pocket guide - getinge login this pocket guide has been produced with the aim of providing a brief...
TRANSCRIPT

POCKET GUIDE
NAVA


Table of contents
4|Introduction15|Background and basic concepts2
13|Starting and running NAVA323|Optimizing the NAVA level425|Example of a weaning procedure528|Alarms and messages632|NAVA features and management tips739|Glossary and definitions841|References9
31.3
CONTENTS

IntroductionThis pocket guide has been produced with the aim of providing abrief and handy introduction to the mode of ventilation known asNeurally Adjusted Ventilatory Assist (NAVA). Based as it is onrespiratory physiology, NAVA gives the user access to informationconcerning both the patient’s ability to breathe and the status of thecentral nervous system.
The main focus of this booklet has thus been to explain in simpleterms the physiological background and distinctive features of NAVAwhile providing easy-to-follow instructions. More information isprovided elsewhere, for example in training material, while operatinginstructions and technical information are covered in the appropriateUser or Service Manuals for the SERVO-i ventilator.
While every effort has been made to keep this presentation as simpleas possible, some technical terms, specialized information andunfamiliar abbreviations are unavoidable. These are explained in thedefinitions and glossary at the back.
41.3
INTRODUCTION

Physiological background to NAVANAVA – Neurally Adjusted Ventilatory Assist – is an optional modeof ventilation for the SERVO-i ventilator. NAVA delivers assist inproportion to and in synchrony with the patient’s respiratory efforts,as reflected by the Edi signal. This signal represents the electricalactivity of the diaphragm, the body’s principal breathing muscle.
The NAVA option comprises the following parts:
1. NAVA software option – if not already factory-installed, thesoftware can be installed using a PC Card.
2. Edi Module3. Edi Cable4. Edi Catheter
51.3
BACKGROUND AND BASIC CONCEPTS
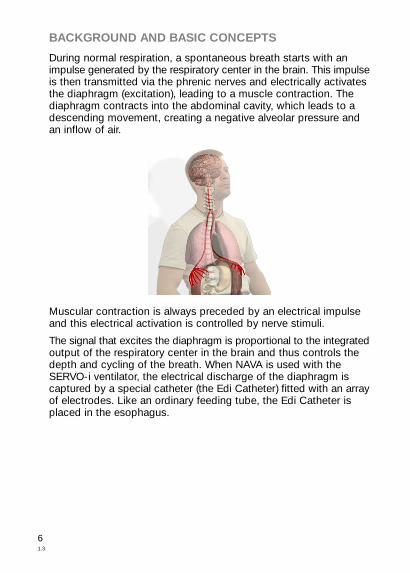
During normal respiration, a spontaneous breath starts with animpulse generated by the respiratory center in the brain. This impulseis then transmitted via the phrenic nerves and electrically activatesthe diaphragm (excitation), leading to a muscle contraction. Thediaphragm contracts into the abdominal cavity, which leads to adescending movement, creating a negative alveolar pressure andan inflow of air.
Muscular contraction is always preceded by an electrical impulseand this electrical activation is controlled by nerve stimuli.
The signal that excites the diaphragm is proportional to the integratedoutput of the respiratory center in the brain and thus controls thedepth and cycling of the breath. When NAVA is used with theSERVO-i ventilator, the electrical discharge of the diaphragm iscaptured by a special catheter (the Edi Catheter) fitted with an arrayof electrodes. Like an ordinary feeding tube, the Edi Catheter isplaced in the esophagus.
61.3
BACKGROUND AND BASIC CONCEPTS

1. Edi Catheter (with electrodes marked in black – the first is thereference electrode, the others are measuring electrodes andthe distance between the measuring electrodese is the InterElectrode Distance or IED)
2. Esophageal wall3. Diaphragm4. Stomach
The electrical activity of the diaphragm (Edi) is captured by theelectrodes and relayed to the SERVO-i, which displays it and deliversassist in proportion to the measured Edi.
Basically, NAVA uses the Edi signal to control the ventilator andassist the patient’s breathing in proportion to his own effort.
71.3
BACKGROUND AND BASIC CONCEPTS

Basic NAVA conceptsNAVA compared with traditional mechanical ventilation
The Edi signal that is picked up by the electrodes on the Edi Catheteris filtered and processed by the Edi Module. The Edi signal ismeasured 62.5 times per second. The processed Edi signal is relayedto the SERVO-i ventilator which will, depending on the NAVA levelchosen, then deliver assist to the patient in proportion to and insynchrony with the Edi signal.
An example of an Edi curve is given in the diagram below for a singlepatient breath. The blue lines represent Edi signals, sampled at arate of 62.5 times per second.
Edi (
μV)
531 Time (s)
At the set trigger level, the ventilator will start to deliver assist inproportion to the Edi signal. NAVA is triggered by an increase in Edifrom its lowest value, known as Edi min, rather than a specific Edilevel. In the diagram below, the Edi min is 0.2 µV and the trigger level0.5, which means that NAVA will be triggered at an absolute level of0.7 µV.
81.3
BACKGROUND AND BASIC CONCEPTS

