peritonitis due to thermoascus taitungiacus (anamorph ...jcm.asm.org/content/39/2/720.full.pdf ·...
TRANSCRIPT

JOURNAL OF CLINICAL MICROBIOLOGY,0095-1137/01/$04.0010 DOI: 10.1128/JCM.39.2.720–724.2001
Feb. 2001, p. 720–724 Vol. 39, No. 2
Copyright © 2001, American Society for Microbiology. All Rights Reserved.
Peritonitis Due to Thermoascus taitungiacus(Anamorph Paecilomyces taitungiacus)
ASHER KORZETS,1,2 MIRIAM WEINBERGER,2,3* AVRY CHAGNAC,1,2
ANNA GOLDSCHMIED-REOUVEN,2,4 MICHAEL G. RINALDI,5,6
AND DEANNA A. SUTTON6
Department of Nephrology, Golda Campus,1 and Department of Internal Medicine C & Infectious Diseases, BeilinsonCampus,3 Rabin Medical Center, Petach-Tikva, Mycology Unit, Chaim Sheba Medical Center, Tel-Hashomer,4 and
The Sackler School of Medicine, Tel-Aviv University, Ramat-Aviv,2 Israel, and Audie L. Murphy Division,South Texas Veterans Health Care System,5 and Fungus Testing Laboratory, Department of Pathology,
University of Texas Health Science Center,6 San Antonio, Texas
Received 21 August 2000/Returned for modification 19 September 2000/Accepted 1 December 2000
The first case of human disease due to the thermophilic ascomycete Thermoascus taitungiacus (the teleo-morph of Paecilomyces taitungiacus) is presented. T. taitungiacus was recovered from four dialysate fluidspecimens of a 57-year-old patient undergoing chronic peritoneal dialysis. Identification was based uponcylindrical conidia, reddish orange nonostiolate ascomata, lack of growth at 20°C, thermotolerance, andascospores that appeared pale yellow, elliptical, thick walled, and predominately echinulate by light microscopybut irregularly verrucose by scanning electron microscopy.
Paecilomyces species are found worldwide in soil, water, anddecaying vegetation (13, 29) and are microscopically similar toPenicillium and some Aspergillus species. While they are un-common human pathogens, they have been associated withserious infections in both immunosuppressed and immuno-competent patients, especially those with defects in the ana-tomic barriers or with a foreign body. Five species in the genusPaecilomyces have been reported to cause infection, includingPaecilomyces variotii, Paecilomyces lilacinus, Paecilomyces mar-quandii, Paecilomyces viridis, and Paecilomyces javanicus (13).The most commonly reported infections are keratitis, endoph-thalmitis, and cutaneous infections. Fungemia, prosthetic valveendocarditis, lung infections, sinusitis, and peritonitis are lessfrequently reported (11, 20, 23, 24, 26, 29). Thermoascus crus-taceus has been reported from monocyte cultures of patientswith AIDS (14). We report what we believe to be the first caseof human mycosis due to the ascomycetous fungus Thermoas-cus taitungiacus causing peritonitis in a patient undergoingchronic peritoneal dialysis (CPD).
Case report. A 57-year-old man presented on 25 October1998 with a 5-day history of abdominal pain. Since 1994 thepatient had been treated with CPD for end-stage renal failuredue to chronic glomerulonephritis and malignant hyperten-sion. He had had two episodes of bacterial peritonitis in 1996.Physical examination on admission revealed diffuse abdominaltenderness compatible with peritonitis. Empirical intraperito-neal treatment with cefazolin, 0.5 g/2 liters, and aztreonam, 0.6g/2 liters, was started following a cell count of the turbid dia-lysate effluent that revealed 250 white blood cells/mm3 (35%neutrophils, 10% lymphocytes, and 55% monocytes). Threeadditional dialysate fluids were collected on October 27 and 29
and November 1. Each was plated onto blood, MacConkey,chocolate, and Sabouraud dextrose agar (SDA) plates (HyLaboratories, Rehovot, Israel), as well as Lowenstein-Jensen medium agar tubes (Heipha Diagnostika, Heidelberg,Germany), and incubated at 35°C. All bacterial cultures werenegative, but by early November a tan-colored mould grew inpure culture on the Sabouraud agar plates from the four sep-arate dialysate fluid specimens. Intravenous amphotericin B(40 mg/day) was started, and the indwelling Tenckhoff catheterwas removed. Hemodialysis was thereafter maintained via atemporary central vein catheter.
