pediatrics study guide.pdf
TRANSCRIPT

Peds Green = Very Important Bold = Important
The Hospitalized Child
The Healthy Family The capacity for clear boundaries (able to establish rules and guidelines) The ability to operate mainly in the present (and not in the past, because they
won’t be able to deal with today) A respect for individual choice and autonomy (respectful attitude and if they
don’t, they that environment can show/lead to abuse) Skills in negotiating The ability to share positive feelings (children need positive environment)
[Entire] Family Reactions to Hospitalization Parent’s Reactions
o Disbelief (OMG)o Anger /& guilt (Why me? Why weren’t you watching them?!)o Fear, anxiety, frustration (outcome is unknown, get angry in ED)
Sibling Reactionso Loneliness (with brother/sister), fears (will this happen to me?), and worry o Anger, resentment, jealous, guilt (this is because the parents and
focus/taking care of the hospitalized child)
Factors that Influence Developmental cognitive level (level of understanding of child) (a 10 year old
have different coping skills than a 2 year old) Previous experience (has an effect on a child’s response to hospitalization
anxiety/fear) Culture (take their culture into consideration!!) Spirituality (promote and enhance it! This encourages and quickens healing) Age appropriate intervention/language (eg. If a 10 year old has a cognitive level
of a 5 yo, then treat them like a 5 year old)
Concept of Illness Preoperational (2-7 yo) Piaget
o Perceives external, unrelated, concrete phenomenon as cause of illness (can’t see casue and effect)
o Perceives cause of illness as proximity between two events occurs by “magic”
Concrete Operational (7-10+ years)*Sees cause as a person, object, or action external as “bad”*Illness has external cause that located inside
Formal Operational (13+ years)

*Sees cause as malfunction or nonfunctioning organ or process (can understand dz process)*Can explain illness in sequence of events*Realizes that psychologic actions and attitudes affect health and illness (feel better to get better)
The Hospitalized ChildSeparation Anxiety
*Major stress from middle infancy thru preschool *Stages
1. Protest2. Despair 3. Detachment
(True separation happens from 2 to 3 yo)
ProtestLater Infancy:
*Cries, screams, searches for parent with eyes (will look at them thru crib), clings to parent, avoids and rejects contact with strangers (7 to 9 months, stranger danger)
Toddler:*Also cries and screams-“NO!,” verbally attacks strangers, physically attacks strangers, attempts to escape to find parent, attempts to physically force parent to stay (cling)
*Behaviors last hours to days (may cry themselves to sleep)*May be continuous ceasing with exhaustion
Despair*Inactive*Withdraws from others*Depressed, sad*Uninterested in environment*Uncommunicative (turn back on you, won’t talk)*Regresses to earlier behavior (thumb sucking, takes bottles, wet bed)*Physical condition may deteriorate (get sicker)*Won’t play
Detachment*Shows increased interest in surroundings (watch tv)*Interacts with strangers (RNs and other parents)*Forms new, superficial relationships*Appears happy*Occurs after prolonged separation(Child will love RN and ignore parents to get back at them)
Loss of Control*Lack of control increases the perception of threat (big threat)*Can affect child’s coping skills*Additional stimuli (sight, sounds, smell) may be overwhelming

*Major areas: physical restriction, (to only room, IV pole), altered routines (these are screwed up; messes with child’s eating, napping, sleeping time, etc) or rituals, dependency (on people-lose dependency and don’t like it!)
InterventionsInfant
*Minimize use of restraints, hep lock IV, use crib with canopy (or bed with plastic verses metal bars, visually appears less constrictive), alter environment with infant seat, stroller, etc (to provide stimulation), provide toys (to decrease isolation and sense of loss of control)
Toddler *Promote home rituals*Promote dietary practices (room service – choose diet and eat at whatever time they want) *Give choices when possible (toys, games) [RN may ask – ‘do you want your meds?’, NO, instead, ask ‘Do you want your meds with juice or water?’]*Take to playroom*Provide opportunity for medical play (stuff animal to show med intervention to reduce anxiety)*Educate parents about regression (if child is potty trained, they may regress to bed wetting and be sure to tell parent that is “normal” and it is ok and will go away)
Pre-Schooler*Encourage autonomy*Take to playroom*Urge to participate in therapeutic play (explain med txmt thru play)*BE TRUTHFUL!!
School Age *Provide opportunities to discuss medical dx*Encourage child to discuss feelings and understanding of condition (give feedback have them explain stuff back) * Allow child to ‘help’ with tasks* Promote choices in care*Reward system
Adolescent*Develop plan of care with adolescent input*Respect need for independence, let them wear normal clothing*Offer choices in routines *Allow for privacy (start at school age (9 years old body image concerns kick in) and privacy necessity)*Be open about medical condition (schedule time in privacy)*Check ID bands**Check IV rate on teen’s pump

*Be sure to sign out of bedside computer, they will chart if given chance
Nursing Diagnosis-Anxiety/fear R/T separation from routine -Anxiety/fear R/T distressing procedures-Pain **Huge issue fear/loss of control-Risk for poisoning or injury from medications R/T sensitivity, dose, etc-Diversional activity deficit-Powerlessness-Risk for injury or trauma R/T environment, equipment, therapies (**Safety HUGE factor, always double check dose, safe dosage, right flush, right dose, have extra line and extra tape on PICC, etc)
Standard of Care*Issues R/T care of minors*Consent for procedures
-parent or legal guardian, mature minor doctrine, emancipated minor, custodial parent, judicial system, no parental consent needed
L-Add Piaget and Erikson!!!
Peds NeuroDrowning-2nd cause of accidental death in children, #1 cause of death in Az-Major pulmonary changes r/t length of submersion and degree of immersion-Cerebral recovery depends on initial resuscitation (emergency response)-Problems associated are: hypoxia, aspiration, hypothermia
Drowning and Near Drowning-Volume of water may be large (pool) or small (bucket of water) -Laryngospasm may occur and hypoxia may follow-When first submerged, initial voluntary apnea occurs -In less than 5 yo, diving reflex may be stimulated
Diving Reflex-Within seconds of face touching cold water (reflex activated in COLD water)-Trigeminal nerve sends sensory afferent impulses to CNS medullary respiratory center-This causes bradycardia, shunting of blood from cutaneous and splachnic (visceral) vascular beds to cerebral and coronary circulations -These reflexes are independent of peripheral chemoreceptors and baroreceptors (CNS elicited)-Augmented by progressively colder water temps and startle response -Within seconds of the first submerged breaths, secondary apnea occurs-Respiratory arrest occurs-Dysrhythmias occur d/t hypoxia

-Eventually cardiac arrest and brain death -Once aspiration of fluid takes place, metabolic acidosis and systemic arterial HTN persist
Aspirate (What they drown in)-Fresh water (bacteria)-Salt water (Na+ content)-Foreign matter (need to have sample taken)-Other material eg chemicals, bacteria-Content of water must be analyzed
Survival (the younger and the colder the water-better chance of survival)-Tolerance depends on age, previous health, water temperature, and promptness and effectiveness of the rescue-Young: <3 min and up to 10 min in water 10-15 degrees C will probably survive-Activation of diving reflex may be most significant factor in survival -Older: cold water may inhibit effective swimming and induce vagally mediated cardiac dysrhythmias and coma with body temp <34 degrees C
Salt Water *hypertonic solution [hyper-party]*-Hypertonic fluid pulls water out of circulation into lungs (party in the lungs!!)-Results in fluid-filled but perfused alveoli-Pulmonary surfactant is washed out (dilutes it)-Hypovolemia can occur with greater amounts of inhalation -Blood volume can decrease to as little as 65% of normal volume
Fresh Water-Can cause increase of blood volume (hypervolemia-party in the body!!)-Hypotonic fluid is absorbed into the circulation when large amounts are aspirated -Surfactant is altered (thickened)-Leads to hypoxia and reflex pulmonary arterial vasoconstriction, myocardial depression (brady), and pulmonary capillary permeability -Get return of fluid to lung and sudden pulmonary edema *Secondary pulmonary edema – rebound effect after being treated
Management in PICU-O2 at a rate to keep SaO2 @ >90%-PEEP with ventilation for severe pulmonary edema, actue resp failure, and/or aspiration pneumonia, pronounced CNS injury (GCS <8)-Positive End Expiratory Pressure = P (+) pops open alveoli; End (increase O2/CO2 exchange across membrane); used with pts with pneumonia; pul edema-Antibiotics only for pneumonia (starts after s/s appear, no prophylatically) -Monitor of ICP controversial but maintain ICP <20 mmHg-Treat seizures -Correct hypovolemia with colloid (eg LR/albumin)/crystalloids

-Maintain electrolyte balance and renal function (acute renal failure – dialysis to reverse; draw these labs often, because the kidneys may have shut down)
Manifestations-Category A: Awake (going to do well)
Fully conscious, may have mild hypothermia, mild chest radiographic changes (b/c may have aspirated something), mild arterial blood gas abnormalities (these kids are crying, awake, coughing)
-Category B: Blunted Sensation (maybe)Obtunded, stuporous, purposeful response to painful stimuli, mild to moderate
hypothermia, respiratory distress (apparent), chest radiographic abnormalities, arterial blood gas abnormalities
-Category C: Comatose (Not very good – 2% less)Unarousable, abnormal response to pain (decorticate, decebrate), abnormal
respiratory pattern (Chain-Stokes), seizures, shock, marked ABG abnormalities, dysrhythmias, metabolic acidosis (d/t apnea), hyperkalemia, hyperglycemia, DIC, sometimes no pulse
Overall Considerations-Help parents deal with guilt (watch pt’s reactions! Support services consideration and find the parent’s coping mechanisms)-Anxiety of not knowing outcome (what is going to happen)-Assess own feelings regarding situation! (know your own coping mechanisms)-Assess coping abilities and resource of family
Infant Signs of ICP-Tense, bulging fontanel-Separated cranial sutures (head circumference measure (Occipital Frontal Circumference)-Irritability-High pitched cry (won’t forget cry once heard)-Increased OFC -Distended scalp veins-Changes in feeding (won’t eat d/t increase of pressure and headache)-Cries with held or rocked-Setting sun sign
Child Signs of ICP (18 mos closing of sutures happens)-Headache-Nausea/Vomiting-Diplopia (increased blinking), blurred vision -Seizures-Until 5 yoa, a child’s suture line may open again with ICP (head shape/size may change)-Squinting