Time (s)
2
10.7
0.2
Edi (
μV
)
Trigger level0.5 μV above Edi min
NAVA also employs the pneumatic trigger, based on flow or pressure,as a secondary source. In combination with the Edi trigger, thisoperates on a first-come-first-served basis.
The ventilator will continue to “amplify” each of the subsequentmeasured Edi signals (the blue lines in the diagram). The pressuredelivered is thus derived from the following formula:
NAVA level x (Edi signal – Edi min) + PEEP
The “amplification” depends on the selected NAVA level and resultsin a smoothly rising pressure curve to the patient.
This curve follows the Edi signal pattern until the Edi signal has fallento 70 % of its peak value, when the patient is allowed to exhale andthe ventilator no longer offers any assist until the next breath isinitiated and the trigger level is again reached. In this example, theresult is the type of pressure curve seen in the illustration below.
When presented on the user interface, these curves can be seen atthe top (pressure) and bottom (Edi) of the screen shot detail below.
91.3
BACKGROUND AND BASIC CONCEPTS

Time (s)
P
Time (s)
PEEP
0.70.2
Edi (
μV
)
Trigg
531
70% of Edi peak
70 %100 %
101.3
BACKGROUND AND BASIC CONCEPTS

The Edi signal can be monitored in all modes of ventilation, invasiveand non-invasive, as well as in Standby (shown below), includingvalues for both Edi peak and Edi min.
In Standby, the values are also trended, enabling the user to followthe Edi trend even if the patient has been extubated.
111.3
BACKGROUND AND BASIC CONCEPTS

The NAVA level
The NAVA level is the factor by which the Edi signal is multiplied toadjust the amount of assist delivered to the patient. This assist isthus proportional to the patient’s Edi and as such, it follows aphysiological pattern.
The NAVA level varies for different patients since they require differentassist levels. It may also need adjusting over time in the same patient.The NAVA level is typically set to between 1.0 and 4.0 cmH20/µV.
The diagram below shows the principles behind how the Edi signalcombines with the chosen NAVA level to affect the delivered pressure.
Time
20
10
μV
Trigg
P
Time
10
20
50
40
30
0
P
Time
10
20
50
40
30
0
50
40
30
Edi signalEdi peak 22 µVEdi min 0.2 µV
NAVA level 1Set PEEP 10 cmH
2O
Estimated P peak 31.8 cmH2O
((22-0.2)x1+10=31.8)
NAVA level 2Set PEEP 10 cmH
2O
Estimated P peak 53.6 cmH2O
((22-0.2) x 2+10=53.6)
The NAVA level should always be adjusted and finetuned in smallsteps and one method of optimizing it is described in greater detailin chapter 4.
121.3
BACKGROUND AND BASIC CONCEPTS

The information below covers the procedures involved in startingand running the NAVA mode. It is divided into two sections, eachfollowed by a brief summary.
Positioning the Edi Catheter• Select the appropriate Edi Catheter for the patient, depending onweight and height.
• Insert the Edi Module into the SERVO-i and connect the Edi Cable.
• Perform the Edi Module function check.
• Measure the distance from the bridge of the Nose (1) to the Earlobe(2) and then to the Xiphoid process (3). This is the NEX measurement.Make a note of it.
1
2
3
131.3
STARTING AND RUNNING NAVA

• Calculate the insertion distance (Y) for the Edi Catheter. This willdepend on whether the Edi Catheter is inserted orally or nasally, aswell as on the size of the Edi Catheter. Use the appropriate table asshown below.
Insertion distance Y for nasal insertion
Calculation of YFr/cm
NEX cm x 0.9 + 18 = Y cm16 Fr
NEX cm x 0.9 + 15 = Y cm12 Fr
NEX cm x 0.9 + 18 = Y cm8 Fr 125 cm
NEX cm x 0.9 + 8 = Y cm8 Fr 100 cm
NEX cm x 0.9 + 3.5 = Y cm6 Fr 50 cm
NEX cm x 0.9 + 2.5 = Y cm6 Fr 49 cm
Insertion distance Y for oral insertion
Calculation of YFr/cm
NEX cm x 0.8 + 18 = Y cm16 Fr
NEX cm x 0.8 + 15 = Y cm12 Fr
NEX cm x 0.8 + 18 = Y cm8 Fr 125 cm
NEX cm x 0.8 + 8 = Y cm8 Fr 100 cm
NEX cm x 0.8 + 3.5 = Y cm6 Fr 50 cm
NEX cm x 0.8 + 2.5 = Y cm6 Fr 49 cm
141.3
STARTING AND RUNNING NAVA

