preventing and managing drug induced anaphylactic shock · anaphylatoxins (c3a, c4a, c5a)...
TRANSCRIPT

1
2013 Joint Conference of Drug Safety Research Centres
In affiliation with the Pacific Rim Association for Clinical Pharmacogenetics (PRACP)
Thomas Y.K. Chan
Division of Clinical Pharmacology
Department of Medicine and Therapeutics, and
Centre for Food and Drug Safety, Faculty of Medicine
The Chinese University of Hong Kong, and
Prince of Wales Hospital Poison Treatment Centre
16 October 2013
Preventing and Managing
Drug Induced Anaphylactic Shock
Using Pharmacogenomics to Improve Drug Safety and Efficacy
Preventing/managing drug induced anaphylaxis
Depend on a good understanding of the pathophysiology
of anaphylaxis, subjects at risk, drugs involved, usual and
usual presentation, prospects for prevention, management
approach and reasons for continuing morbidity/mortality
• Case reports – avoidable, unusual, fulminant
• Causes and intrinsic/extrinsic risk factors for anaphylaxis
• Mechanisms, clinical features and grading of anaphylaxis
• Management approach – adrenaline as the first-line drug
• Strategies – prevention, recognition and management

2
Drug-induced anaphylaxis should be avoidable
M/55, allergic rhinitis, asthma, known allergy to aspirin
and ibuprofen for ~8 years
Took diclofenac 100 mg (own stock) for left knee pain
Sudden onset of SOB, wheeze and flushing 3 h later
Arrived in ED 40 min after onset of symptoms
BP 142/86 mmHg, pulse 104 bpm, RR 32 breaths/min
SaO2 95% (O2 4 L/min), diffuse rhonchi
Adrenaline (1:1000) 0.5 ml i.m.
Hydrocortisone 200 mg i.v., chlorpheniramine 10 mg i.v.
Salbutamol and ipratropium MDI
Home after staying in EMW for 12 hours
Drug-induced anaphylaxis could have been missed
F/55, found collapsed in shopping mall, GCS 3, pupils 3
mm, ambulance arrived in 10 min, spontaneous breathing but
cyanosed, bagging (SaO2 3085%)
Intubated in A&E, BP 179/98 mmHg, pulse 119 bpm, SaO2
99%, 4 limb movements, rhonchi, salbutamol/ipratropium
Woke up 1.5 h and extubated 2 h after ICU admission, acute
onset of SOB before LOC 1 h after taking levofloxacin 1 tab
for toothache, vomited once
Stayed in ICU for 25.5 h and in ward for 2 days
cardiac troponin 79.5 ng/L (<14), ALT 100 IU/L (<55),
WBC 12.3 x 109/L (<9.7), ECG normal
On discharge, BP 118/70 mmHg

3
Drug-induced anaphylaxis could be rapidly fatal
M/51, IVU as out-patient, iopamidol (water-soluble non-
ionic, monomeric, iodinated radiocontrast medium)
After the injection, vomiting, LOC and pulseless, CPR