-Change in behavior-No loud noises
Monitoring ICP and Drainage-Neutral position: HOB up 10 to 20 degrees (neutral position not to occlude lymph/blood flow)-Head and neck neutral (not evidence based)-Temperature: normothermia w/o cooling devices or meds-Medication: Lasix (1st) and Mannitol (2nd) ~ to draw fluid (younger child, infant – more effective Lasix is because of immature kidneys; older – over 2 yo use mannitol 1st, then Lasix)-IV drip of midasolam (Versed) ~ to sedate -Pain meds-Pavulon to decrease muscle response to stimuli (paralyze them)-Anticonvulsants (if seizing)-Steroids with neoplasms (to reduce neuro damage)-Encourage presence of family (want family there at ALL times! Reduces stress of child)-Uninterrupted periods of sleep and rest (cluster activities)
Pediatric Glasgow Coma Scale (Wong page 1014)-Three part assessment
Eyes, verbal response, motor response -Score of 15: unaltered LOC-Score of 3: extremely decreased LOC (worst possible score on the scale)(8 and under, not good outcome) Assessment Parameters-LOC-Pupillary reaction-Vital Signs-Frequency of assessment depends on condition: range from every 15 mins to 2 hrs
ICP Monitoring-Indications for ICP monitoring
Glasgow coma scale <7Glasgow coma scale <8 with respiratory distress Deteriorating neurologic condition Subjective judgment – call doctor if needed (Obtunded on peds, not adults)
Head Injury: Etiology-Falls-Motor Vehicle injuries-Bicycle injuries(Children under 5, LOTS of head injuries)

Pathophysiology of Head Injury-Force on intracranial contents cannot be absorbed by the skull and musculoligamentous support of the head -Especially vulnerable to acceleration-deceleration injuries(Under 5 yo, can protect head because of weak neck muscles, can’t hold themselves steady)
Primary Head Injuries-Those injuries that occur at a time of trauma-Include: skull fractures, contusions, intracranial hematoma, diffuse injury (clotting to swelling (like brain in cranium))
Subsequent Complications of Head Injuries-Hypoxic brain injury-Increased ICP (secondary complication)-Infection (secondary complication)-Cerebral edema(Wear helmets, car seats)
Spina Bifida (lay term for myelomeningocele)-Embryonic neural tube defects-Midline defect that involves failure of the osseous spine to close-AB Occulta: a defect NOT visible externally (no paralysis, sac – just dimple or tuft of hair)-AB Cystica: a visible defect with an external saclike protrusion -Two major forms
Spina Bifida- Meningocele: encases meninges and spinal fluid but NO neural elements, no neural deficit-Myelomeningocele: contains meninges, spinal fluid, and nerves, neural deficit of carrying often serious, deficit-Clinically, the term spina bifida refers to myelomeningocele-Associated with folic acid deficiency-At risk: previous delivery with AB, anencephaly or encephaloele; folic acid <0.4 mg/d; folic taken before conception can reduce risk by 50%
Diagnostic Evaluation-Ultrasound-Elevated concentration of alpha fetal protein in aminotic fluid -16 to 18 weeks of gestation before AFP concentrations normally diminish
Management/Infancy-Prevention of infection-Maintain patency of sac-Neurological examination (ped doctor does this)

-Dealing with impact of anomaly on family-Early closure within 12 to 18 hours verses delay (skin flap)-Surgical objective is satisfactory skin coverage and meticulous closure -SE: meningitis, UTI (d/t non-sterile cathing at home), pneumonia is treated with vigorous antibiotic therapy, latex allergy (meningocele or myelomeningocele – will have latex allergy, reason is unknown)-Have baby lay on side, no back
Reye Syndrome (RS) [child 10 and under]-A disorder defined as toxic encephalopathy associated with other characteristic organ involvement-Characterized by fever, profoundly impaired consciousness, and disordered hepatic function (liver function) -Etiology is unknown/obscure-Most cases follow a common viral illness -Potential association between ASA therapy for fever and development of RS**Don’t give ASA with flu like symptoms!!-Pathophysiology- obscure; often follow viral illness-Diagnostic evaluation – LOC; liver biopsy (determine liver damage)-Therapeutic management – IV fluid, insulin (helps to reverse liver damage), corticosteroids, diuretics -Prognosis – r/t quickness of diagnosis-Nursing considerations: ICP monitoring, assess for bleeding
Other Neuro Conditions-Cerebral Palsy-Muscular Dystrophy
Muscular Dystrophy (MDs)-Largest group of muscular diseases in children (have neuro origin)-All have genetic origin with gradual degeneration of muscle fibers, progressive weakness, and wasting of skeletal muscles-All have increasing disability and deformity with loss of strength
Duchenne MD (DMD)-Also called pseudohypertrophic muscular dystrophy-Most severe and most common of the MD in childhood-X-linked inheritance pattern; one third are fresh mutations (X = male)-Incidence: 1 in 3500 male births
Characteristics of DMD-Onset between ages of 3 and 5 years (usually not good outcome)-Progressive muscle weakness, wasting, and contractures-Calf muscles hypertrophy in most patients -Progressive generalized weakness in adolescence-Death from respiratory or cardiac failure

Diagnostic Evaluation of DMD-Suspected based on clinical appearance-Confirmation by EMG (electromyography), muscle biopsy, and serum enzyme measurement -Serum CPK and AST levels high in first 2 years of life, before onset of weakness; levels diminish as muscle deterioration continues
DMD: Clinical Manifestations-Waddling gait, frequent falls, Gower sign (way a child gets up = walk up body – uses upper arms to ‘walk’ up legs, very distinct movement)-Lordosis (exaggerated curvature of lumbar of spine)-Enlarged muscles, especially thighs and upper arms (hypertrophy of upper muscles)-Profound muscular atrophy in later stages -Mental deficiency common (because loss of muscle)(heart becomes hypertrophic, atrophic, then dies)
Therapeutic Management of DMD-No effective treatment has been established-Primary goal: maintain function in unaffected muscles as long as possible -Keep child as active as possible (PT/OT, wheelchair, feeding devices to promote child’s independency) -ROM, bracing, performance of ADL’s, surgical release of contractures prn-Genetic counseling for family-Child = maintain/promote optimal function-Support/resources for the family
DMD: Nursing Considerations-Helping child and family cope with chronic, progressive, debilitating disease (negative outcome)-Help design a program to foster independence and activity as long as possible -Teach child self-help skills-Appropriate health care assistance as child’s needs intensify (home health, skill nursing facility, respite care for family, etc)
Pediatric Cardiovascular Disorders
Pediatric Indicators of Cardiac Dysfunction-Poor feeding (first sign)-Tachypnea/tachycardia-Failure to thrive/poor weight/activity intolerance-Developmental delays (discover thru ped office visits)- + prenatal history- + family history of cardiac disease-Pediatric Guidelines
Cardiovascular Dysfunction-Divided into 2 major categories:
-Congenital heart disease-Acquired cardiac disorders
Two Types of Cardiac Defects -Congenital
-Anatomic>abnormal function-Acquired
-Disease process (infection, autoimmune response, environmental factors, familial tendencies)
Congenital Heart Disease (CHD)-Incidence: 4-10/1000 live births-Associated Factors:
-Maternal rubella during pregnancy-Maternal alcoholism (cardiac anomalies)-Maternal age >40 (increase incidence of heart defects)-Maternal type 1 diabetes
-Increased of CHD:-Sibling with CHD-Parent with CHD-Chromosomal alteration – Trisomy 21 (over 50% with this has heart dz)-Other non-cardiac anomalies
Classifications of Defects-Historically: cyanotic and acyanotic (blue or not blue)-Current: Hemodynamic characteristics (the way we classify defects now)
-Increased pulmonary blood flow (pink because of increase blood flow to lungs; if they are stressed, then they may become cyanotic)-Decreased pulmonary blood flow (L/R shunting)-Obstruction to blood flow out of the heart (stenosis or defect)-Mixed blood flow
Increased pulmonary blood flow defects-Abnormal connection between two sides of heart
-Either the septum or the great vessels-Increased blood volume on the right side of the heart (increased volume to right side of heart)-Increased pulmonary blood flow -Decreased systemic blood flow (decreased blood flow to body and decreased CO)
Defects with increased pulmonary blood flow-ASD (atrial septal defect), VSD (ventricular septal defect), and PDA (patent ductus arterosis) -Intracardiac communication

-along septum and between great arteries
ASD ( Increased pulmonary blood flow ) *problems depends on size of hole
VSD (decreased CO also) Increased pulmonary flow/circulation
Patent Ductus arteriosus (“ Normal ” murmur you hear on newborn, but will close in 24 to 48 hours)

