primary health care principles, terms and concepts
TRANSCRIPT
Primary Health Care
Principles, terms and concepts

Preamble
• “Primary Care”- 1920 in England.LordDawson reported on “First ContactMedical Care and the Promotion ofPrimary Health Centre”.
• In 1962, the term was used in Britain todenote General Practice
• Prior to Alma Ata, nations had one systemor the other of health care delivery
• Nigeria had BHSS in the 70’s
2

Alma-Ata Declaration
• This was adopted at the International
Conference on Primary Health Care
(PHC), Almaty (formerly Alma-Ata),
Kazakhstan (formerly Kazakh Soviet
Socialist Republic), 6–12 September 1978
• It expressed the need for urgent action by
all governments, all health workers, and
the world community to protect and
promote the health of all people3

Alma-Ata Declaration
• It was the first international declaration
underlining the importance of primary
health care
• The primary health care approach has
since then been accepted by member
countries of the World Health Organization
(WHO) as the key to achieving the goal of
"Health For All"
4

Alma Ata USSR 1978 (12/9/78), defined
PHC as
• Essential Health Care based on
• Practical, Scientifically sound, and Socially
acceptable methods and Technology
• made universally accessible to individuals and
families in the community
• through their full participation
• and at a cost that the community and the country
can afford to maintain at every stage of their
development
• in the spirit of self reliance and self determination”5

REASONS FOR A NEW APPROACH
• Gross inequalities exists b/w developed and developing countries and also within countries – leading to inequity
• High cost of technology
• Access problems
• Sustainability of many health interventions in doubt
• Univalent programmes which never translated into a healthy population
6

BHSS in Nigeria
• Objectives:
- Increase access to appropriate health
services by the end of 1975-1980
- Provision of essential services, correction
of imbalance between rural and urban
areas/regions, utilizing lower cadre of staff
capable of accomplishing task
- Prevention and health promotion services
to be integrated with curative services
- Basic Health Units to achieve integration7

BHSS in Nigeria
• Implementation:
- 1 BHU with Four categories of HF
1 comprehensive HF at apex – 50,000 pop.
4 PHC centers – 10,000 pop. each
20 health clinics – 2,000 pop. each
5 mobile clinics – 40,000 pop. each
- States refused to comply because it meant constructing 25 HF in 1LGA
- After about N200 million at the end of 1983, most of the facilities remained uncompleted all over the country 8

Reasons for failure of BHSS• Reliance on unsustainable structures and
equipments
• Poor inter-sectoral collaboration
• Selection based on political expediency
• The training of health personnel were also
institutional based
• Concentrated on provision of health facilities
and training of health workers
• Little attention to community participation & use
of appropriate technology
• Workers integration problems /same reason for
preference of urban posting persists
9

Evolution of PHC in Nigeria
• The global target of Health for All was
declared in 1978 at Alma ata
• Primary health care (PHC) has been
adopted and accepted universally to be
the approach to achieving this lofty goal.
10

History and Conceptualization
of PHC in Nigeria• In Nigeria, primary healthcare was
adopted in the National Health Policy of
1988 (FMOH, 2004) as the cornerstone of
the Nigerian health system as part of efforts
to improve equity in access and utilization
of basic health services.
• Since then, primary health care in
Nigeria has evolved through various
stages of development. 11

History and Conceptualization
of PHC Cont’d• Historically, there were three major attempts at
evolving and sustaining a community and
people oriented health system in Nigeria.
• The first attempt occurred between 1975 and
1980. The fulcrum of this period was the
introduction of the Basic Health Services
Scheme (BHSS).The Basic Health Services
Scheme came into being in 1975 as an integral
part of Nigeria’s Third National Development
Plan (1975 – 79) 12

Second Historical Attempt on
PHC• A second attempt which was led by
• late Professor Olukoye Ransome-Kuti occurred
between 1986 and 1992
• This period was characterized by the
development of model primary health care in
fifty two (52) pilot local government areas all of
which were implementing all eight
components of primary health care.
• A key result of this dispensation was the
attainment of 80% immunization coverage for
fully 13
Third Historical Attempt at PHC
• The National Primary Healthcare
Development Agency (NPHCDA) was
established in 1992 and heralded the third
attempt to make basic healthcare accessible
to the grassroots
• During this period, which spanned through
2001, the Ward Health System (WHS) which
utilizes the electoral ward (with a
representative councilor) as the basic
operational unit for primary health care
delivery was instituted. 14

