perspectives in diabetes can we really predict...
TRANSCRIPT

Perspectives in Diabetes Can We Really Predict IDDM? POLLY J. BINGLEY, EZlO BONIFACIO, AND EDWlN A.M. GALE
Risk of progresslon to IDDM has been assessed extensively in first-degree relatives of IDDM patients, and highly specific prediction is possible within a small subset of this population. Because -90% of future cases will come from those who have no close relative with IDDM, prediction and intenrention within the general population will become the main prlorlty for the future. This review presents a decision tree analysis of risk of progresslon to IDDM, highlights the different prognosis of markers when applled to those with and without a family history of the disease, and proposes a strategy for disease prediction in the latter. Large collaborative studies In well-characterized populatlons wlll allow new predlctlve markers and models to be evaluated, and strategies of intenrentlon to be tested with maximum efficiency and minimal delay. Dlabetes 42:213-20, 1993
- - - ~ - ~ ~
From the Department of Diabetes and Metabolism, St. Bartholomew's Hospi- tal, London, United Kingdom.
Address correspondence and reprint requests to Dr. Edwin A.M. Gale, Department of Diabetes and Metabolism, St. Bartholomew's Hospital, London FCIA 7BE UK --
~ e c e i d ior publlcatlon 16 October 1992 and accepted In revlsed form 3 November 1992.
IDDM, insulin-dependent diabetes mellitus; ICA, islet cell antibody; JDFU, Juvenile Diabetes Foundation Units; HLA, human leukocyte antigen; IAA, insulin autoantibody; GAD, glutamic acid decarboxylase; FPIR, first-phase insulin response, IVGT, intravenous glucose tolerance test; IGT, impaired glucose tolerance; OGn, oral glucose tolerance test; WHO, World Health Organization; ADA, American Diabetes Association; PPV, positive predictive value; ICARUS, islet cell antibody register user's study; FH, family history.
"All the business of war, and indeed all the business of life, is to endeavour to find out what you don't know b y what you do; that's what I call 'guessing what is on the other side of the hill.' "
-Arthur Wellesley, Duke of Wellington.
T he word prediction first came into the English language from the terminology of astrology ( I ) , and it only attained respectability with the rise of modern science. Even so, we need to be cau-
tious when applying the same term to the movements of the planets or to complex biology. Death apart, there are few certainties about the future behavior of biological systems. The term prediction, as applied to diabetes, implies a degree of inevitability that can, at present, only be achieved (if at all) in a small segment of the total population at increased risk of progression to IDDM. It is therefore both more accurate and more honest to ap- proach the issue in stochastic (probabilistic) terms and to talk of risk assessment rather than prediction and risk reduction rather than prevention, even though these drab alternatives might tend to divest the statements of the investigator of some glamour and potency.
In this reDort, we Dresent a brief overview of current ways of identifying nondiabetic individuals at increased risk of developing IDDM by using a decision tree ap- proach, and we consider the implications of our outlined strategy for current attempts to intervene in the preclini- cal prodrome.
To judge by the literature, pre-IDDM is a rarely de- scribed disorder, with perhaps 100-200 individuals studied prospectively from nondiabetes to insulin depen- dence. Despite this, the literature manifests considerable confidence that the disease can now be predicted with some accuracy by measurement of circulating autoanti-
DIABETES, VOL. 42, FEBRUARY 1993 21 3

body levels and insulin secretion in response to intrave- nous glucose. The aim of much of this activity is to identify a point of no return at which the potential risks of intervention might be justified. This strategy, therefore, strives to attain a specificity of prediction approaching 100%-with the unstated but inevitable consequence of loss of sensitivity. Because the relation of specificity to sensitivity is reciprocal, the more certain we become that individuals included in a predictive model will develop diabetes, the greater the proportion of those at risk we thereby exclude from the possible benefits of interven- tion. To reach these people-the great majority-re- quires an approach that will allow us to structure and evaluate lower degrees of probability.
How do we structure uncertainty? Clinical judgment is often almost reflexive but can be formalized and im- proved by decision analysis (2,3). The probability of a given outcome can be set out in a series of steps known as a decision tree, which provides a means of integrating the knowledge we use when handling a complex and evolving body of information. The probability of a given outcome can be refined at each successive step, and the utility of further diagnostic procedures evaluated in the light of information already available. Bayes' rule, de- scribed in the next paragraph, is intrinsic to this ap- proach.
"The common reasoning error of neglecting the base rate (3)" is most often encountered, within a medical context, in clinical evaluation of diagnostic tests. Simply stated, the predictive power of a test is related to the pre-existing level of risk in the individuals to whom it is applied. If this risk is high, the test will have a high yield of true positives, few false positives, and a high positive predictive power. Conversely, if risk is low, true positives fall, and the false-positive rate will rise, with a corre- sponding reduction in predictive power. Mathematical formulation was first given to these principles by Thomas Bayes, an eighteenth century nonconformist minister who published on divine benevolence and the theory of probability. This concept is inherent in the decision tree approach in which positive selection with sequential criteria results in an effective stepwise increment of the baseline risk. Absolute risk. Many factors influence the absolute risk of developing IDDM. This changes with age, rises to a peak around puberty, and recedes gradually through adult life (4). Dramatic geographical differences have been ob- served, such that a child born in Finland has 10 times the risk of developing diabetes as a child born in Northern Greece (5). Changes occur within a given population over time; the incidence in Finland rose by an average of 2.4% each year between 1965 and 1984 (6), and child- hood diabetes is now some 2-3 times more common in much of Europe than it was in the 1950s and 1960s (7). These considerations greatly modify the subsequent analysis; a test such as lCAs would be expected to have a higher predictive value in Finland than in Greece or in children rather than in adults. Familial risk. This represents the first branch in the decision tree. The lifetime cumulative incidence in sib- lings of a child with IDDM in Europid populations is
ICA 2 4JDFu I
I ICA-
c 0 . 1 %
baseline risk
I FH- 0.08%
FIG. 1. The rlsk of diabetes wlthln 5 yr In a sibling of an IDDM patlent; 6% of siblings will develop iDDM before age 20, glving a 1.5% average risk of IDDM wtthin 5 yr of 1.5%. The risks associated with detectable ICA 24 JDF U and ICA 220 JDF U are derived from life-table analysis in the Bart's-Windsor family study (13).