started, pulseless electrical activity on ECG
Adrenaline 1 mg i.v., fluids i.v. orientated, SBP ~140
mmHg, chest pain, ST ↓ on ECG, faecal incontinence,
very red appearance (vasodilation)
Cardiac arrest, LOC, CPR started, adrenaline 1 mg iv,
narrow complex rhythm, asystole or VF on ECG, DC
shock given, failed resuscitation
Autopsy epiglottis swelling, pulmonary congestion,
coronary atherosclerosis and cardiomegaly
What is anaphylaxis
An acute, potentially life-threatening hypersensitivity reaction,
involving the release of mediators (e.g. histamine) from tissue
mast cells, circulating basophils, recruited inflammatory cells
Multisystem signs and symptoms occurring within minutes or
up to a few hours, after exposure to provoking agents – severe
allergic reactions with CVS and/or RS features
Can be mild, moderate to severe or severe
Developing rapidly, usually reaching peak severity within 5-30
minutes, and may, rarely, last for several days
3-23% of episodes followed by biphasic reactions hours later
(Adapted from: Lockey RF 2004 and Confino-Cohen R et al. 2010)

4
What is anaphylactic shock
Anaphylaxis accompanied by hypotension (SBP >30% ↓ from
baseline or <90 mmHg in adults)
Rarely, patients present with isolated acute hypotension
The main cardiovascular changes during anaphylaxis = fluid
extravasation and vasodilation (causing a mixed distributive–
hypovolaemic shock) plus ↓ myocardial contractivity
Blood volume may decrease by up to 35% within 10 minutes
due to extravasation; severe vasodilation may only respond to
potent vasoconstrictors
Risk factors for shock in anaphylaxis – old age, anti-HT drugs
(Brown SGA. Immunol Allergy Clin N Am 2007; 27: 165-75)
(Lee S et al. J Allergy Clin Immunol 2013; 131: 1103-8)
Causes of anaphylaxis – Hong Kong
Common causes differ between children (foods) and adults (drugs)
282 patients (166M, 116F) aged 1-91 years (median 28) with
anaphylaxis, Prince of Wales Hospital ED, 3/1999 to 2/2003
A precipitant identified in 89%, with 19% of patients claiming
a known allergy to the precipitant
Foods = 49.6% of cases (seafoods – 71%)
Drugs = 40.5% of cases (NSAIDs/aspirin – 25.5%, antibiotics
– 23.5%, Chinese medicines – 21.6%)
Insect bites/stings = 7.1%
Plants/hair dye = 1.6%, gas inhalation = 0.4%, idiopathic = 0.8%
(Smit DV et al. J Emerg Med 2005; 28: 381-8)

5
Drugs causing anaphylaxis – Europe
National Pharmacovigilance System, Portugal
1/2000-10/2010, 918 anaphylaxis cases (6% of ADR reports)
Age 7 days-91 years, mean 48 years, 9% ≤18 years
F = 70% of adults, M = 56% of paediatric population
