peritoneum , intraperitoneal spaces
TRANSCRIPT
Normal Anatomy
Retroperitoneum & Abdominal Wall
(Perirenal Space, Anterior and Posterior Pararenal Space)Potential Intraperitoneal Spaces

Presented By: Gemora, Katrina
Procianos, Geleen AnneRodriguez, Jisa
CLMMRH POST GRADUATE INTERNS
2015-2016
Learning Objectives
1. Understand Retroperitoneum and Abdl wall anatomy.
2. Normal appearance of the various compartments and recess.
3. To illustrate and describe the different types of Intraperitoneal space and their imagingfeatures on CT.

Background
Bounded anteriorly by the posterior parietal peritoneum andposteriorly by the transversalis fascia, and extends from the diaphragm superiorly to the linea terminalis of the lesser pelvis inferiorly.
RETROPERITONEUM
• Behind the posterior parietal peritoneum• Between the diaphragm and the pelvic brim

RETROPERITONEUMRETROPERITONEUM
RETROPERITONEUM
• Divided into:1. Anterior Pararenal Compartment2. Perirenal Compartment3. Posterior Pararenal Compartment
RETROPERITONEUM
Anterior Pararenal Space
• Between the posterior parietal peritoneum and the anterior renal fascia
• Boundaries:– Anterior – Parietal Peritoneum– Posterior – Anterior Renal Fascia– Lateral – Conal Fascia
Anterior Pararenal Space
• Organs:1. Pancreas2. Duodenal Loop3. Ascending Colon4. Descending Colon
Anterior Pararenal Space

Perirenal Space
• Boundaries:– Anterior: Anterior Renal Fascia– Posterior: Posterior Renal Fascia
Perirenal Space
• Anterior Renal Fascia – one layer of connective tissue
• Posterior Renal Fascia – two layers of connective tissue– Anterior layer of Posterior Renal Fascia is
continuous with the Anterior Renal Fascia– Posterior layer of Posterior Renal Fascia is
continuous with Lateroconal Fascia
Perirenal Space

Perirenal Space
• Bridging septum – between the renal fascia and the renal capsule
– Can cause loculations of fluid processes in the perirenal space
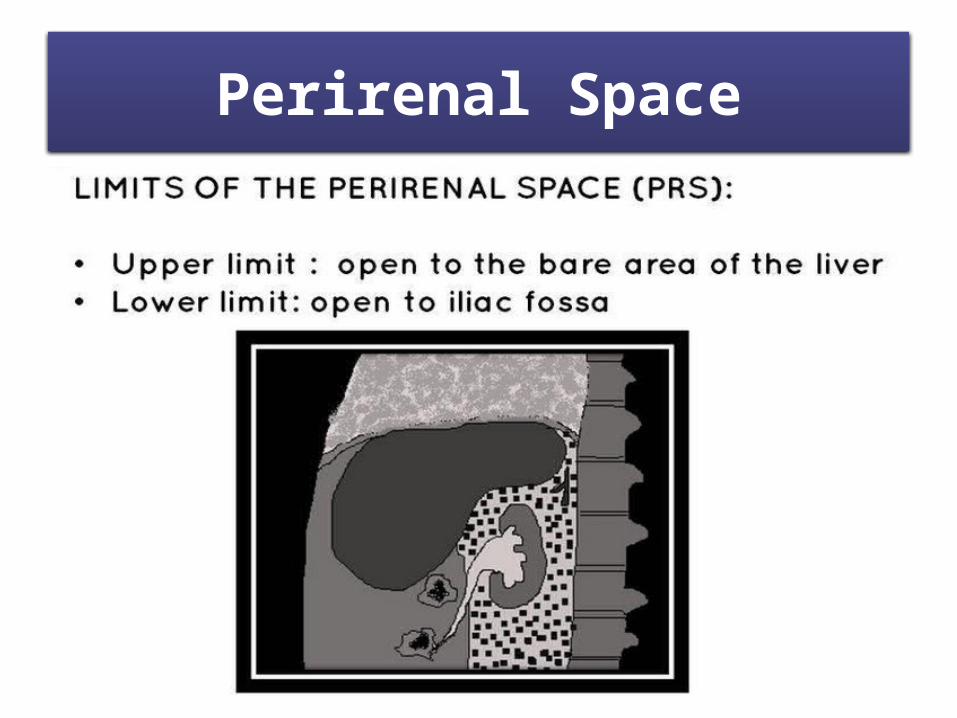
• Right Perirenal Space – open superiorly to the bare area of the liver
Perirenal Space