Definition contd• First level of contact of individuals, the family
and the community with the National Health
System,
• Bringing health-care as close as possible to
where people live and work
15

A model PHC in Nigeria
16

5 universal principles of Primary
Health Care
• Equitable distribution
• Community participation
• Preventive and promotive approach
• Appropriate technology
• A multi-sectoral approach
17

Community Participation
• It is the hallmark of PHC
• It is a process by which individuals and
families assume responsibility for their
own health and those of the community
• It involve identification of needs,
development of strategy to meet identified
needs & strategy for
• implementation, monitoring and evaluation
18

Inter-sectoral Collaboration
• ‘Production’ of health is not something
that the health sector alone can do; it
involves
• efforts/inputs from other sectors including
education, agriculture, livestock, finance,
information, etc
19

Equity
• All primary health care resources and
services should be made accessible and
affordable to all
• Health services must be shared equally
among the people irrespective of their
ability to pay
• At present health services are mainly
concentrated in the major towns & cities
20

Integration of health
programmes
• Various components of primary health
care need to be provided in a coordinated
way and made
• available, to the community, including
referrals.
21

Appropriate Technology
• The technology ( methods of care,
service delivery, procedures and
equipment) should be simple
• and scientifically sound. It should also be
within reach of the individual/community
• This also applies to use of costly
equipment, procedures and techniques
when cheaper, scientifically valid &
acceptable ones are available e.g. ORS22

Components of Primary Health Care
• Immunization against major infectious
diseases
• Prevention and control of locally endemic
and epidemic diseases
• Adequate supply of safe water and basic
sanitation
• Promotion of food supply and proper
nutrition
• Health Education and promotion23

Components of PHC contd
• Maternal and child health care including family
planning
• Appropriate treatment of common diseases and
injuries
• Provision of essential drugs and revolving
system.
• *Dental health care
• *Mental health care
• *Primary eye care
• * Geriatric care 24

Immunization against Major
Infectious diseases• Immunization is the most powerful and
cost-effective means of preventing some
of the deadly diseases of childhood
• The prevention of diseases by
immunization, a conventional public health
measure is today the best known practical,
low-cost community-base way of
protecting children against the major killer
childhood diseases25

Immunization against major
infectious diseases
• Expanded Programme(EPI) now National Program
on Immunization (NPI) has some challenges;
(i) Mobilizing the community so that everyone spreads
the word about immunization.
(ii) Getting the health authorities to ensure constant
availability of vaccines.
(iii) Educating and convincing parents to demand
immunization for their children.
(iv) Motivating mothers to act, to go back repeatedly
until full dose26

Prevention and control of locally
endemic and epidemic diseases
• The prevention and control of locally
endemic and epidemic diseases is an
important aspect of Primary Health Care
• Health for all cannot be achieved unless
positive efforts are made to control the
major communicable and non-
communicable diseases that plague many
developing countries, using appropriate and
affordable ways.27

Prevention and control of locally
Endemic Diseases Cont’d• Major endemic diseases include malaria
infection, viral diseases (yellow fever and lassa
fever), bacterial diseases (cholera, cerebro-
spinal meningitis, typhoid fever. leprosy and
tuberculosis), helminthic infestations
guineaworm,schistosomiasis,onchocercia-sis,
filariasis and loaisis), and sexually transmitted
diseases (HIV/AIDS)
• Some of the diseases often occur as serious
epidemics killing many people, e.g, yellow
fever, lassa fever. cholera and,cerebrospinal
28
Maternal and child health care
including family planning• The aim of maternal and child health
(MCH) services is to reduce to a minimum
the risks of pregnancy and childbirth, as
well as reduce the maternal mortality rate
and childhood mortality rate
• A well-articulated MCH program will as a
matter of necessity include family planning
29

Maternal and Child Heath
including family planning• Family planning has a great potential for
1) reducing maternal mortality by reducing
births that would have occurred among
women in high risk group (old age, high
parity, previously bad obstetric history),
2) reducing unwanted pregnancies that
would have resulted in illegal/unsafe
abortion.
30

