policy, strategy and change: health services planning · what is strategic planning? in any...
TRANSCRIPT
Policy, Strategy and Change:Health Services Planning
Professor Dato’ Dr Hj Abdul Rahim bin AbdullahMBBS(Medicine & Surgery, AUS); MHA(Health Management, AUS); DBA(International Business, UK); MBA(Strategic Management, UK) Public Health Physician & Consultant (Health Management)Chief Surveyor, Malaysian Healthcare Facilities & Services Accreditation Program
UNIMAS28 February 2019
PUBLIC HEALTH SEMINARPOST SEMINAR WORKSHOP
28 February 2019
National Health Policy
NHP
• Relations (Industry, Markets, 7-S McKinsey,….)
• Technical (Services/ Products…
STRATEGIES
Review/ reforms
• Strategic Audit - Purpose
• Restructuring - Process
• Systemic change - People
National Health Policy
NHP NCD
• NHP RA Tobacco• PI Cigarette
Smoke Free -Zones/Areas/ Buildings e.g. restaurants/ eateries
STRATEGY 1 KRA
• Activities/ Action 1 What Why How Who When KPI
• Action 2
• Action 3

National Health Policy
NHP NCD
• NHP RA Tobacco• PI Cigarette
Smoke Free -Zones/ Areas/ Buildings e.g. restaurants/ eateries
STRATEGY 2 KRA
• Activities/ Action 1 What (How) Why Who When KPI
• Action 2
• Action 3
TOC

Delivery
IntermediaryFinancial
Consumer
External Environment Physical
PEST
Industry
Markets
LOMPlan
Organize (7-S)Direct* Control/ InfluenceMotivate.
Processes Institutional
GovernanceStewardship
DirectionPeople Purpose
Health System StructuresHealth Policies
Strategies
HEALTH FACILITY AND SERVICES
TACTICAL PLANS
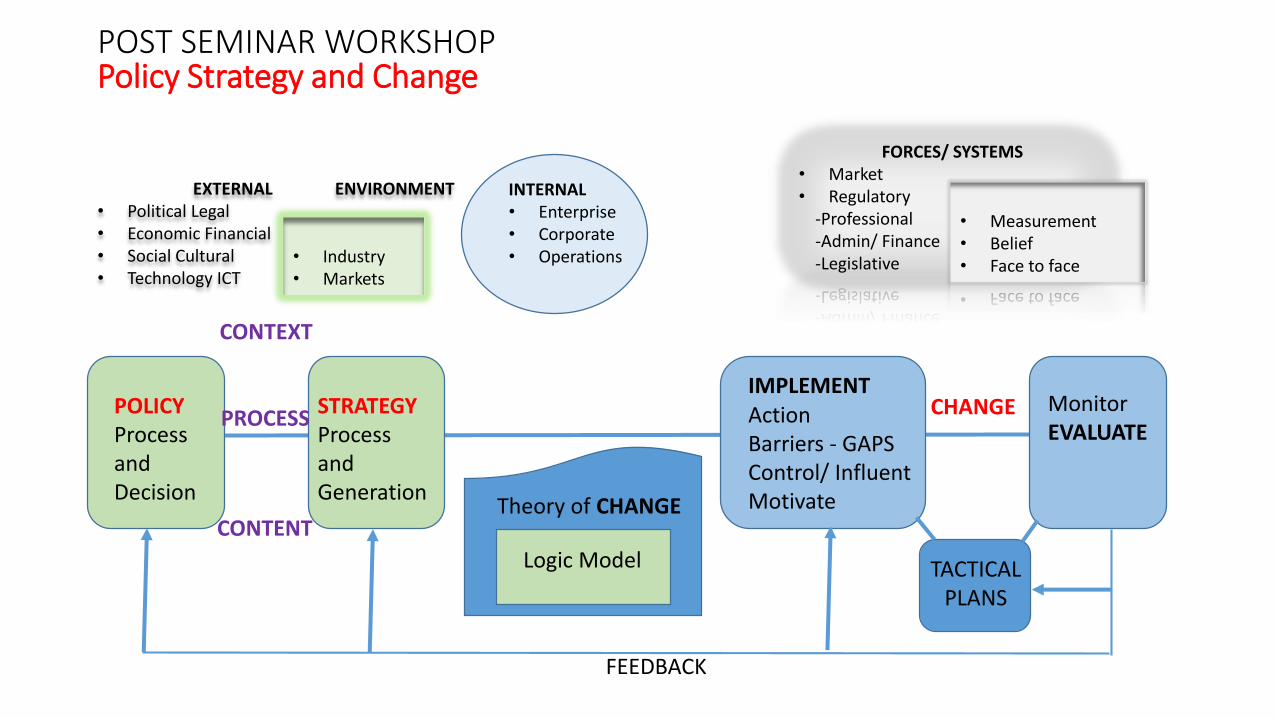
POST SEMINAR WORKSHOPPolicy Strategy and Change
POLICYProcess and Decision
STRATEGYProcessand Generation
IMPLEMENTActionBarriers - GAPSControl/ InfluentMotivate
MonitorEVALUATE
TACTICAL PLANS
FORCES/ SYSTEMS• Market• Regulatory
-Professional-Admin/ Finance-Legislative
EXTERNAL ENVIRONMENT• Political Legal• Economic Financial• Social Cultural• Technology ICT
• Industry• Markets
INTERNAL• Enterprise• Corporate• Operations
• Measurement• Belief• Face to face
Theory of CHANGE
Logic Model
CONTEXT
PROCESS
CONTENT
CHANGE
FEEDBACK
Health System Goals – Policy IntentionsMeasure of Success
OUTCOMES
The essence of our Vision for Health is geared towards achieving :
HEALTH STATUS. Levels of Health and Health Improvements
RISK PROTECTION – Illness, Financial especially against catastrophic illnesses
RESPONSIVENESS - Timeliness, Courteousness
CONSUMER SATISFACTION (vs. Needs, Wants, Demands)
IN A MANNER THAT IS
1. EQUITABLE fair process and just outcomes
2. EFFECTIVE quality and safe
3. EFFICIENTvalue for money and economic value

What is Strategic Planning?
In any situation, for an organisation or an individual,
• the basic purpose of strategic planning is determine where you want to go
• how you are going to get there.
Organisations, like individuals, must also determine
• what sort of future is desirable
• how this is to be achieved
Whenever an organisation or an individual sets a course of action to be
taken to achieve longer-term goals, they are engaging in strategic planning.
GOAL - Something that is desired to be achieved. Strategic Intent.STRATEGY - The basic methodology used to bring about achievement of the goal.