quoted at 5-8% (8,9) against a background cumulative incidence of -0.1-0.5%. In our own family studies, a sibling is -1 5-20 times more likely to develop diabetes before 20 yr of age than children from a background population in the same area with a sibling risk of 6% (P.J.B., E.B., E.A.M.G., unpublished observations) and a background risk of 0.3% (10). Parents and children of an individual with IDDM have been estimated to have 50- 66% the risk of siblings (8). An important consideration is that the proportion of new cases of childhood diabetes with an affected first-degree relative averages - lo%, with little apparent variation between high prevalence and low prevalence populations.
Although relatively few cases arise in family members, most information on risk markers of IDDM has been derived from studies within families, and we will consider this branch of the decision tree first (Fig. 1). We have chosen to illustrate the risks over a 5-yr period of fol- low-up because this has been widely used in prospec- tive studies and is feasible for trials of intervention. Siblings c20 yr of age have an average risk of develop- ing IDDM within 5 yr of 1.5%. Risk of ICA in relatives. Despite the technical difficulties encountered in ICA measurement (1 1) and uncertainty as to the target antigen(s), all current models of diabetes prediction are still based on this marker. lCAs are detect- able in 70-80% of new cases of childhood IDDM (12) and in 5-8% of first-degree relatives, provided a sensi- tive assay is used. Most future cases of IDDM are concentrated in this ICA+ subgroup, within which risk is directly proportional to ICA titer. Thus, 5% of first-degree relatives with ICA 4-19 JDF U and 35% of those with ICA 220 JDF U will require insulin within 5 yr; 60-70% will likely be on insulin within a decade (13,14), even though progression to diabetes does not appear inevitable in the remainder (15). Thus, this single marker has the power to identify a group of relatives who are more likely than not to develop diabetes within 10 yr. ICA measurement, therefore, provides an excellent stepping stone towards more specific prediction.
DIABETES, VOL. 42, FEBRUARY 1993
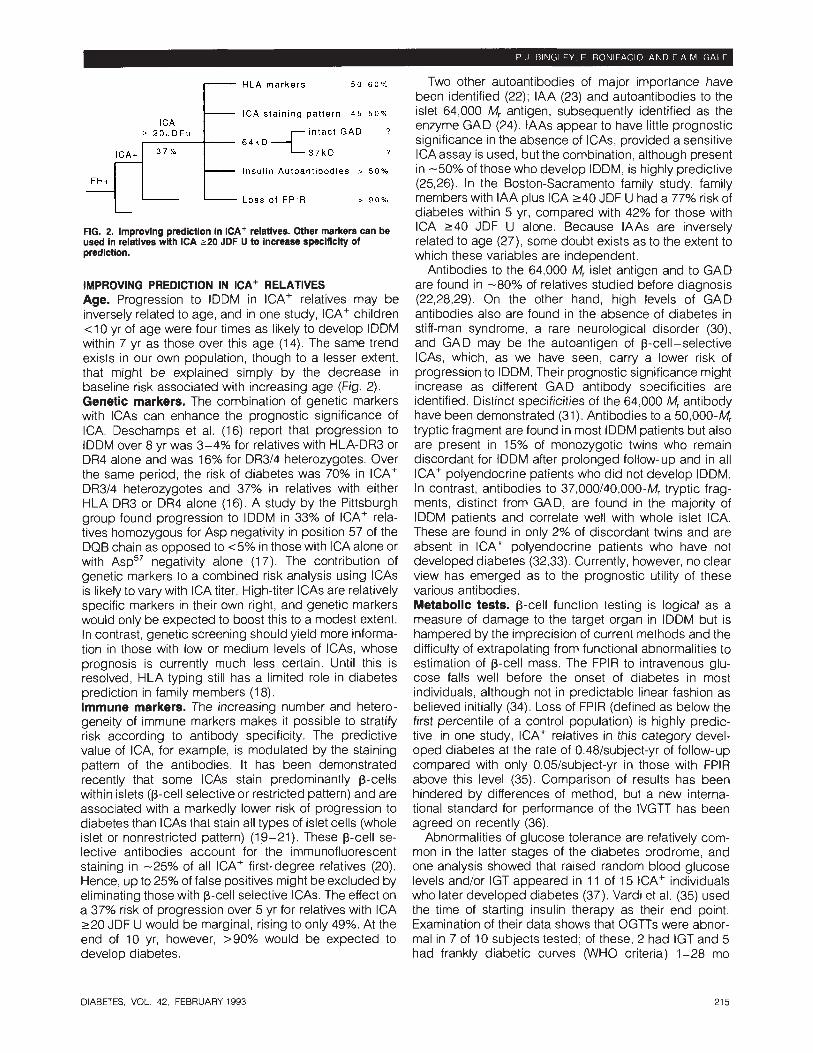
HLA marke rs 50.60% Two other autoantibodies of major importance have been identified (22); IAA (23) and autoantibodies to the
I C A sta in ing pat tern 45.50% islet 64,000 Mr antigen, subsequently identified as the
6 4 k D I ; t GAD I enzyme GAD (24). lAAs appear to have little prognostic significance in the absence of ICAs, provided a sensitive
? ICAassay is used, but the combination, although present Insul in Autoant ibod ies > 50% in -50% of those who develop IDDM, is highly predictive
(2.526). In the Boston-Sacramento family study, family L O S S o f FPIR , 90% members with IAA plus ICA 240 JDF U had a 77% risk of
diabetes within 5 yr, compared with 42% for those with FIG. 2. lmprovlng predictlon In ICA+ relatives. Other markers can be ICA 240 JDF Because lAAs are used in relatives with ICA 220 JDF U to Increase specificity of related to age (27), some doubt exists as to the extent to predlctlon. which these variables are independent.