Perirenal Space
• Organs:1. Kidneys2. Adrenal Glands
Perirenal Space

Perirenal Space
Perirenal Space
Posterior Pararenal Space
• A potential space• Usually filled only with fat• Boundaries:
1. Anterior - Posterior Renal Fascia2. Posterior - Transversalis Fascia
• Limited medially by the lateral edges of the psoas and quadratus lumborum muscles

RETROPERITONEAL ORGANS
1. Pancreas2. Duodenal Loop3. Ascending Colon4. Descending Colon5. Kidneys6. Adrenal Glands

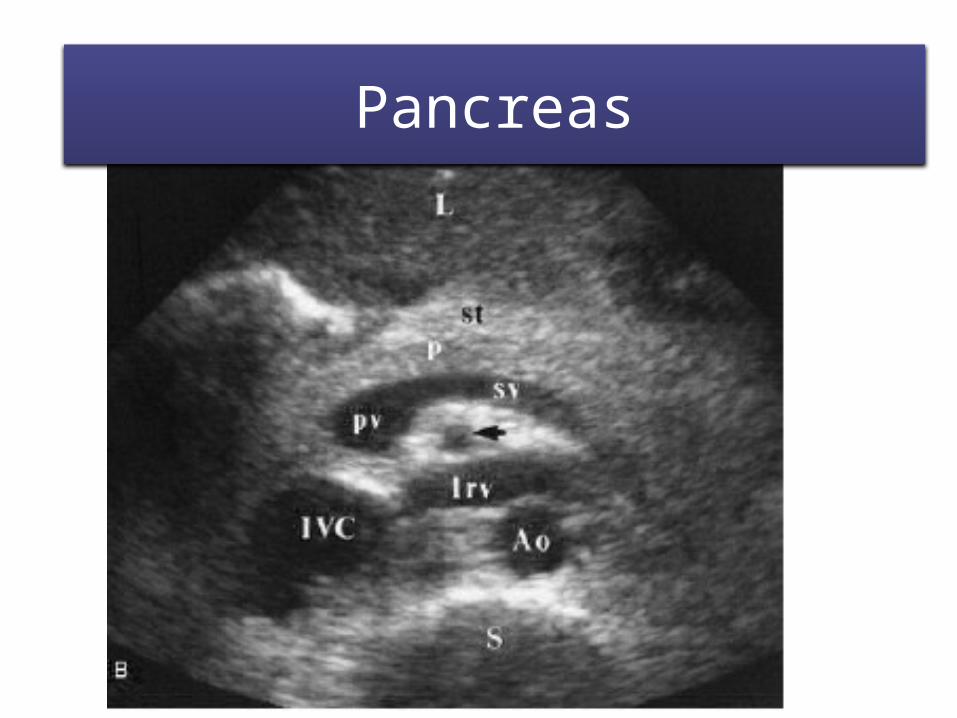
Pancreas
• Elongated, soft, grayish-pink digestive gland• Located inferior to the transpyloric plane• Posterior to the stomach• Transverse mesocolon attached to its anterior
margin• Located in the epigastric and left
hypochondriac regions
Pancreas
• Parts:1. Head – embraced by the curve of the duodenum
– Rests against the IVC posteriorly2. Neck – grooved posteriorly
– Adjacent to pylorus of the stomach3. Body – triangular in cross-section
– Between celiac trunk and SMA3. Tail – end usually contacts the hilum of spleen
Pancreas

Pancreatic Duct
• Main Pancreatic Duct – begins at the tail of the pancreas and runs through the gland
• Accessory Pancreatic Duct – variable; usually connected to the main pancreatic duct
• Ampulla of Vater – pancreatic duct + bile duct
Pancreatic Duct
• ERCP provides visualization of the pancreatic duct
• MRCP – noninvasive method of imaging the pancreatic duct– Secretin injection increases pancreatic secretions
and improve visualization of the pancreatic duct
Pancreatic Duct