Health Education and
Promotion• The process of educating the community on
prevailing health problems and methods of
controlling them is considered by many as the
most important component of primary health
care.
• Information, education and communication
(IEC) activities must lead to a situation where
people not only value good health but know
how to achieve it and what to do individually
and collectively towards achieving good health

Health Education and
Promotion• Health education is central to primary health
care and success in the implementation of the
other components of primary health care
depends mainly on individual and communities
that are:
• (i) adequately informed to recognize their health
problem and to utilize the available health
services and facilities in solving them
• (ii) adequately motivated to feel the need for
additional justified services and to assume
active interest, participation and leadership in
the provision of such services
32

Promotion of Food Supply and
proper nutrition• Nutrition problems constitute the greatest threat
to public health in the world.
• The problem of malnutrition is universal but
most common in Asia, Africa and South
America.
• Food may also be the vehicle of transmission
for many other infectious diseases. These
include typhoid and paratyphoid fever,
shigellosis, streptococcal phyryngitis,
brucellosis, infective hepatitis,amoebiasis,
cholera33

Promotion of Food Supply and
proper nutrition Cont’d• Nutritional rehabilitation is an important aspect
of malnutrition intervention aimed at
rehabilitating malnourished children as quickly
as possible at PHC
• The objective of nutritional rehabilitation has
been expanded beyond mere cheap
convalescence and treatment measures to
include exposure of mothers and the whole
community to farming, household food security,
nutrition and income generation. 34

Provision of essential drugs and
revolving system• The provision of drugs forms an integral part of
overall health delivery primary health care.
• Essential drugs are those drugs that satisfy the
health care needs of the great majority of the
people and which should be available at all
times in adequate amount and appropriate
forms
• They are those basic drugs that must be
available for the treatment of the common
diseases in an area 35
Criteria for selection of essential
drugs1.The drug must be of proven efficiency and
safety.
2. Side effects must be minimal.
3 The quality and availability of dosage form
should be assured
4. The dosage form should have reasonably long
stability under the expected conditions of storage.
5 . Tablets should be preferred to syrups and
solutions because the can keep better.
6.Drugs formulated in single compounds are 36

Basic Requirements for a sound
PHC ( the 8A’s and 4 C’s)
• Appropriateness
– Services provided are essential to meeting
the population’s needs
• Adequacy
– Services provided are proportionate to what is
required by the community
• Affordability
– The cost of the services provided should be
within the means and resources of the
individual and the country 37
Basic Requirements for a sound
PHC ( the 8A’s and 4 C’s)
• Accessibility
– Services provided must be ‘reachable’ (
geographically, economically and culturally)
• Acceptability
– Services provided must elicit adequate
communication between health care providers
and patients and must be trusted by patients
• Availability
– People must be able to obtain the services
they need as at when they need them 38

Basic Requirements for a sound
PHC ( the 8A’s and 4 C’s)
• Assessibility
– People must be able to evaluate the services
that are provided
• Accountability
– It should be possible to review how the
resources have been used to provide services
• Completeness
– Adequate attention should be paid to all
aspects of a medical problem – prevention,
early detection, diagnosis, treatment, follow-
up measures, and necessary rehabilitation39

Basic Requirements for a sound
PHC ( the 8A’s and 4 C’s)
• Comprehensiveness
– Care is provided for all types of health
problems
• Continuity
– The management of patient’s care over time
must be coordinated among providers
• Community full participation
– Beneficiaries of services should be included in
the identification of their health needs and
how to meet such needs. 40
Implementation of PHC in
Nigeria• 1975: Establishment of the National Basic
Health Services Scheme (BHSS)
• 1978: Alma Ata Declaration
• 1985: African Health Ministers’ re-
affirmation to the Alma Ata Declaration
• 1986: Adoption of PHC in Nigeria in 52
LGAs as models ( funded and managed
by FGN)
41

Implementation of PHC in
Nigeria• 1987: Adoption of the Bamako Initiative
by African Health Ministers
• 1988: Launch of Nigeria’s first
comprehensive National Health Policy
based on Primary Health Care
• 1986-90: Establishment of Schools of
Health Technology
• Expansion of PHC to all LGAs
• Achievement of Universal Child
Immunization Target of over 80%42

Implementation of PHC in
Nigeria• 1992: Establishment of the National
Primary Healthcare Development Agency
(NPHCDA)
• 1993: Beginning of the collapse of PHC in
Nigeria
• 1997: Establishment of the National
Programme on Immunization (NPI)
• 2001: Report on Needs Assessment
Survey to Determine the Status of PHC
in Nigeria43

