pharmacoeconomic issues in bisphosphonate treatment of metastatic bone disease
TRANSCRIPT

Pharmacoeconomic Issues in Bisphosphonate Treatment of Metastatic Bone Disease
Bruce E. Hillner
Bisphosphonates provide a supportive benefit to pa-
tients with bone metastases from cancer by reducing
skeletal complications, such as bone pain, pathologic
fractures, and hypercalcemia. Although bisphospho-
nates have important therapeutic effects, such as sig-
nificant improvements in the quality of remaining life,
they do not, as yet, significantly improve the overall
survival of affected patients. Furthermore, as with all
new innovations, they exert a major impact on drug
budgets dedicated for cancer care. Further research is
warranted to identify clinical predictors of the opti-
mum time in the course of the disease to start and stop
therapy, to integrate use of bisphosphonates with
other therapies, to identify their role in the adjuvant
setting, and to determine their cost-benefit conse-
quences. Current cost-effectiveness assessments have
shown that the incremental costs per skeletal-related
event are particularly sensitive to the unit price of the
bisphosphonate modeled. Therefore, pharmacoeco-
nomic evaluations should be combined with clinical
trials to predict accurately the true costs (total re-
source usage) of this health care intervention and to
ultimately assess the rational broad use of these agents.
Semin Oncol 28 (supf~l Il):64-68. Copyright 0 2001 by
W.B. Saunders Company.
B ONE METASTASES ARE a frequent clini- cal problem in patients with cancer. Malig-
nant osteolysis is a common complication of many cancers and can be fatal or cause a rapid deterio- ration in quality of remaining 1ife.l Bisphospho- nates are powerful inhibitors of osteoclast activity and are used in combination with standard che-
motherapy or hormonal therapy for the treatment of cancer-associated osteolytic metastases.2 They
have been used successfully in the treatment of hypercalcemia and the reduction of skeletal-re- lated complications of metastases, such as pain and
fractures.394 The aim of bisphosphonate treatment is to restore the rate of bone resorption to normal. Recent promising data suggest that, in addition to their apoptotic and antiproliferative effects on os-
From the Department of Internal Medicine and Massey Cancer Center, Virginia Commonwealth University, Richmond, VA.
Address reprint requests to Bruce E. Hillner, MD, Virginia Commonwealth Unioersity, Box 98 1070, Richmond, VA 23298- 0170.
Copyright 0 2001 by W.B. Saunders Company 0093-7754/01/2804-1112$35.00/O doi:10.I053/sonc.2001.25432
64
teoclasts, bisphosphonates may exert direct or in- direct antitumor effects.5-s Newer, more potent bisphosphonates, such as ibandronate and zoled- ronate, may improve the inhibition of osteoclast-
mediated bone resorption in tumor-induced hyper- calcemia.9
Specific issues in the use of bisphosphonates for
the treatment of metastatic bone disease need to be addressed, such as when in the course of the disease should treatment be initiated (eg, in the adjuvant or metastatic settings), the optimum du- ration of therapy, the role and safety of different
treatments, and evaluations of their relative cost effectiveness.lO In addition to determining the po- tential clinical and financial effects of current and new therapies, future assessments are needed to identify the factors that accurately predict patient subgroups that are at high risk for developing de-
tectable bony metastases and bony complications, and those that would benefit from treatment. At
present, there are no modifiable risk factors of who will develop bony metastases, whereas the risk of skeletal complications is stratified by the presence of radiographic evidence of bony metastases. Moreover, current studies are underpowered to identify predictors of benefit, principally because of their small size.
The natural history of bone metastases has sev- eral economic implications that play a prominent
role in the debate about reforming the health care system. Cost effectiveness is related to value and is defined as cost per unit of benefit ratio or, alter-
natively, as quality divided by cost (quality/cost). The need for cost-effectiveness analyses is based on the universal situation of limited levels of financial resources. The objectives of these types of analyses are to maximize the net health benefit and to help allocate ethical resources rationally.
The use of new medical innovations, such as bisphosphonates, in metastatic cancer is associated with policy concerns, including a lack of improve- ment in survival and a major impact on cancer
drug budgets. Therefore, cost-effectiveness analy- ses are required to assess the total financial burden of this type of supportive care in oncology. This should be an important consideration in choosing appropriate treatment.
