cdudocs.cdrewu.edu/assets/com/files/05.05.17 perspectives from the... · why? we need change- real...
TRANSCRIPT

Why Community Extension and
Transformation of the Medical
Model Matters: Perspectives
from the Community Health
Worker Model
Hector Balcazar, MS., PhD,
Dean
College of Science and Health
CDU
SPECIFIC LEARNING
0BJECTIVES
Describe Integration of the community health worker approach beyond medical model
Describe the key elements of the community health worker model
Describe outcome metrics used to evaluate community health worker programs

WHY CHW/PS? The Key to WHY is
Where are We Going?

Why? THE CHW/PS MODEL?

WHY? We Need Change- Real Change
in Healthcare and the Interdisciplinary
Workforce that Supports Public Health-
Prevention and Control-Management of
Disease Conditions

Real changes are needed
1. How the community systems work?
2. How the infrastructure is used?
3. How to integrate models?

WHY: Invest Differently-
Power of Prevention
Prevention accounts for 25
of 30 years of life gained in the past century

HEALTH CARE IS VERY EXPENSIVE-NOT EFFECTIVE FOR PREVENTION-CURATIVE MODEL IS WHAT WE HAVE!
“The healthcare sector is far and away the most inefficient economic driver in the U.S.”
Peter Orszag, Director, OMB
30% of what we spend adds no clinical value (5% of GDP) – Institute of
Medicine
4.4 million hospital admissions totaling $30.8 Billion in hospital costs could
have been prevented – AHRQ

Barriers = liability, siloed training,
competition, economics
Community Health
Worker
Non-Physician
Provider
Generalist
Specialist
Most
Highly
Specialized
Specialist
Generalist
Non-Physician
Provider
Community Health
Worker
Handshakes = Incentives to collaborate,
partner, interdisciplinary training to build
better teams
Most
Highly
Specialized

Individuals
Clinics/Hospitals
Communities
Nighborhoods
Society-
Systems, Policy
If We Believe There is Real Rationale for Why?
Where to Interject the CHW Model If We Create
Handshakes for Influencing Change?
Family


Diabetes In the U.S., about 7% of
adults reported having been diagnosed with diabetes; in Doña Ana County, almost 10% of adult residents reported having diabetes.
Hispanics in the El Paso area are more likely to have been diagnosed with diabetes than non-Hispanics.

Sharing the Initial Story
50.8
66.8
44.7
67.2
0
10
20
30
40
50
60
70%
of
Yes
Intervention Group Control Group
Family History of Heart Disease Family History of Diabetes
Fifth one percent of the intervention group and 45% of the control group reported having a relative with cardiovascular disease. In both groups, 67% of the participants reported having a relative with Diabetes.

Use of Medication
More than 40% of the participants in both groups used medication to control the blood pressure. Nearly 30% used medication to reduce the blood cholesterol, and 25% of the intervention group and 22% of the control group used medication to control the diabetes.
0
5
10
15
20
25
30
35
40
45
Intervention Group Control Group
25
22.1
42.1 41.9
2927.3
%
Use of Diabetes Medication Use of Hypertensive Medication Use of Cholesterol Medication

Few Examples
Building Models
Clinical- Community-
Ecological

Strengthening the CHW-Approach
Through Accountability- A Start-
• Start The Legacy!!
• Begin The Journey:
Balcazar et al, 2011-
J Ambulatory Care Manage Vol 34(4):362-372
by Paulina Matias, TX

Versatility of PS-CHS Within Their Roles/
Functions?
Connection
to
community
served*
Cultural
Mediation
Health
Education
Assuring
Access to
Care
Informal Counseling
and
Social Support
Individual and
Community
Advocacy
Provision
of Direct
Service
Individual
and
Community
Capacity
Building