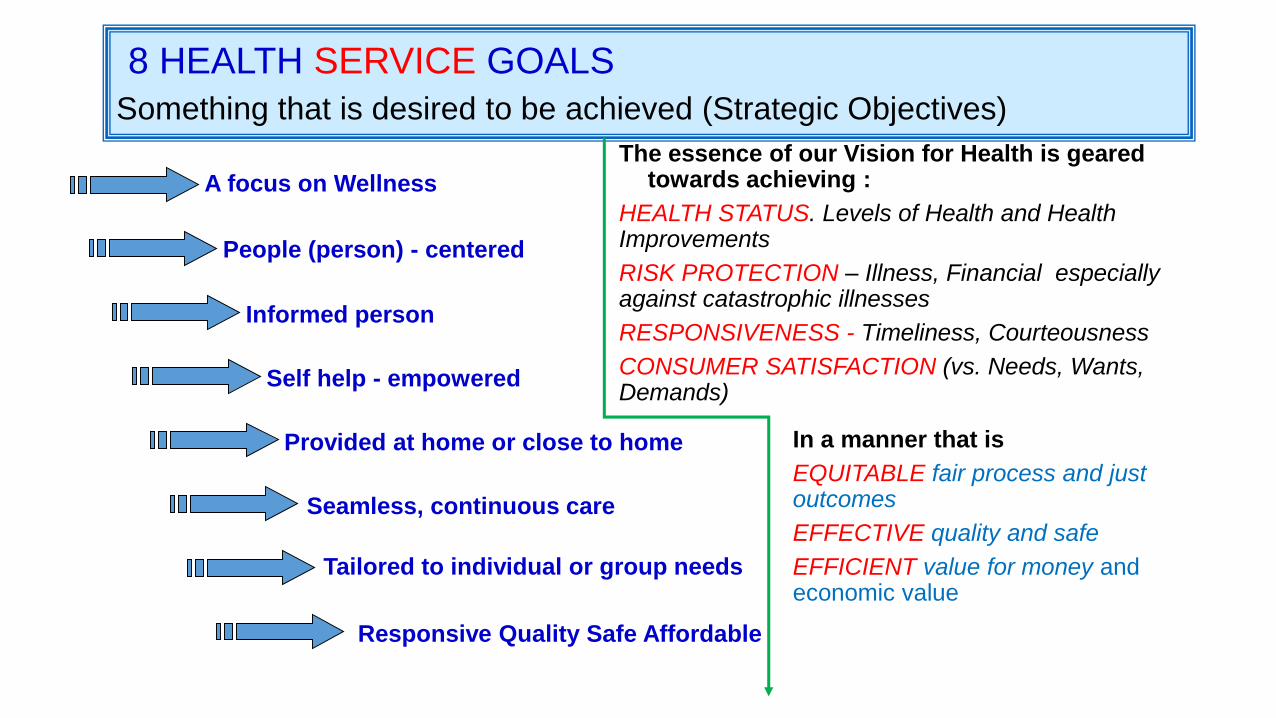
8 HEALTH SERVICE GOALS
Something that is desired to be achieved (Strategic Objectives)
In a manner that is
EQUITABLE fair process and just outcomes
EFFECTIVE quality and safe
EFFICIENT value for money and economic value
The essence of our Vision for Health is geared towards achieving :
HEALTH STATUS. Levels of Health and Health Improvements
RISK PROTECTION – Illness, Financial especially against catastrophic illnesses
RESPONSIVENESS - Timeliness, Courteousness
CONSUMER SATISFACTION (vs. Needs, Wants, Demands)
8 HEALTH SERVICE GOALS
Something that is desired to be achieved (Strategic Objectives)
Seamless, continuous care
Tailored to individual or group needs
Responsive Quality Safe Affordable
Provided at home or close to home
Self help - empowered
Informed person
People (person) - centered
A focus on Wellness
In a manner that is
EQUITABLE fair process and just outcomes
EFFECTIVE quality and safe
EFFICIENT value for money and economic value
The essence of our Vision for Health is geared towards achieving :
HEALTH STATUS. Levels of Health and Health Improvements