Seminars in Oncology, Vol 28, No 4, Suppl I I (August), 2001: pp 64-68

PHARMACOECONOMIC ISSUES 65
EVALUATION OF COST EFFECTIVENESS
A recent study has evaluated the cost effective- ness of pamidronate, the only bisphosphonate ap- proved by the United States Food and Drug Administration in the prevention of bone compli- cations in metastastic breast cancer.10 A post-hoc evaluation was conducted in the cost-effectiveness analysis by using the results of two randomized trials that assessed pamidronate 90 mg adminis- tered intravenously versus placebo, and in which hormonal therapy or chemotherapy was adminis- tered as initial systemic therapy.“-13 The primary endpoint of the trials was skeletal-related events (SREs), which comprised all bony complications including pathologic fractures, radiation for pain relief, surgery to bone, spinal cord compression or collapse, and hypercalcemia. The trials showed the effectiveness of pamidronate in reducing SREs, radiation therapy, and pathologic fractures, and in increasing the time to the first skeletal complica- tion.
costs and quality of life associated with radi- ation were independent of the reason for therapy.
l All women needing surgery for pathologic fractures had hip procedures; pathologic frac- tures not needing surgery or radiation were either asymptomatic or needed only oral an- algesics; when uncertain, higher cost esti- mates for each SRE were used to bias the analysis in favor of pamidronate.
ASSIGNED COSTS AND QUALITY OF LlFEllJTlLlTY VALUES
A hypothetical cohort of women meeting the entry criteria for the two trials was used in the analysis. The calculation of cost-effectiveness ra- tios was based on a societal perspective, the objec- tive of which was to maximize the health benefit within limited levels of financial resources. Only assigned direct health care costs and utility values to each SRE over 24 months in monthly intervals were used. The model developed made the follow- ing assumptions:
The assigned costs per event and quality of life/utility values over 1 month used in the cost- effectiveness analysis are listed in Table 1.i4 The incremental benefit of pamidronate is reflected in a greater quality of life, in which SREs are avoided. The outcomes were measured in terms of quality- adjusted life years (QALYs), in which the quality of life weight assigned to a health state reflects a health status score during that time.
COST-EFFECTIVENESS RATIOS
The primary endpoints of this model were the costs and QALYs, which were subsequently used to estimate costs per SRE avoided and costs per QALY. The cost-effectiveness ratios were esti- mated by using the assigned utility values and SRE event months avoided.
e For patients assigned to pamidronate, treat- ment was continued monthly until death even if SREs occurred; there was no survival benefit from pamidronate; a constant hazard rate of refusal or dropout was included to avoid overestimating the pamidronate costs; the number of deaths per month was pro- jected by using a constant hazard rate based on the observed median survivals; the hazard rate per month was 3% for patients in the hormonal therapy group and 4.9% in the che- motherapy group.