Antibodies to the 64,000 Mr islet antigen and to GAD IMPROVING PREDICTION IN ICA' RELATIVES are found in -80% of relatives studied before diagnosis Age. Progression to IDDM in ICA+ relatives may be (22,28,29). On the other hand, high levels of GAD inversely related to age, and in one study, ICA+ children antibodies also are found in the absence of diabetes in <10 yr of age were four times as likely to develop IDDM stiff-man syndrome, a rare neurological disorder (30), within 7 yr as those over this age (14). The same trend and GAD may be the autoantigen of p-cell-selective exists in our own population, though to a lesser extent, ICAs, which, as we have seen, carry a lower risk of that might be explained simply by the decrease in progression to IDDM. Their prognostic significance might baseline risk associated with increasing age (Fig. 2). increase as different GAD antibody specificities are Genetic markers. The combination of genetic markers identified. Distinct specificities of the 64,000 Mr antibody with lCAs can enhance the prognostic significance of have been demonstrated (31). Antibodies to a 50,000-Mr ICA. Deschamps et al. (1 6) report that progression to tryptic fragment are found in most IDDM patients but also IDDM over 8 yr was 3-4% for relatives with HLA-DR3 or are present in 15% of monozygotic twins who remain DR4 alone and was 16% for DR3/4 heterozygotes. Over discordant for IDDM after prolonged follow-up and in all the same period, the risk of diabetes was 70% in ICA+ ICA+ polyendocrine patients who did not develop IDDM. DR314 heterozygotes and 37% in relatives with either In contrast, antibodies to 37,000/40,000-M, tryptic frag- HLA DR3 or DR4 alone (16). A study by the Pittsburgh ments, distinct from GAD, are found in the majority of group found progression to IDDM in 33% of ICA+ rela- IDDM patients and correlate well with whole islet ICA. tives homozygous for Asp negativity in position 57 of the These are found in only 2% of discordant twins and are DQB chain as opposed to <5% in those with ICA alone or absent in ICA+ polyendocrine patients who have not with Asp5' negativity alone (1 7). The contribution of developed diabetes (32,33). Currently, however, no clear genetic markers to a combined risk analysis using lCAs view has emerged as to the prognostic utility of these is likely to vary with ICA titer. High-titer lCAs are relatively various antibodies. specific markers in their own right, and genetic markers Metabolic tests. p-cell function testing is logical as a would only be expected to boost this to a modest extent. measure of damage to the target organ in IDDM but is In contrast, genetic screening should yield more informa- hampered by the imprecision of current methods and the tion in those with low or medium levels of ICAs, whose difficulty of extrapolating from functional abnormalities to prognosis is currently much less certain. Until this is estimation of p-cell mass. The FPlR to intravenous glu- resolved, HLA typing still has a limited role in diabetes cose falls well before the onset of diabetes in most prediction in family members (1 8). individuals, although not in predictable linear fashion as Immune markers. The increasing number and hetero- believed initially (34). Loss of FPlR (defined as below the geneity of immune markers makes it possible to stratify first percentile of a control population) is highly predic- risk according to antibody specificity. The predictive tive; in one study, ICA+ relatives in this category devel- value of ICA, for example, is modulated by the staining oped diabetes at the rate of 0,48/subject-yr of follow-up pattern of the antibodies. It has been demonstrated compared with only 0.05/subject-yr in those with FPlR recently that some lCAs stain predominantly p-cells above this level (35). Comparison of results has been within islets (p-cell selective or restricted pattern) and are hindered by differences of method, but a new interna- associated with a markedly lower risk of progression to tional standard for performance of the IVGTT has been diabetes than lCAs that stain all types of islet cells (whole agreed on recently (36). islet or nonrestricted pattern) (19-21). These p-cell se- Abnormalities of glucose tolerance are relatively com- lective antibodies account for the immunofluorescent mon in the latter stages of the diabetes prodrome, and staining in -25% of all ICA+ first-degree relatives (20). one analysis showed that raised random blood glucose Hence, up to 25% of false positives might be excluded by levels and/or IGT appeared in 1 1 of 15 ICA+ individuals eliminating those with p-cell selective ICAs. The effect on who later developed diabetes (37). Vardi et al. (35) used a 37% risk of progression over 5 yr for relatives with ICA the time of starting insulin therapy as their end point. 220 JDF U would be marginal, rising to only 49%. At the Examination of their data shows that OGTTs were abnor- end of 10 yr, however, >90% would be expected to mal in 7 of 10 subjects tested; of these, 2 had IGT and 5 develop diabetes. had frankly diabetic curves (WHO criteria) 1-28 mo
DIABETES. VOL. 42, FEBRUARY 1993
-
-
ICA r 2 0 J D F u
-
37% lCA+
FH+ -
-
before insulin was started. Predicting insulin depen- dence according to patterns of insulin secretion without regard to the coexistence of diabetes would be some- what illogical. Therefore, the ADAAd Hoc Committee has recommended that biochemical evidence of diabetes (defined by the OGl7 in asymptomatic individuals) should be the end point used in intervention trials rather than the clinical decision to use insulin (18). Even this approach is limited by poor reproducibility of the 2-h glucose value in the OGl7, so that, paradoxically, we still lack a well-defined reproducible end point for the early diagnosis of borderline diabetes. The dual parameter model. Elevated titers of IAA and loss of the FPlR are each strongly predictive of rapid progression in high-titer lCAC relatives. Preliminary re- ports indicate that a model based on combined analysis gives highly specific prediction in end-stage prediabe- tes, with progression within 3-4 yr in -90% of those identified, although prediction beyond 3 yr is less certain (38). This dual parameter model, described in outline as early as 1988 but not as yet published in full, has, in the interim, exerted enormous influence on attitudes to dia- betes prediction and prevention. It has, for example, been used to evaluate pilot testing of nicotinamide and insulin in high-risk individuals (39,40) and has been used as the basis for planning large-scale intervention studies. A model such as this must evolve through three stages. In the first stage, a retrospective correlation is made in a sample of individuals who have already progressed to diabetes; this is known as the practice set. In the second stage, the predictive formula is applied to an indepen- dent data set (the test set). If further refinement is needed at this stage to improve the fit, the new data should be considered a modified practice set and validated against a new test set. Finally, in the third stage, independent validat~on by other centers would be sought before the model is generally accepted.