RISK PROTECTION – Illness, Financial especially against catastrophic illnesses
RESPONSIVENESS - Timeliness, Courteousness
CONSUMER SATISFACTION (vs. Needs, Wants, Demands)
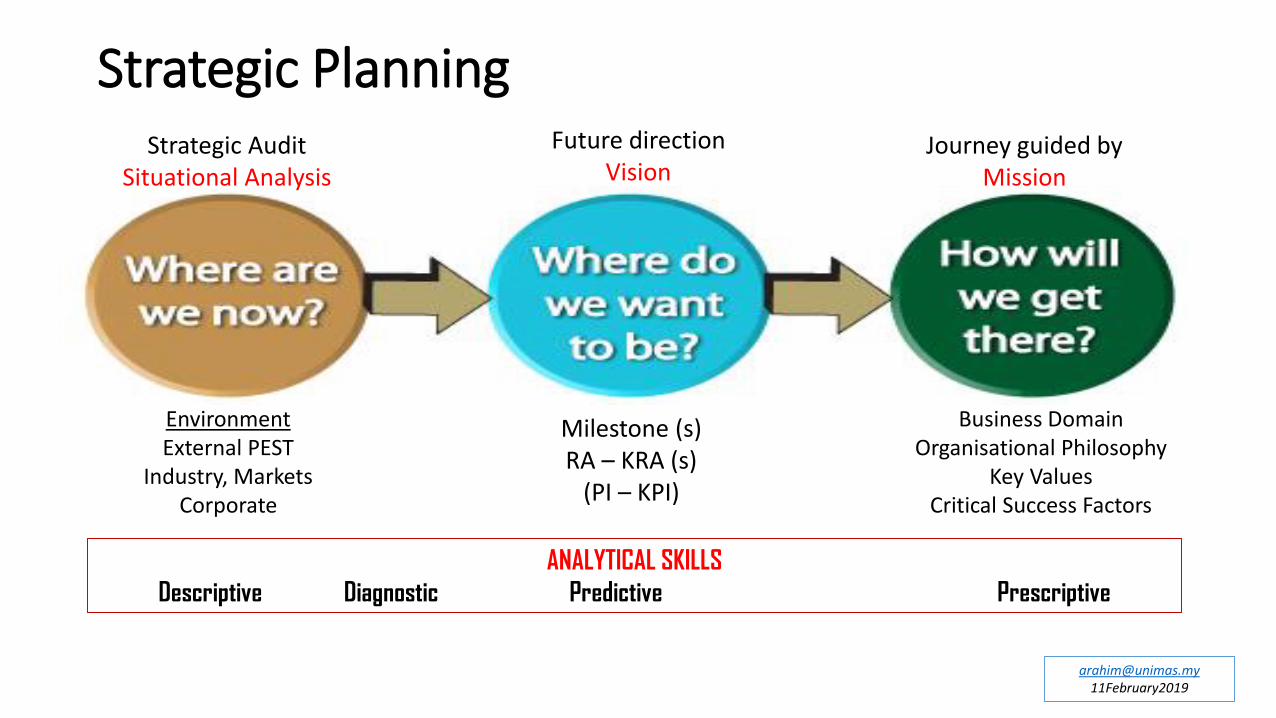
Strategic PlanningStrategic Audit
Situational Analysis
Future directionVision
Journey guided by Mission
Milestone (s)RA – KRA (s)
(PI – KPI)
Business DomainOrganisational Philosophy
Key ValuesCritical Success Factors
ANALYTICAL SKILLS
Descriptive Diagnostic Predictive Prescriptive
EnvironmentExternal PEST
Industry, MarketsCorporate
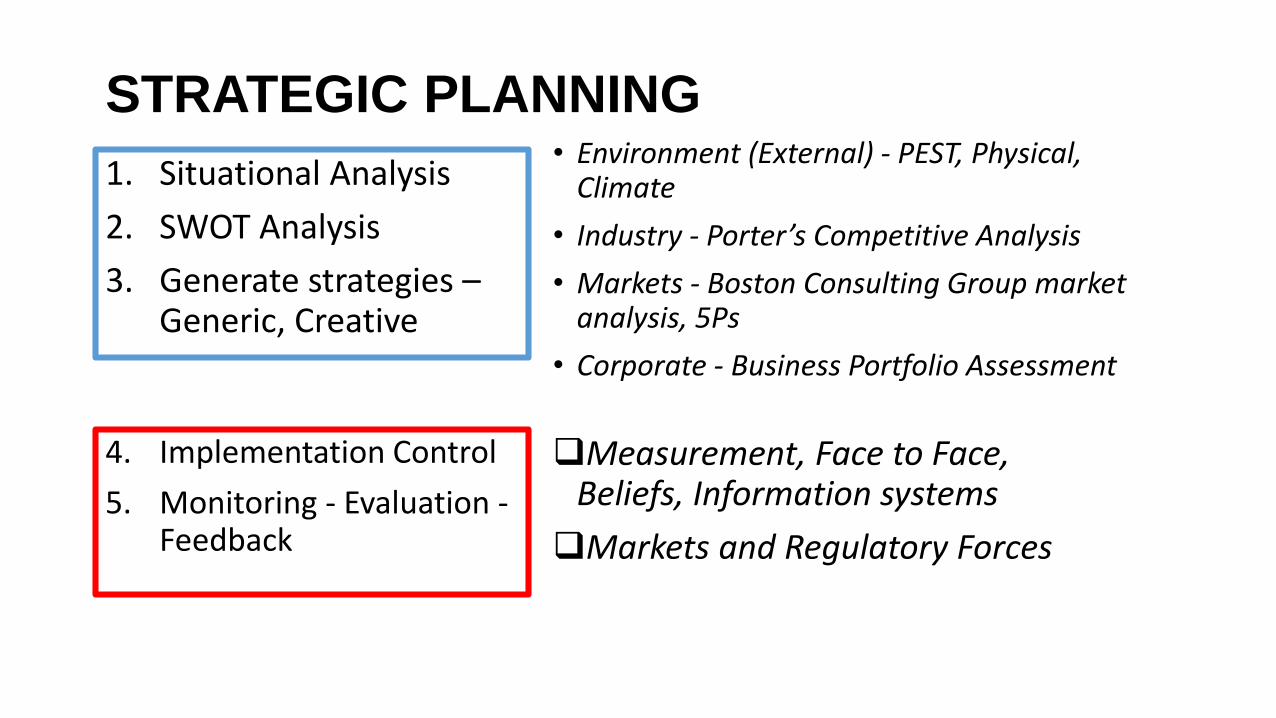
STRATEGIC PLANNING
1. Situational Analysis
2. SWOT Analysis
3. Generate strategies –Generic, Creative
• Environment (External) - PEST, Physical, Climate
• Industry - Porter’s Competitive Analysis
• Markets - Boston Consulting Group market analysis, 5Ps
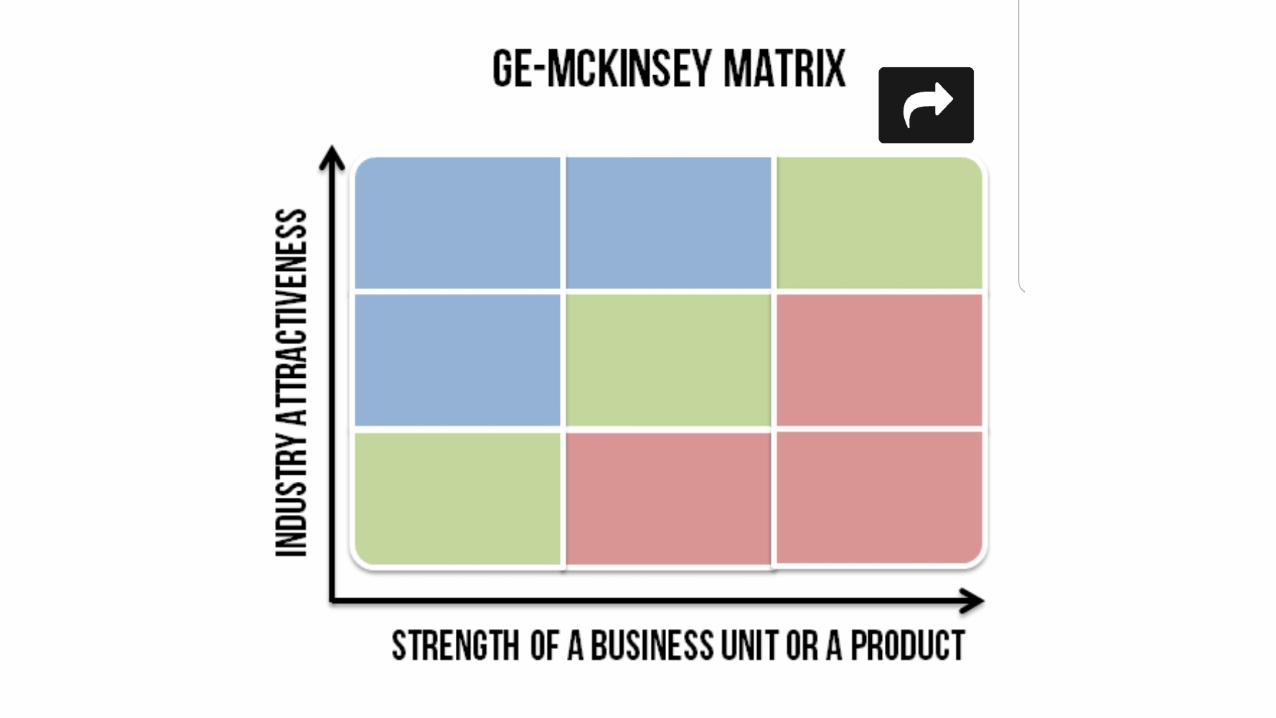
• Corporate - Business Portfolio Assessment
4. Implementation Control
5. Monitoring - Evaluation -Feedback
❑Measurement, Face to Face, Beliefs, Information systems
❑Markets and Regulatory Forces
• Strategic - competitive• Process• Performance