Pancreatic DuctPancreatic Duct
Pancreas
• CT, Ultrasound and MRI are primary imaging modalities of the pancreas
• Delicate feathery appearance on CT
PancreasPancreas

PancreasPancreas

Pancreatic Calcifications

Duodenal Loop
• Descending (second) part and Horizontal (third) part of the duodenum are retroperitoneal
• Descending – to the right and parallel to IVC • Horizontal – anterior to IVC, aorta and IMA• High quality Upper GI Series

Duodenal LoopDuodenal Loop
Ascending Colon
• 12 cm to 20 cm in length• Ascends on the right side of the abdominal
cavity • Cecum to right lobe of the liver• Right colic (hepatic) flexure – where the
ascending colon turns to the left• Separated from anterior abdominal wall by
coils of small intestine and greater omentum

Ascending Colon
• Right Paracolic Gutter – trench or groove at the lateral side of the ascending colon
– Depth of this groove – how much gas the ascending colon contains
– Passageway of fluid from the right hepatorenal recess to the rectouterine and/or rectovesical pouch
Ascending Colon

Descending Colon
• 20 cm to 30 cm in length• Descends from the left colic flexure to the left
iliac fossa• Continuous with the sigmoid colon• Passes anterior to the lateral border of the left
kidney• Caliber is smaller than ascending colon

Colon
• CT Colonography – for polyp and cancer detection
• Single Contrast Barium Enema – for intestinal obstruction
• Double Contrast Barium Enema – for detection of small lesions and inflammatory bowel
• CT – demonstrate intramural and extracolonic components

ColonColon

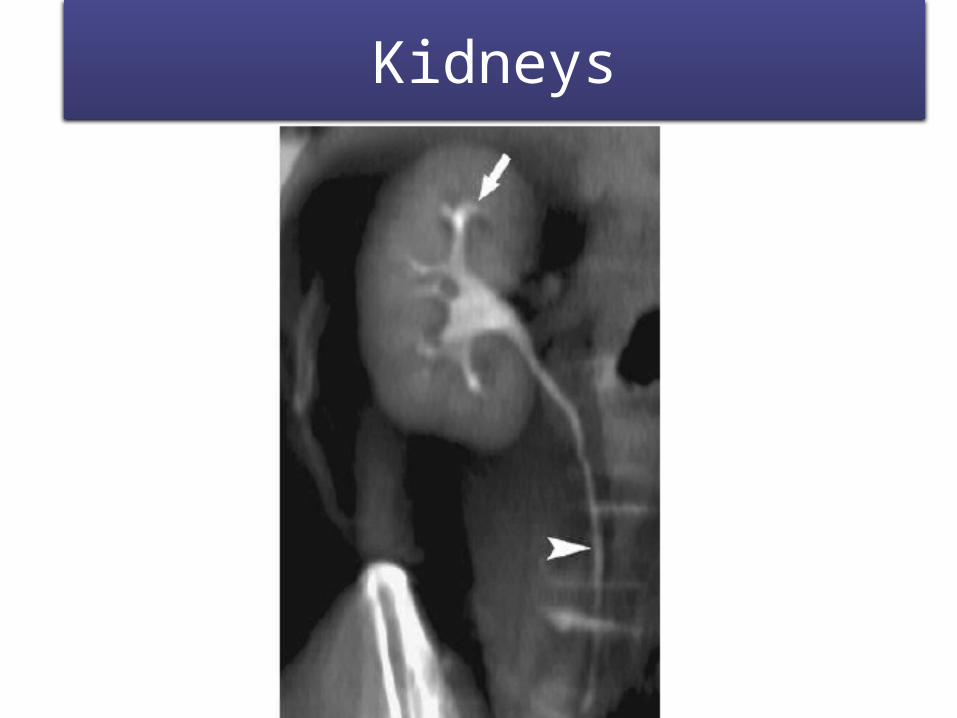
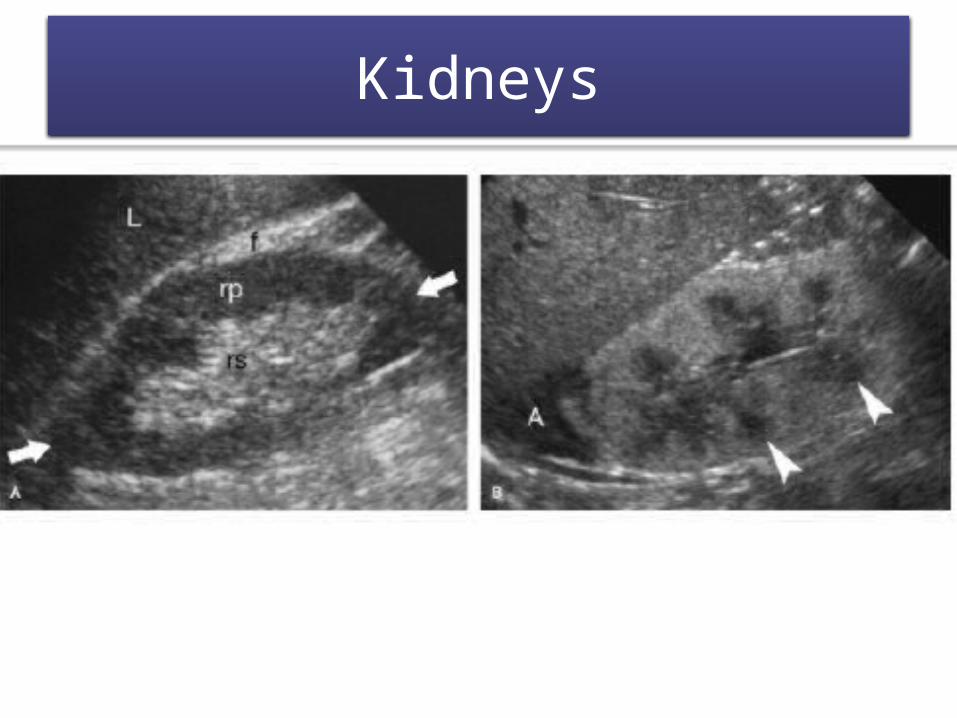
Kidneys
• Lie in the paravertebral gutters at the level of T12 to L3 vertebrae
• Moves about 3cm in vertical direction during movement of diaphragm
• Ureter runs inferiorly from each kidney• Lies in a mass of perirenal fat• Posterior to peritoneum • On the posterior abdominal wall

