prevention, identification & management of fatigue
TRANSCRIPT

Prevention, Identification & Management of Fatigue
Beyond Duty Hour Restrictions
This presentation is brought to you by:
»Dr. Ed Tagge
»Dr. Mark Reeves
»Dr. Chris Church
WHY SLEEPAre you wasting 1/3 of your life?

Sleep
»Improved alertness
~ Faster reaction times
~ Improved dexterity
»Improved cognitive function
~ Frontal lobe function
~ Better mood modulation
~ Improved Memory
»Improved resistance to stress and immune function
»Decreased obesity, Type 2 diabetes and
atherosclerotic diseases
SLEEP PHYSIOLOGYWhy people get sleep at 3 AM
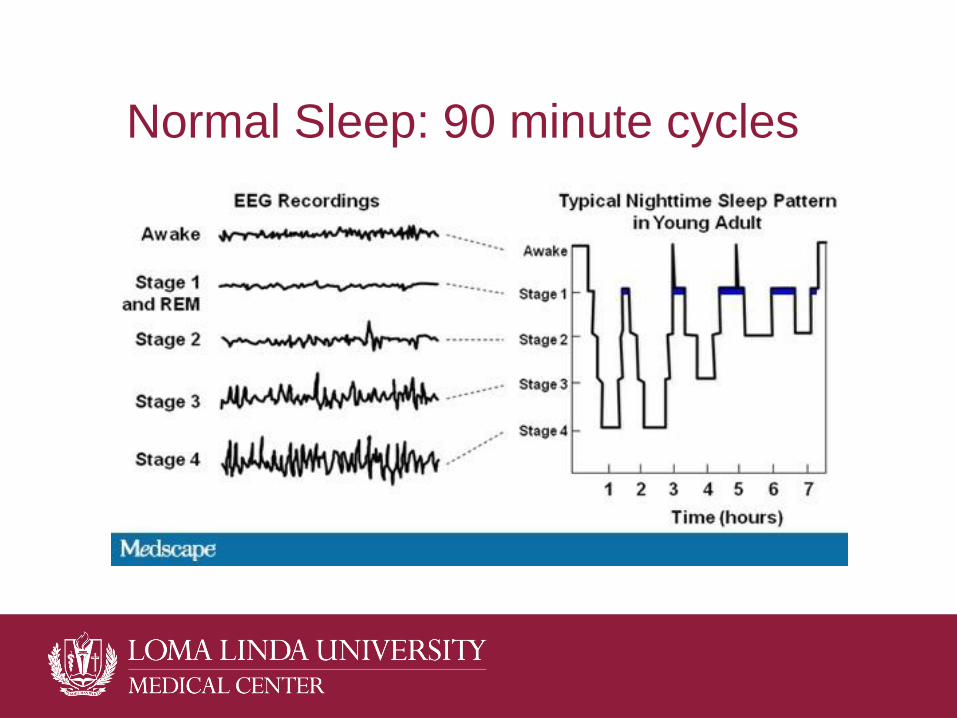
Normal Sleep: 90 minute cycles

