prof. dr. fiaban fiimflek - tıp...
TRANSCRIPT


Yaklafl›k 2 y›l önce yay›n hayat›na bafllayan Maltepe T›p Dergisi’nin yeni say›s›nda bulufltu¤umuz için mut-luyuz. Üniversitemizin ilk bilimsel dergisi olan Maltepe T›p Dergisi ile Fakültemiz, üniversitemizin akademik an-lamda da lokomotifi olmay› sürdürmektedir. Bu süre zarf›nda ülke çap›nda çok say›da meslektafl›m›z›n 100’ünüzerinde çok de¤erli çal›flmalar›n› yay›nlam›fl bulunmaktay›z. Bu bize heyecan ve güç verirken ayn› zamanda so-rumlulu¤umuzu da artt›rmaktad›r.
Dergimizi haz›rlarken güncel iletiflim araçlar›n› ve yüksek teknolojiyi kullanmaya özen gösteriyoruz. Son ikisay›m›zdaki makalelere üniversitemizin internet sitesinden PDF format›nda ulafl›labilmektedir. Bir sonraki say›-m›zda on-line makale gönderme ve de¤erlendirme sistemine geçmeyi böylece hem yazarlar›m›z›n hem de de-¤erli hocalar›m›z›n ifllerini kolaylaflt›rmay› hedeflemekteyiz.
Dergimizin ulusal yay›n sürecinde yer alan tüm araflt›rmac›lara ve yay›na bafllad›¤› ilk günden bu yana ha-z›rlanmas›nda eme¤i geçen tüm arkadafllar›ma teflekkür eder, bu özverili çal›flmalar›n›n önümüzdeki dönemdede devam etmesini dilerim.
DekanProf. Dr. fiaban fiimflek
Önsöz
T.C. Maltepe Üniversitesi T›p Fakültesi Dergisi, y›lda 3 kez yay›nlanan ve yay›nland›¤› tarihten (2009) itibaren hakemli dergidir.
ISSN 1308 - 8661
‹mtiyaz Sahibi Dr. Kemal KÖYMEN
Genel Yay›n Yönetmeni Dr. fiaban fi‹MfiEK
Editör ve Sorumlu Yaz› ‹flleri Müdürü Dr. Bülent ARMAN
Yürütme Kurulu Dr. Nesrin SARIMAN, Dr. Alpay ÖRK‹, Dr. Berna HAL‹LO⁄LU, Dr. Alper KARAO⁄LAN
Yay›n Kurulu Dr. Oya UYGUR BAYRAM‹ÇL‹, Dr. Öner ÇEL‹K, Dr. Rahmi ÇUBUK, Dr. Berna HAL‹LO⁄LU, Dr. Alper KARAO⁄LAN, Dr. Manuk MANUKYAN,Dr. Alpay ÖRK‹, Dr. Nesrin SARIMAN, Dr. Attila SAYGI, Dr. fievki fiAH‹N,Dr. Nuri TASALI, Dr. Orhan TÜRKEN
‹statistik Dan›flman Dr. Turhan fiALVA
Dr. Fehime B. AKSUNGARDr. Osman AKDEM‹RDr. Sedat ALTINDr. Nüvit ALTINKAYADr. Harun ARBATLIDr. Bülent ARMANDr. Oya Uygur BAYRAM‹ÇL‹Dr. H. Serpil BOZKURTDr. Levent ÇEL‹KDr. Nilgün ÇINARDr. Rahmi ÇUBUKDr. Bahad›r DA⁄DEV‹RENDr. Kadir DEM‹RDr. U¤ur DEVEC‹Dr. Gökmen ERCAN
Dr. Sinan EK‹C‹Dr. Aynur ERENDr. R›fk› EVRENKAYADr. Peykan GÖKALPDr. Hakan GÜNDEfiDr. Semih HALEZERO⁄LUDr. Berna HAL‹LO⁄LUDr. Canan HÜRDA⁄Dr. Ahmet ILGAZLIDr. Cem KALAYCIDr. Alper KARAO⁄LANDr. Kubilay KARfiIDA⁄Dr. Sibel KARfiIDA⁄Dr. fievket KAVUKÇUDr. Abud KEBUD‹
Dr. Öncel KOCADr. fieref KÖMÜRCÜDr. Bahire KÜÇÜKKAYADr. Ender LEVENTDr. Manuk MANUKYANDr. Ahmet M‹D‹Dr. Nil Molinas MANDELDr. ‹lker ÖKTEMDr. Alpay ÖRK‹Dr. Ümit ÖZEK‹C‹Dr. Melih ÖZELDr. Eflref ÖZERDr. Güler ÖZTÜRKDr. Esra SA⁄LAMDr. Nesrin SARIMAN
Dr. Attila SAYGIDr. Kamil SERDENGEÇT‹Dr. Gülbüz SEZG‹NDr. Orhun S‹NANO⁄LUDr. fievki fiAH‹NDr. Sad›k fiENCANDr. fiaban fi‹MfiEKDr. Selçuk fi‹MfiEKDr. Nuri TASALIDr. Günay TOSUNDr. Orhan TÜRKENDr. M. Yaflar TÜLBEKDr. Dilek YILMAZ
T›p Fakültesi Dergisi Dan›flma Kurulu
Bask› ve Cilt:Ege Bas›m Ege Plaza Esatpafla Mah., Ziyapafla Cad., No:4 Ataflehir / ‹STANBULTel: (0216) 472 84 01www.egebasim.com.tr
Tasar›m:ATT Bas›m Yay›n Reklam Org. ‹nfl. San. ve Tic. Ltd. fiti.Yal› Mah. Küçükyal› Cad. Ulusoy Apt. No: 44/3 Maltepe / ‹STANBULTel: (0216) 371 17 37 (pbx)Faks: (0216) 371 50 71www.attistanbul.com
Yaz›flma Adresi: T.C. Maltepe Üniversitesi T›p FakültesiFeyzullah Cad. No: 3934843 Maltepe / ‹STANBULTel: (0216) 444 06 20 Faks: (0216) 399 00 60
www.marmarahst.com - www.maltepe.edu.tr

‹çindekiler ContentsCilt:3 Say›:3 / Aral›k 2011
KL‹N‹K ÇALIfiMALARExtracorporeal shock wave lithotripsy treatment of renal and ureteral stones... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Böbrek ve üreter tafllar›n›n vücut d›fl› flok dalgalar› (ESWL) ile tedavisi Maltepe Üniversitesi Hastanesi deneyimiSinano¤lu et al.
Kad›n hastalarda negatif apendektomi ile jinekolojik patolojiler aras›ndaki iliflki. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10The relationship between negative appendectomy and gynecological pathologies in female patientsÇitgez ve Arkadafllar›
Timing of expulsion observed, pain and bleeding after mifepristone and misoprostol – induced abortion. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Mifepriston ve misoprostol ile indüklenen abortusta a¤r›n›n ve kanaman›n bafllama zaman› ve abortusun...Ilir Tasha et al.
Üçlü tedavi sonras› semptomlar› kaybolan ancak Helikobakter pilori pozitifli¤i devam eden... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16The need of medical therapy in asymptomatic, Helicobacter pylori positive antral...Manukyan ve Arkadafllar›
DENEYSEL ÇALIfiMAProksimal tubal oklüzyon iflleminin rat over histopatolojisi üzerine etkilerinin incelenmesi: Deneysel çal›flma . . . . . . . . . . . . . . . . . . . . . . . 19Examination of the histopathological effects of proximal tubal occlusion procedure on rat ovaries: An experimental studyÇelik ve Arkadafllar›
OLGU SUNUMUNazal polipozis ve sinüzitin efllik etti¤i nadir görülen intranazal aktinomikozis... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Unusual intranasal presentation of actinomycosis with nasal polyposis and sinusitisÇiftçi ve Arkadafllar›
Radikülopati ile prezente olan lumbar spinal kondroma: Olgu sunumu... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Lumbar spinal chondroma presented with radiculopathy: A case reportKarao¤lan ve Arkadafllar›
Gemifloxacin-associated fever, maculopapular rash and elevated liver enzymes: A case report... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31Gemifloksasin ile iliflkili atefl, makülopapüler döküntü ve karaci¤er enzimleri yüksekli¤i: Olgu sunumu...Sezgin ve Arkadafllar›
Rapid spontaneous resolution of traumatic acute subdural hematoma... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33Travmatik akut subdural hematomun h›zl› spontan rezolüsyonuY›ld›r›m ve Arkadafllar›
Favorable outcomes of pregnancy with use of sibutramine in a woman with polycystic... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36Polikistik over sendromu olan bir kad›nda sibutramin kullan›m› ile olumlu gebelik sonuçlar›: bir olgu sunumuSa¤lam ve Arkadafllar›
DERLEMEPrematürite ve çocukluk ça¤› psikiyatrik bozukluklar› . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39Prematurity and childhood psychiatric disordersKaraman ve Arkadafllar›

Böbrek ve üreter tafllar›n›n vücut d›fl› flokdalgalar› (ESWL) ile tedavisi Maltepe Üniversitesi Hastanesi deneyimi
Extracorporeal shock wave lithotripsytreatment of renal and ureteral stonesMaltepe University Hospital experience
Orhun Sinano¤lu MD / Maltepe University Department of Urology Istanbul/TURKEYSinan Ekici MD / Maltepe University Department of Urology Istanbul/TURKEY Naci Tatar MD / Maltepe University Department of Urology Istanbul/TURKEYGüven Turan MD / Maltepe University Department of Urology Istanbul/TURKEYAhmet Kelefl MD / Maltepe University Department of Urology Istanbul/TURKEY
ÖZETAmaç: Vücut d›fl› flok dalgalar› ile tafl tedavisi (ESWL)
ürolitiyazis tedavisinde kullan›lan invazif olmayan bir yön-temdir. Bu çal›flman›n amac› ürolitiyaziste kullan›lan ESWLtedavisinin sonuçlar›n› ve uygun endikasyonlar›n› ortayakoymakt›r.
Yöntem: Temmuz 2009-Temmuz 2011 aras›nda üri-ner sistemde soliter tafl nedeniyle ESWL tedavisine al›nan51 hasta çal›flmaya al›nd›. ESWL seanslar›n› takibeden 3 ayiçinde tafls›zl›k durumu ve komplikasyonlar gözlenip de¤er-lendirildi.
Bulgular: Ellibir hastan›n 38’i (% 74.5) erkek 13’ü ka-d›nd› (% 25.5). Hastalar›n yafllar› 20-73 aras› de¤iflmektey-di (ort. 41.7 y›l). K›rkdört hastada (% 86) üç ay sonundatafltan tam ar›nma gerçekleflti. Otuzüç böbrek ve 18 üretertafl›n›n s›ras›yla 29’unda (88 %) ve 13’ünde (72%) ar›nmasa¤land›. ESWL yap›lan 7 hastada baflar› sa¤lanamad›, Üre-terorenoskopik litotripsi ve perkütan nefrolitotomi gibi in-vazif giriflimler uyguland›.
Sonuç: ESWL özellikle ürolitiyazis tedavisinde son dere-ce etkin ve invazif olmayan bir tedavi yöntemidir. Bu çal›fl-mada böbrek ve üreter tafllar›nda baflar› flans› s›ras›yla %88ve %72 bulunmufltur. Ayr›ca tafl üriner sistemde ne kadardistalde ise baflar› flans› o kadar düflmektedir.
Anahtar kelimeler: vücut d›fl› flok dalgalar›, nefroliti-yazis
ABSTRACTObjective: Extracorporeal Shock Wave Lithotripsy
(ESWL) is an effective noninvasive method to treaturolithiasis. This study aims to evaluate the outcome and theappropriate indication of ESWL for urolithiasis.
Material and methods: The data of 51 patientsundergoing ESWL for the management of solitaryurolithiasis during a period of 2 years (July 2009-July 2011)were reviewed. Stone-free status and complications wereobserved and evaluated within a period of three monthsfollowing the last ESWL treatment session.
Results: Out of these 51 patients, 38 were male(74.5%) 13 were female (25.5%). Ages varied from 20 to73 (mean 41.7 years). Forty-four patients (86%) hadcomplete clearance of stone by the end of 3 months. Outof 33 renal and 18 ureteral stones 29 (88%) and 13(72%) were succesfuly cleared. ESWL was unsuccessful in7 patients that required adjunct invasive interventionincluding ureterorenoscopic lithotripsy and percutaneousnephrolithotomy.
Conclusions: ESWL is a highly effective noninvasivemodality in the management of urolithiasis. The successrates in this study for kidney and ureteral stones were foundto be 88% and 72% respectively. Furthermore the moredistal the stone’s position is, the less success ESWL has.
Key words: extracorporeal shock wave lithotripsy,nephrolithiasis
KL
‹N
‹K
Ç
AL
Ifi
MA
LA
R
INTRODUCTIONBefore Chaussy used extracorporeal shock wave
lithotripsy (ESWL) in 1980, invasive methods have beenused in the treatment of urinary stones (1). Since then,(ESWL) has been the treatment of choice for renal stonesof ≤ 2 cm maximal length located in the calices or the renalpelvis (2). Considering its high efficacy, low rate ofmorbidity and complication, 3rd generation lithotriptorsused in outpatient clinics became the major treatmentoption in urolithiasis. The higher trend to treat patientswith ESWL can also be explained with no requirement ofanesthesia. Although the definite time and criteria toevaluate stone-free status of a patient after ESWLtreatment remained controversial for many years, it is nowcertain that clearance of disintegrates by three months isnecessary to say that ESWL is succesful (3). Thedisintegration depends on stone volume (4), stonecomposition and localization, and type of lithotripter,applied shock wave number and energy (5). Clearance ofdisintegrates depends on their localization and is worse forthose in the lower calyces than for those in the middle orupper calyces.
In this study we report the early outcomes of 51patients treated with electrohydrolic Lithoshock ESWLdevice with fluoroscopic stone focusing.
MATERIALS AND METHODSThe data of 51 patients with diagnosis of urolithiasis
undergoing endoscopic shock wave lithotripsy betweenJuly 2009 and July 2011 were reviewed. The diagnosis ofurolithiasis was done either with Kidney Ureter Bladder film(KUB) plus ultrasound (US) or with computed tomography(CT). The calculi were focussed with C-Arm Fluoroscopy.Patients having pain, hydronephrosis due to stoneobstruction, and stone size 5 ≥ mm were treated withESWL. The patients with ureteropelvic junctionobstruction, renal failure and urinary obstruction wereexcluded. Asymptomatic patients with stone size < 5 mmand no obstruction were followed up for spontaneouspassage. If they are not stone-free during this period,ESWL or percutaneous nephrolithotomy for kidney stonesand ureterorenoscopic lithotripsy for ureteral stones werecarried out. Complete blood count, blood urea analysis,coagulation parameters were done before the procedure.
Double-J catheters were inserted to 9 patients (%17)before ESWL sessions.
Parenteral diclofenac or fentanyl was used in order toensure analgesia. Electrohydrolic (Ultralith) ESWL devicewith fluoroscopic C-arm focussing was used. One to 5ESWL sessions (mean 3) were performed. 500 to 3500shock waves (Mean 2567) were applied for each session.Shock wave intensity varied from 10 to 22 kv (mean 18 kv).On 10th, 30th and 90th days following the last ESWLsession, patients were checked with KUB films and/or
ultrasound, stone free status were defined with evidenceof disintegration and spontaneous passage ofdisintegrates.
RESULTSOf these 51 patients, 38 were male (74.5 %) 13 were
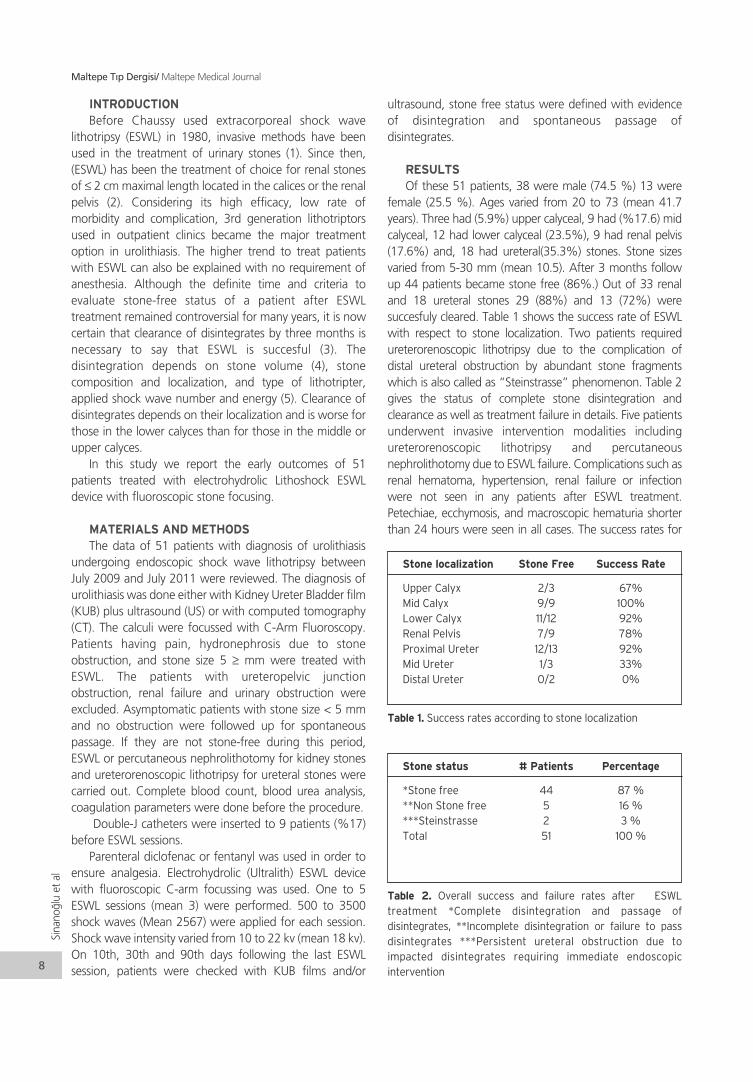
female (25.5 %). Ages varied from 20 to 73 (mean 41.7years). Three had (5.9%) upper calyceal, 9 had (%17.6) midcalyceal, 12 had lower calyceal (23.5%), 9 had renal pelvis(17.6%) and, 18 had ureteral(35.3%) stones. Stone sizesvaried from 5-30 mm (mean 10.5). After 3 months followup 44 patients became stone free (86%.) Out of 33 renaland 18 ureteral stones 29 (88%) and 13 (72%) weresuccesfuly cleared. Table 1 shows the success rate of ESWLwith respect to stone localization. Two patients requiredureterorenoscopic lithotripsy due to the complication ofdistal ureteral obstruction by abundant stone fragmentswhich is also called as “Steinstrasse” phenomenon. Table 2gives the status of complete stone disintegration andclearance as well as treatment failure in details. Five patientsunderwent invasive intervention modalities includingureterorenoscopic lithotripsy and percutaneousnephrolithotomy due to ESWL failure. Complications such asrenal hematoma, hypertension, renal failure or infectionwere not seen in any patients after ESWL treatment.Petechiae, ecchymosis, and macroscopic hematuria shorterthan 24 hours were seen in all cases. The success rates for
Sina
no¤l
uet
al
Maltepe T›p Dergisi/ Maltepe Medical Journal
8
Stone localization Stone Free Success Rate
Upper Calyx 2/3 67%Mid Calyx 9/9 100%Lower Calyx 11/12 92%Renal Pelvis 7/9 78%Proximal Ureter 12/13 92%Mid Ureter 1/3 33%Distal Ureter 0/2 0%
Stone status # Patients Percentage
*Stone free 44 87 %**Non Stone free 5 16 %***Steinstrasse 2 3 % Total 51 100 %
Table 1. Success rates according to stone localization
Table 2. Overall success and failure rates after ESWLtreatment *Complete disintegration and passage ofdisintegrates, **Incomplete disintegration or failure to passdisintegrates ***Persistent ureteral obstruction due toimpacted disintegrates requiring immediate endoscopicintervention

