physiology of the cardiovascular system - zona.fmed.uniba.sk · sino-atrial (sa) node (sinus node)...
TRANSCRIPT

Physiology of the
cardiovascular systemPart 1
Physiological properties of the cardiac muscle –
automacy and rhythmicity, conductivity, excitability,
contractility.
The cardiac cycle. Heart sounds. Arterial pulse.
Regulation of the cardiovascular system.
Practical tasks
•Physiological properties of the cardiac muscle
•Auscultation of the heart sounds
•Examination of the arterial pulse
•Experiments on an isolated heart
© Katarína Babinská MD, PhD, MSc, Institute of Physiology CU, Bratislava

• Heart function – vital function
• Cardiovascular diseases
– high prevalence
– main cause of death
– risk factors include bad lifestyle (nutrition,
lack of physical activity)
– many of them preventable – lifestyle
• Cardiology – complex, quickly developing
branch of medicine
CPR

What is the transmembrane potential?
• is the difference in electric potential between
the interior and the exterior of a biological cell.
• it exists across the membranes of almost all
cells in the body - also in the cardiac muscle
cells
• related to ion distribution across the membrane
and its changes
a cell
electrode
out
electrode
in
oscilloscope
– shows a potential difference
= transmembrane potential

action potential - after stimulation – record shows a curve with a typical shape
-90
Resting membrane potential, action potential
0
mV
t (ms)
resting membrane potential - unstimulated cell – record shows a straight line
-90
0
mV
Changes of the potential are due to ion flows

Physiological properties of the cardiac muscle
1. Automacy and rhythmicity (Chronotropy)
• ability of the cardiac muscle cells (in sinus node) to generate spontaneously action
potentials at a regular pace (= self-excitation)
2. Conductivity (Dromotropy)
• ability to transmit the excitation generated in the sinus node to all the heart muscle
fibres in a pre-defined pattern via a specialised conducting system
3. Excitability (Bathmotropy)
• ability of the cardiac muscle cells to respond to the incoming excitation by AP -
when the stimulus arrives to the cardiac muscle cells it causes their depolarization
4. Contractility (Inotropy)
• capability of the cardiac muscle to respond to a stimulus by contraction

1. Automacy and rhythmicity (Chronotropy)
• ability of the cardiac muscle to generate
spontaneously action potentials
at a regular pace (= self-excitation)
Sino-atrial (SA) node (sinus node)
• generator of electric activity of the heart
• cells capable of self-excitation at regular intervals (in resting state 60-100/min)
• from SA node the excitation is spread to excite all cardiac muscle cells, therefore
❑ SA node = the heart pacemaker (the only normal pacemaker)

Mechanism of the sinus nodal rhytmicity
Sinus node• „unquiet“ cells – instant changes in transmembrane potential
- no real resting membrane potential („straight line“)
- minimum value: -55 mV
Curve of transmembrane potential in sinus node
-55
-40
mV
0t (ms)
1 2 3
1 2 3

Phases of the transmembrane potential in the sinus node
1 2 3
Curve of transmembrane
potential in the sinus node
A. at the beginning Na+ ions leak through the funny channels into the cardiomyocytes
- membrane is untight for Na+ (result: slow depolarization)
B. then T-type of Ca2+ voltage gated channels are activated (at about -50 mV)
- slow influx of Ca2+ ions in concentration gradient → slow depolarization proceeds
- channels A and B are specific for the pacemakers !!!
1. Spontaneous diastolic depolarization (SDD, praepotential)
- a slow increase of the transmembrane potential (from -55 mV to a less negative value)
- without any external stimulus !!!
-
55
A
B

1 2 3 Curve of transmembrane potential in sinus node
2. Depolarization
• a steep rise in transmembrane potential after the threshold -40 mV is reached
• due to opening of the L-type Ca2+ voltage gated channels
• influx of Ca++ ions (in concentration gradient)
• overshoot to positive values (transpolarization)
-
55

