% (8/20) rated well on 1-3 traits only.
Thirty percent (6/20) of sites rated poorly on all measures of organizational climate. Autonomy
and Stress were present most frequently (n=9) and Change was the lowest with only five Clinical
Coaches indicating this trait was present in their unit.
Figure 14: Organizational Climate Traits Present by Inpatient Rehabilitation Unit
*Stress score < 25th
%ile

82
4.4.2.4 Facilitation
4.4.2.4.1 Facilitation Overall
Clinical Coaches self-reported on Opinion Leadership, their mean score on the 6-item
scale was 3.9 + 1.2. The overall mean scores for champion behaviour are reported in Table 14
Table 14: Champion Behaviour Scores for Inpatient Rehabilitation Units (n=22)
Champion Behaviour Mean + SD
Demonstrates conviction about the Fracture
Fighters Program
2.8 + 1.5
Builds involvement and support 2.7 + 1.5
Persists under adversity 2.7 + 1.5
4.4.2.4.2 Facilitation by Inpatient Rehabilitation Unit
Managers (n=22) reported the Champion Behaviours of Clinical Coaches and 13 of 22
(59%) indicated that all three Champion Behaviours were present and 8 of 22 (36%) indicated
that no behaviours were present demonstrating the inconsistency of facilitation across inpatient
rehabilitation units.
4.4.2.5 Implementation Success
Seventeen (85%) inpatient rehabilitation units were incorporating one or more of the
osteoporosis assessment and management best-practices in routine care for patients with fracture
(Table 15). Only 3 sites (15%) reported that none of the best-practice strategies were
implemented. However, only 9 (45%) sites successfully implemented all five of the minimal
best-practice requirements.

83
Table 15: Success Indicators: Best Practice Implementation by Site (N=20)
Minimal Requirements for Post-Fracture Care YES NO
Provide Osteoporosis Education 16 (80%) 4 (20%)
Demonstrate Osteoporosis Exercises 15 (75%) 5 (25%)
Discuss Dietary or Supplemental Calcium & Vitamin D 14 (70%) 6 (30%)
Arranged Bone Mineral Density Test 14 (70%) 6 (30%)
Send letter to Primary Care Physician for Osteoporosis
follow-up
13 (65%) 7 (35%)
Global Success Indicator – 5 Minimal Best-Practices
Implemented
9 (45%) 11 (55%)
4.4.2.5.1 Relationship between Implementation Success and PARiHS Sub-Elements
The mean scores for leadership, organizational climate and facilitation stratified by
implementation success are presented in Tables 16 and 17. Table 16 presents data collected from
Clinical Coaches (n = 20) and Table 17 presents scores reported by Inpatient Rehabilitation
Managers (n = 22). Inpatient rehabilitation units that successfully implemented all minimal best-
practices had a higher mean score than those who failed to implement the program on all
measures of organizational climate, transformational leadership behaviours and facilitation
(Table 16 and 17). In addition, they scored higher on two transactional leadership behaviours
(contingent rewards and management-by-exception active) and lower on management-by-
exception passive and lassez faire leadership behaviours. There were no statistically significant
differences (p< 0.05) in scores between those who successfully implemented best practices
compared to those who were not.

84
Table 16: Coach Reported Leadership Behaviours, Organizational Climate and Facilitation
All Sites (N=20)
Mean + SD
Success (N=9)
Mean + SD
Failed (n = 11)
Mean + SD
MLQ Leadership Behaviours (score range 0-4)
Transformational Behaviours
Idealized Influence Attributed 2.9 + 0.94 3.0 + 0.65 2.8 + 1.15
Idealized Influence Behavior 2.8 + 0.88 2.9 + 0.88 2.7 + 0.91
Inspirational Motivation 3.0 + 0.85 3.1 + 0.70 2.8 + 0.97
Intellectual Stimulation 2.6 + 0.81 2.8 + 0.55 2.4 + 0.96
Individualized Consideration 2.6 + 1.10 2.7 + 1.08 2.5 + 1.17
Transactional Behaviours
Contingent Reward 2.7 + 0.90 2.8 + 0.77 2.6 + 1.02
Management by Exception Active 2.1 + 0.89 2.3 + 0.84 2.0 + 0.95
Management by Exception Passive 1.3 + 0.99 1.3 + 0.94 1.3 + 1.06
Laissez-Faire Behaviour
Laissez-faire Leadership 1.0 + 0.78 0.8 + 0.81 1.1 + 0.75
ORC Organizational Climate (score range 1-5)
Mission Score 3.8 + 0.60 4.0 + 0.40 3.6 + 0.70
Cohesion Score 3.6 + 0.77 3.8 + 0.77 3.4 + 0.74
Autonomy Score 4.0 + 0.53 4.0 + 0.59 4.0 + 0.50
Communication Score 3.4 + 0.69 3.7 + 0.81 3.2 + 0.51
Stress Score 3.1 + 0.88 3.2 + 0.70 3.0 + 1.02
Change Score 3.3 + 0.62 3.6 + 0.68 3.2 + 0.53
Opinion Leadership (score range 1-7)
Score 3.9 + 1.23 4.3 + 1.29 3.6 + 1.14
Table 17: Manager Reported Facilitation
Championship Behaviours (0-4) Mean + SD
N=16
Success (n=8)
Mean + SD
Failed (n = 8)
Mean + SD
Demonstrates conviction about the
Fracture Fighters Program
2.8 + 1.26 3.2 + 0.98 2.5 + 1.80
Builds involvement and support 2.7 + 1.51 3.0 + 1.25 2.4 + 1.80
Persists under adversity 2.8 + 1.50 3.1 + 1.09 2.5 + 1.86
Binary logistic regression resulted in no statistically significant relationships between
leadership behaviours, organizational climate, champion behaviours with successful
implementation (Table 18). Of the transformational leadership behaviours the magnitude of the
odds ratio was the largest for intellectual stimulation 2.1 (CI95: 0.61-7.50), with the other four

85
transformational leadership behaviours ranging from 1.2 – 1.4. As hypothesized laissez-faire
behaviour was negatively associated with successful implementation. The organizational climate
traits of Change, Mission, and Cohesion also had large but not statistically significant
associations with odds ratios of 3.6 (CI95: 0.61-20.7), 3.5 (CI95: 0.64-19.57) and 2.4 (CI95: 0.67-
8.48) respectively. Opinion leadership had an odds ratio of 1.7 (CI95: 0.76 – 3.91)
Table 18: Logistic Regression Models (Success Implementation)
Covariate Odds Ratio
n=20 B Exp (B) 95% CI Lower
95% CI Upper
p-value
Transformational Behaviours
1. Idealized Influence Attributed 0.23 1.26 0.47 3.37 0.65
2. Idealized Influence Behaviour 0.30 1.34 0.47 3.87 0.58
3. Inspirational Motivation 0.37 1.45 0.47 4.43 0.52
4. Intellectual Stimulation 0.76 2.14 0.61 7.50 0.23
5. Individual Consideration 0.18 1.20 0.52 2.76 0.67
Transactional Behaviours
6. Contingent Rewards (CR) 0.35 1.42 0.50 4.01 0.51
7. Management-By-Exception Active (MBEA) 0.39 1.47 0.52 4.21 0.47
8. Management-By-Exception Passive (MBEP) -0.82 0.92 0.37 2.31 0.86
Laissez-Fair Behaviours
9. Laissez-Faire -0.70 0.50 0.14 1.72 0.27
Organizational Climate Traits
10. Mission 1.26 3.54 0.64 19.57 0.15
11. Cohesion 0.87 2.38 0.67 8.48 0.18
12. Autonomy 0.37 1.45 0.26 8.11 0.67
13. Communication 1.14
14. Stress 0.37
15. Change 1.27 3.56 0.61 20.69 0.16
Facilitation
16. Opinion Leadership 1.74 0.76 3.97 0.19
n=16
17. Demonstrates conviction about the Fracture Fighters Program 0.363 1.44 0.68 3.05 0.34
18. Builds involvement and support 0.315 1.37 0.67 2.78 0.38
19. Persists under adversity 0.268 1.31 0.65 2.64 0.45
* The models for communication and stress were rejected as the Homer-Lemeshow chi-square
indicated the model did not have good fit.

86
4.5 DISCUSSION
This study reports the findings from the first application of the PARiHS toolbox for
describing unit level factors potentially related to the success of implementing the Fracture
Fighters program. Overall, managers in inpatient rehabilitation units did not have beneficial
leadership scores as management-by-exception active (leaders focus on ensuring standards are
met), management-by-exception passive (leaders intervene only after mistakes have already
happened) and laissez-faire behaviour (leadership is absent) were at or above the 70th
percentile.
However, Clinical coaches reported high levels of freedom and latitude to do their job
(autonomy). As hypothesized, questionnaire results revealed that there was variation in the
profile of manager leadership behaviours between units with only 30% of clinical coaches
reporting the presence of all five transformational leadership behaviours, 45% reporting 1-4
behaviours and the remaining 25% no transformational leadership behaviours. Similarly,
organizational climate scores were dissimilar between units with only two (10%) reporting
positive scores for mission, cohesion, autonomy, communication, stress and change while 30%
rated poorly on all of these organizational climate traits. Furthermore, facilitation was variable
between units, for example 59% of managers reported clinical coaches were enthusiastic about
the program, consistently got the right people involved, and persisted under adversity, while
according to managers 36% showed none of these champion behaviours. Finally, odds ratios
(although not statistically significant) suggested that higher transformational leadership
behaviour, organizational climate and championship behaviour scores were associated with
implementation success.
These results are consistent with the PARiHS framework which reported that practice
environments are ―messy‖ and that change is complicated by context and facilitation factors that

87
contribute to the ability of health organizations to implement new evidence (Rycroft-Malone et
al. 2002). Although the findings were not statistically significant, they provide additional proof
of principle that the PARiHS hypothesis is indeed accurate. This is an important step to verifying
the importance of the framework in implementation research as only two other investigators have
published studies utilizing quantitative methods to apply the PARiHS framework(Cummings et
al. 2007; Estabrooks et al. 2007; Estabrooks et al. 2008).
In 2007, Estabrooks (2007) included single item measures of culture (freedom to make
important patients care and work decisions), leadership (a nurse manager or immediate
supervisor who is a good manager and leader), evaluation (praise and recognition for a job well
done), and facilitation (opportunity for staff nurses to consult with clinical nurse specialist or
expert nurse/clinician experts) in a survey of 4,421 nurses in Alberta, Canada. The purpose of the
survey was to determine independent factors that predicted research utilization among nurses,
taking into account influences at individual nurse, specialty, and hospital levels. In the multi-
level model, most (87%) of the variation was explained by individual level factors. However,
although organizational determinants explained less variance in the model, they were still
statistically significant when analyzed alone. Results showed an upward linear dose- response
relationship of research utilization to the high-context group as compared to low-context scores.
Similarly, Cummings (2007) also used the same three context variables to sort cases into one of
four mutually exclusive data sets that reflected less positive to more positive context. Then, a
theoretical model of hospital and unit-level influences on research utilization was developed and
tested, using structural equation modeling (300 cases). Nurses working in contexts with more
positive culture, leadership, and evaluation also reported significantly more research utilization,

88
staff development, and lower rates of patient and staff adverse events than did nurses working in
less positive contexts.
The results of the current study add to the evidence provided by Estabrooks (2007) and
Cummings(2007). Although their studies were successful in demonstrating a dose-response
relationship in that higher levels of context (culture, leadership and evaluation) resulted in more
research utilization, a limitation of their studies is the narrow definition of culture, leadership and
evaluation. The application of the PARiHS toolbox allowed us to examine specific aspects of
leadership behaviours, traits of the organization climate as well as behaviours of facilitators that
were driving implementation success in inpatient rehabilitation units. Although logistic
regression revealed no statistically significant associations between successful implementation
and leadership, organizational climate and facilitation covariates – potential important effect
sizes were noted that may be applicable to best-practice implementation. For example, the odds
of successful implementation were increased when managers displayed transformational
leadership behaviours, in particular when managers were intellectually stimulating. Also, staff
awareness of agency mission and clarity of its goals (Mission); Workgroup trust and cooperation
(Cohesion); and the units openness and efforts in keeping up with changes that are needed
(Change) increased the odds of successful implementation as did opinion leadership scores.
Finally, laissez-faire leadership reduced the odds of successful implementation by half.
Estabrooks (2008) more recent study used a more comprehensive measurement of culture
to study the relationship between context and research use in seven patient care units. The
Nursing Unit Culture assessment tool (NUCAT) included co-worker support, questioning
behaviour, continuing education, work creativity and work efficiency. The correspondence
analysis demonstrated that high research utilization units had the highest aggregated mean unit

89
culture scores. Although the NUCAT tool provided five sub-scores of culture, the aggregated
(mean) score did not allow for details as to which contextual elements could be targeted for
implementation improvement.
The increasing emphasis on considering context for evidence implementation speaks to
the importance of the findings of this study. In their 2006 meta-analysis, Dijkstra et al. found
limited studies from inside hospitals that compared the effects of organizational characteristics
with guideline implementation. The findings from this study verify that organizational context is
highly variable even amongst care units with similar mandates and client populations within the
same provincial system. Indicating the importance of consideration that uniform implementation
strategies (such as Fracture Fighters) may result in variable success due to difference in practice
environments. Therefore the addition of the assessment of unit or organizational level barriers
and facilitators to inform implementation is warranted.
Although the Fracture Fighters team did partially tailor the implementation strategy in
each unit through the inclusion of a clinician advisory panel, the tailoring was based on sub-
elements of evidence (patient and clinician experience). We propose that the Fracture Fighters
program could have been strengthened by applying the PARiHS toolbox during the
implementation planning process to identify organizational level strengths and weaknesses. For
example, overall assessment of unit level (context and facilitation) barriers prior to
implementation would have demonstrated that inpatient rehabilitation units in Ontario are highly
autonomous (ORC climate score mean above 75 percentile) but that transactional and laissez-
faire behaviour was much higher than the norm. With this knowledge the Fracture Fighter team
could have included leadership training initiatives along with the osteoporosis educational
training provided to Clinical Coaches. Furthermore, programs with the resources and capacity to

90
tailor implementation strategies to each individual setting could utilize site specific data to
address individual leadership behaviours and organizational climate traits. In addition,
administering the short measure of opinion leadership could provide managers useful
information on selecting local clinicians to champion implementation projects.
4.5.1 Limitations and Suggested Toolbox Revisions
There were a number of limitations to this study. First, due to feasibility issues
(respondent burden) and ethical restrictions (permission to contact), only the Clinical Coach and
unit manager were invited to participate in the survey. Preferably the PARiHS toolbox should be
administered to as many clinicians involved in implementation. This would allow for a more
accurate measure of contextual indicators such as leadership and climate (Avolio and Bass 2004;
Dansereau and Simpson 2006). However, the site response rate to this survey was high in
comparison to other evaluation activities of the Fracture Fighters program (patient survey phase
(8/36); audit Checklists (10/36). A major limitation of this study was the sample size was too
small to show statistically significant changes even when the magnitude of the effect was large.
This also precluded any adjustment for covariates in the regression analysis. In future, because of
the measures selected, this toolbox needs to be applied in studies of a large number of sites and
or individuals. The PARiHS toolbox could also recommend a minimum number of respondents
required for each questionnaire.
We dichotomized leadership behaviours, organizational trait and champion behaviour
scores to develop simple indicators for the presence or absence of each variable. However, in
reality these items are not all or none but ranging on a continuum from low to high as described
by the PARiHS framework. Decisions for implementation planning should be made based on
comparison of mean scores with the standardized score profiles.