Kidneys
• Superior – protected by thoracic cage• Superior poles near median plane• Right lower than left• Left slightly longer than right• Lateral – convex• Medial – concave; where renal sinus and renal
pelvis are located
Kidneys

Kidneys
• Renal Hilum – vertical cleft at the concave part of the kidney; lies in transpyloric plane
• Renal Sinus – occupied by renal pelvis, calices, renal vessels and nerves
Kidneys

Kidneys
• Excretory Urography ( IV Pyelography ) • Multidetector CT with IV Contrast (CT-IVP)
Kidneys

KidneysKidneys
KidneysKidneys
KidneysKidneys
Adrenal Glands
• Superior to the kidneys• Enclosed within a fatty capsule and enveloped
by renal fascia• Shape and relations differ from both sides• Consist of cortex and medulla

Adrenal Glands
• CT- usually the imaging modality of choice in adults
• MR – provide high quality images of adrenal lesions
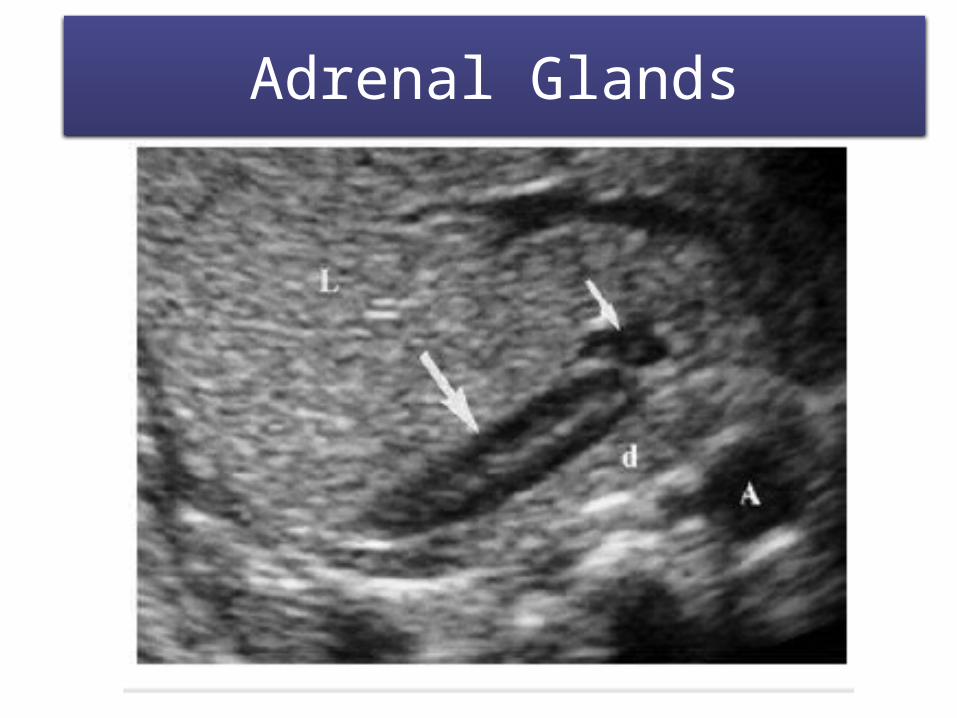
• Ultrasound – excellent for screening the adrenal glands in infants and children
Adrenal Glands
Adrenal GlandAdrenal Glands

Adrenal GlandsAdrenal Glands

Adrenal Calcifications

Anterior Pararenal Space- Extends between the Post. Parietal peritoneum and the Ant. Renal fascia.

Anterior Pararenal

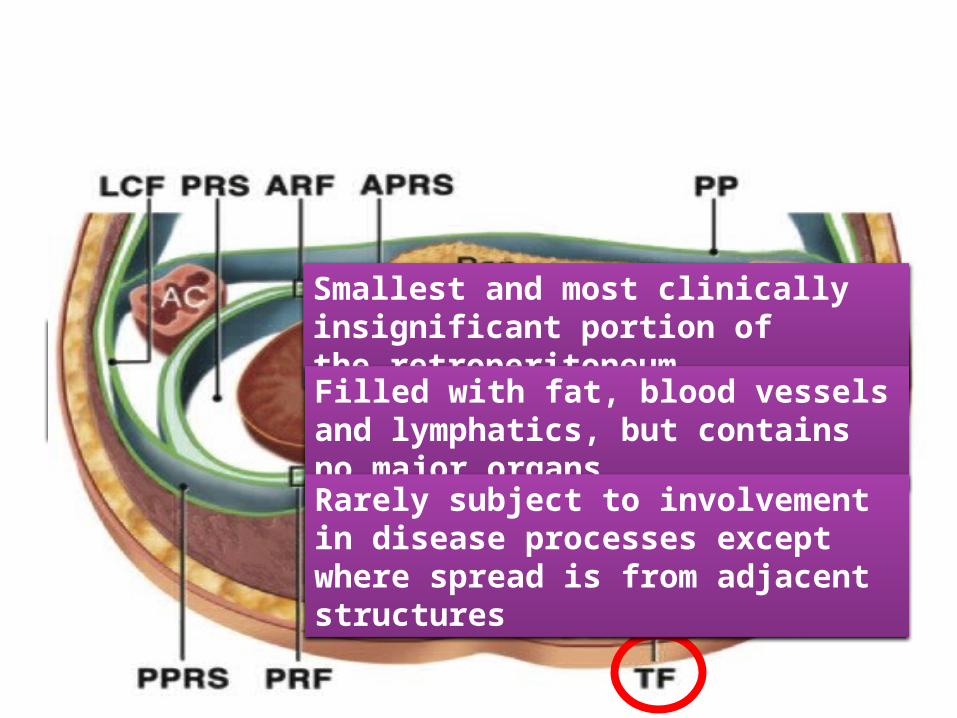
Posterior Pararenal Space
Smallest and most clinically insignificant portion of the retroperitoneum
Filled with fat, blood vessels and lymphatics, but contains no major organs
Rarely subject to involvement in disease processes except where spread is from adjacent structures

Posterior Pararenal Space
Intraperitoneal Spaces
Separate compartments within the peritoneal cavity.
Separated or compartmentalized by various peritoneal ligaments and their attachments.
Significant in the peritoneal diseases, ascites, intraperitoneal collections or peritoneal metastasis.