Versatility: New Accomplishments
Fresh Out Of The Field
Rosenthal et al, [email protected]:2016
• The Community Health Worker Core Consensus (C3) Project:
• 2016 Recommendations on CHW Roles, Skills, and Qualities
• Recognition of 10Roles:
• Participation in Evaluation and Research-Implementing Assessments
• Recognition of 8 Skills• Communication Skills,
• Interpersonal and Relationship-Building Skills,
• Service Coordination and Navigation Skills,
• Capacity Building Skills
• Advocacy Skills,
• Education and Facilitation Skills,
•
Individual and Community Assessment Skills
, Outreach Skills

Our Opportunities
Some Reflections
Key Points: Ingredients: Setting: Clinical, Community, Ecological or Hybrids
Ingredients: Capacity Readiness for the CHW Model including –infrastructure-
stages of development of CHW/PS workforce, coalition, groups

Our Opportunities
Some Reflections
Ingredients: CHW/INPUT Sitting at the Table- What would they bring? What training they have- they need? Can a team be integrated from the get go!
Can we infuse CBPR into the mix?
Ingredients: Can I develop the MODEL of
CHWs with what I have thus far?
How would it look like thus far?

Research Opportunities
Some Reflections
Ingredients: Can I Build The Complete Story of the CHW as a Change Agent
What do I mean by change agent?
What are the core elements and active ingredients of community health worker programs? Practice-Based versus Evidence-Based
Can I establish Fidelity/”Validity”
through a research design, CBPR,
Qualitative, Quantitative Evaluation?

Effectiveness- Right on Target!!!
The Community Guide: What Works to Promote Health?
Interventions Engaging
Community Health Workers-
Community Preventive Services
Task Force Recommendation

Promotores de Salud: A Partnership
Model With Medical/Health Sectors
Promotores
Promotores train family members
Family members train
other family members

Promotoras
MD Visit
AssessmentMD Education
(verbal and printed handouts)
Treatment PlanLabs
MedicationCare Plan
Care that Includes PromotorasBalcazar et al 2009. Prev Chronic Dis (6)1
MD Follow up 1 month:Review labs & initial
treatment plan
MD Follow up x 3 months, as needed
Patient educated and more informed
MD visits are more focused, less follow up required
Extensive Education Using glucometer Education on medication use How to check feet How to identify complications Support for lifestyle changes Mental health screening
Group classes and individual support
Appt scheduledReferral to
Promotora program

Sample Results
8.7
7.4
6.5
7
7.5
8
8.5
9
Baseline 3-month
63.3
90.9
0
20
40
60
80
100
Baseline 3-month
•88% Retention Rate in SM Courses;
•49% of clients return to the support groups;
•LDL Cholesterol
Baseline-116 Twelve Months-97
Average-A1c value Knowledgen=29 n=29

Potential Opportunities: Key Successes to Integration
Open and frequent communication
Wide organizational acceptance of promotoras
Regular status meetings to assess progress, identify issues
Extensive training for promotoras
Thorough documentation
Management support
Provider involvement (training, recruitment, support, participation)
Regularly assess patient satisfaction/feedback

THE SPSC-CHW MODELS: Clinical, Community and Ecological Approaches
SPSC-NCLR- Balcazar et al: Prev Chronic Dis 2005, Health Prom Practice 2006
SPSC-UNT- Am J Health Educ 2007, Medina et al
SPSC-NHLBI-HRSA- Balcazar et al, Prev Chronic Dis Jan 2009
SPSC-CDC-UTSPH- Balcazar et al, JHCPU, Nov 2009
SPSC-UTSPH-UTEP NIH HEART1@2- Balcazar et al, PrevChronic Dis March 2010, Education For Health, 2009; PrevChronic Dis Jan 2012, Health Education & Behavior 2012