91
One unexpected finding was that managers had a tendency to self-report themselves
higher on transformational leadership behaviours then their staff. Failla & Stichler (2008) also
found that nurse managers rated themselves higher on transformational leadership styles than
their staff nurses. They hypothesized that that this may be related to the fact that healthcare
organizations reward nurse manager behaviour for transactional leadership behaviours such as
compliance with policies, expense management and productivity and fail to motivate and support
nurse managers in the development of transformational characteristics – suggesting that
managers aspire to be recognized as transformational leaders but may not actually be
demonstrating transformational behaviours (Failla and Stichler 2008). This finding leads us to
recommend that although the MLQ developers have validated 360 ratings, perhaps for the
purposes of implementation planning it is best to utilize sub-ordinate ratings rather than self-
report. Further research to validate this point is required.
In addition, there are several aspects related to the measurement of the outcome variable
(implementation success) that could be improved. First, the data was collected by self-report,
which could have led to respondents providing more socially desirable responses (more positive
ratings). This could potentially lead to Type III error (attributing failure of an intervention
outcome, to the intervention efficacy rather than failure of implementation). The toolbox could
be improved by including instructions for an independent measure of implementation fidelity,
such as a chart audit to verify best-practices. In addition to improvement of implementation
fidelity, Dopson (2007), recommended that implementation should be viewed as a continuous
rather than discrete event. There are possible change outcomes (such as partial implementation,
modified implementation, a pretense of implementation, or local customization), which could
add richer detail to the framework, compared to a simple successful-not-successful dichotomy.

92
Finally, the cross-sectional nature of the study did not identify improvements or change in the
best-practices. Some inpatient rehabilitation units were already including some of the best-
practices prior to the Fracture Fighters program, therefore we are potentially overstating the
‗success‘ variable in some units. Inclusion of baseline indicators could provide more accurate
data on improvements or changes in best-practice implementation.
In summary, the application of the PARiHS toolbox allowed for the measurement of each
sub-element in the framework, providing detailed information regarding the transformational,
transactional and laissez-faire leadership behaviours of managers, the organizational climate of
inpatient rehabilitation units, and championship behaviours of Clinical Coach facilitators. The
results have allowed for preliminary hypothesis to be generated regarding specific leadership
behaviours (intellectual stimulation) and organizational traits (mission, cohesion, change) that
are potentially driving implementation success and provide support for the idea that addressing
unit level factors during implementation could improve uptake of evidence. Further exploration
of the PARiHS model is warranted, as it seems that attention to unit level factors identified by
the framework could have a role in determining implementation of evidence in practice.
In addition to the toolbox modifications recommended, future research directions are
discussed. Further quantitative evidence is required to show a predictive link between the
PARiHS elements and implementation success. Specifically, through the application of the
PARiHS toolbox, investigators may be able to pinpoint specific leadership behaviours and
organizational climate traits that are driving implementation success at the unit level.
Furthermore, additional studies such as those carried out by Estabrooks(2007) and Cummings
(2007) are needed that investigate the combined effect that these unit level effects have with
individual and system-wide factors on implementation. These two streams of research will give

93
perspective to investigators planning implementation strategies. Specifically, they will be able to
tailor interventions based on the factors that are most likely to increase effective implementation
at multiple levels.
4.6 CONCLUSION
The PARiHS toolbox was an effective method to highlight wide-ranging contextual and
facilitation differences between inpatient rehabilitation unit implementation sites. The findings of
the survey provide support to the PARiHS framework‘s proposition that context and facilitation
along with strong evidence influence implementation success. The practical application of the
toolbox has led to suggestions for its improvement. Further research should utilize the toolbox to
provide evidence of the impact of context and facilitation on the ability to implement new
programs or evidence coupled with the impact of factors at multiple levels. This will provide
validation for the prospective application of the toolbox to guide implementation planning for
future programs like Fracture Fighters.

94
CHAPTER 5 - DISCUSSION
Considerable resources are devoted to clinical and health services research (Haynes and
Haines 1998), however the transfer of research findings into practice is unpredictable and can be
slow and haphazard (Eccles and Improved Clinical Effectiveness through Behavioural Research
Group 2006). It is estimated that 30-40% of individuals do not receive care compliant with
scientific evidence (McGlynn et al. 2003; Grol et al. 2007). Thus, knowledge translation and in
particular implementation science has focused on individual clinicians and identifying the
barriers and facilitators to their use of evidence in practice (Estabrooks et al. 2004) and the
development of interventions to improve the use of research by clinicians in their day to day
practice (Grimshaw, Thomas et al. 2004). Although considering the individual is important, and
many of these interventions have led to improvements in evidence-based care (Oxman et al.
1995; Bero et al. 1998; Grimshaw, Eccles et al. 2004; Grimshaw et al. 2006), there is an
increasing consensus that further success could be achieved if we acknowledge the importance of
barriers and facilitators associated with factors other than the individual (Grol et al. 2007). In
particular, there is an increasing acknowledgement of the role of organizational context (practice
environment) in evidence uptake (Cummings et al. 2004; Dijkstra et al. 2006; Green et al. 2007;
Kitson et al. 2008). Therefore, the overall goal of this thesis was to apply the Promoting Action
on Research Implementation in Health Services (PARiHS) framework to an osteoporosis best-
practice program to describe unit level factors that could have influenced its implementation.
The PARiHS framework (Kitson et al. 1998; Rycroft-Malone et al. 2002) is a KT model
that includes unit level factors (e.g. context or practice environment) that has been gaining
recognition in implementation science as a useful guide for describing implementation success in
health care organizations (Kitson et al. 2008). However, its application has been limited
primarily to qualitative studies due to the lack of validated tools to measure the constructs. One

95
objective of this thesis was to identify a toolbox of measures to operationalize the PARiHS
framework to assess unit level barriers and facilitators to the use of evidence in practice. The
findings from this study provide a stepping stone for the assessment of unit level factors as
defined by PARiHS to guide implementation planning.
Furthermore, through the application of the proposed PARiHS toolbox to a best-practice
program for osteoporosis management in inpatient rehabilitation units, this study provided
support for the constructs of the PARiHS framework. In particular, findings from this study
confirmed our hypothesis that leadership behaviours of managers and the organizational climate
were variable across care units with similar patient populations and care mandates. In addition,
two measures of facilitation identified local clinicians who were more likely to be successful in
facilitating the best practice intervention. These results suggest that attention to these contextual
and facilitation factors along with evidence during implementation planning could lead to
improved implementation success of future programs.
5.1 Implications for Quantitative Applications of the PARiHS Framework
Prior to this study only two other investigators had applied the PARiHS framework using
quantitative methods (Cummings et al. 2007; Estabrooks et al. 2007; Estabrooks et al. 2008).
This study proposed and applied the PARiHS toolbox to a best-practice program for osteoporosis
management of fracture patients in inpatient rehabilitation units leading us to suggest several
implications for future quantitative applications of the PARiHS Framework.

96
5.1.1 Organizational Culture vs. Organizational Climate
This study included a literature review to identify validated measurement tools of each of
the PARiHS sub-elements resulting in a suggested modification of the sub-element of
organizational culture for quantitative applications of the framework. Our findings revealed that
organizational culture and organizational climate were terms often used interchangeably in the
literature. Glisson (2008) defined climate as the ―way people perceive their work environment‖
and culture as ―the way things are done in an organization‖. Denison (1996) found that the
methods and epistemology of recent organizational culture studies were similar and almost
indistinguishable from climate literature of the 1960‘s and 1970‘s concluding that these studies
mistakenly use the terms culture and climate interchangeably. Denison (1996) concluded that
although the two traditions should be viewed as having major differences in interpretation, there
is not a difference in the phenomenon under study. The implications of these findings suggest
that organizational climate and culture could be seen as interchangeable sub-elements within the
PARiHS framework. In essence, if context is being studied through observational methods with a
symbolic interactionist perspective the element under study should be culture. If context is being
evaluated through the use of an interview or survey that relies on the perspective of individuals,
the concept of organizational climate should be used.
5.1.2 The Context Assessment Index (CAI)
During the course of this study another group of researchers published an instrument
based on the PARiHS framework (McCormack et al. 2009). The Context Assessment Index
(CAI) provides a global measure of context as well as measures of leadership, culture and
evaluation and similar to the toolbox proposed in this study, was developed as a planning tool for
improving implementation strategies. To the author‘s knowledge, no studies have been published

97
utilizing the CAI. The proposed PARiHS toolbox differs from the CAI in several respects. First,
inclusion of the Multifactor Leadership Questionnaire and the Organizational Readiness for
Change Climate Scale in the PARiHS toolbox will enable implementation planners to pinpoint
specific behaviours of leaders and organizational traits that are potential barriers to
implementation whereas the CAI only provides global measures of the context sub-elements.
Second, and most notably, the proposed toolbox is inclusive of all PARiHS elements and
respective sub-elements whereas the CAI only includes measures of context neglecting evidence
(research, clinical experience, patient experience) and facilitation. Thus, the proposed toolbox
offers a more comprehensive method for operationalizing the PARiHS framework. Finally,
through application of this comprehensive measure, the PARiHS toolbox will allow further
validation and refinement of the framework by allowing future research to investigate the
relationship between the sub-elements and implementation success whereas the CAI focuses on
implementation planning. Ideally, the toolbox should be used as a complete package to
operationalize the full framework. In summary, there are two potential applications of the
PARiHS toolbox. First, it can be used as a diagnostic and prescriptive guide for implementation
planning and second, it can be used to evaluate program implementation.
5.1.3 The Use of the Proposed PARiHS Toolbox in Implementation Planning
To bridge the gap between research and practice a commonly suggested approach is to
identify barriers to practice change and implement interventions to reduce identified barriers
(Bostrom et al. 2009). For example, Fink et al (2005) implemented multiple organizational
interventions (e.g. integration of evidence-based practice philosophy into nursing job
descriptions, established unit-based journal clubs) based on a low score on the ‗setting‘ subscale
of the BARRIERS scale (Funk et al. 1991). The multi-faceted intervention significantly

98
decreased nurse ratings on the ‗setting‖ subscale; however, they were unable to distinguish
which of the components of the organizational interventions made a difference. This problem is
due to the lack of useful theory (Bostrom et al. 2009) and concrete guidance (Green et al. 2007)
available regarding how to match tools to setting. Dijkstra (2006) completed a meta-analysis of
organizational characteristics to describe their effect on clinical guidelines and discovered there
was limited advice on tailoring strategies to address organizational level barriers, despite the
increased importance given to tailoring in the literature (Dijkstra et al. 2006).
The advantage of utilizing the PARiHS toolbox in implementation planning is that the
scales included to measure contextual (leadership, climate) and facilitation factors also identify
areas that can be targeted for modification. The inclusion of these measures allows the proposed
toolbox to be used as a diagnostic and prescriptive tool during implementation planning. For
example, the MLQ Form 5X, provides scores on nine leadership behaviours which can be
compared to a standardized score profile. Leaders can identify their deficiencies or perceived
deficiencies and identify the specific areas that require improvement. Another example is the
ORC Climate scale‘s ―mapping‖ tool (Dansereau and Simpson 2006) which can be used to
match barriers with implementation strategies. The ORC is intended for use by teams planning to
implement new programs. The maps enable identification of potential problems, and suggest
discussion activities for teams and managers to work through to ensure organizational climate
barriers are addressed prior to implementation (Dansereau and Simpson 2006). Courtney et al.
(2007) demonstrated that providing program directors and clinical supervisors ORC scores
during a feedback session was predictive of engagement in strategies to improve low rated
climate indicators. The inclusion of specific tools and strategies to address the contextual barriers
identified by this proposed PARiHS toolbox fills a need that has not been addressed in prior
studies.

99
5.1 4 Implementation Evaluation
The second potential application of the proposed PARiHS toolbox is to evaluate the
influence of unit level factors on evidence implementation. To date, several qualitative studies
have used the framework to guide content analyses of interview and focus group transcripts as
well as to guide document reviews (Ellis et al. 2005; Wallin et al. 2005). Continual assessment of
barriers and facilitators will allow programs such as Fracture Figures to refine strategies
throughout implementation or apply lessons learned to new programs. This is discussed further
in future directions.
5.2 Limitations
This is one of the first studies to apply the PARiHS framework using quantitative
methods. Notwithstanding this, several limitations to the study exist. First, the method for
selection of measures in the proposed toolbox was based primarily on face validity with the sub-
elements of the PARiHS framework. Although several of the measures included have been well
validated (e.g. MLQ Form 5X) future studies utilizing the toolbox should report on its
psychometric properties. In particular, the suggested items for evidence have not been utilized
previously and need further validation to verify the suggested scale items and scoring method. In
addition, the items included for ―evaluation‖ were specific to the Fracture Fighters program and
will not be generalizable to other programs. Additional work is needed to identify or develop an
appropriate measure for evaluation.
Our experience with applying the toolbox also had several limitations. First, the use of
inpatient rehabilitation units as the unit of analysis resulted in a small sample size and low power
to detect significant differences. Second, due to feasibility issues (respondent burden) and

100
ethical restrictions (permission to contact) only the Clinical Coach and unit manager were invited
to participate in the survey. Preferably the PARiHS toolbox should be administered to as many
clinicians involved in implementation. This would allow for a more accurate measure of
contextual indicators such as leadership and climate (Lehman et al. 2002; Avolio and Bass
2004). Third, the application of the PARiHS framework alone ignored other levels of barriers
(individual, organization/hospital, health system) that could also potentially influence
implementation success.
5.3 Future Directions
5.3.1 Provide Support for the PARiHS Framework
Research is warranted to provide additional empirical support for knowledge translation
theories frameworks and models. Theory-based approaches are important for implementation
science in order to interpret why interventions have positive or negative effects (Eccles et al.
2005). Koh et al (2008) suggests that the effectiveness and utility of the PARiHS framework in
facilitating implementation requires validation by further empirical research. In fact, the PARiHS
framework states successful implementation is a function of the elements evidence, context and
facilitation; however,
“[PARIHS] assumes that these dimensions are both causally and linearly related to one
another. The reality is that we do not know which of the core dimensions or sub-elements
is strongest in creating the right conditions for successful implementation” (Kitson et al.
1998; McCormack et al. 2002).
Furthermore, the developers acknowledge that ―the interaction between facilitation and context
and evidence is still not fully understood‖ (Rycroft-Malone et al. 2002). Through the provision of
a comprehensive measure for the PARiHS framework, the current study provides a vehicle to

101
address some of these issues. We suggest that future research should utilize the proposed
PARiHS toolbox to 1) determine which elements or sub-elements are driving successful
implementation; 2) to determine the relationship between elements and sub-elements within the
framework (e.g. relationship between leadership and climate); and 3) to determine the effect of
unit level factors within a multi-level model that take into account individual and system level
factors. The application of the proposed toolbox will provide information regarding the utility of
applying a comprehensive measure the framework.
In future because of the measures selected, this toolbox needs to be applied in studies of
a large number of sites and or individuals to achieve adequate power. Furthermore,
implementation fidelity should be measured in conjunction with outcomes. Implementation
fidelity is the degree in which an intervention or programme is delivered as intended and unless
measured it cannot be determined whether the lack of impact (outcomes) is due to poor
implementation or inadequacies inherent to the program itself (ie. Type III error)(Carroll et al.
2007).
5.3.2 Prospective Application of the PARiHS Toolbox to Guide Implementation Planning
Multifaceted interventions built upon a careful assessment of barriers and coherent
theoretical base may be more effective than single interventions (Grimshaw et al. 2006). Green et
al (2007) tested a theory-based approach to choosing guideline implementation strategies and
concluded that efforts to improve adherence to practice guideline should focus on barrier
reduction at the system or organizational level rather than in the individual provider alone. As
discussed the application of the proposed PARiHS toolbox can be used as a diagnostic and
prescriptive tool for considering unit level barriers and facilitators for implementation planning.