the kidney stones and ureteral stones were found to be88% and 68% respectively.
DISCUSSIONFollow-up, ESWL, ureterorenoscopic lithotripsy,
percutaneous lithotripsy and open surgery are thetreatment options for urolitihiasis. The management ofurolithiasis depends on the factors such as stone size,localization, presence of obstruction and renal function.Since its introduction in 1980, ESWL became the preferredtreatment option for the majority of renal calculi becauseof its non-invasive nature and low potential ofcomplications (6).
The overall success of ESWL in this study was 88 % and68 % for kidney and ureteral stones, respectively. Thesuccess rate of ESWL in proximal ureteral stones reportedto be 89-95.5 % in the literature and is in accordance withour findings. As to the mid ureteral stones, either ESWL orureterorenoscopic lithotripsy can be prefered. Althoughthe overall ESWL success for mid ureteral stones inprevious reports was about % 65, this rate was muchlower in our study. Furthermore, ESWL was unsuccesful inlower ureteral stones in contrast to previous reports (6).
The surprising fact is ESWL success rate in this study(%92) for lower calyceal stones was higher than thecumulative stone free rate of 41-73% for lower polestones in many reports (7). This high rate can be due tosome facts; First the stone burden in lower calyces was lowin our patients, second we recommended vibratorymassage in hand stand position as suggested a previousreport with stone-free rate of % 62.5 in patients withmassage and up side down position following ESWLsessions in contrast to 35.4 % stone free rate in patientswith ESWL alone (8). The stone-free rate for upper calycealstones is reported to be high in the literature, however thenumber of patients undergoing ESWL for upper calycealstones was very small in our series making the comparisonwith the results of these series impossible.
We evaluated the stone free status with KUB filmsand/or urinary ultrasound by 3 months. These imagingmodalities seem to have lower sensitivity and specifity indetection of small disintegrates and calculi. The questionhere is whether it is necessary to evaluate stone-free rateusing the more sensitive tools such as computedtomography with more radiation exposure, if theseclinically insignificant residual fragments (CIRF) have notherapeutic consequences. Some authors reported that78% of CIRF pass spontaneously, and only around 20% ofpatients with CIRF had recurrent stones requiringtreatment (9). It remains unclear whether these patientswould not have stone recurrences when they had beencompletely stone free. More aggressive and invasivetreatment of lower pole calculi with percutenousnephrolithotomy (PCNL) instead of ESWL is not justified if
the only advantage is a better clearance of CIRF, also itcannot be shown that PCNL has a significantly lower long-term recurrence rate due to fewer CIRF (10).
In conclusion, urolithiasis management with LithoshockESWL device was found to be effective. According to thelocation, the procedure seems more succesful in kidneystones than in ureteral stones, and not succesful in lowerureteral stones which requires mostly invasive endoscopicprocedures.
REFERENCES1. Chaussy C, Schmiedt E, Jocham D, Walter V, Brendel
W. First clinical experience with extracorporeallyinduced destruction of kidney stones by shock waves.J Urol. 1982;127:417-420.
2. Tiselius HG, Ackermann D, Alken P, Buck C, Conort P,Gallucci M. Guidelines on urolithiasis. In: Guidelinesof the EAU. European Association of Urology; 2001.
3. Zehnder P, Roth B, Birkhäuser F, Schneider S, SchmutzR, Thalmann GN et al. A prospective randomised trialcomparing the modified HM3 with the MODULITH®SLX-F2 lithotripter. (Eur Urol. 2011;59:637-644).
4. Albala DM, Assimos DG, Clayman RV, Denstedt JD,Grasso M, Gutierrez-Aceves et al. Lower pole I: aprospective randomized trial of extracorporeal shockwave lithotripsy and percutaneous nephrostolithoto-my for lower pole nephrolithiasis-initial results. J Urol2001;166:2072-2080.
5. Gerber R, Studer UE, Danuser H. Is newer alwaysbetter? A comparative study of 3 lithotriptorgenerations. J Urol 2005;173:2013-2016.
6. Gillanwater JY, Grayhack JT, Howards SS, Ducket JW.Extracorporeal shock wave lithotripsy for thetreatment of urinary calculi. Adult and PediatricUrology. 1996; 1: 913.
7. Danuser H, Muller R, Descoeudres B, Dobry E, StuderUE. Extracorporeal shock wave lithotripsy of lowercalyx calculi: how much is treatment outcomeinfluenced by the anatomy of the collecting system?Eur Urol 2007; 52: 539-546.
8. Chiong E, Hwee ST, Kay LM, Liang S, Kamaraj R,Esuvaranathan K. Randomized controlled study ofmechanical percussion, diuresis and inversion therapyto assist passage of lower pole renal calculi aftershock wave lithotripsy. Urology. 2005;65:1070-1074.
9. Osman MM, Alfano Y, Kamp S, Haecker A, Alken P,Michel MS, et al. 5-year-follow-up of patients withclinically insignificant residual fragments afterextracorporeal shockwave lithotripsy. Eur Urol2005;47:860-864.
10. Zanetti G, Seveso M, Montanari E, Guarneri A, DelNero A, Nespoli R et al. Renal stone fragmentsfollowing shock wave lithotripsy. J Urol 1997; 158:352-355.
Maltepe T›p Dergisi/ Maltepe Medical Journal
9
Cilt
:3Sa
y›:3
/ A
ral›k
201
1
ÖZETAmaç: Akut apandisit her yafl grubunda görülebilen,
eriflkinde akut kar›n hastal›klar›n›n yar›s›ndan fazlas›n› olufl-turan bir hastal›kt›r. Kad›n hastalarda jinekolojik patolojile-rin akut apandisiti taklit etmesi nedeniyle bu oran daha dayükselmektedir. Bu çal›flmada, akut apandisit ön tan›s›ylaameliyat edilen ve normal apendiks saptad›¤›m›z kad›nhastalarda tespit etti¤imiz jinekolojik patolojilerin tedaviyaklafl›mlar›n› ve oranlar›n› sunmay› amaçlad›k.
Yöntem: Ocak 2008 Ocak 2010 tarihleri aras›nda klini-¤imize baflvuran ve akut apandisit ön tan›s›yla opere edilen420 hasta retrospektif olarak incelendi. Hastalar›n tan›lar›fizik muayene, laboratuar bulgular ve radyolojik bulgularagöre konulmufltur. Hastalar›m›zda peroperatif apendiksindurumu ve jinekolojik patoloji makroskobik olarak de¤er-lendirilmifltir.
Bulgular: Hastalar›n 260’› (%61,9) erkek, 160’›(%38,1) kad›nd›. Tüm hastalar›n 28’inde (%6,6) ameliyatesnas›nda normal apendiks saptand›. Bu hastalar›n 19’u(%67) kad›nd›. Negatif apendektomi oran› kad›nlarda er-keklere göre istatistiksel olarak anlaml› bir flekilde dahayüksekti (p<0.01). Normal apendiks tespit edilen 19 kad›nhastan›n 9’unda (%47,4) baflka bir patoloji ile karfl›lafl›lma-m›flt›r. On olguda (%52,6) ise jinekolojik patoloji ile karfl›la-fl›lm›flt›r. Bu hastalar›n 4’ünde (%40) korpus hemorajikumkist rüptürü, 4’ünde (%40) pelvik inflamatuar hastal›k,1’sinde (%10) over kisti, 1’sinde (%10) over torsiyonu tes-pit edilmifltir.
Sonuç: Negatif apendektomilerin kad›n hastalarda is-tatistiksel olarak anlaml› biçimde yüksek olmas›, kar›n a¤r›-s› olan kad›n hastalar›n daha dikkatli de¤erlendirilmesini vejinekolojik patolojilerin de akut apandisiti taklit edebilece¤i-nin ak›lda tutulmas›n› gerektirir.
Anahtar kelimeler: akut apendektomi, apendiks, jine-kolojik patolojiler
ABSTRACTObjective: The rate of acute appendicitis is rather than
half of the acute abdominal pain and can be seen in all agegroups. It is more often in female patients because of thelook likes of gynecological pathologies with acuteappendicitis. In this study, we aimed to present the ratesand the treatment of gynecological pathologies in womenwho were operated with diagnosis of acute appendicitisbut having normal appendix.
Material and methods: Between January 2008 and2010, we retrospectively evaluated 420 patients who wereoperated with the preoperative diagnosis of acuteappendicitis. The patients were evaluated with physicalexamination, laboratory analysis and radiologicexaminations. The diagnosis of acute appendicitis andgynecological pathology were made during the operationby macroscopic examination.
Results: There were 260 (61.9%) male and 160(38.1%) female patients. There were normal appendices in28 (6.6%) patients peroperaitvely. In 28 negativeappendectomy cases there were 19 females (67%).Negative appendectomy rates were statistically morecommon in females than in males (p<0.01). Of the 19females with negative appendectomies 9 (47.4%) had noother pathologies and 10 (52.6%) had gynecologicalpathologies. The gynecological pathologies were corpushemorrhagicum cyst rupture in 4 (40%), pelvicinflammatory disease in 4 (40%), ovarian cyst in 1 (10%)and, ovarian torsion in 1 (10%) cases.
Conclusions: Negative appendectomy rates weremore common in females. As a result, physicans must bemore careful in female patients with abdominal pain, weshould remember that gyncological pathologies can bepresented as acute appendicitis clinics.
Key words: acute appendectomy, appendix, gynecol-ogical pathologies
Kad›n hastalarda negatif apendektomi ilejinekolojik patolojiler aras›ndaki iliflkiThe relationship between negative appendectomyand gynecological pathologies in female patientsDr. Bülent Çitgez / fiiflli Etfal E¤itim ve Araflt›rma Hastanesi, II. Genel Cerrahi Klini¤iDr. Gürkan Yetkin / fiiflli Etfal E¤itim ve Araflt›rma Hastanesi, II. Genel Cerrahi Klini¤iDr. ‹smail Akgün / fiiflli Etfal E¤itim ve Araflt›rma Hastanesi, II. Genel Cerrahi Klini¤iDr. Mehmet Uluda¤ / fiiflli Etfal E¤itim ve Araflt›rma Hastanesi, II. Genel Cerrahi Klini¤iDr. Mehmet Velidedeo¤lu / fiiflli Etfal E¤itim ve Araflt›rma Hastanesi, II. Genel Cerrahi Klini¤iDr. Adem Akçakaya / fiiflli Etfal E¤itim ve Araflt›rma Hastanesi, II. Genel Cerrahi Klini¤i

G‹R‹fiAkut apandisit her yafl grubunda görülebilen, eriflkinde
akut kar›n hastal›klar›n›n yar›s›ndan fazlas›n›n nedeninioluflturan bir hastal›kt›r (1). Tüm özellikleri ve cerrahi teda-visi bilinmesine ra¤men, apandisit hala en yüksek yanl›fl ta-n› oran›na sahip acil cerrahi durumdur (1,2).
Geliflen teknoloji ve artan tan› yöntemleriyle berabernegatif appendektomide (NA) azalma olmas›na ra¤men,akut apandisit tan›s›na yönelik zorluklar devam etmektedirve NA’lar halen büyük bir sorun oluflturmaktad›r (3,4). NA,kad›n hastalarda jinekolojik patolojilerin akut apandisititaklit etmesi nedeniyle daha s›k görülmektedir (4).
Bu çal›flmada akut apandisit ön tan›s›yla laparotomi uy-gulay›p, jinekolojik patoloji ile karfl›laflt›¤›m›z hastalar›, pa-tolojileri ve tedavi yaklafl›mlar›n› sunmay› amaçlad›k.
GEREÇ VE YÖNTEMLEROcak 2008-Ocak 2010 tarihleri aras›nda klini¤imize bafl-
vuran ve akut apandisit ön tan›s›yla opere edilen 420 hastaretrospektif olarak incelendi. Akut apandisit tan›s› fizik mu-ayene, laboratuvar ve radyolojik bulgulara göre konul-mufltur. Kad›n hastalar›m›zda ultrasonografik görüntüleme-nin yan›nda kad›n hastal›klar› konsültasyonu istenmifltir.Hastalar›m›zda jinekolojik patoloji ve peroperatif apendiksindurumu makroskobik olarak de¤erlendirilmifltir. Bulgular is-tatistiksel olarak ki-kare testi ile de¤erlendirilmifltir.
BULGULARHastalar›n 260’› (%61,9) erkek, 160’› (%38,1) kad›nd›.
Tüm hastalar›n 28’inde (%6,6) operasyon esnas›nda nor-mal apendiks ile karfl›lafl›lm›flt›r. Negatif apendektomi sap-tanan 28 hastan›n 19’u (%67) kad›nd›. Negatif apendek-tomiler kad›nlarda erkeklere göre istatistiksel olarak anlam-l› bir flekilde daha s›k gözlendi (p<0.01). Normal apendikstespit edilen 28 hastan›n 18’inde (%64,2) baflka bir pato-loji ile karfl›lafl›lmam›flt›r. On olguda (%35,8) ise jinekolojikpatoloji ile karfl›lafl›lm›flt›r. Bu hastalar›n 4’ünde (%40) kor-pus hemorajikum kist rüptürü, 4’ünde (%40) pelvik infla-matuar hastal›k, 1’inde (%10) over kisti, 1’inde (%10) overtorsiyonu tespit edilmifltir (Tablo 1). Korpus hemorajikumkist rüptürü tespit edilen hastalara kist eksizyonu, kanamakontrolü, over kist rüptürü tespit edilen hastaya kist eksizyo-nu, PID tespit edilen 4 hastaya drenaj ve antibiyoterapi, overtorsiyonu tespit edilen hastaya ooferektomi uygulanm›flt›r.
TARTIfiMAAkut apandisiti taklit edip NA’ya sebep olacak hastal›k-
lar›, jinekolojik nedenler ve jinekoloji d›fl› nedenler olarak ikiana bafll›k alt›nda inceleyebiliriz. Jinekolojik nedenler; ekto-pik gebelik, abortus, over torsiyonu, kist rüptürü, miyomdejenerasyonu, pelvik inflamatuar hastal›kken jinekoloji d›-fl› nedenler; kolelitiazis ve kolesistit, akut pankreatit, peptikülserdir (5). Jinekolojik d›fl› nedenler erkek hastalarda darastlan›labilen cerrahinin içinde oldu¤u hastal›klard›r. Unu-tulmamal›d›r ki, cerrahlar, akut apandisit ön tan›s›yla lapa-rotomi uygulad›klar› hastalarda jinekoljik hastal›klarla karfl›-laflabilirler (5,6). Klini¤imiz bir e¤itim ve araflt›rma hastane-sinde bulundu¤u için jinekolojik patoloji saptanan tüm ol-gularda peroperatif konsultasyon istenmekte ve gereklimüdahale kad›n hastal›klar› ve do¤um uzmanlar› taraf›n-dan yap›lmaktad›r. Korpus hemorajikum kist rüptürü tespitedilen hastalara kist eksizyonu ve kanama kontrolü yap›l›r-ken, over kist rüptürü tespit edilen hastaya kist eksizyonu,PID tespit edilen 4 hastaya drenaj ve antibiyoterapi, over tor-siyonu tespit edilen hastaya ise ooferektomi uygulanm›flt›r.
Literatürler incelendi¤inde NA kad›nlarda istatistikselolarak anlaml› bir flekilde daha s›k görülür (4-8). Bunun ne-deni olarak apendiksin reprodükif dönemdeki kad›nlardaüreme organlar›na olan yak›nl›¤› ve over kisti, PID gibi has-tal›klar›n klinik olarak akut apandisit gibi bulgu vermesi ola-rak belirtilmifltir (8). Normal apandisit ile karfl›lafl›lan kad›nhastalardaki jinekolojik patolojilerle ilgili Seetahal ve arka-dafllar›n›n yapt›klar› çal›flmada 18 ve 45 yafl aras›ndaki23655 NA yap›lm›fl kad›n hastan›n 3879’unda (%16,4) sa¤alt kadran a¤r›s›, 2176’s›nda (%9,2) over kist rüptürü,1608’inde (%6,8) endometriozis patolojileri ile karfl›lafl›l-m›flt›r (4). Nakhgevery ve ark. (9); yapt›klar› çal›flmada ise108 kad›n hastan›n 52’sinde (%48) NA yap›lm›fl, bu hasta-lar›n 23’ünde (%44) normal apendiks, 20’sinde (%38) pel-vik inflamatuar hastal›k, 9’unda (%18) over patolojileri ilekarfl›lafl›lm›flt›r. Çal›flmam›zda ise literatürle benzer flekilde19 NA yap›lan kad›n hastan›n 10’unda jinekolojik patolojisaptanm›fl ve en s›k olarak 4 hastada (%40) PID ve alt kad-ranlarda a¤r›, 4 hastada (%40) hemorajik kist rüptürünerastlanm›flt›r.
Hastan›n anamnezi ve fizik muayene bulgular› akutapandisit tan›s›nda hala en önemli rolü oynamakla beraberNA oranlar›n› azaltmak için görüntüleme yöntemleri, kananalizleri, akut faz reaktanlar› çeflitli klinik skorlama ve tan›-sal modaliteler gelifltirilmifltir (10,11). Olgular›n ço¤undakar›n ultrasonografisi (USG) yard›mc› teknik olarak kullan›l-maktad›r (10-13). Çeflitli yay›nlara göre, akut apandisit ta-n›s›nda kar›n USG’si duyarl›l›k %65-90, özgüllük %90- 100aras›nda, yeterlilik %89-95, pozitif prediktif de¤er %80-89ve negatif prediktif de¤er %76-92 oran›nda de¤ifliklik gös-termektedir (11-13). USG ile apandisitin görülmemifl olma-s› hastan›n apandisit olmayaca¤› anlam›na gelmez ve akutapandisit tan›s›n› d›fllamaz (10). Bizim çal›flmam›zdaki 10NA olgusunda da USG yap›l›p akut apandisitle uyumlu gö-
Cilt
:3Sa
y›:3
/ A
ral›k
201
1
Maltepe T›p Dergisi/ Maltepe Medical Journal
11
Tan›
Hemorajik kist rüptürü % 40
Over kisti % 10
Pelvik inflamatuar hastal›k % 40
Over torsiyonu % 10
Tablo 1. Negatif appendektomili kad›n hastalarda saptad›¤›m›zjinekoljik patolojilerin oranlar›

rüntü saptanmas›na ra¤men operasyon esnas›nda hastalar-da jinekolojik patoloji saptanm›flt›r.
NA oranlar› %11 ile %18 aras›nda de¤iflmektedir (4,8).Geçmifl y›llarda yüksek orandaki NA sonuçlar›, apandisitinperfore olmas›na engel oldu¤u düflünüldü¤ü için kabul edi-lebilir görülüyordu (2,4,8). Bununla birlikte NA, uzun yat›flsüreleri, yüksek enfeksiyon riski ile morbididite ve mortali-teyi artt›rmaktad›r (2). Buna paralel olarak Seetahal ve ark.(4); 1998 ile 2007 aral›¤›nda 475651 apendektomiyi ince-ledikleri derlemede 1998 y›l›nda NA insidans› 5514(%14,7) iken, 2007 y›l›nda 4346 (%8,4) olarak tespit edil-mifltir. Ayn› çal›flmada NA oran›n›n kad›n hastalarda istatis-tiksel olarak daha s›k oldu¤u saptanm›flt›r. Bizim çal›flma-m›zda NA 28 (%6,6) hastaya uygulanm›fl ve bayanlarda is-tatistiksel olarak daha fazla bulunmufltur. Biz NA say›m›z›ndüflüklü¤ünü akut apandisit düflünülen her hastaya bat›nultrasonografisi ve kad›n hastalarda operasyon öncesi ka-d›n do¤um konsültasyonu istememize ba¤lamaktay›z.
Tan› yöntemlerindeki geliflmeye ra¤men negatif apen-dektomi oranlar› kad›nlarda yüksek seyretmektedir. Nega-tif apendektomiyi önlemek için özellikle kad›n hastalar da-ha dikkatli de¤erlendirilmeli ve jinekolojik patolojilerin deakut apandisiti taklit edebilece¤i ak›lda tutulmal›d›r. Bu du-rumun göz önünde bulundurulmas› ve flüpheli olgularda ji-nekolojik patolojilere yönelik tetkik yap›lmas› kad›nlardaNA oranlar›n›n azalt›lmas›nda etkili olaca¤›n› düflündür-mektedir.
KAYNAKLAR1. Lally KP, Cox CS, Andrassy RJ. Appendix. In: Town-
send CM (ed). Sabiston. Textbook Of Surgery. 16 thedition. Philadelphia: WB. Saunders; 2001. 916-927.
2. Flum DR, Koepsell T. The clinical and economic core-lates of misdiagnosed appendicitis: nationwide analy-sis. Arch surg 2002; 137:799-804.
3. Blomqvist PG, Andersson RE, Granath F, Lambe MP,
Ekbom AR. Mortality after appendectomy in Sweden,1987-1996. Ann Surg 2001; 233:455-460.
4. Seetahal SA, Bolorunduro OB, Sookdeo TC, Negativeappendectomy: a 10-year review of a nationally rep-resentative sample. Am J.Surg 2011; 201: 433-437.
5. Bilgin N. Akut apandisit. In: Sayek ‹ (ed). Temel Cerra-hi. 3.bask›. Ankara: Günefl Kitapevi; 2004. 1191-1196.
6. Piper HG, Rusnak C, Orrom W, et al. Current mana-gement of appendicitis at a community center—howcan we improve? Am J Surg 2008;195:585–588.
7. Velanovich V, Satava R. Balancing the normal appen-dectomy rate with the perforated appendicitis rate:implications for quality assurance. Am Surg1992;58:264 –269.
8. Ma KW, Chia NH, Yeung HW, Cheung MT. If not ap-pendicitis, then what else can it be? A retrospectivereview of 1492 appendectomies. Hong Kong Med J.2010;16:12-17.
9. Nakgevery KB, Clarke LE. Acute appendicits in wo-men of childbearing age. Arch Surg 1986. 121: 1053-1055.
10. Gökçe AH, Aren A, Gökçe FS ve ark. Akut apandisit-te ultrasonografinin güvenilirli¤i Ulus Travma Acil Cer-rahi Derg 2011;17:19-22.
11. Sitter H, Hoffmann S, Hassan I, Zielke A. Diagnosticscore in appendicitis. Validation of a diagnostic score(Eskelinen score) in patients in whom acute appendi-citis is suspected.Langenbecks Arch Surg2004;389:213-218.
12. Saidi HS, Chavda SK. Use of a modified Alvorado sco-re in the diagnosis of acute appendicitis. East Afr MedJ 2003;80:411-414.
13. Turan A, Kapan S, Kütükçü E, Yi¤itbafl E, Hatipo¤lu S,Aygün E. Comparison of operative and non operativemanagment of acut appendicitis. Ulusal Travma AcilCerrahi Derg 2009;15:459-462.
Çitg
ezve
Ark
adafl
lar›
Maltepe T›p Dergisi/ Maltepe Medical Journal
12

ÖZETBu çal›flman›n amac› oral, düflük doz 200 mg Mifepris-
tone ve oral 400 mcg Misoprostol ile tedavi edilen hasta-larda a¤r›n›n tam olarak bafllama zaman›, düflü¤ün meyda-na geldi¤i zaman› ve kanama miktar› hakk›nda bilgilerigüncellemektir.
Ekibimiz, 56.güne kadar olan gebeliklerde oral mifes-priston’dan 48 saat sonra misoprostol alan hastalardakramplar, düflük zaman› ve kanaman›n bafllang›ç zaman›n›analiz etti.
Hastalar›n semptom günlüklerinden bilgileri ald›k vesemptom bafllang›c›n› 3 kategoriye ay›rd›k: misoprostolkullan›m›ndan önce, misoprostol kullan›m›ndan 24 saatsonra, ve misoprostol kullan›m›ndan 48 saat sonra.
200 hastadan 175’inde (%87,5) kramplar, gözlenendüflük ve kanama bafllang›ç zaman› ile ilgili bilgiler al›nabil-di, ancak 175 hastadan 30’u (%17,1) embriyoyu tan›ya-mad›klar›ndan çal›flma d›fl› b›rak›ld›lar.
Bütün gruplarda, 6 hasta (%4,13) gebelik materyalinigördü, s›ras›yla 37 (%25,5) ve 49 (%33,7) hastan›n misop-rostol öncesi kanama ve kramp tarz›nda a¤r›s› oldu.
Tedavi gruplar› aras›nda erken kramplar ve kanamas›olan hastalar›n oran› anlaml› olarak yüksek bulundu ve budurum mifepriston ile misoprostol aras›ndaki interval ileba¤lant›l› idi.
Kramplar ve kanama misoprostol kullan›m›ndan 48 sa-at sonra belirgin olarak s›rayla 8 (%5,5) ve 10 (%6,89) has-tada azald›.
Düflük materyalinin görülmesi, kanama, kramplar, mi-soprostol kullan›m›ndan 24 saat sonra en yüksek orandagörüldü.
Anahtar kelimeler: mifepriston, misoprostol, abortus
ABSTRACTThe objectives of this study were to date exactly the
time of onset of pain, expulsion, and bleeding in subjectstreated with low – dose 200 mg Mifepristone orally and400 mcg Misoprostol by mouth as well.
Our team did analysis the cramping, expulsionobserved and bleeding onset patterns in subjects till to 56days pregnant who used misoprostol at 48 hours aftermifepristone orally.
We collected data from patient’s symptom diaries, andwe divided symptom onset into 3 categories: beforemisoprostole use, 24 hours following misoprostol, and 48hours after misoprostol.
Of the 200 patients, cramping, expulsion observed,and bleeding onset data were available for 175 (87.5 %),but 30 of 175 subjects (17.1 %) were not able to identifytheir embryo, so we excluded from the study.
Across all groups, 6 patients (4.13 %) observed theirproduct of pregnancy, 37 (25.5 %) and 49 (33.7 %)experienced respectively bleeding and cramping beforemisoprostol use.
There were a significantly higher percentage ofsubjects who experienced early cramping and bleedingbetween three treatment groups, and this was related tothe interval between mifepristone and misoprostol.
This percentage was significantly reduced in subjectswho experienced cramping and bleeding 48 hours aftermisoprostol use respectively 8 (5.5 %) and 10 ( 6.89 %).
The incidence of expulsion observed, bleeding,cramping was highest 24 hours after misoprostol use.
Key words: mifepristone, misoprostol, abortion
Timing of expulsion observed, painand bleeding after mifepristone andmisoprostol – induced abortionMifepriston ve misoprostol ile indüklenen abortusta a¤r›n›n ve kanaman›n bafllama zaman›ve abortusun oluflma süresi aras›ndaki iliflki
Ilir Tasha MD. / Obstetric – Gynaecology Albanian Association. Obstetric - Gynaecology University Hospital. Tirana. Albania. Nikita Manoku MD. Proffessor / Obstetric – Gynaecology Albanian Association. Obstetric - Gynaecology University Hospital. Tirana. Albania. Donika Beba MD. / Obstetric – Gynaecology Albanian Association. Obstetric - Gynaecology University Hospital. Tirana. Albania.