Phase 1 – HEART INTERVENTION
CBPR RCT
CHAC
192 cases/ 136 controls
2 month CHW-led heart
health education
2 month CHW follow-up
Inputs Evaluation
Clinical Evaluation
BMI, waist circumference
Cholesterol, A1C, blood pressure
HEART Questionnaire
Demographics
Acculturation scale
Stages of change scales
Heart health beliefs
Dietary behaviors
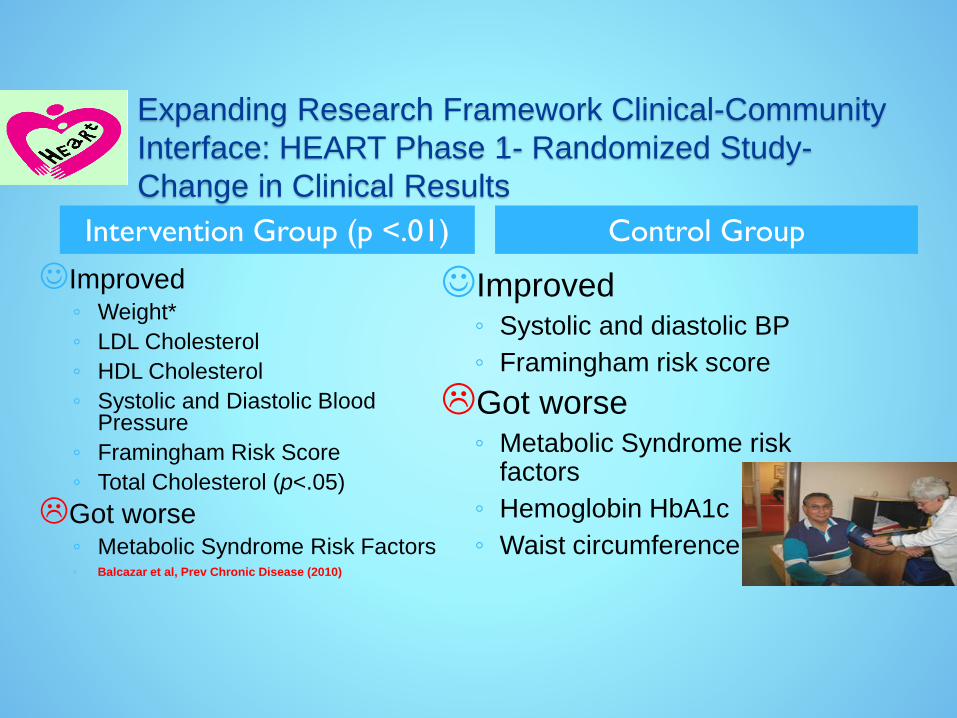
Improved◦ Weight*
◦ LDL Cholesterol
◦ HDL Cholesterol
◦ Systolic and Diastolic Blood Pressure
◦ Framingham Risk Score
◦ Total Cholesterol (p<.05)
Got worse◦ Metabolic Syndrome Risk Factors◦ Balcazar et al, Prev Chronic Disease (2010)
Improved◦ Systolic and diastolic BP
◦ Framingham risk score
Got worse◦ Metabolic Syndrome risk
factors
◦ Hemoglobin HbA1c
◦ Waist circumference
Intervention Group (p <.01) Control Group
Expanding Research Framework Clinical-Community
Interface: HEART Phase 1- Randomized Study-
Change in Clinical Results

The HEART Participant’s Environment
Balcazar et al. 2012 Prev Chronic Dis Vol 9 (11_0100)
www.kentonthemove.org/img/Socio-EcologicalMod..
PolicyAgents: Policy makers
CommunityAgents: Community members, leaders
OrganizationsAgents: YWCA, Parks and Rec Dept., CHALC,
UT—El Paso, UT-SPH, Centro San Vicente, EPCC
InterpersonalAgents: CHWs, family, friends, social networks
IndividualAgents: HEART participant
CBPR Context

Lifestyle/NutritionYour Heart Your Health
Charlas
Cooking Demonstrations
Environmental/Nutrition
Grocery Store Tours
Lifestyle/Fitness
Aerobics
Swimming
Zumba
Environment/Exercise Walking Groups
Soccer and Basketball
CHWPromotores de
Salud
Lifestyle/Environment ProgrammingMy Heart My Community – Mi Corazón Mi Comunidad