Antibiotics (17%), NSAIDs/paracetamol (13%), cytotoxic
drugs (12%), immune-modulators (9%), vaccines (7%) and
radiocontrast media (4 %)
19% led to hospitalisation, 24 (3%) had a fatal outcome
Anaphylaxis can occur at any age and is mostly caused by
widely used drugs (e.g. antibiotics and analgesics)
(Ribeiro-Vaz I et al. Eur J Clin Pharmacol 2013; 69: 673-81)
Intrinsic risk factors for anaphylaxis
• Previous history of anaphylaxis – however, at least
25% of adults and 65% of children with anaphylaxis
do not report a previous episode
• Atopy – orally administered drugs, radiocontrast media,
latex, exercise, idiopathic anaphylaxis
• Female gender – aspirin, muscle relaxants, diagnostic
agents, idiopathic anaphylaxis
• Increased socio-economic status
• ↓ vitamin D level (sunlight exposure) – a strong north-
south gradient in the US for EpiPens prescriptions
(Lee JK et al. Clin Exp Allergy 2011; 41: 932-8; Ben-Shoshan M et al. Allergy 2011; 66: 1-14)

6
Group Name of gene Comments
Anatomic barrier genes Filaggrin Increased risk of developing allergic sensitisation and not necessarily anaphylaxis
Innate immunity genes NLRP3: SNPs (rs4612666 and rs10754558) Significantly associated with susceptibility to food-induced anaphylaxis
Innate immunity and
mast cells genes
C-KIT Mutations associated with anaphylaxis after hymenoptera stings and may also
underlie cases of idiopathic anaphylaxis
SWAP-70 Anaphylactic responses are strongly reduced in mice with mutations in this gene
PAF V279F (>30% of Japanese subjects) Mutations increase the risk for various inflammatory diseases in Japanese subjects
PAF and PAF-AH activity affect severity of anaphylaxis
Sphk1 Sphingosine 1-phosphate receptors play a critical role in regulating human mast cell
functions, including degranulation and cytokine and chemokine release
Rcan Rcan1 is a novel negative regulator in FcεRI-induced mast cell activation
CCRL2 Enhance tissue swelling and leucocyte infiltrates
Adaptive immunity STAT-6 (13/15-GT repeat heterozygosity
and the 15GT repeat homozygosity)
Polymorphisms higher in children in Japanese population with allergic disease
IL-4 (Ile75Val variant of IL-4R∝ gene) Polymorphisms of IL-4 have been implicated in drug allergy especially in women
IL-10 (-819 C>T and -592 C>A variants) Polymorphisms of IL-10 promoter associated with β-lactam anaphylactic reactions
IL-13, 18 (promoter polymorphisms in
IL13-1055, IL18-607 and IL18-656)
Latex allergy phenotype significantly associated with polymorphism in the promoter
