peripheral neuropathy - international waldenstrom’s ... · peripheral neuropathy affects at least...
TRANSCRIPT
PERIPHERALNEUROPATHY
IWMF ED FORUM
PHILADELPHIA
JUNE 8, 2019


EPIDEMIOLOGY
• Peripheral neuropathy affects 3-4% of the general population increasing to 9% with advancing age
• Peripheral Neuropathy affects at least 30 million people in the United States
• Peripheral Neuropathy is reported in 60-70% of patients with Diabetes
• Monoclonal neuropathies (IgA, IgG, IgM) are present in 3% of the general population over 50 years old and increases to 9% by age 90
• 25% of IgM MGUS patients have neuropathy as their presenting complaint
PERIPHERAL NEUROPATHY ETIOLOGIES• Diabetes• Tumors pressing on
nerves• Infections in nerves• Shingles• Spinal cord injuries• Poor circulation• Hypothyroidism• Surgery or radiation• Primary Amyloidosis• Heavy metal
poisoning
• Chemotherapy• Physical injury• Alcohol abuse• Low B-12• Some autoimmune
diseases• HIV• Demyelinating
antibodies (IgM)• Sarcoid• Cancer• Cryoglobulinemia, cold
agglutinins
COMMON CANCERS CAUSINGPERIPHERAL NEUROPATHY
• Breast cancer
• Lung cancer
• Lymphoma
• Ovarian/Testicular
• Multiple Myeloma
• Waldenstrom macroglobulinemia
• Bone marrow transplantation for cancer

DRUG RELATED NEUROPATHY
• Chemotherapy: cisplaten, carboplatin, cytosine, tacrolimus
• Taxanes: Taxol, Taxotere, Jevtana
• IMiDs: Thalomid, Revlimid, Pomalyst, Otezia
• Proteosome inhibitors: Velcade, Kyprolis, Ixazomib
• Alkylating Agents: Cytoxan, Bendamustine
• Interferon
• Amiodarone, metronidazole, HIV meds, Antabuse, Cipro, Levaquin
• Alcohol abuse
NEUROLOGY EVALUATIONS
• Full physical examination of the peripheral and central nervous system