INTRODUCTIONIt was essential to let you know that this study applied for
the first time in our hospital and in our country as well. For thefirst time, women in our country seeking abortion have hadthe option of either a surgical or medical abortion. In addition,we familiarized with idea that many women prefer medicalabortion as it allow them greater privacy and control overtheir abortion. Since 1992 women in Albania have had thelegal right to an abortion. The laws related to abortion werefurther liberalized in 1995 with the passage of the “Law onInterruption of Pregnancy”, which permits abortion up to 12weeks from the presumed date of conception. After thelegalization of abortion in 1992, abortion ratios increaseddramatically between 1992 and 1997 with over 40 abortionfor every 100 live births.(1) However, as family planning hasbecome more available, abortion ratios have decreased inrecent years. Recent estimates range from a ratio of 7.3abortion to 17.2 abortions per 100 live births. (2) In Albania,abortion must be performed by a physician, in either a publicor private health institution (2,3).
Mifepristone, a synthetic progesterone, is used tocompetitively block the effects of progesterone and weakenthe attachment of an early pregnancy on the endometrium.Mifepristone serum levels do not increase proportionally withincreasing oral doses(4,5). Misoprostol, a syntheticprostaglandin, is used 48 hours after mifepristone to inducecervical softening and dilatation, and uterine contractions toassist in the expulsion of the pregnancy (5). The efficacy of thereduced dose has been demonstrated in research by theWorld Health Organisation and in clinical studies in the USA(5,7).
MATERIALS AND METHODSThe study was performed from February 2006 – May
2008 in Obstetric – Gynaecology University Hospital of Tirana, Albania. Our hospital regularly provides abortion serviceusing dilatation and curettage under local anesthesia and isamong the largest abortion provider in Albania. Womenmade two clinic visits ore more. At the first visit, they received200 mg mifepristone and were asked to select clinic or homeadministration of misoprostol.
All subjects more than 18 years old who desiredpregnancy termination, enrolled in our clinic.
Inclusion and exclusion criteria for eligibility in medicalabortion was demonstrated in Table 1.
Eligibility and method selection:If all of the answers to Questions 1 to 16 appear in bold
sections, the woman is eligible for medical abortion (6).
If the woman choose to participate in the study and hassigned the consent form, administered mifepristone
At the initial visit (study day 1), a clinician confirmedgestational age by transabdominal ultrasound.
After the patient signed an informed consent, theyswallowed a single pill of 200 mg mifepristone under directobservation, and study personnel recorded the time. Subjectswere then randomly assigned to self – administered 400 mcgp/os misoprostol at about 48 hours after receivingmifepristone. All subjects were given the option of returningto the clinic for misoprostol swallowing.
Subjects received a symptom diary to record the date andtime of misoprostol use as well as the onset of cramping,expulsion observed and bleeding. All subjects were requiredto return for a follow – up visit at the end of fortnight. At thefollow – up visit, a clinician determined treatment success bypelvic exam or transabdominal ultrasound. The clinician alsocollected symptom diary at this time, and usually confirmedthe times of medication use and the times of symptomsonset. For each subject, we calculated the intervals betweenmifepristone & misoprostol swallowing and the onset ofsymptoms.
We excluded subjects who did not return to their follow– up appointments (subjects lost to follow – up). We alsoexcluded subjects for whom timing intervals could not becomputed due to irresolvable data entry errors and all thissubjects who were not able to identify the embryo. Wedivided timing of symptom (pain, expulsion observed, andbleeding) onset into three categories : before misoprostolswallowing, 24 hours and 48 hours after receiving ofmisoprostol.
Outcome measures included time between mifepristoneand misoprostole use and the onset of symptoms; time of 24hours from receiving of misoprostol to the onset of symp-toms; time of 48 hours from receiving of misoprostol to theonset of symptoms.
Data are drawn from a prospective study of 200 womenwho presented for an abortion with amenorrhea of ≤ 56 days.
RESULTSThis analysis included 200 women who enrolled from
February 2006 – May 2008. In related to symptoms we followed at the same time 145
subjects for; bleeding, cramping and expulsion observed inthree points of the time: before misoprostol use, 24 hoursafter misoprostol use, 48 hours after misoprostol use.
In related to the expulsion observed 6 (4.13 %) of thesubjects noticed their embryo before misoprostol use; 24(16.55 %) of the subjects noticed their conceptus 24 hoursafter receiving the misoprostol; 38 (26.2 %).
Timing of onset of cramping is scheduled as below:49 subjects (33.7 %) experienced onset of pain before
misoprostol use.24 subjects (16.55 %) did experience onset of pain , 24
hours after misoprostol use.8 subjects (5.5%) experienced onset of pain , 48 hours
after receiving misoprostol.
Ilir
Tash
a et
al
Maltepe T›p Dergisi/ Maltepe Medical Journal
14

Timing of onset of bleeding:37 (25.5%) subjects experienced onset of bleeding before
misoprostol use.49 (33.7%) subjects experienced the first bleeding 24
hours after receiving misoprostol.10 (6.89 %) subjects experienced onset of bleeding 48
hours after misoprostol use.There was not a small number of patients that ended their
abortion using only mifepristone. This result was confirmedby our colleagues in China, Tunisia(8).
Across all groups 6 patients (4.13%) observed theirconcepts, 37 (25.5%) and 49 (33.7%) experiencedrespectively bleeding and cramping before misoprostol use.
There was a significantly higher percentage of subjectswho experienced early cramping and bleeding between threetreatment groups, and this was related to the intervalbetween mifepristone and misoprostol.
This percentage was significantly reduced in subjects whoexperienced cramping and bleeding 48 hours aftermisoprostol use respectively 8 (5.5 %) and 10 (6.89 %).
The incidence of expulsion observed, bleeding and,cramping was highest 24 hours after misoprostol use.
DISCUSSIONThis analysis provides information about the timing of
cramps, bleeding and expulsion observed relative tomisoprostol use during medical abortion. The study resultsshowed a high rate of success and high level of satisfactionwith this method.
This study had several limitations.Subject’s self – report of symptoms may have resulted in
recording errors of digit – preference recording. Applicationof 200 mg mifepristone in medical abortion confirmed onemore time that mifepristone serum levels do not increase
proportionally with increasing of oral doses. Providers andpatients may find such information useful if patients could notavoid following up.
REFERENCES1. Nuri, B. In: Trageakes, E. ed. Health Care Systems in
Transition: Albania Copenhagen: European Observatoryon Health Care Systems, 2002;4:60.
2. Herold J, Seither R, Ylli A et al. Reproductive HealthSurvey, Albania 2002: Preliminary Report, Atlanta,GA,USA. Centre for Disease Control, 2003.
3. World Health Organization. Task Force on Postovulatorymethods of Fertility Regulation Comparison of twodoses of Mifepristone in combination with misoprostolfor early abortion. A randomised trial. Br J ObstetGynaecol 2000:107;524 – 530.
4. Schaff E, Eisinger S, Stadalius L, et al. Low – dosemifepristone 200 mg and vaginal misoprostol forabortion. Contraception 1999; 59: 1–6.
5. Ulmann, André. “The development of mifepristone: apharmaceutical drama in three acts”. J Am MedWomens Assoc. 2000; 55: 117–120.
6. Bracken H, Gliozheni O, Manoku N, Moisiu R, Shanon C,TASHA I. et al. Mifepristone medical abortion in Albania:Results from a pilot clinical research study. The EuropeanJournal of Contraception and Reproductive Health Care.2006; 11: 38–46.
7. Winikoff B, Ellertson C, Clark s. Analysis of failure inmedical abortion. Contraception 1996; 54: 323-327.
8. Hagri S, Blum J, Gueddana N, et al. Expanding medicalabortion in Tunisia: Women’s experience from amultisite expansion study, Contraception 2004; 69:63–69.
Cilt
:3Sa
y›:3
/ A
ral›k
201
1
Maltepe T›p Dergisi/ Maltepe Medical Journal
15
1 At least 18 years old (age of patient)? Yes No
2 Positive urine pregnancy test? Yes No
3 Gestational age, LM month....day.....year...... Yes No
4 Willing to come for at least one follow-up visit? Yes No
5 Willing to provide an address and/or phone Nr. where she can be contacted?
Yes No
6 Willing to fill out a short diary of side effects? Yes No
7 Have an IUD in place? Yes No
8 Clotting disorders or anticoagulant therapy? Yes No
9 Long – term glucocorticoide - steroid therapy? Yes No
10 Adrenal insufficiency? Yes No
11 Vaginal bleeding? Yes No
12 Suspicion of ectopic pregnancy? Yes No
13 Documented history of familial porphyries? Yes No
14 Known allergy to mifepristone? Yes No
15 Known allergy to misoprostole? Yes No
16 Signs of severe ill health? Yes No
Table 1

ÖZETAmaç: Üçlü tedavi sonras› semptomlar› kaybolan an-
cak Helikobakter pilori (Hp) pozitifli¤i devam eden hastala-ra ek tedavi gereksinimini ortaya koymak.
Yöntem: Klini¤imizde yap›lan gastroskopilerinde yal-n›zca antral gastrit saptanan semptomatik 321 hastan›n248’inde biyopsi ile Hp (+) gösterildi. Hp(+) hastalaraamoksisilin 1 gr 2x1 klaritromisin 500mg 2x1 14 gün bo-yunca ve pantoprazol 40 mg iki ay boyunca verildi. Tedavisonras› yap›lan gaita analizlerinde 74 hastada Hp eradikas-yonunun baflar›s›z oldu¤u görüldü. Eradikasyonun baflar›s›zoldu¤u bu hastalardan 42’si semptomlar›n›n tümü ile yokoldu¤unu ifade etti. Asemptomatik hastalar iki gruba ayr›l-d›. Birinci gruptakilere tetrasiklin 2x500mg ve metranidazol4x500mg’l›k ikinci basamak tedavisi verildi. ‹kinci gruptakihastalara sadece beslenme önerilerinde bulunuldu. Her ikigrup hasta 6 ay sonra tekrar kontrole ça¤r›ld›.
Bulgular: Birinci gruptaki 21 hastan›n gaitada Hp ana-lizleri tekrarland›. Sadece 9 hastada pozitifli¤in devam etti-¤i ancak bu gruptaki 9 (dördü H(p-)) hastada semptomla-r›n tekrar bafllad›¤› görüldü. Sadece diyet verilmifl olan ikin-ci gruptaki hastalar›n ise 10’u flikayetlerinin tekrarlad›¤›n›ifade etti.
Sonuç: Antibiyotik tedavisi sonras› semptomlar› düze-len ancak Hp pozitifli¤i devam eden hastalarda Hp eradi-kasyonu amac› ile ikinci basamak tedavi vermenin klinikyarar› tart›flmal›d›r.
Anahtar kelimeler: helikobakter pilori, eradikasyon,semptom, antral gastrit.
ABSTRACTObjective: To determine the need of medical therapy
in asymptomatic, Helicobacter pylori positive antral gastritispatients after a triple eradication therapy.
Material and methods: Gasatroscopically detectedsymptomatic antral gastritis patients were evaluated. 248of 321 were Helicobacter pylori (+).These patients weretreated by amoxicilin 1 gr 2x1 clarithromycin 500 mg 2x1for forteen days and pantoprazol 40 mg daily for twomonths. After the therapy 74 patients were still Hp(+)according to the stool analyzes and eradication wasunsuccesfull.. 42 of those patients whom erradicationtherapy failed were completely asymptomatic.Asymptomatic patients were seperated into two groups.First group was treated by tetracycline 2x500mg andmetranidazole 4x500 mg. The second group did not useany drugs and only dietary regulations were suggested. Sixmoths later both groups were controlled again.
Results: The stool analyzes of 21 patients in the firstgroup were repeated. Only 9 were positive but thesymptoms reoccured in 9 (4 Hp(-)) patients. ‹n the secondgroup 10 patients were symptomatic after the dietaryregulations.
Conclusion: The need of second line medical therapyin asymptomatic, Hp positive antral gastritis patients aftera triple erradication therapy is controversial
Key words: helicobacter pylori, eradication, symptom,antral gastritis
Üçlü tedavi sonras› semptomlar› kaybolan ancakHelikobakter pilori pozitifli¤i devam eden antralgastrit hastalar›nda ek tedavi gereksinimi
The need of medical therapy in asymptomatic,Helicobacter pylori positive antral gastritispatients after a triple eradication therapy
Dr. Manuk N Manukyan / Maltepe Üniversitesi T›p Fakültesi Genel Cerrahi Ana Bilim Dal› Dr. U¤ur Deveci / Maltepe Üniversitesi T›p Fakültesi Genel Cerrahi Ana Bilim Dal› Dr. Nefle Yener / Maltepe Üniversitesi T›p Fakültesi Patoloji Ana Bilim Dal›Dr. Ahmet Midi / Maltepe Üniversitesi T›p Fakültesi Patoloji Ana Bilim Dal›Dr. Sertan Kapakl› / Maltepe Üniversitesi T›p Fakültesi Genel Cerrahi Ana Bilim Dal› Dr. Ka¤an Gökçe / Maltepe Üniversitesi T›p Fakültesi Genel Cerrahi Ana Bilim Dal› Dr. Abut Kebudi / Maltepe Üniversitesi T›p Fakültesi Genel Cerrahi Ana Bilim Dal›

Cilt
:3Sa
y›:3
/ A
ral›k
201
1
Maltepe T›p Dergisi/ Maltepe Medical Journal
17
G‹R‹fiHelikobakter pilori (Hp) geçen yüzy›l›n t›bb›na damgas›-
n› vuran en önemli kefliflerden birisidir. Polimorfonükleerlokosit infiltrasyonunun görüldü¤ü kronik aktif gastritlespiral bakterilerin iliflkili olabilece¤i 1983 y›l›nda duyrul-du(1).Ard›ndan kronik aktif gastrit ve peptik ülser etyoloji-sinde önemli bir faktör oldu¤u tespit edildi (2).Hp nedenlikronik gastrit hastalar›n›n %15-20’sinde peptik ülser, yak-lafl›k %1’inde gastrik malinite geliflti¤i bilinmektedir(3,4).Hp eradikasyonu peptik ülser nüksünü azalmakta, erkendönem MALT (mucosa associated lymphoid tissue) lenfo-ma remisyona sokulabilmektedir(5).
Hp dünya nüfusunun yar›s›ndan fazlas›nda görülen yay-g›n bir enfeksiyondur ancak geliflmekte olan ülkelerde ya-p›lan epidemiyolojik çal›flmalar›n yetersizli¤i nedeniyle veri-ler yeterli de¤ildir. Hp tan›s›nda kullan›labilecek özgüllük veduyarl›l›¤› yüksek testler mevcuttur. Bunlardan histopatolo-ji, sitoloji, bakteri kültürü, biyopsi, üreaz testi ve Hp PCRtesti endoskopi gerektirirken; seroloji, üre nefes testi ve ga-itada antijen testi non invaziv testlerdir(6,7). 1990’l› y›llardatercih edilen tedavi rejimleri tekli tedavilerdi, daha sonra üç-lü ve dörtlü tedaviler kullan›lmaya bafllanm›flt›r(8). Bugünyan etkisi az, baflar› oran› yüksek, 1 veya 2 hafta süre ile vesabah akflam uygulanan proton pompa inhibitörü + klarit-romisin 2x500 mg + amoksisilin 2x1000 mg kombinasyo-nudur. Ancak kimler tedavi edilmelidir sorusunun cevab›asemptomatik olan hastalar tedavi edilmemelidir fleklinde-dir. Bizim çal›flmam›z›n amac› Hp pozitif ve semptomatikolup üçlü tedavi sonras› semptomlar› kaybolan ancak Hppozitifli¤i devam eden hastalara ek tedavi gereksinimini or-taya koymakt›r.
GEREÇ VE YÖNTEMKlini¤imizde yap›lan gastroskopilerde yaln›zca antral
gastrit saptanan semptomatik 321 hastada Hp araflt›rmas›için endoskopik ifllem esnas›nda antrumdan iki adet biyop-si al›nd›. Biyopsi örnekleri %10 formalin solusyonu içerisin-de patoloji labarotuvar›na yolland›. Patoloji laboratuvar›nda4 μm kal›nl›¤›nda doku kesitleri elde edildi. Kesitler, Hp en-feksiyonu tan›s› için Giemsa ile boyand›. Ifl›k mikroskobun-da spiral (yay) seklinde basillerin görülmesi ile Hp enfeksi-yonu teflhis edildi.. Hp(+) hastalara amoksisilin 1 gr 2x1 kla-ritromisin 500mg 2x1 14 gün boyunca ve pantoprazol 40mg iki ay boyunca verildi. Tedavi sonras› yap›lan gaita ana-lizlerinde Hp eradikasyonu baflar›s›z olan hastalardanasemptomatik olanlar iki gruba ayr›ld›. Birinci gruptakileretetrasiklin 2x500mg ve metranidazol 4x500mg’l›k ikinci ba-samak tedavisi verildi. ‹kinci gruptaki hastalara sadece bes-lenme önerilerinde bulunuldu. Her iki grup hasta 6 ay ve 1y›l sonra tekrar kontrole ça¤r›ld›.
SONUÇLARYaln›zca antral gastrit saptanan semptomatik 321 has-
tan›n 248’inde biyopsi ile Hp pozitifli¤i gösterildi. Hp(+)
hastalara tedavi sonras› yap›lan gaita analizlerinde 74 has-tada Hp eradikasyonunun baflar›s›z oldu¤u görüldü. Eradi-kasyonun baflar›s›z oldu¤u bu hastalardan 42’si semptom-lar›n›n tümü ile yok oldu¤unu ifade etti. Asemptomatikhastalar iki gruba ayr›ld›. Birinci gruptaki ikinci basamak te-davi verilen 21 hastan›n gaitada Hp analizleri tekrarland›.Sadece 9 hastada (%43) pozitifli¤in devam etti¤i ancak bugruptaki 9 (dördü Hp-) hastada (%43) semptomlar›n tekrarbafllad›¤› görüldü. Sadece diyet verilmifl olan ikinci grupta-ki hastalar›n ise 10’u (%47) flikayetlerinin tekrarlad›¤›n› ifa-de etti.Her iki grup Ki-kare testi ile k›yasland›¤›nda istatis-tiksel olarak fark olmad›¤› görüldü.
TARTIfiMAAntrumda bafllayan yüzeysel gastritin zaman içersinde
tüm mideye yay›lmas›n›n yan›nda, inflamasyonun derinle-flerek tam kat mukozal gastrite ve ard›ndan da atrofi ve in-testinal metaplazi ve displazi gibi daha ciddi histopatolojikde¤iflikliklere yol açabilece¤i anlafl›lm›flt›r. Hp enfeksiyonu-nun en a¤›r komplikasyonu gastrik adenokanserdir. Gastrikmaltoma’n›n prognozu daha iyi olup Hp eradikasyon teda-visinden fayda görülebilir. Hp eradikasyonu ile MALT lenfo-mada sa¤lanan iyileflme %60-83 aras›nda de¤iflmektedir.Hp eradikasyonu ayr›ca skuamöz hücreli özefagus kanseriile de iliflkili bulunmufltur. Baz› vaka raporlar›na göre ise Hperadikasyonu peptik ozefajite neden olabilir. Bu muhteme-len kardia bölgesindeki bakterilerin koruyucu etkisine ba¤-l›d›r(9). Bu bilgiler ›fl›¤›nda antral gastrit ve Hp(+) tespit edi-len hastalarda eradikasyon tedavisi mutlaka verilmelidir.
Hp’de antibiyotiklere karfl› primer (do¤al) direnç ve/ve-ya sekonder (kazan›lm›fl) direnç bulunabilir. Bu durum era-dikasyon tedavilerinde baflar›s›zl›¤a neden olur(10).Ancakeradikasyon baflar›s›z dahi olsa hastalar›n bir k›sm›nda kli-nik semptomlar iyileflmektedir, bu hastalar›n asemptomatikhastalar olarak kabul edilip edilmeyece¤i ve ikinci basamakeradikasyon gereklili¤i tart›flmal›d›r. Çal›flmam›zda Hp era-dikasyonu ilk basamak sonras› baflar›s›z olan iki grup hasta-dan tekrar eradikasyon tedavisi verilen ve verilmeyen gruparas›nda anlaml› farkl›l›k olmad›¤› görülmüfltür.
Antibiyotik tedavisi sonras› semptomlar› düzelen ancakHp pozitifli¤i devam eden hastalarda Hp eradikasyonuamac› ile ikinci basamak tedavi vermenin 1 y›ll›k k›sa dö-nemde klinik yarar› yoktur. Ancak bu durumun yukar›dabelirtilen malinite geliflme gibi olas›l›klar› incelemek içintoplum tabanl› çok yüksek hastal›kl› çal›flmalara ihtiyaçvard›r.
KAYNAKLAR1. Warren JR, Marshall BJ. Unidentified curved bacilli on
gastric epithelium in active chronic gastritis. Lancet1983;1:1273-1275.
2. Marshall BJ, Warren JR. Unidentified curved bacilli inthestomach of patients with gastritis and peptic ulce-ration.Lancet 1984;1:1311-1315.

3. Ramakrishnan K, Salinas RC. Peptic ulcer disease. AmFam Physician 2007;76:1005-1012.
4. Duggan A. Helicobacter pylori: when is treatmentnow indicated? Intern Med J 2002;32:465–469.
5. Zullo A, Hassan C, Andriani A. Eradication therapy forHelicobacter pylori in patients with gastric MALTlymphoma: a pooled data analysis. Am J Gastroente-rol.2009;104:1932-1937.
6. Sezgin O, Alt›ntafl E, Üçbilek E, Tataro¤lu C. Bizmuth-based therapies for the first step eradication of Heli-cobacter pylori. Turk J Gastroenterol 2006;17:90-93.
7. Goodwin CS, Mendall MM, Northfield TC. Helicobac-
ter pylori infection. Lancet 1997; 349:265-2698. Vaira D, Malfertheiner P, Megraud F, Axon AT Delten-
re M, Gasbarrini G, Garcia JMP et al. HpSA EuropeanStudy Group. Diagnosis of Helicobacter infection witha new non-invasive antigen-based assay. Lancet1999; 354:30-33
9. Helikobakter pilori: Nobel t›p ödülünü hak etti mi?Yusuf Bayraktar 8. Ulusal iç hastal›klar› kongresi. P256
10. Ba¤lan HP, Özden A. Helicobacter pylori’nin antibiyo-tiklere direnci. Güncel Gastroenteroloji 2003;7:220-225.
Man
ukya
nve
Ark
adafl
lar›
Maltepe T›p Dergisi/ Maltepe Medical Journal
18

ÖZETAmaç: Bipolar koter kullan›larak yap›lan unilateral proksimal
tubal oklüzyon iflleminin birinci ve alt›nc› aylarda rat over histo-patolojisi üzerine etkilerinin incelenmesi.
Yöntem: Eriflkin 28 Wistar albino rat östrus faz›nda rastgele4 gruba ayr›ld›.
G1 (n=7): Bat›n aç›l›p kapat›lan ve 1 ay sonra sol ooferekto-mi yap›lan grup.
G2 (n=7): Sol proksimal tubal oklüzyon yap›l›p 1 ay sonra solooferektomi yap›lan grup.
G3 (n=7): Bat›n aç›l›p kapat›lan ve 6 ay sonra sol ooferekto-mi yap›lan grup.
G4 (n=7): Sol proksimal tubal oklüzyon yap›l›p 6 ay sonra solooferektomi yap›lan grup.
Sol over örnekleri formaldehitle tespit edildi. HematoksilenEozin ile boyanan preparatlarda over folikül rezervi saptand›. At-retik foliküllerin say›s›, corpus luteum, corpus albicans tespit edil-di. Corpus luteum içi anjiogenesiz varl›¤›ndaki gerileme ve ovar-yan stromada fibrozis varl›¤› incelendi. Overdeki folikül kisti say›l-d›. G1-G2 ile G3-G4 ile karfl›laflt›r›ld›. Ordinal veriler için MannWhitney U testi, nominal veriler için x2 testleri kullan›ld›. p<0.05anlaml› kabul edildi.
Bulgular: G1-G2 ile, G3-G4 ile karfl›laflt›r›ld›¤›nda tüm de¤er-ler benzer bulundu (p>0.05, Mann Whitney U test). Corpus lute-um içi anjiogenezisdeki gerileme G2 ve G4’de anlaml› olmamak-la birlikte azalm›flt›. Hiçbir grupta makroskobik veya mikroskobikkist geliflmedi
Sonuç: Ratlarda bipolar koter kullan›larak yap›lan unilateralproksimal tubal okluzyon ifllemi, erken ve geç dönemde over his-topatolojisi üzerine herhangi bir zararl› etki yapmam›flt›r.
Anahtar kelimeler: ovaryan histopatoloji, proksimal tubaloklüzyon, rat.
ABSTRACTObjective: Examination of the effects of unilateral proximal
tubal oclusion procedure by bipolar electrical coagulation on rat’sovarian histopathology at the first and six months.
Material and Methods: Adult 28 Winstar albino rats ateustrous phase randomly divided into 4 groups.
G1 (n=7): Left oopherectomy, one month after laparatomy.G2 (n=7): Left oopherectomy, one month after proximal
tubal oclusion.G3 (n=7): Left oopherectomy, six months after laparatomy.G4 (n=7): Left oopherectomy, six months after proximal
tubal oclusion.Left ovary specimens fixed with formaldehyde, dyed with
Hematoxylen-Eosin and ovarian reserve examined. The numberof atretic follicles, corpus luteum and corpus albicansdetermined. Angiogenesis in corpus luteum and presence ofovarian stromal fibrosis examined. G1and G2 were comparedwith G3 and G4. Statistical analysis of ordinal results wereexamined by Mann Whitney U test and nominal results by x2 testf. P<0.05 accepted as statistically significant
Results: The results were similiar between G1and G2 whencompared with G3and G4 (p>0.05, Mann Whitney U test ).Angiogenesis regression in corpous luteum were lower in bothG2 and G4. No macroscopic or microscopic cyst formationobtained in all groups.
Conclusion: Proximal tubal occlusion procedure bybipolar coagulation has no harmful effect on rat oavarianhistopathology at both early and late period.
Key words: ovarian histhopathology, proximal tubalocclusion, rat.
Examination of the histopathological effectsof proximal tubal occlusion procedure on ratovaries: An experimental study
Proksimal tubal oklüzyon iflleminin ratover histopatolojisi üzerine etkilerininincelenmesi: Deneysel çal›flma
Dr. Aygen Çelik / Maltepe Üniversitesi T›p Fakültesi Kad›n hastal›klar› ve Do¤umDr. Remzi At›lgan / F›rat Üniversitesi T›p Fakültesi Kad›n hastal›klar› ve Do¤umDr. Berna Halilo¤lu / Maltepe Üniversitesi T›p Fakültesi Kad›n hastal›klar› ve Do¤umDr. Erdin ‹lter / Maltepe Üniversitesi T›p Fakültesi Kad›n hastal›klar› ve Do¤umDr. Tonguç Gündüz / Maltepe Üniversitesi T›p Fakültesi Kad›n hastal›klar› ve Do¤umDr. Nusret Akpolat / F›rat Üniversitesi T›p Fakültesi Patoloji Anabilimdal›Dr. Ekrem Sapmaz / Kad›n Hastal›klar› ve Do¤um AD, F›rat Üniversitesi T›p Fakültesi, Elaz›¤
DE
NE
YS
EL
Ç
AL
Ifi
MA