Viewed in this perspective, the dual parameter model appears promising, but the process of evaluation is clearly far from complete. Its great attraction is that it appears to define what amounts to a point of no return, but this should not be assumed until it is more con- vincingly demonstrated. We have certainly seen persis- tence and even recovery from very low insulin secre- tory responses without progression to diabetes, and we have experienced both false-negative and false- positive results in our efforts to apply the model to our own population (P.J.B., E.B., E.A.M.G., unpublished observa- tions). Larger scale evaluation of this approach is clearly a matter of some urgency.
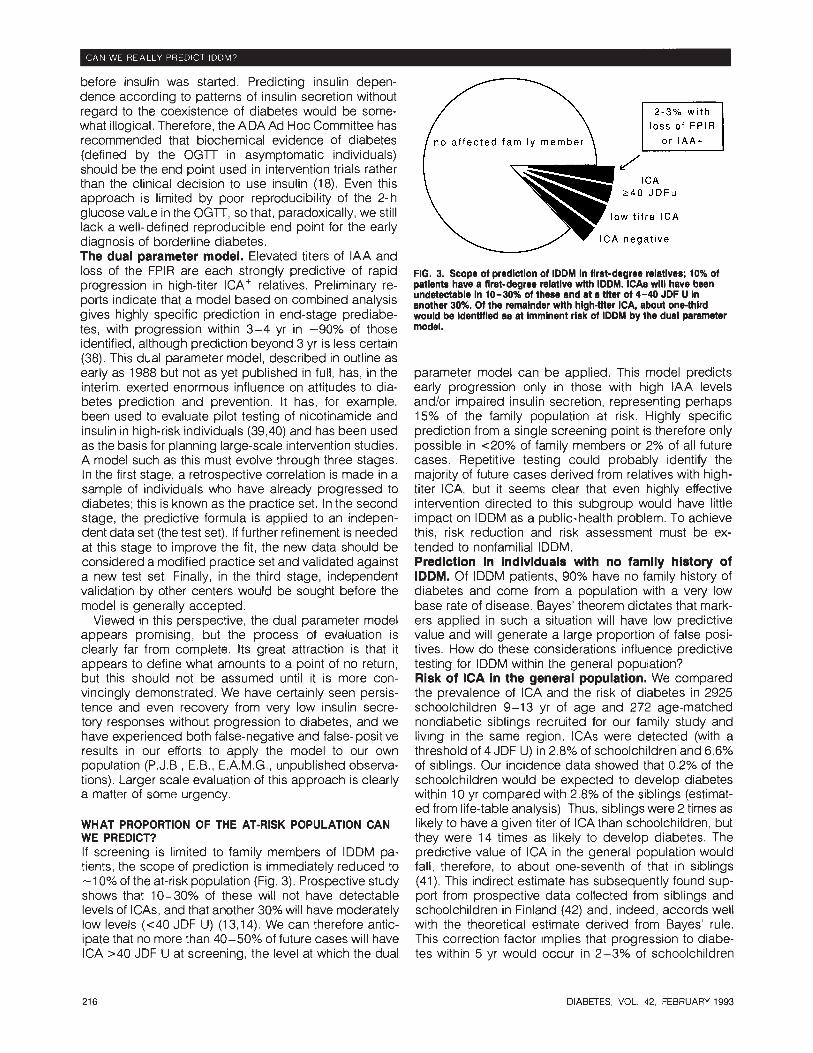
WHAT PROPORTION OF THE AT-RISK POPULATION CAN WE PREDICT? If screening is limited to family members of IDDM pa- tients, the scope of prediction is immediately reduced to -1 0% of the at-risk population (Fig. 3). Prospective study shows that 10-30% of these will not have detectable levels of ICAs, and that another 30% will have moderately low levels (c40 JDF U) (1 3,14). We can therefore antic- ipate that no more than 40-50% of future cases will have ICA >40 JDF U at screening, the level at which the dual
loss of FPlR
J ICA
240 J D F u
low t i t r e ICA
ICA negat ive
FIG. 3. Scope ot prediction ot IDDM in tlrst-degree relatives; 10% ot patients have a tirst-degree relative wlth IDDM. iCAs will have been undetectable in 10-30% ot these and at a titer ot 4-40 JDF U in another 30%. Ot the remainder with high-titer ICA, about one-third would be identitied as at imminent risk ot IDDM by the dual parameter model.