102
An important area of research will be to apply the PARiHS framework and proposed
toolbox prospectively to determine if the identified unit level barriers are indeed modifiable and
to determine the effectiveness of targeted strategies. Future research should also explore the
utility of the framework and proposed toolbox in a variety of health settings (e.g. acute, primary
care). Until the framework is applied prospectively and specific strategies evaluated, it will be
unclear whether the sub-elements identified in the framework are indeed modifiable (e.g.
leadership).
Furthermore, we suggest that the PARiHS model should be used in conjunction with
other models / frameworks that take into account barriers and facilitators to implementation at
multiple levels. Ferlie and Shortell (2001), suggest that there are four levels (individual health
professionals; groups/teams; organizations (hospital); larger health system) of health care at
which interventions to improve that quality of care could be applied. Whereas, Koh (2008)
suggested that potential barriers and facilitators can act at six different levels: the innovation; the
individual professional; patient; social context; organizational context; and economic and
political context.
For example, the PARiHS model could be embedded within the Ottawa Model for
Research Use (OMRU). The ORMU includes six elements central to the research use process:
the potential adopters; evidence-based innovation; the practice environment; strategies for
transferring the evidence into practice, the use of the evidence; and the health-related and other
outcomes of the process. The PARiHS framework and toolbox could be used as a diagnostic
guide for identification of contextual level problems and to identify strategies that address
specific weaknesses in each context within the ―practice environment‖ element of ORMU. In

103
addition, barriers and facilitators at other levels such as the individual adopters will also be
identified and incorporated in implementation strategies.
5.4 CONCLUSION
It is important that implementation plans incorporate strategies to alleviate barriers at
multiple levels including the practice environment. The PARiHS toolbox could be a useful
mechanism for identifying unit level (context and facilitation) barriers requiring attention in
implementation planning. Furthermore, it provides a means for additional quantitative testing of
the PARiHS hypothesis that implementation success is a function of evidence, context and
facilitation.

104
REFERENCES
Adachi, J., G. Ioannidis, L. Pickard, et al. (2003). "The association between osteoporotic
fractures and health-related quality of life as measured by the health utilities index in the
Canadian multicentre osteoporosis study (Camos)." Osteoporosis International 14(11):
895-904.
Antonakis, J., B. J. Avolio and N. Sivasubramaniam (2003). "Context and leadership: An
examination of the nine-factor full-range leadership theory using the multifactor
leadership questionnaire." The Leadership Quarterly 14: 261-295.
Atkins, D. (2009). "QUERI and implementation research: Emerging from adolescence into
adulthood: QUERI series." Implementation Science 4(1): 12.
Avolio, B. J. and B. M. Bass (1991 ). The full range leadership development programs: Basic
and advanced manuals, Bass, Avolio & Associates.
Avolio, B. J. and B. M. Bass (2004). Multifactor leadership questionnaire: Manual and sampler
set, Mind Garden Inc.
Bally, J. M. G. (2007). "The role of nursing leadership in creating a mentoring culture in acute
care environments." Nursing Economics 25(3): 143-49.
Barr, O. (1997). "Interdisciplinary teamwork: Consideration of the challenges." British Journal
of Nursing 6: 1005-1010.
Bass, B. M. and B. J. Avolio, Eds. (1994). Improving organizational effectiveness through
transformational leadership. Thousand Oaks, SAGE Publications Inc.
Bass, B. M., B. J. Avolio and L. Atwater (1996). "The transformational and transactional
leadership of men and women." Applied Psychology 45(1): 5-34.
Bero, L. A., R. Grilli, J. M. Grimshaw, et al. (1998). "Getting research findings into practice:
Closing the gap between research and practice: An overview of systematic reviews of

105
interventions to promote the implementation of research findings." BMJ 317(7156): 465-
468.
Bessette, L., L.-G. Ste-Marie, S. Jean, et al. (2008). "The care gap in diagnosis and treatment of
women with a fragility fracture." Osteoporosis International 19: 79-86.
Bahtsevani, C., A. Willman, A. Khalaf and M. Östman (2008). "Developing an instrument for
evaluating implementation of clinical practice guidelines: A test-retest study." Journal of
evaluation in clinical practice 14(5): 839-846.
Bostrom, A. M., K. Nilsson Kajermo, G. Nordstrom and L. Wallin (2009). "Registered nurses'
use of research findings in the care of older people." Journal of clinical nursing 18(10):
1430-41.
Bowman, C., E. Sobo, S. Asch, et al. (2008). "Measuring persistence of implementation: QUERI
series." Implementation Science 3(1): 21.
Brown, A., A. Cohen, M. Chinman, et al. (2008). "Equip: Implementing chronic care principles
and applying formative evaluation methods to improve care for schizophrenia: QUERI
series." Implementation Science 3(1): 9.
Brown, D. and B. McCormack (2005). "Developing postoperative pain management: Utilising
the promoting action on research implementation in health services (PARIHS)
framework." Worldviews on Evidence-Based Nursing 2(3): 131-141.
Brown, J. P. and R. G. Josse (2002). "2002 clinical practice guidelines for the diagnosis and
management of osteoporosis in Canada." Canadian Medical Association Journal 167(10):
1-34.
Canadian Institutes of Health Research. (2000). "The CIHR act." Retrieved January 8, 2009,
from http://www.cihr-irsc.gc.ca/e/22948.html.
Canadian Institutes of Health Research. (2009). "About knowledge translation." Retrieved July
8, 2009, from http://www.cihr-irsc.gc.ca/e/29418.html.

106
Carroll, C., M. Patterson, S. Wood, et al. (2007). "A conceptual framework for implementation
fidelity." Implementation Science 2: 40.
Chaney, E., L. Rabuck, J. Uman, et al. (2008). "Human subjects protection issues in QUERI
implementation research: QUERI series." Implementation Science 3(1): 10.
Conklin, J. and P. Stolee (2008). "A model for evaluation knowledge exchange in a network
context." CJNR 40(2): 116-124.
Cooper, C. (1997). "The crippling consequences of fractures and their impact on quality of life."
Journal of the American Medical Association 103(2A): 12S-19S.
Courtney, K. O., G. W. Joe, G. A. Rowan-Szal and D. D. Simpson (2007). "Using organizational
assessment as a tool for program change." Journal of Substance Abuse Treatment 33:
131-137.
Cree, M. W., A. G. Juby and K. C. Carriere (2003). "Mortality and morbidity associated with
osteoporosis drug treatment following hip fracture." Osteoporosis International 14: 722-
727.
Cummings, G. G., C. A. Estabrooks, W. K. Midodzi, et al. (2007). "Influence of organizational
characteristics and context on research utilization." Nursing research 56(4): S24-39.
Cummings, G. G., L. Hayduk and C. A. Estabrooks (2006). "Is the nursing work index
measuring up?: Moving beyond estimating reliability to testing validity." Nursing
Research March/April 55(2): 82-93.
Cummings, G. G., A. A. Mallidou and S. Scott-Findlay (2004). "Does the workplace influence
nurses' use of research?" Journal of Wound Ostomy & Continence Nursing 31(3): 106-
107.
Cummings, S. R. and L. J. Melton (2002). "Epidemiology and outcomes of osteoporotic
fractures" Lancet 359: 1761-1767.

107
Curran, G., S. Mukherjee, E. Allee and R. Owen (2008). "A process for developing an
implementation intervention: QUERI series." Implementation Science 3(1): 17.
Dansereau, D. F. and D. D. Simpson (2006). Mapping organizational change: A guidebook on
program needs. TCU Mapping-Enhanced Counseling Manuals for Adaptive Treatment,
Texas Institute of Behavioral Research at TCU.
Davis, D., M. Evans, A. Jadad, et al. (2003). "The case for knowledge translation: Shortening the
journey from evidence to effect." BMJ 327: 33-35.
Denison, D. R. (1996). "What is the difference between organizational culture and organizational
climate? A native's point of view on a decade of paradigm wars." Academy of
Management Review 21(3): 619-654.
Dijkstra, R., M. Wensing, R. Thomas, et al. (2006). "The relationship between organisational
characteristics and the effects of clinical guidelines on medical performance in hospitals,
a meta-analysis." BMC Health Services Research 6: 53.
Dillman, D. A. (1978). Mail and telephone surveys: The total design method. New York, John
Wiley & Sons.
Dobbins, M., D. Ciliska, R. Cockerill, et al. (2002). "A framework for the dissemination and
utilization or research for health-care policy and practice." The Online Journal of
Knowledge Synthesis for Nursing 9(7).
Dopson, S. (2007). "A view from organizational studies." Nursing Research 56(4S): S72-S77.
Doran, D. M. and S. Sidani (2007). "Outcomes-focused knowledge translation: A framework for
knowledge translation and patient outcomes improvement." Worldviews on Evidence-
Based Nursing 4(1): 3-13.
Eccles, M., J. Grimshaw, A. Walker, et al. (2005). "Changing the behavior of healthcare
professionals: The use of theory in promoting the uptake of research findings." Journal of
Clinical Epidemiology 58: 107-112.

108
Eccles, M. and Improved Clinical Effectiveness through Behavioural Research Group (2006).
"Designing theoretically-informed implementation interventions." Implementation
Science 1.
Elliot-Gibson, V., E. R. Bogoch, S. A. Jamal and D. E. Beaton (2004). "Practice patterns in the
diagnosis and treatment of osteoporosis after a fragility fracture a systematic review"
Osteoporosis International 15(10): 767-778.
Ellis, I., P. Howard, A. Larson and J. Robertson (2005). "From workshop to work practice: An
exploration of context and facilitation in the development of evidence-based practice."
Worldviews on Evidence-based Nursing 2(2): 84-93.
Estabrooks, C., Ed. (2004). A nursing and allied health sciences perspective on knowledge
utilization. Using knowledge and evidence in health care: Multidisciplinary perspectives
on evidence-based decision-making in health care, Toronto: University of Toronto Press.
Estabrooks, C., S. Scott, J. Squires, et al. (2008). "Patterns of research utilization on patient care
units." Implementation Science 3(1): 31.
Estabrooks, C. A. (2007). "Prologue: A program of research in knowledge translation." Nursing
Research 56(4S): S4-S6.
Estabrooks, C. A., W. K. Midodzi, G. G. Cummings and L. Wallin (2007). "Predicting research
use in nursing organizations: A multilevel analysis." Nursing Research 56(4S): S7-S23.
Estabrooks, C. A., S. Scott-Findlay and C. Winther (2004). A nursing and allied health sciences
perspective on knowledge utilization. Using knowledge and evidence in health care:
Multidisciplinary perspectives. L. Lemieux-Charles and F. Champagne. Toronto,
University of Toronto Press: 242-280.
Estabrooks, C. A., D. S. Thompson, J. E. Lovely and A. Hofmeyer (2006). "A guide to
knowledge translation theory." The Journal of Continuing Education in the Health
Professions 26: 25-36.
109
Failla, K. R. and J. F. Stichler (2008). "Manager and staff perceptions of the manager's
leadership style." JONA 38(11): 480-487.
Ferlie, E. B. and S. M. Shortell (2001). "Improving the quality of health care in the united
kingdom and the united states: A framework for change." The Milbank Quarterly 79(2):
281-315.
Fink, R., C. J. Thompson and D. Bonnes (2005). "Overcoming barriers and promoting the use of
research in practice." The Journal of nursing administration 35(3): 121-129.
Fleuren, M., K. Wiefferink and T. Paulussen (2004). "Determinants of innovation within health
care organizations: Literature review and Delphi study." Int J Qual Health Care 16(2):
107-123.
Flynn, L. R., R. E. Goldshimth and J. K. Eastman (1996). "Opinion leaders and opinion seekers:
Two new measurement scales." Academy of Marketing Science 24: 137.
Francke, A., M. Smit, A. de Veer and P. Mistiaen (2008). "Factors influencing the
implementation of clinical guidelines for health care professionals: A systematic meta-
review." BMC Medical Informatics and Decision Making 8(1): 38.
Frenk, J. (1992). "Balancing relevance and excellence: Organizational response to link research
with decision making." Social Science and Medicine 35(11): 1397-1404.
Funk, S. G., M. T. Champagne, R. A. Wiese and E. M. Tornquist (1991). "Barriers: The barriers
to research utilization scale." Appl Nurs Res 4(1): 39-45.
Giangregorio, L., A. Papaioannou, A. Cranney, et al. (2006). "Fragility and fractures and the
osteoporosis care gap: An international phenomenon." Seminars of Arthritis &
Rheumatism 35(5): 293-305.
Gibbon, B. (1999). "An investigation of inter-professional collaboration in stroke rehabilitation
team conferences." Journal of Clinical Nursing 8: 246-252.

110
Glisson, C., J. Landsverk, S. Schoenwald, et al. (2008). "Assessing the organizational social
context (OSC) of mental health services: Implications for research and practice."
Administration and Policy in Mental Health and Mental Health Services Research 35(1-
2): 98-113.
Goetz, M., C. Bowman, T. Hoang, et al. (2008). "Implementing and evaluating a regional
strategy to improve testing rates in VA patients at risk for HIV, utilizing the QUERI
process as a guiding framework: QUERI series." Implementation Science 3(1): 16.
Graham, I. and J. Tetroe (2009). "Learning from the U.S. Department of Veterans Affairs quality
enhancement research initiative: QUERI series." Implementation Science 4(1): 13.
Graham, I. D., J. Logan, M. B. Harrison, et al. (2006). "Lost in knowledge translation: Time for a
map?" Journal of Continuing Education in the Health Professions 26(1): 13-24.
Graham, K. and J. Logan (2004). "Using the Ottawa model of research use to implement a skin
care program." Journal of Nursing Care & Quality 19(1): 18-24.
Green, L., L. Wyszewianski, J. Lowery, et al. (2007). "An observational study of the
effectiveness of practice guideline implementation strategies examined according to
physicians' cognitive styles." Implementation Science 2(1): 41.
Greenhalgh, T., G. Robert, F. Macfarlane, et al. (2004). "Diffusion of innovations in service
organizations: Systematic review and recommendations." The Milbank Quarterly 82(4):
581-629.
Grimshaw, J., M. Eccles and J. Tetroe (2004). "Implementing clinical guidelines: Current
evidence and future implications." Journal of Continuing Education in Health Professions
24: 31-37.
Grimshaw, J., M. Eccles, R. Thomas, et al. (2006). "Evidence (and its limitations) of the
effectiveness of guideline dissemination and implementation strategies 1966-1998." J
Gen Intern Med 21: S14-20.