BCG – Business
Portfolio Analysis

Strategic Planning and the 7-S Framework
McKinsey’s 7-S
• Strategy
• Structure
• System(s)
• Staff (qualified)
• Skills
• Shared Values
• Style of leadership/ management
Beyond 7-S
• Purpose
• Process
• People
• Knowledge from Education
• Skills by Training
• Experience for competence
• “Learning Organisation” -Knowledge Management
Policy Implementation Strategies
• Structures
• Content
• ControlStrategies
Strategies
• Generic (SWOT Utilise Strengths, Overcome Weaknesses, Grab opportunities, Nullify Threats)
• Creative (new/ innovative ideas)
Systems
• Measurement system
• Face to Face system
• Belief system
• Market Forces
• Regulatory Forces –Professional, Administrative/Accounting & Finance, Legislation
SWOT ANALYSIS
STRENGTHS OPPORTUNITIES
THREATSWEAKNESSES
INTERNAL EXTERNAL

Integrating Strategy- Culture – [New Initiative/ Service]
External Environment:Politico - LegalEconomic - FinancialSocio - CulturalTechnology - ICTPhysical - Climate
Healthcare
Industry
Top management articulates
New Initiative philosophy &
guiding principles
STRUCTURE STRATEGY SYSTEM
New Initiative
Policies And
Procedures
Internally
consistent?
Strategic Fit? FAR
P
E
R
F
O
R
M
A
N
C
EStyle of Leadership - TnT
Shared Values – Culture/ Brand
Staff – HCW_Resource_Capital
Skills – Competence/ Qualified
Markets
Comparative
advantage
Strategic ManagementANALYSIS OF CHANGE AND
OUTCOME
Professor Dato’ Dr Hj Abdul Rahim bin AbdullahMBBS(Medicine & Surgery, AUS); MHA(Health Management, AUS); DBA(International Business, UK); MBA(Strategic Management, UK) Public Health Physician & Consultant (Health Management)Chief Surveyor, Malaysian Healthcare Facilities & Services Accreditation Program
UNIMAS28 February 2019

Mission
– Business Domain
– Organisational Philosophy
– Key Values
– Critical Success Factors
Vision
• Goals and Result Areas– System
– Service
• Objectives, Performance Indicators and Targets– RAs and PIs
– Key RAs and Key PIs
Analysis of Change - Planning for Change
Logical Model LM
• Clear identification of goals (outcomes)
• Graphically illustrate program components, and creating one helps stakeholders clearly identify outcomes, inputs and activities
Theory of Change Model TOC
• Link outcomes and activities to explain HOW and WHY the desired change is expected to come about
TOC and LMarticulate underlying assumptions
• Both can greatly improve program design and evaluation (but in different ways)
• So what’s the problem?
• Everyone talking about TOCs and LMs, but not meaning the same thing
• Penalized by confusion when stakeholders are not sure
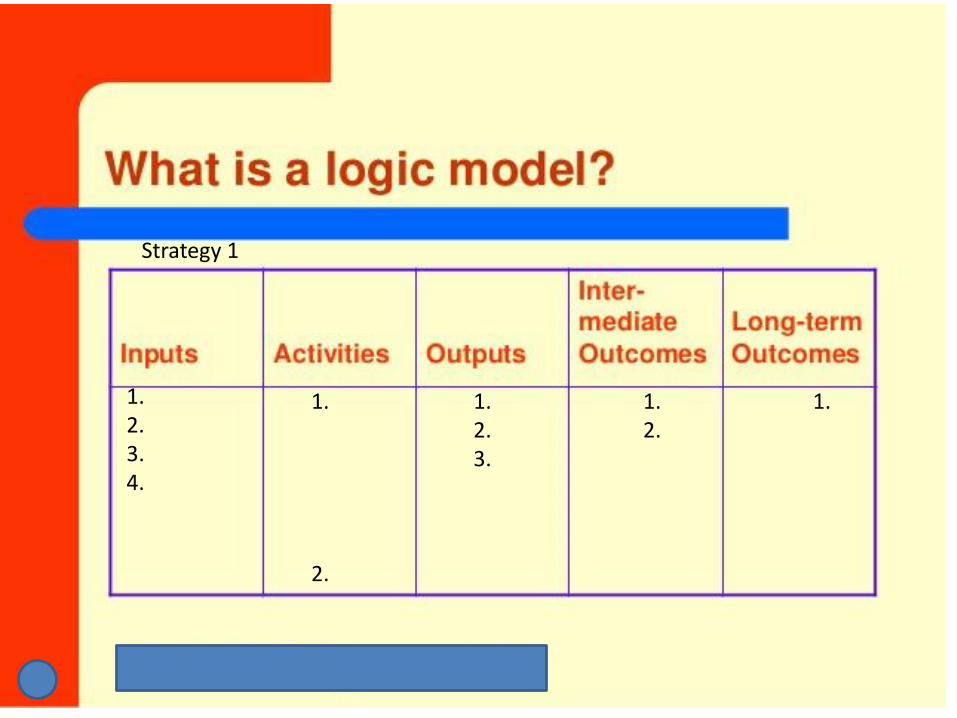
Strategy 1
1.2.3.4.
1.2.3.
1.
2.
1.2.
1.
Logic model (LM)
• Clear identification of goals (outcomes)
• First widespread attempt to depict program components so that activities matched outcomes

