pharmacy accreditation immunotherapy.… · • structure and biochemical changes ... (provenge)...
TRANSCRIPT

The Evolving Role of Specialty
Pharmacists in Cancer
Immunotherapy: New Pathways,
Agents, Opportunities, and
Challenges
Patrick J. Medina, PharmD, BCOP
Professor
Department of Medicine
Stephenson Cancer Center
University of Oklahoma
Oklahoma City, Oklahoma
Pharmacy Accreditation
Pharmacy Times Office of Continuing
Professional Education is accredited by the
Accreditation Council for Pharmacy
Education (ACPE) as a provider of
continuing pharmacy education. This
activity is approved for 1.0 contact hours
(0.10 CEU) under the ACPE universal
activity number 0290-0000-16-032-L01-P.
The activity is available for CE credit
through May 4, 2016.
Faculty Disclosure
Patrick Medina, PharmD, BCOP,
has no relevant financial
relationships with commercial
interest to disclose.
This activity is sponsored by
Pharmacy Times Continuing
Education and supported by
an educational grant from
Bristol-Myers Squibb.
Learning Objectives
• Explain the mechanisms of action behind immune response to cancer and the role of immunotherapy in cancer treatment
• Distinguish new and emerging immunotherapy classes and individual agents and their efficacy, safety, and potential patient responses to therapy in cancer treatment
• Examine strategies to counsel and assist patients to overcome barriers to therapy, including treatment side effects to improve adherence to therapy
Immunotherapy History• Paul Erlich in the late 1800s described
the term “Magic Bullet”
• The basic theory is related to the thought that tumor cells express an antigenic profile distinct from normal cells– Immune system is capable of recognizing
these antigenic differences
• In addition, tumor cells turn off T-cells specific for tumor antigens
Pardoll D. Semin Oncol. 2015;42(4):523-38

How Do Tumor Cells Differ From
Normal Cells?• Clonal in origin
• Dysregulated growth and lifespan
• Altered tissue affinity
• Resistance to apoptosis
• Change in surface phenotypes and markers
• Structure and biochemical changes
– Altered gene expression
• Presence of tumor specific antigens
Hanahan D, et al. Cell. 2011;144(5):646-74.
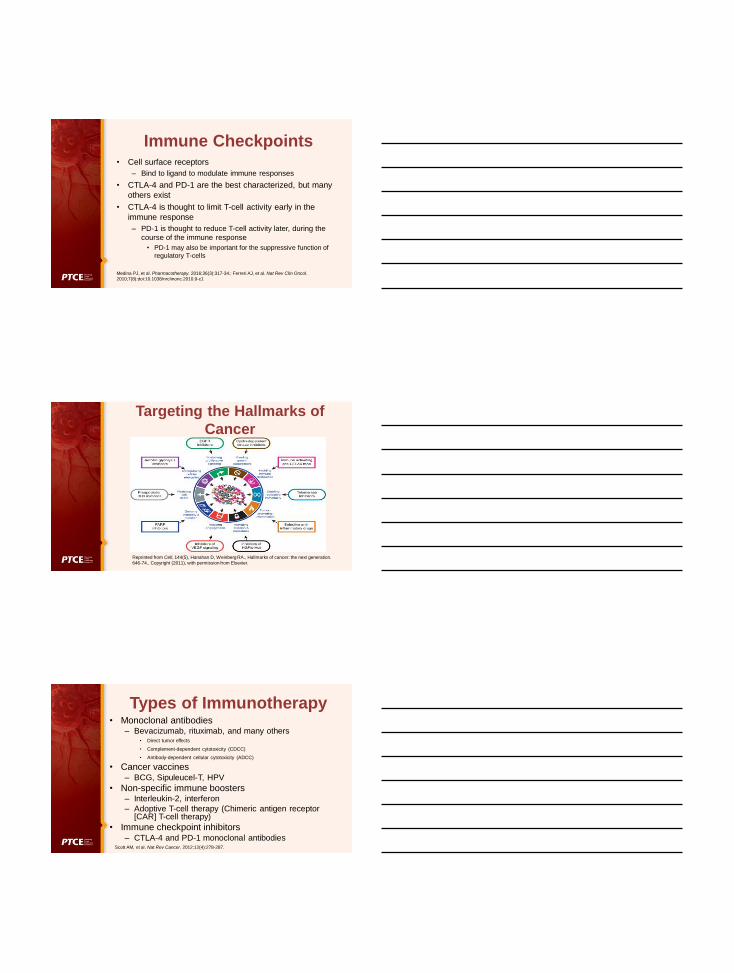
Reprinted from Cell, 144(5), Hanahan D, Weinberg RA., Hallmarks of cancer: the next generation.
