pleural empyema caused by clostridium perfringens
TRANSCRIPT
Respiratory Medicine (1994) 88, 787-788
Pleural empyema
Case Reports
caused by Clostridium perfringens
W. G. BOERSMA*w E. J. VAN DER JAGT~, Y. HOLLOWAY3~ AND P. E. POSTMUS*
Departments of *Pulmonary Diseases and "~Diagnostic Radiology, University Hospital Groningen, and ~Department of Immunology Research, Public Health Laboratory, Groningen, The Netherlands
Introduction
Because of improved sampling and bacteriological techniques broncho-pulmonary infections due to anaerobic microorganisms are now more often rec- ognized. Clostridium perfringens, previously an important pathogen, is rarely isolated as causative microorganism in infection these days.
It is often associated with chronic disease and underlying pleuro-pulmonary pathology (i.e. tuber- culosis) is often found (1). We describe a patient with a pleural empyema caused by Clostridium perfringens, in which the interval between aspiration and the onset of pleural disease was exceptionally prolonged. Clinical symptoms were abnormally mild.
Case Report
A 62-year-old female was hospitalized with a his- tory of intermittent, slowly progressive left-sided chest pain and dyspnoea during the previous 2 weeks. There had been mild fever, and a little productive cough. Before referral she had been treated by her general practitioner with flucloxacillin and subsequently with co-trimoxazole, without any improvement.
She had not been well for the previous 5 weeks since a boil on her right thigh had been treated by incision and drainage under general anesthesia, with oro-tracheal intubation. Pus was not cultured. The patient recalled that she had been shivering the day after the operation.
She was discharged shortly after surgery with a 10-day course of antibiotics (flucloxacillin), and was advised to stay in bed for a few days. The shivering recurred several times, but subsided gradually.
Received 9 July 1992 and accepted in revised form 7 November 1992.
w to whom correspondence should be addressed at: Depart- ment of Pulmonary Diseases, University Hospital, Oostersingel 59, 9713 EZ Groningen, The Netherlands.
0954-6111/94/100787+02 $08.00/0
Her medical history revealed an 8-month stay in a sanatorium for 'pleurisy' at the age of 16. For a few years she had been suffering from chronic obstructive pulmonary disease, with symptoms of bronchial hyperreactivity.
Physical examination revealed a pale, mildly dysp- noeic female. Axillary temperature was 36~ blood pressure, 140/70 mmHg; with a regular pulse rate of 90 ra in- 1. It was noted that the patient was wearing fill dentures. Deep breathing caused left-sided chest pain. Dullness, diminished breath sounds, and fine inspiratory crackling rales were noted over the lower part of the left hemi-thorax. There were no signs of cardiac failure. The incised boil on her right thigh was healed with no signs of infiltration around the scar. Lab findings: ESR, 150mmh-1 ; WBC, 8"0 • 109 1- 1 with a normal differential count.
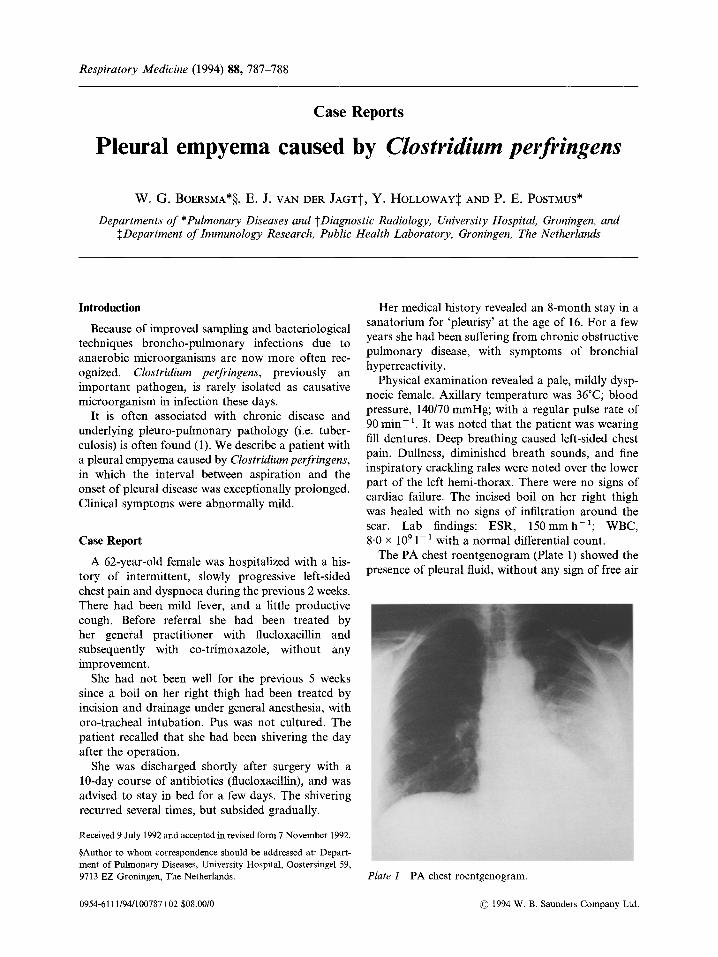
The PA chest roentgenogram (Plate 1) showed the presence of pleural fluid, without any sign of free air
Plate 1 PA chest roentgenogram.