THEORY OF CHANGE (TOC)
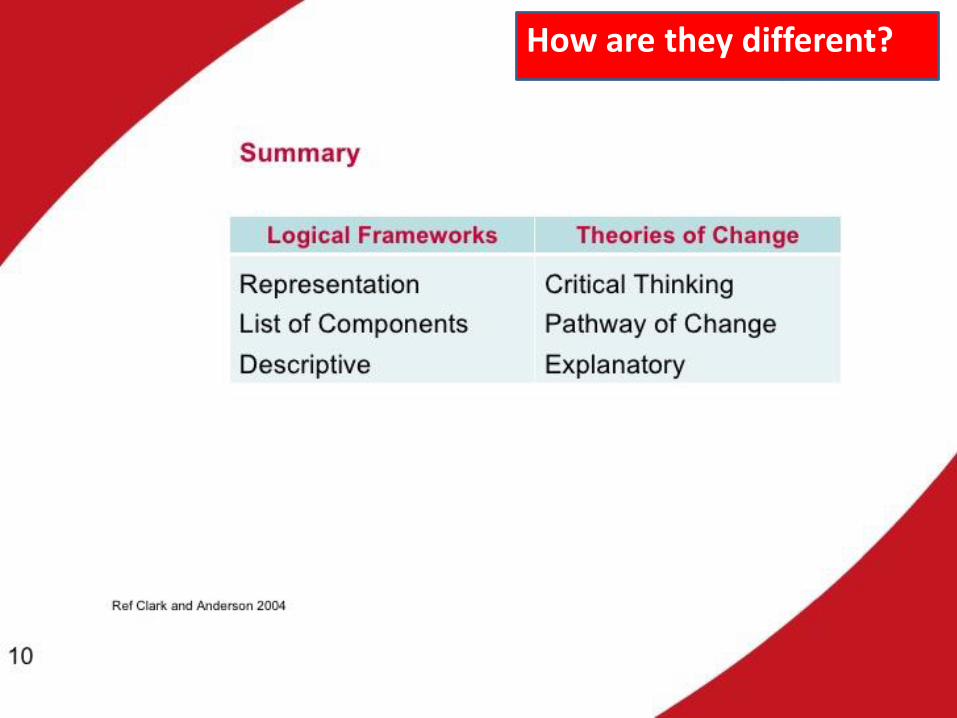
How are they different?
Logic models
• graphically illustrate program components, and creating one helps stakeholders clearly identify outcomes, inputs and activities
• usually start with a program and illustrate its components
Theories of Change
• link outcomes and activities to explain HOW and WHY the desired change is expected to come about
• may start with a program, but are best when starting with a goal, before deciding what programmatic approaches are needed
How are they different?
Logic models
• require identifying program components, so you can see at a glance if outcomes are out of sync with inputs and activities, but they don’t show WHY activities are expected to produce outcomes
• don’t always identify indicators (evidence to measure whether outcomes are met or not)
Theories of Change
• also require justifications at each step – you have to articulate the hypothesis about why something will cause something else (it’s a causal model, remember!)
• require identifying indicators WHY DOES THIS MATTER?
How are they different?
Logic models
• LM would tell you that the after school program is an activity and improved reading scores is an outcome. It might tell you that attendance at the after school program is an intermediate outcome
Theories of Change
• But LM wouldn’t tell you as TOC would that: “students need to attend after-school programs at least 3 days per week for a minimum of 60 days, and the curricula must focus on love of reading and literacy, IN ORDER FOR test scores to rise
How are they different?
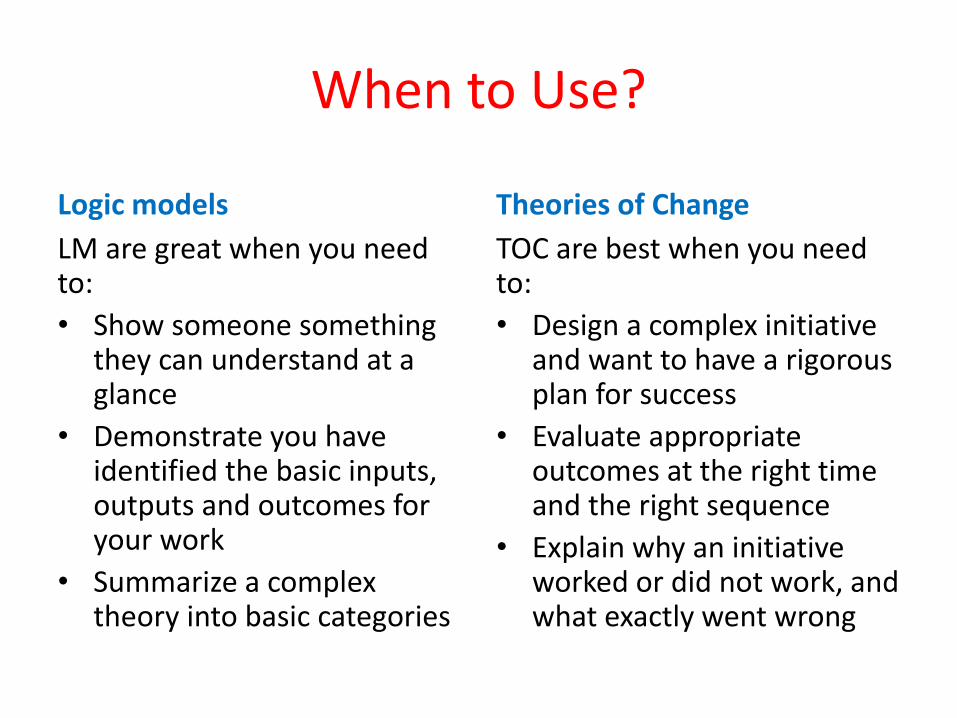
When to Use?
Logic models
LM are great when you need to:
• Show someone something they can understand at a glance
• Demonstrate you have identified the basic inputs, outputs and outcomes for your work
• Summarize a complex theory into basic categories
Theories of Change
TOC are best when you need to:
• Design a complex initiative and want to have a rigorous plan for success
• Evaluate appropriate outcomes at the right time and the right sequence
• Explain why an initiative worked or did not work, and what exactly went wrong
It’s obvious by now:
• Theories of Change are a lot of work and take time.
• On the other hand, Logic Models are often too simplistic to be helpful
So, can we have the best of both worlds?
• We suggest, Undertake a TOC process that is a manageable scope for your organization.
• Make sure you get stakeholders to articulate what has to happen IN ORDER for goals to be met and their assumptions about why
Theories of Change & Logical Model
• Then, Summarize your theory in ways that serve the purposes of your different constituents, etc.
• A Logic Model that is a summary of/ with an underlying theory is a much more powerful tool.
Addressing Barriers to Policy Implementation
Professor Dato’ Dr Hj Abdul Rahim bin AbdullahMBBS(Medicine & Surgery, AUS); MHA(Health Management, AUS); DBA(International Business, UK); MBA(Strategic Management, UK) Public Health Physician & Consultant (Health Management)Chief Surveyor, Malaysian Healthcare Facilities & Services Accreditation Program
UNIMAS28 February 2019
Key technical areas of expertise needed to effectively influence health policy design, implementation, and monitoring and evaluation
• identifies the specific skills, knowledge, and capacities that individuals and organizations should possess in the area.
• standardized indicators listed for each competency and capability map helps to generate a tailored tool for assessing and scoring an organization’s capacity level.
Policy Implementation - Relevance To Policy
• Policy implementation refers to the mechanisms, resources, and relationships that link health policies to program action. It includes both
• Technical Aspects – specifying the institutions responsible for implementation and ensuring that the institutions have the capacity for implementation
• Relational Aspects - the relations among institutions are conducive for collaboration (Hardee et al., 2012).
International experience shows that policies, once adopted, DO NOT always get implemented as envisioned and do not necessarily achieve intended results
(Bhuyan et al., 2010).
Developing a policy is just the first step
• For policies to contribute to the successful delivery of health services, they must be effectively implemented.
• Challenges to implementation are referred to as “implementation barriers.”
• They can be rooted in a variety of causes, including • opposition from key stakeholders, • inadequate human or financial resources,• lack of clarity on operational guidelines or roles and
responsibilities for implementation,• conflicts with other existing policies,• lack of coordination and collaboration between parties
responsible for implementation or• lack of motivation or political will
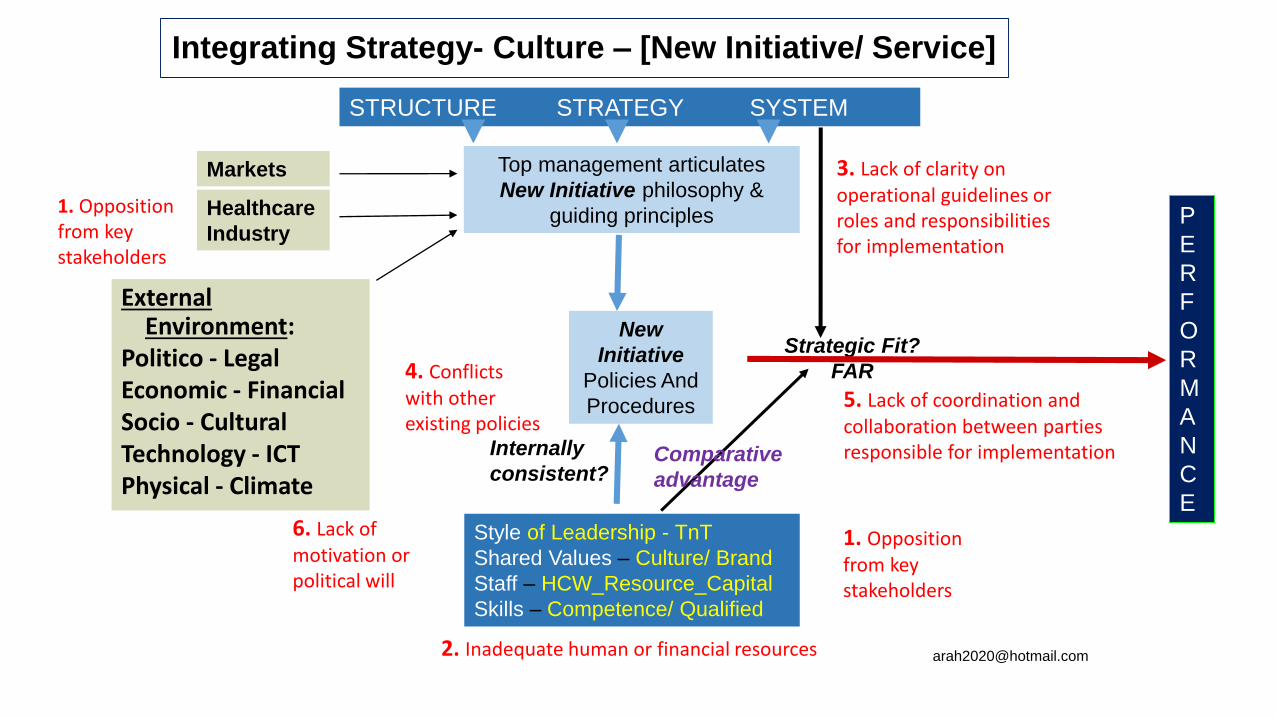
Integrating Strategy- Culture – [New Initiative/ Service]
External Environment:
Politico - LegalEconomic - FinancialSocio - CulturalTechnology - ICTPhysical - Climate
Healthcare
Industry
Top management articulates
New Initiative philosophy &
guiding principles
STRUCTURE STRATEGY SYSTEM
New
Initiative
Policies And
Procedures
Internally
consistent?
Strategic Fit?
FAR
P
E
R
F
O
R
M
A
N
C
E
Style of Leadership - TnT
Shared Values – Culture/ Brand
Staff – HCW_Resource_Capital
Skills – Competence/ Qualified
Markets
Comparative
advantage
1. Opposition from key stakeholders
2. Inadequate human or financial resources
3. Lack of clarity on operational guidelines or roles and responsibilities for implementation
4. Conflicts with other existing policies
5. Lack of coordination and collaboration between parties responsible for implementation
1. Opposition from key stakeholders
6. Lack of motivation or political will
KEY CAPABILITIES [1]To address implementation barriers
• Stakeholders must assess the root cause of the challenge and develop targeted strategies to address each barrier in collaboration with other interested and empowered parties.
• Throughout the policy development, implementation, and monitoring processes, barriers should be continually assessed and addressed.
• Implementation is an ongoing process of decision making by key actors who work in complex policy and institutional contexts and face pressures from interested as well as opposing parties.
• As such, the motivation, flow of information, and balance of power and resources among stakeholders influences policy implementation processes.
• Ultimately, overcoming policy implementation barriers will require commitment and perseverance by a range of stakeholders, possibly over a prolonged period (Bhuyan et al., 2010).