site of these cytokines
Unknown function DOCK8 Absence of DOCK8 protein associated with severe atopy and anaphylaxis
Genes implicated in the pathogenesis of anaphylaxis
Adapted from: Ben-Shoshan M al el. Allergy 2011; 66: 1-14
Mechanisms of anaphylaxis Most cases are IgE mediated, but it is not possible to distinguish IgE from non-IgE cases
Anaphylaxis
Allergic (immunologic)
anaphylaxis
Non-allergic (non-
immunologic) anaphylaxis
IgE mediated Non-IgE mediated (IgG mediated, complements and
coagulation system activation,
immune complexes, etc.)
Direct activation
of mast cells
Excessive amounts of IgE are produced during sensitisation. Specific IgE binds to high affinity IgE receptors
(FcεRI) on mast cells and basophils. Re-exposure to allergen leads to cross-linking of receptor-bound IgE,
triggering cell activation and release of mediators.
7
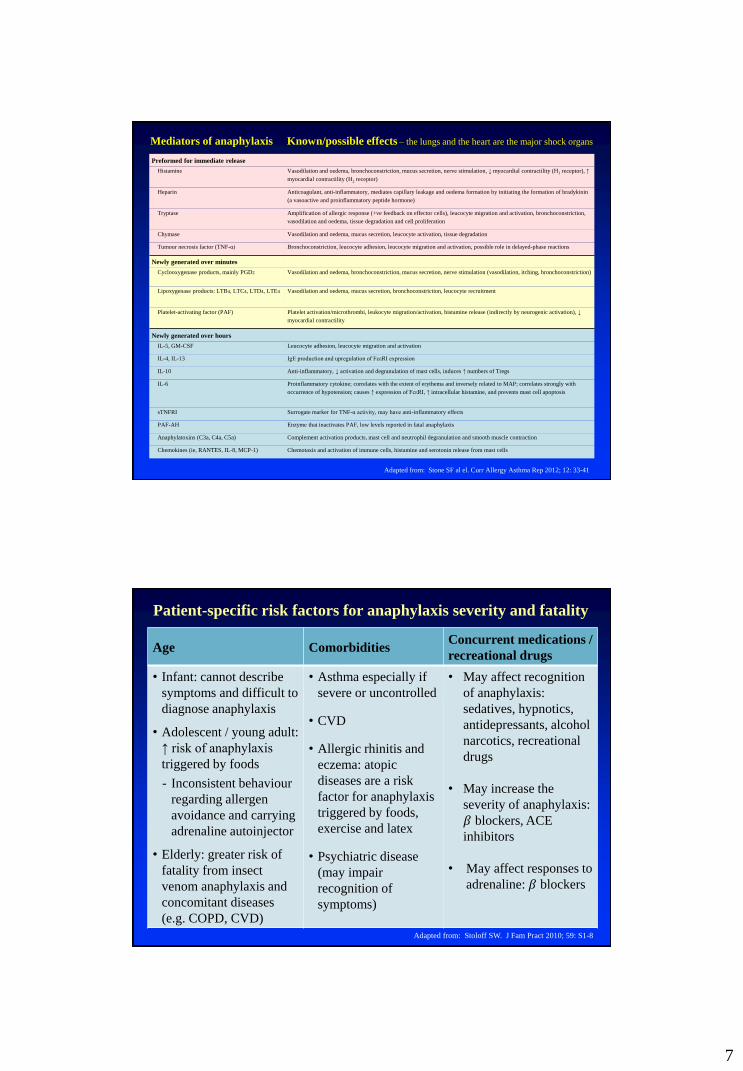
Preformed for immediate release
Histamine Vasodilation and oedema, bronchoconstriction, mucus secretion, nerve stimulation, ↓ myocardial contractility (H1 receptor), ↑
myocardial contractility (H2 receptor)
Heparin Anticoagulant, anti-inflammatory, mediates capillary leakage and oedema formation by initiating the formation of bradykinin
(a vasoactive and proinflammatory peptide hormone)
Tryptase Amplification of allergic response (+ve feedback on effector cells), leucocyte migration and activation, bronchoconstriction,
vasodilation and oedema, tissue degradation and cell proliferation
Chymase Vasodilation and oedema, mucus secretion, leucocyte activation, tissue degradation
Tumour necrosis factor (TNF-α) Bronchoconstriction, leucocyte adhesion, leucocyte migration and activation, possible role in delayed-phase reactions
Newly generated over minutes
Cyclooxygenase products, mainly PGD2 Vasodilation and oedema, bronchoconstriction, mucus secretion, nerve stimulation (vasodilation, itching, bronchoconstriction)
Lipoxygenase products: LTB4, LTC4, LTD4, LTE4 Vasodilation and oedema, mucus secretion, bronchoconstriction, leucocyte recruitment
Platelet-activating factor (PAF) Platelet activation/microthrombi, leukocyte migration/activation, histamine release (indirectly by neurogenic activation), ↓
myocardial contractility
Newly generated over hours
IL-5, GM-CSF Leucocyte adhesion, leucocyte migration and activation
IL-4, IL-13 IgE production and upregulation of FcεRI expression
IL-10 Anti-inflammatory, ↓ activation and degranulation of mast cells, induces ↑ numbers of Tregs
