pharmacy bulletin - jknmelaka.moh.gov.my bulletin 1... · put some of the ointment on the normal...
TRANSCRIPT

PEJABAT KESIHATAN DAERAH
JASIN In 2008, RM1.5 billion
was spent by Ministry
of Health (MOH) on
purchasing drug as
compared to RM 206
million on 1995. De-
spite spending billions
of Ringgit, many pa-
tients still fail to
achieve the targeted
goal of treatment. Na-
tional Health and Mor-
bidity Survey 2006
(NHMS III) reported
that only about 26.3%
of patients who re-
c e i v e d a n t i -
hypertensive treat-
ment were able to
reach the targeted
blood pressure. Failure
to achieve treatment
goals might be contrib-
uted by under-
utilization of medica-
tions and treatment
non-adherence. A sur-
vey done by Pharma-
ceutical Service Divi-
sion, MOH on medica-
tion returned by pa-
tients showed that the
value amounted to RM
200,000 in 2008 and
RM 700,000 in 2009
respectively. There-
fore it is vital to in-
corporate Home Med-
i c a t i o n R e v i e w
(HMR) into current
health care system to
improve health out-
come and reducing
expenditure. HMR is
basically an exten-
sion of services from
health facilities to pa-
tient’s home. It in-
volves systematic re-
view of all prescrip-
t ion and non-
prescription medi-
cines (including nu-
tritional supple-
ments, herbal medi-
cine, vitamins and
other remedies) and
assessment of medi-
cal storage at home.
Throughout the pro-
cess, health care pro-
vider will be able to
identify, resolve and
prevent drug-related
problems at home.
Pharmacist’s roles in
HMR will be channel-
ing information and
advising patient or
caregivers with re-
gards to medication
and therapeutic de-
vices to ensure better
therapeutic outcomes
in the overall man-
agement of the pa-
tient.
By: Nur Syahrina Yunus
Editorial board Advisor:
Pn Fatimah bt Othman
Editor:
Nur Syahrina bt Yunus
Contributor:
Nur Farhana bt Ismail
Tan Chong Seng
Tan Suet Ting
Amreet Kaur Gill
Tan Siong Guan
Azura bt Kasim
Melissa Joan Anbalagan
Team Building 2
Coaprovel 3
Tenvir-EM 5
Heat Stroke 8
Antifungal 9
Psoriasis 10
New staffs in PKDJ 13
Inside this issue:
HOME MEDICATION REVIEW (HMR)
PHARMACY BULLETIN
Edition 1/2016 Volume 1, Issue 1

On 9th April 2016 pharmacy unit
held a Team building Programme
placed at Dewan Kenyalang, Pejabat
Kesihatan Daerah Jasin (PKDJ).
There are about 30 participants
joined including clinic and pharmacy
staff. The program started from 8.00
am until 5.00 pm including many activ-
ities hosted by our invited speakers.
The objective are to strengthen rela-
tionship and integration among work-
ers. To increase the involvement, com-
mitment and motivation among work-
ers, thus creating a harmonious at-
mosphere in the organisations.The
invited speakers, Pn Hanani Osman
and Pn Norzahira Mohd Osman are-
from Counselling Unit, Jabatan
Kesihatan Negeri Melaka (JKNM). She
delivered few talks and activities
throughout the day.
TEAM BUILDING
character, their strengths and pro-
vides opportunity for immediate cor-
rection, guidance and affirmation. It
is a fun and interactive style of team-
building programme.
The activities were divided into
3 parts which involved a few small
groups training such as “Acapella ac-
tivities”, “Peribahasa & Simpulan Ba-
hasa Challenge” and “Straw Team”.
Lastly the advantages of this
program are the participants can
learned new experiences in each ac-
tivities. Furthermore, it reveals their
By: Nur Farhana bt Ismail Page 2

CoAprovel is under FDA Pregnancy category D.
This means that CoAprovel should only be used in
life-threatening emergencies when no safer drug
available.
There is positive evidence that CoAprovel imposes
human fetal risk. The use of drug that affects ren-
in-angiotensin system may result in
fetal injury or death.
NEW DRUGS ON THE block
CoAprovel is a cardiovascular drug that is used to
treat hypertension. It is the combination of an An-
giotensin Receptor Blocker (ARB) irbesartan and a
thiazide diuretic hydrochlorothiazide given as once
daily (OD) dosing.
It is currently sold under the brand of CoAprovel
by Sanofi-Aventis.
INTRODUCTION TO COAPROVEL
Presentations:
CoAprovel 150/12.5
CoAprovel
300/12.5
CoAprovel
300/25
Page 3
Te
nv
ir
-e
m
CO
AP
RO
VE
L
28’s/
box
By: Tan Chong Seng