KEY CAPABILITIES [2]The ability to address policy implementation barriers
A key capability for government, policymakers, and civil society.
• Addressing policy barriers requires individual and institutional skills and competencies to understand the policy environment governing the health system, the configuration of the health system in the context of the government structure, and the needs of beneficiaries/ clients and implementers.
• Requires the ability to critically assess the true root of policy implementation barriers - whether it is sociological, political, structural, institutional, or cultural - and to craft targeted solutions to address them.
• Requires engendering stakeholder buy-in and commitment to take action, determining resources required for the proposed solution, implementing a solution to remove the barrier, and enacting accountability mechanisms to ensure that barriers have been addressed (Bhuyan et al., 2010; Cross et al., 2001).

PERFORMANCE IDEAL [1]
High capacity for addressing policy implementation barriers includes being able to
• Gather and synthesize different types of information from various sources
• Elicit feedback from implementers, partners, and beneficiaries to identify barriers to successful policy implementation and explore root causes
• Identify solutions to challenges and advocate for corrective action
• Maintain systems to facilitate regular reviews of implementation experiences, share best practices across groups, and
• Integrate lessons learned into subsequent policies and action plans
PERFORMANCE IDEAL [2]
• In a high-functioning system, the gap between policy and practice narrows and barriers to realizing results are identified and removed.
• At the highest level of performance, individuals and organizations consider (throughout the policy process) the potential roadblocks and steps to overcome them.
• Attention to barriers starts with policy design and strategic action planning and continues during policy implementation—and thus policy monitoring—to track outcomes, identify challenges, and be alert to unintended consequences or inequities.
PERFORMANCE IDEAL [3]
IDEALLY, the following would exist: • Policies translated into effective strategies, operational guidelines and rules • Efficient allocation and coordination of human and financial resources to
achieve policy goals • Regular systems to review policy and program decisions (e.g., mid- and
end-term reviews, multi-sectoral forums), with broad-based participation • Multi-directional feedback loops involving beneficiaries, implementers, and
policymakers • Mechanisms to ensure follow-up and compliance with policy directives
(e.g., national monitoring board, national policy unit, incentives for compliance, sanctions for non-compliance)
• Systemic monitoring and evaluation of the impacts of policy formulation and implementation
PERFORMANCE IDEAL [3]
In the ideal, the following would exist: • Policies translated into effective strategies, operational guidelines and rules• Efficient allocation and coordination of human and financial resources to
achieve policy goals • Regular systems to review policy and program decisions (e.g., mid- and
end-term reviews, multi-sectoral forums), with broad-based participation • Multi-directional feedback loops involving beneficiaries, implementers, and
policymakers • Mechanisms to ensure follow-up and compliance with policy directives
(e.g., national monitoring board, national policy unit, incentives for compliance, sanctions for non-compliance)
• Systemic monitoring and evaluation of the impacts of policy formulation and implementation
Individual Competencies [1]
KNOWLEDGE OF
• Local and national policy environment, laws, and the
configuration of the health system within government structures
• Specific aspects of the policy to be implemented, including
policy goals, strategies and action plans, roles of different
institutions and stakeholders, and available resources
ATTITUDES/VALUES/ATTRIBUTES
• Elicits stakeholder buy-in and commitment to ongoing engagement

Individual Competencies [2]
SKILLS TO BE ABLE TO
• Collect, analyze, and present quantitative and qualitative data to identify barriers and develop evidence-based solutions
• Engage diverse stakeholders in constructive policy dialogue to identify and address barriers at the appropriate level (national, district, facility, etc.)
• Understand the socio/political/structural/institutional/cultural root of policy implementation barriers and craft targeted solutions to address them
• Conduct cost analysis that aligns budget allocations w actual resources required to implement policies
• Draft operational policy guidance and rules to implement change
• Communicate evidence-based recommendations & influence decision-makers to take corrective action.
• Monitor and document the policy implementation process and impact of adopted solutions
Organizational Capabilities [1]
TECHNICAL ABILITY TO
• Develop implementation plans that include clearly defined policy goals, strategies, action plans, monitoring mechanisms, and operational guidelines
• Integrate best practices and successful approaches to overcoming barriers into organizational and decision-making processes
RELATIONAL ABILITY TO
• Leverage multi-sectoral partnerships and resources to collectively address complex barriers at the appropriate level and facilitate implementation (national, district, facility, etc.)
• Provide training, technical assistance, and mentoring to other organizations on addressing implementation barriers
Organizational Capabilities [2]
ORGANIZATIONAL OPERATIONS AND MANAGEMENT TO SUPPORT - CONTROL / INFLUENCE
• A knowledge management system to share best practices in policy implementation and lessons learned internally and externally
• Regular interactions among staff responsible for program implementation, monitoring and evaluation, and management
• Allocation of sufficient resources (time, money, staff) for policy implementation and regular reviews and monitoring of the implementation process
• Allocation of resources required to take corrective actions to alleviate identified barriers and/or communicate recommended action for other organizations

Organizational Capabilities [2]
ORGANIZATIONAL OPERATIONS AND MANAGEMENT TO SUPPORT - CONTROL / INFLUENCE
• A knowledge management system to share best practices in policy implementation and lessons learned internally and externally
• Regular interactions among staff responsible for program implementation, monitoring and evaluation, and management
• Allocation of sufficient resources (time, money, staff) for policy implementation and regular reviews and monitoring of the implementation process
• Allocation of resources required to take corrective actions to alleviate identified barriers and/or communicate recommended action for other organizations
Organizational Capabilities [3]
ORGANIZATIONAL OPERATIONS AND MANAGEMENT TO SUPPORT - CONTROL / INFLUENCE
• Roll out of new policy directives throughout the organization along with adequate training, supervision, resources, and support for their implementation
• Systems to routinely collect and analyze quantitative and qualitative data from various sources (e.g., periodic assessments, activity appraisals, client satisfaction surveys) and stakeholders (beneficiaries, implementers, and policymakers)
• Mechanisms to ensure compliance with policy directives and understand incentives for compliance as well as sanctions for non-compliance

Organizational Capabilities [3]
ORGANIZATIONAL OPERATIONS AND MANAGEMENT TO SUPPORT - CONTROL / INFLUENCE
• Roll out of new policy directives throughout the organization along with adequate training, supervision, resources, and support for their implementation
• Systems to routinely collect and analyze quantitative and qualitative data from various sources (e.g., periodic assessments, activity appraisals, client satisfaction surveys) and stakeholders (beneficiaries, implementers, and policymakers)
• Mechanisms to ensure compliance with policy directives and understand incentives for compliance as well as sanctions for non-compliance

CAPACITY - STRENGTHENING
ILLUSTRATIVE CAPACITY - STRENGTHENING ACTIVITIES [1]
• Provide technical assistance on• systems and process analysis for anticipating and mitigating against
potential roadblocks during the policy formulation and action planning processes
• monitoring and evaluation plans that track both outcome and process indicators, including qualitative and contextual information
• Support costing exercises that encourage aligning budget allocations with the actual resources required to implement policies and programs
• Train local decision-makers (e.g., district health officials) on operational policy issues and tools and techniques to analyze barriers
ILLUSTRATIVE CAPACITY - STRENGTHENING ACTIVITIES [2]
• Policy monitoring tool or checklist - assist a multi-sectoral team of stakeholders to adapt and apply a proven
• Establishment of feedback mechanisms to gather information from as well as report back to implementers and beneficiaries
• Lessons learned - incorporate systems to document and share these into organizational capacity development plans
• Carry out annual or mid-term reviews and integrate findings - assist government and other stakeholders towards developing subsequent action plans
Ethical Standards in Program Evaluation
DR. ABDUL RAHIM ABDULLAHMBBS (UQLD, AUS); MHA (UNSW, AUS)
DBA (UWCC, UK); MBA (CARBS/UW, UK)

Policy, Planning & Evaluation: Ethical issues
1. Health measurements (inputs, activities-process, outputs, outcomes) and valuation are key issues in health care planning and evaluation
2. The nature of the commodity health care means that health care markets may not function in the same way as markets for other commodities
3. There is more to financing health care than money
4. Knowledge of morbidity and mortality is not enough when it comes to priority setting.
5. Economic appraisal makes for better decision-making both within the health care sector and in other sectors which can affect health
6. We cannot assume efficiency; it needs to be encouraged
7. Improving equity is an important objective of health care; but reducing inequalities come at a price

Strategy 1
1.2.3.4.
1.2.3.
1.
2.
1.2.
1.

Individual Behavior – Consumers, Provides
• -Health Promotion
• -Service Use
• -Information
• -Persuasion
• -Regulation
• -Incentives
• What
• How
Doctors – Supply
- ”Agency” problem. - Clinical ambiguity. - Professional organization. - Licensing limits.- Fee Schedule.- Social authority. - Long training.
- Locational preferences.
Patients – Demand
- Anxiety.
- Ignorance.
- Deference.
- Placebo effect.
- Non-compliance.
- Care about, cannot judge, technical quality
- Prefer action to advice.
1. Measurement: Health measurement, evaluation, and Value Judgements
Learning Objective
Health output measurements and valuation
are key issues in health care planning and
evaluation
Analysts (policy, market, economic) see a health care system as an organization (or firm) that
produces outputs or outcomes such as health.
• What is “health”?
• Can we measure outputs of different services?
• Can we value these outputs?
• Whose “values” are relevant?
• Can we improve on existing measurements and valuations of health outputs?