• Nerve conduction study (NCS)
• Electromyography (EMG)
• MRI scan
• CT scan
• Sural nerve biopsy
• Skin biopsy
PERIPHERAL NEUROPATHY TESTS
• Blood tests: Vitamin B12, blood sugar, serum protein
• Electrophoresis (SPEP), IFE, folic acid, vitamin E, vitamin B6 excess
• Inflammatory disease: ANA, ESR, CRP
• Metabolic: Kidney and liver function, thyroid
• Heavy metal screen – lead, arsenic, mercury
• Anti-MAG, SGPG, Sulfatide, Gm1, GQ1b and other demyelinating antibodies
• Paraneoplastic markers
• Amyloidosis, cryoglobulinemia
• Infectious disease: AIDS, Lyme, Herpes Zoster, Hepatitis B&C, Sarcoidosis
• Spinal fluid examination


WALDENSTROM PN FACTS
• Peripheral Neuropathy is reported in 30% of IgM MGUS patients, 20-50% with Waldenstrom
• Peripheral Neuropathy is reported in 25% among WM patients at diagnosis
• Most Waldenstromer’s with neuropathy have relatively low IgM levels (MGUS)
• Waldenstrom neuropathy is normally symmetrical and starts in the toes
• 50% of IgM neuropathy patients have an anti-Mag IgM antibody (myelin associated glycoprotein)
• WM neuropathy most likely associated with IgM Kappa
• Men > women, older > younger
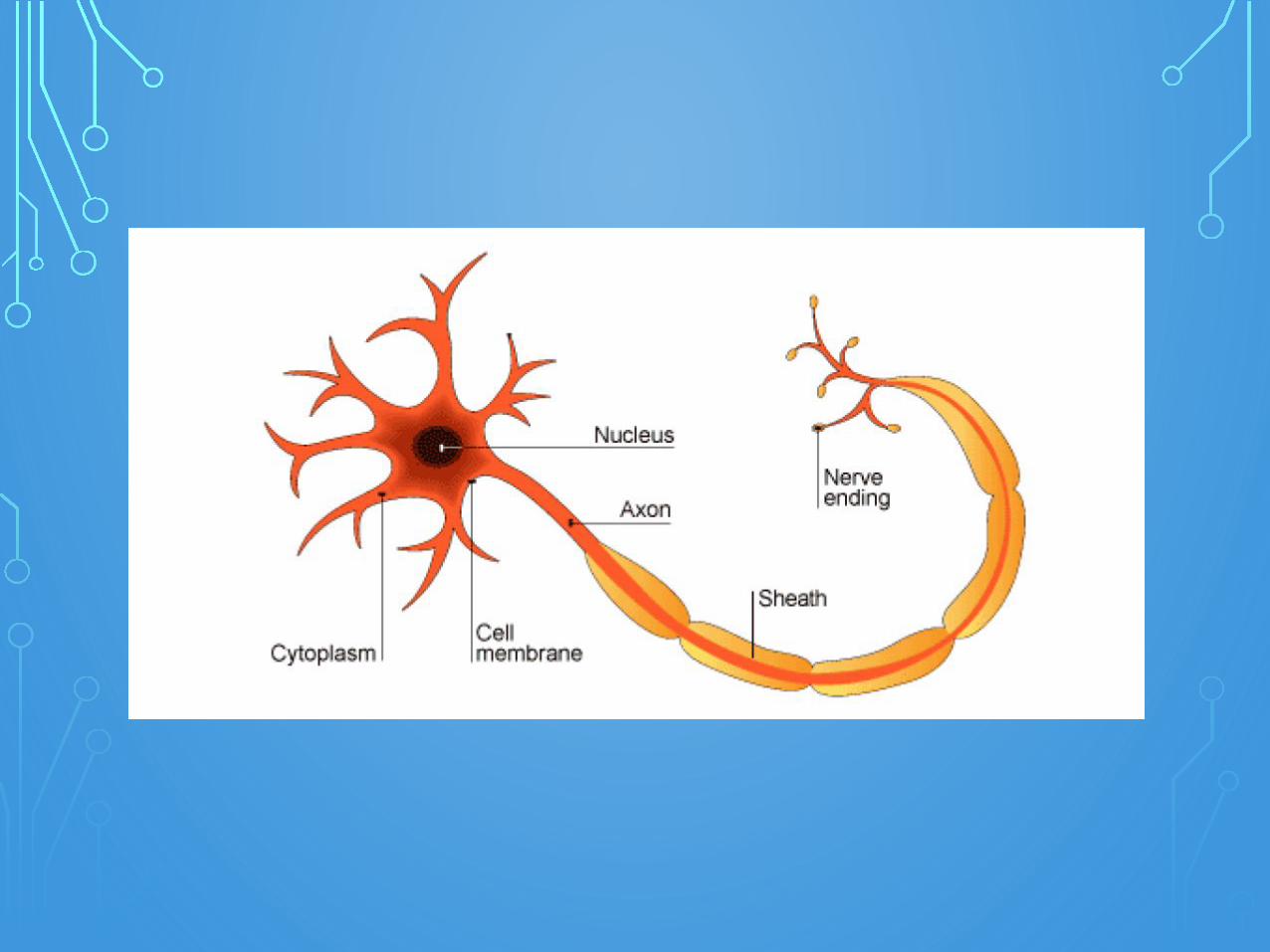
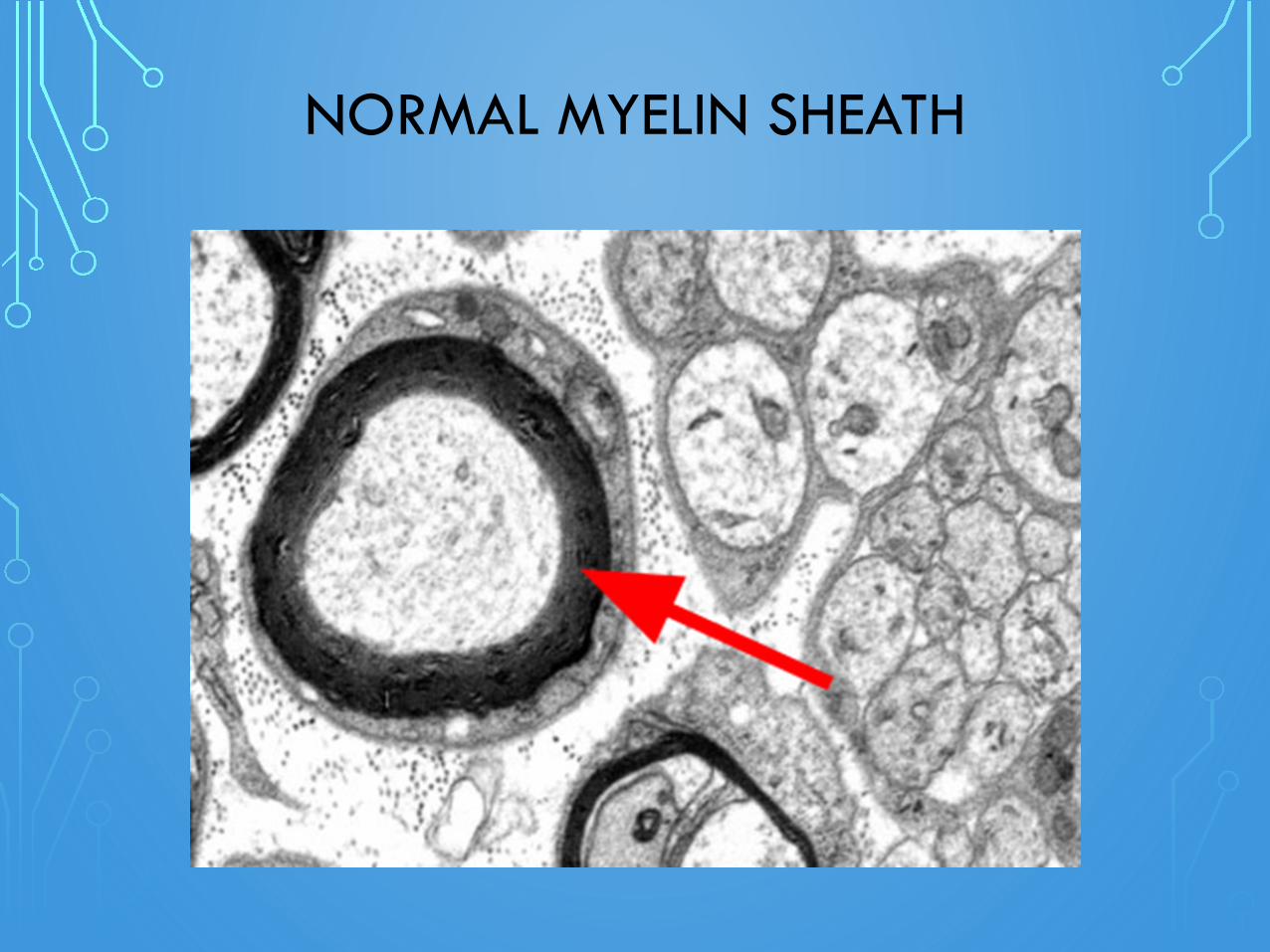
NORMAL MYELIN SHEATH
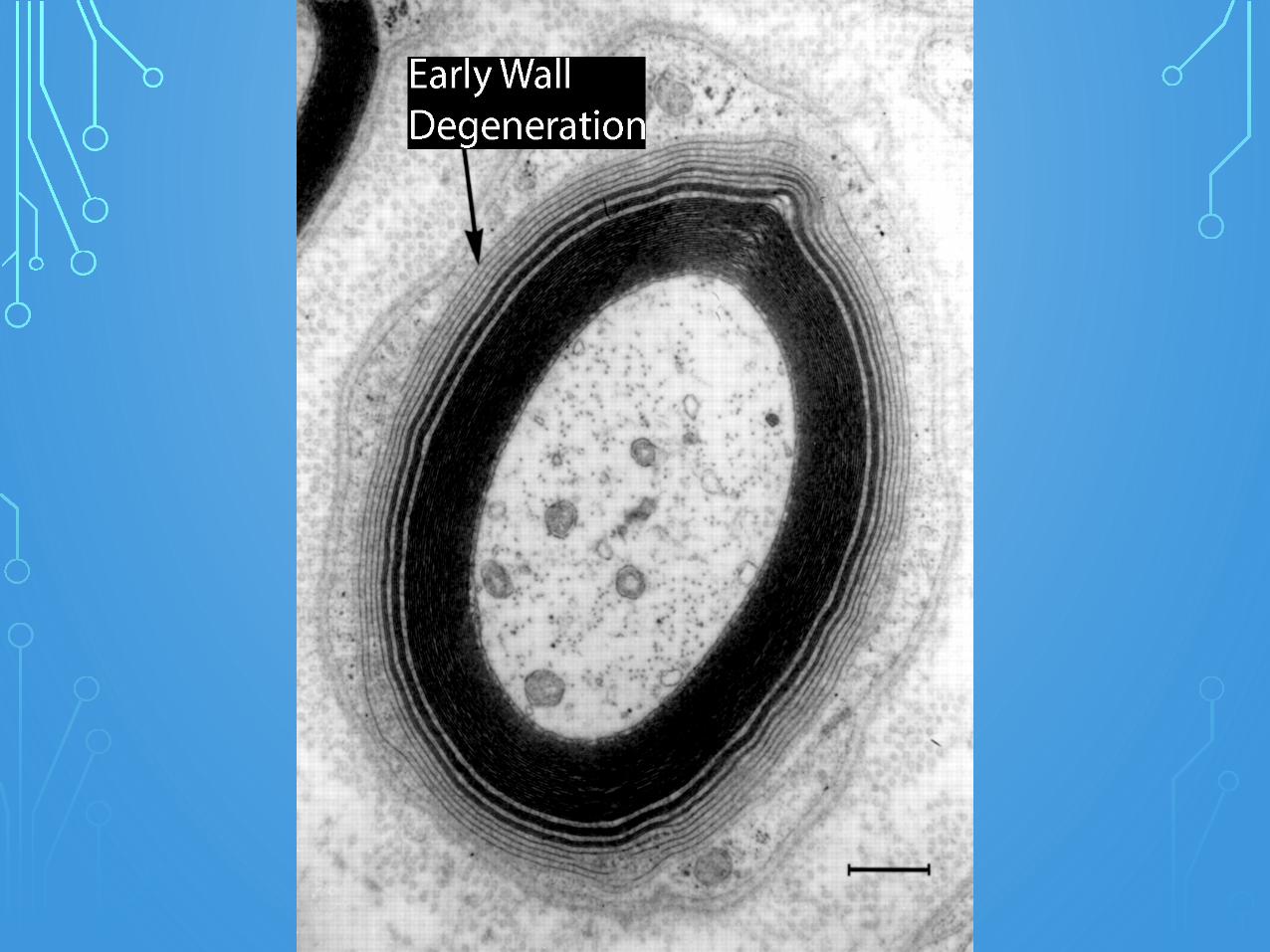
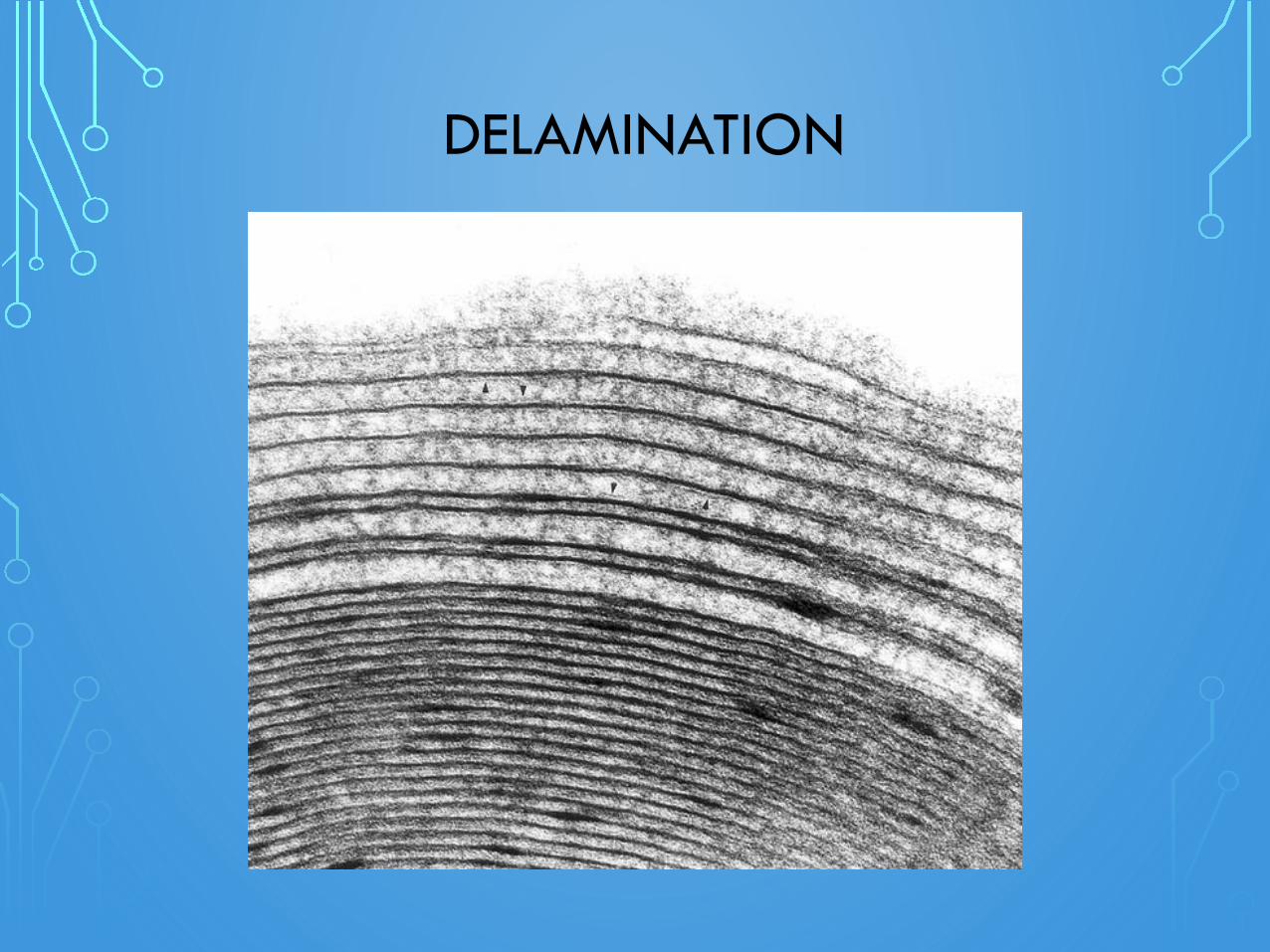
DELAMINATION
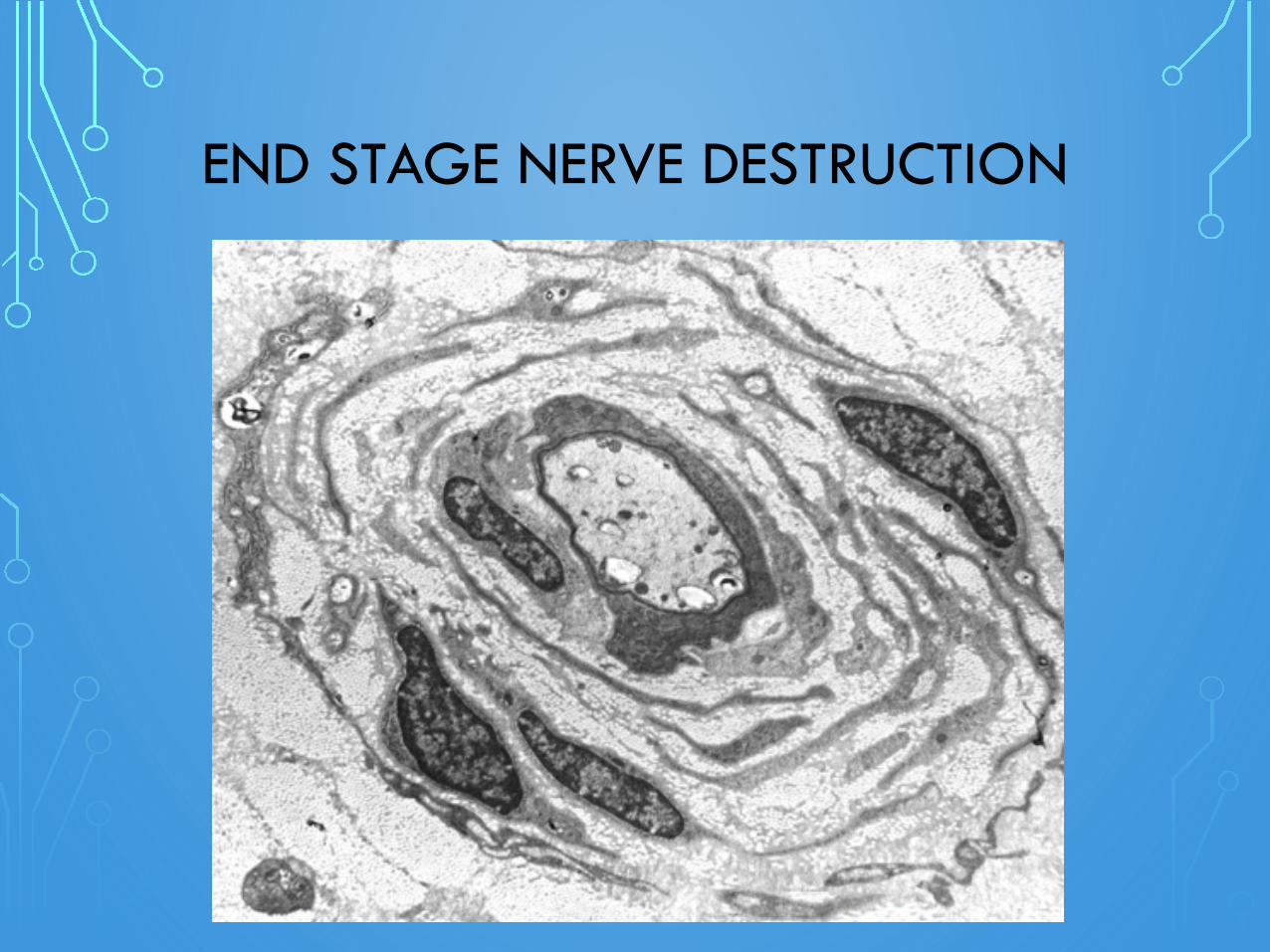
END STAGE NERVE DESTRUCTION



WALDENSTROMNEUROPATHY SYMPTOMS
• Paresthesias: numbness, burning, dysesthesia (painful sensations), pins and needles, sensitivity to touch or temperature, or tingling sensations
• Motor damage – muscle weakness, cramps, spasms, twitching, muscle shrinking
