post-mortem findings in a fetus with 48,xxy, + 21
TRANSCRIPT
PRENATAL DIAGNOSIS, VOL. 1 1,47 1476 ( 199 1)
SHORT COMMUNICATION
POST-MORTEM FINDINGS IN A FETUS WITH 48,XXY, + 2 1
A. SMITH*, G. WATSON?, J. MICHAS*, R. VIERSBACHZ AND D. ELLWOOD$ Tyrogenetics Unit, Oliver Latham Laboratory. Department of Health, N.S. W. , Australia; tAnatomica1
Pathology, Royal Prince Alfred Hospital. Sydney, Australia: SCytogenetics Unit. iht i tut fur Humangenetik der Universitat Bonn, Germany: $Department of Fetal Medicine, King George V Hospital
for Mothers and Babies, Sydney, Australia
SUMMARY A fetus with 48,XXY,+21 was detected on routine amniocentesis at 15 weeks for advanced maternal age. Fibroblast cultures from six different tissues were initiated after termination and each showed the same karyotype without any tissue limited mosaicism. The only pheno- typic abnormality detected at post-mortem examination was bilateral clinodactyly of the fifth finger which had been detected on ultrasound. The maternal serum alpha-fetolprotein and the femur length were normal. Maternal age remains an essential criterion for prenatal diagnosis.
KEY WORDS Down’s syndrome Prenatal Ultrasound
INTRODUCTION
Double aneuploidies ofXXY and trisomy 21 were first detected in 1959 (Ford et al., 1959) and since then, many cases have been published (Smith and Berg, 1976). All of these cases were diagnosed postnatally and came from studies of either consecutive neonates (Hook and Hamerton, 1977) or Down’s syndrome patients (Hecht et al., 1969). The phenotype was invariably that of Down’s syndrome, but there is a dearth of postnatal cases examined pathologically at post-mortem. This would be of interest, to see how the two trisomies interact at the tissue level to cause an effect. We report here the pathological findings at post-mortern of a fetus with 48,XXY, + 2 1 karyotype terminated after amniocentesis and correlate these findings with cytogenetic analysis performed on six different fetal tissues.
METHODS AND RESULTS
Case report
Prenatal diagnosis by amniocentesis was undertaken at 15 weeks’ gestation for advanced maternal age. The mother was 39 and her husband was 42! years of age. She had one normal daughter aged 6 years. There had been no pregnancy losses. Ultrasound at 17 weeks showed a normal placenta, uterus and fetus. The maternal serum alpha-fetoprotein (MSAFP) was 32 ng/ml (0-9 MOM). The fetus had clinodactyly and absent middle phalanges of both fifth fingers. The femur length was nonnal at 2.9 cm. There were no other ultrasound signs of Down’s syndrome.
019’7-385 1/91/070471-O6%05.00 0 1991 by John Wiley & Sons, Ltd.
