professor graham dickson (canada) and professor peter spurgeon (uk)
TRANSCRIPT

Partnering for performance to drive
reform
Professor Graham Dickson (Canada) and Professor Peter Spurgeon (UK)

To explore:
What partnering for performance means
What the research says re having medical leaders as partners in health reform: how does it affect performance?
The need for medical leaders to become engaged as partners in health reform
Purpose
Working together to get results...

What is Productive Health Reform?
Health reform is a transition from where we are at now to where we want to be that is defined within each country’s need as dictated by situation, circumstance and context.
Patient-centred care is the focal point for many jurisdictions.
It is multi-level: e.g., micro (unit, or consultancy-based), macro (hospital or organization-base) or mega (national/provincial) in scope.
Medical leadership is required at all levels for reform to be effective

The action or process of carrying out or accomplishing an action, task, or function
In the context of this session, the action, task or function is productive health reform.
Performance
A relationship that is characterized by mutual cooperation and responsibility, as for the achievement of a specified goal.
The state or condition of being a partner; participation; association; joint interest.
In Law. a. the relation subsisting between
partners. b. the contract creating this
relation. c. the persons joined together as
partners in business
Partnership
The mutual cooperation and sharing of responsibility between medical doctors and others (non-medical administrators, other professions, public) .
The term physician engagement is used to characterize the degree to which we are committed, and successful, in forming partnerships between medical doctors and others.
Partnership (cont.)

Enhancing Engagement in Medical Leadership: A Focus on Medical
Engagement
Professor Peter Spurgeon (Project Director)
Director, Institute of Cinical Leadership, Medical School,
University of Warwick
Enhancing Engagement in Medical Leadership
Joint project undertaken by National Institute for Innovation and Improvement, and Academy of Medical Royal Colleges
Overall goal ‘create a culture of greater medical engagement in management and leadership with all doctors at every level’
Two key products- Medical Leadership Competency Framework- Medical Engagement Scale
Project Benefits
Benefits to the NHS and medical professionals include: Greater commitment and capability to effect
service change and improvement Support the drive towards the new medical
professionalism Greater awareness by medical professionals of the
contribution of effective management and leadership both in operational and strategic activities
Increase and strengthen the pool of medical managers and leaders available to take on senior roles within the service

The Medical Leadership Competency Framework
www.institute.nhs.uk/mlcf

Defining the territory of leadership: the power of frameworks
Other ‘constructions’ of leadership
Canada: LEADSAustralia: RACMA
Medical Leadership Competency Framework
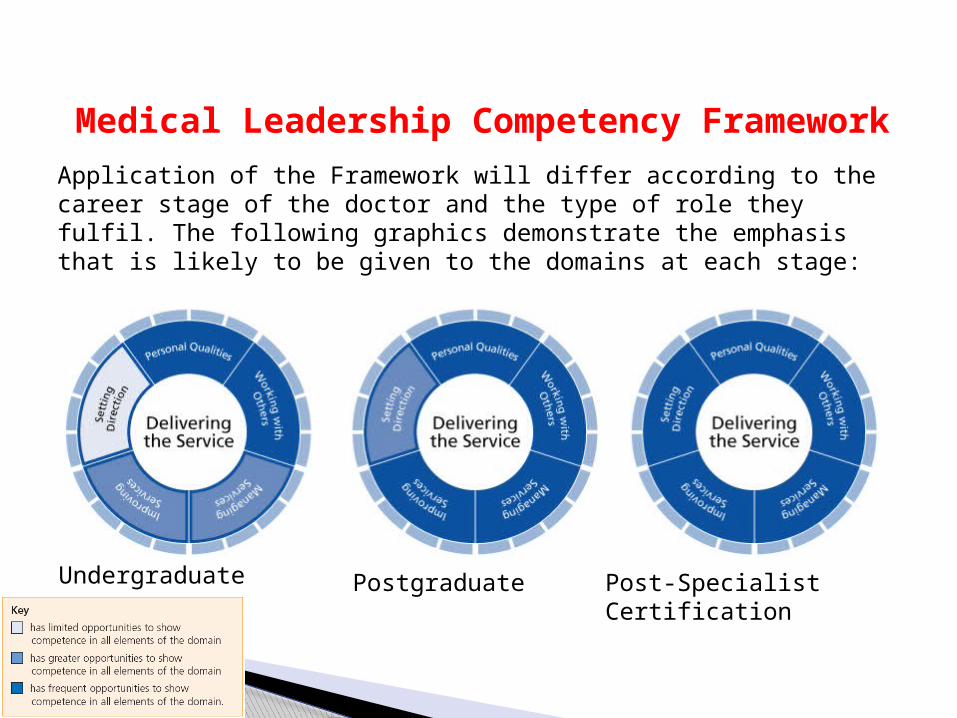
Application of the Framework will differ according to the career stage of the doctor and the type of role they fulfil. The following graphics demonstrate the emphasis that is likely to be given to the domains at each stage:
Undergraduate Post-Specialist CertificationPostgraduate