• The nature and magnitude of the problems in measuring health is apparent. However, we do not want to reject, e.g. health status, measurements totally.
• Even though ideal measurements are difficult, we will find it much easier to make improvements on existing measurements of health.
Health measurement and evaluation
• It is legitimate to have disagreement between individuals, groups or even countries in answering the question “whose values” and the “concept of need” in health care.
• Discussions and clarifying the question and answers may be more important than to get consensus agreement.
• It is not the intention of economists to force one set of values on everyone – or indeed any one person or country.
• It may be a matter of politics at this stage to gain understanding rather than approval.
2. Value Judgements
• The need to measure and value health outputs arises because resources for health improvement are scarce
• Choices have to be exercised as to which outputs to produce and to what extent and which health improvement opportunities to forgo.
Value Judgements
3. Health output measurement is difficult because
3.1 health is multidimensional; it varies in terms of pain, physical disability, mental impairement; by severity; by duration; etc;
3.2 health is a value-laden concept; for example, the loss of health status of a broken leg will differ between a professional footballer and a health economist;
3.3 the reasons for wanting to measure health are many and appropriate measurement will vary depending on the reason.
4. Some reasons for wanting to measure health include:
4.1 international comparisons of populations and/or health care systems;
4.2 evaluating and planning of services, research, clinical practice, etc.;
4.3 measurement of inequalities in health e.g. geographically and by social class.
5. There are very real difficulties in measuring health but it has to be
remembered that
5.1 health measurements are currently done badly and that, it is not perfection that is sought, merely improvements;
5.2 health measurements cannot be escaped.

6. Some of the major underlying problems in health care revolve around questions of valuation
of outputs, in particular:
6.1 whose values -- consumers’, politicians’, the medical practitioner’s, the medical profession’s, etc. -- are relevant to which decisions?
6.2 what methods are available to us to place values on health outputs (e.g. the human capital approach)?
6.3 what is the need for health care and how does it relate to the demand for health care?
7. ‘Needology’ has almost become a science in itself. The concept of need has been defined in many different ways.
Economists (at least) would argue that
7.1 need is relative not absolute (e.g. some needs if met will yield greater benefit than others);
7.2 need should be seen as dynamic not static (e.g. meeting some needs may breed others to be met);
7.3 the concept of ‘total need’ is at best unhelpful and that concentrating on marginal need (i.e. meeting a little more or a little less need than at present) may be more important; and
7.4 decisions on resource allocation should be based not only on the benefit of meeting need (particularly marginal need) but also the costs of meeting need and to differing extents.

Efficiency, Equity and Quality:Competing goals in health and health care
• Equity is an important objective in all health care systems and indeed was instrumental in establishing some of them.– How can equity and inequity be defined?
– Can inequality be measured?
– In what ways can inequalities be reduced between geographical areas or social classes?
– Who utilizes health care?
– The trade off between equity and efficiency is also considered in this topic
Main Message:
• Improving equity is an important objective of health care; but reducing inequalities come at a price

Again students may come with preconceived , probably somewhat vague, ideas about equity.
• Clarification of differences between different concepts of equity and the implications of choosing different definitions are important factors, at least initially. For example, there may well be some confusion about the distinction between equality of access and equality of utilization.
• Measurement issues too are important but ought not be allowed to dominate to the exclusion of debate about principles of equity.
• The equity-efficiency trade-offs is both important and sometimes difficult to get over to students.

1. The nature of health care as a commodity, particularly the ‘caring externality’, suggests that equity may be an appropriate pursuit of a health care system.
Whether it is or not will almost certainly be an ideological/political choice.
2. The definition of equity is fraught with difficulty and the concept is frequently surrounded by lack of clarity.
Explicitness in defining equity can help in policy-making regarding equity. Possibilities include:
i. equality of inputs for equal need;
ii. equality of access for equal need;
iii. equality of utilization for equal need; and
iv. equal health.

The most common dimensions of equity are by:
1. social class;
2. geographical areas (i.e. regions); and
3. spatial distribution of population
3. While horizontal equity (equal treatment of equals) may foster efficiency this is normally not true of vertical equity (the unequal treatment of unequals). In the latter case equity is ‘traded-off’ against efficiency.
4. There are problems in defining and/or measuring
• social class/groups;
• inequalities in health care access;
• inequalities in health care utilization;
• inequalities in health.
Nonetheless various exercises have been undertaken in different countries to measure health and health care inequalities.
5. The use of economics in setting priorities does not necessarily conflict with medical
ethics, provided that
• 1. Medical ethics accept the need for efficient resource use;
• 2. Economics can embrace the values of medical ethics.

Let us now look at priority considerations in, for example, idealised
- Public Health Systems- Private Health Systems

PRIORITY SETTING IN “IDEALISED” HEALTH CARE SYSTEM: PUBLIC vs. PRIVATE PERSPECTIVES
PRIVATE
(? LIBERTARIAN)
PUBLIC
(? RIGID UTILITARIAN)
DEMAND 1. Individuals are best judges of
their own welfare
2. Priorities are determined by
own willingness and ability to
pay
3. Erratic and potentially
catastrophic nature of
demand mediated by private
insurance
4. Matters of equity to be dealt
with elsewhere (e.g. in the
tax and social security
systems)
1. When ill, individuals, individuals are
frequently imperfect judges of their
own welfare
2. Priorities are determined by socials
judgements about needs
3. Erratic and potentially catastrophic
nature of demand made irrelevant
by provision of free (or relatively
free) services
4. Since the distribution of income
and wealth unlikely to be equitable
in relation to the need for health
care, the system must be
“insulated” from its influence

SUPPLY 1. Profit is the proper and
effective way to motivate
suppliers to respond to
the needs of demanders
2. Priorities are determined
by people’s willingness
and ability to pay and by
the costs of meeting
their wishes at the
margin
3. Suppliers have strong
incentive to adopt least-
cost methods of
provision and delivery of
services
1. Professional ethics and
dedication to public service
are the appropriate
motivation, focusing on
success in curing or caring
2. Priorities determined by
where the greatest
improvements in caring or
curing can be affected at
the margin
3. Predetermined limit on
available resources
generates a strong
incentive for suppliers to
adopt least-cost methods of
provision
PRIVATE
(? LIBERTARIAN)
PUBLIC
(? RIGID UTILITARIAN)
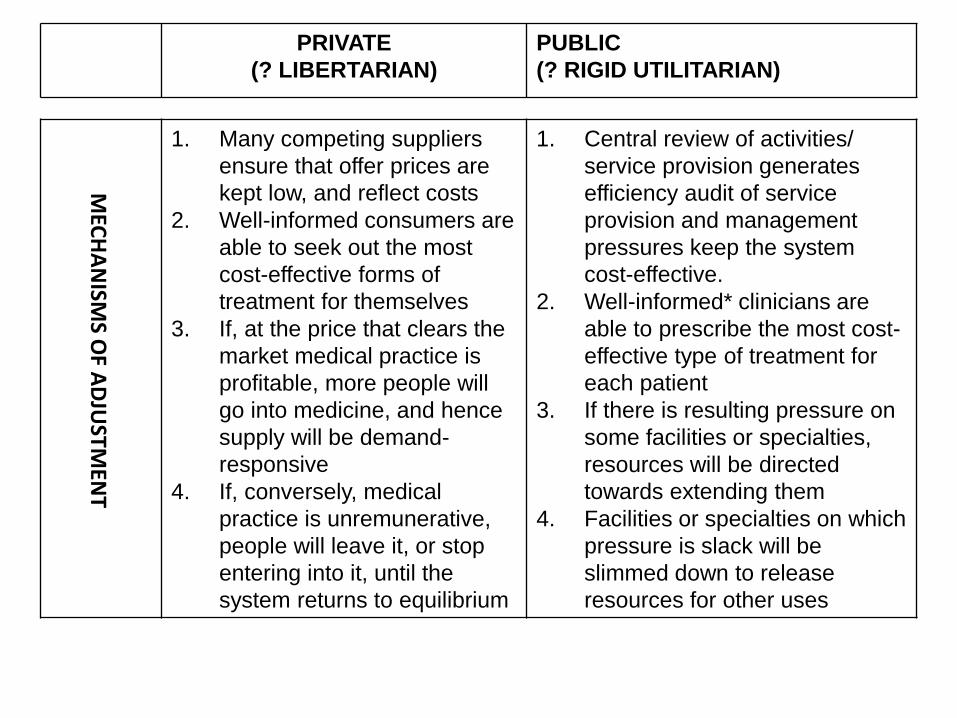
PRIVATE
(? LIBERTARIAN)
PUBLIC
(? RIGID UTILITARIAN)
1. Many competing suppliers
ensure that offer prices are
kept low, and reflect costs
2. Well-informed consumers are
able to seek out the most
cost-effective forms of
treatment for themselves
3. If, at the price that clears the
market medical practice is
profitable, more people will
go into medicine, and hence
supply will be demand-
responsive
4. If, conversely, medical
practice is unremunerative,
people will leave it, or stop
entering into it, until the
system returns to equilibrium
1. Central review of activities/
service provision generates
efficiency audit of service
provision and management
pressures keep the system
cost-effective.
2. Well-informed* clinicians are
able to prescribe the most cost-
effective type of treatment for
each patient
3. If there is resulting pressure on
some facilities or specialties,
resources will be directed
towards extending them
4. Facilities or specialties on which
pressure is slack will be
slimmed down to release
resources for other uses
MEC
HA
NISM
S OF A
DJU
STMEN
T