Received 29 August 1990 Revised 6 February 1991
Accepted 23 February 1991
472 A. SMITH ETAL.
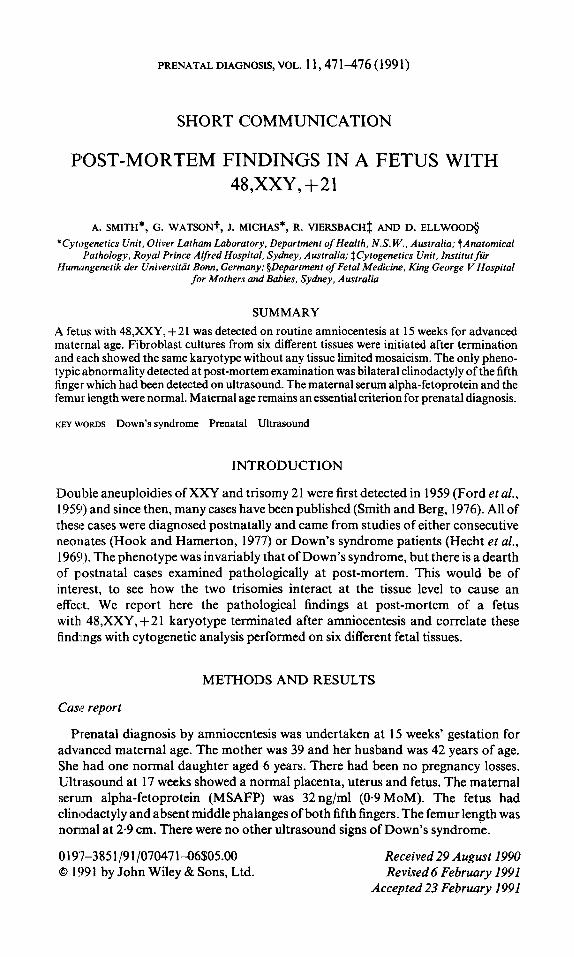
Table 1. Karyotypes found in different tissues
Total KaVotYpe Tissue c ~ I I s 48,X:XY,+21 47,XY,+21 47,XXY 46,XX,+20-21
1 - - Dura mater 37 36 Mesentery 25 25 Skin 25 25 Rib cartilage 2s 25 Right testis 25 23 Left testis 38 37 1
Total 175 171 1 2 1
- - - - - .-
- - .-
- 2 - - -
Cytogenetic methods
Amniotic fluid was set up by standard procedures. 20 ml in two tubes (10 ml each) was centrifuged for 10 mini at 900 cps, the supernatant removed, and the cells were resuspended in media-Changs (Hana Biologica) and Hams F10 (Flow Laboratories)-in three flask slides. They were left undisturbed in a CO, incubator at 37°C for 5 days, when the medium was changed. Cells were harvested in situ from the slide flasks after 3; h of 0.1 pg/ml colchicine, followed by 0-075 M KC1 hypotonic at 37°C for 30 min and fixation with 3: 1 methanol-acetic acid (total fixation time 1 h). GTG banding was perfornied 2 days later. Fourteen cells from nine colonies were fully analysed and each contained 48,XXY, +21.
The pregnancy was terminated at 18 weeks. Tissues were set up in fibroblast culture from dura mater, mesentlery, skin, rib cartilage, and right and left testis. Cells grew rapidly from all tissues. The first subculture was at 10 days and harvesting followed at 12 days. Karyotype (analysis was performed on GTG banded cells in all tissues. The results are shown in Table 1. The karyotype was stable throughout all tissues. There were two cells with 47,XXY and one cell with 47,XY,+21 from the right testis. Of a total of 175 cells analysed, one cell from the dura mater was aberrant. Parental karyotypes from peripheral blood were both normal.
Pathological report
Post-mortem pathological studies revealed a 144.5 g fetus, crown-rump length 145 mm, crown-heel length 205 mm, head circumference 145 mm, hand length 20mm, and foot length 24mm, consistent with 18/40 gestation. The external genitalia were male (Figure 1).