�9 1994 W. B. Saunders Company Ltd.

788 W. G. Boersma et al.
in the pleura1 space. No infiltrates were seen. On the right side there were calcified lesions, probably due to the previous pleural tuberculosis.
Thoracentesis was performed and yielded a puru- lent yellow fluid with protein, 48g1-1 ; LDH, 14400U1-1; amylase, 154U1-~ and glucose, 0 mmol 1 1. Gram stain of the pleural fluid revealed many neutrophils and large Gram-positive bacilli. Ziehl-Neelsen staining was negative and cytological examination revealed no malignant cells. The aerobic culture of the purulent fluid, using conventional methods, did not yield pathogenic microorganisms, but the anaerobic culture yielded Clostridium
perfringens, in heavy growth. In liquid culture the microorganism produced gas.
Cultures from sputum and throat specimens as well as blood cultures were negative.
The patient was treated with 8 x 10 6 units of intravenous penicillin per day, and 2 x 106 units intrapleurally per day. A tube was inserted for pleu- ral drainage and irrigation and was kept in place for 14 days. Antibiotic treatment as described above was also continued during this period. The patient made an uneventful recovery. Later on diabetes mellitus was diagnosed by an abnormal glucose tolerance test.
Discussion
Clostridia rarely cause pleuropulmonary infections in the absence of penetrating chest injuries or thoracotomy with extensive resections. Most cases have iatrogenic causes, usually due to invasive procedures into the pleural cavity. These anaerobic bacteria are normal flora found in the faeces, and may colonize the skin by contamination. During thoracentesis or chest tube drainage clostridia may therefore be introduced into the pleural space (2).
Aspiration of oropharyngeal secretions is also a possible route for pleuropulmonary infection with clostridia species (3). These bacteria are sometimes inhabitants of the oral cavity. In a few cases, such as our patient endotracheal intubation procedures seemed to provide a route of infection (4). In patients with aspiration pneumonia, mixed infections with clostridia and other bacteria have been reported (3,5). Inhaled spores from soil dust may cause necro- tizing pneumonia and empyema (6).
Bacteraemic seeding of clostridia into the pleural space has been documented as the fourth possible route for causing empyema (7).
In contrast to tissue infections with clostridia the course of this disease is less overwhelming, but most patients are acutely ill due to fever, pleuritic pain and respiratory distress. In this case, the course of the illness was rather mild and the interval between surgery and the onset of the disease was long. Gen- erally, the interval is less than 2 weeks (1,2,5,8). The mortality rate is comparable to pleuropulmonary infections caused by aerobic bacteria. At autopsy only a mild necrosis of the infected tissues is found, in contrast to 'gasgangrene'.
An air-fluid level due to gas production may be found on the chest roentgenogram (1,8). Either intra- pleural gas production or pyopneumothorax is the reason for this roentgenological sign. Absence of gas, as found in this patient, is not an argument against this infection.
Prompt thoracentesis combined with appropriate systemic and local antibiotic therapy usually results in cure of this uncommon infection. Treatment with antitoxin or hyperbaric oxygen therapy is contro- versial, and therefore seldom used (9).
References
1. Raft M J, Johnson JD, Nagar D, Ferris FZ, McCormick ML. Spontaneous Clostridial empyema and pyopneu- mothorax. Rev Infect Dis 1984; 6: 715-719.
2. Bayer AS, Nelson SC, Galpin JE, Chow AW, Guze LB. Necrotizing pneumonia and empyema due to Clostridium perfringens. Am J Med 1975; 59: 851-856.
3. Bartlett JG, Gorbach SL, Finegold SM. The bacteriol- ogy of aspiration pneumonia. Am J Med 1974; 56: 202-207.
4. Malmborg A-S, Rylander M, Selander H. Primary tho- racic empyema caused by Clostridium sporogenes. Scand J Infect Dis 1970; 2: 155-156.
5. Goldberg NM, Rifkind D. Clostridial empyema. Arch Intern Med 1965; 115: 421425.
6. Jonsson S, Clarridge J, Young EJ. Necrotizing pneumo- nia and empyema caused by Bacillus cereus and Clostridium bifermentans. Am Rev Respir Dis 1983; 127: 357 359.
7. Bentley DW, Lepper MH. Epyema caused by Clostridium perfringens. Am Rev Respir Dis 1969; 100: 706-710.
8. Hardison JE. Primary Clostridial pneumonia and empy- ema. Chest 1970; 57:390 392.
9. Kwan WC, Lain SC, Chow AW, Lepawski M, Glanzberg MM. Empyema caused by Clostridium per- fringens. Can Med Assoc J 1983; 128: 1420-1422.