Medical Leadership Competency Framework
Working with OthersDoctors showing effective leadership by working with others in teams and networks to deliver and improve services.This requires doctors to demonstrate competence in:Developing networks: working in partnership with colleagues, patients, carers, service users and their representatives within and across systems and improve servicesBuilding and maintaining relationships: listening, supporting others, gaining trust and showing understandingEncouraging contribution: creating an environment where others have the opportunity to contributeWorking within teams: to deliver and improve services.
Medical Leadership Competency Framework
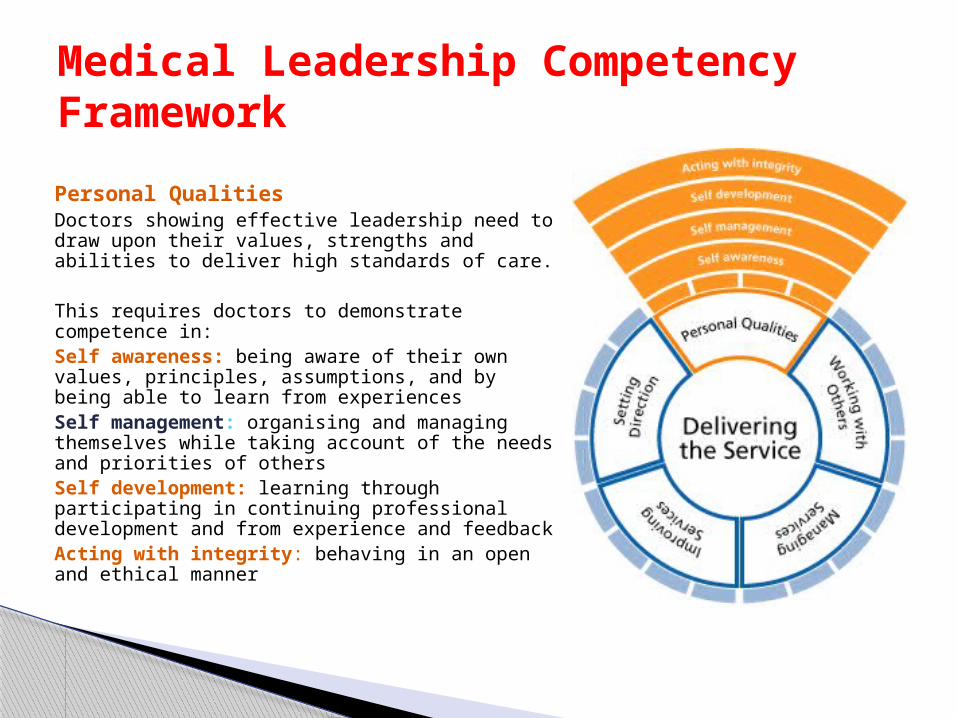
Personal QualitiesDoctors showing effective leadership need to draw upon their values, strengths and abilities to deliver high standards of care.
This requires doctors to demonstrate competence in:Self awareness: being aware of their own values, principles, assumptions, and by being able to learn from experiencesSelf management: organising and managing themselves while taking account of the needs and priorities of othersSelf development: learning through participating in continuing professional development and from experience and feedbackActing with integrity: behaving in an open and ethical manner