646-74., Copyright (2011), with permission from Elsevier.
Emerging Hallmarks of Cancer
Reprinted from Semin Oncol, 42(4), Pardoll D, Cancer and the Immune System: Basic Concepts
and Targets for Intervention, 523-38, Copyright (2015), with permission from Elsevier.
Immune Surveillance
Immune Checkpoints• Cell surface receptors
– Bind to ligand to modulate immune responses
• CTLA-4 and PD-1 are the best characterized, but many
others exist
• CTLA-4 is thought to limit T-cell activity early in the
immune response
– PD-1 is thought to reduce T-cell activity later, during the
course of the immune response
• PD-1 may also be important for the suppressive function of
regulatory T-cells
Medina PJ, et al. Pharmacotherapy. 2016;36(3):317-34.; Ferreri AJ, et al. Nat Rev Clin Oncol.
2010;7(8):doi:10.1038/nrclinonc.2010.9-c1
Reprinted from Cell, 144(5), Hanahan D, Weinberg RA., Hallmarks of cancer: the next generation.
646-74., Copyright (2011), with permission from Elsevier.
Targeting the Hallmarks of
Cancer
Types of Immunotherapy• Monoclonal antibodies
– Bevacizumab, rituximab, and many others• Direct tumor effects
• Complement-dependent cytotoxicity (CDCC)
• Antibody-dependent cellular cytotoxicity (ADCC)
• Cancer vaccines– BCG, Sipuleucel-T, HPV
• Non-specific immune boosters– Interleukin-2, interferon
– Adoptive T-cell therapy (Chimeric antigen receptor [CAR] T-cell therapy)
• Immune checkpoint inhibitors– CTLA-4 and PD-1 monoclonal antibodies
Scott AM, et al. Nat Rev Cancer. 2012;12(4):278-287.

Immunotherapy• Vaccinations
– BCG live vaccine• Stimulates the host to reject the tumor
• Injected into the bladder for bladder cancer
• Causes local response to tumor
• Non-specific
– HPV-16 vaccine• HPV commonly linked to cervical cancer
Gandhi NM, et al. BJU Int. 2013;112(3):288-97.; Beavis AL, et al. Front Oncol. 2016;6:19.
HPV Vaccine• Specific immunotherapy
• Merck (first of 2) – Approved in 2006 (Gardasil)
– Subtypes 16, 18, 6, 11
• ~70% of high-risk types for cervical cancer
• ~90% of types for anogenital warts
• Also associated with head and neck cancers
– Lifetime effectiveness?
• 3 years
– Who?
• 9-26 year olds
• Others at risk
Beavis AL, et al. Front Oncol. 2016;6:19.
Sipuleucel – T (Provenge)
• Adoptive cellular immunotherapy
• Patients undergo 3 rounds of leukapheresis
• Cells then sent to Dendreon:– Antigen-presenting cells (APCs) are isolated and
cultured with PA2024
– PA2024 is a recombinant fusion protein, which serves as immunogen:
• Prostatic acid phosphatase and GM-CSF
• 3 doses of treated cells are administered to patients, each 2 weeks apart
Sonpavde G, et al. Eur Urol. 2012;61(4):639-647.