• Dip the Edi Catheter into water for a few seconds and insert it tothe Y value calculated above. Do NOT use lubricants as this maydestroy the Edi Catheter coating and interfere with the measurementof the Edi signal.
• Connect the Edi Catheter to the Edi Cable.
• To confirm the position of the Edi Catheter, open the “Neuralaccess” menu and select “Edi Catheter positioning”.
• Verify the position of the Edi Catheter by analyzing the ECGwaveforms. Ideally, P and QRS waves are present in the top leads,while the P waves disappear in the lower leads, where QRS amplitudealso decreases. Check that the Edi scale is fixed and that it is setappropriately (greater than or equal to 5 µV).
• If Edi deflections (see screen shots below) are present, observewhich leads are highlighted in blue.
151.3
STARTING AND RUNNING NAVA

1 – Edi deflections
2 – blue highlights
- If the second and third leads are highlighted as shown above,secure the Edi Catheter in this position after marking the EdiCatheter at its final position and making a note of the distance incentimeters.
161.3
STARTING AND RUNNING NAVA

- If the top leads are highlighted (see below), pull out the EdiCatheter in steps corresponding to the Inter Electrode Distance(IED, measured in millimeters) until the blue highlight appears inthe center. Do not exceed four times the IED. Mark the EdiCatheter at its final position.
171.3
STARTING AND RUNNING NAVA

- If the bottom leads are highlighted (see below), insert the EdiCatheter further in steps corresponding to the IED until the bluehighlight appears in the center. Again, do not exceed four timesthe IED. Mark the Edi Catheter at its final position.
- If the Edi signal is very low, there will be no blue highlights. If thishappens, evaluate the Edi signal as described in the second pointbelow.
• Once the position has been verified, secure the Edi Catheter inposition after first checking that the marking on the Edi Catheter isin the right place and observing the ECG waveforms and their bluehighlights. Make sure that the Edi Catheter is not secured to theendotracheal tube. Record the insertion length. Always follow hospitalroutines to check the position of the Edi Catheter when it is used asa gastric feeding tube.
181.3
STARTING AND RUNNING NAVA

• Evaluate the Edi signal. Please note that sedation, muscle relaxants,hyperventilation, excessively high PEEP and neural disorders can allresult in a low or absent Edi signal, even if the Edi Catheter has beenperfectly positioned.
• If possible, perform an expiratory hold and verify that the positiveEdi deflection coincides with a negative deflection in the pressurewaveform.
• Edi Catheter positioning may be reconfirmed after 1-2 hours ifminor adjustments are necessary.
Edi Catheter positioning summarySelect Edi Catheter and measure NEX, calculating the insertiondistance, Y.Dip Edi Catheter in water and insert.Verify the position in the positioning window.Secure the Edi Catheter.
NAVA settings• To set the initial NAVA level, press “Neural access” and select“NAVA preview”.
191.3
STARTING AND RUNNING NAVA

• The gray curve then displayed on the user interface below showsthe estimated pressure based on the Edi and the set NAVA level.
• Simply press “NAVA level” and use the main rotary dial to set itappropriately. Generally, the first NAVA level tried should producethe same pressure as that used in the current ventilation mode, orperhaps slightly lower. By accepting and pressing “Close”, theselected NAVA level is saved to the NAVA ventilation mode window.
• To set the parameters for operating the NAVA mode, choose“NAVA” in the “Select ventilation mode” window. This opens the“Set ventilation mode” parameters window.
201.3
STARTING AND RUNNING NAVA

• The NAVA level displayed is the initial one saved as outlined abovefrom the “NAVA preview” window.
• The other two parameters in the “Basic” column (marked with ared ring above) are PEEP (cmH2O) and oxygen concentration (%).
• Trigg. Edi (marked with a blue ring above) has a default setting of0.5 µV (the upper limit for variable background noise) and the range0-2 µV. The value set here is the one that will trigger the ventilatorto assist the patient.
211.3
STARTING AND RUNNING NAVA

