pay-per-use' concept in healthcare: a grounded theory ... · [email protected];...
TRANSCRIPT

Proceedings o0-7695-1874
‘Pay-per-use’ Concept in Healthcare: A Grounded Theory Perspective Abdullah A. Akbar
University Of Leeds, Leeds, U. K
Abstract Healthcare organizations worldwide are faced with the growing challenge of introducing structural and technological reforms and cost-effective IT solutions that will transform the traditional structure of healthcare provision. Current technological developments have shed optimistic light on the future of IT in healthcare. This paper introduces ‘Pay-Per-Use’ concept in healthcare delivery services, which could prove appropriate for a small country like the State of Kuwait. The research question is directed towards the appropriateness and usefulness of such a concept. The need for effective and efficient healthcare delivery services in health organizations implies the need to establish a healthcare paradigm that is investment,communication,technology, platform,database,application - indepen- dent. The Grounded Theory (GT) forms the basis of the new concept, using a social context and referring to a typical clinical scenario. The social process fundamental to GT provides a specific and systematic approach to understand medical work and network of relationships among healthcare entities. Interpretations and analysis of data in the social context facilitates clearer understanding of concepts and categories and enables the formulation of a theory and a model architecture. The State of Kuwait is a typical example of a small country that is fast advancing in IT, where the new concept can be put to the test within the required infrastructure for the development of a beneficial healthcare delivery system in the country.f the 36th Hawaii International Conference on System Sciences -5/03 $17.00 © 2002 IEEE
1. Healthcare Delivery and IT National healthcare delivery in most countries has come under strong and growing stresses to institute major structural reform. While conditions vary in different countries, the source of these stresses is remarkably common across most nations, being primarily generated by external demands from demography, technology and the economy (Wolvaardt,1998). Those responsible for provision of healthcare understand that it is possible to enhance the quality of patient care and the cost-benefit balance by the effective introduction of inform-ation technology (IT), which will ultima tely transform the traditional structure of healthcare provision (Sosa and Levett, 1995; Warner, 1998). In recent years, two noticeable areas of growth in the computer industry have been the number of distributed applica-tions being shared using multi-databases which typically integrate information from pre-existing, heterogeneous local databases in a distributed environment and present global users with transparent methods to use the total information in the system; and the rapid growth in the area of telecommunications (Kim, 1995). The Internet has great potential to enhance peoples' health by developing communications and improving access to information for care providers, patients, health plan administrators, public health officials, biomedical researchers, and other health profession-als (Sosa et al., 1998). The emergence of the Internet, Intranet, Extranet as preferred communication vehicles makes it possible for healthcare providers to access laboratory results, X-ray and medical records via the World Wide Web (Deluca and Enmark, 2001).
(HICSS’03)

Proceedings0-7695-18
However, solutions to the problems of security, integrity, legality and ethical issues could become critical barriers to realising the objective of the global provision of healthcare (Deluca, 2000). 2. Emerging Problems in Healthcare The poor state of current paper-based medical records and the difficulty of recovering information from disordered documents have posed several problems not only for the healthcare providers but also for researchers, administrators, insurance companies and other third parties who could benefit from having more direct access to patient data (Ball and Collen, 1992). More often than not, it is argued, the current medical record is messy, incomplete, and the terminology used is vague and interpretable in many ways. In the words of Bleich and Lawrence, “The medical record is an abomination. ... it is a disgrace to the profession that created it. The charts confuse rather than enlighten; they provide a forbidding challenge to anyone who tries to understand what is happening to a patient” (Bleich and Lawrence, 1993). Ideally, it is argued, a medical record both supports the physician's clinical problem solving and serves as a ‘repository of information’ for use by multiple parties. It should guide the physician's thought processes towards ‘an efficient, scientific problem-solving method’ and allow for quick, efficient access according to widely diverging needs (Dick et al, 1997). To satisfy these requirements, many authors discuss the necessity to standardize terminology, to restrain the use of ‘free text’ or to automatically code the free text portions. In this way, the building blocks of medical thinking can be delineated and ordered. The record needs to be structured so that bits of information can be recognized by the computer as belonging, for example, to a single class or as standing in a distinctive type of relation (e.g. ‘request’ and ‘response’) (Shortliffe and Barnett,
of the 36th Hawaii International Conference on System Sciences74-5/03 $17.00 © 2002 IEEE
1990; McDonald and Barnett, 1990; Rector et al., 1991, 1993). Healthcare information systems need to be supported by security, integrity and legality for the successful transmission of information and for easy and reliable accessibility by those who need them. 2.1 Challenges of the Electronic Health Record Information management, both administrative and clinical, is critical in today's healthcare environment. Physicians are challenged to increase productivity and simultaneously improve the quality and reduce the cost of the care they provide. Electronic Patient Health Records (EPHRs) are information tools ideally suited to help physicians meet these challenges (Dick et al, 1997;Yamazaki and Satomura, 2000). EPHRs supplement traditional paper-based medical records with computer-based functions for the acquisition, processing, display, and reporting of clinical and related administrative data. The overall prospect of storing health information in electronic form raises concerns about standards, patient privacy, confidentiality of data and security (GMC 1995; Anderson, 1996; Berry, 1997; Pronkin and Shifrin, 1999; Bourka et al, 2001). If the concerns are not sufficiently addressed, they can discourage healthcare organisations from exploiting IT, and the healthcare consumer will be hesitant to share information (Zelmer, 1995; Drucker, 1999). Several major impediments remain as barriers to the full implementation of EPHRs. These impediments include the lack of standards that define complete infrastructure inter-operability among different healthcare information settings, lack of agreement on the data sets and code sets that make up the content and structure of the EPHR applications, lack of standards to ensure data quality and completeness in one operational integra-
(HICSS’03)