1 2 3 Curve of transmembrane potential in sinus node
3. Repolarization
- Ca2+ channels inactivated
- K+ channels open
- K+ moves outwards
- the transmembrane potential returns to its minimum value
-
55

Positive and negative chronotropic effect
Positive
Negative
Baseline
- positive – potentials in sinus node are generated with higher frequency
- negative – potentials in sinus node are generated with lower frequency

2. Conductivity (Dromotropy)
- excitation travels from the sinus node to all the heart muscle fibres in a pre-
defined pattern via a specialised conducting system
The cardiac muscle includes
- working myocardium
(main function: contraction/pumping)
- conduction system
(main function: fast transmission
of action potentials)

Cardiac muscle – syncytium
- cardiomyocytes cells connected by gap junctions
- allow the transport of ions from cell to cell
- transmission of AP from one cardiac muscle cell to another
- all the cells of working myocardium are activated (and contracted) as one unit

Conduction pathways include:
• excitation of the atria – from the SA node → to all muscle cells of atria
1. from a muscle cell to the neighbouring ones via gap junctions (0,3 m/s)
2. interatrial bundles – anterior, middle, posterior (1 m/s) – cardiomyocytes „specilized on
conductivity (from SA node to the AV node)
• excitation of the ventricles - AV node – the only pathway from atria to ventricles
(because atria and ventricles are separated by a non-conductive fibrous tissue)
− SA node to AV node (velocity 1 m/s) :
− through the A-V node (0,03 m/s)
− bundle of Hiss (2 m/s)
− right and left bundle branch (Tawara branches)
− Purkinje fibres (2 - 4 m/s)
− cardiac muscle cells (0,3 m/s)

Duration of the transmission of AP from SA node to myocardium
• first depolarization (and also
contraction) the of atria occurs
• depolarization (and also
contraction) of ventricles
occurs with a time delay
• delay is caused by a slow
transmission through the
AV-node
• the delay allows for efficient
function of the heart as a pump
– first contract the atria
– slightly later contract the ventricles
0,03 s0,16 s
0,22 s
0,17 s
0,18 s0,19 s
0,00 s

• not only the cells of SA node, also other parts of the conduction system are
capable of self excitation - however at slower pace:
❑ atrio – ventricular node 40 – 60/ minute
❑ Purkinje fibres 15 – 40/ minute
- these also begin their self-excitation
(at the same time as SA node)
- normally they do not get self-excited
because the action potential from SA node
arrives here faster and causes their excitation
- they produce potentials only in abnormal
cases
❑ sino-atrial node
= heart pacemaker (the only normal)
❑ ectopic (secondary) pacemakers
– other than S-A node - abnormal (e.g. junctional rhythm – generated in AV node)
Gradient of cardiac automacy
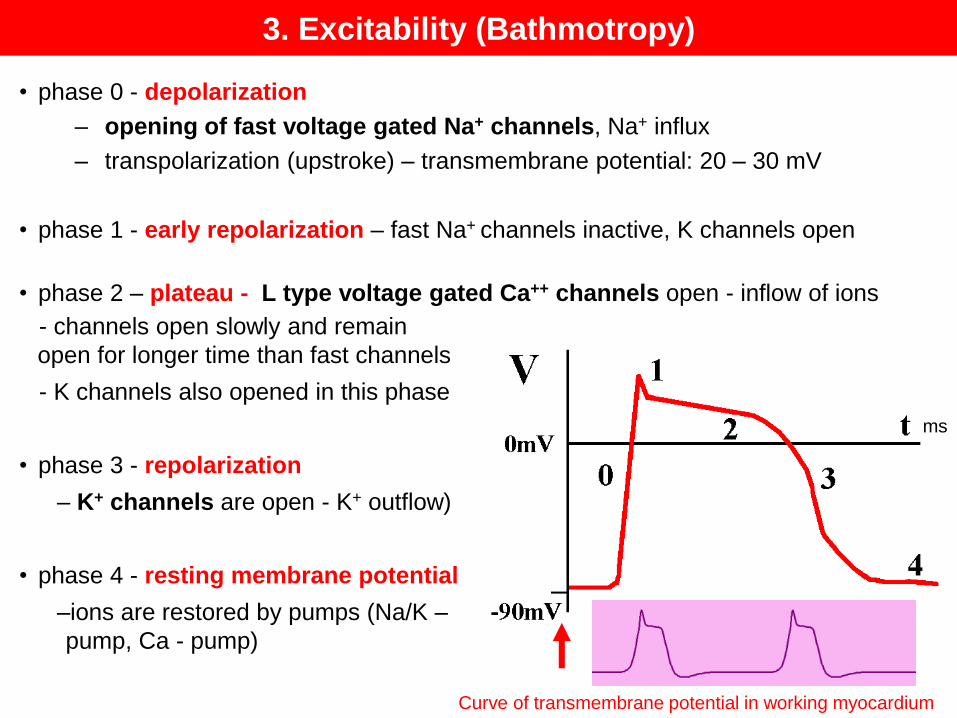
3. Excitability (Bathmotropy)
- channels open slowly and remain
open for longer time than fast channels
- K channels also opened in this phase
• phase 3 - repolarization
– K+ channels are open - K+ outflow)
• phase 4 - resting membrane potential
–ions are restored by pumps (Na/K –
pump, Ca - pump)
• phase 0 - depolarization
– opening of fast voltage gated Na+ channels, Na+ influx
– transpolarization (upstroke) – transmembrane potential: 20 – 30 mV
• phase 1 - early repolarization – fast Na+ channels inactive, K channels open
• phase 2 – plateau - L type voltage gated Ca++ channels open - inflow of ions
Curve of transmembrane potential in working myocardium
ms