• Loss of reflexes
• Progression of symmetrical symptoms up the legs, then arms
• Feeling like a sock is rolled up under your foot or a feeling you are wearing an invisible glove or sock
• Loss of balance, particularly in the dark
• Dizziness, especially when getting up from a bed or a chair
• Fatigue
TYPICAL WALDENSTROM IGM NEUROPATHY
• Sensory neuropathy that is symmetrical
• It begins in the longest nerves, i.e. toes then the hands
• Most WMer’s with neuropathy have relatively low IgM levels (MGUS)
• WM neuropathy most likely associated with IgM Kappa
• 50% of WM IgM neuropathy patients have an anti-Mag IgM antibody
• Early intervention may prevent debilitating neuropathy
• Nerve re-growth may take up to two years to resolve neuropathy after treatment
• Neuropathy is permanent after 2 years if not treated
• Cerebral spinal fluid shows an elevated protein level in 80% of demyelinating PN
NEUROPATHY MEDICATIONS
• Non-narcotic pain relievers (Tylenol, Motrin, Mobic)
• COX-2 Inhibitors - Celebrex
• Narcotics for pain
• Tramadol - Ultram
• Tricyclic antidepressants – nortryptyline, elavil, amitriptyline, Cymbalta
• Topical medications, lidocaine patches
• Alpha 2 adrenergic agonists - clonodine
• Anti-seizure medication to calm nerves (Neurontin/Gabapentin, Lyrica/pregabalin)

WM PERIPHERAL NEUROPATHY TREATMENTS
• Steroids mainly for inflammatory and autoimmune neuropathy (shingles, CIDP, sarcoid)
• IVIG 15-20% effective, only short time results
• Nerve block
• TENS unit
• Plasma exchange (Plasmapheresis)
• Rituximab (30-50% show improvement)
• Standard WM drug therapy often with Rituxan, no drugs that cause neuropathy