To sleep; perchance to REM» Just being asleep is not beneficial
» Restorative sleep MUST include REM
sleep
» All OTC sleep aids, alcohol,
barbiturates, most benzodiazepines,
narcotics and anesthetics (Including
propofol) inhibit REM sleep
» Result in “hung over” or groggy feeling
afterwards
» BTW: Sundowning
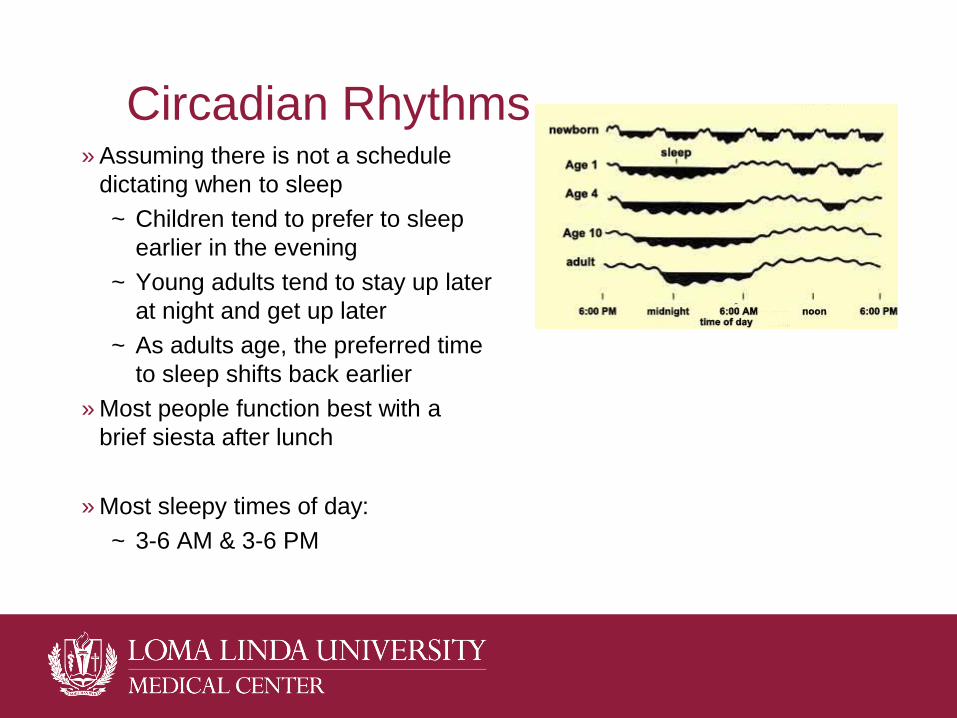
Circadian Rhythms» Assuming there is not a schedule
dictating when to sleep
~ Children tend to prefer to sleep
earlier in the evening
~ Young adults tend to stay up later
at night and get up later
~ As adults age, the preferred time
to sleep shifts back earlier
» Most people function best with a
brief siesta after lunch
» Most sleepy times of day:
~ 3-6 AM & 3-6 PM

MANAGING SLEEP & FATIGUE DURING RESIDENCY
Fatigue Differential Diagnosis
»Too little sleep
»Fragmented sleep
»Circadian rhythm disturbance
»Other conditions that masquerade as fatigue
~ Mood disorder/burnout
~ Hypothyroidism
~ Medications or other substances
»Primary sleep disorders
~ Obstructive sleep apnea
~ Narcolepsy-Cataplexy

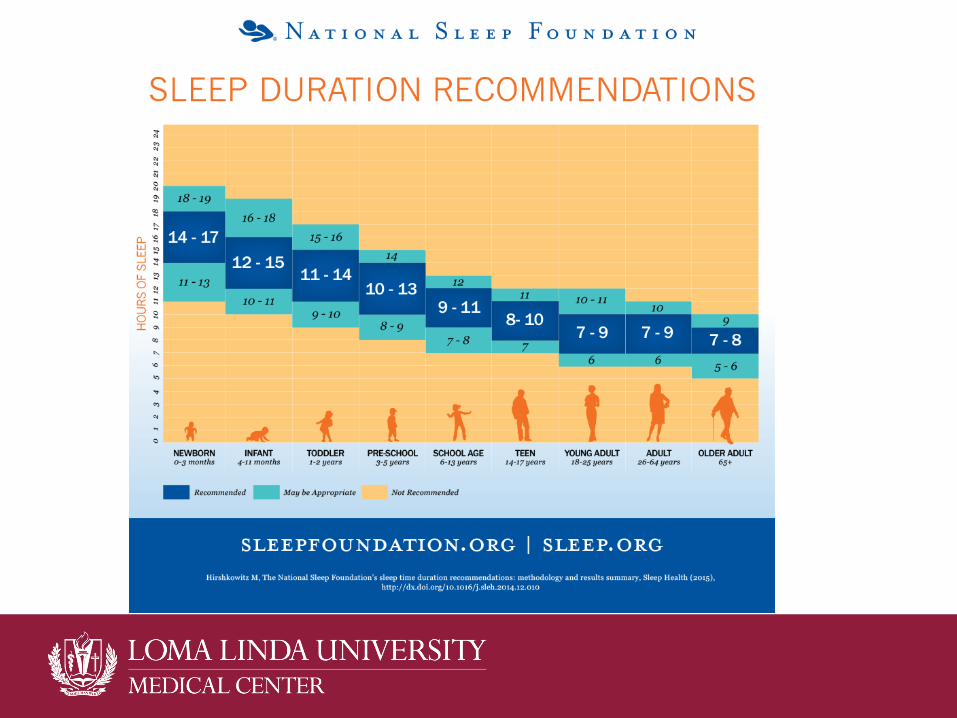
Too Little Sleep
»Most young adults require 7.5 hours of sleep
each night (52 hours per week)
»Impacted by both duty hours and what
physicians do when not on duty
»Shige Okawara, MD
Fragmented Sleep
»Being awakened to disrupt REM sleep also
leads to fatigue
»Knowing you are on-call changes how you sleep
»This occurs with home call as well as in-house
call

