prevention of central line associated bloodstream infections (clabs) quality and patient safety...
TRANSCRIPT

Prevention of Central Line Associated Bloodstream Infections (CLABs)
Quality and Patient SafetyEffectiveness and Outcomes
Beth Israel Medical CenterPetrie and Kings Highway Divisions

CLABs Myths
Our infection rates are below national benchmarks - which is good enough.
CLABs are inevitable. It is the price we pay for sophisticated, complex care of severely ill patients.
CLABs are benign and readily treated with antibiotics.
CLABs are a common accompaniment of complex care and covered by outlier payments.

Lessons Learned
We can come surprisingly close to eliminating hospital acquired infections with determination as opposed to resources
Our data must not only be reportable but actionable Save lives Reduce costs Reduce error and waste
How We Did It
Make data actionable Observe variations in work practices Real time problem solving of origins of
CLABs Implement and test practice changes

Make Data Actionable
Start small Use and monitoring of evidence based
patient care practices or “bundles” with reporting back of data to end users
Counter measures generated by the people who do the work Process that generates sustainable fixes Avoid “workarounds” that are constantly
repeated Set a time to achieve goal
Plan-Do-Study Act (PDSA) methodology

Beth Israel Medical Center
Petrie Division Kings Highway Division
94 ICU beds 3,000 discharges
824 non-ICU beds 43,000 discharges
1,200 central lines placed annually 40% of patients in ICU with central line Average length of stay for patients with central line = 5 days Average length of stay for patients with CLAB = 10 days CLABs rate of 9 per 1,000 device days or 3.8% in 2004

Beth Israel Medical CenterCLABs Prevention
June 2005 ICU MICU, SICU
August 2005 CCU and CSICU
December 2005 Emergency Departments
January 2006 General Medical Surgical Units
April 2006 Operating Room
August 2006 NICU and PICU

Multi-disciplinary CLABs Team
MembersPhysicians Chief Medical Officer Associate Chairman, Department
of Medicine Director
ICU, MICU, SICU Emergency Room Medical and Emergency
Department Residency Programs Intensivist Critical Care Fellow
Infection Control Hospital Epidemiologist Manager Practitioner
Patient Care Services Vice President Director Nurse Manager
ICU, MICU, SICU Emergency Room
Nurse Education Manager
Other Director
Materials Management Housekeeping Respiratory Therapy Quality Improvement
Pharmacist Dietician

Multi-disciplinary CLABs TeamPrinciples
It is not good enough that our infection rates are below national benchmarks.
CLABs are preventable, they are not an inevitable consequence of sophisticated, complex care that we provide to our severely ill patients.

Multi-disciplinary CLABs TeamPrinciples
CLABs can be eliminated by determination as opposed to additional resources.
Strict adherence to evidence based patient care practices, called “bundles” that will improve patient safety and reduce adverse patient outcomes is required.

Multi-disciplinary CLABs TeamPrinciples
Patient hospital length of stay, morbidity and mortality can be reduced through prevention of CLABs.
We can reduce the Medical Center’s costs incurred for the care of patients with CLABs.

CLABs
Mortality = 18% ICU risk 8x >non-ICU Additional $40,000 to
hospital costs Hospitals absorb the
costs!
BIMC USA
Patients in ICU with Central Line
40% 48%
CLABs Rate 3.8% 4%
Increase LOS 5 d 14 d
Nationally: 80,000 CLABs in ICUs per year14,500 CLABs deaths

Used BI BSI information and discharge information from 2004
Costs Incurred For Care of Patients with CLABs
Annual Incremental
Costs
Incremental Cost Per
CLAB PatientCLAB
PatientsDischarges
Per Year
94 ICU Beds $960,000$40,000243,000
$1,510,000Total Incremental CLAB Costs
824 Non-ICU Beds
$550,000$25,0002243,000

Multi-disciplinary CLABs TeamAims and Goals
Process that generates sustainable fixes Avoid “workarounds” that are constantly
repeated Collaborative process Knowledge gained from this process is
shared with all Our data must not only be reportable but
actionable

Beth Israel Medical CenterCLABs Prevention
Physician and Nurse reeducation and recertification on central line insertion technique and maintenance practices
Standardization of practices to ensure Maximal barrier protection utilized Skin prep with chlorhexidine Preference for subclavian site unless
medically contraindicated