Sipuleucel-T: Patient-Specific Therapy
Reprinted from Eur Urol, 61(4), Sonpavde G, Di Lorenzo G, Higano CS, Kantoff PW, Madan R, Shore ND,
The role of sipuleucel-T in therapy for castration-resistant prostate cancer: a critical analysis of the
literature, 639-47, Copyright (2012), with permission from Elsevier.
Talimogene laherparepvec
(Imlygic)
• Based on the herpes simplex virus, type I (HSV-1)
• Modified by deleting the neurovirulence genes preventing fever blister
development and deleting a viral gene that blocks antigen presentation
• T-VEC can target and replicate in cancer cells by using surface-bound nectins
to enter the cell and preferentially replicates in tumor cells by exploiting
disrupted oncogenic and antiviral signaling pathways,
• Also generates an immune response, which is likely enhanced by the
expression of GM-CSF
Lawler SE, et al. J Clin Oncol. 2015;33(25):2812-4
Talimogene laherparepvec• FDA approved for the local treatment of unresectable cutaneous,
subcutaneous, and nodal lesions in patients with melanoma recurrent
after initial surgery
– Recommended starting dose is up to a maximum of 4 mL at a
concentration of 106 plaque-forming units (PFU) per mL
– Subsequent doses should be administered up to 4 mL at a
concentration of 108 PFU per mL
• Shipped frozen, needs to be thawed up to 48 hours
• Warnings for accidental exposure leading to herpetic infections in
health care workers, herpetic infections, injection site complications,
immune-mediated events, and plasmacytoma at injection site– Herpetic infections sensitive to acyclovir and may decrease the efficacy, use caution
– This is a live virus; exposure precautions are necessary
Imlygic (Talimogene laherparepvec) [package insert]. Thousand Oaks, CA: Amgen; 2015.

Antitumor Activity of Talimogene
Iaherparepvec
Andtbacka RH, et al. J Clin Oncol. 2015;33(25):2780-8.
• More than half experienced ≥ 25% increase in the size of lesions
or appearance of new lesions before achieving a response
• Two-thirds of responses expected to be > 1 year
Cytokines• Produced by mononuclear cells
• Activate the immune system to attack the cancer– NK cells, lymphocytes, etc.
• Proteins produced with recombinant technology
• Short t1/2
• Pharmacy principles– Do not shake, refrigerate
Dranoff G. Nat Rev Cancer. 2004;4(1):11-22.
Interferon-alfa (Intron-A)• Naturally-occurring protein
• Secreted by cells in response to viral
infections, tumors, and other biological inducers
• Produce clinical benefits for disease states, such as
cancer, hepatitis, and multiple sclerosis
• Produce general antiprolifertive effects on cancer cells
and/or activate the immune system to fight the cancer
• Used in melanoma, myeloma, and renal cell
http://www.cancer.org/treatment/treatmentsandsideeffects/treatmenttypes/immunotherapy/cancer-
immunotherapy-nonspecific-immunotherapies. Accessed April 1, 2016.

Interleukin-2
(Aldesleukin, Proleukin)
• Endogenous source: T lymphocytes
• Activity
– Growth factor for T-cells
– Stimulation of cytotoxicity in NK and T-cells
– Cofactor in activating macrophages and B cells
• Main therapeutic uses
– Renal cell carcinoma
– Malignant melanoma
http://www.cancer.org/treatment/treatmentsandsideeffects/treatmenttypes/immunotherapy/cancer-
immunotherapy-nonspecific-immunotherapies. Accessed April 1, 2016.
Interleukin-2
• Adverse reactions
– Black box warning
• Vascular leak syndrome
• Increased risk of infection
• Cardiac arrhythmias
• End organ damage
– Infusion related reactions
Proleukin (Interleukin-2) [package insert]. San Diego, CA: Prometheus Laboratories Inc.; 2015.