Refractory periods in the cardiac muscle
• Extrasystole – abnormal premature stimulation resulting in systole
• Absolute refractory period (ARP)
– period of action potential when cardiomyocytes do not react to next stimulation at all
– in myocardium it has a long duration – protection from:
a/ tetanic contraction of the myocardium
b/ premature depolarization (that would make the heart pump less effective – the
heart would have insufficient time to get filled with blood)
• Relative refractory period (RRP)
ARP RRP
ms
extrasystole compensatory pause
no no yes
yes no
- follows the absolute refractory period -
myocardium is more difficult to stimulate
- responds only to very strong excitatory
signals

The all or nothing principle
• the cardiac muscle operates according to the all or nothing principle
– insufficient stimulation (subthreshold stimulus) causes no contraction (no response) of
a cardiac muscle fibre
– sufficient stimulation (threshold and suprathreshold stimulus) causes maximum
contraction of a cardiac muscle fibre
• according to the all or nothing law operate both
1. individual cardiac muscle fibres - similarly to the skeletal muscle
2. the heart as a whole - in contrast to striated muscle – because myocardium
is a syncytium – action potential is quickly transmitted to all heart muscle
cells through gap junctions, thus they are activated in one time
subtheshold threshold suprathresholdstimulus stimulus stimulus
no response maximum maximumcontraction contraction

4. Contractility (inotropy) – excitation/contraction coupling

Automacy and rhythmicity (chronotropy)
- Positive chronotropic effect – increased automacy (faster generation of AP)
- Negative chronotropic effect – decreased automacy (slower generation of AP)
Conductivity (dromotropy)
- Positive dromotropic effect – faster conduction of the AP
- Negative dromotropic effect – slower conduction
Excitability (bathmotropy)
- Positive bathmotropic effect – higher excitability of the cardiac muscle
- Negative bathmotropic effect – lower excitability of the cardiac muscle
Contractility (inotropy)
- Positive inotropic effect – stronger contraction of the cardiac muscle
- Negative inotropic effect – weaker contraction of the cardiac muscle
Neurotransmitters and drugs with effects on the heart

Scheme of the heart
https://cdn-images-1.medium.com/max/400/1*VXiRcJ7OGmnD9BVXNnVvbg.jpeg
Chambers – atria, ventricles
Valves – atrioventricular (tricuspid, bicuspid), seminulnar (aortic, pulmonary)
Circulation – systemic, pulmonary