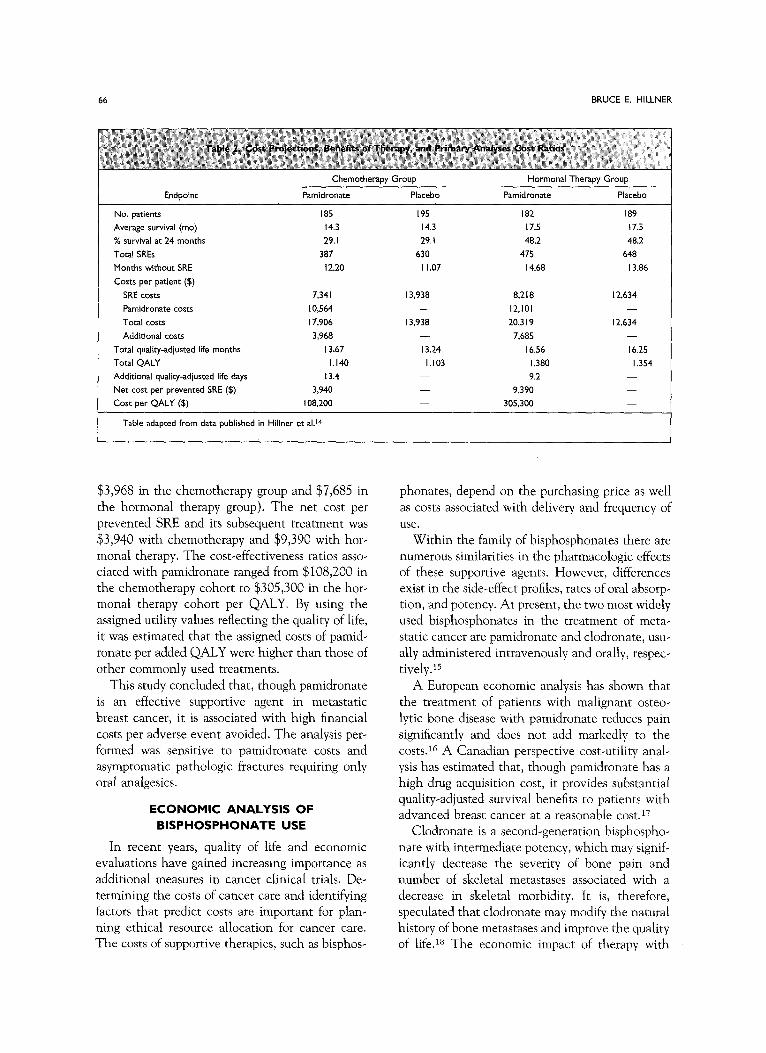
The baseline data obtained for each group are summarized in Table 2. In both systemic therapy groups, the total costs associated with pamidronate therapy exceeded the cost savings from prevented adverse events (additional costs per patient were
Table 1. Assighed Costs and Quality of Life/Utility
;.(
Health State
Costs per Quality of Life/
Event ($) Utility Values
l Patients experienced no more than one ad- verse event per month; death could not occur during the month of an adverse event; pa- tients could have more than one adverse SRE, but the cost and quality of life decrement for each event was assumed to last only I month; systemic therapy costs were excluded, whereas
Pamidronate and no SRE 775 1.0
Radiation 5,500 0.6
Surgery 30,000 0.4
Spinal cord compression 20,000 0.2
Hypercalcemia I0,000 0.2
Other fractures” 600 0.8
*Asymptomatic or required only oral analgesics.
Data from Hillner a al.l4 I
bb BRUCE E. HILLNER
Chemotherapy Group
Endpoint Pamidronate Placebo
No. patients 185 195
Average survival (mo) 14.3 14.3
% survival at 24 months 29. I 29. I
Total SREs 387 630
Months without SRE 12.20 I I .07
Costs per patient (!$)
SRE costs 7,34 I 13,938 Pamidronate cbsts 10,564 -
Total costs 17,906 13,938 Additional costs 3,968 -
Total quality-adjusted life months 13.67 13.24
Total QALY I.140 I.103
Additional quality-adjusted life days 13.4
Net cost prevented SRE ($) per 3,940 -
Cost QALY ($) per 108,200 -
Table adapted from data published in Hillner et al.‘4
Hormonal Therapy Group
Pamidronate Placebo
182 189
17.5 17.5
48.2 48.2
475 648
14.68 13.86
8,218 12,634 12,101 -
20.3 I9 12,634 7.685 -
lb.56 lb.25
I.380 I.354
9.2
9,390
305,300
$3,968 in the chemotherapy group and $7,685 in
the hormonal therapy group). The net cost per prevented SRE and its subsequent treatment was $3,940 with chemotherapy and $9,390 with hor-
monal therapy. The cost-effectiveness ratios asso- ciated with pamidronate ranged from $108,200 in the chemotherapy cohort to $305,300 in the hor- monal therapy cohort per QALY. By using the assigned utility values reflecting the quality of life, it was estimated that the assigned costs of pamid- ronate per added QALY were higher than those of other commonly used treatments.
This study concluded that, though pamidronate is an effective supportive agent in metastatic breast cancer, it is associated with high financial
costs per adverse event avoided. The analysis per- formed was sensitive to pamidronate costs and asymptomatic pathologic fractures requiring only oral analgesics.
ECONOMIC ANALYSIS OF BISPHOSPHONATE USE
In recent years, quality of life and economic evaluations have gained increasing importance as additional measures in cancer clinical trials. De-
termining the costs of cancer care and identifying factors that predict costs are important for plan+ ning ethical resource allocation for cancer care. The costs of supportive therapies, such as bisphos-
phonates, depend on the purchasing price as well as costs associated with delivery and frequency of use.