parameter model can be applied. This model predicts early progression only in those with high IAA levels and/or impaired insulin secretion, representing perhaps 15% of the family population at risk. Highly specific prediction from a single screening point is therefore only possible in ~ 2 0 % of family members or 2% of all future cases. Repetitive testing could probably identify the majority of future cases derived from relatives with high- titer ICA, but it seems clear that even highly effective intervention directed to this subgroup would have little impact on IDDM as a public- health problem. To achieve this, risk reduction and risk assessment must be ex- tended to nonfamilial IDDM. Prediction In individuals with no famlly history of IDDM. Of IDDM patients, 90% have no family history of diabetes and come from a population with a very low base rate of disease. Bayes' theorem dictates that mark- ers applied in such a situation will have low predictive value and will generate a large proportion of false posi- tives. How do these considerations influence predictive testing for IDDM within the general population? Risk of ICA in the general population. We compared the prevalence of ICA and the risk of diabetes in 2925 schoolchildren 9-13 yr of age and 272 age-matched nondiabetic siblings recruited for our family study and living in the same region. lCAs were detected (with a threshold of 4 JDF U) in 2.8% of schoolchildren and 6.6% of siblings. Our incidence data showed that 0.2% of the schoolchildren would be expected to develop diabetes within 10 yr compared with 2.8% of the siblings (estimat- ed from life-table analysis). Thus, siblings were 2 times as likely to have a given titer of ICA than schoolchildren, but they were 14 times as likely to develop diabetes. The predictive value of ICA in the general population would fall, therefore, to about one-seventh of that in siblings (41). This indirect estimate has subsequently found sup- port from prospective data collected from siblings and schoolchildren in Finland (42) and, indeed, accords well with the theoretical estimate derived from Bayes' rule. This correction factor implies that progression to diabe- tes within 5 yr would occur in 2-3% of schoolchildren
DIABETES, VOL. 42, FEBRUARY 1993

H L A m a r k e r s ICA 2 4 J D F u
Suscept ib le D Q combina t ion
I C A s t a i n ~ n g p a t t e r n L 2 0 J D F u 64.. -c;":,r G A D
Dual
FPlR r"' l A A
3pa;;;;er
basel ine risk
FH-
0 . 0 8 %
I A A e t c l C A r 7
2 . 2 %
O t h e r D Q a l l e l e s
I I
.-. . . G e n e t i c m a r k e r s
FIG. 4. A theoretical approach that uses DQ alleles and iCAs to predict IDDM in the general child population. The annual incidence of iDDM in our reglon Is 1611 00,000 to 20 yr of age. A child has a 0.08% risk of developlng iDDM wlthin 5 yr. DQw8, with no protective DQ alleles, is 27 times more common in IDDM patients than In control FIG. 5. The decislon tree.
subjects. This combination would confer a 2.2% risk of IDDM within 5 yr in this populatlon. ICA 2 4 JDF U elevates their calculated rlsk to
with detectable ICA and only 5-10% of those with ICA 2-20 JDF U. As predicted by Bayes' rule, lCAs alone have limited prognostic value in the general population (41). A strategy using multiple markers. Genetic markers are subject to the same limitations. High sensitivity is relatively easy to achieve, but current markers are so prevalent in the general population as to have low specificity. For example, in a recent Finnish study, no Asp residue was found at position 57 on either DQB chain in 74.5% of IDDM patients and 18% of control subjects, giving a relative risk for this genotype combination of 29, but a lifetime absolute risk of only 2%. A panel of four seauence-s~ecific oliaonucleotide Dr0bes was used to idehfy susceptible and DQ alleles, thus achieving the best segregation of patients and control subjects yet described in IDDM. DQw8, in the absence of a protective DQ allele, was found in 82% of IDDM patients compared with 3% of control subjects, giving a lifetime absolute risk in that population of 13.7% (43). Although this is inadequate as a basis for intervention, a strategy combining genetic and immune markers in series would allow much higher levels of risk to be defined within the general population (Fig. 4).
In this approach, the first test is used to identify a subgroup at increased risk, to which the second test then can be applied. The PPV of a test applied to a population of given disease prevalence can be given by the follow- ing formula (44):
PPV = (sensitivity x prevalence)
(sensitivity x prevalence) + [(1 -specificity) (1 -prevalence)].
Assuming that the sensitivity and specificity of ICA are similar in the general population and family members, the expected PPV of ICA 2-4 JDF U for developing IDDM can be estimated by using the sensitivity (88%) and specific- ity (96%) observed for the same assay in the Bart's- Windsor family study. In schoolchildren, this gives an expected PPV of 2% within 5 yr. If, however, ICA testing were confined to those already identified as genetically susceptible by DQ typing (again applying the Finnish oligonucleotide screen), the expected PPV would rise to
35%. If subjects with this susceptible DQ combination and ICA 2-4 JDF U were followed for 10 yr, -60% would be expected to develop IDDM; a level of prediction equivalent to that achieved by ICA 2-20 JDF U in family members. This approach obviously needs testing, bear- ing in mind that the genetic marker can be applied only within the population in which it was developed. More- over, any genetic screening method will be useful only if it can achieve a level of discrimination comparable with that reported in the Finnish study. Finally, note that tests that enhance the predictive power of ICA in family members could be applied in similar fashion to ICA+ genetically susceptible individuals and have the potential to reach equally high levels of specificity, albeit with corresponding loss of sensitivity.
DISCUSSION The approach to diabetes prediction outlined in this decision tree analysis (Fig. 5) has many advantages. It provides a simple and easily visualized framework within which it is possible to summarize and link a vast and evolving mass of data. The framework is flexible, easy to use, can be elaborated to finer detail if required, and the analysis involved could readily be held on computer. The approach forces the user to be explicit, and it is readily apparent that certain steps in our illustrative use of the model are well documented, whereas others rest on scanty data or speculation. Research efforts can be directed to these weak points, and initial judgments can be discarded or updated on the basis of later and more complete information.