Medical Leadership Competency Framework
Managing ServicesDoctors showing effective leadership are focused on the success of the organisation(s) in which they work.Doctors are required to demonstrate competence in:Planning: actively contributing to plans to achieve service goalsManaging resources: knowing that resources are available and using their influence to ensure that resources are used efficiently and safelyManaging people: providing direction, reviewing performance and motivating othersManaging performance: holding themselves and others accountable for service outcomes

Improving ServicesDoctors showing effective leadership make a real difference to people’s health by delivering high quality services and by developing improvements to service.Ensuring patient safety: assessing and managing risk to patients associated with service improvement.Critically evaluating: being able to think analytically, conceptually and to identify where services can be improved.Encouraging innovation: creating a climate of continuous service improvement.Facilitating transformation: actively contributing to change processes that lead to improving healthcare.
Medical Leadership Competency Framework

Setting DirectionDoctors showing effective leadership contribute to the vision and aspirations of the organisation and act in a manner consistent with its values.Identifying the contexts for change: being aware of the range of factors to be taken into accountApplying knowledge and evidence: gathering information to produce an evidence-based challenge to systems and processes in order to identify opportunities for service improvementsMaking decisions: integrating values with evidence to inform decisionsEvaluating Impact: measuring and evaluating outcomes, taking corrective action where necessary and by being held to account for their decisions.
Medical Leadership Competency Framework

Leadership Framework(All staff Groups)

From Competence to Engagement
Competence may be thought of as “can do” but engagement requires “will do”- the motivational aspect.
Engaged employees characterised by- belief and pride in their organisation- commitment to improve the outcome/ product- understanding of the wider organisational context beyond their own job role- respect for colleagues- “willingness to go the extra mile”

Use of Term “Engagement”
Not - as process of consultation - as act “to do”
Rather - Intra individual notion- Reservoir of motivation- Willingness to get involved
UK wide levels of engagement, across sectors said to be relatively low.
Approx 1/3 workforces truly engaged
Hence any increase in the 1/3 increases organisation capacity, and therefore performance
So engagement is reciprocally beneficiala) Organisation- performance, customer
satisfaction, reduced absenteeism, turnoverb) Individual- improved job satisfaction, lowerburnout rate
Definition of engagement built into MES is therefore
“The active and positive contribution of doctors within their normal working roles to maintaining and enhancing the performance of the organisation which itself recognises this commitment in supporting and encouraging high quality care”
(Spurgeon, Barwell and Mazelan 2008)
From Competence to Engagement cont’d.

Origins of the Medical Engagement Scale (MES) Applied Research Ltd.- Established large database re:
attitudinal, individual & cultural aspects of NHS
Existing measure of work satisfaction and personal commitment based on 23,782 NHS staff and 20+ health organisations
Best items from previously established scales selected as relevant to medical engagement and re-analysed using Factor Analysis
Scales adapted to focus on engagement- reliable, valid & relatively easy to administer and complete

Overall items reduced to 30 with reliability scores (Cronbach’s alpha) ranging from 0.70 to 0.93
Inter-scale correlations with key core concepts of engagement suggest -
a) engagement is a conceptually distinct construct
b) the sub-scales are important as engagement is multidimensional
Scores from the pilot trust sites were statistically significant & in the predicted order i.e. top two are rated independently as excellent & have taken steps to promote medical engagement, the last is in the poorest performing category & the opportunistic site is in the middle
MES Reliability & Validity