Amphotericin B was discontinued after 2 weeks of therapydue to intolerance (severe and repeated vomiting), liver toxic-ity (elevated serum alkaline phosphatase levels), and the de-velopment of a deep vein thrombosis of the upper limb. Oralketoconazole (200 mg/day) was then given for 2 weeks but wasstopped due to the appearance of fever, the accumulation ofascitic fluids, and worsening abdominal pain. The patient be-came severely catabolic with an accompanying weight loss of 5kg and hypoalbuminemia of 24 g/liter. Amphotericin B therapywas restarted on December 6 and was given thrice weekly atthe end of each hemodialysis session together with intradialyticparenteral nutrition. Fever abated and abdominal pain im-proved; however, no improvement was seen in either the asciticfluid volume or the ascitic white cell count. On 20 January1999, oral itraconazole (400 mg/day) was substituted for am-photericin B, resulting in a gradual decrease in the accumula-tion of ascitic fluid and complete disappearance of the abdom-inal pain. The patient started to gain weight, and his serumalbumin level increased to 37 g/liter. Itraconazole was discon-tinued after 5 months of therapy. Repeated dialysate fluidcultures since November 1 were all sterile.
In July 1999, one month after the discontinuation of itra-conazole therapy, an enlarging right kidney mass, diagnosedhistologically as renal cell carcinoma, was removed at nephrec-
* Corresponding author. Mailing address: Internal Medicine C &Infectious Diseases, Rabin Medical Center, Beilinson Campus,Petach-Tikva 49100, Israel. Phone: 972-3-9378210. Fax: 972-3-9221605.
720
on July 8, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

tomy. Two years later the patient is doing well on hemodialysisand remains asymptomatic.
Mycologic studies. The mould isolated from the peritonealfluids was initially identified as a Paecilomyces species at theMycology Unit, Chaim Sheba Medical Center, Tel-Hashomer,Israel. It was then referred to the Fungus Testing Laboratory,Department of Pathology, University of Texas Health ScienceCenter at San Antonio, San Antonio, Texas, where the finalidentification of T. taitungiacus was made and susceptibilitytests were performed. The isolate was accessioned as UTHSCR-3084, subcultured onto in-house-made (21) potato flakesagar (PFA) and SDA (Remel, Lenexa, Kans.), and incubatedat 25, 35, and 42°C. A slide culture was also prepared on PFAand incubated at 25°C. Growth of the isolate on PFA (Fig. 1A)and SDA revealed colonies that were initially flat and buffcolored but that quickly (within 6 days) became yellowish or-ange with a brownish yellow reverse. Sparse conidial structuresof the Paecilomyces anamorph were evident between 3 and 4days at 25°C on PFA. Conidia were initially cylindrical torectangular, approximately 7 to 7.8 by 2.9 to 3.9 mm, and thenbecame elliptical to subglobose (Fig. 1C). With the formationof a Paecilomyces anamorph, additional subcultures onto Cza-pek Dox and malt extract agar (MEA) (Remel) at 35°C weremade in an attempt to induce ascospore formation. Colonieson MEA became reddish orange and granular to crust-likewith a brownish orange reverse (Fig. 1B). Globose, nonostio-late ascomata occurred within 7 days on Czapek Dox agar (Fig.1D) and contained asci that were approximately 15.6 by 11.7mm (Fig. 1E). Ascospores were elliptical, pale yellow, thickwalled, approximately 4 to 5 by 6.8 mm, and predominatelyechinulate by light microscopy (Fig. 1F). Ascospores were sub-sequently examined by scanning electron microscopy (SEM).Briefly, stubs were mounted with Spot-O-Glue Avery labels(Diamond Bar, Calif.) and touched to the fungal culture. Prep-arations were coated with gold-palladium using a DentonBench Top Turbo III vacuum evaporator (Morristown,N.J.) and were examined with a LEO 435 VP digital scanningelectron microscope (Thornwood, N.Y.). When viewed byscanning electron microscope, ascospores appeared irregularlyverrucose (Fig. 1G).