• The remaining parameters (in the yellow ring above) refer to NAVAPressure Support (NAVA (PS)) – Trigger Sensitivity, Inspiratory Cycleoff (%) and PS above PEEP (cmH2O) – as well as “Backup ventilation”– PC above PEEP (cmH2O). NAVA (PS) is the mode to which theventilator automatically switches under certain circumstances. It istherefore important to set adequate values for NAVA PressureSupport; otherwise the patient’s Edi signal may be affected and theventilator may be unable to switch back to NAVA. NAVA (PS) andBackup are described in greater detail in Chapter 7.
NAVA settings summarySelect NAVA preview via "Neural access".Adjust the NAVA level.Accept and press "Close" to save the initial NAVA level.Open the NAVA mode window and adjust settings.Set appropriate values for NAVA (PS) and NAVA Backup.Accept and proceed with NAVA ventilation. Remember to setappropriate alarm limits.
221.3
STARTING AND RUNNING NAVA

One way to optimize the NAVA levelThe method below involves a titration procedure suggested in anarticle by Brander et al (see references), which can be summarizedin brief and simple steps as follows:
1. Once a reliable Edi signal with a constant pattern andsatisfactory amplitude has been obtained, the user activatesthe NAVA preview window, setting a NAVA level such that thepressure delivered is equal to or slightly below the set PressureSupport level.
2. Set an Upper Pressure Limit that is acceptable to the patient.3. Open the Neuro Ventilatory Tool.4. In order to increase the patient’s respiratory drive while not
provoking too much distress, the NAVA level is reduced to aminimum level of 0.0 cmH2O/µV or slightly higher, resulting ina minimal level of assist. This is maintained for a few minutesor until the Edi signal reaches its maximum. During this period,the patient should be carefully observed as discomfort orhemodynamic instability may occur.
5. The NAVA level is then gradually increased in steps of 0.1 to0.2 cmH2O/µV, while observing the trend graphs for Ppeak, VTand Edi.
6. As the NAVA level increases, the P peak and VT levels will alsoincrease and the Edi will gradually decrease. Typically, an initialsteep increase in airway pressure and VT is followed by a lesssteep increase in the airway pressure and by a plateau in VT,while the Edi signal continues to decrease. When the Edireaches its minimum level, the increases in airway pressure andVT may resume.
7. When a transition from a steep to a less steep increase in airwaypressure and tidal volume becomes visible, activate the cursorand read off the NAVA level at the end of the transition zone.
231.3
OPTIMIZING THE NAVA LEVEL

8. The NAVA level at the end of the transition zone presumablyrepresents an assist level of adequate respiratory muscleunloading and should be set with the help of the "NAVA level"quick access knob. Normally, the NAVA level is set between 1and 4 cmH2O/µV. If a patient fails to react to an increase in theNAVA level, do not run NAVA.
9. Check and readjust the NAVA level at regular intervals.
Diagram from article by Lecomte, Brander et al (see references).
NAVA level optimization summaryMake sure you have a stable Edi signal in NAVA mode.Open the Neuro Ventilatory Tool and reduce the NAVA level toa minimum for a few minutes or until the Edi signal reaches itsmaximum.Gradually increase the NAVA level in steps of 0.1 to 0.2cmH2O/µV while observing P peak, VT and Edi.Set the NAVA level at which these three parameter curves reacha plateau.
241.3
OPTIMIZING THE NAVA LEVEL

One way to wean patients from NAVAThis chapter describes one procedure that can be followed whenweaning a patient from NAVA. An often overlooked fact is the timethat the patient has been on mechanical ventilation. Lengthy CMVis a good predictor of a more prolonged weaning phase, as shownamong others by Levine (see References).
When the patient is on NAVA, an objective measure of the patient’sprogress becomes available – the Edi signal. The first sign to lookfor is a decline in the Edi signal with unchanged tidal volumes. Thisrepresents an improvement in neuromuscular coupling in the sensethat diaphragm performance is unchanged at a lower level ofstimulation.
As soon as this situation is achieved, the airway pressure will belower. The patient is in effect giving us a signal that he or she is nowready to be weaned. For all practical purposes, the patient can thenbe left with an essentially unchanged NAVA level and will wean him-or herself off the ventilator, while we watch the progress in the shapeof a falling Edi signal.
The process may however be speeded up to allow earlierdisconnection from the ventilator. The procedure suggested belowis one example of how this may be done.
Standard extubation criteria should be met before weaning isattempted, as recommended by Lellouche (see References).
Extubation criteria according to Lellouche
1. P/F ratio over 2002. PEEP of 5 cmH2O or lower3. Efficient cough in patients with abundant secretion4. Epinephrine or norepinephrine infusion rate of 5 mg/h or lower5. Glasgow Coma Score over 86. Little or no sedation.
251.3
EXAMPLE OF A WEANING PROCEDURE