Beth Israel Medical CenterCLABs Prevention
Nursing empowerment to monitor practices Nursing permitted to ask and stop other
persons who do not follow appropriate practices
Hand hygiene compliance

Beth Israel Medical CenterCLABs Prevention
Daily review of line necessity
Root cause analysis performed in real time for every CLAB
Development of a central line insertion kit Barrier precaution components Insertion components Maintenance components

Beth Israel Medical CenterCLABs PreventionEducation and Recertification
Standardization of Practices and Documentation but also:
Hospital SpecificDepartment SpecificUnit Specific

2005 Infection Control Policyfor Prevention of Intravascular Infection
BETH ISRAEL MEDICAL CENTER INFECTION CONTROL POLICY
MANUAL CODE: SUBJECT: Guidelines for Prevention of Intravascular Infection EFFECTIVE: February 2005 DISTRIBUTION: Nursing Units, Nursing Administration/Education Clinical Department Reviewed Revised 8/05 I. Handwashing
A. Wash hands with soap and water or use alcohol based hand rub solution prior to starting the procedure.
B. Verify the patient’s identity by name and birth, explain the procedure and obtain informed consent.
II. Surveillance for Catheter-Related Infection
A. Palpate the catheter insertion site for tenderness daily through the intact dressing. B. Visually inspect the catheter site if the patient develops tenderness at the insertion
site, fever without obvious source, or symptoms of local or blood stream infection.
III. Barrier Precautions During Catheter Insertion & Care
A. Wear clean gloves when inserting a peripheral venous catheter and during catheter dressing site changes required by the Occupational Safety and Health Administration (OSHA). Bloodborn Pathogens standard. Sterile Gloves are not required.
B. Use sterile technique, including the use of a sterile gown and gloves, a mask, cap,
and a large sterile drape (i.e., maximal barrier precautions) for the insertion of central venous lines including PICCs and guidewire exchanges. Use these precautions, even if the catheter is inserted in the operating room.
C. During central line catheter dressing site care, use a mask and sterile gloves.
IV. Selection of Catheter Insertion Site
DISTRIBUTION All Manual Holders PURPOSE To provide the Registered Nurse with the guidelines for dressing and cap change
on a central venous access device (includes single/double lumen catheters, implanted venous access ports, triple lumen catheters and PICC lines.)
POLICY This procedure may be performed by a Registered Nurse whose competence
has been demonstrated.
Central Venous Access Device dressings are changed at least every 7 days or if they become damp, soiled, loose or if inspection of the site or catheter change is necessary. In addition, dressings on implanted ports must be changed when the non-coring needle is changed once every five days. Caps must be changed whenever the integrity of the cap has been compromised but not less than once a week on Mondays.
EQUIPMENT A Dressing Change Tray (sterile) containing:
powder-free vinyl gloves (one pair) dressing ChloraPrep One-Step Biopatch® chlorhexidine foam pad
towel tape mask (optional) cotton tip applicator (optional)
clean gloves (one pair)
PROCEDURE KEY PONTS 1. Verify the patient’s identity by name
and date of birth.
2. Wash hands and don clean gloves.
3. Carefully remove the old dressing completely and discard.
Touch only the outer layer of the dressing to avoid contamination
4. Inspect the insertion site for color, tenderness, swelling or any discharge.
Look for leakage, swelling. bruising, tenderness, redness and general skin condition. Notify physician of any changes.
5. Remove gloves and wash hands
6. Open the Dressing Change Tray and don the sterile gloves
Strict aseptic technique is essential when carrying out any procedure involving central venous access catheter
7. Prep the skin with ChloraPrep One-Step
a. Pinch the wings on the applicator to break the ampule and release the antiseptic
Do not touch the sponge