Discussion of diabetes prediction tends to focus on the possibility of new and improved predictive markers in the hope that some future magic marker, with 100% speci- ficity and 100% sensitivity, will be identified. Sequential analysis of probability suggests that it is highly unlikely that any such marker will emerge. Further, it emphasizes that the prognostic significance of any marker varies in populations at differing levels of risk and shows that sequential analysis can overcome some of these limita- tions, at least in part. It demonstrates that adding in further tests has a limited yield once high specificity has been achieved by the preceding steps in the analysis, so that, for example, genetic testing has limited use in relatives with high titers of ICA. On the other hand,
DIABETES, VOL. 42, FEBRUARY 1993

Percentage of cases predicted
appropr ia te DQ a l le les
ICA2 4 0 J D F u
Max imum pos i t i ve pred ic t ive va lue
FIG. 6. The dual parameter model achieves high speclficlty with few false posltlves in famlly members but reaches a emall segment of the population at rlek. Screening In the general population Is needed to predict the majority of cases, and here predictive value may be increased by serial use of markers, although larger numbers of false positlves are Inevltebie.
genetic testing is likely to prove essential to diabetes prediction within the general population, and the neces- sary level of discrimination can be defined already.
Lack of standardization of assays and clinical proce- dures has been a recurrent theme in the quest for diabetes prediction. The need for standardization of assays led to the establishment of the Immunology of Diabetes Workshops, which have been instrumental in setting standards and assessing comparability. Another problem is that these assays have often been evaluated in inadequate population samples, ICARUS arose from the conviction that research into the pathogenesis of IDDM was being held back because the many clinical and population studies currently underway individually lack the power to evaluate new genetic or immune markers rapidly and definitively or lack the power to provide the basis for intervention trials designed to delay onset of the disease. The basic concept of the register has been to treat ICA+ in a nondiabetic individual as a rare disease, to establish standard methods of investiga- tion and follow- up, and to set up a shared database and bank of serum, served by international reference labora- tories. This resource will provide the basis for larger scale collaborative studies designed to provide rapid and convincing answers to some of the unanswered ques- tions identified in this review.
Two parallel and complementary strategies emerge from the analysis (Figs. 6 and 7). In the shorter term, highly specific prediction is essential if we are to evaluate novel strategies of intervention. With this approach, the smallest possible number of nonprogressors will be exposed unnecessarily to therapy, and hypotheses can be tested within a relatively short time in small samples of high-risk individuals. First-degree relatives are the logical source and are more likely to be motivated to take part. Specific prediction increases the potential benefit of therapy, implying that a higher margin of risk, for exam- ple, that involved in conventional immunosuppression, might be contemplated. Even if highly effective, however,
S t r a t e g y 1 S t r a t e g y 2
AIM: T E S T I N T E R V E N T I O N
S T R A T E G I E S
High speci f ic i ty1 low sens i t i v i ty
famil ies
immune marker
h igh r isk subgroup
AIM: R E D U C E I N C I D E N C E
O F I D D M
Low speci f ic i ty1 high sensit ivity
4 general populat ion
1 genet ic + immune markers
1 moderate r isk subgroup
FIG. 7. Complementary strategies in the prediction of IDDM.
such therapy would have limited relevance to the longer term aim of reducing the future incidence of IDDM.
The second strategy could be applied to a much larger segment of the at-risk population. The future course of attempted diabetes prevention will depend on our ability to identify risk within the total population. The strategy will necessarily entail loss of specificity, meaning that ther- apy would inevitably need to be offered to groups con- taining some individuals who would not in any case have developed the disease. This might seem abhorrent at first sight, especially when children are among those at risk. Risk estimation and risk reduction are nonetheless rou- tine elements of clinical practice. To take an example from another disease, middle-aged individuals with mod- erate hypertension are routinely offered antihypertensive therapy, even though the only confirmed benefit of this in one large trial was to reduce the risk of stroke over the next 10 yr from 2.6% in the placebo group to 1.4% in the treated group (45). We live in a society in which it is considered not only reasonable but necessary to treat this level of risk. In contrast to the level of risk described for hypertension, relatives with ICA 220 JDF U have a risk of diabetes >60% over 10 yr, and, as we have seen, equivalent levels of risk could potentially be identified in the general population.
Viewed in this light, it may seem less unreasonable to offer treatment to the whole group at risk, provided-and this is the key point-this therapy is relatively safe. In this context, a highly effective therapy with a relatively high rate of toxic side effects would offer a lower ratio of risk to benefit than a safer but less efficacious intervention. This must be a prime consideration in the development of novel forms of therapy, and it is logical that agents that appear relatively safe, such as insulin and nicotinamide, should have priority when clinical trials are undertaken.
Screening is itself a form of intervention. The outcome may be highly welcome to the people screened, as when the mother of a diabetic child can be reassured that her other children do not have detectable levels of ICA. But anxiety can be generated where none existed previously, as when the parents of a healthy child are informed that lCAs have been detected in the course of a research study. As confidence in screening procedures improves, they are likely to be used more widely and less critically.
DIABETES, VOL, 42, FEBRUARY 1993
Neaative conseauences of screenina include alertina the 11. Bonifacio E, Boitard C, Gleichman H, Shattock MA, Molenaar JL, --- - - u Bottauo GF: Assessment of precision, concordance, specificity, individual to a ribk for which no effective remedy e k t s . and sensitivity of islet cell antibody measurements in 41 assays,
unnecessary anxiety because of false-positive tests, or Diabetoloaia 33:731-36. 1990 -~ - - - - - -
inappropriate reassurance because of false-negative 12. Landin-Olsson M, Karlsson A, Dahlquist G, Blom L, Lernmark A,
tests, Adequate counselling and support should form an Sundkvist G: Islet cell and other organ specific autoantibodies in all children developing Type 1 (insulin-dependent) diabetes in Sweden
integral part of any screening program, and a simplified during one year and in matched control children. Diabetologia decision tree analysis could prove a useful way of 32387-95, 1989
helping individuals to reach their own decision concern- 13. Bonifacio E, Bingley PJ, Dean BM, Shattock M, Dunger D. Gale EAM, Bottazzo GF: Quantification of islet-cell antibodies and pre-
ing participation. Finally, consider the potential SOC~O~CO- diction of insulin-dependent diabetes. Lancet 335:147-49, 1990 nomic consequences of a positive screening test. The 14. Riley WJ, Maclaren NK, Krischer J, Spillar RP, Silverstein J, Schatz
label that is attached to an individual, perhaps incor- DA3 Schwam S, Malone J, Shah S, Vadheirn C, Rotter JI: A prospective study of the development of diabetes in relatives of
rectly, could harm his or her prospects for employment patients with insulin-dependent diabetes. N Engl J Med323:1167- and health insurance. Such consequences will accumu- 72, 1990
late in parallel with our ability to predict and intervene in 15. MCCUIIOC~ DK, Klaff LJ, Kahn SE, Schoenfield SL, Greenbaum CJ,
IDDM. Mauseth RS, Benson EA, Nepom GT, Shewey L, Palmer JP: Nonprogression of subclinical p-cell dysfunction among first-de- aree relatives of IDDM ~atients: 5-vr follow-UD of the Seattle Familv study. Diabetes 39549-56, 1990.