Scales and Definitions
Scale Definition
[The scale is concerned with the extent to which…..]
Index: Medical Engagement ...doctors adopt a broad organisational perspective with respect to their clinical responsibilities and accountability
Meta Scale 1: Working in an Open Culture ...doctors have opportunities to authentically discuss issues and problems at work with all staff groups in an open and honest way
Meta Scale 2: Having Purpose and Direction ...Medical Staff share a sense of common purpose and agreed direction with others at work particularly with respect to planning, designing and delivering services
Meta Scale 3: Feeling Valued and Empowered ...doctors feel that their contribution is properly appreciated and valued by the organisation and not taken for granted
Sub Scale 1: [O] Climate for Positive Learning ...the working climate for doctors is supportive and in which problems are solved by sharing ideas and joint learning
Sub Scale 2: [I] Good Interpersonal Relationships ...all staff are friendly towards doctors and are sympathetic to their workload and work priorities.
Sub Scale 3: [O] Appraisal and Rewards Effectively Aligned ...doctors consider that their work is aligned to the wider organisational goals and mission
Sub Scale 4: [I] Participation in Decision-Making and Change ...doctors consider that they are able to make a positive impact through decision-making about future developments
Sub Scale 5: [O] Development Orientation ...doctors feel that they are encouraged to develop their skills and progress their career
Sub Scale 6: [I] Commitment & Work Satisfaction ...doctors feel satisfied with their working conditions and feel a real sense of attachment and reward from belonging to the organisation
MES Scale

MES Index: Position on Model for 4 Pilot Trusts
Trust C
Trust A Trust B
Trust D
Many Organisational Opportunities
Few Organisational Opportunities
Restricted Individual Capacities
Expanded Individual Capacities
Doctors feelENGAGED
Doctors feelCHALLENGED
Doctors feelFRUSTRATED
Doctors feelPOWERLESS

Meta-Scales: Position on Model for 4 Pilot Trusts
Trust A
Trust C
Trust B
Trust D
Many Organisational Opportunities
Few Organisational Opportunities
Restricted Individual Capacities
Doctors feelCHALLENGED
Doctors feelENGAGED
Doctors feelPOWERLESS
Doctors feelFRUSTRATED
Trust C
Trust A
Trust B
Trust D
Many Organisational Opportunities
Few Organisational Opportunities
Doctors feelCHALLENGED
Doctors feelENGAGED
Doctors feelPOWERLESS
Doctors feelFRUSTRATED
Trust C
Trust A
Trust B
Trust D
Many Organisational Opportunities
Few Organisational Opportunities
Expanded Individual Capacities
Doctors feelCHALLENGED
Doctors feelENGAGED
Doctors feelPOWERLESS
Doctors feelFRUSTRATED
Meta-Scale 1: Working in an open culture
Meta-Scale 2: Having Purpose & Direction
Meta-Scale 3: Feeling Valued & Empowered
16