Denileukin Diftitox (Ontak)
• Interleukin-2 fused with diphtheria toxin
• Activity
1. Binds to IL-2 receptor
2. Is internalized, releasing diphtheria toxin into
cytosol
3. Inhibits protein synthesis, resulting in cellular death
Baldo BA. Drug Saf. 2015;38(5):455-79.

Denileukin Diftitox• Main therapeutic uses
– Acute graft-versus-host disease
– Cutaneous T-cell lymphoma
– Chronic lymphocytic leukemia
• Adverse reactions
– Acute hypersensitivity
– Same as with IL-2 alone
Baldo BA. Drug Saf. 2015;38(5):455-79.
• Mechanism of action
– Human monoclonal antibody against CTLA-4
• FDA approved for treatment of melanoma
Lipson EJ. Clin Cancer Res. 2011;17(22):6958-62.
Ipilimumab (Yervoy)
Ipilimumab • Unresectable or metastatic melanoma
– 3 mg/kg administered intravenously over 90 minutes
every 3 weeks for a total of 4 doses
• Unresectable or metastatic melanoma, in combination with
nivolumab at the same dose
• Adjuvant melanoma
– 10 mg/kg administered intravenously over 90 minutes
every 3 weeks for 4 doses, followed by 10 mg/kg every
12 weeks for up to 3 years or until documented disease
recurrence or unacceptable toxicity
Yervoy (Ipilimumab ) [package insert]. Princeton, NJ: Bristol Myers Squibb; 2015.; Opdivo (Nivolumab)
[package insert]. Princeton, NJ: Bristol Myers Squibb 2015.

Ipilimumab: Safety• The most common
adverse reactions (≥5%)
in patients who received 3
mg/kg were:– Fatigue (41%)
– Diarrhea (32%
– Pruritus (31%
– Rash (29%)
– Colitis (8%)
• The most common adverse
reactions (≥5%) in patients who
received 10 mg/kg were:– Rash (50%)
– Diarrhea (49%)
– Fatigue (46%)
– Pruritus (45%)
– Headache (33%)
– Weight loss (32%)
– Nausea (25%)
– Pyrexia (18%)
– Colitis (16%)
– Decreased appetite (14%)
– Vomiting (13%)
– Insomnia (10%)
Yervoy (Ipilimumab ) [package insert]. Princeton, NJ: Bristol Myers Squibb; 2015
Immune-mediated adverse
reactions (n = 131)
Grade (3-5)
(%)
Any Immune Reaction 15
Enterocolitis 7
Hypo/hyperthyroidism 4
Dermatitis 2
Hepatotoxicity 1
Neurotoxicity 1
Nephritis 1
Kinetics of Appearance of Ipilimumab
Immune-related Adverse Events
Printed with permission from Weber JS. J Clin Oncol. 2012;30(21):2691-7.
Printed with permission from Hodi FS. N Engl J Med. 2010. 19;363(8):711-23.
Time to response
3.18 months
Overall Survival and Progression-free
Survival for Ipilimumab in Metastatic
Melanoma
Nivolumab (Opdivo)• A human IgG4 monoclonal antibody that binds to the PD-1 receptor and
blocks its interaction with PD-L1 and PD-L2
• FDA approved for:
– Unresectable or metastatic melanoma, as a single agent
– Unresectable or metastatic melanoma, in combination with ipilimumab
– Metastatic NSCLC and progression on or after platinum-based chemotherapy. Patients with EGFR or ALK genomic tumor aberrations should have disease progression on FDA-approved therapy for these aberrations prior to receiving nivolumab
– Advanced renal cell carcinoma who have received prior anti-angiogenic therapy
• The dose is 3 mg/kg every 2 weeks with the exception of when it is used in combination with ipilimumab (dose is 1 mg/kg, followed by ipilimumab on the same day, every 3 weeks for 4 doses, then 3 mg/kg every 2 weeks)
Opdivo (Nivolumab) [package insert]. Princeton, NJ: Bristol Myers Squibb 2015.