CONCLUSlONS 16. Deschamps I, Boitard C, Hors J, Busson M, Marcelli-Barge A, Complexity and uncertainty are intrinsic to risk assess- Mogenet A, Robert J-J, Life table analysis of the risk of Type 1
(insulin-dependent) diabetes in siblings according to islet cell merit in individuals predisposed to IDDM! particularly as antibodies and HLA markers. An 8-vear oros~ective studv. Diabe- , ,- , we strive to extend the s c o ~ e of re diction into the wider toloaia 35951-57, 1992 population. The overview brese"ted here suggests that, 17. LipGn RE, Lpor te RE: Dorman JS, Riley WJ, Trucco M, Becker DJ:
Acombination or HLA-DQ-p non-Asp-57 homozygosity and positive at present, no simple solutions are available, Insteadl a islet cell antibody (ICA) assay predicts insulin-dependent diabetes sustained research effort is likely to be needed. A major in relatives of children with IDDM (Abstract). Diabetes 40 (Suppl.
1):151A, 1991 collaborative research campaign linking the efforts Of 18. American Diabetes Association: Position Statement. Prevention of basic scientists with large-scale population studies offers Type 1 diabetes mellitus. Diabetes 39:1151-52, 1990 a logical approach. It would allow scientific develop- 19. Genovese S, Bonifacio E, Dean BM, McNally JM, Dean EM, Wagner
R, Bosi E, Gale EAM, Bottazzo GF: Distinct cytoplasmic islet cell ments in genetics, immunology, or immunothera~~ to be antibodies with different risks for Type 1 (insulin-dependent) diabe- evaluated in a clinical setting, and, where ap~rowriate, to tes mellitus. Diabetoloaia 35385-88. 1992 be applied to clinical with maxim'uh efficiency 20. Gianani R, Pugliese & Banner-Weir S, Schiffrin AJ, Soeldner JS,
Erlich H, Awdeh Z, Alper CA, Jackson RA, Eisenbarth GS: Prognos- and minimum delay. The challenge is greatl but so is the tically significant heterogeneityof cytoplasmic islet cell antibodies in reward. relatives of patients with Type 1 diabetes. Diabetes 41 :347-53,
1993 21. ~ k i i t J. Caillat-Zucman, Blondel H. Chedin P. Bach JF. Boitard C:
ACKNOWLEDGMENTS We thank the British Diabetic Association for its support of our clinical studies and the Juvenile Diabetes Founda- tion International for its support of ICARUS.
We thank Stephen G. Pauker for introducing us to decision-tree analysis: and those colleagues, in many countries, participating in the EURODIAB ACE, ICARUS, and ENDlT projects.
REFERENCES 1. Shorter Oxford English Dictionary. 3rd ed., Oxford, 1987. The first
citation is in "Dreams and Predictions of Astrologie," Bacon, 1563 2. Pauker SG, Kassirer JP: Decision analysis. N Engl J Med316:250-
58, 1987 3. McNeil BJ, Keeler E, Adelstein SJ: Primer on certain elements of
medical decision making. N Engl J Med 293:211-15, 1975 4. Laakso M, Pyorala K: Age of onset and type of diabetes. Diabetes
Care8:114-17, 1985 5. Green A, Gale EAM, Patterson CC, the EURODIAB Subarea A
Study Group: Incidence of childhood-onset diabetes mellitus: The EURODIAB ACE Study. Lancet 339:905-909, 1992
6. Tuomilehto J, Rewers M, Reunanen A, Lounamaa P. Lounamaa R, Tuomilehto-Wolf E, Akerblom HK: Increasing trend in Type 1 (insu- lin-dependent) diabetes mellitus in childhood in Finland: analysis of age, calendar time and birth cohort effects during 1965 to 1984. Diabetologia 34:282-87, 1991
7. Bingley PJ, Gale EAM: Rising incidence of IDDM in Europe. Diabetes Care 12:289-95, 1989
8. Tillil H, Kobberling J: Age-corrected empirical genetic risk estimates for first degree relatives of IDDM patients. Diabetes 36:93-99, 1987
9. Gamble DR: An epidemiological study of childhood diabetes affect- ing two or more siblings. Diabetologia 19:341-44, 1980
10. Binalev PJ. Gale EAM: The incidence of insulin-de~endent diabe- tes% '~n~ land : a study in the Oxford region 1985-6. Br Med J 298~558-60, 1989
lslet cell antibody heterogeneity among Type 1 (insulin-dependent) diabetic patients. Diabetologia 35792-95, 1992
22. Harrison LC: lslet cell antigens in insulin-dependent diabetes: Pandora's box revisited. lmmunol Today 13:348-52, 1992
23. Palmer JP, Asplin CM, Clemons P, Lyen K, Tatpati 0 , Raghu PK, Paquette TL: Insulin antibodies in insulin-dependent diabetes be- fore insulin treatment. Science 222: 1337-39, 1983
24. Baekkeskov S, Aanstoot HJ. Christgau S, Reetz A, Solimena M, Cascalho M, Folli F, Richler-Olesen H, de Camilli P: Identification of the 64K autoantigen in insulin-dependent diabetes as GABA-syn- thesizing enzyme glutamic acid decarboxylase. Nature (Lond) 347: 151-56, 1990