G‹R‹fi:Hidrosalpinksli olgularda IVF-ET (in vitro fertilizasyon-
embryo transferi) sonuçlar› implantasyon, ve gebelik oran-lar› aç›s›ndan olumsuz yönde etkilenir (1-3). En kötü sonuç-lar özellikle büyük hidrosalpinks tespit edilen vakalarda or-taya ç›kar (4). Hidrosalpinks tedavisinde salpenjektomi ens›k kullan›lan yöntemdir (5–7). Ayr›ca neosalpingostomi,drenaj ve proksimal tubal oklüzyon da kullan›labilir (8–13).Salpingostomi vakalar›nda salpenjektomi veya tubal oklüz-yona göre daha fazla ektopik gebelik saptan›r (8). Drenaj ifl-lemi, al›nan s›v›n›n üç gün içinde tekrar birikmesi sonucun-da implantasyon ve gebelik oranlar› üzerine etkisiz oldu¤utespit edilmifltir (14,15). Salpenjektomi IVF-ET baflar›s›n› an-laml› olarak art›r›r (4–7). Ancak salpenjektominin insanlar-da ve ratlarda over kan ak›m›n› bozarak over fonksiyonlar›ve rezervi üzerine olumsuz etki yapt›¤› ve postoperatif yo-¤un pelvik adezyonlara neden oldu¤u düflünülmüfltür(10,16,17).
Dar P. ve arkadafllar› (18) ektopik gebelik nedeniyle la-paroskopik salpenjektomi yap›lan vakalarda over üzerineherhangi bir olumsuz etki saptamam›flken, Chan ve ark.(19) ektopik gebelik vakalar›nda laparatomi ile yap›lan sal-penjektominin herhangi bir olumsuz etkisinin olmad›¤›n›ancak laparoskopik salpenjektominin overi olumsuz etkile-di¤ini savunmufltur.
Oysa daha kolay ve az invaziv bir ifllem olan, baflar›s› sal-penjektomi ile benzer bulunan proksimal tubal oklüzyon-da, mezosalpinkse travma olas›l›¤› azald›¤› için over rezervidaha az etkilenebilir ve adezyon azalabilir (9,10)
GEREÇ VE YÖNTEMLER: Bu deneysel çal›flma F›rat Üniversitesi T›p Fakültesi De-
ney Hayvanlar› laboratuar›nda yap›ld›. 28 adet düzenli sik-lusa sahip, 190-220 g a¤›rl›¤›nda, 14 haftal›k, eriflkin difliWistar Albino cinsi rat 12 saat ›fl›k (08-22), 12 saat karan-l›k fotoperiyodunda ve 21-23 C sabit s›cakl›ktaki odada,standart pellet yemi ve flehir suyu ile beslendi. Bu çal›flmaiçin F›rat Üniversitesi T›p Fakültesi etik komitesinden izinal›nd› ve deney flartlar› “Guide for the Care and Use of La-boratory Animals” prensiplerine uygun olarak düzenlendi.Deneyden 18 saat önce oral beslenme kesildi, sadece su iç-melerine izin verildi. Vajinal sitoloji takibinde estrus faz›nda(Resim:1) tespit edilen ratlara anestezi sa¤lamak amac›yla400 mg/kg/IP dozunda kloral hidrat uyguland›. Ratlar s›rtüstü operasyon masas›na yat›r›ld›, bat›n orta hat insizyonlaaç›ld›. Ratlar rastgele 4 gruba ayr›ld›.
28 adet 3,5 ayl›k rat rastgele 4 gruba ayr›ld›.G1 (n=7): Bat›n aç›l›p kapat›lan ve 1 ay sonra sol oofe-
rektomi yap›lan grup. G2 (n=7): Bipolar koterle sol proksimal tubal oklüzyon
yap›l›p 1 ay sonra sol ooferektomi yap›lan grup. G3 (n=7): Bat›n aç›l›p kapat›lan ve 6 ay sonra sol oofe-
rektomi yap›lan grup. G4 (n=7): Bipolar koterle sol proksimal tubal oklüzyon
yap›l›p 6 ay sonra sol ooferektomi yap›lan grup. Bat›n tabakalar› ve cilt 3/0 ipekle kapat›ld›. Ratlar deney
sonuna kadar ayr› ayr› yediflerli kafeslerde tutuldu. Sol overdokusu histopatolojik inceleme için %10’luk formaldehitlefikse edildi, parafin bloklara gömüldü, 4 mikrometre kal›n-l›¤›nda kesit al›nd›. Kesitler hematoksilen eozin (HE) ile bo-yand›. Ifl›k mikroskopisi alt›nda incelenen preparatlarda pri-mordial, primer, sekonder ve tersiyer foliküller say›ld›. Hep-si toplanarak over folikül rezervi hesapland› (20). Atretik fo-liküller, corpus luteum (CL), corpus albicans say›ld›. Toplamcorpus geliflimi hesapland›. CL içi anjiogenesiz varl›¤›ndakigerileme incelendi. Ovaryan stromada fibrozis varl›¤› ince-lendi. CL içi anjiogenezisdeki gerileme ve fibrozis varl›¤› içinordinal skala (yok=0p, var=1p, Çok var=2p) oluflturuldu.Overdeki folikül kisti mikroskopik say›ld›. Overdeki folikülkisti için ayr›ca nominal skala (makroskobik olarak yok=0p,var=1p) oluflturuldu. G1-G2 ile G3-G4 ile karfl›laflt›r›ld› (yaflkarfl›laflt›rmal› gruplar). Ordinal veriler için Mann Whitney Utesti, nominal veriler için x2 testleri kullan›ld›, p<0.05 an-laml› kabul edildi.
BULGULAR:Tüm ratlarda deney baflar› ile tamamland›. G1ve G3’de-
ki ratlarda normal over folikül gelifliminin tüm basamaklar›tespit edildi (Resim: 2 ve Resim: 3). Ancak G3’te (Resim: 3)yafllanmaya ba¤l› olarak over follikül rezerv elemanlar›ndaazalma tespit edildi. (P<0.05)
G1-G2 ile G3-G4 ile karfl›laflt›r›ld›¤›nda tüm de¤erlerbenzer bulundu.
Over folikül rezervi elemanlar› G1’de G2’ye göre (Resim2 ve Resim: 4 ile Resim: 5) G3’te G4’e göre yüksek olmas›-na ra¤men (Resim: 3 ve Resim: 6 ile Resim: 7) istatistikselfark tespit edilmedi (p>0.05, Mann Whitney U test).
G2 ve G4’te (Resim: 3 ve Resim 6 ve Resim: 7) atretikfolikül ve fibrozis biraz fazla olmas›na ra¤men istatistikselfark tespit edilmedi (p>0.05, Mann Whitney U test).
CL içi anjiogenezisdeki gerileme G2 ve G4’de azalm›flt›.
Çel
ikve
Ark
adafl
lar›
Maltepe T›p Dergisi/ Maltepe Medical Journal
20
Resim 1: Östrus faz›ndaki bir ratta vajinal smearda sadecekeratinize olmufl (kornufiye) süngerimsi hücreler görülüyor(HE, X 40).
Maltepe T›p Dergisi/ Maltepe Medical Journal
21
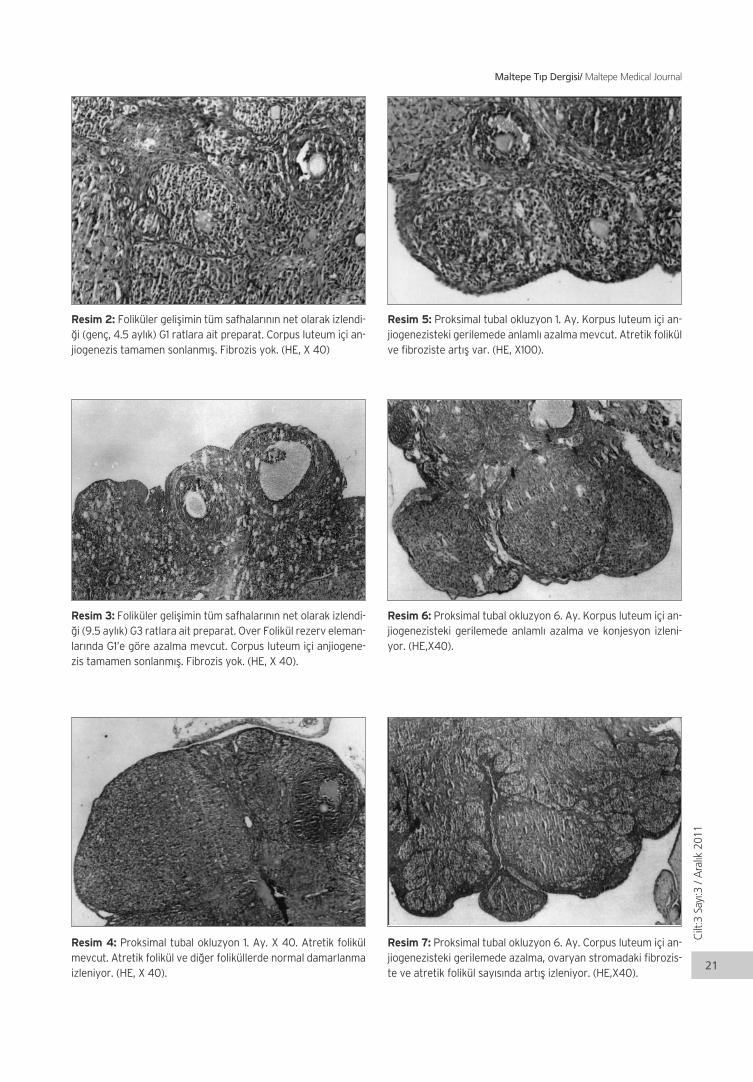
Resim 2: Foliküler geliflimin tüm safhalar›n›n net olarak izlendi-¤i (genç, 4.5 ayl›k) G1 ratlara ait preparat. Corpus luteum içi an-jiogenezis tamamen sonlanm›fl. Fibrozis yok. (HE, X 40)
Resim 3: Foliküler geliflimin tüm safhalar›n›n net olarak izlendi-¤i (9.5 ayl›k) G3 ratlara ait preparat. Over Folikül rezerv eleman-lar›nda G1’e göre azalma mevcut. Corpus luteum içi anjiogene-zis tamamen sonlanm›fl. Fibrozis yok. (HE, X 40).
Resim 4: Proksimal tubal okluzyon 1. Ay. X 40. Atretik folikülmevcut. Atretik folikül ve di¤er foliküllerde normal damarlanmaizleniyor. (HE, X 40).
Resim 5: Proksimal tubal okluzyon 1. Ay. Korpus luteum içi an-jiogenezisteki gerilemede anlaml› azalma mevcut. Atretik folikülve fibroziste art›fl var. (HE, X100).
Resim 6: Proksimal tubal okluzyon 6. Ay. Korpus luteum içi an-jiogenezisteki gerilemede anlaml› azalma ve konjesyon izleni-yor. (HE,X40).
Resim 7: Proksimal tubal okluzyon 6. Ay. Corpus luteum içi an-jiogenezisteki gerilemede azalma, ovaryan stromadaki fibrozis-te ve atretik folikül say›s›nda art›fl izleniyor. (HE,X40).
Cilt
:3Sa
y›:3
/ A
ral›k
201
1
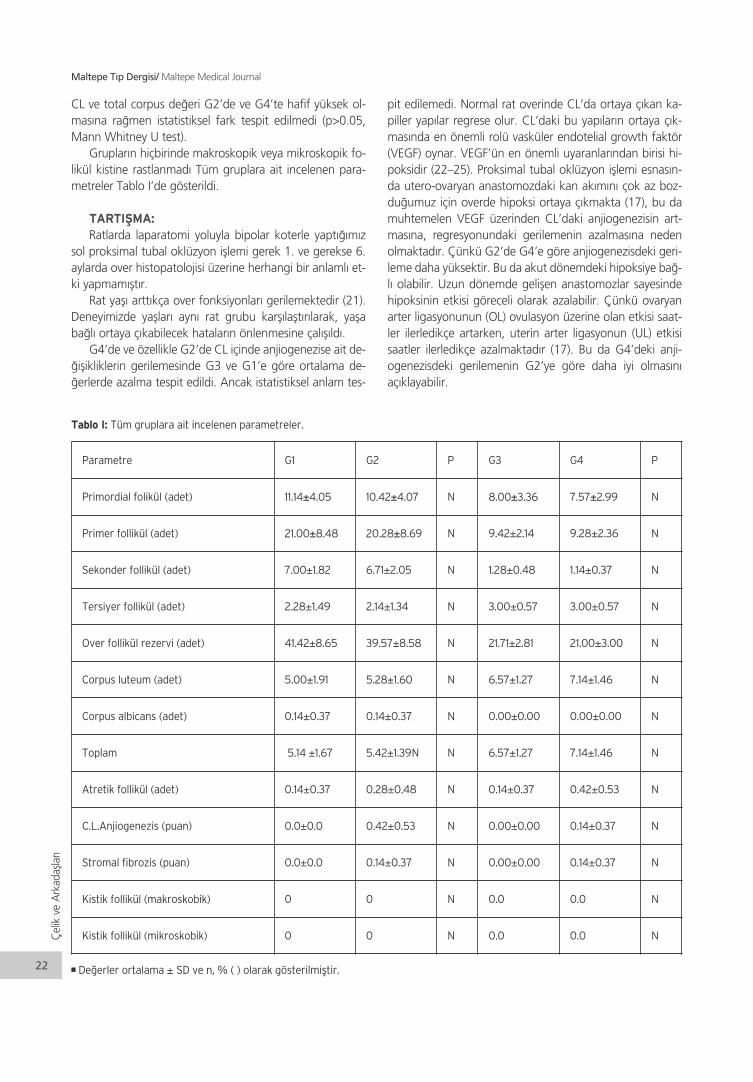
CL ve total corpus de¤eri G2’de ve G4’te hafif yüksek ol-mas›na ra¤men istatistiksel fark tespit edilmedi (p>0.05,Mann Whitney U test).
Gruplar›n hiçbirinde makroskopik veya mikroskopik fo-likül kistine rastlanmad› Tüm gruplara ait incelenen para-metreler Tablo I’de gösterildi.
TARTIfiMA:Ratlarda laparatomi yoluyla bipolar koterle yapt›¤›m›z
sol proksimal tubal oklüzyon ifllemi gerek 1. ve gerekse 6.aylarda over histopatolojisi üzerine herhangi bir anlaml› et-ki yapmam›flt›r.
Rat yafl› artt›kça over fonksiyonlar› gerilemektedir (21).Deneyimizde yafllar› ayn› rat grubu karfl›laflt›r›larak, yaflaba¤l› ortaya ç›kabilecek hatalar›n önlenmesine çal›fl›ld›.
G4’de ve özellikle G2’de CL içinde anjiogenezise ait de-¤iflikliklerin gerilemesinde G3 ve G1’e göre ortalama de-¤erlerde azalma tespit edildi. Ancak istatistiksel anlam tes-
pit edilemedi. Normal rat overinde CL’da ortaya ç›kan ka-piller yap›lar regrese olur. CL’daki bu yap›lar›n ortaya ç›k-mas›nda en önemli rolü vasküler endotelial growth faktör(VEGF) oynar. VEGF’ün en önemli uyaranlar›ndan birisi hi-poksidir (22–25). Proksimal tubal oklüzyon ifllemi esnas›n-da utero-ovaryan anastomozdaki kan ak›m›n› çok az boz-du¤umuz için overde hipoksi ortaya ç›kmakta (17), bu damuhtemelen VEGF üzerinden CL’daki anjiogenezisin art-mas›na, regresyonundaki gerilemenin azalmas›na nedenolmaktad›r. Çünkü G2’de G4’e göre anjiogenezisdeki geri-leme daha yüksektir. Bu da akut dönemdeki hipoksiye ba¤-l› olabilir. Uzun dönemde geliflen anastomozlar sayesindehipoksinin etkisi göreceli olarak azalabilir. Çünkü ovaryanarter ligasyonunun (OL) ovulasyon üzerine olan etkisi saat-ler ilerledikçe artarken, uterin arter ligasyonun (UL) etkisisaatler ilerledikçe azalmaktad›r (17). Bu da G4’deki anji-ogenezisdeki gerilemenin G2’ye göre daha iyi olmas›n›aç›klayabilir.
Maltepe T›p Dergisi/ Maltepe Medical Journal
22
Çel
ikve
Ark
adafl
lar›
Parametre G1 G2 P G3 G4 P
Primordial folikül (adet) 11.14±4.05 10.42±4.07 N 8.00±3.36 7.57±2.99 N
Primer follikül (adet) 21.00±8.48 20.28±8.69 N 9.42±2.14 9.28±2.36 N
Sekonder follikül (adet) 7.00±1.82 6.71±2.05 N 1.28±0.48 1.14±0.37 N
Tersiyer follikül (adet) 2.28±1.49 2.14±1.34 N 3.00±0.57 3.00±0.57 N
Over follikül rezervi (adet) 41.42±8.65 39.57±8.58 N 21.71±2.81 21.00±3.00 N
Corpus luteum (adet) 5.00±1.91 5.28±1.60 N 6.57±1.27 7.14±1.46 N
Corpus albicans (adet) 0.14±0.37 0.14±0.37 N 0.00±0.00 0.00±0.00 N
Toplam 5.14 ±1.67 5.42±1.39N N 6.57±1.27 7.14±1.46 N
Atretik follikül (adet) 0.14±0.37 0.28±0.48 N 0.14±0.37 0.42±0.53 N
C.L.Anjiogenezis (puan) 0.0±0.0 0.42±0.53 N 0.00±0.00 0.14±0.37 N
Stromal fibrozis (puan) 0.0±0.0 0.14±0.37 N 0.00±0.00 0.14±0.37 N
Kistik follikül (makroskobik) 0 0 N 0.0 0.0 N
Kistik follikül (mikroskobik) 0 0 N 0.0 0.0 N
Tablo I: Tüm gruplara ait incelenen parametreler.
n De¤erler ortalama ± SD ve n, % ( ) olarak gösterilmifltir.

Anderson ve ark ( 26 ) uterusta yap›lan luteolitik faktör-ler (bunlar luteal hücrelerdeki mitokondri ve lizozomlar› et-kileyerek CL’un regresyonunu sa¤larlar) oldu¤unu ve kanak›m›n›n bozulmas› nedeniyle bu maddelerin overe tafl›na-mad›¤› için CL’un regresyonunda gecikme oldu¤unu tespitetmifllerdir. Gruplar aras›nda istatistiksel fark olmamaklaberaber G2 ve G4’teki CL’un ortalama de¤erlerinin G1 veG2’ye göre daha fazla olmas› ile uyumludur.
Ovaryan fibrozis ve atretik folikül say›s› G1 ve G3’de aziken, G2 ve G4’de çok hafif artm›flt›r. ‹nsan over stroma ya-p›s› yaflla birlikte de¤ifliklik gösterir. Reprodüktif yaflta, kor-teks farkl› evrelerdeki foliküllerle doludur ve medulla elastikfibrillerle gevflek konnektif doku, kan damarlar›, lenfatiklerve sinir liflerinden oluflur. Menapozdan sonra over hacmigözle görülür derecede azal›r. Stromada daha fazla fibrözkonnektif doku ile birlikte korpus albikans, kan damarlar›,lenfatikler ve sinirler bulunur (27). Kan veya lenfatik dola-fl›m bozuklu¤unda kollajen neoformasyonu sitimüle olur(20). Uterin ve tubal lenfatikler broad ligament içerisindebirbirlerine çok yak›n seyrederler (28). Bulgular›m›za göreproksimal tubal oklüzyon ifllemi esnas›nda kollajen oluflu-munda art›fla neden olan lenfatik dolafl›mda hasar meyda-na gelebilir.
G1 ve G3’de istatistiksel olarak anlaml› olmamakla birlik-te, over folikül rezervi ortalama de¤erleri G2 ve G4’e göredaha fazla idi. Bunun nedeni over folikül rezervindeki azal-maya kompansatuar olarak fibrozisde art›fl olmas›d›r (20).
Akut veya kronik hipoksi durumunda overlerde, di¤erorganlarda oldu¤u gibi hipoksi induced faktör-1 ( HIF-1 )aktive olur (30-32). HIF-1 alfa ve hipoksik ortam, foliküller-de regresyon ve apoptozise, sonuçta atretik foliküllerde ar-t›fla ve foliküler rezervde azalmaya neden olur (30). G2 veG4’teki atretik foliküllerdeki ve fibrozisdeki istatiksel olarakanlams›z art›fl›n nedeni kronik hipoksinin apoptotik etkisineba¤l› olabilir (32). HIF-1 alfa ayn› zamanda VEGF sal›n›m››n›art›r›r. VEGF anjiogenezisi, vasküler geçirgenlikte art›fl›, over-lerde follikülogenezisin normal iflleyiflini, overde folikül kistigeliflimini, uzun dönemde ise fibroblast growth faktör-2 üze-rinden fibrozis geliflmesini uyar›r (24,25,29,33). G2 ve G4’te-ki hafif derecede fibrozis art›fl›n›n nedeni VEGF olabilir.
Çünkü VEGF, 3. haftadan itibaren fibrozisi uyaran fib-roblast growth faktör-2’nin sentezini modüle eder. G4’defibrozisin G2’ye göre biraz fazla olmas›n›n nedeni G2’ninbir ayl›k zaman diliminde iflleme tabi tutulmas› olabilir. Ay-r›ca VEGF’in direk kollajen sentezini uyar›c› etkisi de vard›r(33, 34 ).
IVF tedavisinden önce unilateral veya bilateral hidrosal-pinksli kad›nlarda proksimal tubal okluzyon yap›lmas› ge-belik oranlar›n› klinik olarak anlaml› derecede yükseltir. Sal-penjektominin teknik olarak uygulanmas›n›n zor oldu¤uvakalarda ise proksimal tubal okluzyon tercih edilebilir (35).
Sonuç olarak, ratlarda laparatomi yoluyla bipolar koter-le yapt›¤›m›z sol proksimal tubal oklüzyon iflleminin birincive alt›nc› aylar›n sonunda over histopatolojisi üzerine an-
laml› say›labilecek herhangi bir olumsuz etki yapmam›flt›r.Bu bulgular ›fl›¤›nda hidrosalpenks tespit edilen vakalardaenfeksiyon, torsiyon ve oosit toplanmas›n› engellemesiniönlemek için salpenjektomi yerine proksimal tubal oklüz-yon tercih edilebilen bir yöntem olabilir.
KAYNAKLAR:1. Akman MA, Garca JE, Damewood MD, Watts LD and
Katz E. Hydrosalpinx affects the implantation of pre-viously cryopreserved embryos. Hum Reprod 1996;11: 1013–1014.
2. Camus E, Poncelet C, Goffinet F, Wainer B, Merlet F,Nisand I, et al. Pregnancy rates after IVF in cases of tu-bal infertility with and without hydrosapinx: meta-analysis of published comparative studies. Hum Rep-rod. 1999;14:1243-1249.
3. Andersen AN, Yue Z, Meng FJ and Petersen K. Lowimplantation rate after in-vitro fertilization in patientswith hydrosalpinges diagnosed by ultrasonography.Hum Reprod 1994;9: 1935–1938.
4. Strandell A, Lindhard A, Waldenstrom U, Thorburn J,Janson PO, Hamberger L. Hydrosalpinx and IVF outco-me: a prospective randomized multicentre trial inScandinavia on salpingectomy prior to IVF. Hum Rep-rod 1999;14:2762–2769.
5. Daftary GS, Kayisli U, Seli E, Bukulmez O, Arici A, Tay-lor HS. Salpingectomy increases peri-implantation en-dometrial HOXA10 expression in women with hydro-salpinx. Fertil Steril 2007;87:367-372.
6. Zarei A, Al- Ghafri W, Tulandi T. Tubal surgery. ClinObstet Gynecol. 2009;52:344-350.
7. Shelton KE, Butler L, Toner JP, Oehninger S, MuasherSJ. Salpingectomy improves the pregnancy rate in in-vitro fertilization patients with hydrosalpinx. HumReprod 1996;11: 523-525.
8. Yao M, Tulandi T. Current status of surgical and non-surgical management of ectopic pregnancy. Fertil Ste-ril 1997;67:421-433.
9. Murray DL, Sagoskin AW, Widra EA, Levy MJ. The ad-verse effect of hydrosalpinges on in vitro fertilizationpregnancy rates and the benefit of surgical correction.Fertil Steril 1998;69: 41-45.
10. Surrey ES, Schoolcraft WB. Laparoscopic manage-ment of hydrosalpinges before in vitro fertilization-embryo transfer: salpingectomy versus proximal tubalocclusion. Fertil Steril 2001; 75: 612-617.
11. Sharara FJ, Scott RT, Marut EL, Queenan JT. In-vitrofertilization outcome in women with hydrosalpinx.Hum Reprod 1996;11: 526–530.
12. Van Voorhis BJ, Sparks AET, Syrop CH, Stovall DW.Ultrasound-guided aspiration of hydrosalpinges is as-sociated with improved pregnancy and implantationrates after in-vitro fertilization cycles. Hum Reprod1998;13:736–739.
Cilt
:3Sa
y›:3
/ A
ral›k
201
1
Maltepe T›p Dergisi/ Maltepe Medical Journal
23