The cardiac cycle
• The cardiac cycle is the series of events comprising a complete contraction and
relaxation of the heart's four chambers:
1. filling of the ventricles (diastole of the ventricles)
2. period of isovolumic (isometric) contraction of the ventricles
3. period of ejection
4. period of isovolumic relaxation of the ventricles

1. Filling of the ventricles (ventricular diastole)
• starts after previous systole – when ventricles relax
• intraventricular pressures fall below atrial pressures (= 0 in diastole)
• the AV valves open and ventricular filling begins
• the blood flow during ventricular filling generates the third heart sound (S3) -
by tensing of chordae tendineae and AV ring during ventricular filling
Filling of the ventricles has 3 periods:
1A. Rapid filling (great A-V pressure difference)
1B. Slow filling (smaller A-V pressure difference)
1C. Systole of the atria – generates the fourth heart sound (S4)
• at the very end of the ventricular filling, the ventricular
volumes are maximal = the end-diastolic volume (EDV)
•the left ventricular EDV is typically about 120 ml

• a rapid increase in myocyte tension
and intraventricular pressure
• as intraventricular pressure exceeds atrial pressure
- the AV valves close
• closing of the AV valves results in the first heart sound (S1)
(the 1st sound is caused by the closing of the AV valves + vibration of the myocardium)
• ventricular pressure rises rapidly without a change in ventricular blood volume
(no ejection so far)
• ventricular blood volume does not change because all valves are closed during
this phase ("isovolumic" or "isovolumetric“)
2. Isovolumetric contraction

3. Ejection
• intraventricular pressures exceed the pressures within
the aorta and pulmonary artery
• this causes the aortic and pulmonary valves to open
• pressure gradient propels blood into the aorta and pulmonary
artery from their respective ventricles
• pressures in the ventricles (systole)
• left ventricle 125 mm Hg
• right ventricle 25 mm Hg
• about 70 ml of blood are ejected = stroke (systolic) volume
• ejection fraction = systolic volume/ end-diastolic volume
• normal value at rest 60 %
4. Isometric (isovolumetric) relaxation
• the ventricles relax
• the intraventricular pressures fall (below in aorta and pulmonary artery)
• pressure in aorta and pulmonary artery exceeds the pressurein the ventricles → the aortic and pulmonary valves abruptly close causing the second heart sound (S2)
• In diastole the pressures in the ventricles fall to
• left ventricle 0 mm Hg
• right ventricle 0 mm Hg
• end-systolic volume - the volume of blood that remains in a ventricle (50 ml in the left ventricle)
• left atrial pressure continues to rise because of venous return from the lungs.
Task: Auscultation of the heart sounds