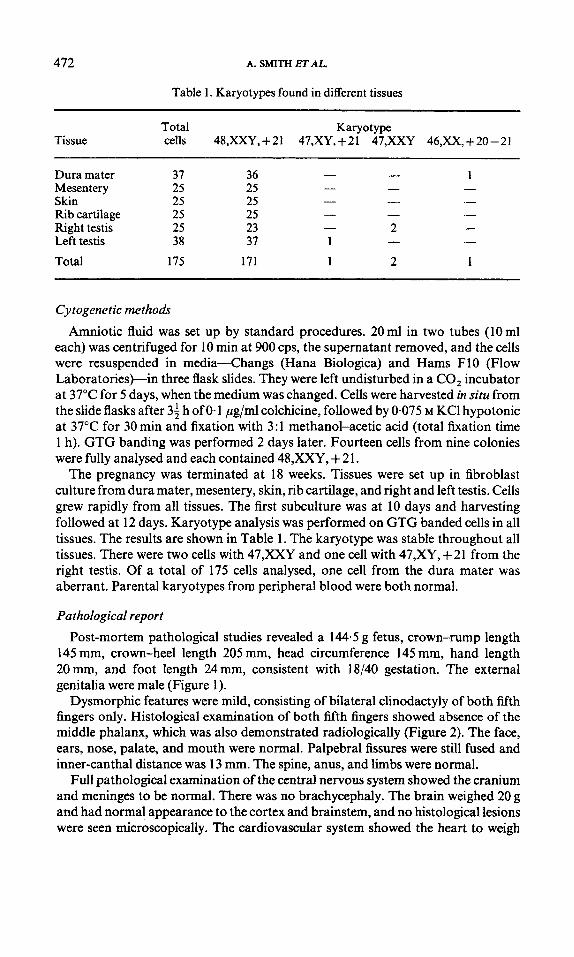
Dysmorphic features were mild, consisting of bilateral clinodactyly of both fifth fingers only. Histological examination of both fifth fingers showed absence of the middle phalanx, which was also demonstrated radiologically (Figure 2). The face, ears, nose, palate, and mouth were normal. Palpebral fissures were still fused and inner-canthal distance was 13 mm. The spine, anus, and limbs were normal.
Full pathological examination of the central nervous system showed the cranium and meninges to be normal. There was no brachycephaly. The brain weighed 20 g and had normal appearance to tlhe cortex and brainstem, and no histological lesions were seen microscopically. The cardiovascular system showed the heart to weigh

413
Figure I . The fetus at 18 weeks’ gestation. The external appearance, weight, length, ;and head circum- ference were normal. Bilateral clinodactyly was evident
0.7 g and had normal chamber morphology and vascular connections. The coronary sinus, foramen ovale, and interventricular septum were normal. The aorta and the arch branches were normal. Microscopically, the myocardium was normal.
474 A. SMITH ET AL.
Figure 2. X-Rays of the left hand (a) and right hand (b) showing clinodactyly and absence of ossification centre for the middle phalanx of the fifth finger bilaterally
Other systems were also normal. The lungs together weighed 4.0g and were normal with development consistent with 17 weeks. The right horizontal fissure was deficient. The oesophagus, stomach, duodenum, small intestine, appendix, and colon were normal. There was no Meckel’s diverticulum. The liver weighed 5-5 g and was normal. The gall bladder was normal; the pancreas appeared normal; the spleen weighed 0.1 g and was normal; the adrenals together weighed 0-5 g and were normal. The kidneys together weighed 0.7 g and were normal. External genitalia were nor- mal male. Normal testes were present in pelvic location and both were histologically normal for 17 weeks with recognizable germ cells and a normal tubular architecture. Examination of the placenta showed second-trimester chorionic villi with mild villous oedema, but no evidence of villitis or ischaemic changes. Stem vessels and intervillous spaces were normal.
DISCUSSION
Double aneuploidy in prenatal studies is an uncommon finding. There were four cases involving autosomal trisorny and either XXX or XXY in the 52 965 amnio- centeses reported in the European Collaborative Study (Ferguson-Smith and Yates, 1984Fan incidence of 1 in 13 241. This case is the first double aneuploidy that we have detected in 2850 prenatal siamples performed for maternal age over 37 years. The frequency of 1 in 13 000 found in the European study is greater than a calculated

A FETUS WITH 48,XXY,+21 475
expected figure of 1 in 360000 (taking the expected frequency of each trisomy together). A much higher incidence of double trisomies was also found1 at birth than would be expected by chance (Hook and Hamerton, 1977). In a recent case of 46,X.+21, it was possible to show by DNA studies that both non-disjunctional events took place in the mother (Ikonen et al., 1989) and further studies of this nature will throw light on the biological mechanisms involved in double aneuploidy.