Within the family of bisphosphonates there are numerous similarities in the pharmacologic effects of these supportive agents. However, differences exist in the side-effect profiles, rates of oral absorp- tion, and potency. At present, the two most widely used bisphosphonates in the treatment of meta- static cancer are pamidronate and clodronate, usu- ally administered intravenously and orally, respec- tively.i5
A European economic analysis has shown that the treatment of patients with malignant osteo-
lytic bone disease with pamidronate reduces pain significantly and does not add markedly to the costs.16 A Canadian perspective cost-utility anal- ysis has estimated that, though pamidronate has a high drug acquisition cost, it provides substantial quality-adjusted survival benefits to patients with advanced breast cancer at a reasonable cost.17
Clodronate is a second-generation bisphospho-
nate with intermediate potency, which may signif- icantly decrease the severity of bone pain and number of skeletal metastases associated with a decrease in skeletal morbidity. It is, therefore, speculated that clodronate may modify the natural history of bone metastases and improve the quality of life.i8 The economic impact of therapy with

PHARMACOECONOMIC ISSUES 67
prophylactic clodronate as an adjunct to chemo- therapy in the treatment of multiple myeloma has
recently been shown to increase the total costs.19 However, future work is required to determine the effect of prophylactic clodronate on the quality of
life of affected patients. This will enable clinical benefits and additional costs of this agent to be compared with other therapies.
THIRD GENERATION BISPHOSPHONATES AND PHARMACOECONOMICS
Infusions of pamidronate are time consuming,
whereas a small percentage of oral clodronate is absorbed, with the size and number of clodronate capsules required limiting compliance. The devel-
opment of new, more potent bisphosphonates may offer greater convenience by simplifying treat- ment. The third generation of bisphosphonates,
such as zoledronate and ibandronate, may improve the therapeutic effectiveness of this supportive therapy. Zoledronate is the most potent bisphos- phonate administered in humans; it is 100 to 850 times more potent than pamidronate in in vitro or animal models. Very low doses (l-2 mg) adminis- tered intravenously have been shown to achieve
normocalcemia in patients with tumor-induced hypercalcemia. 20 Ibandronate is another potent bisphosphonate that is available in both intrave-
nous and oral formulations. This new supportive agent is licensed in Europe for the treatment of hypercalcemia and is in clinical development for the treatment of osteoporosis as well as metastatic bone disease. A phase III double-blind, placebo- controlled trial of ibandronate in breast cancer metastatic to bone has shown that monthly infu- sions of ibandronate 6 mg result in a significant
reduction in skeletal-related morbidity.21 Both zoledronate and ibandronate are expected to be available in the United States soon.
It is probable that shorter infusion times of intravenously administrated bisphosphonates may reduce costs and oral administration could reduce
the cost even further. The efficacy and safety of currently available oral bisphosphonates in the treatment of bone metastases in cancer patients have recently been reviewed by using data derived from double-blind, placebo-controlled studies.2z The findings suggested that oral bisphosphonates are not as effective as intravenous formulations in reducing skeletal complications in patients with bone metastases because of their low oral bioavail-
ability. Therefore, new, more potent oral formula-
tions with higher bioavailability are currently in clinical development and are expected to improve the therapeutic effectiveness and convenience of treatment. Further development of this formula-
tion is currently awaited. Because pamidronate is currently the only
bisphosphonate approved by the United States Food and Drug Administration in the prevention of bone complications in metastatic breast cancer, competing bisphosphonates, such as zoledronate
and ibandronate, might permit cost leveraging. However, by using the model developed recently in the cost-effectiveness analysis of pamidronate in
this indication, and assuming that newer bisphos- phonates are priced roughly comparably with pamidronate, the benefits of these agents are likely
to be associated with substantial incremental costs.1° Market forces and pharmacoeconomic evaluations of this type may exert an impact on pricing, such that bisphosphonate treatment strat- egies become dominant with lower associated costs and higher quality-adjusted survival.
CONCLUSIONS
Future research should move from hypothetical cohorts assessed via models to evaluate the role of new generation bisphosphonates by using prospec-
tive data collected within clinical trials or inte- grated health delivery systems and to focus on medical improvement, quality of life, and cost effectiveness. Moreover, the duration of symptoms associated with SREs and their link with patient mortality should also be addressed. In this way, the difficult task of prioritizing limited health funding
from a disease-management perspective will be targeted. Pharmacoeconomic analyses will require new sources of funds that will not use scarce re-
sources from clinical trial groups. In summary, bisphosphonates are an important
class of agents used in the treatment of metastatic
bone disease. However, they do not prolong over- all survival in affected patients and they exert a major impact on the treatment costs of metastatic cancer. It is becoming increasingly clear that it is both practical and efficient to combine pharmaco- economic evaluation of bisphosphonates within a clinical trial to improve the estimates of direct and indirect costs of total resource consumption asso- ciated with the treatment of bony complications. It is expected that evaluation of their cost effec-

68 BRUCE E. HILLNER
tiveness would ultimately lead to rational use of these supportive agents in the area of oncology.