Circadian Rhythm Shifts
»Night Float changes sleep patterns like jet lag
»Trying to re-set from daytime waking to
nighttime waking takes days
»Even when well rested prior to a night float shift,
most people will feel sleepy around 3-6 AM

Symptoms of Sleep Deprivation»Boring lectures put you to sleep instead of annoying you
»Yawning
»Inattention
»More microsleeps
»Increased tolerance for risk
»Mood
»Psychomotor slowing
»Decreased cognitive functions & Increased Errors
»MVA
»Under-estimating how sleepy you are
Confusional Arousal
»Increased following sleep deprivation
»Occurs after being asleep for 30 minutes while
in deep (slow wave) sleep
»AKA
~ Sleep inertia
~ Sleep drunkenness
»Symptoms
~ Confusion
~ Amnesia
Assessing Sleepiness
»Acute
~ Reaction time
»Chronic sleep deprivation
~ Do you feel rested after a sleeping?
~ Epworth Sleepiness Scale
http://web.stanford.edu/~dement/epworth.html
David F. Dinges, PhDPsychologist, University of Pennsylvania
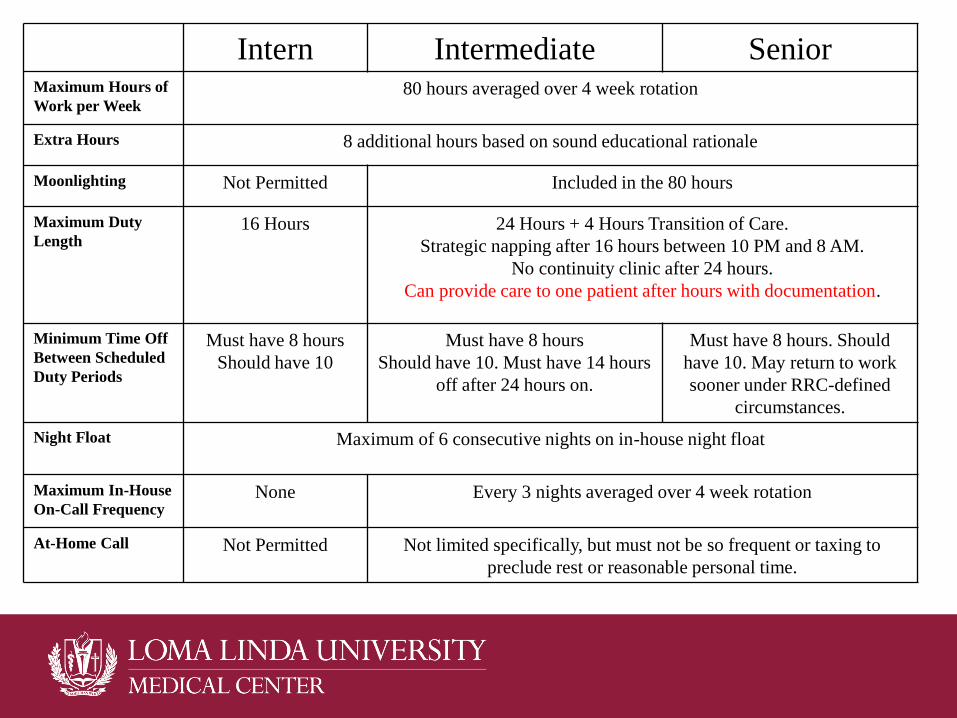
Intern Intermediate SeniorMaximum Hours of
Work per Week80 hours averaged over 4 week rotation
Extra Hours 8 additional hours based on sound educational rationale
Moonlighting Not Permitted Included in the 80 hours
Maximum Duty
Length16 Hours 24 Hours + 4 Hours Transition of Care.
Strategic napping after 16 hours between 10 PM and 8 AM.
No continuity clinic after 24 hours.
Can provide care to one patient after hours with documentation.
Minimum Time Off
Between Scheduled
Duty Periods
Must have 8 hours
Should have 10
Must have 8 hours
Should have 10. Must have 14 hours
off after 24 hours on.
Must have 8 hours. Should
have 10. May return to work
sooner under RRC-defined
circumstances.
Night Float Maximum of 6 consecutive nights on in-house night float
Maximum In-House
On-Call FrequencyNone Every 3 nights averaged over 4 week rotation
At-Home Call Not Permitted Not limited specifically, but must not be so frequent or taxing to
preclude rest or reasonable personal time.
Did Duty Hour Restrictions Improve Patient Safety?» 2004
» 2011