111
Grimshaw, J. M., R. E. Thomas, G. MacLennan, et al. (2004). "Effectiveness and efficiency of
guideline dissemination and implementation strategies." Health Technology Assessment
8(6): 1-72.
Grol, R., M. Bosch, M. E. J. L. Hulscher, et al. (2007). "Planning and studying improvement in
patient care: The use of theoretical perspectives." Milbank Quarterly 85(1): 93-138.
Grol, R. and J. Grimshaw (2003). "From best evidence to best practice: Effective implementation
of change in patients' care." Lancet 362(9391): 1225-1230.
Haentjens, P., G. Lamraski and S. Boonen (2005). "Costs and consequences of hip fracture
occurrence in old age: An economic perspective." Disability & Rehabilitation 27(18-19):
1129-41.
Hakkennes, S. and K. Dodd (2008). "Guideline implementation in allied health professions: A
systematic review of the literature." Qual Saf Health Care 17(4): 296-300.
Hanley, D. and R. Josse (1996). "Prevention and management of osteoporosis: Consensus
statements from the scientific advisory board of the Osteoporosis Society of Canada: 1.
Introduction." CMAJ 155(7): 921-923.
Hannan, E. L., J. Magaziner, J. J. Wang, et al. (2001). "Mortality and locomotion 6 months after
hospitalization for hip fracture: Risk factors and risk-adjusted hospital outcomes." JAMA
285(21): 2736-2742.
Harvey, G., A. Loftus-Hills, J. Rycroft-Malone, et al. (2002). "Getting evidence into practice:
The role and function of facilitation." Journal of Advanced Nursing 37(6): 577-588.
Haynes, B. (2004). An evidence-based medicine perspective on the origins, objectives,
limitations, and future developments of the movement. Using knowledge and evidence in
health care. L. Lemieux-Charles and F. Champagne. Toronto, University of Toronto
Press: 227-241.
Haynes, B. and A. Haines (1998). "Getting research findings into practice: Barriers and bridges
to evidence based clinical practice." BMJ 317(7153): 273-276.

112
Hogan, D. L. and J. Logan (2004). "The Ottawa model of research use: A guide to clinical
innovation in the NICU." Clinical Nurse Specialist 18(5): 255-261.
Howell, J. M. (2005). "The right stuff: Identifying and developing effective champions of
innovation." Academy of Management Executive 19(2): 108-119.
Howell, J. M., C. M. Shea and C. A. Higgins (2005). "Champions of product innovations:
Defining, developing, and validating a measure of champion behaviour." Journal of
Business Venturing 20: 641-661.
Jaglal, S. B., C. Evans, V. Quan, et al. (2006). The rehabilitation component of Ontario's first
osteoporosis strategy. 2nd Annual Toronto Rehabilitation Research Day, Toronto,
Ontario.
Jaglal, S. B., S. E. Munce, V. Quan, et al. (2008). "Assessment of a provincial strategy for
osteoporosis best practices: Fracture fighters -- the Ontario Osteoporosis Strategy for
inpatient rehabilitation." J Bone Miner Res 23(S1): M401.
Jaglal, S. B., P. G. Sherry and J. Schatzker (1996). "The impact and consequences of hip fracture
in Ontario" Canadian Journal of Surgery 39(2): 105-11.
Kanste, O., J. Miettuenen and H. Kyngas (2007). "Psychometric properties of the multifactor
leadership questionnaire among nurses." Journal of Advanced Nursing 57: 201-212.
Kennedy, I. (2001). Learning from Bristol: The report of the public inquiry into children's heart
surgery at the Bristol royal infirmary. London, The Stationery Office.
Khan, A. A., A. B. Hodsman, A. Papaioannou, et al. (2007). "Management of osteoporosis in
men: An update and case example." CMAJ 176(3): 345-8.
Kimberly, J. and J. M. Cook (2008). "Organizational measurement and the implementation of
innovations in mental health services." Administration and Policy in Mental Health and
Mental Health Services Research 35(1-2): 11-20.

113
Kitson, A. L., G. Harvey and B. McCormack (1998). "Enabling the implementation of evidence
based practice: A conceptual framework." Quality in Health Care 7: 149-158.
Kitson, A. L., J. Rycroft-Malone, G. Harvey, et al. (2008). "Evaluating the successful
implementation of evidence into practice using the PARIHS framework: Theoretical and
practical challenges." Implementation Science 3: 1.
Klotzbuecher, C. M., P. D. Ross, P. B. Landsman, et al. (2000). "Patients with prior fractures
have an increased risk of future fractures: A summary of the literature and statistical
synthesis." J Bone Miner Res 15: 721-739.
Koh, S. S. L., E. Manias, A. M. Hutchinson, et al. (2008). "Nurses' perceived barriers to the
implementation of a fall prevention clinical practice guideline in Singapore hospitals."
BMC Health Services Research 8:105.
Kontos, P. and B. Poland (2009). "Mapping new theoretical and methodological terrain for
knowledge translation: Contributions from critical realism and the arts." Implementation
Science 4(1): 1.
Koval, K. J. Z., J.D. (1994). "Functional recovery after fracture of the hip." The Journal of Bone
and Joint Surgery 76-A(5): 751-758.
Krein, S., S. Bernstein, C. Fletcher, et al. (2008). "Improving eye care for veterans with diabetes:
An example of using the QUERI steps to move from evidence to implementation:
QUERI series." Implementation Science 3(1): 18.
Lehman, W. E. K., J. M. Greener and D. D. Simpson (2002). "Assessing organizational readiness
for change." Journal of Substance Abuse Treatment 22(4): 197-209.
Logan, J. and I. D. Graham (1998). "Toward a comprehensive interdisciplinary model of health
care research use." Science Communication 20(2): 227-246
Logan, J., M. B. Harrison, I. Graham, et al. (1999). "Evidence-based ulcer practice: The Ottawa
model of research use." Canadian Journal of Nursing Research 31: 37-52.

114
Lorrain, J., G. Paiement, N. Chevrier, et al. (2003). "Population demographics and
socioeconomic impact of osteoporotic fractures in Canada." Menopause 10: 228-234.
Magaziner, J., W. Hawkes, J. R. Hebel, et al. (2000). "Recovery from hip fracture in eight areas
of function." J Gerontol A Biol Sci Med Sci 55(9): M498-507.
Marchionni, C. and J. Ritchie (2008). "Organizational factors that support the implementation of
a nursing best practice guideline." Journal of nursing management 16(3): 266-274.
Marottoli, R. A., L. F. Berkman and L. M. J. Cooney (1992). "Decline in physical function
following hip fracture." Journal of the American Geriatric Society 40(9): 861-6.
McCormack, B., A. Kitson, G. Harvey, et al. (2002). "Getting evidence into practice: The
meaning of 'context' " Journal of Advanced Nursing 38: 94-104.
McCormack, B., G. McCarthy, J. Wright, et al. (2009). "Development and testing of the context
assessment index (CAI)." Worldviews on Evidence-Based Nursing 6(1): 27-35.
McGlynn, E. A., S. M. Asch, J. Adams, et al. (2003). "The quality of health care delivered to
adults in the United States." N Engl J Med 348(26): 2635-2645.
Meijers, J. M. M., M. A. P. Janssen, G. G. Cummings, et al. (2006). "Assessing the relationships
between contextual factors and research utilization in nursing: Systematic literature
review." Journal of Advanced Nursing 55(5): 622-635.
Mossey, J. M., E. Mutran, K. Knott and R. Craik (1989). "Determinants of recovery 12 months
after hip fracture: The importance of psychosocial factors." Am J Public Health 79(3):
279-286.
Ontario Action Plan Committee (2003). Osteoporosis action plan: An osteoporosis strategy for
Ontario. Toronto, Ontario, Ministry of Health and Long-Term Care.
Ontario Osteoporosis Strategy. (2009). "The Ontario Osteoporosis Strategy for inpatient
rehabilitation." Retrieved July 14, 2009, from
http://www.fracturefighters.ca/Alias/Application/FFW/FFW/Home.htm.

115
Oxman, A. D., M. A. Thomson, D. A. Davis and R. B. Haynes (1995). "No magic bullets: A
systematic review of 102 trials of interventions to improve processional practice."
Canadian Medical Association Journal 153: 1423.
Papaioannou, A., C. Kennedy, G. Ioannidis, et al. (2008). "The osteoporosis care gap in men
with fragility fractures: The Canadian multicentre osteoporosis study." Osteoporosis
International 19(4): 581-587.
Pathman, D. E., T. R. Konrad, G. L. Freed, et al. (1996). "The awareness-to-adherence model of
the steps to clinical guideline compliance - the case of paediatric vaccine
recommendations." Medical Care 34(9): 873-889.
Patton, M. Q. (2002). Qualitative research and evaluation methods. Thousand Oaks, Sage
Publications.
Poole, K. E. S. and J. E. Compston (2006). "Osteoporosis and its management " BMJ 333(7581):
1251-1256.
Rogers, E. M. (1995). Diffusion of innovations. New York, Free Press.
Rycroft-Malone, J. (2007). "Theory and knowledge translation: Setting some coordinates."
Nursing Research 56(4S): S78-S85.
Rycroft-Malone, J., A. Kitson, G. Harvey, et al. (2002). "Ingredients for change: Revisiting a
conceptual framework." Quality and Safety in Health Care 11(2): 174-180.
Sackett, D. L., W. M. C. Rosenberg, J. A. M. Gray, et al. (1996). "Evidence based medicine:
What it is and what it isn't." BMJ 312(7023): 71-72.
Sales, A., C. Helfrich, P. M. Ho, et al. (2008). "Implementing electronic clinical reminders for
lipid management in patients with ischemic heart disease in the Veterans Health
Administration: QUERI series." Implementation Science 3(1): 28.
Sansone, C., C. C. Morf and A. T. Panter, Eds. (2003). The sage handbook of methods in social
psychology. Thousand Oaks, SAGE Publications.

116
Scott, S. D., C. A. Estabrooks, M. Allen and C. Pollock (2008). "A context of uncertainty: How
context shapes nurses' research utilization behaviors." Qualitative health research 18(3):
347-357.
Sharp, N. D., S. L. Pineros, C. Hsu, et al. (2004). "A qualitative study to identify barriers and
facilitators to implementation of pilot interventions in the Veterans Health Administration
(VHA) northwest network." Worldviews on Evidence-Based Nursing 1(2): 129-139.
Shirley, M. R. (2006). "Evidence-based practice: How nurse leaders can facilitate innovation."
Nursing Administration Quarterly 30: 252-265.
Shojania, K. G. and J. M. Grimshaw (2005). "Evidence-based quality improvement: The state of
the science." Health Aff 24(1): 138-150.
Smith, M. and P. Barnett (2008). "The role of economics in the QUERI program: QUERI series."
Implementation Science 3(1): 20.
Smitherman, G. (2005). "Mending Ontario's fracture care: The Osteoporosis Society of Canada ",
from
http://www.health.gov.on.ca/english/media/speeches/archives/sp_05/sp_022205.html.
Stacey, D., M.-P. Pomey, A. O'Connor and I. Graham (2006). "Adoption and sustainability of
decision support for patients facing health decisions: An implementation case study in
nursing." Implementation Science 1(1): 17.
Stetler, C., L. McQueen, J. Demakis and B. Mittman (2008). "An organizational framework and
strategic implementation for system-level change to enhance research-based practice:
QUERI series." Implementation Science 3(1): 30.
Stetler, C., B. Mittman and J. Francis (2008). "Overview of the VA quality enhancement
research initiative (QUERI) and QUERI theme articles: QUERI series." Implementation
Science 3(1): 8.

117
Sudsawad, P. (2007). Knowledge translation: Introduction to models, strategies and measures.
Austin, TX, Southwest Educational Development Labratory, National Centre for the
Dissemination of Disability Research.
Sutherland, J. M. and J. Walker (2008). "Challenges of rehabilitation case mix measurement in
Ontario hospitals." Health Policy 85(3): 336-348.
Tejeda, M. J., T. A. Scandura and R. Pillai (2001). "The multifactor leadership questionnaire
revisited: Psychometric properties and recommendations " The Leadership Quarterly 12:
31-52.
TCU Institute of Behavioural Research (2004) "Organizational functioning." TCU Assessment
Fact Sheet. Retrieved January 16, 2009 from, http://www.ibr.tcu.edu/evidence/TCU-
ORC-AFS.pdf
Thomas, L., N. Cullum, E. McColl, et al. (1999). “Guidelines in professions allied to medicine.”
Cochrane Database Sys Rev 1: CD000349.
Thompson, G. N., C. A. Estabrooks and L. F. Degner (2006). "Clarifying the concepts in
knowledge transfer: A literature review." Journal of advanced nursing 53(6): 691-701.
Titler, M. G. (2007). "Translating research into practice " AJN 107(6): 26-33.
Vroom, V. H. and A. G. Jago (2007). "The role of the situation in leadership." Journal of the
American Psychological Association 62(1): 17-24.
Wallace, C. and M. Legro (2008). "Using formative evaluation in an implementation project to
increase vaccination rates in high-risk veterans: QUERI series." Implementation Science
3(1): 22.
Wallin, L. (2009). "Knowledge translation and implementation research in nursing."
International Journal of Nursing Studies 46: 576-587.