Post-termination pathology showed virtually no abnormality in this case either macroscopically or microscopically. There was no growth retardation at this stage. It is known that the features of Down’s syndrome may be difficult to detect before birth (Smith and Berg, 1976) and Klinefelter’s syndrome has not been thoroughly evaluated prenatally. The testes were normal although the karyoltype showed 48,X:XY, + 21. The only phenotypic abnormality after thorough ultrasound and pathological examination was bilateral clinodactyly. This case emphasizes the potential importance of this sign in the prenatal period as an indicator of Down’s syndrome. Sonographic findings suggestive of the other common autosomal trisclmies (1 8 and 13) frequently include abnormalities of the hands (Holzgreve, 1990). In a discussion on the sonographic detection prenatally of Dowin’s syndrome, Benacerraf et al. (1987) concentrated on femur length and nuchal skin fold thick- ness, showing from their data that using these two parameters alone, fetuses with Down’s syndrome could be identified with a sensitivity of 75 per (cent. If other sonographic anomalies such as atrio-ventricular canal defect anid meconium peritonitis were added, the sensitivity of detection rose to 82 per cent in the second trimester. However, Toi et al. (1987) dispute this high sensitivity and pin-point the ‘low specificity of these features for Down’s syndrome. We suggest that clino- dactyly should be sought in routine second-trimester scanning although it could be important to establish data on the normal time of appearance of the middle phalanx on ultrasound, to reduce the possibility of false-positive ultrasound diagnosis.
Diespite the double aneuploidy, this case may not have been selected for amrdocentesis based on the combined criteria including MSAFP, nuchal skin fold, and femur length, all of which were entirely normal. Karyotyping in the advanced maternal age group must remain an option in prenatal diagnosis at the present time.
REFERENCES
Benacerraf, B.R., Gelman, R., Frigoletto, F.D. (1987). Sonographic identification of second- trimester fetuses with Down’s syndrome, N . Engl. J . Med., 317, 1371-1376.
Ferguson-Smith, M.A., Yates, J.R.W. (1984). Maternal age specific rates for chromosome aberrations and factors influencing them: report of a collaborative European study on 5;! 965 amniocenteses, Prenat. Diagn., 4 (Special Issue), 5-54.
Ford, C.E., Polani, P.E., Briggs, J.H., Bishop, P.M.E. (1959). The chromosomes in a patient shhowing both mongolism and the Klinefelter syndrome, Lancet, 1,709.
Hecht, F., Nievaard, J.E., Duncanson, N., Miller, J.R., Higgins, J.V., Kimberling, W.J., Walker, F.A., Smith, G.S., Thuline, H.C., Tischler, B. (1969). Double aneuploidy: the frequency of XXY in males with Down’s syndrome, Am. J . Hum. Genet., 2,1,352-354.
Hol:zgreve, P.D.W. (1990). Fetal anomalies, Curr. Opinion obstet. gynaecol., 12,215-22 1. Hook, E.B., Hamerton, J.L. (1977). The frequency of chromosome abnormalities detected in
consecutive newborn studiesdifferences between studies-results by sex and by seventy of phenotypic involvement. In: Hook, E. B., Porter, I. H. (Eds). PopuZuti#on Cytogenetics S,fudies in Humans. New York: Academic Press, 63-80.

476 A. SMITH E r AL.
Ikonen, R.S., Lindlof, M., Janas, M.O., Simola, K.O.J., Millington-Ward, A., de la Chapelle, A. (1989). Co-incident maternal meiotic nondisjunction of chromosomes X and 21 without evidence of autosomal asynapsis, Hum. Genet., 83,235-238.
Smith, G.F., Berg, J.M. (1976). Down S Anomaly, 2nd ed., Edinburgh: Churchill Livingstone, 206-2 16.
Toi, A., Simpson, G.F., Filly, R.A. (1!)87). Ultrasonically evident fetal nuchal skin thickening: is it specific for Down’s syndrome?, Am. J. Obstet. Gynecol., 156, 150-153.