COAPROVEL GENERAL
COUNSELLING
POINTS
If you are pregnant and is pre-
scribed with CoAprovel, please
inform your doctor immediately
so that this drug can be stopped
as soon as possible.
Previous allergic reaction from
sulfonamide-containing drugs
(i.e Bactrim) and is prescribed
with CoAprovel, might cause
cross-hypersensitivity to
hydrochlorothiazide.
If you are on both ACE inhibi-
tors (-pril) and CoAprovel,
please inform your doctor imme-
diately to stop either one of the
drugs.
Please consult your doctor or
pharmacist before starting to take
any potassium supplement.
By: Tan Ch ong Seng Page 4

INTRODUCTION TO TENVIR-EM
Page 5
Tenvir-em is the combination of Tenofovir Disoproxil Fumarate 300mg and Emtricitabine 200mg.
Description
Blue colored capsule shaped biconvex film coated tablet plain on both sides.
Indication
Tenvir-EM is indicated for combination
with other antiretroviral agents (such as
NNRTI or PI) for the treatment of HIV-1 infec-
tions in adults.
How to take Tenvir-EM?
Usual dose:
Adult : One tablet each day with or without
food.
Not for children and adolescents.
RM154.00/30 tabs
CO
AP
RO
VE
L
Te
nv
ir
-e
m
NEW DRUGS ON THE BLOCK
By: Tan Suet Ting

Possible side effects
Very common side effects
1. Dizziness, headache, diarrhea, nausea & vomiting.
2. Muscle pain and weakness (if creatinine kinase levels in
the blood increased).
Common side effects
1. Abdominal disturbance
2. Difficulty in sleeping, abnormal dreams
3. Flatulence
4. Rashes
Pregnancy Category : B
Lactation : excreted in breast milk and should not be
used while nursing.
*If you have difficulty swallowing, you can use the tip of a spoon to crush
the tablet, then mix the powder with about 100ml (half a glass) of water,
If you forget to take Tenvir-EM, what should you do?
If you do miss a dose of Tenvir-EM : take it as soon as you can, and then
take your next dose at its regular time.
If it is almost time for your next dose : forget about the missed dose. Wait
and take the next dose at the regular time. Do not take double dose to make
up for the forgotten tablet.
If you throw up less than 1 hour after taking Tenvir-EM : take another
tablet. You do not need to take another tablet if you were sick more than 1
hour after taking Tenvir-EM.
Page 6 By: Tan Suet Ting

Page 7

It is the most severe form of heat illness wherein the body overheats and can’t cool down by sweating because of dehydration
Page 8 By: Amreet Kaur Gill

Antifungal cream How to use Antifungal Cream effectively?? The effectiveness of the cream is best achieved by follow-
ing these steps: Clean and thoroughly dry the affected ar-ea. Apply the cream to the affected area (skin surface),
usually twice a day or, as directed by your doctor. Be sure to apply enough amount of cream to cover until the sur-roundings of the affected area. Continue to use this medication for 1 MORE WEEK after
the symptoms disappear. (Stopping the medication too early may allow the fungus to continue growing, which may result in re-infection)
Miconazole and Clotrimazole
are antifungal creams com-
monly used in Klinik
Kesihatan. These antifungal
creams are used to treat skin
infections such as athlete's
foot, jock itch, ringworm, and
other fungal skin infections
(Candidiasis).
By: Tan Siong Guan Page 9
:
Topical Rx Phototherapy Systemic Rx
Coal Tar
Keratolytics
Topical steroids*
Vit D3 analogues
Dithranol (anthralin)
Emollients
NB-UVB
Oral PUVA
Bath PUVA
Topical PUVA
Methotrexate
Acitretin (retinoid)
Sulphasalazine
Ciclosporin
Hydroxyurea
Systemic steroids*
Safe Still safe Potential risk
Psoriasis is a noncontagious skin condition that produces plaques of thick-ened, scaling skin. The dry flakes of skin scales are thought to result from the excessively rapid proliferation of skin cells that is triggered by inflam-
matory chemicals produced by specialized white blood cells called lympho-cytes. Psoriasis commonly affects the skin of the elbows, knees, and
scalp.There are many effective treatment choices for psoriasis. The best treatment is individually determined by the treating physician and depends,
in part, on the type of disease, the severity, and the total body area in-volved. Here are treatments given to patient with psoriasis.
Areas usually af-
fected
Psoriasis on
hands
Psoriasis on
legs
By: Azura Kasim Page 10