118
Wallin, L., A. Rudberg and L. Gunningberg (2005). "Staff experiences in implementing
guidlines for kangaroo mother care - a qualitative study." International Journal of Nursing
Studies 42: 61-73.
Weiner, B. J., H. Amick and S.-Y. D. Lee (2008). "Conceptualization and measurement of
organizational readiness for change: A review of literature in health services research and
other fields." Medical Care Research and Review 65(4): 379-436.
Yano, E. M. (2008). "The role of organizational research in implementing evidence-based
practice: QUERI series." Implementation Science 3: 29.
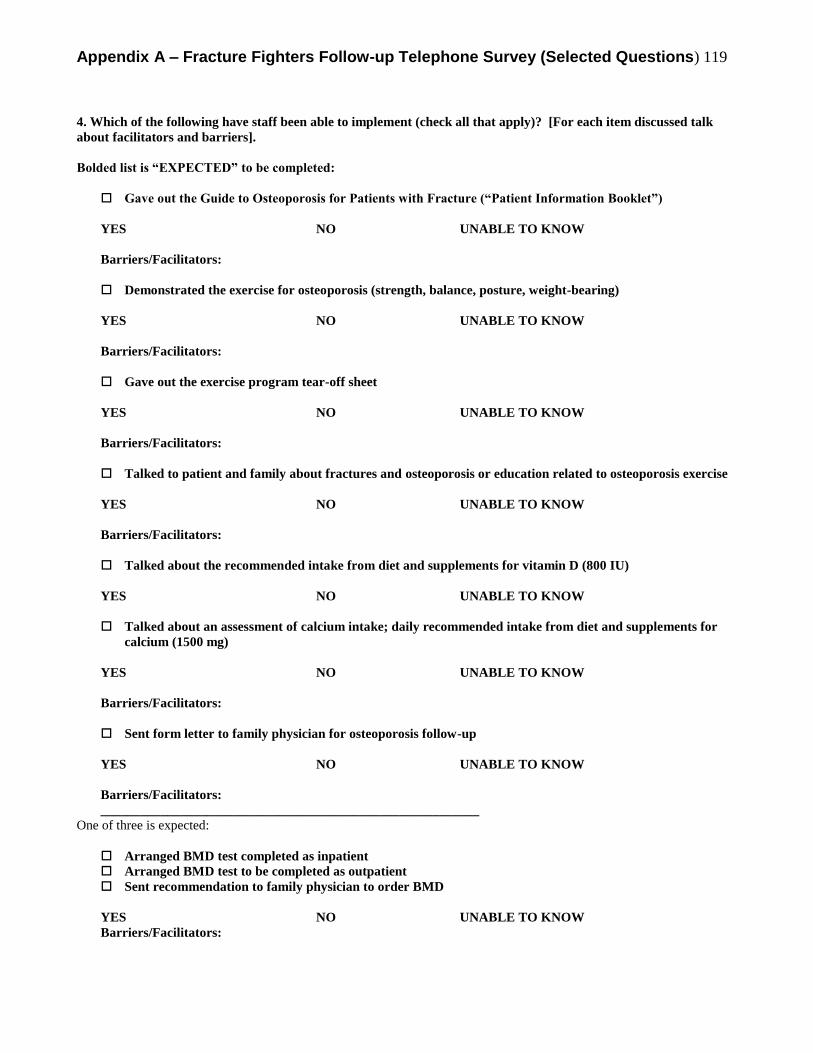
Appendix A – Fracture Fighters Follow-up Telephone Survey (Selected Questions) 119
4. Which of the following have staff been able to implement (check all that apply)? [For each item discussed talk
about facilitators and barriers].
Bolded list is “EXPECTED” to be completed:
Gave out the Guide to Osteoporosis for Patients with Fracture (“Patient Information Booklet”)
YES NO UNABLE TO KNOW
Barriers/Facilitators:
Demonstrated the exercise for osteoporosis (strength, balance, posture, weight-bearing)
YES NO UNABLE TO KNOW
Barriers/Facilitators:
Gave out the exercise program tear-off sheet
YES NO UNABLE TO KNOW
Barriers/Facilitators:
Talked to patient and family about fractures and osteoporosis or education related to osteoporosis exercise
YES NO UNABLE TO KNOW
Barriers/Facilitators:
Talked about the recommended intake from diet and supplements for vitamin D (800 IU)
YES NO UNABLE TO KNOW
Talked about an assessment of calcium intake; daily recommended intake from diet and supplements for
calcium (1500 mg)
YES NO UNABLE TO KNOW
Barriers/Facilitators:
Sent form letter to family physician for osteoporosis follow-up
YES NO UNABLE TO KNOW
Barriers/Facilitators:
_________________________________________________________
One of three is expected:
Arranged BMD test completed as inpatient
Arranged BMD test to be completed as outpatient
Sent recommendation to family physician to order BMD
YES NO UNABLE TO KNOW
Barriers/Facilitators:

Appendix A – Fracture Fighters Follow-up Telephone Survey (Selected Questions) 120
Unbolded List is “Not expected” to be completed:
Talked about a falls risk assessment
YES NO UNABLE TO KNOW
Barriers/Facilitators:
Talked about/distributed education about home environmental modifications
YES NO UNABLE TO KNOW
Barriers/Facilitators:
Osteoporosis medications initiated (based on BMD and/or risk factors)
YES NO UNABLE TO KNOW
Barriers/Facilitators:
Gave out a referral to CCAC PT for osteoporosis exercises
YES NO UNABLE TO KNOW
Barriers/Facilitators:
Gave out a referral to CCAC OT for home safety assessment
YES NO UNABLE TO KNOW
Barriers/Facilitators:

Appendix B – Knowledge Translation Theories, Models and Frameworks 121
Reference Title of KT Model,
Framework,
Theory
Key Concepts and Descriptions
Research Use Models (Types)
C. Weiss (1979)
Use models are based on the implicit view about the nature and role of the
relationship between science and practice 1. Knowledge
Driven -one way relationship
-knowledge is valuable in and of itself
-if knowledge is scientifically rigorous and legitimate, the
diffusion of knowledge will occur 2. Problem Solving
(Pull) /
Instrumental
Model
-research users (practitioners, policy makers) formulate
requests to scientists or experts in order to solve specific
problems
3. Interactive /
Deliberative -based on the assumption that the co-production of
knowledge by practitioners/users and researchers is key
-knowledge is not valuable in and of itself, but gains value
through interpretation by potential users 4. Political /
Strategic -knowledge is one resource among others to be
accumulated, exchanged or used in political nature
amongst a system of actors
-knowledge will diffuse as a result of negotiations between
actors 5. Tactical -radical type of strategic use
-knowledge is a resource that can be manipulated to
legitimize a particular position to gain some type of
advantage 6. Enlightenment -knowledge is valuable in and of itself, but not in an
instrumental way
Landry (1999) 7. Science Push -see above 8. Pull -see above 9. Interactive -see above
Logan & Graham
(1998); Graham
and Logan (2004)
10. Ottawa Model of
Research Use
(OMRU)
- integral to the OMRU process is the systematic
assessment, monitoring,
and evaluation of the state of each of the six elements prior
to, during and following any research transfer efforts
-6 elements that must be evaluated and taken into account
when developing an intervention 1) practice environment;
2) potential research adopters; 3) the evidence-based
innovation; 4) research transfer strategies; 5) evidence
adoption; 6) outcomes
-requires further development in incorporating the need for
rapidly
changing clinical assessments and in the area of validated
instruments supporting its elements and the relationships

Appendix B – Knowledge Translation Theories, Models and Frameworks 122
Reference Title of KT Model,
Framework,
Theory
Key Concepts and Descriptions
between them.
Estabrooks 2006
guide to kt theory
11. CURN (Conduct
and Utilization of
Research in
Nursing)
-knowledge is transferred through linkages when a practice
problem is encountered
-relies on reciprocal relationship between users and
producers of knowledge. Underpinned by a problem-
solving solution
Horsley 1978 CURN Identification of a clinical problem
Find and appraise research evidence
Evaluate relevance of evidence for local context
Design practice innovation and devise implementation plan
Clinical trial
Review evidence from evaluation
If positive, the devise plan to extend and disseminate to
other areas
Stetler (2001) 12. Stetler Model -knowledge transfer is influenced by internal processes and
external contexts
-relies on individual and organization to pull research into
practice
-assumes clinician is knowledge oriented rather than rule
oriented
-linking relationship
-framework for research utilization (6 phases) Preparation,
validation, comparative evaluation, decision-making
translation/application, evaluation, emphasis on
practitioners not managers to facilitate practice change
Stetler and Marram’s (1976) model of research utilization, revised by
Stetler in 1994 and 2001, was elaborated to support and guide the
individual’s utilization of nursing research findings in clinical practice.
Stetler (1994) adds that a nurse actively chooses and decides when to
use research-based knowledge in his or her clinical practice.
Estabrooks 2006
guide to kt theory
13. Iowa Model of
Research Use in
Practice
-triggers in practice act as catalysts for knowledge seeking
-relies on clinicians to pull research into practice when a
triggere is encountered and traditional knowledge cannot be
used to solve a problem
Estabrooks 2006
guide to kt theory
14. NCAST
(Nursing Child
Assessment
Satellite
Training)
-KT occurs through social channels in a predictable way
-researchers involves practitioners through the entire
research process
-relies on researcher to translate and push finding through
channels
Estabrooks 2006
guide to kt theory
15. WICHEN
(Western
Interstate
Commission on
Higher
-based on concepts of diffusion and planned change
-5 phase resource linkage model
-relies on nurses being organizational change agents
-uses problem solving approach

Appendix B – Knowledge Translation Theories, Models and Frameworks 123
Reference Title of KT Model,
Framework,
Theory
Key Concepts and Descriptions
Education in
Nursing(
Grol 2007 16. Education
Theories
17. Adult Learning
Theories
Implementation of change should be linked to professional
needs and motivation; intrinsic motivation is crucial; people
change based on experiencing problems in practice
Lavis
2003 JHSRP v8
165
18. Tool Assessment tool that research funders and research
organizations can use to measure the impact of health
research
Political
Lavis 2004
textbook
19. A framework
for
understanding
the role of ideas
in policy
change
6 models of politics are presented within the framework
range (closed decision making environment open
conflict between opposing interests)
Purpose of framework 1) Used to identify policy changes that may have come
about because of ideas
2) Used to determine the role that those ideas played in the
politics associated with the developments in question
*find potential cases for study and inform their exploration
-uses Research Use models to can help to explain the role of
ideas
Lavis 2003
milbank 81 (2)
221-48
20. What should be transferred to decision makers (the
message)?
To whom should research knowledge be transferred (the
target audience)?
By whom should research knowledge be transferred (the
messenger)?
How should research knowledge be transferred (the KT
process and support system)?
With what effect should research knowledge be
transferred (evaluation)?
Lomas 2000 21. -contextual influence on policy decision making process
-premise is establishing links between research work and
decisionmaker world (2 communities theory)
-includes schematic figure
Cognitive Theories
Grol 2007 22. Cognitive
Theories
-implementation of change needs to take into account
professional decision processes and they need good
information and methods to support their decisions in
practice

Appendix B – Knowledge Translation Theories, Models and Frameworks 124
Reference Title of KT Model,
Framework,
Theory
Key Concepts and Descriptions
-weigh consequences of different behaviours
e.g. cognitive-psychosocial model – clinicians do not act
rationally but on the basis of the previous experience and
contextual information (illness scripts or cognitive
structures)
Bucknall 2007
NR
23. Decision
Theory
-a finding becomes “evidence” only after an individual
decides the information is relevant and useful
-traditional view critized bc of inability to deal with
complexity of decisions
- non-traditional considers context surrounding the decision
maker, situational assessment, cognitive processes
Motivational Theories
Grol 2007 24. -implementation of change needs to foucs on attiutes,
perceived social norms, and experienced control related to
the desired performance
Ceccato 2007 25. Theory of
Planned
Behaviour
-attitudes, subjective norms, perceived behaviour controls
motivation to perform + behaviour intention action
Diffusion
Rogers 26. Diffusion of
Innovation
-innovation defined as any idea, practice, or item that is
perceived to be new by an individual, organization, or other
unit of adoption
-there are four interacting factors: the innovation,
communication channels, social system and time
Innovation- Decision Process (Knowledge Persuasion
Decision Implementation Confirmation)
Characteristics of the Innovation (Relative Advantage,
Complexity, Trialability, compatibility, observability)
Dobbins 2002 27. Framework for
Research
Dissemination
and Utilization
-based on ROGERS
-adoption of research evidence into health care decision
making is influenced by a variety of characteristics related
to the individual, organization, environment and innovation
-demonstrates how these characteristics interact as the
progress through the innovation – diffusion process
Havelock 1969 28. Research
Dissemination
Utilization
Conceptual
29. Framework
-based on Diffusion Theory
-knowledge building and institutionalization
Greenhalgh 2004 30. Spread of Ideas Estabrooks 2006 guide to kt - Operationalization of the
Greenhalgh framework, however, would be an unusually
complex undertaking.
31. Health Use of marketing (attractive product) is adapted to the

Appendix B – Knowledge Translation Theories, Models and Frameworks 125
Reference Title of KT Model,
Framework,
Theory
Key Concepts and Descriptions
promotion needs of a specific target audience
-promotes the attributes of the innovation
Grol 2007 32. Communication
Theories
-importance of the source of innovation (credibility), the
framing and rehearsal of messages, and the characteristics
of the message recipients
Organizational Change
Champagne
The Ability to
Manage Change
in Health Care
(White Paper)
33. Factors to be
Considered
with Producing
Change in
Organizations
-based on extensive review of 10 organizational change
models
-implementation climate, organizational structure,
(organicity, complexity, integration) trust, compatibility
with values, involvement, collectives leadership
34. Organizational
Determinants of
Change
-leaders must be human, participatory and empowering
35. Hierarchial,
Rational Model
-mechanistic view of organizations (popularized by classic
management theories)
-Change will be effective if it was well planned and the
planned process was followed
-leaders must be forward-looking and must program and
plan change with care and attention
-face validity, unsure of effectiveness
36. Organizational
Development
Approach
-an applied management approach (participatory
management style, decentralized decision make, job
enrichment programs and communication system)
-bottom up approach
-change will succeed if managers can promote the values of
participation and consensus, for example by enhancing
organizational quality of life
-extensively researched, yet variable success rates
suggesting explanatory and prescriptive power of model is
low
37. (Individual
Learning)
Psychological
Model
-emphasis on individual reaction to change
-change will be implemented if people’s natural resistance
can be overcome
-consistent with changing attitudes and relationships of
attitudes towards behaviour (assumes a sequential relation
among beliefs, attitudes, intentional and behaviours)
-leaders must be charismatic, astute psychologists who can
overcome the resistance of their troops
-managerial role is reduced to that of learning facilitator
-extensively researched, yet variable success rates
suggesting explanatory and prescriptive power of model is
low

Appendix B – Knowledge Translation Theories, Models and Frameworks 126
Reference Title of KT Model,
Framework,
Theory
Key Concepts and Descriptions
38. Structural
Model
-organizations that are successful in introducing change
stand out for their structures and their ability to adjust
structures to the requirements of change
-idea of organic organizations
-successful implementation influenced by organizational
attributes (size, centralization, formalization, levels of
expertise); context (competitiveness, degree of
urbanization); managerial attributes (locus of control,
attention to innovation)
-provide strong explanation for failed implementation, but
lessons to be drawn in terms of action and change
management are not strong
39. Political Model -adoption and implementation of change is an power game
-result in adjustment to internal and external pressures
-influential stakeholders are important
-provide strong explanation for failed implementation, but
lessons to be drawn in terms of action and change
management are not strong
40. Strategic
Management
Approach
-top strategist must work a radical transformation in
organizational culture, strategy and structure after periods
of crisis and tumult
- leaders must be entrepreneurial, visionary, strategist,
daring and ever prepared for crisis and opportunity
-face validity, unsure of effectiveness
41. Environmental
Perspectives
-environment surrounding the organization
Ecological & Institutional Models - In both cases executives are limited in their ability to
implement a strategy
- Ecological – limitation due to organizational inertia
(mechanism of change will be the result of the inertia – a
new organization)
- Institutional – executives limited by institutional
environments, change is dictated by institutional
standards
-provide strong explanation for failed implementation, but
lessons to be drawn in terms of action and change
management are not strong
42. Guru
Approaches
-change is nature, inevitable and urgent and can be brought
about by effective leadership
-combination of strategic management model, rational,
psychological, organizational development, structural and
political
Champagne
43. Organizational
Learning
-change will be successful if it is accomplished by a
collective learning process based on experimentation, trial