13. Aboulghar MA, Mansour RT, Serour GI, Settar MA,Awad MM, Amin Y. Transvaginal ultrasonic guidedaspiration of pelvic inflammatory cystic masses beforeovulation induction for in vitro fertilization. Fertil Ste-ril 1990;53: 311–314.
14. Sowter MC, Akande VA, Williams JAG, Hull MG. Isthe outcome of in-vitro fertilization and embryo trans-fer treatment improved by spontaneous or surgicaldrainage of a hydrosalpinx?. Hum Reprod 1997;10:2147–2150.
15. Bloechle M, Schreiner T , Lise K. Recurrence of hydro-salpinges after transvaginal aspiration of tubal fluid inan IVF cycle with development of a serometra. HumReprod 1997;12: 703–705.
16. San Filippo JS, Lincoln SR. Surgical treatment of disea-ses of the ovary. In: Keye WR, Chang RJ, Rebar RW,Soules MR, eds. Infertility: evaluation and treatment.Philadelphia: WB Saunders, 539–551.
17. Zackrisson U, Mikuni M, Peterson MC, Nilsson B, Jan-son P and Brannstrom M. Evidence for the involve-ment of blood flow-related mechanisms in the ovula-tory process of the rat. Hum Reprod 2000;15:264–272.
18. Dar P, Sachs GS, Strassburger D, Bukovsky I, Arieli S.Ovarian function before and after salpingectomy inartificial reproductive technology patients. Hum Rep-rod. 2000;15:142-144.
19. Chan CC, Ng EH, Li CF, Ho PC. Impaired ovarian blo-od flow and reduced antral follicle count following la-paroscopic salpingectomy for ectopic pregnancy.HumReprod. 2003;18: 2175-2180.
20. Souza AZ, Fonseca AM, Izzo VM, Clauzet RM, Salva-tore CA. Ovarian histology and function after totalabdominal hysterectomy. Obstet Gynecol. 1986;68:847-849.
21. Anzalone CR, Hong LS, Lu JK, LaPolt PS. Influences ofage and ovarian follicular reserve on estrous cycle pat-terns, ovulation, and hormone secretion in the Long-Evans rat. Biol Reprod 2001;64: 1056-1062.
22. Trollmann R, Amann K, Schoof E, Beinder E, WenzelD, Rascher W,et al. Hypoxia activates the human pla-cental vascular endothelial growth factor system invitro and in vivo: up-regulation of vascular endotheli-al growth factor in clinically relevant hypoxic ischemi-a in birth asphyxia. Am J Obstet Gynecol 2003;188:517-523.
23. Neeman M, Abramovitch R, Schiffenbauer YS, Tem-pel C. Regulation of angiogenesis by hypoxic stress:from solid tumours to the ovarian follicle. Int J ExpPathol. 1997;78: 57-70. Review.
24. Abulafia O, Sherer DM. Angiogenesis of the ovary.Am J Obstet Gynecol. 2000;182: 240-246.
25. Geva E, Jaffe RB. Role of vascular endothelial growthfactor in ovarian physiology and pathology. Fertil Ste-ril 2000;74: 429-438.
26. Anderson LL, Bland KP, Melampy RM. Comparativeaspectes of uterine luteal relationship. Recent ProgrHorm Res 1969; 25: 57.
27. Rolaki A, Drakakis P, Millingos S, Loutradis D, Makri-ginnakis A. Novel trends in follicular development, at-resia and corpus luteum regression: role for apopto-sis. Reprod Biomed Online 2005; 11: 93-103.
28. Barber HRK: Anatomy, embriology, and comparativeanatomy. Ovarian Carcinoma: Etiology, Diagnosis andtreatment. Edited by HRK Barber. New york, Masson,1978, 13-27.
29. Gordon JD, Mesiano S, Zaloudek CJ, Jaffe RB. Vascu-lar endothelial growth factor localization in humanovary and fallopian tubes: possible role in reproducti-ve function and ovarian cyst formation. J Clin Endoc-rinol Metab 1996;81: 353-359.
30. Ferrara N, Frantz G, LeCouter J, Dillard-Telm L, PhamT, Draksharapu A, et al. Differential expression of theangiogenic factor genes vascular endothelial growthfactor (VEGF) and endocrine gland-derived VEGF innormal and polycystic human ovaries. Am J Pathol2003;162: 1881-1893.
31. Hejmadi MV, Dajas-Bailador F, Barns SM, Jones B,Wonnacott S. Neuroprotection by nicotine againsthypoxia-induced apoptosis in cortical cultures involvesactivation of multiple nicotinic acetylcholine receptorsubtypes. Mol Cell Neurosci. 2003;24: 779-786.
32. Tanaka T, Hanafusa N, Ingelfinger JR, Ohse T, Fujita T,Nangaku M. Hypoxia induces apoptosis in SV40-im-mortalized rat proximal tubular cells through the mi-tochondrial pathways, devoid of HIF1-mediated upre-gulation of Bax. Biochem Biophys Res Commun.2003;12:222-231.
33. Rosmorduc O, Wendum D, Corpechot C, Galy B, Seb-bagh N, Raleigh J, et al. Hepatocellular hypoxia-indu-ced vascular endothelial growth factor expression andangiogenesis in experimental biliary cirrhosis. Am JPathol. 1999;155: 1065-1073.
34. Corpechot C, Barbu V, Wendum D, Kinnman N, ReyC, Poupon R, et al. Hypoxia induced VEGF and colla-gen I expressions are associated with angiogenesisand fibrogenesis in experimental cirrhosis. Hepatology2002;35:1010-1021.
35. Kontoravdis A, Makrakis E, Pantos K, Botsis D, Delige-oroglou E, Creatsas G . Proximal tubal occlusion andsalpingectomy result in similar improvement in in vit-ro fertilization outcome in patients with hydrosalpinx.Fertil Steril 2006;86:1642-1649.
Çel
ikve
Ark
adafl
lar›
Maltepe T›p Dergisi/ Maltepe Medical Journal
24

ÖZETAktinomikozun sadece nazal kavite ile s›n›rl› oldu¤u du-
rumlar nadirdir. Bu vaka sunumunda, intranazal aktinomi-koz, kronik rinosinüzit ve tek tarafl› nazal polipozis izlenen37 yafl›nda kad›n hasta bildirilmektedir. Hastan›n paranazalsinus bilgisayarl› tomografisinde (BT) sol maksiller sinüste veetmoid sinüslerde havalanma kayb› izlenmifltir. Hastan›n solnazal pasaj›n›n tamamen poliplerle oblitere oldu¤u ve po-liplerin içerisinde yüksek metalik dansitesi olan bir obje ol-du¤u izlenmifltir. Yüksek metalik dansitesi olan objenin bo-yutlar› 0.5 cm x 0.5 cm olarak ölçülmüfltür. Hastaya nazalpolipektomi ve fonksiyonel endoskopik sinus cerrahisi ya-p›lm›flt›r. Yüksek dansiteye sahip objenin, nazal poliplerleorta konka aras›nda s›k›flm›fl bir kalsifiye materyal yuma¤›oldu¤u anlafl›lm›flt›r. Kalsifiye materyal ve polipler histopa-tolojik inceleme sonucu tan›s› ‘izole intranazal aktinomi-koz’ olarak saptanm›flt›r. Hastal›¤›n bu formu oldukça na-dirdir. Bu vaka sunumunda, literatürün ›fl›¤› alt›nda, hasta-l›¤›n etyopatogenezi, tan›sal yaklafl›mlar ve tedavi modali-telerini tart›flarak, aktinomikozun çok nadir görülen bir kli-nik prezentasyonunu bildirmeyi amaçlad›k.
Anahtar kelimeler: nazal polip, aktinomikoz
G‹R‹fi‘Aktinomikoz’ terimi zaman zaman yanl›fl anlafl›lmalara
yol açabilmektedir. Fungal bir enfeksiyon olmad›¤› halde,‘mikoz’ teriminden dolay› halen fungal bir enfeksiyon oldu-¤u düflünülmektedir. Hastal›¤›n etkeni anaerobik, filamen-töz ve gram pozitif bir organizma olan Aktinomyces isreli-i’dir. Hastal›k oldukça yavafl ve progresif bir seyir izler ve bir-
ABSTRACTActinomycosis involving the nasal cavity is a rarely
encountered situation. We report the case of a 37 yearsold woman diagnosed as having intranasal actinomyco-sis, chronic rhinosinusitis and unilateral nasal polyposis.Paranasal computerized tomography (CT) showed loss ofaeration of the left maxillary sinus and ethmoid cells. Theleft nasal passage was obliterated by polyps and anobject with a high metallic density. The dimensions of theobject were 0, 5 x 0, 5 cm. Nasal polypectomy and func-tional endoscopic sinus surgery were performed. Thehigh density object was found to be a lump of calcifiedmaterial located between the nasal polyps and middleturbinate. The material and nasal polyps were sent tohistopathological evaluation. The diagnosis was‘intranasal actinomycosis’ which is a rarely encounteredclinical presentation of the disease. In our case report, wepresent the history, diagnostic approaches and treatmentmodalities of the disease under the scope of the litera-ture.
Key words: nasal polyps, actinomycosis
birine benzer lezyonlar oluflturur(1). Hastal›¤›n insidans›1970’lerde ABD’de 1:300.000 kifli/y›l iken, 1984 y›l›nda Al-manya’da 1:40.000 kifli/y›l oldu¤u bilbirilmifltir(2). Aktino-mikoz tüm sosyoekonomik seviyedeki insanlar› ve tüm ›rk-lar› etkilemektedir ve erkek – kad›n oran› 3:1 dir. Bu oran›n,erkeklerde kad›nlara oranla fasiyal ve oral travma görülme
Dr. Zafer Çiftçi / Erzurum Bölge E¤itim ve Araflt›rma Hastanesi, KBB Klini¤iDr. Damla Nihan Çak›r / Nam›k Kemal Üniversitesi T›p Fakültesi, KBB Hastal›klar› ve Bafl – Boyun Cerrahisi Anabilim Dal›Dr. Aklime Ifl›k / Nam›k Kemal Üniversitesi T›p Fakültesi, KBB Hastal›klar› ve Bafl – Boyun Cerrahisi Anabilim Dal›Dr. Öner Çelik / Maltepe Üniversitesi T›p Fakültesi, KBB Hastal›klar› ve Bafl – Boyun Cerrahisi Anabilim Dal›Dr. Erdogan Gültekin / Nam›k Kemal Üniversitesi T›p Fakültesi, KBB Hastal›klar› ve Bafl – Boyun Cerrahisi Anabilim Dal›
Nazal polipozis ve sinüzitin efllik etti¤inadir görülen intranazal aktinomikozis
Unusual intranasal presentation ofactinomycosis with nasal polyposis andsinusitis
OL
GU
S
UN
UM
U

olas›l›¤›n›n daha yüksek olmas› ve oral hijyen azl›¤›na ba¤l›oldu¤u düflünülmektedir. Hastal›¤›n bi–modal yafl da¤›l›mpaterni vard›r. Hastal›k 11–20 yafllar aras›nda görülebil-mekte ancak bir çok seride 4 ve 5. dekadlar aras›nda belir-gin bir insidans art›fl› oldu¤u bildirilmektedir (3). Aktinomi-kozun 5 – 16 yafl aras›ndaki çocuklarda s›kl›kla karfl›lafl›ld›-¤› da bildirilmifltir (4). Aktinomikozun nazal kavitede görül-mesi çok daha nadir görülen bir durumdur ve literatürdebir kaç vakada bu durum bildirilmifltir (5, 6). Bu vaka sunu-munda, 37 yafl›ndaki bir kad›n hastada, tek tarafl› nazal po-lipozis ve sinüzitin efllik etti¤i, sol nazal kavite ile s›n›rl› ka-lan bir aktinomikoz vakas› sunulmaktad›r. Tek tarafl› intra-nazal aktinomikoz ile nazal polipozis ve sinüzit birlikteli¤i-nin oldu¤u bir vaka daha önce hiç bildirilmemifltir. Aktino-mikozun geleneksel tedavisinde medikat tedavi, arkas›n-dan cerrahi tedavi ve gerekirse tamamlay›c› medical tedavikullan›l›rken, bizim vakam›zda cerrahi tedavi sonras› yap›-lan takiplerde hastal›¤a dair bulgu ve semptom izlenmedi-¤i için, medikal tedavi kullanma ihtiyac› görülmemifltir.
OLGU SUNUMUOtuzyedi yafl›nda bayan hasta Nam›k Kemal Üniversitesi
T›p Fakültesi Hastanesi Kulak Burun Bo¤az poliklini¤i’ne soniki y›ldan beri devam eden nazal obstrüksiyon, nazal ak›nt›,bafl a¤r›s› ve burundan kötü koku gelmesi flikayetleriyle bafl-vurdu. Hastan›n sistemik herhangi bir hastal›k, immünsup-resyon, diyabet veya alkol kullan›m› anamnezi yoktu. Yirmipaket – y›l sigara anamnezi vard›. Geçirilmifl bir nazal trav-ma veya nazal cerrahi hikayesi olmayan hastan›n oral hijye-ninin iyi oldu¤u ve herhangi bir dental sorununun olmad›¤›görüldü. Nazal endoskopik muayenesinde sol nazal kaviteyioblitere eden polipler izlendi. Paranazal sinus BT’sinde solmaksiller sinus ve etmoid hücrelerin, mukoza hipertrofisi,polipler ve sekresyonlar nedeniyle oblitere oldu¤u izlendi.Sol nazal pasaj nazal poliplerce ve yüksek metalik dansitesiolan bir obje ile oblitere görünümdeydi. Objenin boyutlar› 0,5 cm x 0, 5 cm olarak ölçüldü. (Resim 1 ve 2). Tam kan sa-y›m› ve sedimentasyon h›z› normal olarak bulundu.
Hastaya nazal polipektomi ve fonkiyonel sinus cerrahisiuyguland›. Yüksek dansiteli objenin kalsifiye materyal yu-ma¤› oldu¤u izlendi. Objenin orta konkan›n lateralinde lo-kalize oldu¤u ve poliplerle çevrili oldu¤u görüldü. Kalsifiyemateryal ve nazal polipler histopatolojik de¤erlendirme içingönderildi. Histopatolojik tan› ‘aktinomikoz’ olarak bidirildi.‹ki ay sonra çekilen paranazal sinus BT’de paranazal sinusaerasyonunun tamamen restore oldu¤u, nazal kavite veparanazal kavitede hastal›¤a ait herhangi bir residüel bul-guya rastlanmad›¤› görüldü (Resim 3).
TARTIfiMA Aktinomikoz fistül traktlar›, multipl abseler ve fibrozisle
seyreden subakut veya kronik, süpüratif ve granülomatözbir enfeksiyondur. Actinomycete ailesinin sufllar›n›n nedenoldu¤u bir hastal›kt›r. Hastal›¤a, s›kl›kla anaerobik gram
pozitif bir mikoorganizma olan Actinomyces israelii nedenolur (7). Aktinomiçesler oral kavite floras›n›n önemli bir k›s-m›n› olufltururlar ancak alt gastrointestinal sistem ve kad›ngenital sisteminde daha nadir olarak bulunurlar. Aktinomi-kozis vakalar›n›n % 50’si bafl – boyun bölgesindedir (servi-ko – fasiyal aktinomikoz), % 15’i toraksta, % 20’si bat›ndayer al›r ve geri kalan› pelvis, kalp ve beyinde yer al›r (3). En-feksiyonun karakteristik bulgusu a¤›zda, akci¤erlerde veyasindirim sisteminde a¤r›l› abseler oluflumudur. Nadiren, tekbafl›na veya di¤er dento – maksillo – fasiyal hastal›klarla ilifl-kili olarak paranazal sinus aktinomikozu da görülebilmek-tedir (8).
Çift
çive
Ark
adafl
lar›
Maltepe T›p Dergisi/ Maltepe Medical Journal
26
Resim 1: Preoperatif BT, koronal kesit.
Resim 2: Preoperatif BT, aksiyel kesit.
Resim 3: Postoperatif BT, hiçbir enfeksiyon bulgusu izlenme-mektedir.

Aktinomiçes sufllar› insanlarda oral kavitenin do¤al flo-ra elemanlar›ndand›r ve genellikle kona¤a zarar vermezler.Bununla beraber, enflamatuar yan›tl› bir enfeksiyona ne-den olduklar›nda, parazitik bir rol oynamaya bafllarlar.Mycobacterium tuberculosis’e benzer bir flekilde konakhücreler taraf›ndan fagosite edilseler bile hayatta kal›rlar veintrasellüler parazitler olarak adland›r›labilirler (9).
Orofarengeal bölgenin veya paranazal sinüslerin akti-nomikozunda genellikle travma veya cerrahi hikayesi var-d›r. Difl çürükleri veya oral hijyen eksikli¤inin de enfeksiyo-na neden olabilece¤i bildirilmifltir (10). Bununla beraber, bi-zim vakam›zda, yukar›da bahsedilen faktörlerden hiç biribulunmuyordu.
SONUÇ Paranazal sinüslerin aktinomikozu nadir görülen bir du-
rumdur ve hastal›¤›n klinik prezentasyonu spesifik bir tan›akla getirmez (11). Bizim vakam›zda, nazal polipozis nede-niyle, nazal endoskopide hastal›¤›n boyutlar› ile ilgili yeterlibilgi al›namad›¤› için, hastan›n paranazal sinus BT’si çekil-mifltir. Medikal tedaviye yan›ts›z rinosinüzit vakalar› parana-zal sinus BT ile de¤erlendirilmelidir.
Aktinomikoz vakalar›n›n ço¤unda, sadece medikal te-davi kullan›m› yeterli olmaktad›r. Seçilmifl vakalarda, ta-mamlay›c› tedavi olarak cerrahi kullan›labilir. Aktinomikozistedavisinde tercih edilen ilaç Penisilin G dir. Tedavi enfeksi-yon bulgular› ortadan kalk›ncaya kadar devam edilmelidir.Bizim vakam›zda hastan›n operasyondan iki ay sonra çeki-len kontrol BT’sinde, rezidüel veya rekürren enfeksiyonadair bir bulguya rastlanmam›flt›r. Hastal›k sadece cerrahi gi-riflim ile tedavi edilmifltir ve detekleyici antimikrobiyal teda-viye ihtiyaç duyulmam›flt›r.
Medikal tedaviye yan›t vermeyen ve kronik bir seyir iz-leyen rinosinüzit vakalar›nda, ay›r›c› tan›da aktinomikoz dü-flünülmelidir.
KAYNAKLAR1. Pulverer G, Schütt-Gerowitt H, Schaal KP. Human cer-
vicofacial actinomycoses: microbiological data for1997 cases .Clin ‹nfect Dis. 2003;37:490-497.
2. Ryan KJ; Ray CG. Sherris Medical Microbiology (4thed.). McGraw Hill. ISBN 0–8385–8529–9
3. Mabeza GF, Macfarlane J. Pulmonary actinomycosis.Eur Respir J 2003; 21: 545–551.
4. Melgarejo Moreno P, Hellin Meseguer D, Marco Gar-rido A, Galindo Ortego X, Ruiz Macia JA, Hostalet F Acorrelation between age and Actinomyces in the ade-notonsillar tissue of children B-ENT. 2006;2:95-97.
5. Chobaut JC, Maniere C, Badet JM, Spicarolen T, Kan-telip B. Actinomycosis in otorhinolaryngology. Apro-pos of a case with localization in the nasal cavity. AnnOtolaryngol Chir Cervicofac. 1994; 111:292–294.
6. Ozcan C, Talas D, Görür K, Aydin O, Yildiz A. Acti-nomycosis of the middle turbinate: an unusual causeof nasal obstruction. Eur Arch Otorhinolaryngol.2005; 262:412-415.
7. Mehta V, Balachandran C Primary cutaneous actinomy-cosis on the chest wall Dermatol Online J. 2008; 14:13.
8. Lee JD, Kim PG, Jo HJ, Park DH, Seo EJ. A case of pri-mary hepatic actinomycosis. J Korean Med Sci. 1993;8:385–389.
9. Friduss ME, Maceri DR. Cervicofacial actinomycosis inchildren. Henry Ford Hosp Med J. 1990; 38:28–32.
10. Zwaveling-Soonawala N, Spanjaard L, van de Wete-ring M, Winterberg DH. Intracranial actinomycosis ina child with dental caries. Ned Tijdschr Geneeskd.2003; 147:2386–2389.
11. Damante JH, Sant’Ana E, Soares CT, Moreira CR.Chronic rhinosinusitis unresponsive to medical the-rapy; a case of maxillary sinus actinomycosis focusingon computed tomography findings. DentomaxillofacRadiol, 2006; 35:213–216.
Cilt
:3Sa
y›:3
/ A
ral›k
201
1
Maltepe T›p Dergisi/ Maltepe Medical Journal
27