Heart sounds
▪ heart sounds are the noises (sound) generated during the cardiac cycle (lub-dub)
▪ sounds are examined by
- auscultation by a stethoscope
- phonocardiography – a curve is recorded
• the first sound (systolic) – „lub“
– the first of the paired heart sounds, following the longer diastolic period
– generated by closing of AV valves (bicuspid and tricuspid)
and vibrations of ventricular myocardium
• the second sound (diastolic) – „dub“
– generated by closing of semilunar valves
– shorter duration and higher frequency than the first heart sound
• the third sound
– generated by blood flow into ventricles during the period of rapid filling
• the fourth sound
– generated by the systole of atria
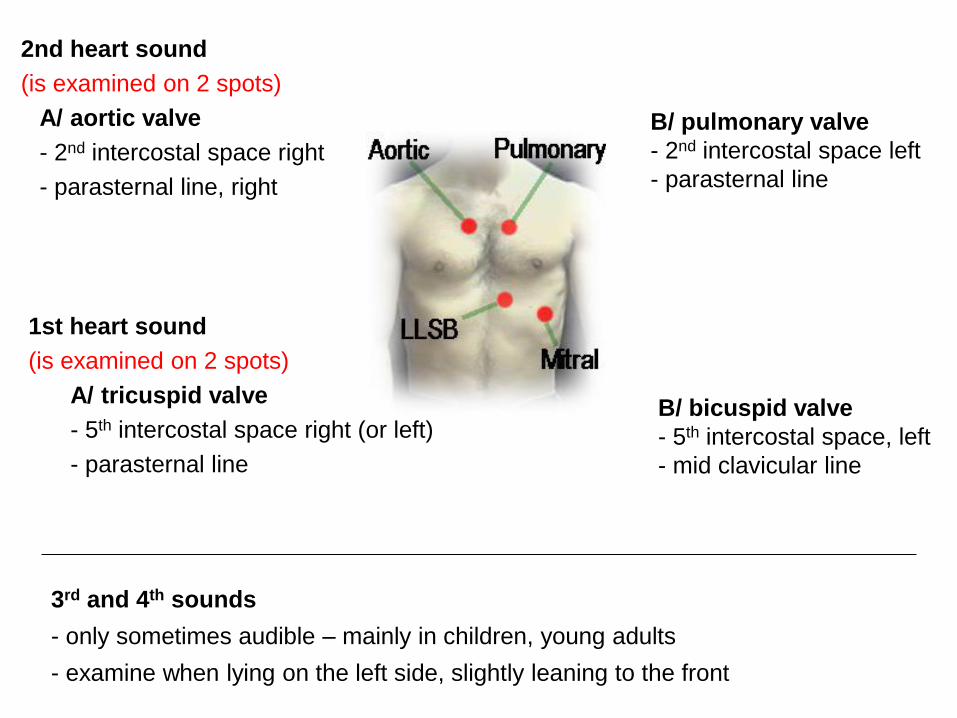
1st heart sound
(is examined on 2 spots)
A/ tricuspid valve
- 5th intercostal space right (or left)
- parasternal line
2nd heart sound
(is examined on 2 spots)
A/ aortic valve
- 2nd intercostal space right
- parasternal line, right
3rd and 4th sounds
- only sometimes audible – mainly in children, young adults
- examine when lying on the left side, slightly leaning to the front
B/ pulmonary valve
- 2nd intercostal space left
- parasternal line
B/ bicuspid valve
- 5th intercostal space, left
- mid clavicular line
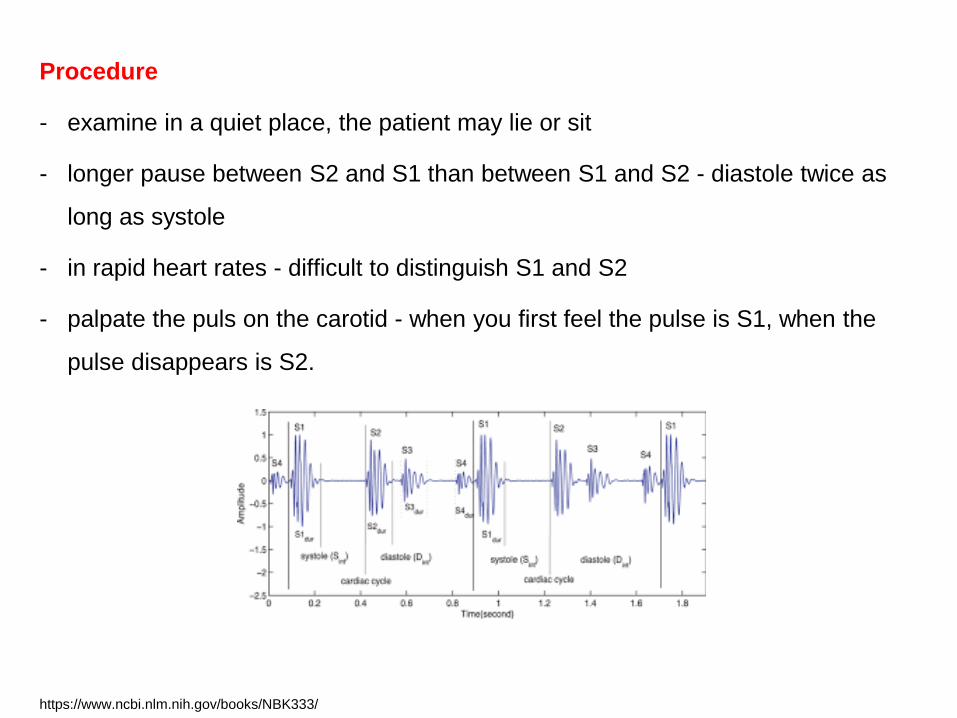
Procedure
- examine in a quiet place, the patient may lie or sit
- longer pause between S2 and S1 than between S1 and S2 - diastole twice as
long as systole
- in rapid heart rates - difficult to distinguish S1 and S2
- palpate the puls on the carotid - when you first feel the pulse is S1, when the
pulse disappears is S2.
https://www.ncbi.nlm.nih.gov/books/NBK333/