Temperature studies were also performed by inoculating fiveplates of MEA (Remel) in triplicate with a 1-mm portion ofthe case isolate. Plates were incubated at 18 to 20, 25, 30, 35,and 42°C for 6 days, and zone sizes were measured with cali-pers. Temperature studies performed on day 6 indicated meancolony diameters at 20, 25, 30, 35, and 42°C of 0, 16, 85, 85, and60 mm, respectively. The most abundant ascocarp formationoccurred at 30 and 35°C, while maximum conidial productionoccurred at 42°C.
Susceptibility studies. The case isolate and the P. variotiicontrol strain UTHSC 90-459 were evaluated for in vitro an-tifungal susceptibility by the National Committee for ClinicalLaboratory Standards broth macrodilution method M27-A(19) modified for mould testing (9, 10). Results indicated 24-and 48-h MICs of amphotericin B of 0.25 mg/ml. Itraconazole24- and 48-h MICs were ,0.015 and 0.06 mg/ml, respectively.Based upon achievable drug concentrations using standarddosing regimens, the isolate appeared susceptible, in vitro, toboth antifungal agents tested.
Paecilomyces species lacking known teleomorphs that have
TA
BL
E1.
Com
parisonof
featuresof
thermophilic
Therm
oascusspecies
Feature
Characteristics
of:
T.taitungiacus a
T.crustaceus b
T.aegyptiacus c
T.aurantiacus d
T.therm
ophilus e
Conidiogenesis
PhialidicPhialidic
PhialidicPhialidic
Annellidic
Anam
orphP
.taitungiacus fP
.crustaceusP
.aegyptiacus gN
oneor
evanescentP
aecilomyces-like
Polypaecilium
species9
daysgrow
that:
16°C2
22
22
20°C2
12
26
25°C1
11
21
30°C1
11
21
35°C1
11
11
40°C1
11
11
50°C1
11
11
LM
hascospore
texturePredom
inatelyechinulate
iF
inelyechinulate
Nearly
smooth
Finely
echinulateSm
oothSE
Mascospore
textureIrregularly
verrucoseF
inelyechinulate
Slightlyverruculose
Very
minutely
verrucosej
Verruculose
k
aT
.taitungiacusK
.Y.C
henand
Z.C
.Chen
sp.nov.b
T.crustaceus
(Apinis
andC
hesters)Stolk.
cT.aegyptiacus
Ueda
andU
dagawa.
dT
.aurantiacusM
iehe.eT
.thermophilus
(Sopp)von
Arx.
fConidia
ofall
Paecilom
ycesanam
orphsw
ereinitially
cylindrical,laterbecom
ingellipticalto
subgloboseor
globoseat
maturity.
gNot
allauthoritiesbelieve
thisis
adistinct
species(13).
hL
M,light
microscopy.
iEchinulate
isdefined
ashaving
sharplypointed
spines,delicatelyspiny.
jVerrucose
indicatesdelicately
verrucose.k
Verruculose
isdefined
ashaving
small,rounded
processesor
warts.