ÖZETKondromalar s›k rastlanan k›k›rdak kaynakl› benign ke-
mik tümörleri olmakla beraber spinal yerleflimli kondroma-lar nadirdir. Spinal yerleflimli kondromalar klinik olarak lo-kal kitle, lokal a¤r›, kord bas›s› semptomlar›, cauda equinasendromu veya daha da seyrek olarak radiküler semptom-lar ile belirti verebilirler. Burada bel a¤r›s›n›n sol baca¤›nayay›lmas› flikayetiyle baflvuran bir lumbar spinal kolon kon-droma olgusu sunulmufltur. Bu olgularda lezyonun preope-ratif de¤erlendirilmesi dikkatli yap›lmal›, major nörolojik ha-sar geliflmeden önce kitlenin eksizyonu yap›lmal› ve lezyo-nun malin transformasyon gösterme potansiyeli nedeniylelezyonun histopatolojik de¤erlendirmesi yap›lmal›d›r.
Anahtar kelimeler: kondroma, lumbar vertebra, radikülo-pati
G‹R‹fiKondromalar s›k rastlanan k›k›rdak kaynakl› benign ke-
mik tümörleri olup genellikle el ve ayaklar›n uzun kemikleriile daha seyrek olarak kaburgalar ve pelviste lokalize olurlar.Spinal yerleflimli kondromalar ise oldukça nadirdir ve tümkondromalar›n yaklafl›k %3’ü ile spinal tümörlerin yaklafl›k%2’sini olufltururlar (1). Omurgan›n herhangi bir noktas›n-dan köken alabilirler ve klinik olarak lokal kitle, lokal a¤r›,kord bas›s› semptomlar›, cauda equina sendromu veya da-ha da seyrek olarak radiküler semptomlar ile belirti verebilir-ler. Özellikle lumbar bölgede disk hernisi veya spinal stenozbulgular› ile ortaya ç›kabilen kondromalar, histolojik olarakküçük bölgelerde malignite gösterebildiklerinden ay›r›c› ta-n›da hat›rlanmal›d›r (2). Biz de bel ve bacak a¤r›s› ile ortayaç›kan ve radyolojik olarak osteoartrotik de¤ifliklik olarak de-¤erlendirilen bir spinal kondroma olgusunu bildiriyoruz.
ABSTRACTAlthough chondromas are common benign cartilagi-
nous bone tumors, spinal chondromas are very unusual.However, spinal chondromas may present with local mass,local pain, spinal cord compression symptoms, caudaequina syndrome; they also present with radicular symp-toms rarely. Here, a patient with the chief complaint: pro-gressive low back pain radiating left leg, is presented as acase of lumbar spinal chondroma. In this kind of cases;preoperative evaluation of the lesion must be done careful-ly, total excision of the lesion must be done before neuro-logical damages develop, and also histopathological stud-ies must be done because of a potential risk of maligntransformation as a cardinal importance.
Key words: chondroma, lumbar vertebrae, radiculopathy
OLGU66 yafl›nda kad›n hasta yaklafl›k bir y›ld›r devam eden
bel a¤r›s›n›n son bir ayd›r sol baca¤›na yay›lmas› ve analje-zik tedaviye yeterli yan›t al›namamas› flikayeti ile baflvurdu.L3 dermatomuna uyan hipoestezi d›fl›nda nörolojik muaye-nesinde baflka bir özellik saptanmad›. Lumbar spinal MR;L2-3 seviyesinde dural keseye sol posterolateralden bas›oluflturan faset eklemde osteoartrozik de¤iflikliklere sekon-der osseöz tüberkül olarak de¤erlendirildi (fiekil 1, fiekil 2).Hasta operasyona al›narak sol L2 hemiparsiyel laminektomiile sol L2-3 faset eklem medialinden kaynakland›¤› izlenimiveren sar›ms› beyaz renkli kitleye ulafl›ld› ve kitle total ola-rak ç›kar›ld› (fiekil 3). Lezyonun histopatolojik incelemesin-de mavi-gri renkli prolifere kondrosit lobülleri izlendi ve ke-sin tan› kondroma olarak rapor edildi (fiekil 4). Operasyonsonras›nda hastan›n yak›nmalar›n›n geriledi¤i görüldü.
Radikülopati ile prezente olan lumbarspinal kondroma: Olgu sunumu
Lumbar spinal chondroma presentedwith radiculopathy: A case report
Dr. Alper Karao¤lan / T.C.Maltepe Üniversitesi T›p Fakültesi Nöroflirürji Anabilim Dal›, ‹stanbulDr. Bilal Kelten / T.C.Maltepe Üniversitesi T›p Fakültesi Nöroflirürji Anabilim Dal›, ‹stanbulDr. Osman Akdemir / T.C. Taksim E¤itim ve Araflt›rma Hastanesi, Nöroflirürji Klini¤i, ‹stanbulDr. Mehmet Alpay Çal / T.C.Maltepe Üniversitesi T›p Fakültesi Nöroflirürji Anabilim Dal›, ‹stanbul
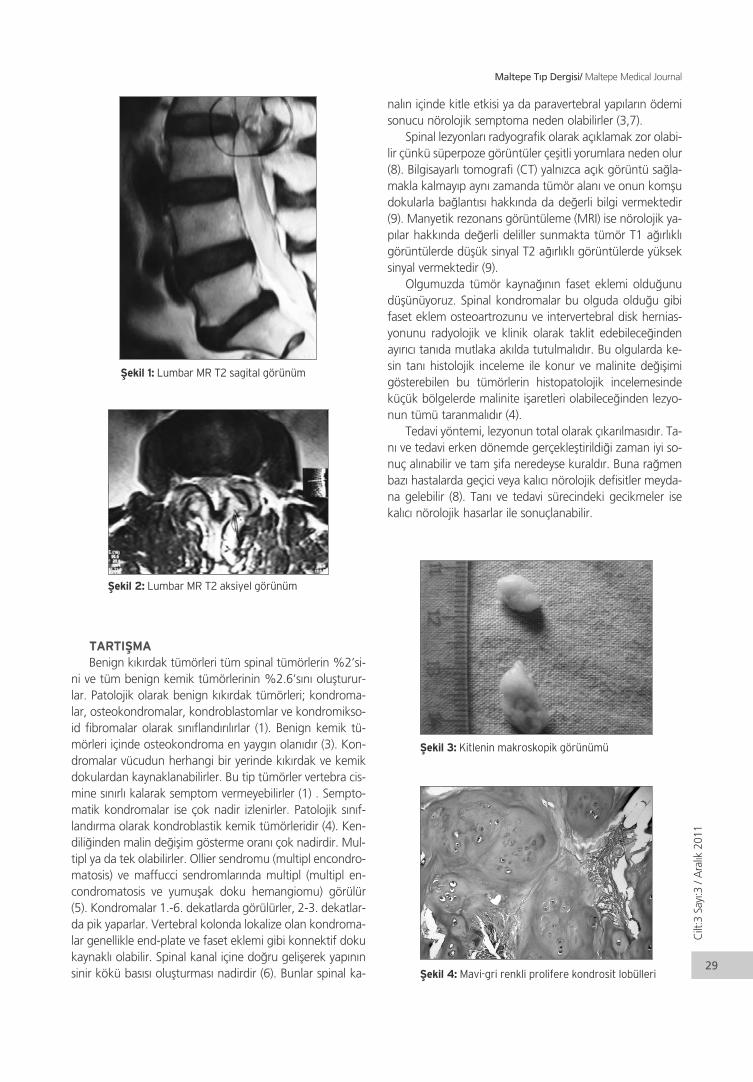
TARTIfiMABenign k›k›rdak tümörleri tüm spinal tümörlerin %2’si-
ni ve tüm benign kemik tümörlerinin %2.6’s›n› oluflturur-lar. Patolojik olarak benign k›k›rdak tümörleri; kondroma-lar, osteokondromalar, kondroblastomlar ve kondromikso-id fibromalar olarak s›n›fland›r›l›rlar (1). Benign kemik tü-mörleri içinde osteokondroma en yayg›n olan›d›r (3). Kon-dromalar vücudun herhangi bir yerinde k›k›rdak ve kemikdokulardan kaynaklanabilirler. Bu tip tümörler vertebra cis-mine s›n›rl› kalarak semptom vermeyebilirler (1) . Sempto-matik kondromalar ise çok nadir izlenirler. Patolojik s›n›f-land›rma olarak kondroblastik kemik tümörleridir (4). Ken-dili¤inden malin de¤iflim gösterme oran› çok nadirdir. Mul-tipl ya da tek olabilirler. Ollier sendromu (multipl encondro-matosis) ve maffucci sendromlar›nda multipl (multipl en-condromatosis ve yumuflak doku hemangiomu) görülür(5). Kondromalar 1.-6. dekatlarda görülürler, 2-3. dekatlar-da pik yaparlar. Vertebral kolonda lokalize olan kondroma-lar genellikle end-plate ve faset eklemi gibi konnektif dokukaynakl› olabilir. Spinal kanal içine do¤ru geliflerek yap›n›nsinir kökü bas›s› oluflturmas› nadirdir (6). Bunlar spinal ka-
nal›n içinde kitle etkisi ya da paravertebral yap›lar›n ödemisonucu nörolojik semptoma neden olabilirler (3,7).
Spinal lezyonlar› radyografik olarak aç›klamak zor olabi-lir çünkü süperpoze görüntüler çeflitli yorumlara neden olur(8). Bilgisayarl› tomografi (CT) yaln›zca aç›k görüntü sa¤la-makla kalmay›p ayn› zamanda tümör alan› ve onun komfludokularla ba¤lant›s› hakk›nda da de¤erli bilgi vermektedir(9). Manyetik rezonans görüntüleme (MRI) ise nörolojik ya-p›lar hakk›nda de¤erli deliller sunmakta tümör T1 a¤›rl›kl›görüntülerde düflük sinyal T2 a¤›rl›kl› görüntülerde yükseksinyal vermektedir (9).
Olgumuzda tümör kayna¤›n›n faset eklemi oldu¤unudüflünüyoruz. Spinal kondromalar bu olguda oldu¤u gibifaset eklem osteoartrozunu ve intervertebral disk hernias-yonunu radyolojik ve klinik olarak taklit edebilece¤indenay›r›c› tan›da mutlaka ak›lda tutulmal›d›r. Bu olgularda ke-sin tan› histolojik inceleme ile konur ve malinite de¤iflimigösterebilen bu tümörlerin histopatolojik incelemesindeküçük bölgelerde malinite iflaretleri olabilece¤inden lezyo-nun tümü taranmal›d›r (4).
Tedavi yöntemi, lezyonun total olarak ç›kar›lmas›d›r. Ta-n› ve tedavi erken dönemde gerçeklefltirildi¤i zaman iyi so-nuç al›nabilir ve tam flifa neredeyse kurald›r. Buna ra¤menbaz› hastalarda geçici veya kal›c› nörolojik defisitler meyda-na gelebilir (8). Tan› ve tedavi sürecindeki gecikmeler isekal›c› nörolojik hasarlar ile sonuçlanabilir.
Cilt
:3Sa
y›:3
/ A
ral›k
201
1
Maltepe T›p Dergisi/ Maltepe Medical Journal
29
fiekil 1: Lumbar MR T2 sagital görünüm
fiekil 2: Lumbar MR T2 aksiyel görünüm
fiekil 3: Kitlenin makroskopik görünümü
fiekil 4: Mavi-gri renkli prolifere kondrosit lobülleri

KAYNAKLAR1. Gaetani P, Tancioni F, Merlo P, Villani L, Spanu G,
Baena RR. Spinal chondroma of the lumbar tract: ca-se report. Surgical Neurology. 1996;46(6):534-539.
2. Panelos J, Voulgaris S, Michos E, Doukas M, Charala-bopoulos K, Batistatou A. Chondrosarcoma of thespine: A rare case with unusual presentation. Diag-nostic Pathology. 2006;1:39.
3. Faik A, Filali SM, Lazrak N, El Hassani S, Hajjaj-Hassou-ni N. Spinal cord compression due to vertebral osteoc-hondroma:report of two cases. Joint Bone Spine2005;72:177–179.
4. Camins MB, Jenkins III AL, Singhal A, Perrin RG. Tu-mors of the Vertebral Axis: Benign, Primary Malignantand Metastatic Tumors. In: Winn HR, editor. You-mans Neurological Surgery. 5th Saunders, 2001;4835-4868.
5. Lane J, Cammisa FJ, Glasser D. Benign cartilage tu-mors of the spine. In: Sundaresan N, Schmidek HH,Schiller AL, Rosenthal DI, eds. Tumors of the spine: Di-agnosis and Clinical Management. WB Saunders, PL.1990;146-148.
6. Emanuelson I, Kyllerman M, Roos A. Hereditary mul-tiple exostosis with spinal cord compression in a 13-year-old boy. J Neurol Neurosurg Psychiatry.1994;57:238-239.
7. Scarborough M, Moreau G. Benign cartilage tumors.Ortop Clin North America 1996;27:583-589.
8. Albrecht S, Crutchfield JS, Segal GK. On spinal oste-okondromas. J Neurosurg 1992;77:247-252.
9. Woertler K. Benign bone tumors and tumor-like lesi-ons: value of cross-sectional imaging European Radio-logy 2003;8:1820-1835.
Kar
ao¤l
anve
Ark
adafl
lar›
Maltepe T›p Dergisi/ Maltepe Medical Journal
30

ÖZETGirifl: Fluorokinolonlar 25 y›ldan daha uzun süredir kul-
lan›lmakta olan genifl spektrumlu antibiyotiklerdir. Jeneras-yon say›lar› artt›kça etkinlik spektrumu da artm›flt›r, ancakyan etkilere dikkat etmek gereklidir ve bu ilaçlar gerçek en-dikasyonlar› d›fl›nda kullan›lmamal›d›r. Burada ilaçla iliflkiliyan etkilerin genifl yelpazesini vurgulamak ve antibiyotikle-rin rasyonal kullan›m›na dikkat çekmek üzere bir gemiflok-sasin toksisitesi olgusu sunulmaktad›r.
Olgu sunumu: Burada, nazal polip nedeni ile ameliyathaz›rl›¤› yap›lmakta iken profilaktik olarak gemifloksasine320 mg. tb kullan›m› sonras›nda, yüksek atefl, ›fl›¤a duyar-l›l›k, ciltte makulopapüler döküntüler ve yüksek karaci¤erenzimleri nedeni ile acil servise müracaat eden 33 yafl›ndabir erkek hasta sunulmaktad›r. Yap›lan genifl incelemedebaflka herhangi bir infeksiyöz ya da metabolik neden sap-tanmad›. Hastan›n klinik durumu ilac›n kesilmesinden son-ra, herhangi bir tedavi ifllemi yap›lmaks›z›n kendili¤indentamam› ile düzeldi.
Sonuç: Bu olgu klinisyenlerin antibiyotik kullan›rken nekadar dikkatli olmalar› gerekti¤ini vurgulamaktad›r. Çeflitliinfeksiyon hastal›klar›n›n tedavisi için gemifloksasin ve di-¤er fluorokinolonlar›n kullan›m› giderek artarken artan birdikkat ve kontrol sürdürülmelidir. Zira bu ilaçlar nadir ola-rak bildirilen yan etkilerin olas›l›klar›n› art›rabilmektedir.
INTRODUCTIONQuinolones are chemically obtained synthetic
medications. Starting from the incidental production ofnalidixic acid during synthesis of chloroquin, they havebeen a large family of wide spectrum chemotherapeuticsever since (1). They have a large list of indications fromcommunity acquired pneumonias to nosocomialpneumonias, from complicated urinary system infections
to bone infections and from gastrointestinal infections topelvic infections (2). Because quinolones, especially thenew generation forms, are readily absorbable from thegastrointestinal tract and because the pharmacokinetics ofthe medication is favorable (e.g. rapid elevation to peakserum values, better tissue distribution, longer eliminationtime etc), they are commonly used in daily clinical practice.It is important, however, to be aware of the possible
ABSTRACTIntroduction: Fluoroquinolones are wide spectrum
bactericidal antibiotics being used for over 25 years.Increasing number of generations increased spectrum ofefficacy, but caution is needed for side effects and thesemedications should not be used without true indication.We report with a case a gemifloxacin toxicity to underlinethe wide spectrum of medication-related adverse effectsand to draw attention to rational use of antibiotics.
Case presentation: We report a 33-year-old manpresented with high fever, photosensitivity, maculopapularrash and elevated liver enzymes after prophylactic use ofgemifloxacine 320 mg tablet, in the course of preparationfor surgery for nasal polyp. A thorough diagnosticinvestigation did not reveal any other metabolic orinfectious etiology. His clinical findings resolved completelyafter cessation of the medication without any definitivetreatment.
Conclusion: This case highlights the need for cliniciansto be cautious when using antibiotics. Continued care andcaution is recommended as gemifloxacin and otherfluoroquinolone usage is increasing for various infectiousdiseases, since these medications may increase likelihoodof adverse effects, which are reported infrequently.
Gemifloxacin-associated fever, maculopapularrash and elevated liver enzymes: A case report
Gemifloksasin ile iliflkili atefl, makülopapüler döküntüve karaci¤er enzimleri yüksekli¤i: Olgu sunumu
Gulbuz Sezgin, MD / Maltepe University Departments of Internal MedicineMelahat Cengiz, MD / Maltepe University Departments of Infectious DiseasesOya Uygur-Bayramicli, MD / Maltepe University Departments of GastroenterologyA.Melih Ozel, MD / Maltepe University Departments of Gastroenterology

serious side effects of these commonly used medications,which may cause serious organ injuries.
We report a case of gemifloxacine related macu-lopapular rash accompanied by high fever and elevatedliver enzymes to draw attention to this important clinicalpossibility.
CASE PRESENTATIONA 33-year-old man presented to the emergency
department with facial and corporal rash and fever for twodays. Ten days earlier he had taken prophylacticgemifloxacine tablets 320 for 7 days, in the course ofpreparation for surgery for nasal polyp. Skin rashes andfever occurred right after the cessation of the medicationand he was seen by a physician who prescribedantihistaminic tablets which were not helpful in controllingeither the fever or the rashes two days before his arrival toour hospital. He complained that his rashes increased inthese two days and his fever was 38,3 °C in the emergencyroom. He was admitted to the hospital. His past medicalhistory was non-contributory. Physical examinationrevealed normal findings except for high fever (38,3 °C),high heart rate (124/min) and conjunctival redness.Laboratory findings were also normal except for elevationof alanin aminotranspeptidase (ALT 96 IU/L, range:15-65).Cultures (urine, throat, blood) and viral markers forhepatotropic viruses were negative as were CMV IgM,Coxackie A and B IgM, and Rubeola IgM. The patient wasput on IV fluids and antihistaminics and palliative measuresfor his fever (e.g. lukewarm bath). Next day his feverstarted lowering and his rashes were coalesceing alongwith resolution of conjuctival redness and photosensitivity.On the third day his symptoms were normal and he wasdischarged pending outpatient follow up. His laboratorytests returned to normal the next week after his dischargefrom the hospital with no fever or rashes.
DISCUSSIONA case for gemifloxacin-related rash, photosensitivity
and liver enzyme elevation was consistent with thispatient’s presentation and with treatment initiation. Thesearch for other reasons in this patient revealed no otherprobable cause and the patient did not have any symptomprogression after the cessation of the medication.
Because of its easy use single dose administration andhigh bioavailability (>70%) gemifloxacine has found awide area of usage among medical community dealingwith infectious diseases (2); however increasing usage
brought increased side effects such as gastrointestinalintolerance, hypersensitivity reactions, central nervoussystem reactions etc. (3).
Any kind of antibiotics can lead to medication-relatedfever and fluoroquinolone related fever cases have beenreported (4). Fever in our patient had started right aftermedication usage and no other causative agent have beenrevealed with diagnostic work up and gemifloxacineseemed like the only probable cause. Accompanyingmaculopapular rash is a known adverse effect ofgemifloxacine (5). Ball et al has reported such rash withgemifloxacine without severe eruptions (5). Fever and rashresolved completely without any definitive treatment in afew days. Photosensitivity was a mild symptom and lastedshorter than fever and rash and we believe that thesesymptoms are interrelated.
Pharmacokinetic studies has shown that gemifloxacineis a well tolerated medication and that elevations ALT levelswere reported with use of 600 mg gemifloxacine for 6days (5). This patient used standard dose of the medication(320 mg) for 7 days and elevated ALT level has returned tonormal in a week without any other therapeuticintervention which makes us believe that it is related withthe medication.
CONCLUSIONThis case highlights the need for clinicians to be
cautious when using antibiotics. Continued care andcaution is recommended as gemifloxacin and otherfluoroquinolone usage is increasing for various infectiousdiseases, since these medications may increase likelihoodof adverse effects, which are infrequently reported.
REFERENCES1. Andriole VT: The quinolones: past, present and
future. Clin Infect Dis 2005;41:119-129.2. Von Bambeke FV, Michot JM, von Eldere JV, Tulkens
PM: Quinolones in 2005:an update. Clin MicrobiolInfect 2005; 11: 256-280.
3. Stahlmann R, Lode H: Safety considerations offluoroquinolones in the elderly: an uptake. DrugAging. 2010; 27: 193-209.
4. Smith CR: The adverse effect of fluoroquinolones. JAntimicrob Chemother. 1987;19: 709-712.
5. Ball P, Mandell L, Patou G (eds): A new respiratoryfluoroquinolone, oral gemifloxacin: a safety profile incontext, Int J Antimicrob Agents 2004; 23: 421-429.
Sezg
inve
Ark
adafl
lar›
Maltepe T›p Dergisi/ Maltepe Medical Journal
32
ÖZETTravmatik akut subdural hematom yaflam› tehdit eden
bir durumdur. Akut subdural hematomun birkaç saat için-de spontan rezolüsyonu nadir görülür. Bu olguda travma-tik akut subdural hematomun 5 saat içerisinde h›zl› rezolüs-yonunu iliflkili mekanizmalar eflli¤inde tart›flarak sunduk.
Anahtar kelimeler: akut subdural hematom, bilgisa-yarl› tomografi, h›zl› rezolüsyon
ABSTRACTTraumatic acute subdural hematoma is a life
threatening situation. Spontaneous resolution of acutesubdural hematoma within a few hours is seen rarely. Wepresent a case of rapid resolution of traumatic acutesubdural hematoma with resolution in 5 hours and wediscuss the mechanisims related to the resolution of acutesubdural hematoma.
Key words: acute subdural hematoma, computedtomography, rapid resolution
INTRODUCTIONPosttraumatic acute subdural hematoma is a
neurosurgical emergency condition characterized by %from 60 to 80 mortality rates. Acute subdural hematomas(ASDH) seem to result either from large angularacceleration-deceleration forces that result in rupture ofbridging veins over the cerebral surface or from impact,with distortion and failure of deep draining veins (1).According to the thickness of hematoma and the patient'sneurological status of acute subdural hematomas can betreated conservatively and followed by serial computedtomography (CT) scanning.
Rapid spontaneous resolution of the hematomatreated conservatively has been reported in the few cases(2-7). In the literature the earliest resolution was reportedwithin 3 hours (5).
A case of spontaneous rapid resolution of ASDH whichthe CT scan 5 hours after admission showing resolution ofsubdural hematoma was reported in this study.
CASE REPORTAn 17 year old male sufferred a traumatic head injury
in a traffic accident was transferred to our hospital. Onadmission, he was lethargic, had a Glasgow Coma Score(GCS) score of 14, pupils were isocoric and reacted normallyto light. The CT scan revealed a subdural hematoma with athickness of 6 mm in the right posterior parietal region(Figure 1). There was no cranial fracture.
The follow-up CT was performed 5 hours after the initialCT. The follow-up CT scan showed complete resolution ofacute subdural hematoma (Figure 2).
DISCUSSIONTraumatic acute subdural hematoma is life threatening
condition that requires immediate therapeutic intervention(4,8). spontaneous resolution of traumatic acute subduralhematoma is seen rarely. Because these patients usuallyundergo an operation on an emergency basis (8).
Several possible mechanisms for the spontaneousresolution of hematoma have been proposed (8,9).Dilution and wash out of the hematoma by cerebrospinalfluid due to tearing of the arachnoid membrane (7,10,11),extracranial redistribution of the hematoma through skullfractures (12), compression and redistribution of the
Rapid spontaneous resolution oftraumatic acute subdural hematoma
Travmatik akut subdural hematomunh›zl› spontan rezolüsyonu
Aziz Y›ld›r›m, MD, Specialist in Neurosurgery / Department of Neurosurgery, Bingol State Hospital, Bingol, Turkey;Veysel Burulday, MD, Specialist in Radiology / Department of Radiology, Bingol State Hospital, Bingol, Turkey;Alper Karao¤lan, MD, Assistant Professor in Neurosurgery / Department of Neurosurgery, Maltepe University, School of Medicine, Istanbul, Turkey;Bilal Kelten, MD, Assistant Professor in Neurosurgery / Department of Neurosurgery, Maltepe University, School of Medicine, Istanbul, Turkey;

hematoma by acute brain swelling (13), redistribution ofthe subdural hematoma to the spinal subdural space (14).In addition, the HIV virus that causes acute subduralhematoma due to cerebral atrophy and hematoma withspontaneous resolution has also been reported (15).
Matsuyama et al. reported total disappearance of anacute subdural hematoma with a thickness of a 1.5 cm.They speculated, the absence of cerebral contusion isnecessary for spontaneous resolution of ASDH (5). Lee etal. reported the thickness of subdural hematoma above2.5 cm is an obstacle to total spontaneous resolution ofASDH (8). In our case the thickness of subdural hematomawas 6 mm and we observed complete rapid spontaneousresolution of hematoma.
Several studies have been presented with an even morerapid resolution of ASDH in recent years. Resolution oftraumatic acute subdural hematoma showing an earliestresolution was reported within 3 hours (5). In our case, wepresent this time (time between two CT) within 5 hours.
Case of ASDH (Glasgow Coma Scale (GCS) 11-15, athin hematoma <1 cm, no focal neurologic deficits) can besafely managed non-surgically with close observation andserial scans (3). These cases should be carefully monitoredclinically and radiologically. As we have shown in ourstudy, early spontaneous resolution of traumatic acutesubdural hematomas can be seen.
REFERENCES1. Huang SH, Lee HM, Lin CK, Kwan AL, Hwong SL, Loh
JK. Rapid resolution of infantile acute subduralhematoma: a case report. Kaohsiung J Med Sci 2005;21: 291-294.
2. Tsui EY, Fai Ma K, Cheung YK, Chan JH, Yuen MK.Rapid spontaneous resolution and redistribution ofacute subdural hematoma in a patient with chronicalcoholism: a case report. Eur J Radiol 2000;36: 53-57.
3. K›r›s T, Atabey R, Toplamaoglu H. Rapid resolution ofacute subdural hematoma. Turkish Neurosurgery1997; 7: 24-27.
4. Mirzai H, Yaldiz C, Eminoglu M, Orguc S.Neurological Picture. Ultra fast resolution of acutepost traumatic subdural hematoma. J NeurolNeurosurg Psychiatry 2005; 76: 1738.
5. Matsuyama T, Shimomura T, Okumura Y, Sakaki T.Rapid resolution of symptomatic acute subduralhematoma: case report. Surg Neurol 1997; 48: 193-196.
6. Niikawa S, Sugimoto S, Hattori T, Ohkuma A, KimuraT, Shinoda J, et al. Rapid resolution of acute subduralhematoma: report of four cases. Neurol Med Chir(Tokyo) 1989; 29: 820-824.
7. Duman H, Ziyal ‹M, Turkmenoglu O, Musluman M,Ayd›n Y. Early spontaneous resolution of symptomaticacute subdural hematoma: A childhood case. TürkNöroflirürji Dergisi 2001; 11: 222-225.
8. Lee CH, Kang DH, Hwang SH, Park IS, Jung JM, HanJW. spontaneous rapid reduction of a large acutesubdural hematoma. J Korean Med Sci 2009; 24:1224-1226.
9. Watanabe A, Omata T, Kinouchi H. Rapid reductionof acute subdural hematoma and redistribution ofhematoma. Neurol Med Chir (Tokyo) 2010; 50: 924-927.
Y›ld
›r›m
ve A
rkad
aflla
r›
Maltepe T›p Dergisi/ Maltepe Medical Journal
34
Figure 1: Initial computed tomography (CT) scan showing acutesubdural hematoma in the right posteriorparietal region
Figure 2: Second CT scan 5 hours after admission showingresolution of subdural hematoma in the right posteriorparietalregion
10. Inamasu J, Nakamura Y, Saito R, Kuroshima Y,Mayanagi K, Ohba S, Ichikizaki K. Rapid resolution oftraumatic acute subdural hematoma by redistribution.Am J Emerg Med 2002; 20: 376-377.
11. Polman CH, Gijsbers CJ, Heimans JJ, Ponssen H, ValkJ. Rapid spontaneous resolution of an acute subduralhematoma. Neurosurgery 1986; 19: 446-448.
12. Kundra S, Kundra R. Extracranial redistributioncausing rapid spontaneous resolution of acutesubdural hematoma. Neurol India 2005; 53: 124.
13. Nagao T, Aoki N, Mizutani H, Kitamura K. Acute
subdural hematoma with rapid resolution in infancy:case report. Neorosurgery 1986; 19: 465-467.
14. Bartolotti C, Wang H, Fraser K, Lanzino G. Subacutespinal subdural hematoma after spontaneousresolution of cranial subdural hematoma: causalrelationship or coincidence?: case report. J Neurosurg2004; 100: 372-374.
15. Cohen JE, Eger K, Montero A, Israel Z. Rapidspontaneous resolution of acute subdural hematomaand HIV related cerebral atrophy: case report. SurgNeurol 1998; 50(3): 241-244.
Cilt
:3Sa
y›:3
/ A
ral›k
201
1
Maltepe T›p Dergisi/ Maltepe Medical Journal
35