Murmurs - abnormal heart sounds produced by abnormal patterns of blood flow in the
heart (e.g. due to defective heart valves)
Results and conclusions
- normal sounds are sharp without additional sounds (murmurs)
- evaluate rhythm (regular/irregular)
- evaluate accent:
- the 1st heart sound
- lower-pitched, duller and longer than the 2nd heart sound
- usually louder at the apex than is the second sound.
- at the base usually the second sound normally louder than the first sound
- evaluate synchronisation – normal sounds are synchronized, i.e. closing of 2
valves generates 1 synchonized sound
https://www.ncbi.nlm.nih.gov/books/NBK333/

Measurement of the arterial pulse

Arterial pulse
- systole - ejection of blood from left ventricle into aorta
- aorta and large arteries – elastic type of arteries
- rise in volume/pressure in aorta - distention of the aortic vessel wall
Pulse (wave) - a wave of vibration of the vessel wall caused by ejection of blood
during cardiac systole that is transmitted down the aorta and arteries
-it can be plapated over superficial arteries
- central pulse: carotid artery, a. femoralis (branches of aorta)
- peripheral pulse: radial a., popliteal a., etc.
diastole
systole
diastole

Arterial pulse – a pulse wave
- caused by closing of the aortic valve)
Velocity of the pulse wave
1. is higher than velocity of the blood flow !!!
2. inverse association with arterial elasticity – therefore increases with age
(elasticity drops down due to atherosclerosis)
3. decreases with the diameter of the vessel
more elastic
less elastic
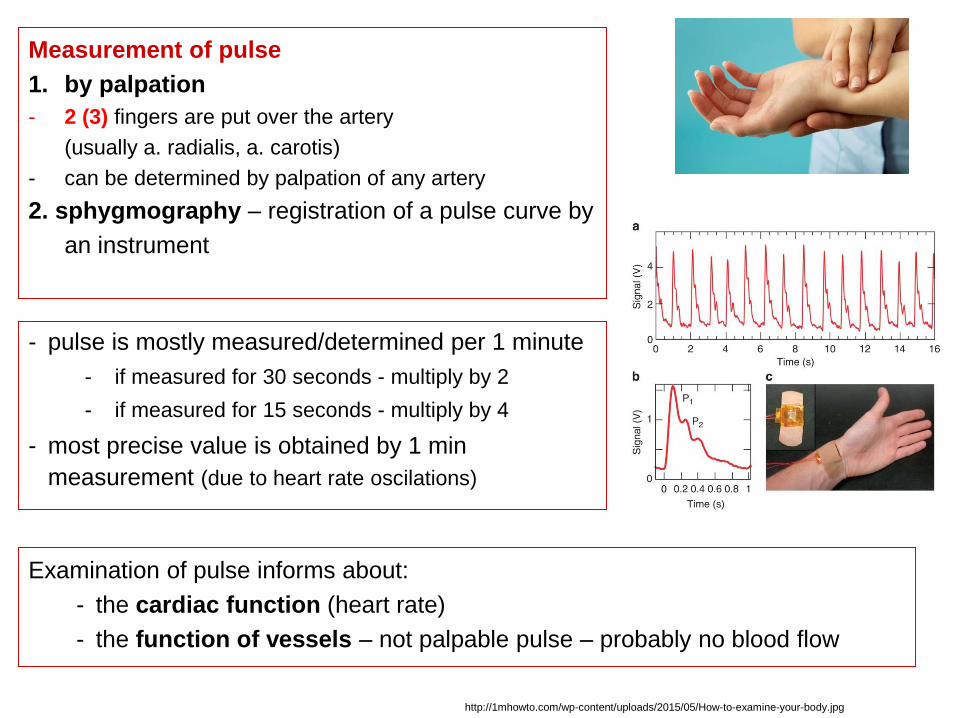
Measurement of pulse
1. by palpation
- 2 (3) fingers are put over the artery
(usually a. radialis, a. carotis)
- can be determined by palpation of any artery
2. sphygmography – registration of a pulse curve by
an instrument
- pulse is mostly measured/determined per 1 minute
- if measured for 30 seconds - multiply by 2
- if measured for 15 seconds - multiply by 4
- most precise value is obtained by 1 min
measurement (due to heart rate oscilations)
Examination of pulse informs about:
- the cardiac function (heart rate)
- the function of vessels – not palpable pulse – probably no blood flow
http://1mhowto.com/wp-content/uploads/2015/05/How-to-examine-your-body.jpg