Beth Israel Medical CenterCLABs Prevention
Education and Recertification
Indications Anatomy Procedure
“Time Out” Universal Protocol Patient Position Skin Preparation Maximal Barrier Precautions Anesthesia Approach Dressing Additional Expectations
Clean up Monitor for complications
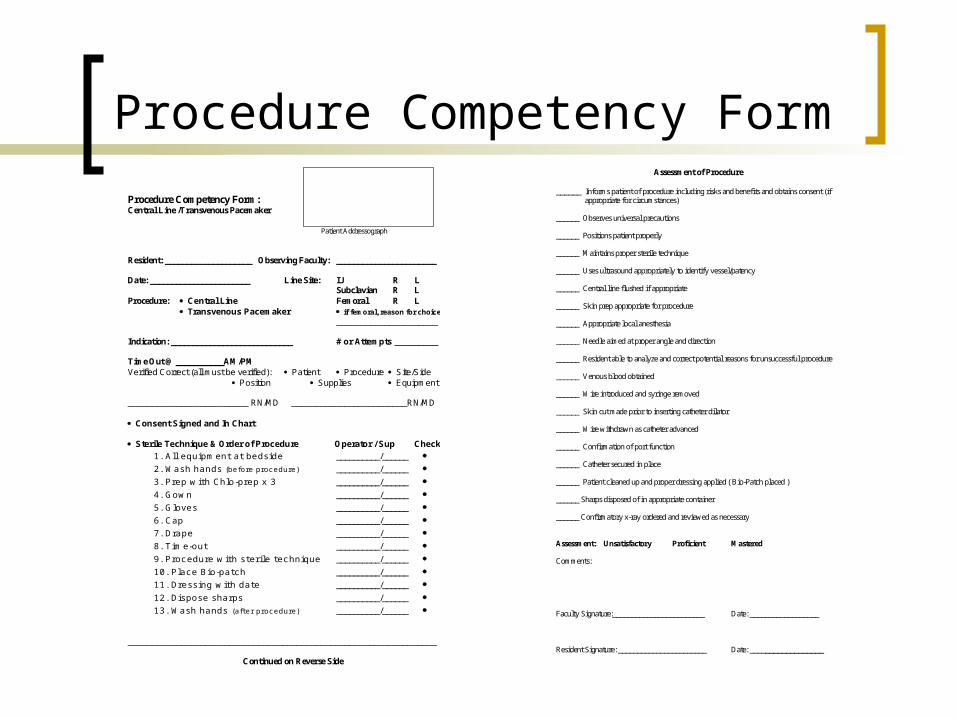
Procedure Competency Form Procedure Competency Form: Central Line /Transvenous Pacemaker Patient Addressograph Resident: ____________________ Observing Faculty: _______________________ Date: _______________________ Line Site: IJ R L
Subclavian R L Procedure: Central Line Femoral R L
Transvenous Pacemaker if femoral, reason for choice _____________________
Indication: ____________________________ # or Attempts _________ Time Out @ ___________AM/PM Verified Correct (all must be verified): Patient Procedure Site/Side
Position Supplies Equipment
_________________________ RN/MD ________________________RN/MD Consent Signed and In Chart Sterile Technique & Order of Procedure Operator / Sup Check
1. All equipment at bedside __________/______
2. Wash hands (before procedure) __________/______
3. Prep with Chlo-prep x 3 __________/______
4. Gown __________/______
5. Gloves __________/______
6. Cap __________/______
7. Drape __________/______
8. Time-out __________/______
9. Procedure with sterile technique __________/______
10. P lace Bio-patch __________/______
11. Dressing with date __________/______
12. Dispose sharps __________/______
13. Wash hands (after procedure) __________/______ ________________________________________________________________
Continued on Reverse Side
Assessment of Procedure
______ Informs patient of procedure including risks and benefits and obtains consent (if appropriate for circumstances)
______ Observes universal precautions ______ Positions patient properly ______ Maintains proper sterile technique ______ Uses ultrasound appropriately to identify vessel/patency ______ Central line flushed if appropriate ______ Skin prep appropriate for procedure ______ Appropriate local anesthesia ______ Needle aimed at proper angle and direction ______ Resident able to analyze and correct potential reasons for unsuccessful procedure ______ Venous blood obtained ______ Wire introduced and syringe removed ______ Skin cut made prior to inserting catheter dilator ______ Wire withdrawn as catheter advanced ______ Confirmation of port function ______ Catheter secured in place ______ Patient cleaned up and proper dressing applied ( Bio-Patch placed ) ______ Sharps disposed of in appropriate container ______ Confirmatory x-ray ordered and reviewed as necessary Assessment: Unsatisfactory Proficient Mastered
Comments:
Faculty Signature:________________________ Date: __________________ Resident Signature: _______________________ Date: __________________
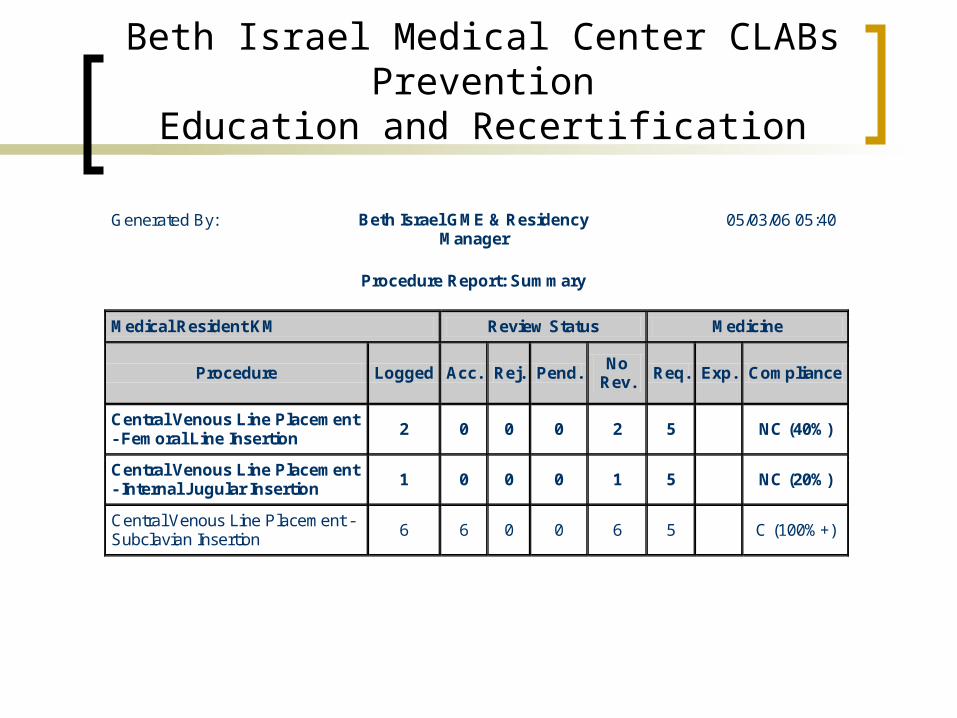
Beth Israel Medical Center CLABs PreventionEducation and Recertification
Generated By: Beth Israel GME & Residency Manager
Procedure Report: Summary
05/03/06 05:40
Medical Resident KM Review Status Medicine
Procedure Logged Acc. Rej. Pend. No
Rev. Req. Exp. Compliance
Central Venous Line Placement - Femoral Line Insertion
2 0 0 0 2 5 NC (40%)
Central Venous Line Placement - Internal Jugular Insertion
1 0 0 0 1 5 NC (20%)
Central Venous Line Placement - Subclavian Insertion
6 6 0 0 6 5 C (100%+)