Appendix B – Knowledge Translation Theories, Models and Frameworks 127
Reference Title of KT Model,
Framework,
Theory
Key Concepts and Descriptions
and error
-rarely used to guide implementation of organizational
change
Edmondson 2004
-hospitals do not learn from failure bc culture of medicine
discourages admission of error thereby diminishing
potential to learn from mistakes
-workarounds and quick fixes are the dominant response to
failure rather than root cause analysis and systematic
problem solving
Grol 2007 44. Organizational
Learning
-the creation or availability of conditions in the organization
for continuous learning at all levels can lead to successful
change
-no empirical research on the theory as applied to ehatlh
care
Champagne
45. Theories of
Complexity
-change will be facilitated by encouraging complexity in the
internal organization and by promoting communication and
participation to stimulate self-organization, learning and
adjustment to environmental diversity
-rarely used to guide implementation of organizational
change
Grol 2007 46. Complexity
theory
-focus on system as a whole, find patterns in behaviour
(attractors) and link change plan to these, and test and
improve the plan
Dopson 2007
Organizational
Studies -within organizational
studies, there
has been a shift from a
dimension-based view
of context to
arguments that
conceptualize context
as consisting of broad
social network
structures and as
interactive,
interpreted,and enacted
phenomena.
47. Contingency
Theory
-attributes of the environment in which organizations are
located interact to restrict the range of viable or appropriate
organizational forms
-plays down the influence of influence of organizational
actors (leader)
-The contribution of this theory for understanding knowledge translation is
that it highlights that different styles for promoting knowledge translation
need to take into account the organizational context and there needs to be a
match between style and context. For example, directive leadership styles
are unlikely to succeed in very pluralistic contexts where power is diffuse.
48. Institutional
Theory
-adoption of innovation or change is not a means of
improving performance but a means of achieving
legitimacy within an organizational field
-choice to change based on fads and institutional pressures
-implication for knowledge translation is that organizations are more likely
to adopt best-practice recommendations where there are highly visible
models of success
within their institutional environment and where there is significant
competition

Appendix B – Knowledge Translation Theories, Models and Frameworks 128
Reference Title of KT Model,
Framework,
Theory
Key Concepts and Descriptions
Dobson 2007 49. Social Network
Theory
*Communities of
practice
-stress the importance of social relationships as the relevant
context for investigation
-attributes of individuals are less important then their
relationships and ties to others in the network
-communities of practice is a variant of this theory, involves
the study of the ways in which people work together and are
bound to one another in their persuit of solving common
issues
-a more promising approach to the study of knowledge translation is to
consider the complex interdependencies among all those within the
figuration, both those who seek to translate knowledge and those who resist
doing so
Grol 2007 50. Social Network
and Influence
Theory
Change demands local adaption of innovation and use of
local networks and opinion leaders in dissemination,
including identifying innovators and key persons in the
social network
Dopson 2007 51. Social
Psychological
Perspective
-external conditions only become known, through the
perceptions of organizational members, therefore context is
fundamentally a mental concepts
-context is wholey inacted by the by the social construction
of actors
Edgar 2006
-individual nurse
and practice
setting and socio-
political context
52. Joint Venture
Model of
Research
Utilization
1) leadership – practice of influencing people to achieve
goals
E.g nurses attribute feelings about workplace, level of
organizational commitment to leadership of nurse manager
(provide recognition, meeting nurses personal needs,
offering help or guidance, using leadership skills, meeting
unit needs, supporting the team) REF: McNeese-Smith
1997
2) emotional intelligence
3) person (individual) – self-efficacy, willingness to try new
ideas, perceived advantage of implementing knowledge,
understanding of research, professional autonomy, self-
critical inquiry, critical thinking skills, mentorship,
motivation
**Job Characteristics Model of Work Motivation (Hackman
and Oldham 1980) – most widely used model of motivation
at work -> motivation, performance, satisfaction (work
motivation arises from the characteristics of jobs)
4) message – complexity, consumer preference, clarity,
relevance; observable, testable, simple, norms of
environment
5) empowered workplace
6) socio-political environment

Appendix B – Knowledge Translation Theories, Models and Frameworks 129
Reference Title of KT Model,
Framework,
Theory
Key Concepts and Descriptions
Elder 1999 53. Health
Behaviour
Change Model
Stages of Change
Prochaska (1997) 54. Transtheoretical
Model
Health Behaviour Change. Progress through 6 stages
1) Precontemplation
2) Contemplation
3) Preparation
4) Action
5) Maintenance
6) termination
Pathman (1996) 55. Awareness-to-
Adherence
As applied to physician guidelines.
Behaviour and cognitive stages that physician must pass
through in order to adopt guidelines
1) Awareness
2) Agreement
3) Adoption
4) Adherence
Grol 2007 56. Social Learning
Theory
-changing performance take place through demonstration
and modeling and through reinforcement by others
e.g. Bandura Social Cognitive Theory
Grol 2007 57. Theories of
teamwork
-more effective teams are better able to make necessary
change to improve care because they share goals and are
able to share knowledge
Grol 2007 58. Theories of
professional
development
-professional loyalty, pride and consensus and
“reinvention” of change proposal by professional body are
important
Grol 2007 59. Theories of
leadership
Involvement and commitment of leaders and (top)
management in change process are important
Grol 2007 60. Theory of
innovative
organizations
Implementation should take into account the type of
organization; decentralized decision making (teams) about
innovation is important
Grol 2007 61. TQM (Total
Quality
Management)
or CQI
(continuous
quality
improvement)
-Improvement is a continuous cyclic process, shich plans
for change continually adapted on the basis of previous
experience; organization-wide measure are aimed at
improving culture, collaboration, customer focus, and
process
-pdsa cycles
Grol 2007 62. Theories of
integrated care
-change multidisciplinary care processes and collaboration
instead of individual decision making
Grol 2007 63. Reimbursement
theories
Attractive rewards and (financial) incentives can influence
the volume of specific activities

Appendix B – Knowledge Translation Theories, Models and Frameworks 130
Reference Title of KT Model,
Framework,
Theory
Key Concepts and Descriptions
64. Pay for
performance
Grol 2007 65. Theory of
contracting
-contractual agreements can guide professional and
organizational performance
Estabrooks 2006
guide to kt theory
66. Organizational
Innovation
Models
-tend to focus on explanation rather than
prescription and are circumscribed in the particular
aspect of innovation they address
Estabrooks 2006
guide to kt theory
67. Model of
Territorial
Rights and
Boundaries
Innovations are perceived as threats to existing
organizational practices and interests
Estabrooks 2006
guide to kt theory
68. Dual Core
Model of the
innovation
-innovations originate from cores that serve different
purposes
Estabrooks 2006
guide to kt theory
69. Ambidextrous
Model
-high structural complexity, low formalization and low
centralization initative innovation but the inverse conditions
facilitate implementation
-orgs with diverse and differentiated task structures initative
more innovations and those whith formalized and
centralized structures implement more innovations
Estabrooks 2006
guide to kt theory
70. Bandwagon
Model
-orgs are promoted to adopt and innovation through fear
that other organizations are benefitting
-adoption occurs regardless of how the innovation is
perceived by an organization
Estabrooks 2006
guide to kt theory
71. Desperation
Reaction Model
-innovations intended to address desparte situations diffuse
differently than other innovations.
Interactive Models
Jacobsen 2003 72. Understanding
the User
Context
Domains to consider when planning research-decision
maker:
User group
Issue
Research
Researcher-user relationship
Dissemination strategy
*Lists questions to ask for each domain
Majdzadeh (2008) 73. A knowledge translation cycle is described, with five
domains: knowledge creation, knowledge transfer, research
utilization, question transfer, and the context of
organization. Discussion: The knowledge translation cycle
offers a theoretical basis for identifying basic requirements
and linking mechanisms in the translation of knowledge for
research utilization.
74. Five stages: building a case for action, identifying

Appendix B – Knowledge Translation Theories, Models and Frameworks 131
Reference Title of KT Model,
Framework,
Theory
Key Concepts and Descriptions
contributory factors and points of intervention, defining
opportunities for action, evaluating potential interventions
and selecting a portfolio of specific policies, programmes
and actions. Each stage is cumulative and culminates in the
development of a plan to support the combination of
research evidence, theoretical perspectives and contextual
factors into a plan for translation into action
Kontos & Poland
(2009)
75. Critical
Realism and the
Arts Research
Utilization
Model
(CRARUM)
CRARUM has the potential to strengthen the science of
implementation research by addressing the complexities of
practice settings, and engaging potential adopters to
critically reflect on existing and proposed practices and
strategies for sustaining change
Stetler (2008) 76. QUERI Quality
Enhancement
Research
Initiative
1) Identify high-risk/high-volume diseases or problems.
2) Identify best practices.
3) Define existing practice patterns and outcomes across the
VA and current variation from best practices.
4) Identify and implement interventions to promote best
practices.
5) Document that best practices improve outcomes.
6) Document that outcomes are associated with improved
health-related quality of life.
Within Step 4, QUERI implementation efforts generally
follow a sequence of four phases to enable the refinement
and spread of effective and
sustainable implementation programs across multiple VA
medical centers and clinics. The phases include:
1) Single site pilot,
2) Small scale, multi-site implementation trial,
3) Large scale, multi-region implementation trial, and
4) System-wide rollout
Boissel (2004) 77. Eight-step
approach to
bridge the gap
between
research
information and
physician
prescription
-designed to optimize the indirect channel
1. identify and comprehensivly collect pertinent research
data
2. summarize individual study data – standardized format
3. assign level of evidence score for each study
4. rand related studies by assigned score
5. summarize – perform a meta-analysis
6. prepare coherent messages from summaried findings of
relevant studies
7.Relevant, efficient and neutral presentation
8. Transmit message “just in time” to physicians (e.g.

Appendix B – Knowledge Translation Theories, Models and Frameworks 132
Reference Title of KT Model,
Framework,
Theory
Key Concepts and Descriptions
online, e-bulletins)
Burrows (1995)
78. Review current practice motivation to change identify
relevant evidence and appraise implement in practice
Goode 1992 79. EB
multidisciplinar
y clinical
practice model.
Organisational commitment change agents planned
change process outcome (research based practice)
Provide an example of how model was used to improve
quality and decrease cost
Boissel, J.-P., E. Amsallem, M. Cucherat, et al. (2004). "Bridging the gap between therapeutic research results and physician prescribing decisions: Knowledge transfer, a prerequisite to knowledge translation." European Journal of Clinical Pharmacology 60(9): 609-616.
Bucknall, T. (2007). "A gaze through the lens of decision theory toward knowledge translation
science." Nursing Research 56(4S): S60-66. Burrows, D. E. and K. McLeish (1995). "A model for research-based practice." Journal of
Clinical Nursing 4(4): 243-247. Ceccato, N. E., L. E. Ferris, D. Manuel and J. Grimshaw (2007). "Adopting health behaviour
change theory throughout the clinical practice guideline process." Journal of Continuing Education in the Health Professions 27(4): 201-207.
Champagne, F. (2002). The ability to manage change in health care organizations.
Commision on the Future of Health Care in Canada. Dobbins, M., D. Ciliska, R. Cockerill, et al. (2002). "A framework for the dissemination and
utilization or research for health-care policy and practice." The Online Journal of Knowledge Synthesis for Nursing 9(7).
Dopson, S. (2007). "A view from organizational studies." Nursing Research 56(4S): S72-S77. Edgar, L., S. Lambert, R. Herbert, et al. (2006). "The joint venture model of knowledge
utilization: A tool for change in nursing." Canadian Journal of Nursing Leadership 19(2): 41-55.
Estabrooks, C. A., D. S. Thompson, J. E. Lovely and A. Hofmeyer (2006). "A guide to
knowledge translation theory." The Journal of Continuing Education in the Health Professions 26: 25-36.

Appendix B – Knowledge Translation Theories, Models and Frameworks 133
Graham, K. and J. Logan (2004). "Using the ottawa model of research use to implement a skin care program." Journal of Nursing Care & Quality 19(1): 18-24.
Greenhalgh, T., G. Robert, F. Macfarlane, et al. (2004). "Diffusion of innovations in service
organizations: Systematic review and recommendations." The Milbank quarterly 82(4): 581-629.
Goode, C. J. and F. Piedalue (1999). "Evidence-based clinical practice." Journal of Nursing
Administration 29(6): 15-21. Grol, R., M. Bosch, M. E. J. L. Hulscher, et al. (2007). "Planning and studying improvement in
patient care: The use of theoretical perspectives." Havelock, R. G. (1969). Planning for innovation through dissemination and utilization of
knowledge. Ann Arbor, Center for Research on Utilization of Scientific Knowledge. Horsley, J.-A., Y. Crane and J. D. Bingle (1978). "Research utilization as an organizational
process." Journal of Nursing Administration 8(7): 4-6. Jacobson, N., D. Butterill and P. Goering (2003). "Development of a framework for knowledge
translation: Understanding user context." Journal of Health Services and Policy Research 8(2): 94-99.
Kontos, P. and B. Poland (2009). "Mapping new theoretical and methodological terrain for
knowledge translation: Contributions from critical realism and the arts." Implementation Science 4(1): 1.
Landry, R. N., N. Amara and M. Lamari (2001). "Utilization of social science research
knowledge in canada." Research Policy 30(2): 333-349. Lavis, J. N., S. E. Ross, C. McLeod and A. Glidner (2003). "Measuring the impact of health
research." Journal of Health Services Research and Policy 8(3): 165-170. Lavis, J. N. (2004). "A political science perspective on evidence-based decision-making."
Using Knowledge and Evidence in Health Care: Multidisciplinary Perspectives on Evidence-Based Decision-Making in Health Care(Journal Article): 70-85.
Lavis, J. N., D. Robertson, J. M. Woodside, et al. (2003). "How can research organizations
more effectively transfer research knowledge to decision makers?" Milbank Quarterly 81(2): 221-248.
Logan, J. and I. D. Graham (1998). "Toward a comprehensive interdisciplinary model of
health care research use." Science Communication 20.

Appendix B – Knowledge Translation Theories, Models and Frameworks 134
Lomas, J. (2000). "Connecting research and practice." ISUMA: Canadian Journal of Policy Research 1(1): 140-144.
Majdzadeh, R., J. Sadighi, S. Nejat, et al. (2008). "Knowledge translation for research
utilization: Design of a knowledge translation model at tehran university of medical sciences." Journal of Continuing Education in the Health Professions 28(4): 270-277.
Pathman, D. E., T. R. Konrad, G. L. Freed, et al. (1996). "The awareness-to-adherence
model of the steps to clinical guideline compliance - the case of pediatric vaccine recommendations." Medical Care 34(9): 873-889.
Prochaska, J. O. and W. F. Velicer (1997). "Behavior change: The transtheoretical model of
health behavior change." American Journal of Health Promotion 12: 38-48. Rogers, E. M. (1995). Diffusion of innovations. New York, Free Press. Stetler, C. B. (2001). "Updating the stetler model of research utilization to facilitate evidence-
based practice." Nursing Outlook 49(6): 272-279. Stetler, C., B. Mittman and J. Francis (2008). "Overview of the va quality enhancement
research initiative (queri) and queri theme articles: Queri series." Implementation Science 3(1): 8.
Weiss, C. H. (1979). "The many meanings of research utilization." Public administration
review 39(Journal Article): 426-431.