In previous times also other qualities of the pulse were evaluated
3. amplitude large/small (magnus/parvus)
4. velocity of the pulse wave increase (celer/ tardus)
5. suppressibility (mollis – easily suppressive, durus – hardly suppressive)
Task:
a/ find the pulse over different arteries (carotid, radial, popliteal, dors. pedis, etc.)
b/ measure the a pulse rate / min in a volunteer
c/ evaluate if the pulse rate is: normal/abnormal, reular/irregular
Evaluation of the pulse examination
1. frequency
• normal 60-100/ min
• bradycardia <60/ min
(normal in sleep, trained people, abnormal causes: e.g. hypothyrosis, heart disease)
• tachycardia (pulsus frequens) >100/ min
(normal in physical activity, stress, abnormal causes e.g. hyperthyrosis, heart disease)
2. rhythm – regular / irregular
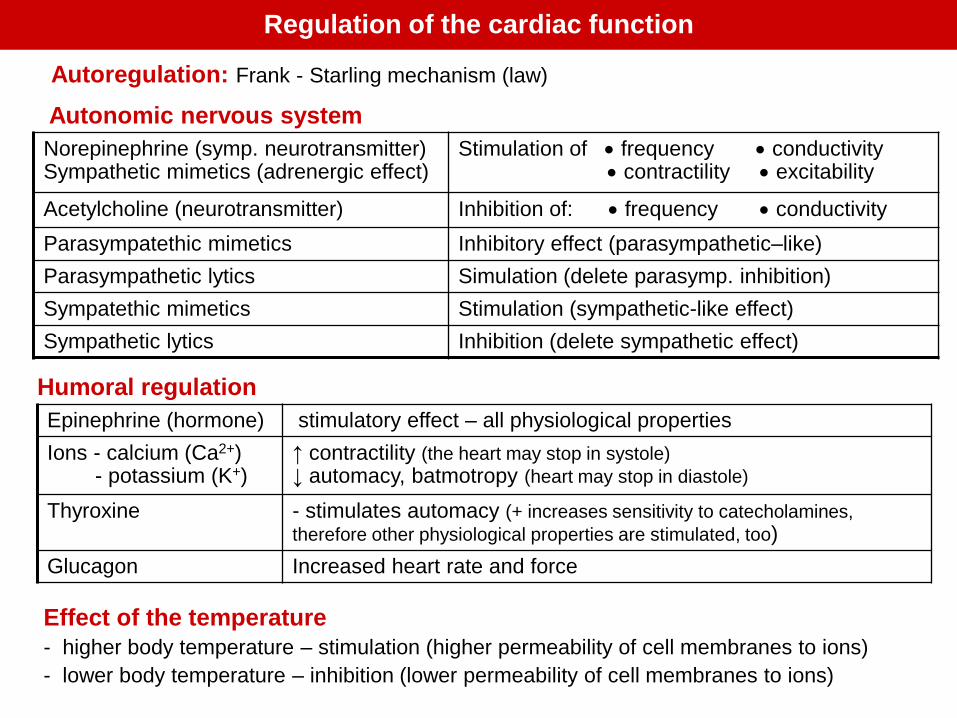
Regulation of the cardiac function
Autoregulation: Frank - Starling mechanism (law)
Autonomic nervous system
Norepinephrine (symp. neurotransmitter)Sympathetic mimetics (adrenergic effect)
Stimulation of • frequency • conductivity• contractility • excitability
Acetylcholine (neurotransmitter) Inhibition of: • frequency • conductivity
Parasympatethic mimetics Inhibitory effect (parasympathetic–like)
Parasympathetic lytics Simulation (delete parasymp. inhibition)
Sympatethic mimetics Stimulation (sympathetic-like effect)
Sympathetic lytics Inhibition (delete sympathetic effect)
Humoral regulation
Epinephrine (hormone) stimulatory effect – all physiological properties
Ions - calcium (Ca2+)- potassium (K+)
↑ contractility (the heart may stop in systole)
↓ automacy, batmotropy (heart may stop in diastole)
Thyroxine - stimulates automacy (+ increases sensitivity to catecholamines,
therefore other physiological properties are stimulated, too)
Glucagon Increased heart rate and force
Effect of the temperature
- higher body temperature – stimulation (higher permeability of cell membranes to ions)
- lower body temperature – inhibition (lower permeability of cell membranes to ions)