Beth Israel Medical CenterCLABs PreventionStandardization of Practices
Enforcement of Policy and ProcedureProcedure NoteInsertion KitNursing Empowerment
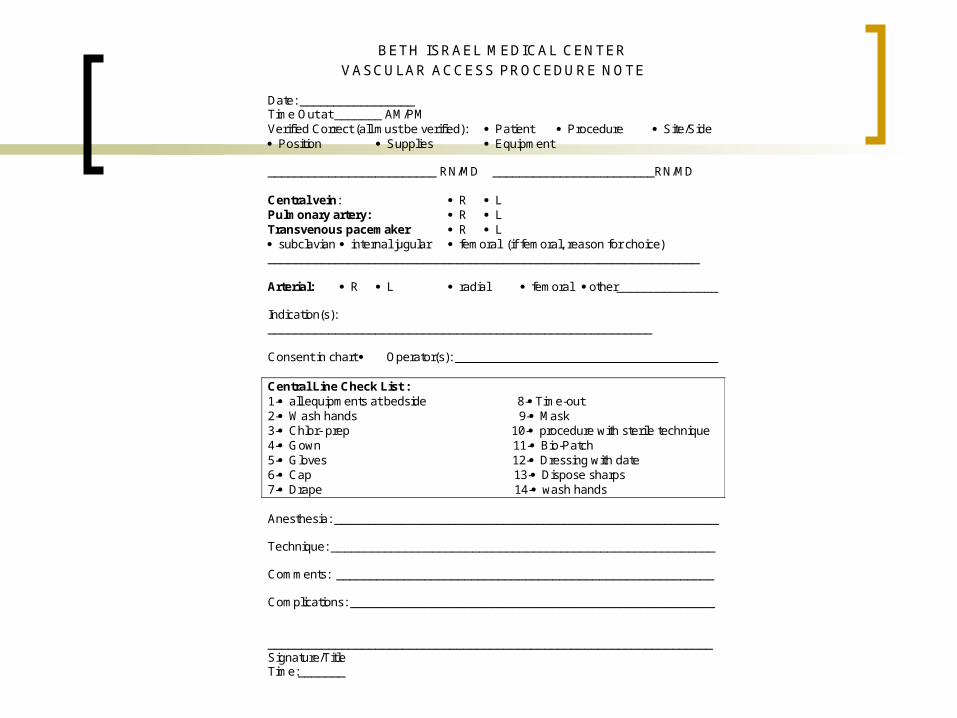
BETH ISRAEL MEDICAL CENTER VASCULAR ACCESS PROCEDURE NOTE
Date: _________________ Time Out at _______ AM/PM Verified Correct (all must be verified): Patient Procedure Site/Side Position Supplies Equipment _________________________ RN/MD ________________________RN/MD Central vein: R L Pulmonary artery: R L Transvenous pacemaker R L subclavian internal jugular femoral (if femoral, reason for choice) ________________________________________________________________ Arterial: R L radial femoral other_______________ Indication(s): _________________________________________________________ Consent in chart Operator(s): _______________________________________ Central Line Check List : 1- all equipments at bedside 8- Time-out 2- Wash hands 9- Mask 3- Chlor- prep 10- procedure with sterile technique 4- Gown 11- Bio-Patch 5- Gloves 12- Dressing with date 6- Cap 13- Dispose sharps 7- Drape 14- wash hands Anesthesia: _________________________________________________________ Technique: _________________________________________________________ Comments: ________________________________________________________ Complications: ______________________________________________________ __________________________________________________________________ Signature/Title Time:_______