VOL. 39, 2001 NOTES 721
on July 8, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
722 NOTES J. CLIN. MICROBIOL.
on July 8, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

been cited as human etiologic agents include P. variotii, P.lilacinus, P. marquandii, P. viridis, and P. javanicus (13). Ho-mothallic Paecilomyces species are reported by their teleo-morph name, Thermoascus (2, 5, 14, 25, 27, 28). As the nameimplies, these are thermophilic or at least thermotolerantfungi. Their identification in clinical laboratories is based upongrowth characteristics, temperature studies, and the micro-scopic morphology of both the anamorph and teleomorphforms, i.e., conidiogenous cells and conidia in the genus Pae-cilomyces, and ascomata, asci, and ascospores in the genusThermoascus. The case isolate was initially identified in SanAntonio as T. crustaceus based upon its yellow-orange to red-dish orange colonies, the Paecilomyces anamorph displayingcylindrical to rectangular-shaped conidia, growth at 25, 30, 35,and 42°C, and nonostiolate, reddish yellow ascomata produc-ing thick-walled, slightly roughened ascospores as viewed bylight microscopy. Ascospores measured 6.5 to 8 by 4.5 to 5 mm.However, in preparation for submission of this paper, SEMstudies of the ascospores did not match those reported for T.crustaceus in that they were irregularly verrucose (Fig. 1G)rather than finely echinulate. Recently, Chen and Chen (5)reported a new thermophilic species of Thermoascus that failedto grow at 20°C and produced ascospores that were echinulateby light microscopy but irregularly verrucose by SEM. Theirregularly verrucose ascospores in the case isolate matchedthose described by Chen and Chen (5) for T. taitungiacus. Anidentification of T. crustaceus was eliminated due to the asco-spore morphology and lack of growth at 20°C (5). Other Ther-moascus species excluded from consideration were Thermo-ascus aegyptiacus with slightly verrucose ascospores and nogrowth at 20°C (27), Thermoascus aurantiacus that frequentlylacks an anamorphic state, has minutely verrucose ascospores,and fails to grow at 30°C (5, 28), and Thermoascus thermophiluswith nearly smooth ascospores and a Polypaecilium anamorph(2). Features of thermophilic Thermoascus species are dis-played in Table 1. The etymology for the species name T.taitungiacus comes from the region Taitung in Taiwan, wherethe organism was isolated from field soils (5). The recovery ofthis organism from Israel broadens the geographic region forthis new species. T. taitungiacus has not been previously asso-ciated with human disease.
Laboratory contamination is unlikely in the case presented,as T. taitungiacus was isolated in pure growth from four differ-ent dialysate fluids over a period of 8 days. Moreover, ourpatient had clinical and laboratory evidence of CPD-associatedperitonitis and considerable morbidity due to a protracted
symptomatic disease course and the development of a hyper-catabolic state. In addition to Tenckhoff catheter removal, herequired an extended period of systemic antifungal therapyand parenteral alimentation. Paecilomyces and Thermoascusspecies are a rare cause of fungal peritonitis (E. Bibashi, L.Sigler, E. Mitsopoulos, E. Roilides, M. Rinaldi, D. Sutton, D.Tsakiris, and M. Papadimitriou, Abstr. 13th Congr. Int. Soc.Hum. Anim. Mycol., abstr. P142, 1997). The first case wasreported in 1990 by Lye (16). Since then only 14 additionalcases have been published, 13 of which were identified as P.variotii (1, 3, 6, 8, 12, 15–18, 22). Paecilomyces peritonitis isassociated with substantial morbidity. Ten of 14 reported pa-tients had to be removed from CPD and were placed on he-modialysis (1, 6, 8, 12, 16–18); however, no fatalities wereassociated with Paecilomyces peritonitis. This stands in contrastwith the high mortality rate (up to one-third of cases) reportedin CPD-related peritonitis due to other fungi (4). The optimalapproach for the treatment of Paecilomyces peritonitis is dif-ficult to derive from the published data. Removal of the Tenck-hoff catheter was the rule in the majority of the patients (1, 3,6, 8, 12, 16–18); however, the antifungal regimens differedwidely among the patients, even within the same center (17).Of note, one patient did not receive any antifungal therapy(18), while another received fluconazole despite the fact thathis Paecilomyces isolate appeared resistant, in vitro, to the drug(8). All eight tested Paecilomyces isolates from the reportedcases appeared susceptible, in vitro, to itraconazole (1, 3, 12,17; Bibashi et al., Abstr. 13th Congr. Int. Soc. Hum. Anim.Mycol.). Eight of nine tested isolates were susceptible to am-photericin B (1, 8, 12, 17, 18, 22; Bibashi et al., Abstr. 13thCongr. Int. Soc. Hum. Anim. Mycol.), five of five to flucytosine(1, 3, 17), and only two of ten to fluconazole (1, 3, 8, 12, 17, 22;Bibashi et al., Abstr. 13th Congr. Int. Soc. Hum. Anim. My-col.). T. taitungiacus can be added to an enlarging list of op-portunistic filamentous fungi associated with human infectionin general and CPD-associated peritonitis in particular. Fur-ther case studies are required to elucidate the clinical course ofinfection and the optimal treatment strategies.