Intraperitoneal Spaces
1. Supramesocolic Space
2. Inframesocolic Space
3. Pelvic Spaces
Intraperitoneal Spaces
1.Supramesocolic Space
2.Inframesocolic Space
3. Pelvic Spaces
Right Supramesocolic Space
Left Supramesocolic Space

Intraperitoneal Spaces
1. Supramesocolic Space
2. Inframesocolic Space
3. Pelvic Spaces
1. R Inframesocolic Space2. L Inframesocolic Space3. R And L Para-colic Gutters

Intraperitoneal Spaces
1. Supramesocolic Space
2. Inframesocolic Space
3. Pelvic Spaces
1. Para-vesical Spaces2. Rectovesical Pouch3. Rectouterine Pouch (Pouch
Of Douglas): In Females

Intraperitoneal Spaces
Supramesocolic Space Intraperitoneal space above the root of the transverse mesocolon
Arbitrarily divided into R and L spaces and subspaces
These are normally in communication with each other, but may become separated by inflammatory membranes or disease.
Subphrenic space is divided into R and L by the falciform ligament.
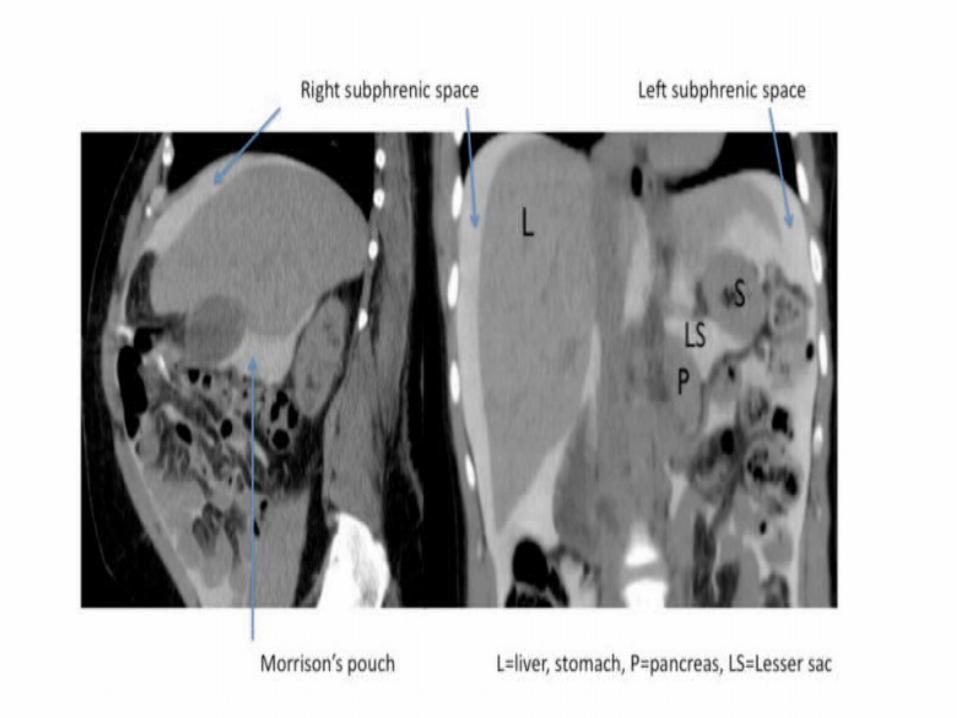
Intraperitoneal SpacesRIGHT SUPRAMESOCOLIC SPACE1. R Subphrenic Space2. Ant. R Subhepatic
Space3. Post. R Subhepatic
Space (Morison Pouch)
LEFT SUPRAMESOCOLIC SPACE1. Ant. L Perihepatic
Space2. Post. L Perihepatic
Space3. Ant. L Subphrenic
Space4. Post. L Subphrenic
(Perisplenic) Space