Obstructive Defects-Blood exiting the heart encounters a narrowing or “stenosis”
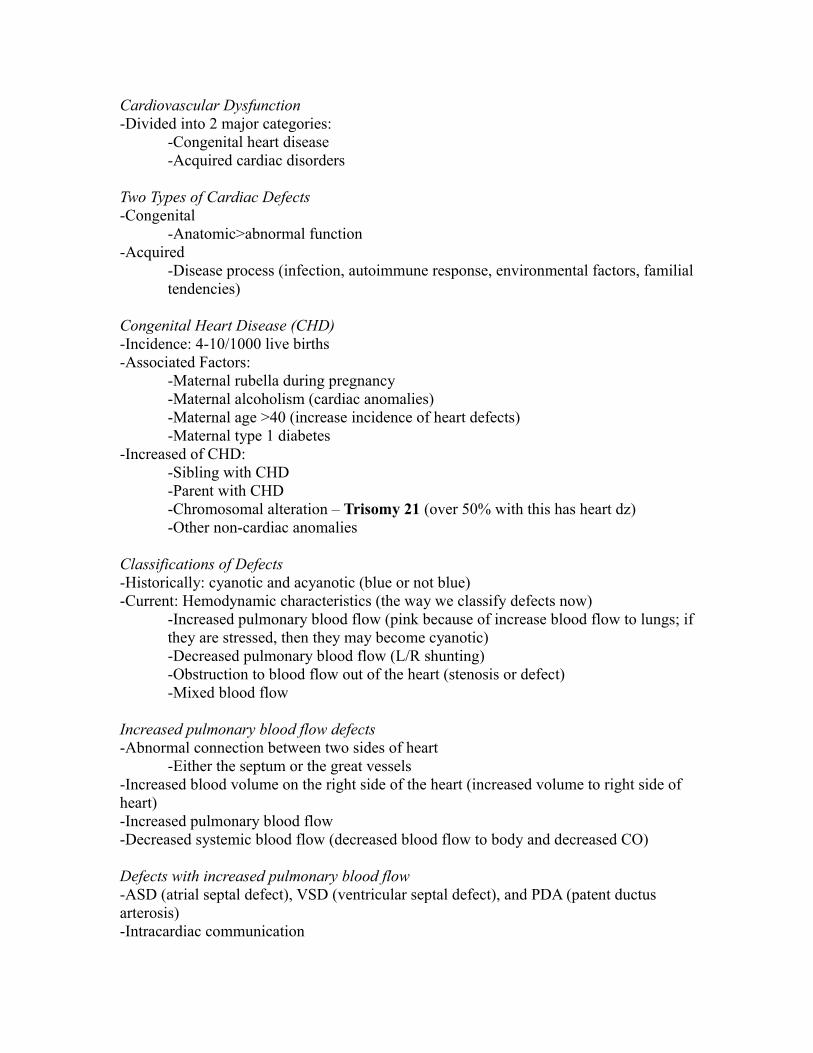
-Valvular/Subvalvular/Supravalvular-Coarctation of the aorta-Aortic/Pulmonic stenosis
Coarctation of Aorta ( Blood pressure differences in the upper to lower extremities d/t decreased blood flow to body)
Aortic Stenosis ( decrease systemic volume and decrease CO; ventricular hypertrophy )
“Acyanotic” treatment: these with surgery, suture may not be midline based on type/length of surgery (healing time in baby could be mere days, don’t cry a lot because it hurts to cry, they use glue instead of wire, etc)
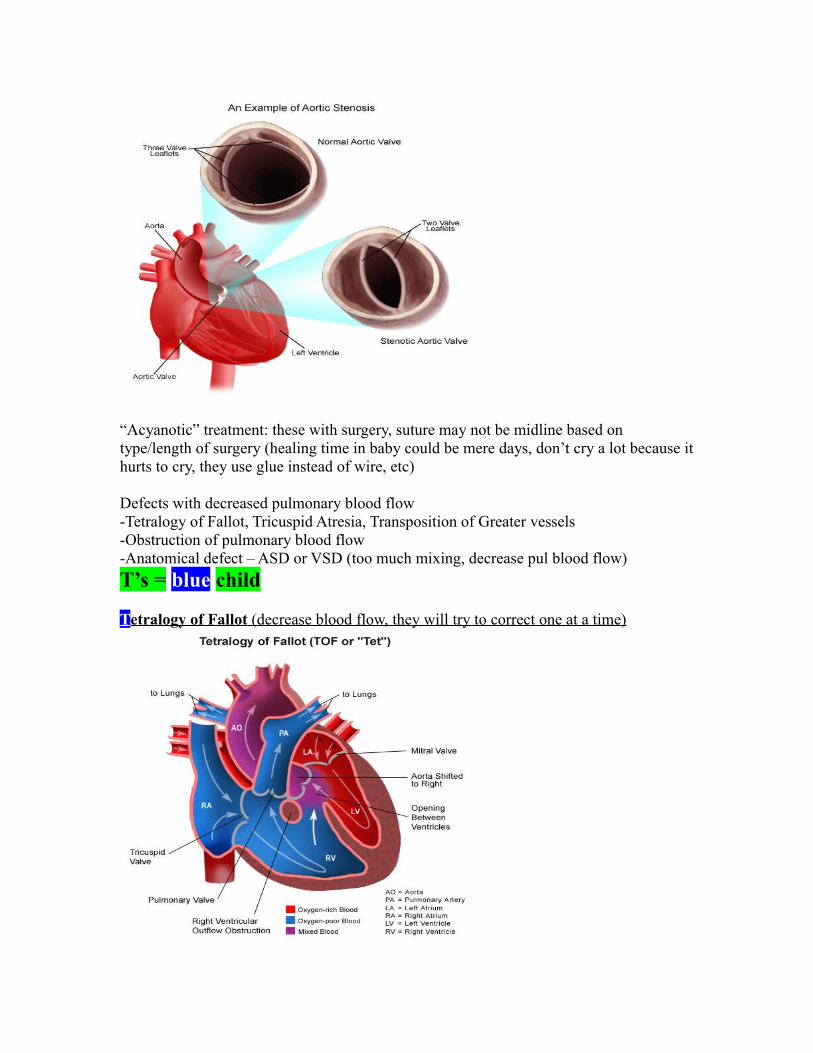
Defects with decreased pulmonary blood flow-Tetralogy of Fallot, Tricuspid Atresia, Transposition of Greater vessels-Obstruction of pulmonary blood flow-Anatomical defect – ASD or VSD (too much mixing, decrease pul blood flow)
T’s = blue child
T etralogy of Fallot (decrease blood flow, they will try to correct one at a time)

T ricuspid atresia (No valve at all! Correct early)
Mixed Defects-Transposition of the Great Arteries-Truncus arteriosus-Survival depends on mixing blood from the pulmonary and systemic circulations within the heart chambers
T ransposition of Greater Vessels (* Immediate surgery ; 2 independent functioning parts of the heart)
Congestive Heart Failure

-Heart cannot pump an adequate amount to meet metabolic needs (not a dz process for peds)-Right sided failure-Left sided failure*Sx of something else going on
Management -Goals:*Improve cardiac function (fix the structure)*Remove accumulated fluid*Decrease cardiac demands*Improve oxygenation, decrease consumption
CHF in children-Impaired myocardial function
-Tachycardia, fatigue, weakness, restless, pale, cool extremities, decreased bp, decreased urine output
-Pulmonary congestion (left sided)-Tachypnea, dyspnea, respiratory distress, exercise intolerance, cyanosis
-Systemic venous congestion (right sided)-Peripheral and periorbital edema, weight gain, ascities, heptaomegaly, neck vein distention
*1st place see edema = periorbital edema Edema – weight gain, dependent areas like back, bottom check those areas
How do we do that?-Digoxin-ACE inhibitors – Capoten, Vasotec (cardiac function)-Diuretics – Lasix, Aldactone (get rid of fluid)-Bed rest (**Need rest!!), oxygen (make sure have right flow rate based on size), sedation (decrease O2 demand metabolically)
Nursing Care-Help with adjustment -Educated (about drugs, what is going on, what happened, Lasix- dosage amount)-Help with coping-Prepare family for surgery (what is going to happen/what to expect)Dig- check apical pulse for about 120 bpm – below, DON’T give to neonates!
Acquired Cardiovascular Disorders-Bacterial infective endocarditis-Rheumatic fever
Rheumatic Fever/Rheumatic Heart Disease-RF
Inflammatory disease occurs after Group A
B-hemolytic streptococcal pharyngitis (strep throat)Infrequently seen in US, big problem in third worldSelf limiting
-Affects joints, skin, brain, serous surfaces, and heart-Rheumatic heart disease
Most common complication of RFDamage to valves as result of RF
*Especially mitral valve atrophy – regurg/back flow
Clinical Manifestations-Carditis-Polyarthritis-Erythema marginatum (red rash)-Subcutaneous nodules (all over skin)
Prevention of RHD-Treatment of streptococcal tonsillitis/pharyngitis (**Immediately!)
Penicillin G – IM x 1Penicillin V – Oral x 10 daysSulfa – oral x 10 daysErythromycin (if allergic to above) – oral x 10 days
-Treatment of recurrent RFSame as above
Kawasaki Disease (viral disease)-Acute, self limiting systemic vasculitis with cardiac comps-Patho: occurs in 5 stages that start with inflammation of capillaries of heart to scarring (2), thickening (3), calcification (4) and stenosis of arteries (5)-Clinical Manifestations:
-Acute: strawberry tongue, fever, conjunctivitis, rash, and lymphadenopathy-Subacute: fever ends, desquamation (peeling) of palms and soles, thrombocytosis, risk of coronary artery aneurysm -Concalescent: arthritis still present, elevated ESR and platelets
-Evaluation: 5 of 6 criteria, ECG (need to have 5/6 of sx to diagnosis)
Kawasaki DiseaseIV(IG)ASA 80-100 mg/kg/day-then, 3-5 mg/kg/day-anti-plateletsASA is a HUGE toxic med when taken at that toxic does!!!!!!!!! Toxicity s/e like GI bleeding (d/t damage to GI tract)
Type of Fracturesa. Avulsionb. Displacementc. Greenstick-pediatric specific/conscious sedation and break itd. Impacted
e. Longitudinal f. Obliqueg. Spiral-hones in on child abuseh. Transversei. Completej. Periosteal hinge (page 1154 Wong)
-Closed fractures are the most common
Fracture Healing (probably no questions on this)1. Fracture hematoma 2. Granulation tissue3. Callus formation4. Ossification5. Consolidation6. Remodeling
Collaborative Care-Overall goals of treatment:
- Anatomical realignment of bone fragments (reduction)- Immobilization of maintain alignment (casting, splinting)- Restoration of normal function (if all goes will, on own; PT/OT)
Nursing Management (Nursing Assessment)-Neurovascular assessment
**Color, temperature, capillary refill, peripheral pulses (equal bilaterally), edema, sensation, motor function, pain
…From block 2The 5 P’sPain and point of tendernessPulse-distal to the fracture sitePallor-color of extremity Paresthesia-sensation distal to the fracture site, numbness or tingling?Paralysis-movement distal to the fracture site
Fractures-Maybe placed in traction first (week or so because they case child)-Common injury in children-Methods of treatment are different in pediatrics than in older adult population)-Rare in infants, except with MVC/abuse-Clavicle most frequently broken bone in childhood, especially in those under 10 yo-School age: bike, sports injuries
Epiphyseal Injuries-Weakest point of long bones is the cartilage growth plate (epiphyseal plate)-Frequent site of damage during trauma-May affect future bone growth

