periprosthetic leak closure - transapical approach pan... · periprosthetic leak closure -...
TRANSCRIPT

Periprosthetic Leak Closure - Transapical Approach
Pan Xin
Shanghai Chest Hospital Affiliated to Shanghai Jiaotong University,Shanghai,China,200030

Disclosures
Nothing to disclose with regard to commercial support!

Background
• PVL is one of the most important complications after surgical valve replacement or transcatheter valve implantation.
• Typically this is associated with dehiscence of sewing ring sutures, often
precipitated by infection, annular calcification or technical factors.
• The majority of these leaks are trace to mild and are asymptomatic; moderate to severe PVL can lead to significant hemodynamic and clinical consequences.

Background
1% to 3% of patients with symptomatic paravalvular leak require intervention:
• Heart failure(larger the size of the leak)
• Hemolytic anemia(multiple leaks)
• Both
• infective endocarditis
• pulmonary hypertension
All of those effect on patient’s quality of life,
cause an increase in mortality
Background
• Medical treatment is largely palliative, Including heart failure therapy, repeated blood transfusions or erythropoietin injections
• Open Surgical reoperation is the gold standard of therapy for PVLs Options so far ,which include resuturing or replacing
- higher morbidity and mortality - re-PVL: because of underlying tissue friability, inflammation, or
calcification

Pre-surgery
Post-surgery
Intraoperative inspection:
LA view 4 to 6 o’clock,suture rupture
Operation mode: resuturing
Pre-surgery

Transcatheter Umbrella Closure of Valvular
and paravalvular leaks.
Houihan et ,al. J Am Coll Cardiol
1992;20:1371–7.

Transcatheter closure involves obstructing the flow
through the PVL by delivering occluders at the site of
leak,preventing or reducing the amount of
regurgitation
Technical success :the correct deployment of a stable
occlusive device through the PVL with a lack of
significant residual regurgitation and prosthetic valve
malfunction or interference
Clinical success: an improvement in ≥1 NYHA-FC
and/or improvement in mechanical haemolysis
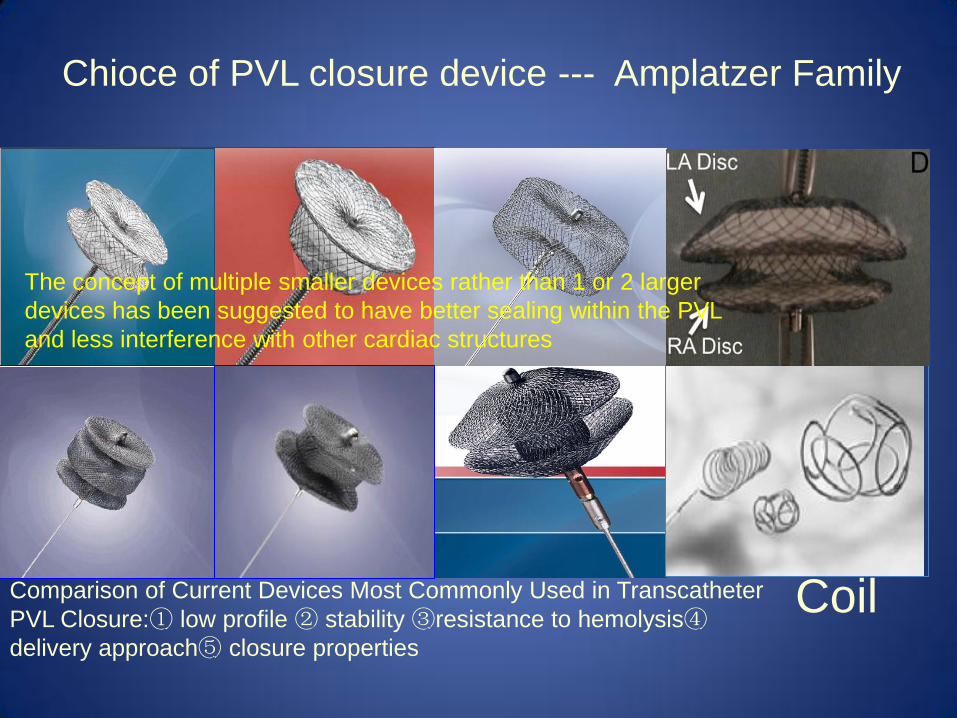
Comparison of Current Devices Most Commonly Used in Transcatheter
PVL Closure:① low profile ② stability ③resistance to hemolysis④delivery approach⑤ closure properties
Coil
Chioce of PVL closure device --- Amplatzer Family
The concept of multiple smaller devices rather than 1 or 2 larger
devices has been suggested to have better sealing within the PVL
and less interference with other cardiac structures