The Levels of Medical Engagement
Embedded
Expanded
Energised
Expectant
Excluded
Doctors are fully involved at all levels in leading the design and delivery of service innovations
Doctors traditional roles have become expanded to embrace some aspects of managing healthcare
Doctors are keen to become more involved in the planning, design and delivery of services
Doctors understand the importance of becoming involved in the management agendaDoctors are not part of the management process and confine their activities to their traditional role
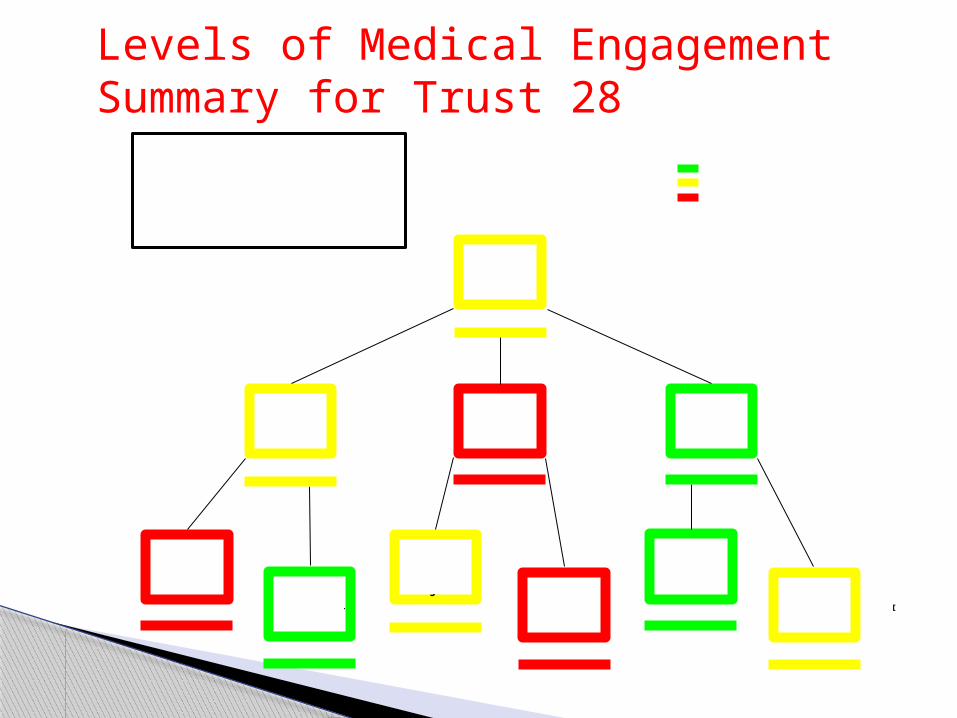
Levels of Medical Engagement Summary for Trust 28
Climate for Positive Learning
Good Interpersonal Relationships
Appraisal & Rewards
Effectively Aligned Participation
in DM & Change
Development Orientation
Commitment & Work
Satisfaction
Working in an Open &
Fair Culture
Having Purpose & Direction
Being Valued & Empowered
Professional Engagement
O
I
LOW
LOW
LOW
HIGH
HIGH
HIGH
MEDIUM
MEDIUM
MEDIUM
MEDIUM
Medical Engagement Scales:
Relative Normative Feedback Trust 28
KEY
High Relative Engagement (Top 1/3rd Trusts)
Medium Relative Engagement (Middle 1/3rd Trusts)
Low Relative Engagement (Bottom 1/3rd Trusts)

Levels of Medical Engagement for All Trusts in Current Sample
29
Engagement Meta Scale 1 Meta Scale 2 Meta Scale 3 Sub Scale 1 Sub Scale 2 Sub Scale 3 Sub Scale 4 Sub Scale 5 Sub Scale 6
Trust 1 6 10 4 7 4 23 7 3 11 7
Trust 2 15 24 13 11 23 21 20 8 12 10
Trust 3 26 23 26 26 20 22 26 23 26 25
Trust 4 22 20 22 14 22 14 23 12 16 13
Trust 5 4 4 5 4 6 5 5 6 5 4
Trust 6 11 5 17 19 7 4 14 21 13 19
Trust 7 12 9 18 15 13 6 13 25 9 23
Trust 8 27 26 28 28 26 26 29 26.5 28 28
Trust 9 19 22 10 23 15 27 10 10 27 17
Trust 10 7 6 6 10 5 12 15 1 22 6
Trust 11 10 11 9 13 8 15 8 11 19 9
Trust 12 2 2 3 1 2 1 3 5 1 2
Trust 13 14 15 16 12 19 10 11 26.5 8 18
Trust 14 9 7 8 8 10 9 6 13 6 12
Trust 15 3 3 2 3 3 8 2 4 4 3
Trust 16 8 8 11 6 9 11 16 7 10 5
Trust 17 20.5 14 23 17 11 20 22 20 17 16
Trust 18 29 29 29 29 29 25 28 29 29 27
Trust 19 18 17 20 16 18 13 25 9 21 11
Trust 20 30 30 30 30 30 30 30 28 30 30
Trust 21 1 1 1 2 1 2 1 2 3 1
Trust 22 23 25 19 20 25 24 18 19 14 21
Trust 23 24 21 25 24 22 16 24 24 24 22
Trust 24 5 12 7 5 12 7 4 17 2 8
Trust 25 20.5 16 15 21 16 17 19 16 23 20
Trust 26 28 28 27 27 28 28 27 22 25 29
Trust 27 16 13 14 22 14 18 12 15 18 24
Trust 28 17 18 24 9 27 3 17 30 7 14
Trust 29 25 27 21 25 24 29 21 18 15 26
Trust 30 13 19 12 18 17 19 9 14 20 15