25. Ziegler AG, Ziegler R, Vardi P, Jackson RA, Soeldner JS, Eisenbarth GS: Life-table analysis of progression to diabetes of anti-insulin autoantibody-positive relatives of individuals with Type 1 diabetes. Diabetes 38:1320-25, 1989
26. Atkinson MA, Maclaren NK, Riley WJ, Winter WE, Fisk DD, Spillar RP: Are insulin autoantibodies markers for insulin-dependent dia- betes mellitus? Diabetes 35894-98, 1986
27. Vardi P, Ziegler AG, Mathews JH, Dib S, Keller RJ, Ricker AT, Wolfsdorf JI, Herskowitz RD, Rabizadeh A, Eisenbarth GS, Soeldner JS: Concentration of insulin autoantibodies at onset of Type 1 diabetes: inverse log-linear correlation with age. Diabetes Care 11:736-39, 1988
28. Atkinson MA, Maclaren NK, Scharp DW, Lacy PE, Riley WJ: 64,000 M, autoantibodies as predictors of insulin-dependent diabetes. Lancet 3351 357-60, 1990
29. Thivolet CH, Tappaz M, Durand A, Petersen J, Stefanutti A, Chate- lain P, Vialettes B, Scherbaum W, Orgiazzi J: Glutamic acid decar- boxylase (GAD) autoantibodies are additional predictive markers of Type 1 (insulin-dependent) diabetes in high risk individuals. Diabe- tologia 35570-76, 1992
30. Solimena M, Folli F, Aparisi R, Poua G, De Camilli P: Autoantibodies to GABA-ergic neurons and pancreatic p-cells in stiff-man syn- drome. N Engl J Med 322:1555-60, 1990
31. Christie MR, Vohra G, Champagne P, Daneman D. Delovitch TL: Distinct antibody specificities to a 64 kD islet cell antigen in Type 1 diabetes as revealed by trypsin treatment. J Exp Med 172:789-95, 1990
DIABETES, VOL. 42, FEBRUARY 1993

32. Christie MR, Tun RYM, Lo SSS, Cassidy D, Brown TJ, Hollands J, Shattock M, Bottazzo GF, Leslie RDG: Antibodies to GAD and tryptic fragments of the islet 64K antigen as distinct markers for development of IDDM: studies with identical twins. Diabetes 41: 782-87, 1991
33. Genovese S, Cassidy D, Bonfacio E, Bottazzo GF, Christie MR: Antibodies to 37140kD tryptic fragments of 64 kD antigen are markers of rapid progression to Type 1 insulin-dependent diabetes (Abstract). Diabetes Res Clin Pract 14 (Suppl. I):S11, 1991
34. Srikanta S, Ganda OP, Gleason RE, Jackson RA, Soeldner JS, Eisenbarth GS: Pre-Type 1 diabetes: linear loss of p-cell response to intravenous glucose. Diabetes 33:717-20, 1984
35. Vardi P, Crisa L, Jackson RA: Predictive value of intravenous glucose tolerance test insulin secretion less than or greater than the first percentile in islet cell antibody positive relatives of Type 1 (insulin-dependent) diabetic patients. Diabetologia 34:93-102, 1991
36. Bingley PJ, Colman PG, Eisenbarth GS, Jackson RA, McCulloch DK, Riley WJ, Gale EAM: Standardization of IVGl7 to predict IDDM. Diabetes Care 151 31 3-1 6, 1992
37. Tarn AC, Smith CP, Spencer KM, Bottazzo GF, Gale EAM: Type 1 (insulin-dependent) diabetes: a disease of slow clinical onset? Br Med J 294:342-45, 1987
38. Colman PG, Eisenbarth GS: Immunology of Type 1 diabetes - 1987.
In Diabetes Annual. 4th ed. Alberti KGGM, Krall LP, Eds. Amster- dam, Elsevier, 1988, p. 17-45
39. Dumont Herskowitz R, Jackson RA. Soeldner JS, Eisenbarth GS: Pilot trial to prevent Type 1 diabetes: progression to overt IDDM despite oral nicotinamide. J Autoirnmun 2:733-37, 1989
40. Keller RJ, Jackson RA, Eisenbarth GS: Preservation of p-cell func- tion in islet cell antibody (ICA) positive first degree relatives treated with insulin (Abstract). Diabetes 41 (Suppl. 1):13A
41. Bingley PJ, Bonifacio E, Shattock M, Gillmor, HA, Sawtell PA, Dunger DB, Scott RDM, Bottazzo GF, Gale EAM: Can islet cell antibodies predict insulin dependent diabetes in the general popu- lation? Diabetes Care 16:45-50, 1993
42. Knip M, Vahasalo P, Karjalainen J, Lounamaa R, Akerblom H, the Study Group in Childhood Diabetes in Finland: natural course of pre-type 1 diabetes in high risk individuals (Abstract). Diabetologia 35 (Suppl. 1):A32
43. Reijonen H, llonen J, Knip M. Akerblom HK: HLA-DQBl alleles and absence of Asp 57 as susceptibility factors of IDDM in Finland. Diabetes 40: 1640-44, 1991
44. Fletcher RH, Fletcher SW, Wagner EH: Clinical Epidemiology. 2nd ed. Baltimore, Williams and Wilkins, 1988, p. 56-58
45. Medical Research Council Working Party: MRC trial of treatment of mild hypertension: principal results. Br Med J 291:97-104, 1985
DIABETES, VOL. 42, FEBRUARY 1993