Weaning procedure example:1. The first sign that it is possible to wean the patient is a decline
in the Edi signal with maintained tidal volume.2. Please remember the following differential diagnosis – sedation
bolus or increase in maintenance dose of opiates/sedatives. Ifan increase in sedation is not the cause of the decline in theEdi signal, however, then the decrease provides confirmationof an improvement in neuromuscular coupling. The mechanicalefficiency of the diaphragm has improved and the patient willbe receiving less support – weaning has in effect been startedautomatically.
3. When the patient is stable and the tidal volume is unchangedwhile the Edi signal is declining or unchanged, reduce the NAVAlevel in steps of 0.1-0.2 cmH2O/µV.
4. If VT is reduced and the Edi signal increases disproportionally,go back to the previous setting. The reaction may indicate oneof the two following situations:a. The patient is not yet ready to be weaned. Allow the patient
to rest on the previous setting and try again later.b. The initial assist is too low (look for a slow upstroke in the
Edi and flow curve, and an increase in neural Ti). This iscommonly seen in COPD patients who require a high initialgas delivery in order to overcome intrinsic PEEP. Thephenomenon may actually lead to a higher peak pressureand a high Edi peak, with a lengthening of the inspiratoryphase and a shortening of expiration, thus increasingintrinsic PEEP. In such a situation, it may be wise to remainat the previous setting and allow the patient to wean him-or herself off at an unchanged NAVA level.
5. Weaning progress can be monitored by the decline in the Edisignal. When the peak pressure minus PEEP has fallen to 10cmH2O, extubation may be attempted.
261.3
EXAMPLE OF A WEANING PROCEDURE

Summary of weaning exampleWhile keeping the NAVA level unchanged, verify a decrease inthe Edi amplitude with a maintained tidal volume.Decrease the NAVA level in steps of 0.1-0.2 cmH2O/µV. Observea decrease in peak pressure minus PEEP with a maintainedtidal volume.The patient is considered to have been weaned when the peakpressure minus PEEP is 10 cmH2O.
271.3
EXAMPLE OF A WEANING PROCEDURE

High-priority alarmsAsynchrony alarm
In case of asynchrony, the ventilator will switch back and forthwithout triggering an alarm until one of the following conditions isfulfilled:
the ventilator has been in NAVA (PS) for more than 120 seconds;there have been six switches from NAVA to NAVA (PS) in the lastfive minutes.
In either case, the asynchrony alarm will be activated and themessage “Pneumatic-Edi out of synch” will appear, since themeasured Edi signal is out of phase with the pressure and flowsignals generated by the patient. There will also be a message totell the user to check the Edi Catheter position. In addition, the usershould check and if necessary adjust the trigger settings. Theventilation mode can also be changed.
When the asynchrony alarm has been activated, the ventilator willthen search for synchrony indices. As soon as synchrony isre-established, the message “Pneumatic-Edi synch restored” will bedisplayed. Press the OK button or simply wait for ten seconds, and
281.3
ALARMS AND MESSAGES

the ventilator will switch back to NAVA. You can also choose toreturn to NAVA manually by pressing the “Back to NAVA” key onthe user interface if the patient’s Edi signal is in synchrony with thepneumatic breath.
If asynchrony is still detected, a message will appear followed by aquestion, as shown in the screen shot below.
Users then need to confirm that they wish to return to NAVA.
No Edi monitoring alarm
The message “Edi monitoring not active” appears when the NAVAmode is activated without an Edi Module being connected. If thisoccurs, simply insert the Edi Module.
291.3
ALARMS AND MESSAGES

Medium-priority alarmsEdi Module alarms:
In case of disconnection, the message “Edi Module disconnected”appears when the Module is not properly inserted.In case of error, the message “Edi module error” appears to signifya hardware error. In this case, the Edi Module should beunplugged and reinserted. If this does not help, change the EdiModule and contact a service technician.
Edi Catheter alarms:
In case of connection failure, the message “No Edi Catheterconnected” appears. When this happens, the Edi Catheter shouldbe properly connected.In case of error, the message “Edi Catheter error” appears. AnEdi Module Test should then be performed and if it is successful,the Edi Catheter is to blame and should be replaced.If the Edi Catheter has been incorrectly positioned or has shiftedposition, the message “ Edi Catheter out of position” appears tosignal that the position of the Edi Catheter should be checked.
Low Edi activity alarm:
The message “low Edi activity” appears when the measured Ediactivity is low while using NAVA. When this happens, check theEdi Catheter position, and if necessary adjust the Edi triggersetting. Failing this, change to another ventilation mode.
301.3
ALARMS AND MESSAGES