ÖZETSibutramin fliflmanl›¤›n uzun vadeli tedavisi için kullan›-
lan bir ilaçt›r. Gebelikte sibutramine maruz kalma ile ilgili s›-n›rl› say›da yay›nlanm›fl veri mevcuttur. Bu makalede, gebeoldu¤unun fark›nda olmadan 1-6. gebelik haftalar› aras›n-da 15 mg/gün sibutramine maruz kalan polikistik over sen-dromlu 29 yafl›ndaki Kafkas kökenli kad›n olgu sunulmufl-tur. Gebeye 38. haftada sezaryen yap›lm›fl ve 4150 gr a¤›r-l›¤›nda sa¤l›kl› erkek yeni do¤an dünyaya gelmifltir. Bebekbir sene boyunca takip edilmifl ve bu süre içinde hiçbir kon-jenital anomali ya da geliflimsel bozuklu¤a rastlanmam›flt›r.Polikistik over sendromlu bir kad›nda,fliflmanl›k tedavisi içinsibutraminin kullan›m› s›ras›nda baflar›l› spontan gebelik veolumlu gebelik sonuçlar›n›n sunumu, bu ilaca gebeliktemaruziyetle ilgili s›n›rl› bilgiye katk›da bulunacakt›r.
Anahtar kelimeler: sibutramin; polikistik over sendro-mu; gebelik; sezaryen; fliflmanl›k
INTRODUCTIONThe prevalance of obesity has started to increase
markedly during the last decades and the importance ofobesity has been recognised as a major public healthproblem affecting both the developed and the developingcountries (1). At all ages women are commonly found tohave a higher mean body mass index (BMI) and higherrates of obesity than men (2). Polycystic ovary syndrome
(PCOS) is the most common form of female infertility andassociated with a number of metabolic disturbances.Obesity is encountered in % 30- 70 of PCOS-affectedwomen (3). The world health organization (WHO) acceptsa body mass index (BMI) of 30 kg/m2 or higher as obese.Antiobesity pharmacotherapy is accepted as appropriatefor patients with a BMI of 30 kg/m2 or higher withoutconcomitant risk factors or a BMI of 27- 29. 9 kg/m2 with
ABSTRACTSibutramine is a drug used for long-term management
of obesity. There is limited published data aboutsibutramine exposure during pregnancy. In this article, wepresent a 29-year-old, Caucasian woman with polycysticovary syndrome who exposed to 15 mg/day of sibutramineduring gestational weeks 1- 6 without knowing that shewas pregnant. At 38th weeks, cesarean section wasperformed and a healthy male newborn weighted 4150gram was born. We followed the infant for one year. Nocongenital abnormalities and developmental disorderswere seen during this period. This report of the successfulspontaneous pregnancy and favorable pregnancyoutcomes following the use of sibutramine for obesitymanagement in a woman with polycystic ovary syndromemay contribute to the limited knowledge about theexposure to this drug during pregnancy.
Key words: sibutramine; polycystic ovary syndrome;pregnancy; cesarean section; obesity
Esra Sa¤lam, M.D. Associated Professor / Department of Medical Pharmacology, Maltepe University, ‹stanbulEmine Nur Özdamar, M.D. / Department of Medical Pharmacology, Maltepe University, ‹stanbul‹. Yaman Sa¤lam, M.D., Ph.D. / Medical Genetics Laboratory, Medical Park Göztepe Hospital, Kad›köy, ‹stanbul
Favorable outcomes of pregnancy with useof sibutramine in a woman with polycysticovary syndrome: a case report
Polikistik over sendromu olan bir kad›ndasibutramin kullan›m› ile olumlu gebeliksonuçlar›: bir olgu sunumu

Cilt
:3Sa
y›:3
/ A
ral›k
201
1
Maltepe T›p Dergisi/ Maltepe Medical Journal
37
a major obesity–related comorbidity (eg. hypertension,diabetes) (4). There are only a few kinds of drugs availablefor the treatment of obesity. Sibutramine is a serotoninnorepinephrine reuptake inhibitor that is approved forlong-term management of obesity (5,6). To a smallerdegree sibutramine also inhibits the reuptake of dopamine(5). It is reported that sibutramin in combination withlifestyle modifications result in significant weight reductionin obese patients with PCOS (7).
There is limited published data about sibutramineexposure during pregnancy. ‹n this report, we present apregnant woman who used sibutramin in early pregnancyand her fetal outcomes.
CASE REPORTOur case was a 29-year-old, Caucasian primigravida
who had a cesarean delivery of a healthy male infant oneyear ago. She had some medical problems includingpolycystic ovary syndrome, hypothyroidism and metabolicsyndrome. On physical examination, her calculated bodymass index (BMI) was 32 kg/m2. The patient reportedtaking 15 mg/day of sibutramine for losing weight duringgestational weeks 1- 6, without knowing that she waspregnant. A chest x-ray was taken for check up ingestational week 5th. Her quad screen test in gestationalweek 17th showed increased risk of trisomy 18.Amniocentesis result was normal. Her serial obstetricalultrasounds showed normal fetal growth. At 38th weeks,she delivered a male infant (4150 gr; 51 cm) by cesareansection. The infant had Apgar scores of 9 and 10, at 1 and5 min, respectively. We followed the infant for one year.No congenital abnormalities and developmental disorderswere seen during this period.
DISCUSSIONOrginally developed as an antidepressant, sibutramine
is an orally administered agent for the treatment ofobesity. Sibutramine is a serotonin norepinephrinereuptake inhibitor that induces weight loss by suppressingappetite, enhancing satiety and inducing thermogenesis(8, 9, 10). Sibutramine is usually started at a dose of 10 mgdaily and the dose may be increased up to 15 mg dailyafter 4 weeks in nonresponders (11).
Pharmacotherapy during pregnancy, presents a specialconcern because of potential teratogenic effects of thedrugs. Physiologic changes of pregnancy affect thepharmacokinetics of medications used by pregnant womanand some medications can reach the fetus and cause harm(12). Sibutramine belongs to pregnancy category C, henceits use is not recommended during pregnancy (13). Fromthe studies in rats, there was no evidence of teratogenicityat sibutramine doses of 1, 3 or 10mg/kg/day. Whereas inrabbits maternal toxicity and increased cardiovascularanomalies were found at high doses (13).
There is little published evidence about humanpregnancy outcomes following prenatal exposure tosibutramin (14, 15, 16, 17). Kadioglu et al. (14) reportednormal fetal outcomes of two pregnant women exposedto sibutramine during the first trimester. Einarson et al.(15)observed 10 pregnant women who took sibutramineduring the first trimester of pregnancy. Among these 10women, 7 delivered normal healthy babies, 2 hadspontaneous abortions and 1 had therapeutic abortion. Asubsequent study described two pregnant womenexposed to sibutramine during the second trimester ofpregnancy. Among the two women, one delivered anormal healthy newborn, one had spontaneous abortion(16). Lastly, a study of 52 pregnant women exposed tosibutramine during the first trimester showed no increasein congenital anomalies or adverse pregnancy outcomes(17).
PCOS is a common clinical disorder characterized byovulatory dysfunction, hyperandrogenaemia, rapid LH(GnRH) pulsatility, increased LH concentrations and LH:FSH ratios (18). It has been suggested that psychologicalstress and neurotransmitter levels may be linked to someof the hormonal derangements, including inappropriategonadotropin secretion and elevated adrenal androgenlevels in women with polycystic ovary syndrome (19).Increased prevalance of depression has been found inwomen with PCOS and an assosiation between depressionand insulin resistance and BMI has been observed (20). Ithas been suggested that serotonin has an inhibitory effecton GnRH stimulated LH release (21) and dopamine hasalso been shown to supress serum LH levels (22). Based onthis findings, in this case sibutramine may have increasedthe chance of spontaneous pregnancy by reducing stressand increasing the levels of serotonin and dopamine whichsupress LH release.
This report of the successful spontaneous pregnancyand favorable pregnancy outcomes following the use ofsibutramine in a woman with polycystic ovary syndromemay contribute to the limited knowledge about theexposure to this drug during pregnancy.
REFERENCES1. James WPT.: The epidemiology of obesity: the size of
the problem. J Intern Med 2008; 263: 336–352. 2. Haslam DW, James WPT.: Obesity. Lancet 2005; 366:
1197-1209.3. Vrbikova J, Hainer V.: Obesity and polycystic ovary
syndrome. Obesity Facts 2009;2: 26- 35. 4. Padwal RS, Majumdar SR.: Drug treatments for
obesity: orlistat, sibutramine and rimonabant. Lancet2007; 369: 71-77.
5. Tziomalos K, Krassas GE, Tzotzas T.: The use ofsibutramine in the management of obesity andrelated disorders: An update. Vascular Health and
Risk Management 2009;5: 441- 452.6. Glazer G.: Long term pharmacotherapy of obesity
2000: a review of efficacy and safety. Arch InternMed 2001;161:1814- 1824.
7. Lindholm A, Bixo M, Bjorn I et al.: Effect ofsibutramine on weight reduction in women withpolycystic ovary syndrome: a randomized, double-blind, plasebo-controlled trial. Fertil Steril 2008;89:1221-1228.
8. Luque CA, Rey JA.: The discovery and status ofsibutramine as an anti-obesity drug. Eur J Pharmacol2002;440:119-128.
9. Halford JCG, Harrold JA, Boyland EJ, Lawton CL,Blundell JE.: Serotonergic drugs: effects on appetiteexpression and use for the treatment of obesity.Drugs 2007;67: 27- 55.
10. Halford JCG.: Pharmacotherapy for obesity. Appetite2006;46:6-10.
11. Linne Y, Rossner S.: Pharmacotherapy of obesity.Clinics in Dermatology 2004;22: 319- 24.
12. Sachdeva P, Patel BG, Patel BK.: Drug use inpregnancy; a point to ponder. Indian J Pharm Sci.2009; 71: 1–7.
13. Erkekoglu P, Giray B, Sahin G.: Toxicologicalevaluation of antiobesity drug use during pregnancyand lactation. Hacettepe Medical Journal 2008; 39:121-133
14. Kadioglu M, Ulku C, Yaris F,et al.: Sibutramine use inpregnancy: report of two cases. Birth Defects Res AClin Mol Teratol 2004;70:545-546.
15. Einarson A, Bonari L, Sarkar M, McKenna K, Koren G.:
Exposure to sibutramine during pregnancy: a caseseries. Eur J Obstet Gynecol Reprod Biol 2004; 116:112.
16. Ramzi F, Elias D, Mona S, Zreik TG.: Sibutramine inpregnancy. Eur J Obstet Gynecol Reprod Biol2005;122:243-244.
17. De Santis M, Straface G, Cavaliere AF, Carducci B,Caruso A.: Early first-trimester sibutramine exposure:pregnancy outcome and neonatal follow-up. DrugSafety 2006;29: 255-259.
18. Blank SK, McCartney CR, Marshall JC.: The originsand sequelae of abnormal neuroendocrine function inpolycystic ovary syndrome. Human ReproductionUpdate 2006;12: 351–361.
19. Lobo RA, Granger LR, Paul WL, Goebelsmann U,Mishell DR Jr.: Psychological stress and increases inurinary norepinephrine metabolites, plateletserotonin, and adrenal androgens in women withpolycystic ovary syndrome. Am J Obstet Gynecol1983;145:496-503.
20. Rasgon NL, Rao RC, Hwang S, et al.: Depression inwomen with polycystic ovary syndrome: clinical andbiochemical correlates. Journal of Affective Disorders2003;74: 299–304.
21. Apfelbaum ME.: Effect of serotonin on the basal andgonadotrophin- releasing hormone- induced releaseof luteinizing hormone from rat pituitary glands invitro. Life Sciences 1987;41: 2069-76.
22. Smyte GA.: The role of serotonin and dopamine inhypothalamic-pituitary function. ClinicalEndocrinology 1977; 7: 325-41.
Sa¤l
amve
Ark
adafl
lar›
Maltepe T›p Dergisi/ Maltepe Medical Journal
38

DE
RL
EM
E
Prematürite ve çocukluk ça¤›psikiyatrik bozukluklar›
Prematurity and childhoodpsychiatric disorders
Dr. Gökflin Karaman / Maltepe Üniversitesi T›p Fakültesi Çocuk ve Ergen Ruh Sa¤l›¤› ve Hastal›klar› Anabilim Dal›Dr. Beril Taflk›n / Maltepe Üniversitesi T›p Fakültesi Çocuk ve Ergen Ruh Sa¤l›¤› ve Hastal›klar› Anabilim Dal›Klinik Psikolog Elif Atla / Maltepe Üniversitesi T›p Fakültesi Çocuk ve Ergen Ruh Sa¤l›¤› ve Hastal›klar› Anabilim Dal›
ÖZETPerinatal etkenlerin, çeflitli psikiyatrik bozukluklar›n ge-
lifliminde rolleri olabilece¤i uzun süredir düflünülmektedir.Do¤um a¤›rl›¤› ve gestasyonel yafl azald›kça psikiyatrik bo-zukluklar›n geliflme riskinin artt›¤› ileri sürülmüfltür. Bu göz-den geçirmede erken do¤um ve/veya düflük do¤um a¤›rl›-¤› ile çocukluk ça¤› bafllang›çl› psikiyatrik bozukluklar ara-s›ndaki iliflkinin incelenmesi amaçlanm›flt›r. Bu psikiyatrikbozukluklar içinde, bafllang›c› çocukluk ça¤›na özgü olupen çok çal›fl›lanlar dikkat eksikli¤i - hiperaktivite bozuklu¤u,yayg›n geliflimsel bozukluklar ve emosyonel bozukluklard›r.Erken do¤an ve/veya düflük do¤um a¤›rl›¤› olan bebekler-de dikkat eksikli¤i ve hiperaktivite bozuklu¤unun dikkat ek-sikli¤inin önde geldi¤i alt tipinin geliflme riski daha yüksekbulunmufltur. Yayg›n geliflimsel bozukluklar ve prematüriteiliflkisinin incelendi¤i çal›flmalarda, düflük do¤um a¤›rl›¤›n-dan çok gebelik haftas›na göre beklenen a¤›rl›¤›n alt›ndado¤man›n ve erken do¤umun daha önemli bir risk faktörüoldu¤u sonucuna ulafl›lm›flt›r. Emosyonel bozukluklar ileprematürite iliflkisi ele al›nd›¤›nda, bu grupta özellikle ank-siyete ve depresyonun s›k gözlendi¤i, ayr›ca k›z çocuklar›için artm›fl bir risk bulundu¤u ortaya konmufltur. Sonuçolarak erken ve/veya düflük do¤um a¤›rl›¤› ile çocukluk ça-¤› bafllang›çl› psikiyatrik bozukluklar›n geliflimi aras›nda biriliflki oldu¤u aç›kt›r. Bu bebeklerde biliflsel ve davran›flsal ge-liflimin yak›ndan gözlenmesi ve olas› psikiyatrik bozuklukla-r›n erken dönemde saptanmas› erken müdahale flans›n›artt›racakt›r.
Anahtar kelimeler: prematürite, düflük do¤um a¤›rl›-¤›, psikiyatrik bozukluk, dikkat eksikli¤i ve hiperaktivite bo-zuklu¤u, yayg›n geliflimsel bozukluklar, emosyonel bozuk-luklar.
ABSTRACTPerinatal factors have long been implicated in the
genesis of psychiatric disorders. For many yearsepidemiologic studies have identified preterm birth and lowbirth weight as a significant risk factor for psychiatricdisorders. This review aims to evaluate the relationship ofpreterm birth/low birth weight and the childhoodpsychiatric disorders. The most studied disorders areattention deficit/hyperactivity disorder, pervasive develop-mental disorders and emotional disorders. In regard toattention deficit/hyperactivity disorder research findingsindicate that children with very low birth weight especiallyhave increased risk of attention problems. As for pervasivedevelopmental disorders, preterm birth and being small forgestational age are increased risk factors rather than lowbirth weight. Regarding emotional disorders preterm birthis a risk factor mainly for anxiety and depression and withinthis group it can be claimed that female children are at riskmore than male children. In conclusion it is obvious thatthere is a relationship between preterm birth/ low birthweight and childhood-onset psychiatric disorders.Monitoring the cognitive and behavioral development inthese infants will allow early detection of possiblepsychiatric disorders and increase the chances of earlyintervention.
Key words: prematurity, low birth weight, psychiatricdisorder, attention deficit/hyperactivity disorder, pervasivedevelopmental disorder and emotional disorder.

G‹R‹fiSon y›llarda perinatal bak›ma verilen önemin artmas› ve
yeni do¤an yo¤un bak›m ünitelerinin yayg›nlaflmas› ile bir-likte preterm ve/veya düflük do¤um a¤›rl›kl› bebekler aras›n-da sa¤ kalma oranlar› giderek artmaktad›r. Erken do¤umkavram› 3 kategoriden oluflmaktad›r; erken do¤um (<37hafta, ED), çok erken do¤um (<32 hafta, ÇED) ve afl›r› de-recede erken do¤um (<28 hafta, AED). Düflük do¤um a¤›r-l›¤› da 3 alt s›n›fa ayr›lmaktad›r; düflük do¤um a¤›rl›kl›(<2500gr., DDA), çok düflük do¤um a¤›rl›kl› (<1500 gr.,ÇDDA) ve afl›r› düflük do¤um a¤›rl›kl› (<1000 gr., ADDA).Ayr›ca gebelik haftas›na göre beklenen a¤›rl›¤›n alt›nda do-¤an bebekler (GHDDA) ise ayr› bir grup oluflturmaktad›r (1).
Preterm bebeklerdeki azalan mortalite, beraberinde art-m›fl morbiditeyi getirmifltir (2). Morbidite içerisinde davra-n›flsal sorunlar ve nörobiliflsel ifllevlerdeki bozukluklar ile ilgi-li fark›ndal›k ise artmaktad›r (3,4). Perinatal etkenlerin, fli-zofreni baflta olmak üzere çeflitli psikiyatrik bozukluklar›ngelifliminde rolleri olabilece¤i uzun süredir düflünülmektedir.‹ki binli y›llar›n bafl›nda erken do¤umun ve düflük do¤uma¤›rl›¤›n›n ilerleyen yafllarda psikiyatrik bozukluklar için risketkeni olarak ele al›nmalar› gerekti¤i ortaya konulmufltur (5,6). Yak›n dönemde yap›lm›fl epidemiyolojik bir çal›flmadado¤um a¤›rl›¤› ve gestasyonel yafl azald›kça psikiyatrik bo-zukluklar›n geliflme riskinin artt›¤› bulunmufltur (7).
ÇDDA veya ÇED bebekler aras›nda bu riskin en yüksekoldu¤u gösterilmifltir (4,7,8). Erken do¤um ve düflük do-¤um a¤›rl›¤› ile belirli psikiyatrik bozukluklar aras›ndaki ilifl-ki de çeflitli çal›flmalarla ortaya konmufltur. Bu psikiyatrikbozukluklar içinde, bafllang›c› çocukluk ça¤›na özgü olupen çok çal›fl›lanlar dikkat eksikli¤i - hiperaktivite bozuklu¤u(DEHB) ve yayg›n geliflimsel bozukluklard›r (YGB) (9-13).Çocukluk ça¤›nda gözlenen di¤er psikiyatrik bozukluklar-dan duygu durum bozuklu¤u ve anksiyete bozukluklar› daemosyonel bozukluklar ad› alt›nda incelenmifltir (4).
Bu gözden geçirmede erken do¤um ve/veya düflük do-¤um a¤›rl›¤› ile çocukluk ça¤› bafllang›çl› psikiyatrik bozuk-luklar aras›ndaki iliflkinin incelenmesi amaçlanm›flt›r. Pub-Med, Science Direct ve Türk Psikiyatri Dizini “prematürite,düflük do¤um a¤›rl›¤›, psikiyatrik bozukluk, DEHB, YGB,emosyonel bozukluklar” anahtar kelimeleri ile taranm›flt›r.
D‹KKAT EKS‹KL‹⁄‹ VE H‹PERAKT‹V‹TE BOZUKLU⁄UDEHB dünyada oldu¤u gibi ülkemizde de en s›k rastla-
nan nörogeliflimsel bozukluklardan biridir. Okul ça¤›ndakiçocuklar aras›nda s›kl›¤› %4-12 aras›nda bildirilen DEHB’nin etiyolojisinde genetik etkenlerin önemi bilinmektedir(14-16). ‹kiz ve aile geneti¤i çal›flmalar› DEHB için ortalamakal›t›labilirli¤in %60-94 aras›nda oldu¤unu ortaya koymak-tad›r. Bununla birlikte çevresel etkenlerin de hastal›k gelifli-minde pay› vard›r(17, 18) Bu çevresel etkenler aras›nda ge-liflmekte olan beyni etkileyen perinatal olaylar ayr›ca önem-lidir. DEHB erken do¤anlar ve/veya düflük do¤um a¤›rl›kl›
bebekler aras›nda en s›k rastlanan ve en s›k çal›fl›lm›fl psiki-yatrik bozukluklardand›r (11). Stjernqvis ve ark.’n›n1999’da yapt›klar› AED’li çocuklarla zaman›nda do¤an ço-cuklar›n karfl›laflt›r›ld›¤› çal›flmada DEHB s›kl›¤› AED grubun-da %20, zaman›nda do¤an grupta %8 olarak bulunmufl-tur (p<0.005)(19). Bir baflka çal›flmada Indredavik ve ark.(2004) ÇDDA çocuklar aras›nda DEHB belirtileri s›kl›¤›n›%25, tan› alanlar› %7 olarak bulmufllard›r (9). Johnson veark. (2010) 26 haftadan daha erken do¤an 219 çocuk ilezaman›nda do¤an 152 çocu¤u karfl›laflt›rm›fllard›r AED gru-bunda DEHB tan›s› alanlar›n oran› %11.5 iken kontrol gru-bunda bu oran %2.9’dur (OR=4.3)(20).
ÇDDA ve ADDA çocuklar aras›nda DEHB s›kl›¤› %16-19 aras›nda bildirilmektedir (21-23). Bu oran erken ve çokerken do¤mufl çocuklar aras›nda %9-20 bulunmufltur (24).Afl›r› erken do¤an bebekler aras›nda DEHB görülme oran›ise %17-20 olarak bildirilmektedir (19).
Düflük do¤um a¤›rl›kl› ve/veya erken do¤an çocuklararas›nda DEHB s›kl›¤› artm›fl görülmekle birlikte bu gruptaDEHB belirtilerinin, alt tip s›kl›¤›n›n ve efl tan›l› durumlar›ntoplumsal örneklemlerdeki DEHB’den farkl› olabilece¤inigösteren çal›flmalar da bulunmaktad›r. Indredavik veark.’n›n (2004) yapt›klar› araflt›rmada çok düflük do¤uma¤›rl›kl› 56 çocuk ile 83 sa¤l›kl› çocuk karfl›laflt›r›lm›fl ve ÇDDgrubunda DEHB belirtileri içinde dikkatsizlik skorlar›n›n kon-trol grubuna göre anlaml› düzeyde yüksek oldu¤u saptan-m›flt›r (p<0.001). Bu çal›flmada AED’li çocuklar aras›ndaDEHB dikkat eksikli¤inin önde geldi¤i tipinin kontrol grubu-na göre daha s›k rastland›¤› bulunmufltur. Bileflik ve hiperak-tivite - dürtüselli¤in önde geldi¤i tipler için iki grup aras›ndaanlaml› bir fark bulunmam›flt›r (9). Inredavik ve ark.’n›n2010 y›l›nda 61 çocukla yapt›klar› çal›flmada da benzer so-nuçlar bulunmufltur (25). ADD ‘li bebekler ile yap›lan bir ça-l›flmada bu grupta alt tiplerinden yaln›zca dikkat eksikli¤ininönde geldi¤i tip için riskin artt›¤› gösterilmifltir (20).
YAYGIN GEL‹fi‹MSEL BOZUKLUK VE PREMATÜR‹TEKronik nörogeliflimsel bir bozukluk olan otizm her 2000
çocuktan birinde ve spektrum olarak otizm ise çeflitli arafl-t›rmalara göre her 150-300 çocuktan birinde görülmekte-dir (13,26). Otizmin etiyolojisine iliflkin nörogeliflimsel teoriesas olarak genetik etkenlere odaklanmaktad›r. Di¤er ta-raftan genetik geçiflin %100’ün alt›nda bir oranda olmas›çevresel etkenleri gündeme getirmektedir. Bu etkenler ara-s›nda perinatal risk faktörleri say›labilir(13). Otizmde bir riskfaktörü olarak prematürite ve/veya düflük do¤um a¤›rl›¤›-n›n rolü çeflitli çal›flmalarda araflt›r›lm›flt›r. Williams ve ark.(2008) prematürite ile otizm aras›nda iliflki oldu¤unu orta-ya koymufllard›r (27). Yap›lan iki çal›flmada GHDDA ya daDDA’n›n otizm riskini yaklafl›k 2 kat artt›rd›¤› ortaya kon-mufltur (28, 29).
Düflük do¤um a¤›rl›¤›n›n di¤er obstetrik komplikasyon-lardan ba¤›ms›z bir risk faktörü olarak ele al›nd›¤› befl arafl-
Kar
aman
ve A
rkad
aflla
r›
Maltepe T›p Dergisi/ Maltepe Medical Journal
40