-Treatment may include open reduction and internal fixation to prevent growth disturbance
Bone Healing and Remodeling-Typically rapid healing in children -Neo-natal period-2 to 3 weeks-Early childhood-4 weeks-Later childhood-6 to 8 weeks-Adolescence-8 to 12 weeks
The Child in a CastCast application technique-the material gets warm and the child will cry because of reacting to the castNursing Considerations-inform the child that it will get very warm (distract them); be careful and hold the casting material with the palm of our hands, indentations will cause pressure and hurt skin integrity; have to watch what kind of material is put over pillow, if it is plastic, could cause more intense heat feel Cast Care at Home- be careful about what kind of toys we give children in a cast ex Legos stuck in cast to see what happens; can cause skin problems; edges will fray and waterproof tape in a petal shape (petaling) and salvage the castInfection-heat, smell, drainage, check CNS – use back side of hand to check for heatDouble hip spinca with children who are not potty trained get double diapered in hospital as well as at homeCast Removal- use a saw, do not touch saw, demonstrate how the saw works that it will stop when it touches the skin, have then hear it, etc, children that are 2 are going to scream anyways and will probably have to restrain them, so expectation is age appropriateSkin Care- white, flaky, lighter, atrophied muscle; -mild/pH balanced soap and water (baby wash) first, apply lotions couple days later
Complications of fractures – Fat Embolism Syndrome (FES)Clinical Manifestations- Symptoms of ARDS: Assess for this frequently***Chest pain, tachypnea, cyanosis, decreased PaO2, dyspnea, apprehension, tachycardia-Rapid and acute course **, feeling of impending disaster, pt may become comatose in a short time (1st 8 to 12 hrs)
FES Collaborative Care-Treatment directed at prevention-Careful immobilization of a long bone fracture
Most important preventative factor = immobilization-Symptom management-Fluid resuscitation-Oxygen-Reposition as little as possible

Osteomyelitis-Inflammation and infection of bony tissue-May be caused by exogenous or hematogenous sources -Signs/symptoms begin abruptly; resemble sx of arthritis and leukemia (pain, fever)-Marked leukocytosis-Bone cultures obtained from biopsy or aspirate-Early x-rays may appear normal -Bone scans for diagnosis (definitive)
Therapeutic Management for Osteomyelitis-May have sub-acute presentation with walled off abscess rather than spreading infection-Prompt, vigorous IV antibiotics for extended period (3-4 weeks for up to several months)-Monitor hematologic, renal, hepatic responses to treatment
Physiologic Effects of Immobilization-Muscular system
Decrease muscle strength and endurance, atrophy, loss of joint mobility-Skeletal system
Bone demineralization (prevention – wt bearing, gravity tilt table), negative calcium balance -Metabolism
Decreased metabolic rate, negative nitrogen balance, hypercalcemia, decreased production of stress hormone
-Cardiovascular systemDecreased efficiency of orthostatic neurovascular reflexes, diminished vaspressor mechanism, altered distribution of blood volume, venous stasis/thrombosis, dependent edema
-Respiratory systemDecreased need for oxygen, diminished vital capacity, poor abdominal tone and distention, mechanical or biochemical secretion retention, loss of respiratory muscle strength
-GI systemDistention caused by poor abdominal muscle tone, difficulty feeding in prone position, gravitation effect on feces (constipation), anorexia
-Integumentary systemDecreased circulation and pressure leading to decreased healing capacity
-Urinary systemAlteration of gravitational force, difficulty voiding in supine position, impaired urethral peristalsis (trauma d/t privacy issues and won’t pee, so get UTI/urinary retention, might have to cath children because of this)
Psychologic Effects on Immobility -Diminished environmental stimuli-Altered perception of self and environment-Increased feelings of frustration, helplessness, and anxiety

-Depression, anger and aggressive behavior-Developmental regression
Nursing Considerations-Complete bed rest and immobility of limb-Pain management concerns-Long term IV access for antibiotic administration-Nutritional considerations-Long term hospitalization/therapy -Psychosocial needs
Juvenile Rheumatoid Arthritis (JRA)-AKA juvenile chronic arthritis -AKA idiopathic arthritis of childhood -Possible causes can be viral, familiar, unknown-Peak age: age 1-3 years and 8-10 years-Often undiagnosed-children just hurt and don’t know why, may not have severity of edema and can’t tell, sed rates are not elevated like it is in adults
JRA (cont)-90% of children have negative rheumatic factor, there is no good testing to determine JRA-Symptoms may “burn out” and become inactive -Chronic inflammation of synovium with joint effusion, destruction of cartilage, and ankylosis of joints as disease progresses, same traumatic occurrence as in adults
American College of Rheumatology Diagnostic Criteria-Age of onset <16 years-One or more affected joints-Duration of arthritis >6 weeks-Exclusion of other forms of arthritis
Therapeutic Management of JRA-No specific cure, but treat the symptoms-Goals of therapy: preserve function, prevent deformities, and relieve symptoms-Iridocyclitis/uveitis
-inflammation of iris and ciliary body-don’t see this in adult, specific to JRA-unique to JRA-requires treatment by ophthalmologist
JRA Pharmacology-NSAIDs=1st (anti inflammatory)-SAARDs-systemic slow acting anti rheumatic drug=2nd choice-Corticosteroids-Cytotoxic agents (Methrexate)-Immunologic modulators

Increased Intracranial Pressure (ICP)-Early signs and symptoms may be subtle-As pressure increases, signs and symptoms become more pronounced and level of consciousness (LOC) deteriorates
*Clinical Manifestations of Increased ICP in Infants-Irritability, poor feeding-High pitched cry, difficult to soothe -Fontanelles: tense, bulging-Cranial sutures: separated -Eyes: setting-sun sign-Scalp veins: distended
*Clinical Manifestations of Increased ICP in Children-Headache-Vomiting: with or without nausea-Seizures -Diplopia (Increased blinking), blurred vision
Behavioral Signs of Increasing ICP-Irritability, restlessness-Drowsiness, indifference, decrease in physical activity and motor skills-C/O fatigue, somnolence-Inability to follow commands, memory loss-Weight loss
Late Signs of Increasing ICP-Decreased LOC-Decreased motor response to command-Decreased sensory response to painful stimuli-Alterations in pupil size and reactivity-Papilledema-Decerebrated or decorticate posturing-Cheyne-Stokes respirations
Nursing Care of the Unconscious Child-Outcome and recovery of unconscious child may depend on level of nursing care and observation skills-Emergency management
Airway, reduction of ICP, treatment of shock
Assessment Parameters-LOC, papillary reaction, VS, frequency of assessment depends on condition; range from q 15 mins to 2 hrs
Pain Management for the Comatose child

-Signs of pain, increased agitation and rigidity, pain increases ICP, alteration in VS (usually increase in HR, RR, BP, and decrease in O2 sats)
Drug Therapies for Pain-Opioids-Fentanyl + Versed + Vercuronium -Acetaminophen and codeineAll based on child and level of sedation needed
Status Epilepticus-Definition: seizure lasting longer than 30 mins or series of seizures without regaining premorbid level of consciousness
Maintain airway (1st and O2), est IV access (for fluids), meds Metabolic acidosis state, tachy, neurons firing constantly, 50% mortality rate
Status Epilepticus-Diastat (prefilled rectal syringe)-Versed (intranasal)-IV Ativan or valproic acid-IV loading with Phenytoin for ongoing management #1 Ativan
Emergency Management-High dose sedatives-Maintain patent airway-Prepare for respiratory support
Types of CP-Spastic-Athetoid (wormlike movement of body)/dyskinetic-Ataxic (not in rhythm)-Mixed/dystonic (most common type)-Spastic
-most common clinical type-presents most often as hypotonia
Possible Motor Signs of CP-Poor head control after age 3 months-Stiff or rigid limbs-Arching back/pushing away-Floppy tone-Unable to sit without support at age 8 months-Clenched fists after age 3 months
* Possible Behavioral Signs of CP -Excessive irritability

-No smiling by age 3 months (norm 6 weeks to 2 months)-Feeding difficulties
-persistent tongue thrusting (4 mos extrusion reflex should go away)-frequent gagging or choking with feeds
CP and IQ-Wide variation-70% of CP patients have normal IQ-Difficult to assess-Rigid, atonic, and quadriparetic CP have highest incidence of profound impairment
Pharmacology-IV IgG-Digoxin-ACE inhibitors-ASA, NSAIDS-Lasix-Aldactone
Cardiopulmonary Resuscitation (CPR)-Pediatric cardiac arrest frequently represents the terminal event following respiratory failure or progressive shock-Pediatric cardiac arrest rarely results from sudden cardiac collapse, as in adult populations
Causes of Cardiac Arrest-Vary with age and underlying chronic medical condition-Out of hospital causes include: trauma, SIDS, poisoning, choking, severe asthma attack, drowning-In hospital causes typically d/t underlying condition
Standards of Care-CPR-Pediatric advanced life support (PALS)
The Child with Cognitive ImpairmentCognitive Impairment-Any type of mental difficulty or deficiency -Mental retardation
Early Behavioral Signs of Cognitive Impairment-Non-response to contact, voice, movement, touch-Irritability/hard to consol-Poor/slow feeding ***good indication-Poor eye contact during feeding-Diminished spontaneous activity
Functional Impairments (At least 2 of these 10)-Communication (red flag for something going on), home living, community sue, leisure, health (DS has more health concerns because usually born with cardiac issues [GI issues too]) and safety (big issue for them), self care (not able to meet these needs as quickly), social skills, functional academics, work, self direction
Mental Retardation – American Academy of Mental Retardation-Subaverage intellectual function (IQ less than 75)-Onset before age 18-Functional impairment
Causes of MR-Intrauterine infection (PROM)and intoxication-Trauma (prenatal, perinatal, post natal) -Metabolic or endocrine d/o (diabetic mommy)-Inadequate nutrition (anorexic mommy)-Postnatal brain dz-Chromosomal anomalies (trisomy 21)-Pre-maturity, LBW, post maturity are potential causes-Environmental influences like lead and toxins-Unknown prenatal influences-Psychiatric d/o with onset in childhood
Primary Prevention of MR-Rubella immunization #1 cause for MR is exposure to measles -Genetic counseling-Use of folic acid supplements-Educate about fetal alcohol syndrome and lack of nutrition -Educate about lead exposure
Classification of MR-Educable/mild – IQ 50 to 75-Trainable/moderate – IQ 35 to 55-Severe – IQ 20 to 40-Profound – IQ less than 20
Down syndrome-Also called trisomy 21
Extra chromosome 21 in 92% to 95%Translocation of chromosome 21 in 3% to 6%Mosaicism in 1% to 3%
Down syndrome-Etiology unknown – likely multiple causes-Most common chromosome abnormality (1 in 800 to 1000 live births)