Overall quality score
Financial management
score
Core standards score (as a provider of services)
Existing commitments score (as a provider of services)
National priorities
score (as a provider of services)
21 65.8 Good Excellent Fully Met Fully Met Good
12 65.2 Good Good Fully Met - Good
15 63.4 Excellent Good Fully Met Fully Met Excellent
5 62.0 Excellent Excellent Fully Met Fully Met Excellent
24 60.8 Good Excellent Fully Met - Good
1 60.4 Excellent Excellent Fully Met Fully Met Excellent
10 59.9 Good Excellent Almost Met Fully Met Good
16 59.8 Good Fair Fully Met Almost Met Excellent
14 59.7 Excellent Excellent Fully Met Fully Met Excellent
11 58.8 Excellent Excellent Fully Met Fully Met Excellent
25 56.8 Fair Fair Almost Met Fully Met Poor
4 56.7 Fair Fair Almost Met Fully Met Fair
22 55.7 Fair Fair Partly Met Almost Met Good
23 55.3 Fair Good Almost Met Partly Met Excellent
29 54.4 Good Excellent Fully Met Fully Met Good
3 54.3 Fair Excellent Fully Met Fully Met Poor
26 53.1 Fair Fair Almost Met Almost Met Fair
8 52.7 Good Good Fully Met Almost Met Good
18 52.1 Fair Fair Fully Met Partly Met Good
20 47.0 Poor Poor Almost Met Not Met Fair
CQC - NHS performance ratings 2008/09
Trust ID .
(Trust names withheld for
confidentiality)
Overall Medical
Engagement Scale Index
. (in descending
order)
The table below illustrates the quantitative data in more concrete terms by showing the difference in performance level achieved on Care Quality Commission ratings by those Trusts in the top 10 and bottom 10 on the MES.
CQC Ratings Against Top/Bottom MES Scores

CQC Ratings Against Top/Bottom MES Scores
Overall quality score
Financial management
score
Core standards score (as a provider of services)
Existing commitments score (as a provider of services)
National priorities
score (as a provider of services)
21 65.8 Good Excellent Fully Met Fully Met Good
12 65.2 Good Good Fully Met - Good
15 63.4 Excellent Good Fully Met Fully Met Excellent
5 62.0 Excellent Excellent Fully Met Fully Met Excellent
24 60.8 Good Excellent Fully Met - Good
1 60.4 Excellent Excellent Fully Met Fully Met Excellent
10 59.9 Good Excellent Almost Met Fully Met Good
16 59.8 Good Fair Fully Met Almost Met Excellent
14 59.7 Excellent Excellent Fully Met Fully Met Excellent
11 58.8 Excellent Excellent Fully Met Fully Met Excellent
25 56.8 Fair Fair Almost Met Fully Met Poor
4 56.7 Fair Fair Almost Met Fully Met Fair
22 55.7 Fair Fair Partly Met Almost Met Good
23 55.3 Fair Good Almost Met Partly Met Excellent
29 54.4 Good Excellent Fully Met Fully Met Good
3 54.3 Fair Excellent Fully Met Fully Met Poor
26 53.1 Fair Fair Almost Met Almost Met Fair
8 52.7 Good Good Fully Met Almost Met Good
18 52.1 Fair Fair Fully Met Partly Met Good
20 47.0 Poor Poor Almost Met Not Met Fair
CQC - NHS performance ratings 2008/09
Trust ID .
(Trust names w ithheld for
confidentiality)
Overall Medical
Engagement Scale Index
. (in descending
order)
Overall quality score
Financial management
score
Core standards score (as a provider of services)
Existing commitments score (as a provider of services)
National priorities
score (as a provider of services)
21 65.8 Good Excellent Fully Met Fully Met Good
12 65.2 Good Good Fully Met - Good
15 63.4 Excellent Good Fully Met Fully Met Excellent
5 62.0 Excellent Excellent Fully Met Fully Met Excellent
24 60.8 Good Excellent Fully Met - Good
1 60.4 Excellent Excellent Fully Met Fully Met Excellent
10 59.9 Good Excellent Almost Met Fully Met Good
16 59.8 Good Fair Fully Met Almost Met Excellent
14 59.7 Excellent Excellent Fully Met Fully Met Excellent
11 58.8 Excellent Excellent Fully Met Fully Met Excellent
25 56.8 Fair Fair Almost Met Fully Met Poor
4 56.7 Fair Fair Almost Met Fully Met Fair
22 55.7 Fair Fair Partly Met Almost Met Good
23 55.3 Fair Good Almost Met Partly Met Excellent
29 54.4 Good Excellent Fully Met Fully Met Good
3 54.3 Fair Excellent Fully Met Fully Met Poor
26 53.1 Fair Fair Almost Met Almost Met Fair
8 52.7 Good Good Fully Met Almost Met Good
18 52.1 Fair Fair Fully Met Partly Met Good
20 47.0 Poor Poor Almost Met Not Met Fair
CQC - NHS performance ratings 2008/09
Trust ID .
(Trust names w ithheld for
confidentiality)
Overall Medical
Engagement Scale Index
. (in descending
order)