SURVIVAL GUIDE TO DOCTORING AT NIGHT

Maintain Healthy Sleep Habits»Sleep in a cool, dark, quiet room in a comfortable bed.
»Avoid napping > 90 minutes during the day.
»Sleep at the same time each day when possible.
»Avoid large meals, large volumes of liquids, caffeine,
nicotine, and alcohol close to bedtime.
»Exercise in the morning or late afternoon.
~ A relaxing exercise, like yoga, can be done before bed.
»Get exposure to natural light while awake.
»Establish a regular relaxing bedtime routine.
»Associate your bed with sleep. Avoid “tossing & turning”
»Do NOT use sedatives on a regular basis
Fatigue Mitigation - Before
»Be well rested
~ Start night float without sleep debt
»Prior to a night float shift, take a 1 sleep cycle
nap in the afternoon
»Before starting night float, eat a good meal & be
hydrated.
»If you can shift your sleep cycle, postpone sleep
~ Days→Evenings→Night
Fatigue Mitigation - During
»Nap 20-30 minutes early in a night shift
~ set an alarm to avoid a full sleep-cycle nap
»Eat a meal in the middle of the shift
»Stay hydrated
»Work in bright lights
~ especially between 3 AM and 6 AM
»Consider use of caffeine BEFORE getting sleepy
~ Take caffeine just before a nap because the effects of
oral caffeine start 20 minutes after consumption
~ Benefit lasts about 4 hours

Caffeine Dosing Options (mg)
»Average cup of instant coffee (200 ml) 75
»Average cup of brewed coffee (200 ml) 100–250
»Average cup of tea (200 ml) 50
»Herbal tea 0
»Decaffeinated tea or coffee 3–5
»Hot chocolate 5–7
»Coke or Pepsi (regular or diet) 30-45
»Red Bull (250 ml can) 80
»Bar of plain chocolate (50 g) up to 50
»Bar of milk chocolate (50 g) up to 25

Fatigue Mitigation - Afterwards»Avoid driving long distances
~ Especially after a night shift
~ Cab rides OR Loma Linda Inn
~ Use sunglasses
»If possible, go to bed prior to 10 AM
»Sleep in a cool, dark quiet room
~ Eye pads, ear plugs, white noise
~ Avoid interruptions
»Do NOT use alcohol, OTC sedatives, narcotics, or
Propofol to initiate sleep
»When you get the chance, repay sleep debt.

Fatigue Mitigation: Expertise
»David Hinshaw, Sr., MD
»Recognizing when the
unusual is present and
slowing down

Competence in working safely at night
»Patients will get sick between 3 AM and 6 AM