-Most common genetic cause of MR-Maternal age
Age 30: incidence approx 1 in 950Age 40: incidence approx 1 in 100In about 5% of cases extra chromosome is from fatherMost DS infants have mothers younger than 35 yo [because this populous has most babies]
Down syndrome: Manifestations-Head [flat forehead], face [alignment], eyes, musculoskeletal [hypertonia/floppy]-Chest, neck [short with extra skin], abdomen-Genitalia, skin [modeling – blue discoloration]-Hands, feet – Simian crease on palms and soles of feet-cardiac issues
DS Congenital Anomalies-40 to 50% heart defects-Renal, Hirschsprung, TE fistula-Altered immune function-Skeletal defects
Atlantoaxial instability
DS IQ-Wide variation from severely retarded to low-average intelligence-Generally mild to moderate MR
Hyperlipidemia-Identify kids at risk and treat early-Treatment: dietary (restrict intake of cholesterol and fats)-If no response to diet Rx (colestipol/Colestid or cholestyramine/Questran)
Respiratory and Ventilatory d/oPneumonia: Subjective – I can’t breath, My chest hurtsObj – Fever, decrease O2 ,crackles, wheezing, tripod, decrease cap refill, decrease breath sounds, increase HR, increase RR, cough, sputum, increase BP (anxiety), change in color, accessory muscle useAssess: ineffective breathing pattern, impaired gas X, poor tissue perfusion, anxiety Plan: Dx: CXR, CBC, sputum C & S, ABGsRx: O2, bronchodilator, corticosteroids, antibioticsWhat to do: Elevate HOB [CNA], O2 on [LPN], pain [IV-RN or PO – LPN], inhaler [LPN], start IV [RN or cert LPN]Education: prevention, vaccines, and what to expect during proceduresADDRespiratory Assessment

-History: social [smoking], nutritional [height - wt loss/gain], cardiopulmonary [CHF], elimination [renal issues], sleep/rest [apnea esp overwt pts; need to sleep to heal]
Complaints Associated with Respiratory d/o-Dyspnea/difficulty breathing, chest pain, cough, sputum, hemoptysis [frequently seen with resp dysfunction]
Nursing Assessment-History of lung disease-Exposures to lung toxins-Smoking-Related hospitalizations [how long and for what?] -Spinal cord trauma-Extreme obesity d/t apnea-Use of O2, inhalers, nebulizers, immunosuppressant therapy-Previous intubation-Thoracic or abdominal surgery r/t complications-Exercise-Immunizations [up to date? Maybe cause of issues?]-Anorexia-Weight gain/loss-Diaphoresis-Dizziness-Dyspnea, wheezing, coughing, sputum, palpitations, swollen feet-Changes in sleep pattern d/t possible fluid shift -Fatigue-H/A-Chest pain-Anxiety
Focused Respiratory Assessment-Sudden increase restlessness and agitation ***1st sign/indication of hypoxia-Sudden decreased LOC (increase lethargy)-Significant change in pattern of breathing-Increased cyanosis or duskiness [look at pt’s color]-Increased use of accessory muscles [trouble breathing? Tripod?]-Increased dyspnea or orthopnea-Increase in adventitious breath sounds or development of abnormal breath sounds
Lab and Diagnostic Tests-Pulse Ox-CXR [check heart size]-Pulmonary angiograms [assess broncho tree]-Bronchoscope [get a specimen for adults and remove a foreign object for peds, like watch battery]-ETCO2 monitoring

-ABGs-V/Q scans [pin point PE and where not perfusing]-PFTs [pulmonary function test – lung status]
ETCO2/ End tidal carbon dioxide-ETCO2 monitoring
End tidal carbon dioxideAnalysis of CO2 thru infrared analysers [and how much CO2 has built up in lungs]Zero at beginning of exhalation and gradually plateausLow = hyperventilation; high = hypoventilation [hypo = retaining CO2]
ABGs-pH – amount of free H+ available in blood [7.35 - 7.45]-PaCO2 – partial pressure of carbon dioxide in arterial blood (resp component) [CO2 35 - 45]-HCO3 – concentration of bicarbonate in the blood (renal component) [HCO3 22 - 26]-Bases Excess – an indirect reflection of bicarbonate concentration in the bodyEx.pH 7.48 (increase alk)pCO2 51 (increase)HCO3 29 (increase) Metabolic alk with resp compensationEx.pH 7.26pCO2 42 NHCO3 17Metabolic acidosis
Respiratory d/o that predispose to failure-Obstructive lung dz: anomalies, aspiration, infection, tumors, anaphylaxis and larygnospasm from local irritation (drowning, intubation)-Restrictive lung dz: pneumonia, cystic fibrosis, Pneumothorax, pulmonary edema, asthma [what exacerbates the asthma]-Respiratory center depression [trauma, opioids]-Pulmonary diffusion defects
Mechanics of Ventilation -Air pressure variances – air flows from higher pressure to lower pressure---inspiration lowers pressure inside of the thorax, below that of atmospheric pressure---therefore air is drawn in---“sucking chest wound”-Airway resistance---asthma, tumor, mucous affect this…(determined by size of airway)-Compliance measure of elasticity expandability (emphysema, Pneumothorax, ARDS)-Lung function
Lung volumes-

Lung capacity-
Lung Function-Lung volumes
Tidal – volume inhaled and exhaled with each breathInspiratory reserve – amt inhaled after inhalationExpiratory reserve – amount exhaled after exhalationResidual – what remains in lungs after exhalation
-Lung capacity [how much can the lung really, really hold]Vital – max of volume exhaled from max inspirationInspiratory – max inhaled after normal expirationFunctional residual – volume remaining after expiration (residual volume)Total lung – the total of TV, IRV, ERV, and RV
Balance and Imbalance in ventilation and perfusion-ALT IN PERFUSION-change in PA [pulmonary arterial] pressure-alveolar pressure-gravity-ALT IN VENTILATION-blockage [exudate from pneumonia]-gravity
Ventilation – Perfusion Relationship aka V/Q ratio-Demonstrates relationship between alveolar ventilation to pulmonary capillary prefusion-Written V/Q ratio-For every 4 L of fresh air going into the alveoli, 5 L of blood flows past thus average ratio is 4:5 or 0.8. [Almost 1:1 ratio]-Ventilation and perfusion are both greatest in the bases of the lungs and greatest amount of gas exchange occurs in this portion of the lungs-V/Q ratio is gravity dependent
Possible Ventilation/Perfusion (VQ) States-Normal – ventilation matches perfusion- Low ventilation – perfusion exceeds ventilation (pneumonia, atelectasis, tumor, mucous plug)-High ventilation – alveoli have inadequate blood supply to allow gas exchange (pulmonary emboli, cardiogenic shock)-Silent unit – absence of ventilation and perfusion (Pneumothorax, severe ARDS)-All of these imbalances cause shunting of blood in some form resulting in HYPOXIA – treatment = oxygen
Pulmonary Function Tests-Tidal volume – amount of air in and out in one breath (7-9 mL/kg)-Vital capacity – max amt of air expired after a maximal inspiration (4,800 mL)-Minute ventilation – total volume of expired air in 1 minute (5-10 L/min)