Techniques for PVL Closure
• Femoral Approach--aortic PVL and mitral PVL
• TS(Transseptal) Approach-- mitral PVL

Techniques for PVL Closure
Transapical(TA) Approach

The advantages of Transapical Approach
• Both valves are easily accessible
• Mechanical heart valve does not preclude the route
• Short and direct route to access both the mitral and aortic valve
• Allows a direct control and manipulation of the guidewire and cath
• Simultaneous occluder device implantation is easily performed
• Coaxial alignment of the catheter and the lesion are relatively easily accomplished
• Significant decrease in the procedural and fluoroscopy times for closure of mitral PVLs compared with conventional procedures

Contraindications to the TA access
• In patients with a hypocoagulable state, or any other bleeding
diathesis
• Undisturbed native pericardium
• LV thrombus, a calcified LV apex, or an unstable prosthesis due to significant dehiscence.

Factors that may favor the TA approach for mitral valve
• The presence of double mechanical valves
• Posterior and medial septal mitral PVLs(1-6 o’clock position)
• Tortuousity of the tract of PVL, which may surrounded by extensive annular calcification
• Multiple leaks or crescentic /irregular /large leak,which need multiple devices to seal the leakage simultaneously
• Peripheral atherosclerotic disease
• Transseptal route complicated(depending on operator and institutional experience and comfort)
• TS or femoral approach is either inadvisable or has been
previously unsuccessful

Case A man aged 40 years with previous aortic and mitral mechanical valve replacements
2 years before, had worsening symptoms of heart failure, despite maximal medical
therapy. From echo, moderate to severe mitral PVL was detected,which located at
medial septal around 1~4 o ′ clock, EuroSCORE II was13.4%

Technical Approach • Preprocedural Planning and Guidance
Such evaluation requires multimodality imaging with 2DTEE,3DTEE,CTA.
• 2DTTE- convenience for screening,and long-term follow-up
• 2DTEE-an approximate assessment of the morphology and extent of the leak
• 3DTEE-provides a precise picture of the location, size, extent, shape, and morphology of the defect, as well as the distance between the PVL and the valve struts and leaflets to avoid impingement of the device to the adjacent structures.

Technical Approach • For TA access, CTA is necessary to provide guidance of PVL closure and
avoid complications
CTA helps to label skin entry, LV entry, and angulation to PVL
location(s) such that they are in direct line with the target; combined
with coronary angiography to allow the route and site of entry to be
away from coronary arteries, lung parenchyma,papillary muscles

Technical Approach
Open Surgical TA • Hybrid approach with both interventional and surgical teams in the hybrid
operating room
• Minithoracotomy ; direct visualization;enable the use of multiple sheaths for simultaneous device implantation
• Surgical exposure helps to visualize the blood vessels and lung tissue,aids in avoiding or minimizing bleeding complications
• Fairly traumatic procedure
Direct Completely Percutaneous TA • Perform in the cath lab
• Minimize sheath(5F) size at the LV apex, externalize the apical wire and deliver the devices via the femoral or TS approach
• Less invasive
• Potential risk of bleeding

Major Complications for PVL closure - results from our experience
TA approach(n=10):
• Minithoracotomy in 8;Transcutaneous in 2
• Device selection: mVSD,PDA occluder, AVPⅡ
• Procedure Success 9(90%),one occured residual moderate to severe PVL requiring surgery
• No death, No device emboliaztion,No valve impingement.Major bleeding with Hemothorax(n=3),requiring thoracocentesis(n=2),rethoracotomy(n=1).Device-related hemolysis(n=2)
N=67

Current major Publications on Transapical Transcatheter PVL Closure
First
Author Year
Patients Approach Used
Occluder
Device
Procedure
Success
Early
Safety
Reoperatio
n Summary
(Mitral,
Aortic)
(Minithora
cotomy)
(Transcuta
neous)
Ruiz et al 2011 43 (33,10) 0 24
VSD, ASD,
PDA,
AVPⅡ
37 (86%) ? 1 (2%)
Sorajja et
al 2011 115 (90, 25) 0 13
VSD, ASD,
PDA,
AVPⅡ
11 (85%) 9 (69%) 0 (0)
Hematothorax (n=4)
requiring
thoracocentesis (n=2);
empyema (n=1)
Taramasso
et al 2014 139(100,39) 17 0
AVPⅢ,
AVPⅡ 16(94%) 14(82%) 1(6%)
Device embolization
requiring emergent
open heart
surgery(n=1)
Nijenhuis
et al 2014 37 (30, 7) 37 0
VSD, ASD,
AVP,
AVPⅢ
32 (86%) 30 (81%) 6 (16%)
Major bleeding (n=4);
prosthetic interference
requiring reoperation
(n=1); recurrent PVL
requiring reoperation
(n=1). Clinical efficacy
is 49% (n=18)