Protocol
- you will administer different cardioactive drugs to yor patient and monitor their
effect
- the cardiac action will be shown by a curve determined by its frequency and
amplitude
Task: Sim Heart
- Sim Heart is a simulation program that monitors the cardiac activity and the
effects of cardio-active drugs
Evaluate (for each substance given) the effect of your treatment
• chages in frequency (heart rate – chronotropy)
• changes in amplitude (strength) of the cardiac contraction - inotropy
substance A substance B

Your patient need the following substances include
A/ Neurotransmitters
1. sympathetic:
– epinephrine (adrenaline, Adr) – stimulatory effect on the cardiac muscle
(the cardiac muscle has mainly beta1 receptors)
2. parasympathetic: acetylcholine (ACh) – generates inhibitory effect on the
cardiac muscle
B/ Calcium blockers - cardio-active drugs
- calcium - decisive role in the electromechanical coupling of cardiac contraction
- due to limited intracellular calcium storage the heart is dependent on the
calcium flowing in from the extracellular space
- calcium blockers like verapamil block the calcium channels

C/ Substances with competitive effect (antagonists, inhibition)
• the action of neurotransmitters can be suppressed by specific blockade of their
receptors with appropriate receptor antagonists (competitive inhibition).
– atropine competes for the muscarinic a receptors and it is inhibitor of the ACh
– propranolol blocks the epinephrine action by binding to beta receptors,
phentolamine binds to adrenergic alpha receptors
D/ Cardiac glycosides (digitalis glycosides) - cardio-active drugs
• increase the force of heart contraction
• may trigger (e.g. strophantin) arrythmias

3. Select a substance
1. Switch on
4. Choose the appropriate
concentration: always 10-4
5. Transfer the selected tube
into the apparatus and
preset the dose (100)
2. Change the settings
Speed 1 cm/s
Resolution 5mV/Div
– the curve of basal activity of
the heart will appear
6. Start testing the effects of a substance by
pressing the arrow down and arrow left
- to stop testing press the STOP button

- indicate if the effect was positive (+), negative (-) or no change was observed (0)
- draw a curve showing the change
Protocol / Results
Substance Chrono-
tropy
Inotropy Curve
Epinephrine
Epinephrine, and add α
blocker phentolamine
Epinephrine, than add β
blocker propranolol
Atropine
Atropine, and add its
antagonist acetylcholine
Verapamil
Strophantine