REFERENCES
1. Alscher, D. M., E. Pfinder-Nohe, D. Rumpf, C. Pauli-Magnus, C. Knabbe, U.Kuhlmann, and T. Mettang. 1998. Moulds in containers with biologicalwastes as a possible source of peritonitis in two patients on peritonealdialysis. Perit. Dial. Int. 18:643–646.
2. Apinis, A. E. 1967. Dactylomyces and Thermoascus. Trans. Brit. Mycol. Soc.50:573–582.
3. Chan, T. H., A. Koehler, and P. K. Li. 1996. Paecilomyces variotii peritonitisin patients on continuous ambulatory peritoneal dialysis. Am. J. Kidney Dis.27:138–142.
4. Chan, T. M., C. Y. Chan, S. W. Cheng, W. K. Lo, C. Y. Lo, and I. K. Cheng.1994. Treatment of fungal peritonitis complicating continuous ambulatoryperitoneal dialysis with oral fluconazole: a series of 21 patients. Nephrol.Dial. Transplant. 9:539–542.
5. Chen, K.-Y., and Z.-C. Chen. 1996. A new species of Thermoascus with aPaecilomyces anamorph and other thermophilic Thermoascus species fromTaiwan. Mycotaxon 60:225–240.
6. Crompton, C. H., J. W. Balfe, R. C. Summerbell, and M. M. Silver. 1991.Peritonitis with Paecilomyces complicating peritoneal dialysis. Pediatr. In-fect. Dis. J. 10:869–871.
7. Eisenberg, E. S., I. Leviton, and R. Soeiro. 1986. Fungal peritonitis in pa-tients receiving peritoneal dialysis: experience with 11 patients and review ofthe literature. Rev. Infect. Dis. 8:309–321.
8. Eisinger, R. P., and M. P. Weinstein. 1991. A bold mold? Paecilomycesvariotii peritonitis during continuous ambulatory peritoneal dialysis. Am. J.Kidney Dis. 18:606–608.
9. Espinel-Ingroff, A., M. Bartlett, R. Bowden, N. X. Chin, C. Cooper, Jr., A.Fothergill, M. R. McGinnis, P. Menezes, S. A. Messer, P. W. Nelson, F. C.Odds, L. Pasarell, J. Peter, M. A. Pfaller, J. H. Rex, M. G. Rinaldi, G. S.