Other messages"Regulation pressure limited" appears as a text message activatedduring NAVA at a level 5 cmH20 below the set Upper Pressure Limit.If you then increase the NAVA level, the ventilator will make a beepingsound to draw your attention to the message. The maximum availablepressure level is thus 5 cmH20 below the preset upper pressure limit.
311.3
ALARMS AND MESSAGES

The NAVA respiration cycleSince the Edi signal varies with each breath, the assist pressureswill vary accordingly. In summary, inspiration will start when thepatient triggers a breath and gas flows into the lungs at a varyingpressure proportional to the patient’s Edi signal.
The breath may be triggered either by the Edi or pneumatically, byflow or pressure. The assist to the patient will remain proportionalto the patient’s Edi signal. The maximum time for inspiration is 2.5seconds for adults and 1.5 seconds for infants.
Expiration begins when the pressure increases 3 cmH2O above theinspiratory target pressure, or when the Edi decreases below 70%of the peak value during ongoing inspiration (40% for low Edi signals),or if the Upper Pressure Limit is exceeded, or when the maximumtime for inspiration specified above is exceeded.
Trigger colors
T T Edi trigger indicator Flow/pressure trigger indicator
The User Interface has different trigger colors depending on howinspiration is triggered: the Edi trigger indicator is pale pink, whilethe flow or pressure trigger indicator is purple.
Using the Edi Catheter as a feeding tubeThe Edi Catheter is a single-use gastric feeding tube with an arrayof 10 electrodes (nine measuring and one reference electrode). TheEdi catheter has been validated for use for 5 days, both for feedingand when using the NAVA function.
Noting Edi Catheter insertion lengthRemember to mark the Edi Catheter at its final position and make anote of the final distance in centimeters in the hospital chart.
321.3
NAVA FEATURES AND MANAGEMENT TIPS

Switching between NAVA and NAVA (PS)The ventilator will switch to NAVA (PS) if one or more of the followingconditions are fulfilled during NAVA ventilation:
- The Edi respiratory rate differs from the pneumatic respiratoryrate by more than 25% for at least 5 s. The calculated respiratoryrates are based on the last 20 s.
- The Edi Ti/Ttot is more than 0.5, calculated over the last 20 s ifthe Edi Catheter position is classified as invalid.
- The Edi Ti/Ttot is more than 0.6, calculated over the last 20 s ifthe Edi Catheter position is classified as valid.
- The Edi Catheter is disconnected.- There is ECG leakage into the Edi signal.
Note: Pneumatic respiratory rate and Ti/Ttot are shown onthe user interface. Edi respiratory rate and Edi Ti/Ttot are notshown on the user interface.
The ventilator switches back automatically from NAVA (PS) to NAVAif the difference between the Edi-based respiratory rate and thepneumatic rate is not too large.
331.3
NAVA FEATURES AND MANAGEMENT TIPS

NAVA Backup functionThere is also a NAVA Backup function. In case of apnea with apermanently low Edi signal and no pneumatic trigger, the ventilatorwill switch to NAVA Backup (Pressure Control) after the set apneatime. The apnea time is set in the Alarm profile. Default settings arethen used for the following:
InfantAdultValues
1:2/0.5 s1:2/0.9 sI:E ratio/Ti
30 bpm15 bpmRespiratory Rate
5%/0.15 s5%/0.15 sInspiratory rise time
The apnea alarm can be set in infant mode (5-45 seconds) and inadult mode (15-45 seconds). The backup pressure level is adjustable.
341.3
NAVA FEATURES AND MANAGEMENT TIPS