MES Scales
Examples of CQC Indicators
Patient Survey Key Indicators
IPSurfConfDoc IPSurfInvDeci SINAP15 NHFD01
Index of Medical Engagement 0.67 0.59 Meta 1 - Working in a Collaborative Culture 0.60
0.62
Meta 2 - Having Purpose & Direction
0.55 Meta 3 - Being Valued and Empowered 0.69 0.57 0.58 Sub 1 - Climate for Positive Learning
0.59 0.55
Sub 2 - Good Interpersonal Relationships 0.66
0.66 Sub 3 - Appraisal and Rewards Effectively Aligned
0.64
Sub 4 - Participation in Decision-Making & Change
0.62 Sub 5 - Development Orientation 0.72 0.61
Sub 6 - Work Satisfaction 0.64 0.62
KEY: IPSurConfDoc = Inpatient Survey 2012 Q25 "Did you have confidence and trust in the doctors treating you?" IPSurInvDeci = Inpatient Survey 2012 Q32 "Were you involved as much as you wanted to be in decisions about your care and treatment?"
SINAP15 = Key Indicator 8: Number of potentially eligible patients thrombolysed NHFD01 = National Hip Fracture Database: measure of cases assessed as achieving compliance with all nine Best Practice Tariff standards of care
MES Scales
Application to PerformanceBenefits of Engagement (U.K.) Better patient mortality rates Fewer serious untoward accidents Better financial management Higher patient experience scores Better resource utilisation Achievement of service targets
USA hospitals with more engagement have better service performance and financial stability
Engagement has significant currency in private sector
“Engage for Success” national focus
U.K. levels of engagement quite low across all sectors

Medical Engagement and Organisational PerformanceWhat can we learn from trusts with high levels of medical engagement?
• Leadership, stable, relationship oriented, leading by example• A future-focused and outward-looking culture• Attention to selection and appointment of the right doctors to leadership
and management• Providing support, development and leadership opportunities• Effective communication• Promotion of understanding, trust and respect between doctors and
managers• Setting expectations, enforcing professional behaviour and firm decision-
making• Clarity of roles and responsibilities and empowerment

High Medium LowMedical Engagement Index
20.5% 9.8% 69.7%
Meta-Scale 1: Working in a Collaborative Culture
21.0% 18.3% 65.4%
Meta-Scale 2: Having Purpose and Direction
14.8% 10.0% 79.7%
Meta-Scale 3: Feeling Valued & Empowered
22.1% 8.3% 69.7%
Percentage of Respondents (n = 399) who fell into High, Medium and Low Normative Bands
Directions:◦ At your table, discuss what
health reform challenges—from a patient-centred focus-- you are facing in your own area of responsibility.
◦ To what extent are doctors truly engaged as it relates to health reform in your country?
◦ Would the MES engagement scale be useful to you in improving engagement?
Prepare to report out.
Activity
A&Q