Nivolumab: Safety• Most common adverse reactions (≥20%) in patients with metastatic NSCLC
were fatigue, musculoskeletal pain, decreased appetite, cough, and
constipation.
Immune adverse reactions
(n = 287) Any Grade (%)
Median Time to
Onset (Months)
Pneumonitis 3.4 7.2
Enterocolitis 17 2.7
Adrenal Insufficiency 0.3 NR
Renal Toxicity 0.3 1.5
Hepatotoxicity 0.3 7.8
Hypothyroid 7 2.9
Hyperthyroid 1.4 2
Rash 6 NR
Opdivo (Nivolumab) [package insert]. Princeton, NJ: Bristol Myers Squibb 2015.
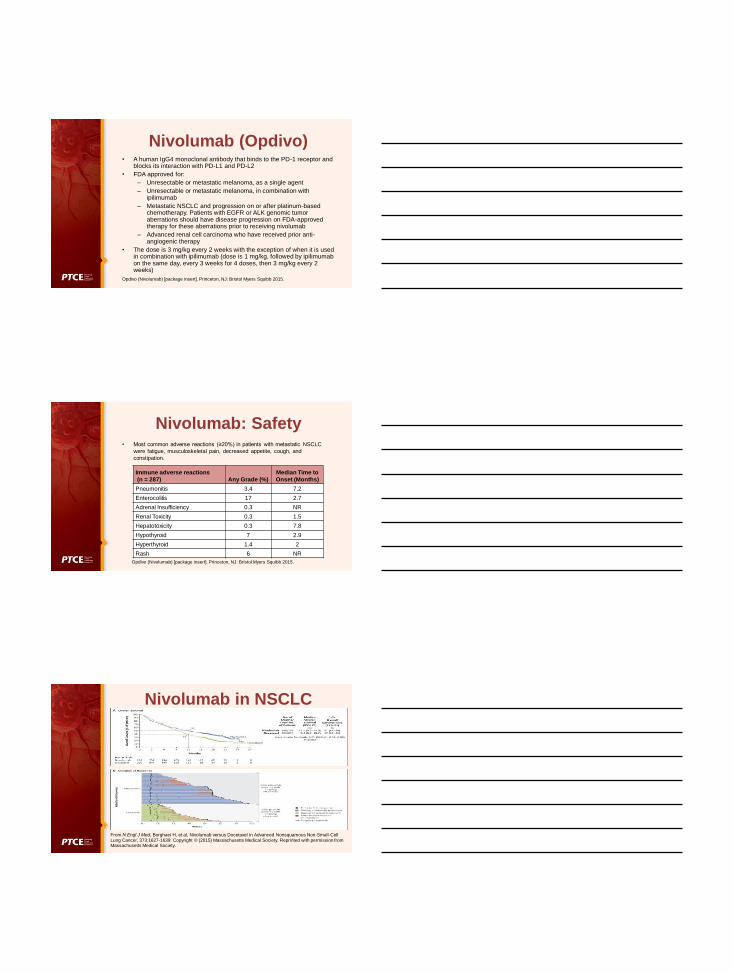
Nivolumab in NSCLC
From N Engl J Med, Borghaei H, et al, Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer, 373:1627-1639. Copyright © (2015) Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
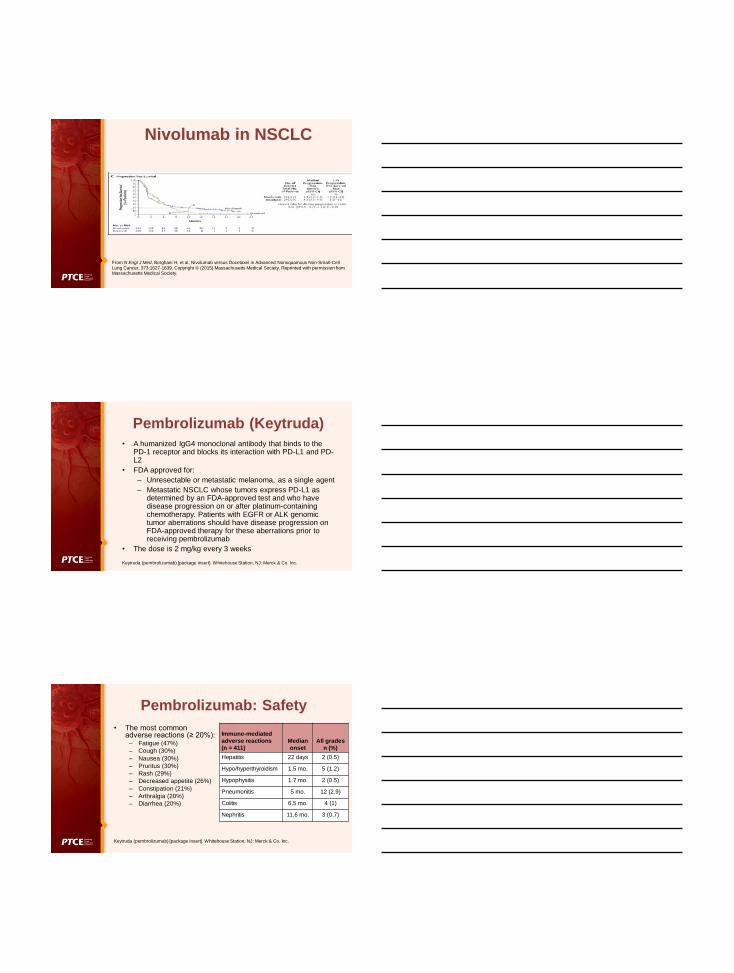
Nivolumab in NSCLC
From N Engl J Med, Borghaei H, et al, Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer, 373:1627-1639. Copyright © (2015) Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
Pembrolizumab (Keytruda)
• A humanized IgG4 monoclonal antibody that binds to the PD-1 receptor and blocks its interaction with PD-L1 and PD-L2
• FDA approved for:
– Unresectable or metastatic melanoma, as a single agent
– Metastatic NSCLC whose tumors express PD-L1 as determined by an FDA-approved test and who have disease progression on or after platinum-containing chemotherapy. Patients with EGFR or ALK genomic tumor aberrations should have disease progression on FDA-approved therapy for these aberrations prior to receiving pembrolizumab