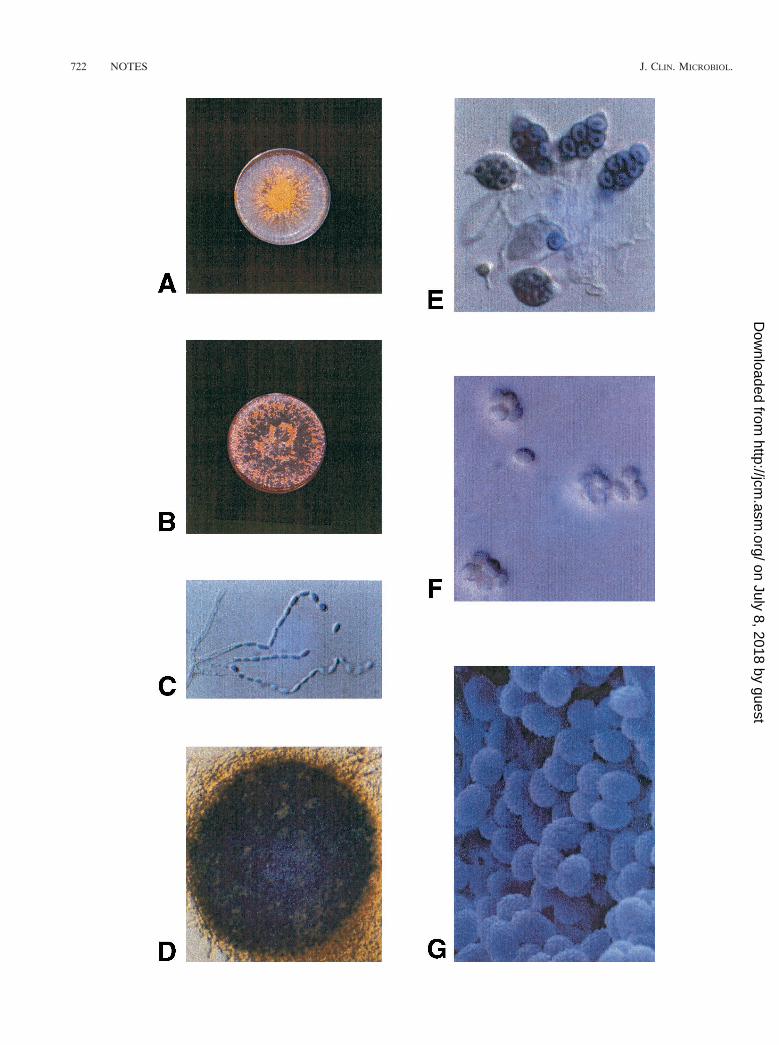
FIG. 1. Macroscopic and microscopic features of T. taitungiacus(anamorph P. taitungiacus). (A) Colonial morphology of T. taitungi-acus after 7 days of incubation at 35°C on PFA. Magnification, 3920.(B) Colonial morphology of T. taitungiacus after 7 days of incubationat 35°C on Czapek Dox and malt extract agar. Magnification, 3920.(C) P. taitungiacus anamorph from slide culture on PFA after 7 days ofincubation at 25°C on PFA. Magnification, 3920. (D) Nonostiolateascoma of T. taitungiacus. Magnification, 3230. (E) Asci containingascospores of T. taitungiacus. Magnification, 3920. (F) Predominatelyechinulate ascospores of T. taitungiacus viewed by light microscopy.Magnification, 3920. (G) Irregularly verrucose ascospores of T. tai-tungiacus viewed by scanning electron microscopy. Magnification,33,000.
VOL. 39, 2001 NOTES 723
on July 8, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

Shankland, T. J. Walsh, and I. Weitzman. 1997. Multicenter evaluation ofproposed standardized procedure for antifungal susceptibility testing of fil-amentous fungi. J. Clin. Microbiol. 35:139–143.
10. Espinel-Ingroff, A., K. Dawson, M. Pfaller, E. Anaissie, B. Breslin, D. Dixon,A. Fothergill, V. Paetznick, J. Peter, M. Rinaldi, and T. J. Walsh. 1995.Comparative and collaborative evaluation of standardization of antifungalsusceptibility testing for filamentous fungi. Antimicrob. Agents Chemother.39:314–319.
11. Gucalp, R., P. Carlisle, P. Gialanella, S. Mitsudo, J. McKitrick, and J.Dutcher. 1996. Paecilomyces sinusitis in an immunocompromised adult pa-tient: case report and review. Clin. Infect. Dis. 23:391–393.
12. Kovac, D., J. Lindic, T. Lejko-Zupanc, A. F. Bren, B. Knap, M. Lesnik, A.Gucek, and D. Ferluga. 1998. Treatment of severe Paecilomyces variotiiperitonitis in a patient on continuous ambulatory peritoneal dialysis. Neph-rol. Dial. Transplant. 13:2943–2946.