REFERENCES
1. Coleman RE: Skeletal complications of malignancy. Can-
cer 80:1588-1594, 1997 2. Clezardin P, Gligorov J, Delmas P: Mechanisms of action
of bisphosphonates on tumor cells and prospects for use in the
treatment of malignant osteolysis. Joint Bone Spine 67:22-29,
2000 3. Coleman RE: Uses and abuses of bisphosphonates. Ann
Oncol 11:179-184, 2000
4. Kanis JA: Rationale for the use of bisphosphonates in breast cancer. Acta Oncol35:61-67, 1996
5. Die1 IJ: Antitumour effects of bisphosphonates: First ev- idence and possible mechanisms. Drugs 59:391-399, 2000
6. Die1 IJ, Solomayer EF, Bastert G: Bisphosphonates and the prevention of metastasis: First evidences from preclinical
and clinical studies. Cancer 88:3080-3088, 2000 7. Pluijm G, Lowik C, Papapoulos S: Tumour progression
and angiogenesis in bone metastasis from breast cancer: New
approaches to an old problem. Cancer Treat Rev 26:11-27,
2000 8. Yoneda T, Michigami T, Yi B, et al: Use of bisphospho-
nates for the treatment of bone metastasis in experimental
animal models. Cancer Treat Rev 25293-299, 1999 9. Body JJ: Current and future directions in medical therapy.
Cancer 88:3054-3058, 2000
10. Hillner BE: The role of bisphosphonates in metastatic breast cancer. Semin Radiat Oncol 10:250-253, 2000
11. Theriault RL, Lipton A, Hortobagyi GN, et al: Pamid-
ronate reduces skeletal morbidity in women with advanced breast cancer and lytic bone sessions: A randomised, placebo-
controlled trial. Protocol 18 Aredia Breast Cancer Study Group. J Clin Oncol 17:846-854, 1999
12. Hortobagyi GN, Theriault RL, Lipton A, et al: Lone
term prevention of skeletal complications of metastatic breast cancer with pamidronate. Protocol 19 Aredia Breast Cancer
Study Group. J Clin Oncol 16:2038-2044, 1998
13. Hortobagyi GN, Theriault RL, Porter L, et al: Efficacy of pamidronate in reducing skeletal complications in patients with breast cancer and lytic bone metastases. Protocol 19
Aredia Breast Cancer Study Group. N Engl J Med 335:1785- 1791, 1996
14. Hillner BE, Weeks JC, Desch CE, et al: Pamidronate in
prevention of bone complications in metastatic breast cancer:
A cost-effectiveness analysis. J Clin Oncol l&72-79, 2000 15. Body JJ, Bartl R, Burckhardt P, et al: Current use of
bisphosphonates in oncology. International Bone and Cancer
Study Group. J Clin Oncol 16:3890-3899, 1998 16. Gessner U, Koeberle D, Thuerlimann B, et al: Economic
analysis of terminal care for patients with malignant osteolytic bone disease and pain treated with pamidronate. Support Care
Cancer 8:115-122, 2000 17. Dranitsaris G, Hsu T: Cost utility analysis of prophylac-
tic pamidronate for the prevention of skeletal related events in patients with advanced breast cancer. Support Care Cancer 7~271.279, 1999
18. Kanis JA, McCloskey EV: Clodronate. Cancer 80:1691- 1695, 1997
19. Bruce NJ, McCloskey EV, Kanis JA, et al: Economic impact of using clodronate in the management of patients with
multiple myeloma. Br J Haematol 104:358-364, 1999
20. Body JJ, Lortholary A, Romieu G, et al: A dose-finding study of zoledronate in hypercalcemic cancer patients. J Bone
Miner Res 14:1557-1561, 1999 21. Body JJ, Lichinitser MR, Diehl IE, et al: Double-blind
placebo controlled trial of ibandronate in breast cancer meta- static to bone. Proc Am Sot Clin Oncol 18:575a, 1999 (abstr)
22. Major PP, Lipton A, Berenson J, et al: Oral bisphospho- nates: A review of clinical use in patients with bone metastases.
Cancer 88:6-14, 2000