t›rmada bu grupta otizm riskinin artmad›¤› sonucuna ula-fl›lm›flt›r (28-32).
Gestasyonel yafl›n risk faktörü olarak ele al›nd›¤› dörtaraflt›rmadan birinde göreli riskin 35 hafta alt›nda do¤ançocuklar için 2.45 kat daha fazla oldu¤u saptanm›flt›r (32).Hultmann ve ark. (2002) GHDDA bebeklerde otizm riskininartt›¤›n› göstermifllerdir (OR = 2.1) (29). 2005 y›l›nda yap›-lan di¤er bir çal›flmada GHDDA otizm için ba¤›ms›z bir riskfaktörü oldu¤u (göreli risk: 1.28), do¤um a¤›rl›¤›n›n ise ilifl-kili olmad›¤› bulunmufltur (32). Schendel ve ark. 2008’dekiçal›flmalar›nda 2500 gram alt›nda ve 33 haftadan erkendo¤an bebekler aras›nda otizm riskinin 2 kat artt›¤›n› ve buriskin k›z bebekler aras›nda daha yüksek oldu¤unu sapta-m›fllard›r (13). Johnson ve ark. 2010 y›l›nda yapt›klar› çal›fl-mada 219 afl›r› prematüre bebek ile 152 zaman›nda do¤a-n› karfl›laflt›rm›fllard›r. Afl›r› prematüre grupta otizm s›kl›¤›%8 bulunurken zaman›nda do¤anlar aras›nda otizm tan›s›alan çocuk olmam›flt›r (20).
EMOSYONEL BOZUKLUKLARÇocukluk ça¤› psikiyatrik bozukluklar› içerisinde anksi-
yete bozukluklar›na ve ergenlikle birlikte duygu durum bo-zukluklar›na s›kça rastlanmaktad›r (33). Her iki tan› grubu-nun da prematürite ve/veya düflük do¤um a¤›rl›¤› ile iliflkisibirçok çal›flmada araflt›r›lm›flt›r.
Farooqi ve ark. 2006 tarihinde 86 çocukla yapt›¤› arafl-t›rmada afl›r› prematüre çocuklar›n anksiyete, depresyon veiçe kapal›l›k skorlar›n›n kontrole göre artm›fl oldu¤unu sap-tam›fllard›r (34). Düflük do¤um a¤›rl›¤› olan çocuklarla ya-p›lm›fl çal›flmalarda ise benzer flekilde depresyon ve anksi-yete skorlar›n›n kontrole göre daha yüksek oldu¤u sonucu-na ulafl›lm›flt›r. Botting ve ark.’n›n 1997’de 137 çocuklayapt›klar› çal›flmada depresyon ve yayg›n anksiyete skorlar›düflük do¤um a¤›rl›¤› olan çocuklarda daha yüksek bulun-mufltur (35). 2003 y›l›nda 263 çocukla yap›lan bir çal›flma-da afl›r› düflük do¤um a¤›rl›¤› olan çocuklarda depresyonskorlar›n›n daha yüksek oldu¤unu saptam›fllard›r (36). Hackve ark.’n›n 2004 y›l›nda 474 çocukla yapt›klar› çal›flmalar›n-da düflük do¤um a¤›rl›kl› grupta özellikle k›z çocuklar›ndakontrole göre daha yüksek anksiyete ve depresyon skorubulundu¤unu göstermifllerdir (37). Horwood ve ark.’n›n1998’de 1413 çocukla yapt›klar› bir araflt›rmada düflük do-¤um a¤›rl›¤› olan çocuklarda anksiyete ve geri çekilme skor-lar›n›n kontrol grubuna daha yüksek oldu¤u bulunmufltur(38). Spittle ve arkadafllar›n›n 2009 y›l›ndaki 130 haftadanerken do¤an ya da 1.250 gramdan düflük a¤›rl›kl› 88 erkençocukla yapt›klar› çal›flmada, erken do¤an grupta emosyo-nel bozukluklar kontrol grubuna göre daha s›k gözlemlen-mifltir (39). Johnson ve ark. 371 çocukla yapt›klar› çal›flma-da afl›r› düflük do¤um a¤›rl›¤› olan çocuklarda anksiyete bo-zukluklar›n›n kontrole göre 3,5 kat daha yüksek orandabulundu¤unu saptam›fllard›r (20). 2011 y›l›nda yay›nlad›k-lar› bir baflka çal›flmada ise AED’li çocuklar aras›nda emos-yonel bozukluk s›kl›¤›n› %9, zaman›nda do¤an çocuklar
aras›nda ayn› oran› %2 olarak bildirilmifltir (4). Di¤er taraf-tan Indredavik ve Johnson iki ayr› çal›flmada çok düflük do-¤um a¤›rl›¤› olan çocuklarda rastlanan emosyonel bozuk-luklara biliflsel yetersizliklerin efllik etti¤ini göstermifllerdir (9,20).
TARTIfiMA Çocukluk ça¤›nda s›k rastlanan psikiyatrik bozuklukla-
r›n etiyolojisinde genetik faktörlerin önemli rol oynad›¤› bi-linmektedir. Ancak genetik yatk›nl›¤›n yan› s›ra hastal›k ge-liflimine katk›da bulunan çevresel etkenler de bulunmakta-d›r. Bu çevresel etkenler aras›nda perinatal olaylar›n çeflitlipsikiyatrik bozukluklar›n gelifliminde rolleri olabilece¤i dü-flünülmektedir. Psikiyatrik ve geliflimsel problemlerle iliflkiliperinatal risk faktörleri içinde en belirgin olanlar erken do-¤um ve düflük do¤um a¤›rl›¤›d›r. Bu alanda yap›lm›fl çal›fl-malar gözden geçirildi¤inde, çocukluk ça¤›nda bafllayanpsikiyatrik bozukluklar aras›nda en s›k DEHB, YGB ve emos-yonel bozukluklar›n erken do¤um ve/veya düflük do¤uma¤›rl›¤› ile iliflkili oldu¤u görülmektedir. Erken ve/veya düflükdo¤um a¤›rl›kl› do¤an her dört bebekten birinde bafllang›-c› çocukluk ça¤›na özgü olan psikiyatrik bozukluklardan bi-rinin geliflti¤i bildirilmifltir (15).
DEHB bu riskli grupta en s›k görülen çocukluk ça¤› psi-kiyatrik bozuklu¤udur (9,24). Erken do¤an ve/veya düflükdo¤um a¤›rl›¤› olan bebeklerde DEHB’nin dikkat eksikli¤i-nin önde geldi¤i alt tipinin geliflme riski daha yüksek bulun-mufltur (9). Erken ve/veya düflük do¤um a¤›rl›¤› ile do¤ançocuklarda görülen tablo klasik DEHB’den farkl› olarak er-kek predominans›n›n azald›¤›, sosyal iliflkilenme zorluklar›-n›n belirgin oldu¤u, y›k›c› davran›fllar›n bulunmad›¤› ve te-mel olarak çal›flan bellek ve iflleme h›z›yla ilgili sorunlar›n önplanda oldu¤u, özgül klinik bir durum olarak ortaya ç›k-maktad›r (40). Bu farkl› klinik grupta DEHB’ nin gidifli, teda-vi yan›t› ve efl tan›lar aç›s›ndan tan›mlanabilir yeni özellikle-rin olup olmad›¤› ise araflt›r›lmay› bekleyen konulardand›r.
YGB ve prematürite iliflkisinin incelendi¤i çal›flmalarda,düflük do¤um a¤›rl›¤›ndan çok GHDDA ve erken do¤umundaha önemli bir risk faktörü oldu¤u sonucuna ulafl›lm›flt›r(28, 29). Bu ba¤›ms›z bir risk faktörü olabilece¤i gibi, YGB’den sorumlu olan genetik faktörlerle iliflkili obstetrik efl so-runlar da durum için aç›klay›c› olabilir. Bu ayr›m›n daha netyap›labilmesi için YGB deki ad› geçen risk faktörlerine iliflkinileri çal›flmalar›n genetik faktörlerin obstetrik efl sorunlarlailiflkisi de göz önüne al›narak yap›lmas› gerekmektedir.
Emosyonel bozukluklar ile prematürite iliflkisi ele al›nd›-¤›nda, bu grupta özellikle anksiyete ve depresyonun s›kgözlendi¤i, ayr›ca k›z çocuklar› için artm›fl bir risk bulundu-¤u ortaya konmufltur (36, 37). DEHB gibi, emosyonel bo-zukluklar›n da bu popülasyonda özel bir klinik tablo ile or-taya ç›kabilece¤i düflünülmektedir.
Sonuç olarak, erken ve/veya düflük do¤um a¤›rl›¤› ileçocukluk ça¤› bafllang›çl› psikiyatrik bozukluklar›n geliflimiaras›nda bir iliflki oldu¤u aç›kt›r. Bu bebeklerde biliflsel ve
Cilt
:3Sa
y›:3
/ A
ral›k
201
1
Maltepe T›p Dergisi/ Maltepe Medical Journal
41

davran›flsal geliflimin yak›ndan gözlenmesi ve olas› psikiyat-rik bozukluklar›n erken dönemde saptanmas› erken müda-hale flans›n› artt›racakt›r.
KAYNAKLAR1. Xu Y, Filler J. W. Linking assessment and intervention
for developmental/ functional outcomes of prematu-re, lowbirth- weight children. Early Childhood Educa-tion Journal 2005; 32: 6-13.
2. Neyzi O, Ertu¤rul T. ‹nce Z. Pretermlerin fizik özellikle-ri. Pediatri Cilt 2 ‹çinde: 3. bask›. ‹stanbul: Nobel T›pKitapevi; 2002: 326-327.
3. Marlow N. Neurocognitive outcome after very pre-term birth. Arch Dis Child Fetal Neonatal Ed 2004; 89:F224–F228.
4. Johnson S, Marlow N. Preterm Birth and ChildhoodPsychiatric Disorders. Pediatric Research 2011; 69:11R-18R.
5. Bhutta AT, Cleves MA, Casey PH, Cradock MM,Anand KK. Cognitive and behavioral outcomes ofschool-aged children who were born preterm. a ma-tanalysis JAMA 2002; 288:728–737.
6. Aarnoudse-Moens CS, Weisglas-Kuperus N, van Go-udoever JB, Oosterlan J. Meta-analysis of neurobeha-vioural outcomes in very preterm and/or very lowbirth weight children. Pediatrics 2009;124: 717–728.
7. Abel KM, Wicks S, Susser ES, Dalman C, PedersenMG, Mortensen PB, Webb RT. Birth weight, schizop-hrenia, and adult mental disorder: is risk confined tothe smallest babies? Arch Gen Psychiatry 2010; 67:923–930.
8. Gale CR, Martyn CN. Birth weight and later risk ofdepression in a national birth cohort. Br J Psychiatry2004; 184: 28–33.
9. Indredavik MS, Vik T, Heyerdahl S, Kulseng S, FayersP, Brubakk AM. Psychiatric symptoms and disorders inadolescents with low birth weight. Arch Dis Child Fe-tal Neonatal 2004 Ed 89: F445–F450.
10. Linnet KM, Wisborg K, Agerbo E, Secher NJ, ThomsenPH, Henriksen TB. Gestational age, birth weight, andthe risk of hyperkinetic disorder. Arch Dis Child 2006;91: 655–660.
11. Lindström K, Lindblad F, Hjern A. Preterm Birth andAttention-Deficit/Hyperactivity Disorder in Schoolchil-dren. Pediatrics 2011; 127: 858-865.
12. Burd L, Severud R, Kerbeshian J, Klug MG. Prenataland perinatal risk factors for autism. J Perinat Med1999 27: 441–450.
13. Schendel D, Bhasin TK. Birth weight and gestationalage characteristics of children with autism, includinga comparison with other developmental disabilities.Pediatrics 2008 121: 1155–1164.
14. Hechtman L, McGough JJ. Dikkat Eksikli¤i Bozukluk-lar›.In: Kaplan & Sadock’s Comprehensive Textbook
of Psychiatry (Çev: Öner Ö, Aysev A.). Ayd›n H, Boz-kurt A. (Editörler), 8.bask›. Ankara, Günefl T›p Kitabe-vi. 2007; 3183-3205.
15. Öner Ö, Arsev AS. Dikkat Eksikli¤i Hiperaktivite Bo-zuklu¤u. Arsev AS, Taner YI, (editörler). Çocuk ve Er-gen Ruh Sa¤l›¤› ve Hastal›klar›’nda. ‹stanbul, GoldenPrint. 2007; 397-421.
16. Taflk›n B, Dedeo¤lu C, Yazgan Y. Okuldaki DEHB kli-niktekinden farkl› m›? Dikkat eksikli¤i hiperaktivite bo-zuklu¤u alt tipleri ile cinsiyet ve davran›flsal özellikleraras›ndaki iliflkinin klinikd›fl› bir grupta de¤erlendiril-mesi. 21. Ulusal Çocuk ve Ergen Ruh Sa¤l›¤› ve Hasta-l›klar› Kongresi Özet Kitab›; Antalya 2011; 211.
17. Millichap JG. Etiologic classification of attention-defi-cit/hyperactivity disorder. Pediatrics 2008; 121: 358-365.
18. Haberstick BC, Timberlake D, Hopfer CJ, Lessem JM,Ehringer MA, Hewitt JK. Genetic and environmentalcontributions to retrospectively reported DSM-IVchildhood attention deficit hyperactivity disorder.Psychol Med 2008; 38: 1057–1066.
19. Stjernqvist K, Svenningsen NW. Ten-year follow-up ofchildren born before 29 gestational weeks: health,cognitive development, behaviour and school achi-evement. Acta Paediatr 1999 88: 557–562.
20. Johnson S, Hollis C, Hennessy E, Kochhar P, Wolke D,Marlow N. Psychiatric disorders in extremely pretermchildren: Longitudinal finding at age 11 years in theepicure study. J Am Acad Child Adolesc Psychiatry2010 49: 453–463.
21. Szatmari P, Saigal S, Rosembaum P, Campbell D, KingS. Psychiatric disorders at five years among childrenwith birthweights _1000 g: a regional perspective.Dev Med Child Neurol 1990 32: 954–962.
22. Szatmari P, Saigal S, Rosenbaum P, Campbell D.Psychopathology and adaptive functioning amongextremely low birthweight children at eight years ofage. Dev Psychopathol 1993 5: 345–357.
23. Ross G, Lipper EG, Auld PA. Educational status andschool-related abilities of very low birth weight pre-mature children. Pediatrics 1991 88: 1125–1134.
24. Foulder-Hughes LA, Cooke RW. Motor, cognitive,and behavioural disorders in children born very pre-term. Dev Med Child Neurol 2003 45: 97–103.
25. Indredavik MS, Vik T, Evensen AI, Skranes J, TaraldsenG, Brubakk A. Perinatal risk and psychiatric outcomein adolescents born preterm with very low birth we-ight or term small for gestational age. J Dev Behav Pe-diatr 2010; 31: 286–294.
26. Autism and Developmental Disabilities MonitoringNetwork, United States 2006. Prevelance of autismspectrum disorder. In: Surveill Summer Dec 18 2009;58:1-3.
27. Williams K, Helmer M, Duncan GW, Peat JK, Mellis
Kar
aman
ve A
rkad
aflla
r›
Maltepe T›p Dergisi/ Maltepe Medical Journal
42

CM. Perinatal and maternal risk factors for autismspectrum disorders in New South Wales, Australia.Child Care Health Dev 2008 34: 249–256.
28. Eaton WW, Mortensen PB, Thomsen PH, FrydenbergM. Obstetric complications and risk for severe psycho-pathology in childhood. J Autism Dev Disord 2001;31: 279-285.
29. Hultman CM, Sparen P, Cnattingius S. Perinatal riskfactors for infantile autism. Epidemiology 2002; 13:417-423.
30. Croen LA, Grether JK, Selvin S. Descriptive epidemio-logy of autism in a California population: who is atrisk? J Autism Dev Disord 2002; 32: 217-224.
31. Glasson EJ, Bower C, Petterson B, De Klerk N, ChaneyG, Hallmayer JF. Perinatal factors and the develop-ment of autism: a population study. Arch Gen Psychi-atry 2004; 61: 618-627.
32. Larsson HJ, Eaton WW, Madsen KM, et al. Risk factorsfor autism: perinatal factors, parental psychiatric his-tory, and socioeconomic status. Am J Epidemiol 2005;161: 916-928.
33. Costello EJ, Mustillo S, Erkanli A, Keeler G., Agnold A.Prevelance and development of psychiatric disordersin childhood and adolescence. Arch Gen Psychiatry.2003; 60: 837-844.
34. Farooqi A, Hagglof B, Sedin G, Gothefors L, SereniusF. Mental health and social competencies of 10- to12-year-old children born at 23 to 25 weeks of gesta-tion in the: a Swedish national prospective follow-up
study. Pediatrics 2007 120: 118–133.35. Botting N, Powls A, Cooke R, Marlow N. Attention
deficit hyperactivity disorder and other psychiatricoutcomes in very low birthweight children at 12 ye-ars. J Child Psychol Psychiatry 1997; 38: 931–941.
36. Saigal S, Pinelli J, Hoult L, Kim MM, Boyle M. Psycho-pathology and social competencies of adolescentswho were extremely low birth weight. Pediatrics2003; 111: 969 –975.
37. Hack M, Youngstrom EA, Cartar L, Schluchter M, Tay-lor HG, Flannery D, Klein N, Borawski E. Behavioraloutcomes and evidence of psychopathology amongvery low birth weight infants at age 20 years. Pediat-rics 2004; 114: 932–940.
38. Horwood LJ, Mogridge N, Darlow BA. Cognitive edu-cational and behavioral outcomes at 7 to 8 years in anational very low birthweight cohort. Arch Dis ChildNeonatal Ed. 1998; 79: F12–F20.
39. Spittle AJ, Treyvaud K, Doyle LW, Roberts G, Lee KJ,Inder TE, Cheong JL, Hunt RW, Newnham CA, Ander-son PJ. Early emergence of behavior and social-emo-tional problems in very preterm infants. J Am AcadChild Adolesc Psychiatry 2009; 48: 909-918.
40. Diamond A. Attention-deficit disorder (attention-defi-cit/hyperactivity disorder without hyperactivity): a ne-urobiologially and behaviorally distinct disorder fromattention-deficit/hyperactivity disorder (with hyperac-tivity). Dev Psychopathol 2005; 17: 807–825.
Cilt
:3Sa
y›:3
/ A
ral›k
201
1
Maltepe T›p Dergisi/ Maltepe Medical Journal
43
4) Makale ile ilgili yaz›flmalardan sorumlu yazar›nisim, adres ve telefonu numaras›.
5) Makale daha önce bir yerde sunulmufl ise bafll›ksayfas›n›n en alt›nda belirtilmelidir.
b) Özet ve Anahtar KelimelerÖzetler 250 kelimeyi geçmeyecek flekilde k›sa litera-
tür bilgisi, çal›flman›n amac›n›, gereç ve yöntemi, var›lansonuçlar› k›sa ve aç›k bir flekilde belirtilmelidir.
c) Yaz› MetniKlinik ve deneysel araflt›rma yaz›lar› girifl, gereç ve
yöntem, sonuçlar ve tart›flma bölümlerinden oluflturul-mal›d›r.
d) KaynaklarKaynaklar yaz›da kullan›ld›¤› s›rayla numaralanmal›,
dergi isimleri Index Medicus’taki stil ile k›salt›lmal›d›r. Al-t›dan fazla yazar olan makalelerde ilk üç yazar›n ismi ya-z›ld›ktan sonra di¤er isimler ve ark. (et al) k›salt›lmas› ilegönderilmelidir. Dergiler için yazar soyadlar›, adlar›n›n ilkharfleri, makalenin bafll›¤›, derginin ad›, tarih, bölüm sa-y›s› ve sayfa olarak s›ralanmal›d›r.
Örnek: Templeton PA, Coston CI, Zorhouni EA.:Current uses of CT and MR imaging in the stagini of thelung cancer. Radiol Clin North Am 1990, 28: 631- 46.Kitaplar için: Yazar isimleri, bölüm ad›, editör ismi, kitapad›, bas›m, flehir, yay›nevi, tarih ve sayfalar fleklinde s›ra-lanmal›d›r.
Örnek: Winfield HN, Schuersler W. Pelvic Iymphade-necomy. ‹n Claymon RV, Mc Dougo.II EM (eds). Lapa-roscopic Urology, Guolity Medical Publiser, St. Louis,1993, P. 225 – 260.
e) Tablolar, Resimler ve Alt Yaz›larTablolar ayr› sayfalarda k›sa bir bafll›k içerecek flekil-
de metinde bahsedilifl s›ras›na göre numaraland›r›larakhaz›rlanmal›d›r.
Foto¤raflar siyah beyaz ve net kalitede olmal›d›r. Fo-to¤raflar›n arkalar›nda metindeki kullan›l›fl s›ras› ve üstk›sm›n› gösterir bir ok iflareti konulmal›d›r. Resim altyaz›-lar› ayr› bir sayfada aral›kl› yaz›lmal›, resimler ayr› bir zarfiçerisinde gönderilmelidir.
* Yay›nlanan yaz›lar›n sorumlulu¤u yazarlara aittir.Gönderilen yaz›lar iade edilemez.
YAZARLARA B‹LG‹
1) Maltepe T›p Dergisi, sa¤l›k alan›ndaki bilimselaraflt›rmalar, teknolojik geliflmeler, derlemeler, klinik ça-l›flmalar, olgu bildirimleri, bilimsel toplant› özetleri, edi-töre mektuplar, literatür özetleri ve biyografileri yay›nlar.
2) Dergi y›lda 3 say› yay›nlan›r.3) Derginin yaz› dili Türkçe ve ‹ngilizcedir.4) Yay›nlanmak üzere dergiye gönderilen yaz›lar›n
dergiye kabul edildikten sonra her türlü yay›n hakk› der-giye aittir.Yaz›lar yay›n kurulu taraf›ndan incelendiktensonra gerekli görülen düzeltmelerin yap›lmas› için yaza-ra geri gönderilir.Editör ve yay›n kurulu gerekli gördü-¤ünde yaz›lar›n bilimsel dan›flma kurulu taraf›ndan ince-lenmesini isteyebilir.Yaz›lar teslim tarihi göz önüne al›na-rak yay›n kurulunun belirledi¤i s›raya göre yay›nlan›r.
Yaz›m Kurallar›a) Dergiye gönderilen araflt›rmalar ve derlemeler oni-
ki, bilimsel toplant› özetleri on, olgu bildirimleri befl, edi-töre mektuplar, literatür özetleri ve biyografiler ise üçdaktilo sayfas›n› geçmemelidir.
b) Yaz›lar A4, beyaz birinci hamur ka¤›d›n bir yüzü-ne kenarlardan 2.5 cm boflluk kalacak flekilde 2 sat›raral›k olarak daktilo edilmesi, bilgisayar yaz›c›s› kullana-caksa iyi kalite yaz›m modu seçilmelidir.
c) Gönderilen yaz›lar s›ra ile flu bölümlerden oluflma-l›d›r.Bafll›k sayfas›, Türkçe özet ve anahtar kelimeler, in-gilizce özet ve anahtar kelimeler, yaz› metni, kaynaklar,tablolar, resim ve flekiller için alt yaz›. Olgu bildirimlerin-de ise girifl, bafll›k, ingilizce bafll›k, Türkçe özet, ‹nglizceözet, olgu ve olgular›n sunumu, tart›flma ve kaynaklar-dan oluflmal›d›r.
d) Yaz›n›n tamam› 3 kopya olarak kal›n bir zarf için-de katlanmadan gönderilmelidir. Ayr›ca yaz›n›n Micro-soft Word Belgesi olarak kaydedilmifl disket ya da Cd’ side eklenmelidir.
Yaz› Düzenia) Bafll›k sayfas›1) Makalenin Türkçe ve ingilizce bafll›¤›2) Yazarlar›n tafl›d›¤› en yüksek akademik ünvan›,
yazarlar›n aç›k ad› ve ba¤l› bulundu¤u kurum.3) Çal›flman›n yap›ld›¤› kurum veya kurumlar›n ad›.