Levels of Health Care
• Primary health care
• Secondary health care
• Tertiary health care
44

Primary Health Care
• The “first” level of contact between the
individual and the health system
• Essential health care (PHC) is provided
• A majority of prevailing health problems
can be satisfactorily managed
• The closest to the people
• Provided by the primary health centers
45

Misconceptions about PHC
• PHC is only of relevance to poor developing countries which
cannot afford modern medical care
• PHC is second best medicine acceptable only to the rural poor
and urban slum dwellers
• PHC is a stopgap solution to be replaced by something better at
a later stage and
• PHC is a separate stand-alone service isolated from the main
health care system.

Secondary Health Care
• More complex problems are dealt with.
• Comprises curative services
• Provided by the district/general hospitals
• The 1st referral level
47
Tertiary Health Care
• Offers specialist care
• Provided by regional/central level
institution
• Provide training programs
48

Referral system
• A process by which a healthcare provider
transfers the responsibility of the patients
management temporarily/permanently to
another health care provider or
professional
• Two-way referral is the desired
– allows for cross-fertilization of ideas, better
interaction and enhances transfer of
knowledge between providers
49

Current status of PHC in Nigeria• Ward Health System: represents the current national
strategy for the delivery of PHC services.
• Utilises the electoral ward from which a representative councillor is elected as the basic operational unit
• Aims of WHS:
- To promote full & active community participation at the grass root level
- To improve access to quality health care and ensure equity
- To promote local initiatives and encourage poverty alleviation activities in the ward
- To reinforce political commitment at grass root level
- To reduce morbidity and mortality especially amongst women and children under five years
50

PHC Under one roof (PHCUOR)
• The PHC under one roof (PHCUOR)
policy was formulated in 2011 to address
the problem of fragmentation in PHC and
ensure the integration of PHC services
under one authority.
• Its impact is yet to be felt on health status
and utilization of PHC in Nigeria since
PHC under one roof became a national
policy only few years ago. 51

PHCUOR Cont’d
• The inability of PHC centers to provide
basic medical services to the Nigerian
population have made both secondary and
tertiary health-care facilities experience an
influx of patients.
• This has had its toll on the secondary and
tertiary levels of care
52

Committees at PHC level
• LG PHC Management Committee
• PHC Technical Committee
• Ward Development Committee
• Village Development Committee
53

PHC Organogram
LGA Chairman
Secretary
Medical Officer of Health/PHCC
APHCC APHCC APHCC APHCC APHCC APHCC
Ward level Coordinators/Station heads
Station heads
Village level coordinators
LGPHC Management committee
PHC Technical Committee
Ward Development Committee
Village Development Committee
DPM Supervisory
councilor for
health
54

Health Manpower at the PHC
• Medical Officer of Health
• Community Health Officer ± midwifery skills
• Public Health Nurse
• CHEW
• JCHEW
• Environmental health Officer/Technician/assistant (EHO/EHA/EHT)
• Pharmacy technicians
• Others: lab technician, record staff, administrative officer &
• Support staff - Health assistants/Health attendant
55

Medical Officer of Health
• 1856: the Association of Metropolitan
Medical Officers of Health.
• Ladipo Oluwole
• 2007: Association of Medical Officers of
Health in Nigeria
Managerial functions
Technical functions
Clinical functions
56

Monitoring and evaluation of
PHC activities• Instrument of evaluation
– Routine reporting systems
– Sentinel reporting system
– Coverage survey
– Outbreak investigation
– Program review
– Cost analysis
– Cold chain & logistic evaluation
57

Indicators for monitoring PHC• Proportion of population with access to
media outlets
• Measurement of adult literacy activities in
the community
• Immunization coverage
• % of deliveries attended by a trained
health worker
• Disease incidence and prevalence,
mortality rate
• Provision & availability of essential drugs58

Indicators for monitoring PHC
• Proportion of pregnant women receiving
ante natal and post natal care
• Proportion of eligible women (15-45 years)
receiving family planning advice or actually
using modern method of family planning
• Percentage of children U5 years below
reference value of weight –for-age
• Number of children U5 year treated with
home made rehydration salt59