IL-6 Proinflammatory cytokine; correlates with the extent of erythema and inversely related to MAP; correlates strongly with
occurrence of hypotension; causes ↑ expression of FcεRI, ↑ intracellular histamine, and prevents mast cell apoptosis
sTNFRI Surrogate marker for TNF-α activity, may have anti-inflammatory effects
PAF-AH Enzyme that inactivates PAF, low levels reported in fatal anaphylaxis
Anaphylatoxins (C3a, C4a, C5a) Complement activation products, mast cell and neutrophil degranulation and smooth muscle contraction
Chemokines (ie, RANTES, IL-8, MCP-1) Chemotaxis and activation of immune cells, histamine and serotonin release from mast cells
Mediators of anaphylaxis Known/possible effects – the lungs and the heart are the major shock organs
Adapted from: Stone SF al el. Curr Allergy Asthma Rep 2012; 12: 33-41
Patient-specific risk factors for anaphylaxis severity and fatality
Age Comorbidities Concurrent medications /
recreational drugs
• Infant: cannot describe
symptoms and difficult to
diagnose anaphylaxis
• Adolescent / young adult:
↑ risk of anaphylaxis
triggered by foods
- Inconsistent behaviour
regarding allergen
avoidance and carrying
adrenaline autoinjector
• Elderly: greater risk of
fatality from insect
venom anaphylaxis and
concomitant diseases
(e.g. COPD, CVD)
• Asthma especially if
severe or uncontrolled
• CVD
• Allergic rhinitis and
eczema: atopic
diseases are a risk
factor for anaphylaxis
triggered by foods,
exercise and latex
• Psychiatric disease
(may impair
recognition of
symptoms)
• May affect recognition
of anaphylaxis:
sedatives, hypnotics,
antidepressants, alcohol
narcotics, recreational
drugs
• May increase the
severity of anaphylaxis:
𝛽 blockers, ACE
inhibitors
• May affect responses to
adrenaline: 𝛽 blockers
Adapted from: Stoloff SW. J Fam Pract 2010; 59: S1-8
8
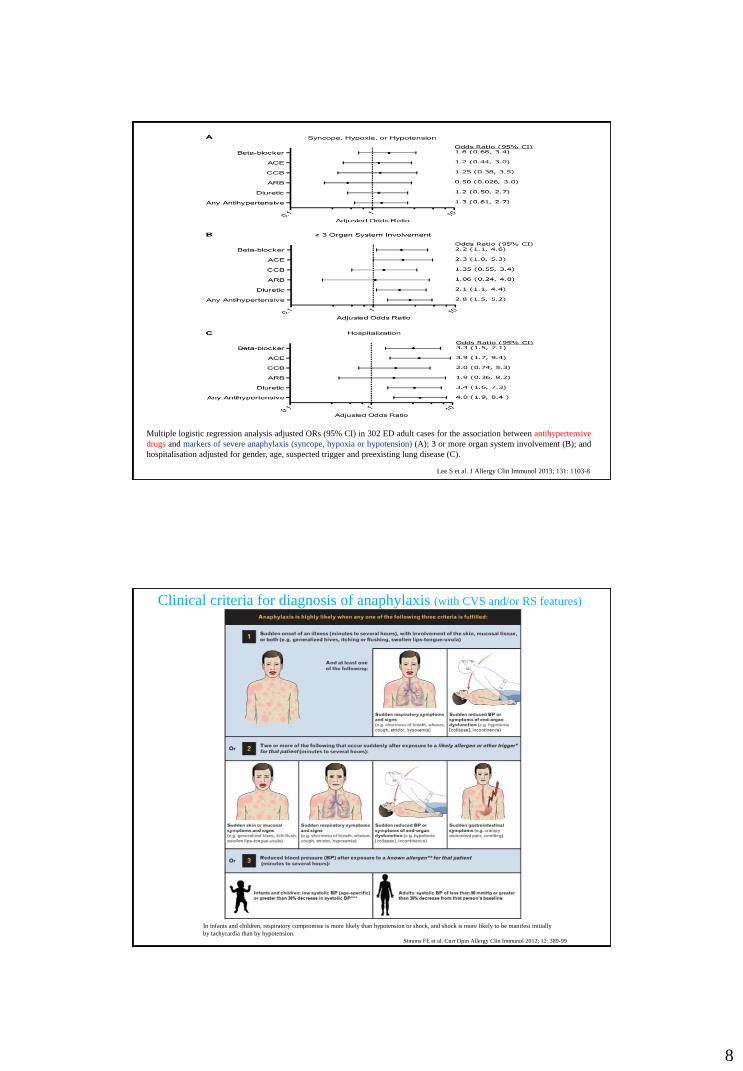
Multiple logistic regression analysis adjusted ORs (95% CI) in 302 ED adult cases for the association between antihypertensive
drugs and markers of severe anaphylaxis (syncope, hypoxia or hypotension) (A); 3 or more organ system involvement (B); and
hospitalisation adjusted for gender, age, suspected trigger and preexisting lung disease (C).
Lee S et al. J Allergy Clin Immunol 2013; 131: 1103-8
Simons FE et al. Curr Opin Allergy Clin Immunol 2012; 12: 389-99
Clinical criteria for diagnosis of anaphylaxis (with CVS and/or RS features)
In infants and children, respiratory compromise is more likely than hypotension or shock, and shock is more likely to be manifest initially
by tachycardia than by hypotension.