PRIVATE
(? LIBERTARIAN)
PUBLIC
(? RIGID UTILITARIAN)
# principles and what type of mechanisms by experts*Are we well-informed? How much information is necessary to be well-informed?
CRITERIA
OF
SUCCESS
1. Consumers will judge the
system by their ability to
get someone to do what
they demand, when,
where and how they want
it
2. Producers will judge the
system by how good a
living they can make out
of it
1. Electorates judge the
system by the extent to
which it improves the health
status of the population at
large in relation to the
resources allocated to it
2. Producers judge the system
by its ability to enable them
to provide the treatment they
believe to be most cost-
effective
From A. Williams – (undated)Priority Setting in Private and Health Care Centre of Health Economics, Univ. of York

Ethical Standards in Policy Evaluation
Dr Zafar AhmedMBBS, MBA, M Econ. PhD
5th UNIMAS Public Health Seminar 2019
Post Conference Workshop: 28th February 2019
Computer Lab, Faculty of Medicine & Health Sciences, UNIMAS
Policy Evaluation Measures: Objective Vs Subjective (Ethical)
standards

Presentation Overview
• What is Evaluation
• Assessment Vs Evaluation
• Evaluation Types
• Evaluation Perspectives
• Morality and Ethics
What is Evaluation
• The systematic investigation of the merit, worth, or significance of an ‘object’
• A rigorous process aiming at providing a structured judgement on a health program, a policy, a process or a project to assist decision-making
• The systematic assessment of the operation and/or outcomes of a program or policy, compared to a set of explicit or implicit standards as a means of contributing to the improvement of the program or policy
When to Conduct Evaluation?
Conception Completion
Planning a NEW Policy
Assessing a DEVELOPINGPolicy
Assessing a STABLE, MATURE Policy
Assessing a Policyafter it has implemented
The stage of Policy development influences the reason for
Policy evaluation.
Types of Policy Evaluation
• Process Evaluation
• Outcome Evaluation

Process Evaluation
• Process evaluation or evaluation of Policy implementation
• Focus on PROCESS: • Degree of the implementation,
• Quality of the implementation,
• Barriers,
• Facilitating factors
Process Evaluation
• Focus on PROCESS:
• Process • Focus on quality vs. implementation
• Focus on the gap between what was done vs. planned
Outcome evaluation
• Focus on RESULTS: looks at the program in terms of its results
• So we Question such as:
• Has the program Made a difference in attitudes, believes, knowledge, behaviour, skills, health status or well- being of the participants?
Policy Evaluation Perspectives
Three perspectives
• Organization’s perspective
• Funding agency and/or public’s perspective
• Evaluator’s perspective
What is Ethics
• Also called “Moral Philosophy”
• It deals with what is morally good and bad, right and wrong
• It refers to well-founded standards of right and wrong that prescribe what humans ought to do, usually in terms of: • rights, • obligations, • benefits to society, • fairness, or • specific virtues
• Ethics refers to the study and development of one's ethical standards.
• Feelings, laws, and social norms can deviate from what is ethical.

Ethics Review
• Morals: Rules that define what is right and wrong
• Ethics-process of examining moral standards and looking at how we should interpret and apply such standards in real world situations

Evaluation Ethics…
• Involves the application of fundamental ethical principles to
• planning,
• conducting
• Evaluating &
• publishing of Policy evaluation
Principles for doing Ethical Policy evaluation
• Ethical dilemmas during and after the Policy evaluation• Who own the Policy & assets?
• Who owns the data?
• Whose interpretation counts?
• Who has veto power?
• What are the evaluator’s obligations after the evaluation data are collected?
• Can the data be used against the Policy objective?
• Will the data be used on their behalf?
• Do evaluators have an obligation to protect the communities and the social groups they study or just to guard the rights of individuals?
Principles for doing Ethical research
• The relationship between society and science.
• Making Decisions to Maximize Benefit and Minimize Risk• Think about the consequences of doing a given study as opposed to not doing
the study
• Consider all options and methods to find a research strategy that balances being ethical, being practical, with the likelihood of obtaining good quality data
Assure That Benefits Outweigh Risks
• Evaluator must be justified on the basis of a favorable benefit/risk assessment for the evaluation. Benefits must outweigh risks.
• This is similar to the principal of beneficence or “do no harm.” Researchers must protect participants from harm and maximize their well-being.
The evaluator’s Own Ethics
• The ultimate responsibility lies with the investigator, it’s you who make decision about the ethics of research. It’s up to you who judge what is wrong and what is right.
• Consider carefully the costs and benefits of conducting or not conducting current research
• Try to take participants’ point of view
Ethics
• Ethics – principles for guiding decision making and reconciling conflicting values• People may disagree on ‘ethics’ because it is based on people's personal value
systems
• What one person considers to be good or right may be considered bad orwrong by another person
Measurement: Health measurement, evaluation, and Value Judgements
Analysts (policy, market, economic) see a health care system as an organization (or firm) that produces outputs or outcomes such as health.
• What is “health”?
• Can we measure outputs of different services?
• Can we value these outputs?
• Whose “values” are relevant?
• Can we improve on existing measurements and valuations of health outputs?

• The nature and magnitude of the problems in measuring health is apparent. However, we do not want to reject, e.g. health status, measurements totally.
• Even though ideal measurements are difficult, we will find it much easier to make improvements on existing measurements of health.
Health measurement and evaluation
• It is legitimate to have disagreement between individuals, groups or even countries in answering the question “whose values” and the “concept of need” in health care.
• Discussions and clarifying the question and answers may be more important than to get consensus agreement.
• It is not the intention of economists to force one set of values on everyone – or indeed any one person or country.
• It may be a matter of politics at this stage to gain understanding rather than approval.
2. Value Judgements
• The need to measure and value health outputs arises because resources for health improvement are scarce
• Choices have to be exercised as to which outputs to produce and to what extent and which health improvement opportunities to forgo.
Value Judgements
3. Health output measurement is difficult because
3.1 health is multidimensional; it varies in terms of pain, physical disability, mental impairement; by severity; by duration; etc;
3.2 health is a value-laden concept; for example, the loss of health status of a broken leg will differ between a professional footballer and a health economist;
3.3 the reasons for wanting to measure health are many and appropriate measurement will vary depending on the reason.
4. Some reasons for wanting to measure health include:
4.1 international comparisons of populations and/or health care systems;
4.2 evaluating and planning of services, research, clinical practice, etc.;
4.3 measurement of inequalities in health e.g. geographically and by social class.
5. There are very real difficulties in measuring health but it has to be remembered that
5.1 health measurements are currently done badly and that, it is not perfection that is sought, merely improvements;
5.2 health measurements cannot be escaped.
6. Some of the major underlying problems in health care revolve around questions of valuation of outputs, in particular:
6.1 whose values -- consumers’, politicians’, the medical practitioner’s, the medical profession’s, etc. -- are relevant to which decisions?
6.2 what methods are available to us to place values on health outputs (e.g. the human capital approach)?
6.3 what is the need for health care and how does it relate to the demand for health care?