13. Kwon-Chung, K. J., and J. E. Bennet (ed.). 1992. Medical mycology. Lea &Febiger, Philadelphia, Pa.
14. Kwon-Chung, K. J., T. Folks, and K. W. Sell. 1984. Unusual isolates ofThermoascus crustaceus from three monocyte cultures of AIDS patients.Mycologia 76:375–379.
15. Liu, K., D. N. Howell, J. R. Perfect, and W. A. Schell. 1998. Morphologiccriteria for the preliminary identification of Fusarium, Paecilomyces, andAcremonium species by histopathology. Am. J. Clin. Pathol. 109:45–54.
16. Lye, W. C. 1990. Paecilomyces peritonitis in a patient on continuous ambu-latory peritoneal dialysis. Nephrol. Dial. Transplant. 5:1053–1054.
17. Marzec, A., L. G. Heron, R. C. Pritchard, R. H. Butcher, H. R. Powell, A. P.Disney, and F. A. Tosolini. 1993. Paecilomyces variotii in peritoneal dialysate.J. Clin. Microbiol. 31:2392–2395.
18. Nankivell, B. J., D. Pacey, and D. L. Gordon. 1991. Peritoneal eosinophiliaassociated with Paecilomyces variotii infection in continuous ambulatory peri-toneal dialysis. Am. J. Kidney Dis. 18:603–605.
19. National Committee for Clinical Laboratory Standards. 1997. Referencemethods for broth dilution antifungal susceptibility testing of yeasts. Ap-proved standard M27-A. National Committee for Clinical Laboratory Stan-dards, Wayne, Pa.
20. Orth, B., R. Frei, P. H. Itin, M. G. Rinald, B. Speck, A. Gratwohl, and A. F.Widmer. 1996. Outbreak of invasive mycoses caused by Paecilomyces lilaci-nus from a contaminated skin lotion. Ann. Intern. Med. 125:799–806.
21. Rinaldi, M. G. 1982. Use of potato flakes agar in clinical mycology. J. Clin.Microbiol. 15:1159–1160.
22. Rinaldi, S., E. Fiscarelli, and G. Rizzoni. 2000. Paecilomyces variotii perito-nitis in an infant on automated peritoneal dialysis. Pediatr. Nephrol. 14:365–366.
23. Rodrigues, M. M., and D. MacLeod. 1975. Exogenous fungal endophthalmi-tis caused by Paecilomyces. Am. J. Ophthalmol. 79:687–690.
24. Saberhagen, C., S. A. Klotz, W. Bartholomew, D. Drews, and A. Dixon. 1997.Infection due to Paecilomyces lilacinus: a challenging clinical identification.Clin. Infect. Dis. 25:1411–1413.
25. Stolk, A. C. 1965. Thermophilic species of Talaromyces Benjamin and Ther-moascus Miehe. Antonie Leeuwenhoek 31:262–276.
26. Tan, T. Q., A. K. Ogden, J. Tillman, G. J. Demmler, and M. G. Rinaldi. 1992.Paecilomyces lilacinus catheter-related fungemia in an immunocompromisedpediatric patient. J. Clin. Microbiol. 30:2479–2483.
27. Ueda, S., and S.-I. Udagawa. 1983. Thermoascus aegyptiacus, a new thermo-philic ascomycete. Trans. Mycol. Soc. Japan 24:135–142.
28. Upadhyay, M. M., M. S. Framelo, S. O. Goetz, and M. A. Melan. 1984. A newvariety of a thermophilic mold, Thermoascus aurantiacus var. levisporus.Mycopathologia 87:71–80.
29. Williamson, P. R., K. J. Kwon-Chung, and J. I. Gallin. 1992. Successfultreatment of Paecilomyces variotii infection in a patient with chronic granu-lomatous disease and a review of Paecilomyces species infections. Clin. In-fect. Dis. 14:1023–1026.
724 NOTES J. CLIN. MICROBIOL.
on July 8, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from