9
History of asthma 54 (19.1%)
History of allergy 116 (41.1%)
Clinical features
・Urticaria 223 (79.1%)
・Angioedema 171 (60.6%)
・Flushing or general pruritus 209 (74.1%)
・Dyspnoea 185 (65.6%)
・Wheeze/bronchospasm 85 (30.1%)
・Laryngeal oedema 31 (11%)
・Tongue swelling 21 (7.5%)
・Chest pain – non-specific 16 (5.7%)
・Angina 1 (0.35%)
・Abdominal pain or diarrhoea 27 (9.6%)
・Vomiting 23 (8.2%)
・Dysphagia 1 (0.35%)
・Headache 2 (0.71%)
・Syncope 16 (5.7%)
・Dizziness 39 (13.8%)
・Systolic BP (mmHg) 129 [108.5-150]
・Diastolic BP (mmHg) 68 [55.5-81]
・Peak expiratory flow rate (L/min) 300 [220-400]
282 patients with anaphylaxis, Prince of Wales Hospital, 3/1999 to 2/2003
Smit DV al el. J Emerg Med 2005; 28: 381-8
Numbers (%) of patients or medians (IQR [25–75])
Severity Defined by
Mild
(skin and subcutaneous tissues
only)†
Generalised erythema, urticaria,
periorbital oedema or angioedema
Moderate
(features suggesting respiratory,
cardiovascular or
gastrointestinal involvement)
Dyspnoea, stridor, wheeze, nausea,
vomiting, dizziness (presyncope),
diaphoresis, chest or throat
tightness or abdominal pain
Severe
(hypoxia, hypotension or
neurological compromise)
Cyanosis or SpO2 ≤92%,
hypotension (SBP <90 mmHg in
adults), confusion, collapse, loss of
consciousness or incontinence
Severity of generalised hypersensitivity reactions
Adapted from: Brown SGA. Emerg Med Australas 2006; 18: 155-69
†The Mild grade does not represent anaphylaxis according to the National Institute of Allergy and Infectious Disease-Food
Allergy and Anaphylaxis Network and World Allergy Organization definitions.

10
294 Korean subjects admitted to the ED with anaphylaxis, 1/2000-12/2009
Park HJ et al. Am J Emerg Med 2012; 30: 1674-8
Symptoms or signs, n (%) Non-shock (n=175) Shock (n=119) P value
Cutaneous
Urticaria
Itching
Flushing
Angioedema
166 (94.9)
99 (56.6)
69 (39.4)
41 (23.4)
28 (16.0)
97 (81.5)
50 (42.0)
61 (51.3)
32 (26.9)
15 (12.6)
<.001
.014
.045
.500
.419
Respiratory
Dyspnoea
Hoarseness
Cyanosis
Laryngeal oedema
Cough
Wheezing
100 (57.1)
93 (53.1)
6 (3.4)
2 (1.1)
5 (2.9)
5 (2.9)
5 (2.9)
68 (57.1)
65 (54.6)
2 (1.7)
21 (17.6)
1 (0.8)
1 (0.8)
5 (4.2)
1.000
.803
.480
<.001
.407
.407
.533
Cardiovascular
Syncope
Chest discomfort
Palpitation
Sweating
Cardiac arrest
50 (28.6)
3 (1.7)
40 (22.9)
3 (1.7)
4 (2.3)
0 (0.0)
102 (85.7)
45 (37.8)
16 (13.4)
3 (2.5)
15 (12.6)
1 (0.8)
<.000
<.001
.044
.689
<.001
.405
Gastrointestinal
Nausea
Vomiting
Abdominal pain
Diarrhoea
56 (32.0)
22 (12.6)
19 (10.9)
25 (14.3)
19 (10.9)
34 (28.6)
21 (17.6)
21 (17.6)
10 (8.4)
4 (3.4)
.531
.227
.096
.126
.019
Neurologic
Dizziness
Headache
Seizure
27 (15.4)
23 (13.1)
6 (3.4)
0 (0.0)
61 (51.3)
59 (49.6)
3 (2.5)
2 (1.7)
<.001
<.001
.743
.163
Characteristics Non-biphasic (n=195) Biphasic (n=13) P value
Male (%) 106 (54.4) 4 (30.8) 0.173
Median age, years 22 18.5 0.564
Atopy (%) 118 (60.5) 4 (30.8) 0.069
- Allergic rhinitis (%) 47 (22.6) 4 (30.8) 0.526
- Asthma (%) 31 (15.9) 3 (23.1) 0.771
- Food allergy (%) 45 (23.1) 2 (15.4) 0.764
Drug allergy (%) 36 (18.5) 0 0.13
Previous allergic reactions (%) 78 (40) 5 (38.5) 0.855
Underlying disease (%) 87 (44.6) 5 (38.5) 0.885
Presenting symptoms:
・Urticaria/angioedema (%) 169 (86.7) 12 (92.3) 1.00
・Bronchospasm (%) 100 (51.3) 4 (30.8) 0.252
・Abdominal pain (%) 57 (29.2) 7 (53.8) 0.121
・Hypotension (%) 63 (32.3) 5 (38.5) 0.879
・Shock (%) 56 (28.7) 5 (38.5) 0.665
・Unconsciousness (%) 7 (3.6) 1 (7.7) 0.409
Treatment:
・Intramuscular injection of adrenaline (%) 170 (87.2) 13 (100) 0.467
・Adrenaline use (%) 192 (98.5) 12 (92.3) 0.229
・Injected H1 antagonist (%) 180 (92.30 11 (84.6) 0.288
・Injected H2 antagonist (%) 114 (58.5) 9 (69.2) 0.636
・Steroid use (%) 169 (86.7) 10 (76.9) 0.398
・β-agonist use via nebuliser (%) 59 (30.3) 4 (30.8) 1.00
Time interval Median (IQR) Median (IQR)
・Time from contact – onset (minutes) 30 (17.5-107.5) 120 (10-240) 0.501
・Time from onset – hospital arrival (minutes) 60 (30-120) 180 (105-360) 0.002
・Time from onset – adrenaline (minutes) 70 (40-135) 240 (122.5-380) 0.002
・Time from hospital arrival – adrenaline (minutes) 15 (10-15) 25 (16.5-30) 0.001
208 cases of anaphylaxis with or without biphasic reactions, Thailand, 2004-2008
Lertnawapan R al el. Allergol Int 2011; 60 :283-9

11
Soar J et al. Resuscitation 2008; 77: 157-69.
Pros
• Adrenaline has a vasodilation effect in skeletal muscle
• Skeletal muscle is highly vascular, leading to rapid absorption
• Drug injected into vastus lateralis reaches central circulation
promptly
• Peak pharmacologic effects are achieved promptly
• Benefit-to-risk ratio perceived to be optimal when this route is used
for first-aid treatment
• Most commonly recommended route worldwide Cons
• Currently available auto-injector needle lengths and gauges are not
optimal for intramuscular injection in overweight or obese people
• Not effective if muscle perfusion is poor or absent due to shock or
cardiorespiratory arrest
Adrenaline – pros / cons of intramuscular administration in anaphylaxis
Simons KJ et al. Curr Opin Allergy Clin Immunol 2010; 10: 354-61

12
Pros
• Optimal route of administration for patients with severe anaphylaxis who have
not responded to intramuscular adrenaline and/or are experiencing profound
hypotension or shock, or in whom cardiorespiratory arrest is imminent
Cons
• Establishing a peripheral intravenous route for adrenaline administration may
be difficult in the above patients
• Narrower benefit-to-risk ratio than adrenaline administered by other routes,
partly attributed to iatrogenic error
• For safe administration in hypotension or shock, it is optimally given through
an infusion pump and central line by physicians trained and experienced in
continuous dose titration of vasopressors against continuously monitored heart
rate and function, blood pressure and oxygenation
• Errors in adrenaline dosing combined with errors in assessment of cardiac rate
and function and blood pressure can be catastrophic for the patient
Adrenaline – pros / cons of intravenous administration in anaphylaxis
Simons KJ et al. Curr Opin Allergy Clin Immunol 2010; 10: 354-61
ED management
・IV fluids 88 (31.2%)
・Adrenaline (i.v., i.m., s.c.) 188 (66.7%)
・H1 antagonists 269 (95.4%)
・H2 antagonists 4 (1.4%)
・Steroids 258 (91.5%)
・Salbutamol 95 (33.7%)
・Ipratroprium 44 (15.6%)
・Intubation 4 (1.4%)
Disposition
・Discharge ED 4 (1.4%)
・Discharge against advice 9 (3.2%)
・Observation ward 154 (54.6%)
・General ward 93 (33%)
・Intensive care unit 27 (7.8%)
282 patients with anaphylaxis, Prince of Wales Hospital, 3/1999 to 2/2003
Smit DV et al. J Emerg Med 2005; 28: 381-8

13
Follow-up care of patients with anaphylaxis
Patients should understand their drug allergy status and
action plans in case of emergency
Further work up and referral to the experts
Skin prick testing is useful to help identify the cause of
anaphylaxis, but does not predict the severity of reactions
Except for β-lactam antibiotics and a few other drugs,