Central Line Insertion Kit

Compliance - Central Line Bundle
0102030405060708090
100
Rate (% )
Aug Oct Dec Feb Apr Jun Aug
Time

ResultsData from PDSA Cycles
Number of CLABS
Costs of CLABS
2004 46 $1,510,000
2005 18 $705,000
2006 7 $392,000
2007 2 $112,000
Incremental cost per episode of CLAB ranges from $25,000 to $56,000(CDC data: Burke 2003)

ResultsData from PDSA Cycles
Number of CLABS
Attributable Morbidity
and Mortality
2004 46 9
2005 18 4
2006 7 2
2007 2 0
Attributable morbidity and mortality: 12 – 25%(Wenzel 2001)

ResultsData from PDSA Cycles
Significant reduction in CLABs 95% reduction for institution Achievement of zero CLABs on a variety of units Reduction in morbidity and mortality
Daily review of need for line necessity 20% decrease in central line days
Reduction in costs incurred in caring for patients with CLABs $1,500,000 costs avoided 90% reduction in costs from 2004 Costs to implement
Additional $15 per line inserted Total additional costs $30,000

Beth Israel Medical CenterCLABs Prevention
Unit Longest Duration of Days Without CLAB
CCU 644
ICU 601
ED 547
SICU 483
PICU 396
non-ICU 345
MICU 344
CSICU 300

Beth Israel Medical CenterCLABs Prevention ICUs
0
1
2
3
4
5
2004 2005 2006 2007
Rate
Rate per 1,000 Line Days Rate per 100 Patients

BETH ISRAEL MEDICAL CENTER CLABs Prevention CCU
0
2
4
6
8
10
Q42005
Q12006
Q22006
Q32006
Q42006
Q12007
Q22007
Q32007
YEAR
Rate
per
1,0
00 lin
e d
ays
CCU NHSN NYS

Beth Israel Medical CenterCLABs PreventionRoot Cause Analyses
Within 24 hours of a CLABAll involved patient care staff
4 – 12 personsED, ICU, non-ICU20 – 45 minutesCollaborative, non-punitive process