Conventional surgery and transcatheter closure via surgical transapical approach for paravalvular
leak repair in high-risk patients
Conclusions: A transcatheter closure via a surgical TAp approach appears to be a
safe and effective therapeutic option in selected high risk patients with PVL and is
associated with a lower hospital mortality than surgical treatment
European Heart Journal – Cardiovascular Imaging (2014) 15,
1161–1167

What can we learn from the recent literature about transcatheter closure of PVLs by systematic review?
Procedural Access Technical Success
Clinical Success
30-days safety
1-year cardiovascular mortality
Moderate or Severe residual regurgitation
Average procedural time
Transfemoral Approach & Transseptal Approach
82% 48% 91% 15% 14% 139± 47.0min
Tansapical Approach
88% 49% 84% 17% 7% 89± 31min
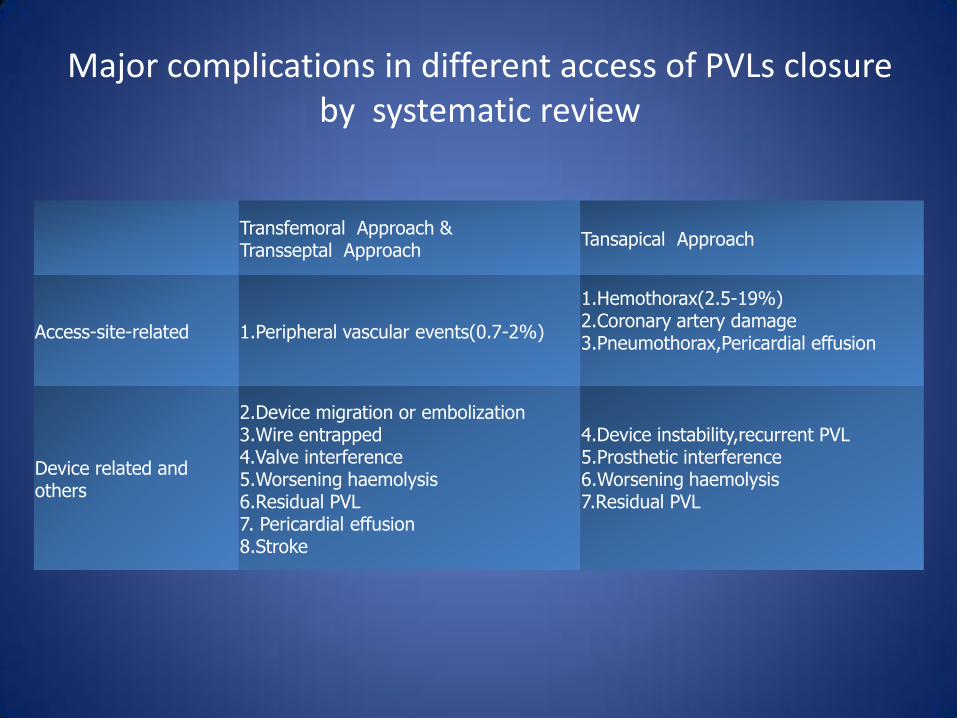
Major complications in different access of PVLs closure by systematic review
Transfemoral Approach & Transseptal Approach
Tansapical Approach
Access-site-related 1.Peripheral vascular events(0.7-2%)
1.Hemothorax(2.5-19%) 2.Coronary artery damage 3.Pneumothorax,Pericardial effusion
Device related and others
2.Device migration or embolization 3.Wire entrapped 4.Valve interference 5.Worsening haemolysis 6.Residual PVL 7. Pericardial effusion 8.Stroke
4.Device instability,recurrent PVL 5.Prosthetic interference 6.Worsening haemolysis 7.Residual PVL

Proper closure of TA access is Vital!
• Apical access site related hemothorax was the most frequent serious complication occurring in the procedure or post-procedure of PVL closure
• Perform either surgically by direct securing of the purse-string sutures or percutaneously by placing closure device
• Considered to be safe, preferred method is open surgical TA compared with direct percutanous TA

Summary
• Transapical approach might be a good or rather attractive alternative for PVL closure, especially for postero-medially located or anatomically hard to access calcified tracted mitral PVLs
• Because of the direct and short nature of the approach, the TA access has been shown to have a relatively high technical success, furthermore, to decrease fluoroscopy and procedure times in the selected patients
• Although there are several complications that potentially be associated with this route, there are have been advancements in multi-modality imaging and the technique of closure of TA access, which may guide the procedure and minimize these complications

If structural interventionalists master the technique of percutaneous
apical access and closure, this will open up a new port into the heart
and facilitate the development of new approaches and procedures.
--From Dr Charanjit S.Rihal

Thank you for your attending!