Indicators for monitoring PHC
• Percentage of population with safe water
in home or within 200m of portable water
source200 meters of potable
• Percentage of population with adequate
facilities for excreta disposal or living
within 50m of a pit latrine or toilet
• Percentage of population living within 5km
or ½ to 1 hr travel time of a HF
60

Challenges of PHC implementation
• Poor political will
• Funding gaps
• Structural problems of the three –tiered
• Allocative & managerial inefficiencies
• Lack of human resource planning
• Gaps in recruitment of skilled manpower
• Developmental inequalities
• Dearth of human resources especially in rural areas
61

Challenges of PHC implementation
• Poor coordination
• Fragmentation of programmes due to
multiplicity of implementing partners and
development partners
• Lack of clear definition of roles and
responsibilities of the various levels of
government with respect to health in
general
• Corruption/fraud/mismanagement of
resources and lack of accountability &
tranparency 62

Challenges of PHC implementation
• Little attention paid to inter-sectoral
collaboration which is supposed to be one
of the pillars of PHC
• No clearly defined policy on the financing
of PHC services
• Inadequate equipment and poor condition
of infrastructure
• Lack of essential drug supply
63
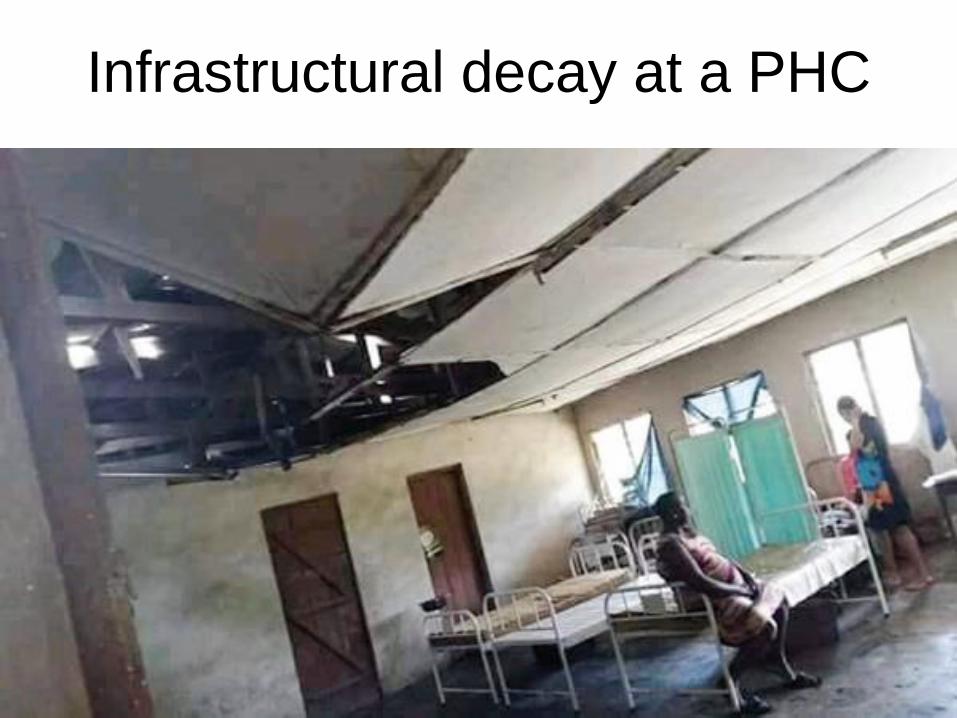
Infrastructural decay at a PHC
64

Infrastructural Decay at a PHC
65

Recommendations
• Government should;
1. Increase political will and provide technical support for PHC implementation
2. Address funding gaps and inequalities
3. Human resource for health development through; recruitment of skilled manpower
4. Ensure transparency and accountability in disbursement of PHC funds
5. Address infrastructure and equipment deficits bedeviling PHCs. 66

References
• Aigbiremolen, A.O., Alenoghena, I., Eboreime,
E., Abejegah, C; Primary Health Care in
Nigeria: From conceptualization to
Implementation; Journal of Medical and Applied
biosciences Vol 6(2)35-43
• Bolaji Samson Aregbeshola and Samina
Mohsin Khan;Primary Health Care in Nigeria:
24 Years after Olikoye Ransome-Kuti’s
Leadership;Front Public Health 2017(5):48
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC
5346888/67

Thank you for your attention
68