SuctioningDuring suctioning, or in case of patient disconnection, it is importantto use the Suction Support function to avoid activating theasynchrony alarm (see the Alarms chapter below). The function isnot used when a closed suction system is in use.
What to do if…… there is no Edi signal, or if it is low:Check that the Edi Catheter is correctly placed and connectedby using the Edi Catheter Positioning Window. If it is, check thepatient for signs that the PS level is too high, or of hyperventilationor oversedation.… the patient is apneic:In case of apnea, the SERVO-i will automatically switch to Backupventilation, which is the Pressure Control mode. The apnea timeis set under the alarm profile.… the Edi Catheter has been accidentally removed:If the Edi Catheter is pulled out by mistake, the SERVO-i willautomatically switch to NAVA (PS).
Treating COPD patientsWhen treating COPD patients, it may sometimes be necessary toincrease the flow to ensure that the patient is both comfortable andadequately ventilated. An easy way to do this with NAVA is toincrease the assist level by switching to a higher NAVA level andchecking the values of Ppeak, Vt, RR and Edi to see if the assistlevel is adequate.
Monitoring the Edi signalThe Edi signal can be monitored in all modes of ventilation, includingEdi peak and Edi min, on a breath-by-breath basis. This enablesclinicians to follow an important respiratory parameter easily andreliably at a level not previously accessible in practical clinical work.
Edi values in standby are also trended and can be followed in thetrend graphs. The values are not sent to the monitoring system duringstandby.
351.3
NAVA FEATURES AND MANAGEMENT TIPS
The Ventilation Record CardThe Ventilation Record Card enables patient data and screen shotsto be transferred from the SERVO-i to a computer, where they canbe accessed. This feature is useful for teaching as well as fordiagnostic purposes. For more details, refer to the relevant SERVO-itraining material and user manuals.
Disconnection of the Edi ModuleIf the Edi Module becomes disconnected, the SERVO-i willautomatically switch to NAVA (PS) and an alarm will be activated.
Scale settingsIt is important to verify that the Edi scale is fixed and set appropriately(i.e. greater than or equal to 5 µV). Avoid clipping the Edi signal byimposing too low an upper limit on the scale.
NAVA and HelioxNAVA can be used together with Heliox.
TrendsTrends are extremely useful when following a patient’s progress onNAVA.
Coughing and hiccupsIf a patient is suffering from hiccups, they may trigger the ventilatorand cause a short assist delivery.
If a patient coughs, NAVA will provide assist during the inspirationphase prior to the cough, and the expiratory valve will open duringthe coughing itself. The usual safety mechanisms, such as the UpperPressure Limit, are in place to handle coughing while using the NAVAmode.
361.3
NAVA FEATURES AND MANAGEMENT TIPS
ECG “leak through”
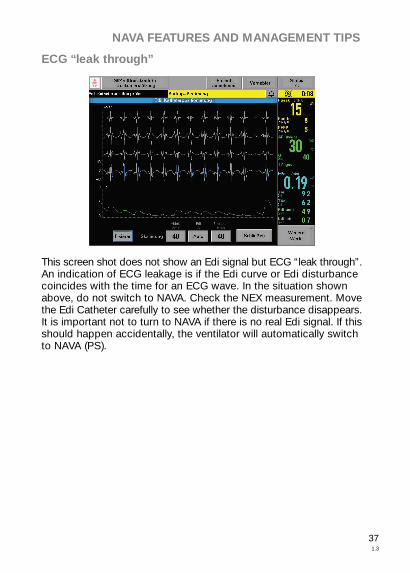
This screen shot does not show an Edi signal but ECG “leak through”.An indication of ECG leakage is if the Edi curve or Edi disturbancecoincides with the time for an ECG wave. In the situation shownabove, do not switch to NAVA. Check the NEX measurement. Movethe Edi Catheter carefully to see whether the disturbance disappears.It is important not to turn to NAVA if there is no real Edi signal. If thisshould happen accidentally, the ventilator will automatically switchto NAVA (PS).
371.3
NAVA FEATURES AND MANAGEMENT TIPS

Asynchrony
This screen shot is an example of total asynchrony. In such a case,do not switch to NAVA. The only thing to do is to start again fromthe beginning and measure the NEX carefully. Open the Edi catheterpositioning window and proceed as usual with verification beforetrying to run NAVA again.
381.3
NAVA FEATURES AND MANAGEMENT TIPS

List of termsCMV - Controlled Mechanical Ventilation.
ECG – electrocardiogram, a recording of the electrical activity of theheart.
Edi – the electrical activity of the diaphragm. Varying versions of theacronym EAdi are sometimes used to denote the same thing.
Edi peak – the highest value of the Edi signal during a single breathcycle.
Edi min – the lowest value of the Edi signal during a single breathcycle.
Fr – abbreviation for French. The French catheter scale is commonlyused to measure the outer diameter of cylindrical medical instrumentsincluding catheters. In millimeters, the diameter is equal to thenumber of French units divided by 3.
IED – inter-electrode distance, the distance in millimeters betweentwo measuring electrodes on the Edi Catheter.
MV – minute volume.
MVe – expiratory minute volume.
NAVA – Neurally Adjusted Ventilatory Assist, an optional mode ofventilation for the SERVO-i that mimics normal respiration andenhances patient-ventilator interaction.
NAVA level – the “gain factor” by which the patient’s Edi signal ismultiplied to deliver assist in proportion to the patient’s own breathingeffort.
NEX – measurement developed specifically to help with the insertionand positioning of the Edi Catheter. The distance measured is fromthe bridge of the Nose to the Earlobe and then to the tip of theXiphoid process.
P mean – mean airway pressure.
P peak – maximum inspiratory pressure.
PEEP – positive end expiratory pressure, measured in cmH20.
391.3
GLOSSARY AND DEFINITIONS