Beth Israel Medical CenterCLABs PreventionRoot Cause Analyses
Process that generates sustainable fixesAvoid “workarounds” that are constantly repeatedKnowledge gained from this process is shared with all
Beth Israel Medical CenterCLABs Prevention
Root Cause Analysis – August 2005
84 year old female with a history of hypertension, CHF, cardiac arrhythmia with pacer, insulin dependent diabetes
Admitted to ICU with CHF exacerbation, pleural effusion
Developed acute renal failure requiring dialysis Nephrologist places Shiley catheter Groin site chosen Difficult procedure requiring multiple attempts Maximal barrier precautions not fully utilized
Nursing staff attempt to assist Call intensivist to place line
Blood cultures positive for C. albicans 48 hours later

Beth Israel Medical CenterCLABs Prevention
Root Cause Analysis – August 2005
Nephrologist conducts RCA Credentialed Central line indicated Urgent not emergent Supplies available and easily obtainable but not fully
utilized for maximal barrier precautions Need to ask for assistance sooner rather than later
Corrective Actions Central line insertion kit Nursing staff empowered and more comfortable with role Reeducation and recertification of nephrologist

Beth Israel Medical CenterCLABs Prevention
Root Cause Analyses
2005 Central Line Care
Dressings Access
Insertion Practices Maximal barrier precautions Supplies never an issue Certification of physicians
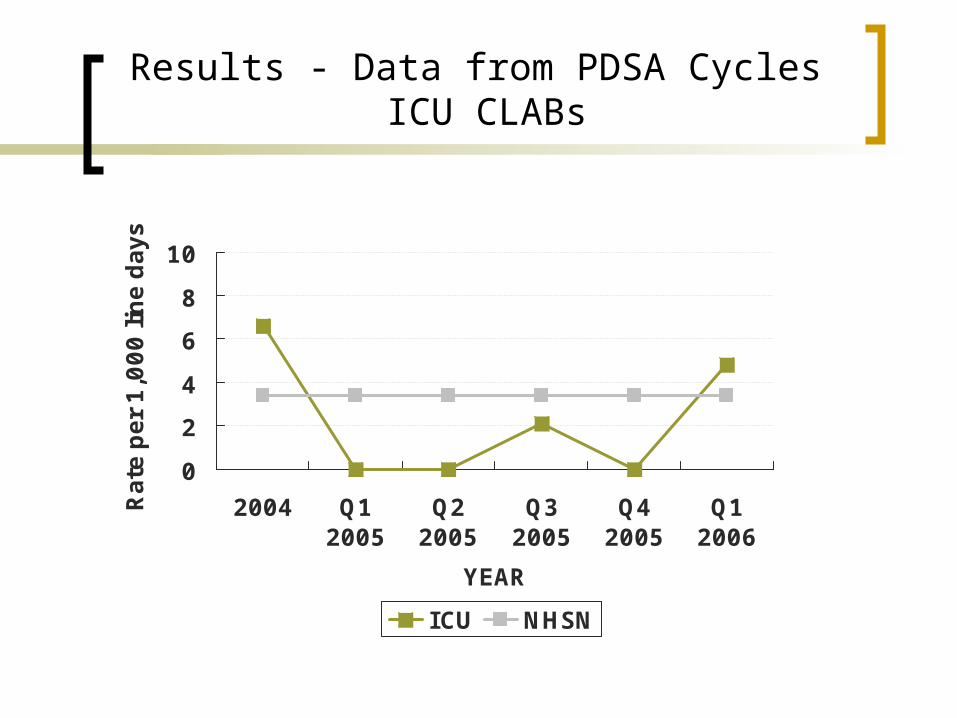
Results - Data from PDSA Cycles ICU CLABs
0
2
4
6
8
10
2004 Q12005
Q22005
Q32005
Q42005
Q12006
YEAR
Rate
per
1,0
00 lin
e d
ays
ICU NHSN

Beth Israel Medical CenterCLABs Prevention
Root Cause Analyses
2006 Central Line Care
Dressings Access
Maintaining the momentum

Results - Data from PDSA Cycles ICU CLABs
0
2
4
6
8
10
2004
Q1 20
05
Q2 20
05
Q3 20
05
Q4 20
05
Q1 20
06
Q2 20
06
Q3 20
06
Q4 20
06
Q1 20
07
Q2 20
07
Q3 20
07
YEAR
Rate
per
1,0
00 lin
e d
ays
ICU NHSN