• Exercise
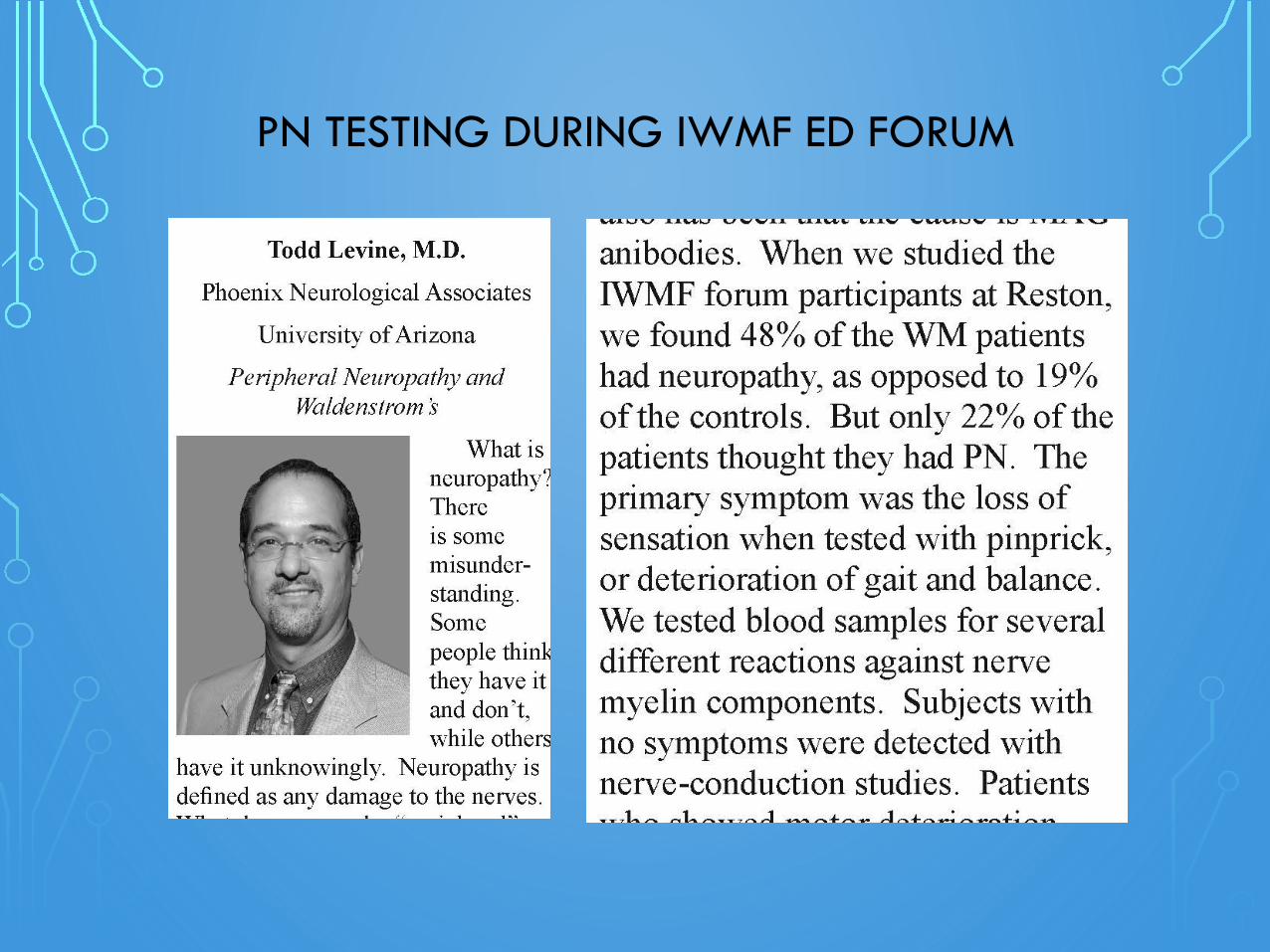
PN TESTING DURING IWMF ED FORUM
PERIPHERAL NEUROPATHY WM MANTRAS
• The presence of neuropathy alone is not a justification for treatment, but steady progression with accumulating disability should prompt action
• Treatment goal should be to lower the IgM as low as possible, especially with anti-MAG presence. Rituxan may not be enough. WM standard treatment protocols should be used.
• Stability rather than improvement is the likely outcome of treatment in someone with chronic neuropathy (>2 years)
PERIPHERAL NEUROPATHY WM MANTRAS
• Quality of life is paramount
• Drugs that induce neuropathy should not be used
• Supportive – orthotics, balance training, occupational and recreational rehab
• Medications and exercise to maintain function and quality of life
THE END