• The dose is 2 mg/kg every 3 weeks
Keytruda (pembrolizumab) [package insert]. Whitehouse Station, NJ: Merck & Co. Inc.
Pembrolizumab: Safety
• The most common adverse reactions (≥ 20%):
– Fatigue (47%)
– Cough (30%)
– Nausea (30%)
– Pruritus (30%)
– Rash (29%)
– Decreased appetite (26%)
– Constipation (21%)
– Arthralgia (20%)
– Diarrhea (20%)
Immune-mediated
adverse reactions
(n = 411)
Median
onset
All grades
n (%)
Hepatitis 22 days 2 (0.5)
Hypo/hyperthyroidism 1.5 mo. 5 (1.2)
Hypophysitis 1.7 mo. 2 (0.5)
Pneumonitis 5 mo. 12 (2.9)
Colitis 6.5 mo. 4 (1)
Nephritis 11.6 mo. 3 (0.7)
Keytruda (pembrolizumab) [package insert]. Whitehouse Station, NJ: Merck & Co. Inc.

Pembrolizumab vs Ipilimumab in Metastatic Melanoma
From N Engl J Med, Robert et al, Pembrolizumab versus Ipilimumab in Advanced Melanoma, 372:2521-2532. Copyright © (2015) Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
Pembrolizumab vs Ipilimumab in Metastatic Melanoma
From N Engl J Med, Robert et al, Pembrolizumab versus Ipilimumab in Advanced Melanoma, 372:2521-2532. Copyright © (2015) Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
Adverse Events in the As-Treated Population
From N Engl J Med, Robert et al, Pembrolizumab versus Ipilimumab in Advanced Melanoma, 372:2521-2532.
Copyright © (2015) Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.