Beth Israel Medical CenterCLABs Prevention
Use and monitoring of evidence based patient care practices or “bundles” with reporting back of data to end users resulted in the rapid and sustained elimination or decreased incidence of CLABs on many units
Limited additional resources were necessary for the success of this initiative
Efforts were effective for all areas of the hospital where central lines are inserted
As compliance with insertion bundle improves, line maintenance has assumed a greater role in the prevention of CLABs
Culture change regarding goal of zero CLABs infections is applicable for all hospital acquired infections and patient safety issues

GNYHA/UHF CLABs Collaborative
Participating Hospitals• Beth Israel Medical Center• Bronx-Lebanon Hospital Center• Brookdale Hospital Medical Center• Cabrini Medical Center• Good Samaritan Hospital Medical Center• Interfaith Medical Center• Kingsbrook Jewish Medical Center*• Kingston Hospital*• Lenox Hill Hospital• Long Beach Medical Center• Long Island College Hospital• Lutheran Medical Center• Montefiore Medical Center• Mount Sinai Hospital• Mount Sinai Hospital of Queens• New York Downtown Hospital• New York Hospital Queens*• New York Methodist Hospital• New York-Presbyterian Hospital• New York University Medical Center• North General Hospital• Our Lady of Mercy Medical Center
• North Shore-Long Island Jewish Health System, including:
– Forest Hills Hospital– Franklin Hospital– Glen Cove Hospital– Huntington Hospital– Long Island Jewish Medical Center– North Shore University Hospital– Plainview Hospital– Southside Hospital– Staten Island University Hospital– Syosset Hospital
• Peninsula Hospital Center• Richmond University Medical Center*• Sound Shore Medical Center of
Westchester• St. Catherine of Siena Medical• St. Charles Hospital• St. Joseph’s Medical Center, Yonkers*• St. Luke’s - Roosevelt Hospital Center• St. Luke's Cornwall Hospital• St. Vincent’s Medical Center, Manhattan*• Stamford Hospital• The Parkway Hospital*• Trinitas Hospital• Winthrop University Hospital*• Wyckoff Heights Medical Center
*Hospitals that joined the CLABs Collaborative in the second round of participation (i.e., in August/September 2006).

GNYHA-UHF CLABs Collaborative Characteristics of Participating
Hospitals• 38 hospitals participating, 56 ICUs*• At inception of Collaborative, hospital practice was widely variable
across participants:
GREAT OPPORTUNITIES FOR IMPROVEMENT!
Area of Focus Consistently Use Inconsistently Use
Do Not Use
Daily Goals Sheet 21 7 26
Interdisciplinary Rounds 45 9 2
Central Line Bundle 11 27 17
Ventilator Bundle 16 30 10
Responses obtained from ICUs within participating hospitals.
*Note that these were responses from the original group of 38 CLABs Collaborative participating hospitals.

GNYHA-UHF CLABs Collaborative Design
• Systematic model for change that would
– Meet needs of hospitals within the region
– Use existing staffing and financial resources

GNYHA/UHF CLABs Collaborative Design
• Hospital leadership involvement and commitment• Interdisciplinary teams / Physician and Nurse champions• Evidence-based interventions: Implemented “Central Line Bundle”• 3 learning sessions: Reviewed key interventions for eliminating CLAB infections,
guidelines for inserting central line, materials needed, maintaining central lines, hospital best practices, and approaches to sustaining improvements.
• Bi-weekly conference calls: Shared information / tools specific to reducing CLAB infections.
• Collaborative web site for information-sharing: http://jeny.ipro.org/clabs • “Expert on Call” clinical consultant• Reinforcement of “zero tolerance” for CLAB infections• Standardized Materials: Teams developed and used standardized data collection
and definitions• Root Cause Analysis (RCA): Real time RCAs encouraged to identify reasons for
CLABs and develop solutions for prevention • Tracking Success: Aggregate and hospital-specific results reported monthly and
site visits made by Collaborative sponsors to identify areas in need of support
Central Line Bundle: Hospital teams identified the “central line bundle” as a strategy to prevent infection during central line insertion. Components include: hand hygiene, use of maximal barrier precautions,
chlorhexidine skin use, site of line placement, and review of line necessity. All necessary supplies should be available at the patient’s bedside when needed (creation of central line insertion kit).