TLC-Total lung capacity -Amount of air in lungs at end of maximal inhalation -The sum of RV (residual volume) and VC (vital capacity)-TLC depends on size and age of the child
Stages of Edema formation in Acute Respiratory Distress SyndromeA. Normal alveolus and pulmonary capillaryB. Interstitial edema occurs with increased flow of fluid into the interstitial
space (there is an increased permeability and fluids leak into that membrane) C. Alveolar edema occurs when the fluid crosses the blood – gas barrier
(alveoli’s membrane then opens up too allowing the fluid to fill it up also)This creates pulmonary edema!!
Etiology and Patho-Develop from a variety of direct or indirect lung injuries-Exact cause for damage to alveolar – capillary membrane not known (not sure what triggers it)-Patho changes of ARDs thought to be due to stimulation of inflammatory and immune system response-Neutrophils are attracted and release mediators producing changes in lungs
Increase pulmonary capillary membrane permeability Destruction of elastin and collagen Formation of pulmonary microemboli Pulmonary artery vasoconstriction
-Injury or exudative phase**1 – 7 days after direct lung injury or host insultNeutrophils adhere to pulmonary microcirculation
Damage to vascular endotheliumIncreased capillary permeability
-Engorgement of peribronchial and perivascular interstitial space -Fluid crosses into alveolar space
Intrapulmonary shunt develops as alveoli fill with fluid and blood passing thru cannot be oxygenated
-Alveolar cells type 1 and 2 are damaged Surfactant dysfunction atelectasis
-Hyaline membranes line alveoli [and forms a scar]Contribute to atelectasis and fibrosis [which the scar causes this]
-Severe V/Q mismatch and shunting of pulmonary capillary blood result in hypoxemiaUnresponsive to increasing O2 concentrations
-Lungs become less compliant-Increase airway pressure must be generated-Increase WOB [work of breathing]-Increase RR-Decrease tidal volume
Produces respiratory alkalosis from increase in CO2 removal Decrease CO and tissue perfusion [because fluid in lung and not in vasculature]
-Reparative or proliferative phase1-2 weeks after initial lung injuryInflux of neutrophils, monocytes, and lymphocytes (WBCs to rescue)Fibroblast proliferation (increase fibrin production)Lungs becomes dense and fibrousLung compliance continues to decrease
-Hypoxemia worsensThickened alveolar membrane
Causes diffusion limitation and shunting-If reparative phase persists, widespread fibrosis results -If phase is arrested, lesions resolve
-Fibrotic or chronic/late phase2-3 weeks after initial lung injuryLung is completely remodeled by sparsely collagenous and fibrous tissues
Decrease lung compliance Reduced area for gas exchange
Pulmonary HTNResults from pulmonary vascular destruction and fibrosis
Clinical Progression -Some persons survive acute phase of lung injury
Pulmonary edema resolvesComplete recovery
-Survival chances are poor for those who enter fibrotic phaseRequires long term mechanical ventilation (if they survive)
Clinical Manifestations-Initial presentation often insidious -May only exhibit dyspnea, tachypnea, cough [irritating], and restlessness-Auscultation may be normal for have fine, scattered crackles-Mild hypoxemia-Chest X ray may be normal or show minimal scattered interstitial infiltrates
Edema may not show until 30% increase in lung fluid content-Symptoms worse with progression of fluid accumulation and decreased lung compliance -Evident discomfort and WOB-Pulmonary function tests reveal decreased compliance and lung volume-Tachypnea-Diaphoresis-Cyanosis-Pallor-Decreases in sensorium/change in LOC-As ARDS progresses, profound respiratory distress requires endotracheal intubation and positive pressure ventilation

-Chest X ray termed whiteout or white lung d/t consolidation and coalescing infiltrates widespread throughout the lungs -If prompt therapy not initiated, sever hypoxia, hypercapnea, and metabolic acidosis may ensue
Complication of Ventilation -Immune [bacterial pneumonia, sepsis]-GI [paralytic ileus, gastric distention, stress ulcers and hemorrhage, malnutrition]-CV [dysrhythmias [because the heart gets squished], decreased CO]-Hematologic [thrombocytopenia, DIC – from micro clots]-Renal *common [acute renal failure – intraabdominal pressure from vent]
Complications-Nosocomial pneumonia
Strategies for prevention Infection control measuresElevating HOB 45 degrees or more to prevent aspiration Mouth care, sterile technique, replace equipment often
-BarotraumaRupture of over distended alveoli during mechanical ventilation To avoid, ventilation with smaller tidal volumes
Results in higher PaCO2“Permissive hypercapnia”
-Volu-pressure traumaOccurs when large tidal volumes used to ventilate noncompliant lungs
Alveolar fractures and movement of fluids and proteins into alveolar spaces
Avoid by using small tidal volumes or pressure ventilation-Stress ulcers
Bleeding from stress ulcer occurs in 30% of pts with ARDS on PPVManagement strategies include correction of predisposing conditions, prophylactic anti ulcer agents, and early initiation of enteral nutrition
-Renal failure Occurs from decreased renal tissue oxygenation from hypotension (renal first to go!), hypoxemia, or hypercapnia May also be caused by nephrotoxic drugs used for infections associated with ARDS
Nursing Assessment -Abdominal distention, ascities-Somnolence, confusion, delirium-Changes in pH, PaCO2, SaO2-Decreased tidal volume, FVC-Abnorm x-ray, pulmonary artery and pulmonary artery wedge pressures
Planning

-Patient with at least 60 mmHg and adequate lung ventilation to maintain normal pH following recovery will have
PaO2 within normal limitsSaO2 >90%Patent airwayClear lungs on auscultation
Respiratory Therapy -Oxygen
High flow systems used to maximize O2 deliverySaO2 continuously monitored Give lowest concentration that results in PaO2 60 mmHg or greater [because you can hyper-oxygenate them, so the 60 mmHg]
-Risk for O2 toxicity increases when FIO2 exceeds 60% for more than 48 hoursARDS pt’s commonly need intubation with mechanical ventilation because PaO2 cannot be maintained at acceptable levels
-Mechanical ventilation May still be necessary to maintain FIO2 at 60% or greater to maintain PaO2 at 60 mmHg or greaterPEEP [opens collapsed alveoli] at 5 cm H2O to compensate for loss of glottic function; if they have any fluid what so ever in the lungs, will have PEEP
-Additional pressures from PEEP can compromise venous return to right side of the heart
Decreases preload, CO and BP-Can cause hyperinflation of alveoli, compression of capillary bed, reduction in blood return to left side of heart, and reduction in BP-Can result in barotraumas and volu-pressure trauma-Alternatives to PEEP used if hypoxemic failure persists-Positioning strategies **Lay pt on unaffected side!!!! To clear the bases!!!**
Turn from prone to supine position (keep pt moving often)May be sufficient to reduce inspired O2 or PEEP
Fluid pools in dependent regions of lung-Mediastinal and heart contents place more pressure on lungs when in supine position than when in prone position
Predisposes to atelectasis-Prone position typically revered for refractory hypoxemia not responding to other therapies
Plan for immediate repositioning for cardiopulmonary resuscitation -Lateral rotation therapy to provide continuous, slow, side to side turning-Vibratory pack for chest PT [to loosen up secretions]
Obtain baseline assessment prior to initiation
Medical Supportive Therapy-Maintenance of cardiac output and assessing tissue perfusion
Continuous hemodynamic monitoringArterial cath

-Pulmonary artery cath is normally inserted to allow monitoring of pulmonary artery pressure, pulmonary wedge pressure, and CO
Administration of crystalloid fluids or colloid fluids, or lower PEEP if CO falls-Use of inotropic drugs may be necessary -Hemoglobin usually kept at levels >9 or 10 within SaO2 >/= 90%-Packed RBCs-Maintenance of fluid balance-May be volume depleted and prone to hypotension and decreased CO from mechanical ventilation and PEEP-Monitor PAWP, daily weights, and I&Os, to assess fluid status
ARDS and RDS-Similarities
Decreased surfactant Congestive atelectasis and hyaline membrane formation {ARDS hyaline
membrane is not as thick}-Differences
Cause of deficient surfactant Chest compliance [infant is more collagenous]
Respiratory Distress Syndrome (RDS)-Syndrome of immature infants-Also called IRDS and HMD [hyaline membrane]-Etiology
100-1500 gms and 26 – 37 weeks gestation Diabetes mommy, c-section, intrauterine bleeding, lack of surfactant because they are so small
Intubation -ET tube into the mouth or NT (nares) for placement in the trachea-Emergency situation when a pt can’t maintain their own airway, mechanical ventilation, suctioning-Done by MD RN or other trained personnel [paramedics, respiratory therapy]-Cuff is inflated to prevent air leaking, to minimize the possibility of aspiration, and to minimize movement; and to keep upper and lower airways separate
Care of the client with artificial airways-Oropharyngeal/nasopharyngeal airways-Tracheostomy tube-Endotracheal tube-Intubation---3 checks for placement: listen gastric area, listen left and right anterior lung fields, lateral lung fields to ensure both lungs are getting air-Suctioning for patent airway-Extubation - ween pt from vent, deflate cuff and extubate pt-Communication – some pts are alert and awake, in order to communicate, give them pen/paper or whiteboard

-Safety/prevent of injuries – confused because of hypoxia and could rip out vent
Emergency Trach tube-Intubation
Curved hemostatObturatorReplacement tubeSuction – before endotracheal tube in placed
-Endotracheal tubesAssess chest excursionListen over epigastric and bilat lung fieldsCXR just to confirm placement and in correct spot
-Suctioning via tube [inline suction cath, in closed system that can be used for 24 hours, good because it doesn’t keep introducing ways for bacteria to infiltrate]-Warm, humidified oxygen (esp with ped population, this is to assist with secretion loosening)-Up to 3 weeks allow vent to be in, if need longer, then trach to decrease irritation of and trauma to the tracheal lining, reduce incidence of vocal cord paralysis-Disadvantages = discomfort, depressed cough reflex, thicker secretions (because vent irritating the tracheal lining), inability to talk
Nursing Care of ET-Max suction pressures
Infant: 60-100 mmHg (5 seconds)Children: 100-120 mmHg (5 seconds)Adults: 120-150 mmHg (10 seconds)
-Check for minimal air leak in cuff -Cuff pressures checked with manometer (to measure air in cuff)-Maintenance of trach tube
Cuff, ties (not loosening, snug (finger breadth room on each side) and if there is secretions on the ties, CHANGE IT!!!), plugs (assist with communication), oral care
Nursing Diagnosis-Ineffective airway clearance-Ineffective breathing pattern-Risk for imbalance fluid volume-Anxiety-Impaired gas exchange-Imbalance nutrition: less than body requirements
Care of intubated child/adult -Assess vent for signs of malfunction [make sure vent is on]-Assess vent for deviation from desired settings
-Promote effectiveness of vent by positioning, suctioning [whenever the pt needs in, prn basis and sats start to drop], ensure adequate humidification [check all tubing and humidification is on and water bubbling], support pt and family -Assess child
VS, pulmonary status, oxygenation, airway patencyNutrition statusI&OSkin integrity (especially face and lips or neck and stoma or even ears)
-Sedation [most time pts are sedated]
Extubation-Intentional -Unintentional [if they extubated, grab emergency ambu bag and call code because they are not breathing] [peds have two inner cannulas because skin closes quickly and may need smaller cannula]ET tube extubated – call code and nasal pharyng Extubation – just stick it back in-Use humidified mask to prevent airway edema
Mechanical Ventilation-Ventilation verses respiration
Vent is gross movement of air in and out of lungs, that is it, can’t cause O2 CO2 exchangeComposed of air that fills the conduction airways; does not take part in gas exchange as well as air that fills the alveoliRespiration is exchange of O2 and CO2 across a semi-permeable membrane Respiration remains dependent on lung tissues and pulmonary capillaries
-A pressure breathing device that maintain ventilation and O2 delivery for a prolonged period-In ICU, tele, med/surg and long term care facilities, even at home-Indications: low PaO2, high PaCO2, acidosis, post op thoracic or abdominal surgeries, over dose, neuromuscular diseases, trauma, shock, coma-ETCO2 monitoring – end tidal PCO2 monitoring (capnography) – continuous recording of the carbon dioxide level in expired air in mechanically ventilated pts
Features and Settings-Controlled Ventilation (CV) = 100% of the RR via the vent at the preset fixed rate and volume [machine is set and machine will function, no matter what] *most common [delivers preset volume or pressure regardless of pt’s own Inspiratory efforts – usually used for pts who are apneic]-Assist/Control (A/C) = vent is activated by the pt attempting to inhale and delivers air -Intermittent Mandatory Ventilation (IMV) = allows pt to breath spontaneously but gives a mandatory breath at preset rate per min-Synchronized Intermittent Mandatory Ventilation (SIMV) = vent will start mandated breath after pt initiates a breath *most common [ventilator breaths are synchronized with pt’s respiratory effect – usually used to wean pts from mechanical ventilation -