Intra-peritoneal space below the root of the transverse mesocolon.
The supramesocolic space lies above the transverse mesocolon's root.
Contains the paracolic gutters are peritoneal recesses on the Post. abdl wall Lat. to the Asc and Desc. colon.
Inframesocolic Space
Intraperitoneal Spaces

R paracolic gutter is continuous superiorly with the R subhepatic and subphrenic spaces.
Larger than the L paracolic gutter, which is partially separated from the L subphrenic spaces by the phrenicolic ligament.
Inframesocolic Space
Intraperitoneal Spaces
Both paracolic spaces are in continuity with the pelvic peritoneal spaces.

R inframesocolic space- Smaller than its counterpart. Bounded SUP: Transverse colon To the right: Root of the Small Bowel Mesentery.
Inframesocolic Space
Intraperitoneal Spaces
L inframesocolic space- Larger of the two compartments and is in free communication with the pelvic peritoneal space on the right of the midline. - The sigmoid colon and its associated mesentery form a partial barrier on the left of the midline.



Intraperitoneal Spaces
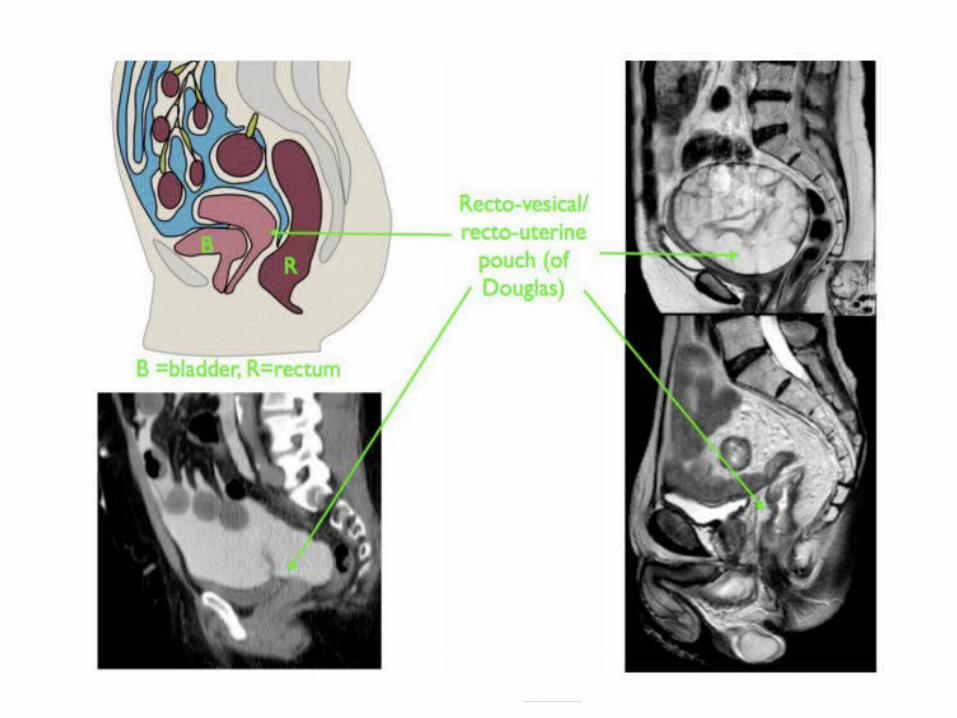
Pelvic Space Inf. reflection of the peritoneum over the fundus of the urinary bladder and the front of the rectum at the junction of its middle and lower thirds
In females, the reflection is also over the Ant. and Post. surface of the uterus and the upper Post. vagina.
Urinary bladder subdivides the pelvis into R and L paravesical spaces

Intraperitoneal Spaces
Pelvic Space Males there is only 1 potential space for fluid collection Post. to the bladder, the rectovesical pouch
In females, the reflection is also over the Ant. and Post. surface of the uterus and the upper Post. vagina.
Females there are 2 potential spaces Post to the bladder, the uterovesical pouch, and Post. to the uterus the deeper rectouterine pouch (Pouch of Douglas).


Thank You.