Appendix C – Outline of PARiHS Elements 135
EVIDENCE
Research LOW ---------------------------------------------------------------------------------------------------------------HIGH
Poorly conceived, designed and/or
executed research
Well conceived, designed, executed research appropriate to
question
Seen as only type of evidence See as one part of decision
Not valued as evidence Lack of uncertainty acknowledged
Seen as certain Social construction acknowledged
Judged as relevant
Importance weighed
Conclusions drawn
Clinical
Experience
LOW ---------------------------------------------------------------------------------------------------------------HIGH
Anecdote, with no critical reflection and
judgement
Clinical experience/ expertise reflected upon, tested by
individuals and groups
Lack of consensus within similar group Consensus within similar groups
Not valued as evidence Valued as evidence
Seen as only one type of evidence Seen as one part of the decision
Judged as relevant
Importance weighed
Conclusions drawn
Patient
Experience
LOW ---------------------------------------------------------------------------------------------------------------HIGH
Not valued as evidence Valued as evidence
Patients not involved Multiple biographies used
Seen as only type of evidence Partnerships with health care professionals
Seen as only one part of a decision
Judged as relevant
Importance weighed
Conclusions drawn
CONTEXT
Context LOW ---------------------------------------------------------------------------------------------------------------HIGH
Lack of clarity around boundaries Physical/social/cultural/structural/system bound clear defined
Lack of appropriateness and transparency Appropriateness and transparent decision making processes
Lack of power and authority Power and authority processes
Lack of resources
Lack of information and feedback Information and feedback
Not receptive to change Receptiveness to change
Culture LOW ---------------------------------------------------------------------------------------------------------------HIGH
Unclear values and beliefs Able to define culture(s) in terms of prevailing values/ beliefs
Low regard for individuals Values individuals and clients
Task driven organization Promotes learning organization
Lack of consistency Consistency of individual role/experience to value:
Relationships with others
Teamwork
Power and authority
Rewards and recognition
Leadership LOW ---------------------------------------------------------------------------------------------------------------HIGH
Traditional, command and control Transformational leadership
Lack of role clarity Role clarity
Lack of teamwork Effective teamwork
Poor organizational structures Effective organizational structures
Autocratic decision making processes Democratic inclusive decision making
Didactic approach to
learning/teaching/managing
Enabling/empowering approach to learning/ teach/ managing
Evaluation LOW ---------------------------------------------------------------------------------------------------------------HIGH
Absence of any form of feedback Feedback on 1) individual; 2) team; 3) system performance
Narrow use of performance information
sources
Use of multiple sources of information on performance
Evaluations rely on single rather than
multiple methods
Use of multiple methods 1) clinical; 2) performance; 3)
economic; 4) experience of evaluations
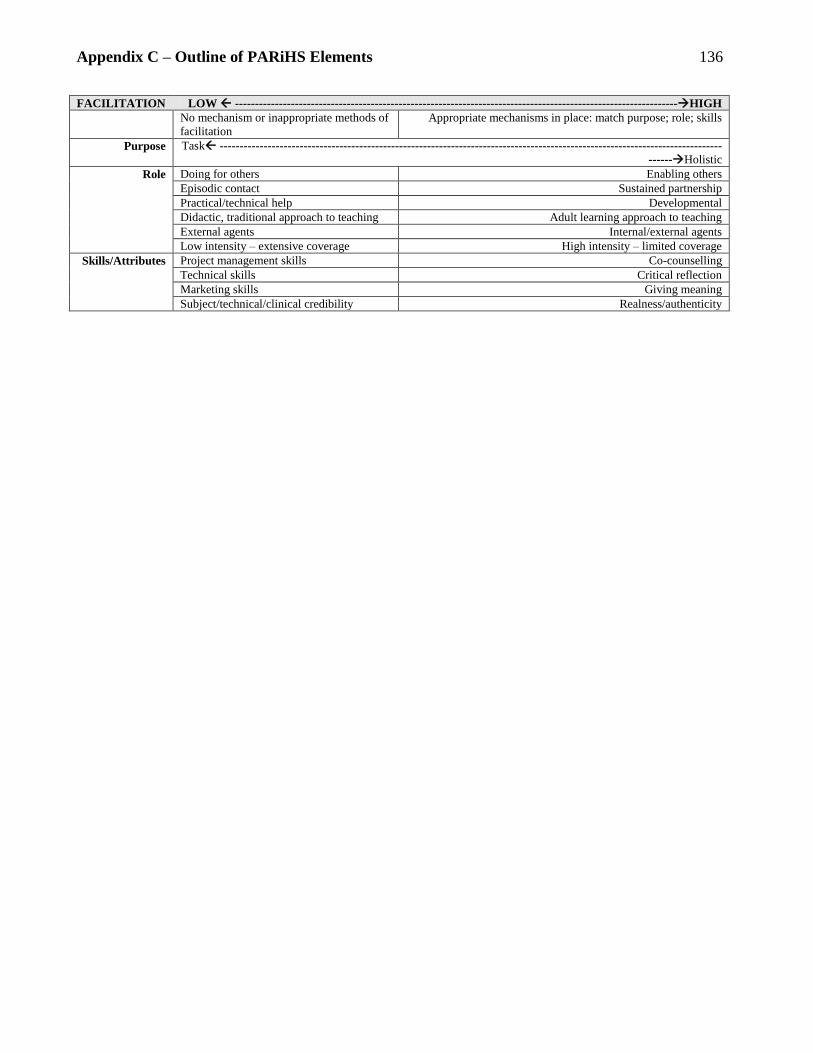
Appendix C – Outline of PARiHS Elements 136
FACILITATION LOW ---------------------------------------------------------------------------------------------------------------HIGH
No mechanism or inappropriate methods of
facilitation
Appropriate mechanisms in place: match purpose; role; skills
Purpose Task ------------------------------------------------------------------------------------------------------------------------------
------Holistic
Role Doing for others Enabling others
Episodic contact Sustained partnership
Practical/technical help Developmental
Didactic, traditional approach to teaching Adult learning approach to teaching
External agents Internal/external agents
Low intensity – extensive coverage High intensity – limited coverage
Skills/Attributes Project management skills Co-counselling
Technical skills Critical reflection
Marketing skills Giving meaning
Subject/technical/clinical credibility Realness/authenticity

Appendix D – Information Letters and Consent Forms 137
Clinical Coach Version Title of research project: Promoting Action on Research Implementation in Health Services
(PARIHS) Framework: Application to the Fracture Fighters Program Investigator: Ms. Vinita Bansod, MSc Student Department of Health Policy, Management and Evaluation, University of Toronto 155 College Street, Suite 425 Toronto, ON M5T 3M6 [email protected] or [email protected] Telephone: (416) 351-3732 x 2321 Fax: (416) 351-3746 Supervisor: Dr. Susan Jaglal Department of Physical Therapy, University of Toronto 160-500 University Avenue Toronto, ON M5G 1V7 [email protected] (416) 978-0315 Sponsor/Funding: The Fracture Fighters program is funded by the Ministry of Health and Long-Term Care Ontario Osteoporosis Strategy. The student investigator has received funding for Master studies from the Canadian Institutes of Health Research. Background & Purpose of Research: This study is being completed as part of a Master’s thesis in the Department of Health Policy, Management and Evaluation at the University of Toronto. Participants will include 36 inpatient rehabilitation clinicians who participated in the Fracture Fighters program as a Clinical Coach as well as their managers. The goal of this study is to apply the Promoting Action for Research Implementation in Health Services Framework to the Fracture Fighters program in order to describe factors that may have influenced the implementation of osteoporosis best practices for fracture patients. These factors include: the research and program content; organizational culture in participating inpatient rehabilitation units; management styles and the skills of clinical coach facilitators. This survey is the first of two sets of surveys included in the study. The second set of surveys will be completed with inpatient rehabilitation managers. Eligibility: To participate in this study you must be a Clinical Coach from one of thirty-six inpatient rehabilitation units participating in the Fracture Fighters program. Procedures (What is required of you?) If you are interested in participating, please sign the bottom of this (YELLOW) consent form and complete the BLUE survey provided in your package to the best of your ability. You are being provided a copy of the consent form to keep for your records. The survey should take between 20-30 minutes to complete. When you are finished with the survey, please mail it back in the envelope provided or fax to: (416) 351-3746 ATTENTION Vinita Bansod

Appendix D – Information Letters and Consent Forms 138
Voluntary Participation & Early Withdrawal: Your participation is entirely voluntary. You may choose to participate or withdraw at any time. You may also refuse to answer specific survey questions. Refusal to participate will not result in any penalty, loss of benefits (including legal) to which you are otherwise entitled. Risks/Benefits: There are no direct benefits to participating in the study. You will receive $50 for completing the survey. The results could also possibly help with planning future best-practice programs in a more effective way. The risks to participating are minor, your individual results will only be known to the student investigator and will never be reported in an individual manor. There is no risk that individual information will be shared with your department, hospital or colleagues. There are no costs to participating in this study. Privacy & Confidentiality All information you provide will be kept strictly confidential. Confidentiality can only be guaranteed to the extent permitted by law. No identifying information will be included in any reports or summaries of this research. Only the student researcher (Vinita Bansod) will have access to paper copies of the surveys and consent forms. Individual responses will not be shared with the Fracture Fighters implementation team, your hospital, unit manager or staff. All survey responses will be inputted into a computerized password protected database. No names or identifying information will be included in the database. Hard copies of the survey and consent forms will be locked in separate secure filing cabinets, only accessible to the student investigator. Hard copies will be destroyed at the completion of this thesis project (September 2009). Electronic copies will be retained for 5 years as per the requirements of research institutions. Publication of research findings: Publication of the results of the survey will only be reported in aggregate. Individual responses will not be reported and no respondent names will be included. Research participants may request a copy of the final thesis report. If you have questions about your rights as a research participant, please contact Jill Parsons, Health Sciences Ethics Review Officer, Ethics Review Office, University of Toronto, at telephone 416-946-5806 or by email: [email protected].” Signature:________________ Printed Name: _____________________ Date: ________________ Additional information: Please provide your mailing address so we may send you your $50 gift card.

Appendix D – Information Letters and Consent Forms 139
Manager Version Title of research project: Promoting Action on Research Implementation in Health Services
(PARIHS) Framework: Application to the Fracture Fighters Program Investigator: Ms. Vinita Bansod, MSc Student Department of Health Policy, Management and Evaluation, University of Toronto 155 College Street, Suite 425 Toronto, ON M5T 3M6 [email protected] or [email protected] (416) 351-3783 x 2321 Supervisor: Dr. Susan Jaglal Department of Physical Therapy, University of Toronto 160-500 University Avenue Toronto, ON M5G 1V7 [email protected] (416) 978-0315 Sponsor/Funding: The student investigator has received funding for Masters studies from the Canadian Institutes of Health Research. Background & Purpose of Research: This study is being completed as part of a Masters thesis in the Department of Health Policy, Management and Evaluation at the University of Toronto. Participants will include 36 inpatient rehabilitation clinicians who participated in the Fracture Fighters program as a Clinical Coach as well as their managers. The goal of this study is to apply the Promoting Action for Research Implementation in Health Services Framework to the Fracture Fighters program in order to describe factors that may have influenced the implementation of osteoporosis best practices for fracture patients. These factors include: the research and program content; organizational culture in participating inpatient rehabilitation units; management styles and the skills of clinical coach facilitators. This survey is the second of two sets of surveys included in the study. The first set of surveys was completed by clinical coaches of the Fracture Fighters program. Eligibility: To participate in this study you must be a manager of one of thirty-six inpatient rehabilitation units participating in the Fracture Fighters program. Procedures (What is required of you?) If you are interested in participating, please sign the bottom of this consent form and provide suggested dates and times to complete a telephone survey. If you agree, the student investigator will call you during your suggested time to complete a short 5-10 minute survey.

Appendix D – Information Letters and Consent Forms 140
Voluntary Participation & Early Withdrawal: Your participation is entirely voluntary. You may choose to participate or withdraw at any time. You may also refuse to answer specific survey questions. Refusal to participate will not result in any penalty, loss of benefits (including legal) to which you are otherwise entitled. Risks/Benefits: There are no direct benefits to participating in the study. You will receive a $50 gift card for completing the survey. In addition, the survey results could possibly help with planning future best-practice programs in a more effective way. The risks to participating are minor, your individual results will only be known to the student investigator and will never be reported in an individual manor. There is no risk that individual information will be shared with your department, hospital or colleagues. There are no costs to participating in this study. Privacy & Confidentiality All information you provide will be kept strictly confidential. Confidentiality can only be guaranteed to the extent permitted by law. No identifying information will be included in any reports or summaries of this research. Only the student researcher (Vinita Bansod) will have access to paper copies of the surveys and consent forms. Individual responses will not be shared with the Fracture Fighters implementation team, your hospital, unit manager or staff. All survey responses will be inputted into a computerized password protected database. No names or identifying information will be included in the database. Hard copies of the survey and consent forms will be locked in separate secure filing cabinets, only accessible to the student investigator. Hard copies will be destroyed at the completion of this thesis project (September 2009). Electronic copies will be retained for 5 years as per the requirements of research institutions. Publication of research findings: Publication of the results of the survey will only be reported in aggregate. Individual responses will not be reported and no respondent names will be included. Research participants may request a copy of the final thesis report. If you have questions about your rights as a research participant, please contact Jill Parsons, Health Sciences Ethics Review Officer, Ethics Review Office, University of Toronto, at telephone 416-946-5806 or by email: [email protected].” Signature:____________________ Printed Name:_______________ Date:_________________
Schedule for Phone Call (You may also request evenings and weekends) Preferred Dates/Times for Call: _____________________________________________________ Preferred Phone Number: _____________________________________________________ Please provide your mailing address so we may send you your $50 gift card:

Appendix E – Survey Instruments CLINICAL COACH QUESTIONNAIRE ID/NAME: ____141
SECTION A: EVIDENCE
This first set of questions will ask you to rate the evidence provided by the Fracture Fighters program. This includes evidence from research, clinical expertise and patient experiences. Please rate each statement on the following scale:
Research
1. I value the research evidence provided by Fracture Fighters 1 2 3 4 5
2. The Fracture Fighters research evidence fits with my understanding of fractures and osteoporosis management
1 2 3 4 5
3. The Fracture Fighters research evidence is useful in thinking about the issue of osteoporosis management for fracture patients
1 2 3 4 5
4. I am clear about what the key messages for the Fracture Fighters intervention are
1 2 3 4 5
5. There is consensus amongst my colleagues about the usefulness of Fracture Fighters research to the issue of osteoporosis management in fracture patients
1 2 3 4 5
Clinical Expertise
6. I have reflected on my own clinical experience in relation to fractures and osteoporosis
1 2 3 4 5
7. I have shared and critically reviewed my clinical experience in relation fractures and osteoporosis
1 2 3 4 5
8. I have shared and critically reviewed my clinical experience with knowledgeable colleagues outside of my (clinical) workplace
1 2 3 4 5
9. There is a consensus of (clinical) experience about the FF osteoporosis best-practices
1 2 3 4 5
10. Clinical experience will be used as one part of the evidence for implementing the program
1 2 3 4 5
11. The consensus of clinical experience fits with my understanding of fractures and osteoporosis
1 2 3 4 5
Patient Experiences
12. We routinely (and systematically) collect patients’ experiences about fractures and osteoporosis follow-up
1 2 3 4 5
13. Patients experiences will be used as one part of the evidence 1 2 3 4 5
14. I value patient experiences as evidence 1 2 3 4 5
15. The evidence of patients experiences fits my understanding of the issue(s) 1 2 3 4 5
16. Patient experiences are useful in thinking about the osteoporosis best-practices
1 2 3 4 5
17. There is a consensus amongst my colleagues about the usefulness of patient experiences to osteoporosis management in fracture patients
1 2 3 4 5
Strongly Disagree Disagree Neutral Agree Strongly Agree
<1> <2> <3> <4> <5>