-Pressure Support (PS) = when pt breaths, vent pressure rises to preset level to match pt’s Inspiratory pressure-Positive End Expiratory Pressure (PEEP) = used to increase functional residual capacity or resting volume of the lungs [positive pressure applied at the end of expiratory – used with CV, A/C, and SIMZ to improve oxygenation by opening collapsed alveoli]-Continuous Positive Airway Pressure (CPAP) = positive pressure throughout the respiratory cycle of the spontaneous breathing pt or with vent on IMV [similar to PEEP but used only with spontaneously breathing pts – maintains constant positive pressure in airways so resistance is decreased]
Need for Vent Support-Acute vent failure [they stop breathing]-Acute hypoxia-Pulmonary mechanisms [RR, vital capacity, negative inspiratory force, minute ventilation]-PaCO2 > 50, ph < 7.3-PaO2 < 50 [>35 breaths/min; vital capacity < 15 mL/kg; < -20cm H2O; > 10 L/min]
Types of Vents-Negative pressure-Positive pressure [named by how they cycle]
Pressure cycled, volume cycled, time cycled, flow cycled
Negative Pressure Vents-First used in 40 and 50’s during polio outbreak and was called the Iron Lung-Entire body encased and compressed diaphragm to cause internal negative pressure-Used with neuromuscular problems, CNS d/o and injury, severe COPD
Positive Pressure Vents [Vents we see in hospitals and homes]-3 types
Pressure cycled [gas driven or electrically powered, preset volume by Inspiratory pressure] Timed cycled [determine RR by time]Volume cycled [delivers preset tidal volume that has been programmed into vent, delivered regardless of pressure required, artificial airway is necessary]
High Frequency Vent [for neonates and small children]-Jet, low interrupter, and positive pressure-Use a rapid cycling rate [like up to 200 breaths per min]-Deliver small tidal volumes with each cycle -Lung volume held relatively constant, cycle of inflation and deflation is reduced -Gas exchange maintained with less lung injury
Weaning-Criteria- vital capacity of 10-15 mL/kg of body weight (1000 average), spontaneous inspiratory force, PaO2 greater than 60%, stable vital signs

-Alert and awake-Good respiratory muscle strength-Patent airway and be able to clear own arrhythmia -No life threatening arrhythmias-Little or no vasopressor drugs-Chest reasonably clear per CXR and auscultation-PaO2 > 60 with 40-60% O2-Cough effectively-Generate Inspiratory force to initiate independent ventilation
Oxygen Toxicity-S/S: bronchial irritation, dry cough, decrease in vital capacity, alveolar collapse, prolonged exposure causes structural damage -End Stage: progressive atelectasis, consolidation, fibrosis, ocular retinal damage leading to blindness (retrolental fibroplasias – peds specific)
Nursing Diagnosis-Ineffective airway clearance-Ineffective breathing pattern-Risk for imbalance fluid volume-Anxiety-Impaired gas exchange-Imbalance nutrition: less than body requirements
Evaluation-No abnormal breath sounds-Effective cough and expectoration-Normal RR, rhythm, and depth-Synchronous thoracoabdominal movement-Appropriate use of accessory muscles-Decreased or absent peripheral edema-Normal pulmonary artery or pulmonary artery wedge pressures-Decreased anxiety-Verbalization of positive attitude toward outcome-PaO2 and PaCO2 within normal ranges-Maintenance of weight or weight gain-Serum albumin and protein within normal ranges
ECMO Complications [Extra corpro membrane oxygenation]-Machine does what the lungs would normally do-Usually on children under 5-Right internal jugular, reservoir are and sends to pump where there is a membrane which is the ‘lung’ and has oxygen that comes in contact with children’s blood and oxygenates them and the leaves the right carotid -Complications = hemorrhage, blood membrane interaction, technical mishaps, inclusion criteria, institutional expense

Chest Drainage-Used to re-expand the involved lung, remove excess air, fluid, and blood after trauma or surgery-Principle of negative pressure-pressure in the chest cavity is lower than the pressure of the atmosphere, causing air to move into the lung during inspiration-When the chest is opened, the negative pressure is lost- which may collapse the lung
Chest Drainage -Single bottle system [water seal, drainage, air vent]-Two bottle system [water seal, vent, drainage]-Three bottle system [drainage, water seal, suction or vent]-Commercial systems [pleur-evac; atrium]-Chest tube is connected to the drainage system using a one way valve -Water in the second chamber acts as a seal and allows air and fluid to drain from the chest into the first chamber without reentry of air-Water level fluctuates with breathing-Suction creates a negative pressure to promote drainage of fluid and air-pneumo = high position on the chest-hemo = lower on the side because of gravity
Nursing interventions for chest drainage-Assess respirations, ROM affected side, C & DB q 2 hours, ambulate, pain meds, low or semi Fowlers, observe system for proper functioning, -Maintain chest drainage system [below chest level, assess tubing, tape connectors, note and record drainage, assess patency of tubing, and change collection chamber prn: clamp, removal procedure]
Nursing Care Chest Tubes-Water level in suction control, taping connections, suction, stripping, assessment (patency, crepitus, drainage), air leaks, potential complications (disconnections, accidental removal), insertion, removal
Subcutaneous Emphysema-Air enters the tissue – causes crackling sensation when palpated-Not serious unless interferes with breathing, spontaneously absorbed if the underlying air leak is treated-assess and monitor the edema and watch for tracheal deviation, big issue then!-Treatment – high concentrations of oxygen – helps promote reabsorption of SQ air by washing nitrogen from the blood and improving its diffusion from the SQ tissues
FIRE!!!Ouch!!Temp < 104 F – no injuryTemp > 104 F – logarithmic increase in tissue distractionWater = 140 F – full thickness burn in 3 seconds

Water = 158 F – full thickness burn in 1 second**For peds precaution turn hot water heater at 120 F to prevent burns in children at home
Pathogenesis-Burns follow common patterns of tissue response-Zone of coagulation [like the center of the bull’s eye]
Skin necrosis is this zone is irreversible -Zone of ischemia [the middle of the target area]
Dynamic areTissue may die or survive in this area
-Zone of hyperemia [outer part of target area]
Classification of Burn Depth-Superficial [1st degree] Ex. Sunburn
Minor epithelial damage of the epidermis; red/skin blanches on touch; tender, pain eased with cooling; dry; no blisters; heals in 3 to 7 days
Superficial Partial Thickness (2nd degree)-Thin walled, fluid filled blisters; pink; moist, shiny, weeping; blanche with pressure; exquisitely tender to touch, sensitive to cool air; heal in 2 to 3 weeks usually without scarring
Deep Partial Thickness (2nd degree) -Extend into reticular dermis; blisters are thick walled and commonly ruptured; color is mixed red and white; sense when pressure is applied; heal in 3 to 6 weeks with potential for hypertonic scarring; contractures are common sequelae, ex. Splash scalds
Full thickness (3rd degree)-Destruction of both dermis and epidermis; deep, red, black, yellow or white/leathery/charred; dry; edema present; insensate; greater than 1.0 cm in diameter requires skin grafting; ex. Immersion scalds, flames, chemical and high voltage electrical images
Full Thickness (4th degree burn)-Full thickness destruction of skin, subcutaneous tissue, with involvement of fascia, bone or other structures; requires extensive debridement and complex reconstruction; prolonged disability
Severity ClassificationMajor Burn Injury (Partial thickness)- >25% BSA in adults – going to a burn center- > 20 % in children < 10 years, adults > 50 years – should also go to a burn center-Full thickness- >10 % of BSA (also go to a burn center too because it is full)-Anatomical sites: face, eyes, hands, feet, perineum – also go to burn center because of importance of these sites, they will send that pt to a burn center