such allergens are generally not available for skin testing
or in vitro testing
The level of serum specific IgE does not correlate with
reaction severity and cannot be used to identify subjects
at risk for anaphylaxis
(Lee JK et al. 2011 and Simons FER 2009)
Waserman S et al. Allergy 2010; 65: 1082-92
Theme Description Gap
Anaphylaxis
management
Lack of knowledge to identify the signs and
symptoms, or correctly diagnose anaphylaxis
Adrenaline is not the most commonly prescribed
treatment
Patients are not diagnosed accurately
Lack of awareness and adequate knowledge of anaphylaxis
No published criteria or professional consensus on prescribing adrenaline for
severe allergy
Infrequent, inappropriate or no use of adrenaline
Auto-injector prescription is low
Adrenaline use
Inadequate or no training provided to patients
on how to use adrenaline auto-injectors
Adrenaline administration is inadequate or delayed
Physicians lack knowledge on epinephrine use
Parents of children with allergies have unmet information needs from
their physicians, including not knowing the definition of anaphylaxis and
the symptoms requiring epinephrine
Patients receive infrequent or no instruction, demonstration, or training
on how to use auto-injectors
Patients unsure when or how to use an auto-injector
Adrenaline either not given or administration was delayed
Lack of knowledge or consensus on appropriate dosage of adrenaline
Few physicians have or know how to use an auto-injector training device
In acute severe reactions, differences exist on treatment recommendations, and
adrenaline is used less than other medications (e.g. steroids, β blockers)
Follow-up care
Infrequent or no referral to an allergy
specialist after acute reaction
Patients are not given enough information
about how to manage anaphylaxis
Patients do not have an anaphylaxis action plan
Few patients are being referred to an allergy specialist after an allergic reaction
Lack of follow-up is common in patients who experienced an acute reaction
Physicians did not think that advising patients to go to the hospital after
taking adrenaline was necessary
Few patients are given accurate information and advice by their family
physicians about managing anaphylaxis
Few patients with acute allergic reactions were given discharge instructions
Poor identification of or provision of guidance of which allergens to avoid
Patients do not have action plans or there is no consensus on what should be included
in action plans; missing essential components or auto-injector instructions
Anaphylaxis management gaps categorised by a Canadian panel of allergy experts in a systematic review

14
Anaphylaxis – Prevention, Recognition, Management
Anaphylaxis can occur at any age and is mostly caused by widely
used drugs (e.g. antibiotics, analgesics, cytotoxic drugs, RCM)
Drug induced anaphylaxis is preventable by checking and clearly
documenting drug allergy status and educating patients
Drug induced anaphylaxis can have unusual clinical presentations,
biphasic reactions, rapid clinical deterioration and fatal outcome
Patient-specific risk factors for anaphylaxis severity and fatality –
age, comorbidities (CVD, COPD) or concomitant drugs
Markers of severe anaphylaxis – including very rapid onset, shock,
cyanosis, syncope, neurological compromise
Adrenaline i.m. and fluids i.v. – first-line treatment of anaphylaxis
Continuing training to address gaps in knowledge and management