Immunotherapy
Introduces a New Era of
Toxicity Management
Immune-related adverse events
(irAEs)
The 5 Pillars of Immunotherapy
Toxicity Management
Printed with permission from Champiat S. Ann Oncol. 2016;27(4):559-74.
Enterocolitis/ Pneumonitis/ Neuropathies*
• Grade 1 (< 4 stools/day over baseline)
– Monitor and continue therapy
• Grade 2 (4-6 stools/day over baseline)
– Monitor and continue therapy when ≤ grade 1
– Symptoms persist, start prednisone 1mg/kg/day with a 4 week
taper and continue therapy when ≤ grade 1
• If symptoms persist or relapse on taper start IV steroids
• Grade 3/4
– IV methylprednisolone 2 mg/kg and discontinue therapy (GI consult
and hospitalization recommended)
– Consider infliximab 5 mg/kg IV ever 2 weeks if symptoms persist
Fecher LA, et al. Oncologist 2013;18(6):733-743.; Champiate S, et al. Ann Oncol. 2016;27(4):559-574.
*Please consult current package insert for individual products
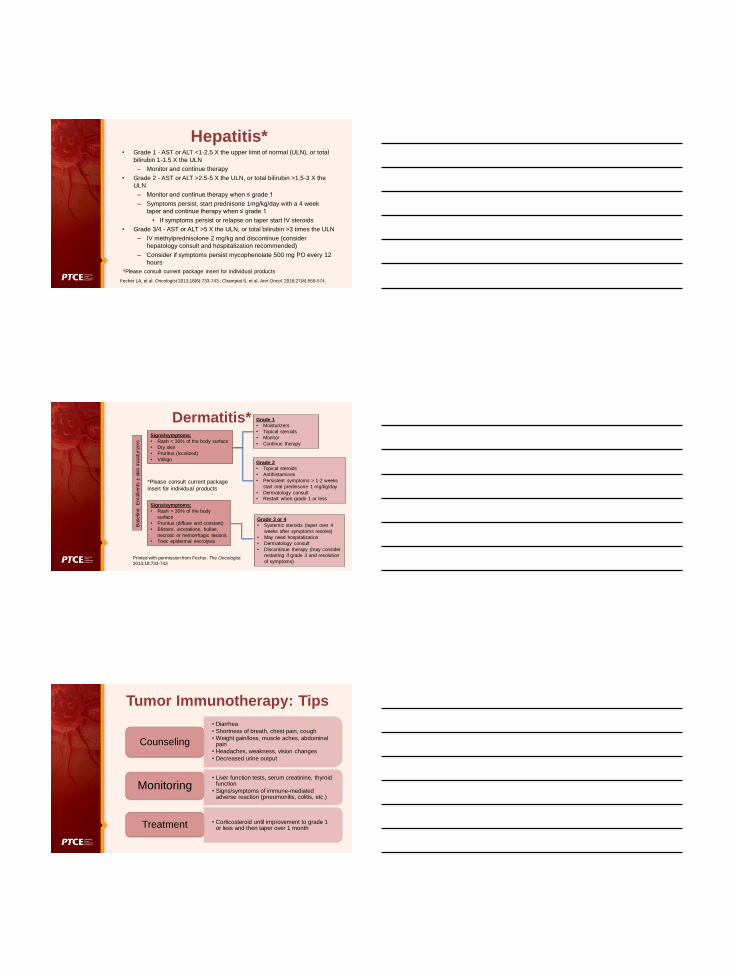
Hepatitis*• Grade 1 - AST or ALT <1-2.5 X the upper limit of normal (ULN), or total
bilirubin 1-1.5 X the ULN
– Monitor and continue therapy
• Grade 2 - AST or ALT >2.5-5 X the ULN, or total bilirubin >1.5-3 X the
ULN
– Monitor and continue therapy when ≤ grade 1
– Symptoms persist, start prednisone 1mg/kg/day with a 4 week
taper and continue therapy when ≤ grade 1
• If symptoms persist or relapse on taper start IV steroids
• Grade 3/4 - AST or ALT >5 X the ULN, or total bilirubin >3 times the ULN
– IV methylprednisolone 2 mg/kg and discontinue (consider
hepatology consult and hospitalization recommended)
– Consider if symptoms persist mycophenolate 500 mg PO every 12
hours
Fecher LA, et al. Oncologist 2013;18(6):733-743.; Champiat S, et al. Ann Oncol. 2016;27(4):559-574.