-High voltage electrical injury-These injuries should go to a burn center!!
Moderate Burn Injury – hospitalization but not burn center, unless involving eyes, ears, face, hands, feet, perineum-Partial thickness
15 – 25% of BSA in adults10 – 20% of BSA in children
-Full thickness2 – 10% of BSA not involving eyes, ears, face, hands, feet, perineum
-No electrical or inhalation injuries, pulmonary or endocrine d/os-Hospitalization, not necessarily in burn center
Minor Burn Injury = urgent care unless it involves eyes, ears, feet, hands, perineum-Burn < 15% of BSA in adults; < 10% of BSA in children-Full thickness burns < 2 % of BSA not on face, hands, perineum, ears, feet-Adult < 60 years of age-No chronic d/o-Consider outpatientt management
Carbon Monoxide/Sulphur Dioxide-Deadly poisons because of inhalation injury
Inhalation InjuriesCarbon Monoxide -Produced from incomplete combustion of C containing materials-Colorless, odorless, tasteless, nonirritating-Ngb has 20 X affinity for CO than O2-Carboxyhemoglobing < 10 ppm is acceptable, 10 to 20 ppm means check spirometry, 20 to 50 severe exposure Sx: fatigue, irritability, dysrhythmias, ataxia, vomiting, syncope, coma HTN tinnitus changes in LOC, cherry red skin
Inhalation Injury-Sulfur Dioxide (SO2) and Nitrous Oxide (NO)
Toxic, inhaled in soot, mix with H2O to form corrosive acids and alkalisToxic fumes from burning plastic more dangerous than smokeNoxious gases, hydrogen cyanide, HCl, sulfuric acid, halogens
Pre-Hospital Management-Remove victim from source of burn-Remove from heat source-Remove burned clothing, restrictive clothing, jewelry -Wash skin with cool water for no longer than 30 mins; NO ICE!!!-Beware of hypothermia
Minimize heat loss by placing pt between clean dry sheets
Uncovering the Blister Controversy-Pros of unroofing
Blister fluid may be deleterious to wound healingUndrained fluid confined by necrotic skin can lead to a closed space infection
-Cons to unroofing Natural biologic dressingIntact blister roof prevents bacterial colonization
-Suppresses bactericidal activity-Suppresses phagocytosis and intracellular destruction of P aeruginosa-Retards normal fibinolytic process that works to maintain dermal vascular patency after a burn injury
Additional Management Concerns-Ileus can occur in pts with burn injuries > 20 % of BSA-NG tube to prevent vomiting and aspiration-Give tetanus prophylaxis if indicated-Do not give prophylactic antibiotics
Emergency dept management: airway-Look for signs of inhalation injury [hx, physical]-Give 100% O2-Intubate rather than observe-Fiberoptic bronchoscopy-Check carbon monoxide level-Cyanide poisoning can also occur
Escharotomy-Assess peripheral pulses [recognize diminished or absent pulse; most common cause of diminished pulses is inadequate resuscitation]-High index of suspicion of circumferential burns-Treatment-If urine output is good and pulses are not, do emergent escharotomy-Thoracic escharotomy occasionally need to improve chest wall compliance
Resuscitation Formulas-Parkland formula (most popular)
4 mL/kg/% of BSA burned is given in 24 hours + maintenance fluidKnow how to use Parkland formula and calculate½ in the first 8 hours from the time of the burn60 kg with BSA burn of 25% and within in first 8 hours4 ml x 60 kg x 25 (for the %) = 6,000 mLBut, must give ½ in first 8 hrs, so we must give 3,000 mL or 3L And the next 16 hours you give the rest of the 3,000 mL(if she asks, you would for that problem you would give 375 mL/hr for the first 8 hours and 187.5 ml/hr for the next 16 hours)

-Galveston formula5000 mL/m2 BSA burned (losses) + 2000 mL/m2 BSA (maintenance)
Most common error is over hydration!
Summary of Resuscitation Fluids-Pros of hypertonic solutions: total quantity of fluid reduced less edema, better urine formation -Cons: hypernaturemia, renal failure, death-Pros of colloid solutions: decreases extravasation of fluid less edema-Cons: may increase relative risk of mortality, vascular permeability ? up to 36 hrs post injury, what is happeningIsotonic solutions are better for initial therapy
Topical Agents-Silver sulfadiazine (SSD); biobrane; bacitracin; mafenide acetate (sulfamylon cream); duoderm; silver nitrate
Cardiovascular-Elevated HR-Burns of > 40% TBSA produce myocardial dysfunction
-Plasma volume drops; decrease CO; increased peripheral vascular resistance
Fluid Replacement-Dramatically improves outcome; must be implemented carefully in elderly and children; loss of capillary seal leads to massive fluid and electrolyte shifts from intravascular to interstitium; usually restored 18 – 36 hours; initial 24 hours of fluid therapy is aimed at maintaining vital organ function (kidneys, brain, heart); assess urine output, VS, mentation, cap refill, peripheral pulses; fluid of choice: LR [adults]; children: D 5 ½ NS; Infant: D5 ¼ NS
Pulmonary -Insufficiency occurs at 2 points: immediate: inhalation and 10 days – 2 weeks: infection-Eschar formation on circumferential burns to chest prevent adequate expansion-Inhalation injury: facial burns with charred lips and tongue; carbonaceous sputum; wheezing; stridor; cough; tachypnea; singed nasal hair; altered LOC, enclosed space, assess for CO poisoning-With 60-70% of pts with inhalation injury die-Result of contact with smoke causes ulceration of mucous membranes, edema, excessive secretions, decreased cilliary action, bronchospams, inactivation of surfactant, atelectasis-Leads to air flow obstruction-Treatment: high flow humidified O2; nasal intubation (over endo); pulmonary toilet, pharmacologic interventions; ventilatory support; ABGs; carboxyhemoglobin, bronchoscopy
Peripheral Vascular

-Assess each extremity for color, temperature, pulses, cap refill, sensation, pain and motor movement-Elevate burn extremity above level of heart-Remove jewelry and constrictive clothing-Compartment Syndrome: occurs with 3 rd degree circumferential burns and edema and do not elevate above heart
Sx: pain on passive stretching, decrease sensation, weakness, swelling, pain beyond expected for injury
Neuro and Cognitive-May experience confusion, flat affect, unable to concentrate, short term memory loss-Seizures, H/A, peripheral nerve damage, loss of muscle strength, -Spinal cord injury with high voltage injuries-Long term or permanent numbness, tingling, sensitivity, paralysis-Altered LOC may be due to hypoxia, hypercarbia, hypovolemia, cerebral edema, carbon monoxide or trauma-CT scan-Glasgow coma scale-Pain: chronic or acute [anxiety contributes, MS and Midazolam, coping using multifaceted approach]
Gastrointestinal -Complications include paralytic ileus, gastric dilation, constipation, stress ulcers-TBSA > 20% needs gastric tube for emptying and decompression-Antacids to neutralize acids and histamine receptors agonist to decrease gastric acid production-Intestinal mucosa loses ability to contain bacteria within the intestinal lumen (bacterial translocation) and goes to other parts of the body: cause of Multi Organ Dysfunction System aka MODS (e coli gets into vasculature and causes sepsis)
Metabolic-Initially depressed but, within a few days, marked hormonal changes occur resulting in hype-metabolic state (remains until wounds close)-Increase in CO, O2 consumption, CO2 production, caloric requirements, energy consumption, HR, RR, and body temp-Increased calories and protein needed-Labs: serum albumin, urinary urea nitrogen and creatinine, total lymphocyte count
Hemodynamic Status (don’t test on this)-Burn Shock -Pro-inflammatory mediators released
Increased capillary permeability caused by inflammatory response leads to fluid shifts into the interstitial spacesDirect myocardial depression d/t decreased circulating volume Fluids lost by evaporation
-Place two large bore IV’s through non burned tissue

-Evaluate burned areas to minimize edema-Place Foley cath
Renal -Urine output: child <30 kg: 2 ml/kg/hr; > 30 kg = adult (adult 30 -50 ml/hr)-Muscle damage from electrical current or crush injury, urine may be red to reddish-brown color because of myoglobin-Myoglobin is released from damaged muscle and can clog renal tubules-Need output of 75 to 100 ml/hr in an adult or 2 ml/kg/hr in child with Myoglobin-Solubility of Myoglobin increases in alkalinization of urine so add HCO3 to IV
Emergent Labs-Hgb Elevated r/t fluid volume loss-Hct Elevated r/t fluid volume loss-Urea nitrogen Elevated r/t fluid vol loss-Glucose Elevated stress response-Na Decreased lost with plasma leak-K Elevated r/t disruption Na/K pump, tissue destruction, RBC hemolysis-Cl Elevated r/t fluid volume loss and reabsorption in urine-Protein Low r/t loss in wound-Albumin Low r/t wound and vascular membrane loss
Wound Healing-Performed in warm environment to prevent hypothermia-Cleansing: with H2O (hydrotherapy)-Debridement: partially done with hydrotherapy, wet to dry or wet to moist dressings-Mechanical with scissors, forceps, chemical, surgical -Topical anti microbial therapy:
Neomycin: painless, no allergy, only superficial and donorAGNO3 (silver nitrate): excellent spectrum, no allergy or pain Silvadene: broad coverage, minimal sensitivity and allergy-Mafenide acetate: excellent penetration, {gram (–)}coverage, painful 15 – 30 mins really, really painful!!
Wound Care-Open vs closed dressing-Biologic dressings obtained from animals (xenografts or heterografts) or from humans (allografts or homografts)-Synthetic: film materials such as Opsite or Tegaderm, composite (used on wounds with exudate) ex. Lyofoam-Biosynthetic: used on all types of wounds and Biobrane or Curabsorb are examples-Closure: Autograft (full thickness [not very common] and split thickness (meshed/sheet by cloning))
Burn Rehab-Behavioral changes
Anxiety, fear, grief, depression, sleep problems, acute stress d/o, aggressive or regressive behavior
-Pain adequate pain control-Physical mobility
PT/OT-Daily care includes cleansing with mild soap and water, applying emollients, protect from mechanical trauma, sun exposure for 1 year-Scar management achieved with compression garments for 12 to 18 months-Pressure also helps reduce local blood supply, improving scar’s appearance
Nursing Diagnosis-Impaired gas exchange -Ineffective airway clearance-Fluid volume deficit-Pain -Impaired tissue Integrity-Altered tissue perfusion-Altered nutrition-Sensory/alterations -Body Image disturbance -Risk for infection-Knowledge deficit
Rule of Nines (She will ask one question on this!)Face 4.5 % and back 4.5% Head = 9%Trunk 18% Each leg back = 9% and front 9%
Non-accidental Burns-History inconsistent with burn pattern-Question family members separately-Scald burns with well demarcated lines and absence of splash marks (these are not accidental burns)-Scald burns that are full thickness (usually not by accident)-Patterned contact burns
***Test Break Down***Respiratory ?s 21 PE, COPD (asthma, pneumonia, ventilators (know these ET/chest tubes))
Peds (1 to 2 ?s per area) 16 ?s totalDrowning, near drowning, etc
Burns 12 ?s
RN role 1 ? on prioritization