Appendix E – Survey Instruments CLINICAL COACH QUESTIONNAIRE ID/NAME: ____142
SECTION B: MULTI-FACTOR LEADERSHIP SCALE
Name of Manager:__________________________________________ The next questionnaire is to describe the leadership style of your inpatient rehabilitation manager (NAME) as you perceive it. Please do your best to answer all items. If an item is irrelevant, or if you are unsure or do not know the answer, let me know and we can leave the answer blank. Please answer this questionnaire anonymously.
Instructions: Judge how frequently each statement fits the person you are describing. Use the following rating scale:
THE PERSON I AM RATING. . .
1. Provides me with assistance in exchange for my efforts 0 1 2 3 4
2. Re-examines critical assumptions to question whether they are appropriate 0 1 2 3 4
3. Fails to interfere until problems become serious 0 1 2 3 4
4. Focuses attention on irregularities, mistakes, exceptions, and deviations from standards
0 1 2 3 4
5. Avoids getting involved when important issues arise 0 1 2 3 4
6. 0 1 2 3 4
7. 0 1 2 3 4
8. 0 1 2 3 4
9. 0 1 2 3 4
10. 0 1 2 3 4
11. 0 1 2 3 4
12. 0 1 2 3 4
13. 0 1 2 3 4
14. 0 1 2 3 4
15. 0 1 2 3 4
16. 0 1 2 3 4
17. 0 1 2 3 4
18.
0 1 2 3 4
Not at all Once in awhile Sometimes Fairly Often Frequently, if not always
<0> <1> <2> <3> <4>

Appendix E – Survey Instruments CLINICAL COACH QUESTIONNAIRE ID/NAME: ____143
19. 0 1 2 3 4
20. 0 1 2 3 4
21. 0 1 2 3 4
22. 0 1 2 3 4
23. 0 1 2 3 4
24. 0 1 2 3 4
25. 0 1 2 3 4
26. 0 1 2 3 4
27. 0 1 2 3 4
28. 0 1 2 3 4
29. 0 1 2 3 4
30. 0 1 2 3 4
31. 0 1 2 3 4
32. 0 1 2 3 4
33. 0 1 2 3 4
34. 0 1 2 3 4
35. 0 1 2 3 4
36. 0 1 2 3 4
37. 0 1 2 3 4
38. 0 1 2 3 4
39. 0 1 2 3 4
40. 0 1 2 3 4
41. 0 1 2 3 4
42. 0 1 2 3 4
43. 0 1 2 3 4
44. 0 1 2 3 4
45. 0 1 2 3 4
Not at all Once in awhile Sometimes Fairly Often Frequently, if not always
<0> <1> <2> <3> <4>

Appendix E – Survey Instruments CLINICAL COACH QUESTIONNAIRE ID/NAME: ____144
SECTION C: ORGANIZATIONAL CLIMATE The next set of questions will ask you about your view of the organizational climate of your inpatient rehabilitation unit. Please rate each statement on the following scale:
Mission
1. Some staff get confused about the main goals for this inpatient rehabilitation
unit. ® 1 2 3 4 5
2. Program staff understand how this inpatient rehabilitation unit fits as part of the treatment system in your community.
1 2 3 4 5
3. Your duties are clearly related to the goals of this inpatient rehabilitation unit. 1 2 3 4 5
4. This inpatient rehabilitation unit operates with clear goals and objectives. 1 2 3 4 5
5. Management here has a clear plan for this inpatient rehabilitation unit. 1 2 3 4 5
Cohesion
6. Staff in your inpatient rehabilitation unit all get along very well. 1 2 3 4 5
7. There is too much friction among staff members in my inpatient rehabilitation
unit. ® 1 2 3 4 5
8. The staff in my inpatient rehabilitation unit always work together as a team. 1 2 3 4 5
9. Staff in my inpatient rehabilitation unit are always quick to help one another when needed.
1 2 3 4 5
10. Mutual trust and cooperation among staff in my inpatient rehabilitation unit are strong.
1 2 3 4 5
11. Some staff in my inpatient rehabilitation unit do not do their fair share of
work. ® 1 2 3 4 5
Autonomy
12. Treatment planning decisions for clients here often have to be revised by a
supervisor. ® 1 2 3 4 5
13. Management here fully trusts your professional judgment. 1 2 3 4 5
14. Clinicians here are given broad authority in treating their own clients. 1 2 3 4 5
15. Clinicians here often try out different techniques to improve their effectiveness.
1 2 3 4 5
16. Staff members are given too many rules here. ® 1 2 3 4 5
Strongly Disagree Disagree Uncertain Agree Strongly Agree
<1> <2> <3> <4> <5>

Appendix E – Survey Instruments CLINICAL COACH QUESTIONNAIRE ID/NAME: ____145
Communication
17. Ideas and suggestions from staff get fair consideration by program management.
1 2 3 4 5
18. The formal and informal communication channels here work very well. 1 2 3 4 5
19. Program staff are always kept well informed. 1 2 3 4 5
20. More open discussions about program issues are needed here. ® 1 2 3 4 5
21. Staff members always feel free to ask questions and express concerns in this program.
1 2 3 4 5
Stress
22. You are under too many pressures to do your job effectively. 1 2 3 4 5
23. Staff members often show signs of stress and strain. 1 2 3 4 5
24. The heavy workload here reduces program effectiveness. 1 2 3 4 5
25. Staff frustration is common here. 1 2 3 4 5
Change
26. Novel treatment ideas by staff are discouraged. ® 1 2 3 4 5
27. It is easy to change procedures here to meet new conditions. 1 2 3 4 5
28. You frequently hear good staff ideas for improving treatment. 1 2 3 4 5
29. The general attitude here is to use new and changing technology. 1 2 3 4 5
30. You are encouraged here to try new and different techniques. 1 2 3 4 5
Strongly Disagree Disagree Uncertain Agree Strongly Agree
<1> <2> <3> <4> <5>

Appendix E – Survey Instruments CLINICAL COACH QUESTIONNAIRE ID/NAME: ____146
SECTION D: EVALUATION
Please check which parts of the Fracture Fighters program your inpatient rehabilitation unit participated in. 1. Did your unit participate in the environmental scan ? □ YES □ NO
2. Are you a member of the Fracture Fighters advisory committee? □ YES □ NO
3. Do you provide your manager with regular updates about the Fracture Fighters program? □ YES □
NO
4. Did your unit participate in the audit checklist phase of the project? □ YES □ NO
5. Did you circulate the Fracture Fighters newsletter to your colleagues? □ YES □ NO
6. Is your unit participating in the Patient Survey phase of the project? □ YES □ NO
SECTION E: OPINION LEADERSHIP
For each of the following statements, please indicate the number that most closely matches your view of the opinions stated. The items are scaled from 1 to 7, with a higher number meaning stronger agreement B1. My opinion on osteoporosis best-practices seems not to count with other people ®
Strongly Disagree Strongly Agree
<1> <2> <3> <4> <5> <6> <7>
B2. When they choose how to treat fracture patients other people do not turn to me for advice ®
Strongly Disagree Strongly Agree
<1> <2> <3> <4> <5> <6> <7>
B3. Other people [rarely] come to me for advice about osteoporosis best practices ®
Strongly Disagree Strongly Agree
<1> <2> <3> <4> <5> <6> <7>
B4. People know how to treat fracture patients based on what I have told them
Strongly Disagree Strongly Agree
<1> <2> <3> <4> <5> <6> <7>
B5. I often persuade colleagues to treat fracture patients they way that I do
Strongly Disagree Strongly Agree
<1> <2> <3> <4> <5> <6> <7>
B6. I often influence my colleagues opinions about treating fracture patients
Strongly Disagree Strongly Agree
<1> <2> <3> <4> <5> <6> <7>

Appendix E – Survey Instruments CLINICAL COACH QUESTIONNAIRE ID/NAME: ____147
SECTION F: FRACTURE FIGHTERS BEST-PRACTICES
Please select the Osteoporosis best practices that your inpatient rehabilitation unit currently implements Education Gave out the Guide to Osteoporosis for Patients with Fracture (“Patient Information Booklet”) □ YES □ NO Exercise Demonstrated the exercise for osteoporosis (strength, balance, posture, weight-bearing) □ YES □ NO Nutrition Talked about the recommended intake from diet and supplements for vitamin D (800 IU) □ YES □ NO Post-Fracture Follow-up Arranged BMD test completed as inpatient □ YES □ NO Arranged BMD test to be completed as outpatient □ YES □ NO
Sent recommendation to family physician to order BMD □ YES □ NO Sent form letter to family physician for osteoporosis follow-up □ YES □ NO
SECTION H: Demographics and Practice Information
1) Age: __________
2) Gender □ male □female
3) What is your profession? □PT □OT □SLP □RN □RPN □ Other _________
4) Highest Degree obtained? □Certificate □BSc □Entry level masters □Other ______
5) Year of Graduation __________
6) Years in present unit/job? __________
7) FTE Status/Number of Hours? __________

Appendix E – Survey Instruments CLINICAL COACH QUESTIONNAIRE ID/NAME: ____148
Thank you for your feedback on the Fracture Fighters implementation strategy. Finally, are there any
additional comments about barriers and facilitators to implementing the program that you would like
to mention?
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________

Appendix E – Survey Instruments MANAGER QUESTIONNAIRE ID/MANAGER NAME: ____149
SECTION A: CHAMPION BEHAVIOUR SCALE
When answering the following set of questions, please think about the staff member who was trained for or acted as the Clinical Coach for the Fracture Fighters Program (Insert Name of Coach: __________________________) Please rate the following statements on this scale:
(Name of Coach) Demonstrates conviction in the Fracture Fighters Program
46. Expresses confidence in what the Fracture Fighters program can do 0 1 2 3 4
47. Points out reasons why the Fracture Fighters program will succeed 0 1 2 3 4
48. Enthusiastically promotes the Fracture Fighters program’s advantages 0 1 2 3 4
49. Expresses strong conviction about the Fracture Fighters program 0 1 2 3 4
50. Keeps pushing enthusiastically for the Fracture Fighters program 0 1 2 3 4
51. Shows optimism about the success of the Fracture Fighters program 0 1 2 3 4
(Name of Coach) Builds involvement and support
52. Gets the key decision makers involved 0 1 2 3 4
53. Secures the top level support required 0 1 2 3 4
54. Gets problems into the hands of those who can solve them 0 1 2 3 4
55. Gets the right people involved in the innovation 0 1 2 3 4
56. Makes improvements based on feedback received 0 1 2 3 4
(Name of Coach) Persists under adversity
57. Persists in the face of adversity 0 1 2 3 4
58. Does not give up when others say it cannot be done 0 1 2 3 4
59. Sticks with it 0 1 2 3 4
60. Knocks down barriers to the implementing the Fracture Fighters program 0 1 2 3 4
61. Shows tenacity in overcoming obstacles 0 1 2 3 4
Not at All Frequently, if not always <0> <1> <2> <3> <4>

Appendix E – Survey Instruments MANAGER QUESTIONNAIRE ID/MANAGER NAME: ____150
SECTION B: SELF-RATED LEADERSHIP QUESTIONNAIRE This next section is to describe your leadership style as you perceive it. Please answer all items on this answer sheet. If an item is irrelevant, or if you are unsure or do not know the answer, leave the answer blank. Forty-five descriptive statements are listed on the following pages. Judge how frequently each statement fits you. The word “others” may mean your peers, clients, direct reports, supervisors, and/or all of these individuals.
Use the following rating scale:
1. I provide others with assistance in exchange for their efforts 0 1 2 3 4
2. I re-examine critical assumptions to question whether they are appropriate 0 1 2 3 4
3. I fail to interfere until problems become serious 0 1 2 3 4
4. I focus attention on irregularities, mistakes, exceptions, and deviations from standards
0 1 2 3 4
5. I avoid getting involved when important issues arise 0 1 2 3 4
6. 0 1 2 3 4
7. 0 1 2 3 4
8. 0 1 2 3 4
9. 0 1 2 3 4
10. 0 1 2 3 4
11. 0 1 2 3 4
12. 0 1 2 3 4
13. 0 1 2 3 4
14. 0 1 2 3 4
15. 0 1 2 3 4
16. 0 1 2 3 4
17. 0 1 2 3 4
18. 0 1 2 3 4
19. 0 1 2 3 4
Not at all Once in awhile Sometimes Fairly Often Frequently, if not always
<0> <1> <2> <3> <4>

Appendix E – Survey Instruments MANAGER QUESTIONNAIRE ID/MANAGER NAME: ____151
20. 0 1 2 3 4
21. 0 1 2 3 4
22. 0 1 2 3 4
23. 0 1 2 3 4
24. 0 1 2 3 4
25. 0 1 2 3 4
26. 0 1 2 3 4
27. 0 1 2 3 4
28. 0 1 2 3 4
29. 0 1 2 3 4
30. 0 1 2 3 4
31. 0 1 2 3 4
32. 0 1 2 3 4
33. 0 1 2 3 4
34. 0 1 2 3 4
35. 0 1 2 3 4
36. 0 1 2 3 4
37. 0 1 2 3 4
38. 0 1 2 3 4
39. 0 1 2 3 4
40. 0 1 2 3 4
41. 0 1 2 3 4
42. 0 1 2 3 4
43. 0 1 2 3 4
44. 0 1 2 3 4
45. 0 1 2 3 4
Not at all Once in awhile Sometimes Fairly Often Frequently, if not always
<0> <1> <2> <3> <4>
Appendix E – Survey Instruments MANAGER QUESTIONNAIRE ID/MANAGER NAME: ____152
SECTION C: DEMOGRAPHICS
1) Age: __________________________________________
2) Gender □ male □female
3) What is your profession? □PT □OT □SLP □RN □RPN
□ Other ___________________________________
4) Highest Degree obtained? □Certificate □BSc □ Entry level masters
□Other ____________________________________
5) Year of Graduation __________________________________________
6) Years in present unit/job? __________________________________________
7) FTE Status/Number of Hours? __________________________________________
Thank you for your feedback on the Fracture Fighters implementation strategy. Finally, are there any
additional comments about barriers and facilitators to implementing the program that you would like
to mention?
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________

Appendix F: Standard score values 153
Multifactor Leadership Questionnaire (Form 5X) (Avoilo & Bass, 2004)
Organizational Readiness for Change Score Profile (TCU, 2004)