Topical Treat-
ment Types of Tar Counseling points
Tar Polytar Shampoo Used twice a week on the scalp. Rub in gently and do not scratch the
scalp as it will worsen the condition
Coal Tar bath Ideally add into a bathtub of water and soak for 15-20 minutes.
Alternatively, dilute with water and apply on the skin using a cloth or
sponge, leave for 15 minutes then rinse off with water
Ung Cocois Rub onto the scalp thoroughly at night, wrap with a towel or shower cap
to avoid staining the pillowcase. Leave for 6-8 hours and rinse off the
next morning
Liquor Picis Car-
bonis (LPC) Applied at night on lesions after applying emollient. May cause skin irri-
tation and therefore if not well tolerated, steroids may be reconsidered
Keratolytics 2% Salicylic acid
cream Can be used in combination with steroid (1%HCT, BVC 1:2 or BVC 1:4)
on the scalp
Salicylic acid oint-
ment (2%, 4%, 10%,
20%, 40%)
Apply onto thick areas
Topical Steroid
Topical steroids
should be ap-
plied 5 minutes
after the applica-
tion of emollient
and should be
used twice daily
Very potent
Clobetasone propio-
nate 0.05%
(Dermovate)
To be applied on thick lesions on hands and feet
Potent
Betamethasone val-
erate (0.1%, 1:2, 1:4,
1:10)
Mometasone furoate
0.1% (Elomet)
To be applied on itchy and reddish areas on the body, limbs or scalp (1:2,
1:4)
Moderate
Clobetasone butyrate
0.05% (Eumovate)
Can be used on the face, hairline, ears and neck
Mild
Hydrocortisone (1%,
0.5%)
Can be used on the face and scalp
Page 11 By: Azura Kasim
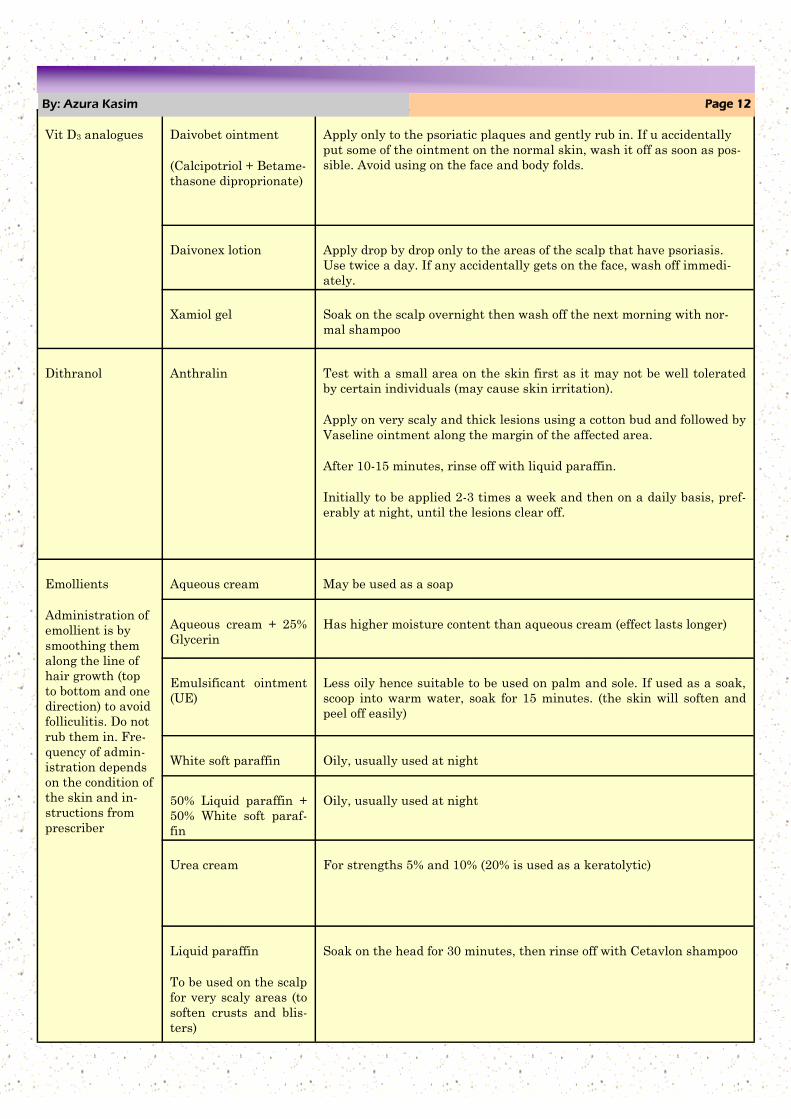
Vit D3 analogues Daivobet ointment
(Calcipotriol + Betame-
thasone diproprionate)
Apply only to the psoriatic plaques and gently rub in. If u accidentally
put some of the ointment on the normal skin, wash it off as soon as pos-
sible. Avoid using on the face and body folds.
Daivonex lotion Apply drop by drop only to the areas of the scalp that have psoriasis.
Use twice a day. If any accidentally gets on the face, wash off immedi-
ately.
Xamiol gel Soak on the scalp overnight then wash off the next morning with nor-
mal shampoo
Dithranol Anthralin Test with a small area on the skin first as it may not be well tolerated
by certain individuals (may cause skin irritation).
Apply on very scaly and thick lesions using a cotton bud and followed by
Vaseline ointment along the margin of the affected area.
After 10-15 minutes, rinse off with liquid paraffin.
Initially to be applied 2-3 times a week and then on a daily basis, pref-
erably at night, until the lesions clear off.
Emollients
Administration of
emollient is by
smoothing them
along the line of
hair growth (top
to bottom and one
direction) to avoid
folliculitis. Do not
rub them in. Fre-
quency of admin-
istration depends
on the condition of
the skin and in-
structions from
prescriber
Aqueous cream May be used as a soap
Aqueous cream + 25%
Glycerin
Has higher moisture content than aqueous cream (effect lasts longer)
Emulsificant ointment
(UE)
Less oily hence suitable to be used on palm and sole. If used as a soak,
scoop into warm water, soak for 15 minutes. (the skin will soften and
peel off easily)
White soft paraffin Oily, usually used at night
50% Liquid paraffin +
50% White soft paraf-
fin
Oily, usually used at night
Urea cream For strengths 5% and 10% (20% is used as a keratolytic)
Liquid paraffin
To be used on the scalp
for very scaly areas (to
soften crusts and blis-
ters)
Soak on the head for 30 minutes, then rinse off with Cetavlon shampoo
Page 12 By: Azura Kasim