0%
20%
40%
60%
Ch
an
ge in
% o
f p
eo
ple
co
nsu
min
g
5 F
&V
/day
Quartiles for number of total sessions attended
Baseline to 4-month change in % consuming 5 Fruits &
Vegetables/day by quartiles
1 2 3 4
**
**
**
Figure: Greater utilization of community resources (attendance) is associated with
greater increases in proportion of participants consuming 5 fruits and vegetables a day at
4-months

Sustainability! Not on Target!!!
Effectiveness,
Versatility,
Workforce Dev.,
Occupation Reg.
Regulation,
Financing, Eval.
and Research
Advocay!

New Directions: Building Sustainabilty
Through Financial Models for CHWs
Structures amenable to greater inclusion of
CHWs: FQHCs payment formulas with HRSA,
Medicaid, Medicare
Structures that promote diversion of ERs-
Hospitals
Structures for long term care and chronic
disease management
Examples of Return on Investment (ROI):
Molina Health Care, New Mexico, Arkansas
Long Term Care, Many More

What is Being Learned From Programmatic Level
Efforts of CHWs- Towards and Advocacy-Policy Model
to Build Sustainability
National Community Health Worker Advocacy
Survey- Sabo et al., 2015
The strongest correlate of advocacy was
membership in CHW association
Community health workers are highly effective
in networking and advocacy efforts to advance
the workforce
Employers stand to benefit from CHW
professional advocacy and play a major role
CHW professional advocacy has resulted in
policy change

What is Being Learned From Programmatic Level
Efforts of CHWs- Towards And Advocacy-Policy Model
to Build Sustainability
“To ensure sustainability of workforce. CHW
networks, employers, state and federal, and
allies should be INTENTIONAL in creating
opportunities for CHWs to promote: 1)
professional identity, 2) increase public image of
CHW roles and skills, 3) develop professional
collaboration, 4) promote workforce-related
legislative and policy initiatives to advance and
sustain the workforce”
” More broadly, CHWs should make up at least
51% of any governing board making decision
regarding the workforce”

Individuals
CHWs Philosophy,
Orientation
CommunitiesSociety
NECESSARY Perspective YES: Synergy and
Cooperation: The Influence of CHWS-
Promotores –Getting Out of the Margins of Work
Family

TRANSFORMATIONAL MODELS with
CHWs in the Context of Variety of Teams-
Approaches-Philosophies towards Building
Equity-Justice
Can we create and validate an agenda of transformational opportunities for CHWs as part of interdisciplinary team packages of key functions, with: health and health care, prevention, wellness, life satisfaction?
Can CHWs help close the gap for meeting a Transformational Agenda?
Can we Move to A HOLISTIC APPROACH TO THIS TRANSFORMATION –IN and OUT OF THE HEALTH SYSTEM?
ARE WE BUILDING ONLY A HEALTH STORY or A HUMAN STORY WITH CHWS- PROMOTORES DE SALUD for A Better World, A better Country?

Moving Toward and Empowerment/Transformational Model: The
Will to Create Change Through Advocacy for Policy Enactment
and Application
Individual Policy Components: Recognition.
Credentialing, Training and Supervision, Scope
of Practice, Career Paths and Workforce
Development
Work-force-level Policies: Financing,
Occupational Regulations, Parameters of
Evaluation
System Level Policy Integration: Strengthen
Community Action, Effective Systems’ Change
for Health Equity
Torres, Balcazar et al, Critical Public Health, 2017

THANKS-
Hector Balcazar and HEART team
And Team: Carl Rush, Lee Rosenthal, Jackie
Scott- from the Institute for Health Policy, The
University of Texas Health Science Center
Houston, School of Public Health, and El Paso
Regional Campus, the HEART TEAM!