Examples of Findings fromRoot Cause Analyses
Central Line–Associated Bloodstream Infection
Lack of Education and Staffing
Line Maintenance
Technique not adequate
Line not changed on timely basis
Dressing not changed using aseptic techniques
IV tubing not labeled properly to change
Line not manipulated appropriately
Line in for too long
Not compliant with hand hygiene
Line inserted w/o sterile technique
Inadequate use of maximal barrier precautions
Inadequate prep before insertion
Femoral line chosen instead of subclavian
Inexperienced residents and clinicians
Clinicians not knowledgeable about Central Line Bundle
Nurses do not properly know how to change dressings
MD does not get someone to assist with line insertion
Nurses too busy to check & change dressings

Barriers and Solutions
Barrier Solution
Development of central line insertion & maintenance kits
Creation of monitoring tools to assurecompliance with bundle componentsEmpowerment of nursing staff to stopprocedure when bundle not followed
Development of Department/Hospital-wideeducational programs re: insertion and maintenance
Lack of Education & Staffing
Daily rounds to assess line necessity and assure appropriate maintenance
Lack of Compliance•Maintenance•Technique
Reorganization of staffing to monitor and assure compliance
Creation of protocols in which nursing signs off on dressing rounds
Lack of Standardized Data Collection
Adoption of CDC’s NHSN definitions
Monthly data fed back (CLAB infection rates) to participating hospitals and staff

GNYHA-UHF Collaborative 15-Month Data Results*
Bundle Implementation1: • 88% reported full implementation; remaining 12% in process of fully implementing • Mean pre-bundle implementation CLAB infection rate = 4.02 infections / 1,000
central line days• Mean post-bundle implementation rate = 1.79 infections / 1,000 (p Value <0.0001)Overall Aggregate CLAB Infection Data: • Mean baseline rate = 4.86 infections / 1,000 central line days• Mean fifteen-month study period2 infection rate = 2.38 infections / 1,000• 51% overall decrease (p Value <0.0001)Comparison of CLAB Infection Data in 3-month Cohorts during 15-
month Study Period2: • Mean first three months (July through September 2005) = 3.10 infections / 1,000
central line days• Mean last three months (July through September 2006) = 1.76 infections / 1,000• 43% decrease during the course of the study period (p Value = 0.015)Maintaining Zero CLAB Infections during 15-month Study Period2: • 29 hospitals (81%) maintained zero for at least 3 months • 8 hospitals (22%) maintained zero during the last 6 months
*Includes data from 36 of the 38 original participating hospitals
Notes:
1 Bundle implementation, reported by 34 of the 38 original participating hospitals through an Interventions Survey developed by Collaborative sponsors, April 2006.
2 Study Period includes data collected by 36 of the 38 original participating hospitals from July 2005 through September 2006.

Monthly ICU Central Line Infection Rates for Hospitals Participatingin the GNYHA/UHF CLABS Quality Improvement Collaborative
Round 1 Hospitals
2.15
1.65
2.272.46
1.681.94 2.02
2.37
1.87
2.442.21
1.33
2.02
1.65
1.80
4.525.01 4.26
3.18
2.55
2.33
2.70
2.47
2.772.69 2.04
0.00
1.00
2.00
3.00
4.00
5.00
6.00
Baseline Jul-05 Sep-05 Nov-05 Jan-06 Mar-06 May-06 Jul-06 Sep-06 Nov-06 Jan-07 Mar-07 May-07
Cen
tral
Lin
e In
fect
ion
s p
er 1
,000
Cen
tral
Lin
e D
ays

Monthly ICU Central Line Infection Rates for Hospitals Participatingin GNYHA/UHF CLABS Quality Improvement Collaborative
Round 2 Hospitals
5.13
2.62 1.88
0.88
4.75
2.45
3.31
1.73
0.68 0.81
0.00
1.00
2.00
3.00
4.00
5.00
6.00
Baseline Oct-06 Nov-06 Dec-06 Jan-07 Feb-07 Mar-07 Apr-07 May-07 Jun-07
Cen
tral
Lin
e In
fect
ion
s p
er 1
,000
Cen
tral
Lin
e D
ays

Decreasing Incidence of MDROs!
BIMC Petrie KHD
MRSA 65% 50%
VRE 15% 25%
MDR Klebsiella 15% 20%
MDR Acinetobacter 45% 50%
C. difficile 10% 35%
Costs avoided: $1.5 million

Thank You