By: Melissa Joan Page 13

By: Melissa Joan Page 14
Nama: Julia bt Shamsuddin
Umur: 33 tahun
Asal: Perak
Perkhidmatan: Hospital Melaka (4 tahun)
Klinik Kesihatan Umbai (terkini)
Impian: Menceburi perniagaan dalam bidang kesihatan
bersama suami
Nama: Izzura Akmal bt Mohd Shoib
Umur: 28 tahun
Asal: Melaka
Perkhidmatan: Hospital Banting, Hospital Melaka (4 tahun)
Klinik Kesihatan Kemendor (terkini)
Impian: Melanjutkan pengajian dalam bahasa Korea & menjelajah seluruh dunia
Nama: Melissa Joan Anbalagan
Umur: 26 tahun
Asal: Selangor
Perkhidmatan: Klinik Kesihatan Jasin (terkini)
Impian: Melanjutkan pengajian ke peringkat doktor falsafah & menjadi seorang pensyarah.
Nama: Tan Chong Seng
Umur: 25 tahun
Asal: Perak
Perkhidmatan: Klinik Kesihatan Umbai (terkini)
Impian: Melancong ke luar negara & meluaskan
ilmu pengetahuan dalam semua bidang.

‘FAMILY DAY’
KM CHALET KUALA LINGGI
23 APR 2016
MAJLIS PERPISAHAN
STAF
28 JAN 2016
MAJLIS PERSARAAN
EN OW ENG KAR & EN
SHAFIE
14 MEI 2016
MAJLIS
SAMBUTAN
HARI JADI
1
2
3
4

‘’GAME
BOWLING’
FARMASI PKD
JASIN
30 OGOS 2016
KEMPEN
KENALI UBAT
ANDA (QUMC)
KURSUS
TEAM BUILDING
& SOFT SKILL
7
5
6