Ti/Ttot – ratio of inspiration time to total breathing cycle time.
Trigg. Edi – neurally triggered assist (i.e. triggered by the patient’sEdi signal rather than pneumatically) is triggered by an increase inthe Edi from the Edi min, rather than at an absolute level.
VT – tidal volume, i.e. the volume inspired and expired with eachnormal breath.
VTe – expiratory tidal volume.
VTi – inspiratory tidal volume.
401.3
GLOSSARY AND DEFINITIONS
ReferencesSinderby C, Beck J. Neurally Adjusted Ventilatory Assist (NAVA): AnUpdate and Summary of Experiences. Neth J Crit Care 2007:11(5):243-252.
Sinderby C, Beck J, Spahija J, de Marchie M, Lacroix J, Navalesi P,Slutsky AS. Inspiratory muscle unloading by neurally adjustedventilatory assist during maximal inspiratory efforts in healthysubjects. Chest 2007; 131(3): 711-717.
Beck J, Campoccia F, Allo JC, Brander L, Brunet F, Slutsky AS,Sinderby C. Improved synchrony and respiratory unloading byneurally adjusted ventilatory assist (NAVA) in lung-injured rabbits.Pediatr Res 2007; 61(3), 289-294.
Allo JC, Beck JC, Brander L, Brunet F, Slutsky AS, Sinderby CA.Influence of neurally adjusted ventilatory assist and positiveend-expiratory pressure on breathing pattern in rabbits with acutelung injury. Crit Care Med 2006; 34(12): 2997-3004.
Brander L, Leong-Poi H, Beck J, Brunet F, Hutchison SJ, SlutskyAS, Sinderby C. Titration and implementation of Neurally AdjustedVentilatory Assist in critically ill patients. Chest (official journal of theAmerican College of Chest Physicians), November 2008.
Lecomte F, Brander L et al.: Titration of Neurally Adjusted VentilatoryAssist (NAVA) in Rabbits; ATS 2006 Poster Board; Poster publicationpage A 142.
Levine S. et al.: Rapid Disuse Atrophy of Diaphragm Fibers inMechanically Ventilated Humans. The New England Journal ofMedicine, March 27, 2008, vol. 358 no. 13.
Lellouche F. et al.: A multicenter randomized trial of computer-drivenprotocolized weaning from mechanical ventilation. Am J Respir CritCare Med, 2006 Oct 15; 174(8): 894-900.
Emeriaud G, Beck J, Tucci M, Lacroix J, Sinderby C. Diaphragmelectrical activity during expiration in mechanically ventilated infants.Pediatr Res 2006; 59(5): 705-710.
411.3
REFERENCES

Beck J, Gottfried SB, Navalesi P, Skrobik Y, Comtois N, Rossini M,Sinderby C. Electrical activation of the diaphragm during pressuresupport ventilation in acute respiratory failure. Am J Respir Crit CareMed 2001; 164(3): 419-424.
Sinderby C, Spahija J, Beck J, Kaminski D, Yan S, Comtois N,Sliwinski P. Diaphragm activation during exercise in chronicobstructive pulmonary disease. Am J Respir Crit Care Med 2001;163(7): 1637-1641.
Sinderby C, Navalesi P, Beck J, Skrobik Y, Comtois N, Friberg S,Gottfried SB, Lindstrom L. Neural control of mechanical ventilationin respiratory failure. Nat Med 1999; 5(12): 1433-1436.
Websites:www.criticalcarenews.com
www.medicalterms.com
421.3
REFERENCES


Maquet Critical Care ABSE-171 54 Solna, SwedenPhone: +46 8 730 73 00www.maquet.com
For local contact:Please visit our websitewww.maquet.com
GETINGE Group is a leading global provider of equipment andsystems that contribute to quality enhancement and cost efficiencywithin healthcare and life sciences. Equipment, service andtechnologies are supplied under the brands ArjoHuntleigh for patienthandling and hygiene, disinfection, DVT prevention, medical beds,therapeutic surfaces and diagnostics, GETINGE for infection controland prevention within healthcare and life science and MAQUET forSurgical Workplaces, Cardiovascular and Critical Care.
© M
aque
t C
ritic
al C
are
AB
200
9. A
ll rig
hts
rese
rved
. • M
AQ
UE
T re
serv
es t
he r
ight
to
mod
ify t
he d
esig
n an
d s
pec
ifica
tions
con
tain
ed h
erei
n w
ithou
t p
rior
notic
e.O
rder
No.
MX
-046
3 •
Prin
ted
in S
wed
en •
090
318
• R
ev 0
1 E
nglis
h •
Poc
ket
Gui
de