*Please consult current package insert for individual products
Dermatitis*
Baselin
e:
Em
olli
ents
±skin
mois
turizers
Signs/symptoms:
• Rash < 30% of the body surface
• Dry skin
• Pruritus (localized)
• Vitiligo
Signs/symptoms:
• Rash > 30% of the body
surface
• Pruritus (diffuse and constant)
• Blisters, ulcerations, bullae,
necrotic or hemorrhagic lesions
• Toxic epidermal necrolysis
Grade 2
• Topical steroids
• Antihistamines
• Persistent symptoms > 1-2 weeks
start oral prednisone 1 mg/kg/day
• Dermatology consult
• Restart when grade 1 or less
Grade 1
• Moisturizers
• Topical steroids
• Monitor
• Continue therapy
Grade 3 or 4
• Systemic steroids (taper over 4
weeks after symptoms resolve)
• May need hospitalization
• Dermatology consult
• Discontinue therapy (may consider
restarting if grade 3 and resolution
of symptoms)Printed with permission from Fecher. The Oncologist.
2013;18:733-743
*Please consult current package
insert for individual products
Tumor Immunotherapy: Tips
• Diarrhea
• Shortness of breath, chest pain, cough
• Weight gain/loss, muscle aches, abdominal pain
• Headaches, weakness, vision changes
• Decreased urine output
Counseling
• Liver function tests, serum creatinine, thyroid function
• Signs/symptoms of immune-mediated adverse reaction (pneumonitis, colitis, etc.)
Monitoring
• Corticosteroid until improvement to grade 1 or less and then taper over 1 monthTreatment

Patient ID CardName, Family name:
Immunotherapy drug(s):I am currently receiving an immunotherapy, which may increase the risk of
occurrence of autoimmune diseases and in particular:
pneumonitis (inflammation of the lungs)
colitis (inflammation of the gut) hepatitis (inflammation of the liver)
nephritis (inflammation of the kidneys)
endocrinopathy: hypophysitis, thyroid dysfunction, diabetes, adrenal
insufficiency (inflammation of the hormone producing organs)
cutaneous rash (inflammation of the skin)
as well as other immune-related adverse events: neurological,
hematological, ophthalmological,… The management of these
dysimmune adverse events is specific and sometimes urgent. It
absolutely requires coordination with the health care team which has
prescribed the treatment:
Prescriber ID and contact information (reported at the back of this card)
Champiat S, et al. Ann Oncol. 2016;27(4):559-574.
Barriers to Care• Cost
Melanoma
• Ipilimumab $158,282
• Nivolumab $103,220
• Pembrolizumab $14,500/month at lower dose (up to 1 million per year if
higher doses used)
• Talimogene $65,000/dose
• Combination of ipilimumab + nivolumab $295,566
–Patient with a 20% co-pay = $60,000 out of their own pocket
–All companies have patient support programs that should be routinely
used
• Adverse effect management can be tricky, and patients may have to come off
and on drugs
• Responses often take time, pseudoprogression is possible
Andrews A. Am Health Drug Benefits. 2015; 8(Spec Issue): 9.
Additional Resources
• American Cancer Society
– http://www.cancer.org/treatment/treatmentsandsid
eeffects/treatmenttypes/immunotherapy/index
• Research Cancer Immunotherapy
– www.researchcancerimmunotherapy.com
• National Cancer Institute
– http://www.cancer.gov/research/areas/treatment/i
mmunotherapy-using-immune-system