Proceeding0-7695-18
tion architecture, and lack of national legislation in several countries to protect adequately the privacy of health records. Even though these impediments have not been completely overcome on a local or national basis, the requirements of a mobile international society are already starting to demand the need for a framework for a global EPHR. Today, healthcare delivery is not just restricted to the local hospitals and doctors. Medical expertise is global and the patient can now be diagnosed and treated by a team of doctors distributed globally, yet all contributing collectively to patient healthcare delivery. This new healthcare delivery mechanism necessitates the global availability of the patient’s health information. 3. Research Objectives The major objectives of the research described here are: to propose a conceptual IT solution to growing healthcare problems, which is suitable for healthcare system of a country such as State of Kuwait; to set the basic framework wherein the concept can be applied; to identify and interpret a suitable model and delineate the architecture that suits the proposed concept; and, finally, to demonstrate the future implications of the concept with reference to Kuwait’s healthcare. Therefore, the focus of the research is to address the question: Can the pay-per-use concept allow easy and international access to electronic patient record and is it an appropriate approach for Kuwait’s healthcare? The research considers the benefits and the impact of the pay-per-use concept in healthcare delivery. The research seeks to address the following requirements and challenges in health care delivery: accessing to patient health records anywhere with security; delineate a system architecture that allows authorities to update healthcare systems, permits selection and deployment of the best available
atwiTiwpr 4Tcca‘iccpmp‘w‘bomcwaarHsatedohawwaep(ht
s of the 36th Hawaii International Conference on System Sciences (74-5/03 $17.00 © 2002 IEEE
pplication and facilitates maintaining he patient health record information ith security utilising an independent
nfrastructure on a ‘pay-per-use’ basis. o address the stated objectives, it is
mportant to understand medical work ithin a social setting, which in turn rovides a realistic approach to the esearch problem.
. Significance of Scenarios he medical record is a tool, and a rucial one at that, aiding memory, ommunication, and so forth but it is not ‘mirror’ of that work. It does not represent’ the work, but it ‘feeds into’ t, it structures and transforms it in omplex ways: it structures the ommunication between healthcare ersonnel, shapes medical decision aking, and frames relations between
ersonnel and patients. Recent studies of thinking-in-action’ have shown that hat we often consider to be
intellectual tasks’ in fact often appear to e highly embodied activities, in which ngoing interactions with the immediate aterial and social surroundings play a
rucial role (Clancey, 1995). Medical ork is essentially a social process and
n interactive activity. The unit of the nalysis should therefore be the process ather than the data. ealthcare scenarios typically depict
equence of distinct actions that ccomplish a particular task and detail he chain of interactions performed or xperienced by healthcare experts. They escribe one or more episodes or events f the healthcare disciplines. They ighlight goals suggested by the ppearance and behaviour of the system, hat people try to do with the system; hat procedure are adopted, not
dopted, carried out successfully or rroneously, and what interpretations eople make of what happens to them Carroll, 1999). The use of scenario in uman-computer interaction work seeks o describe and direct the appearance,
HICSS’03)

Proceeding0-7695-18
operation, and application of technology and its consequences for people, organizations, and their practices. They have been used to generate requirements, detect ambiguities in requirements, uncover missing features and incon-sistencies among specified features, verify and validate requirements, and integrate analysis of functional and non-functional, or ‘quality,’ requirements, such as security, safety, reliability, portability, and cost (Carroll 1999). They emphasize qualitative descriptions of human activity, directly engaging the laws of the social and behavioural sciences – our knowledge of what people need to do and wish to do, what they are most likely to do, how they will go about doing it, what they are most likely to recall or forget, what sorts of errors they are most susceptible to make, and so forth. A realistic artificial clinical scenario cited in this research makes useful interpretation of explanatory reference to architecture see figure 1. This will enable stakeholders to judge whether or not the architecture is a socially embedded process by which actors make sense of their situation. Patient visits and the eventualities form the episode. A retrieved record is ‘event-driven’ not ‘content-driven’ because of the different structure of the content in each discipline. Hence, the same scenario can be applied to various disciplines and thus prove the internal and external validity. A scenario can be broadened to include national and international boundaries. Therefore two concepts are derived from each intervention (visit #, event #): one that constitutes the electronic patient health record content management for each episode; the other that promotes global access where heterogeneous database and different standards and structures are encountered. Then the relationships among concepts that ‘ground’ the information architecture model which will form the basic
twt 5TmGteGoToTsadAiiuHUAp`qoaaGtcsagactibadtsaco
s of the 36th Hawaii International Conference on System Sciences 74-5/03 $17.00 © 2002 IEEE
echnology for using the ‘pay-per-use’ ithin ‘investment- independence’
heory.
. Grounded Theory (GT) Approach o understand the ‘sociality’ element in edical and IT work, we put forward the T method as an appropriate theoretical
ool for investigation and for the xplanation of the research process. laser and Strauss (1967) were the riginal proponents of Grounded heory, which led to the development f the discovery of the empirical theory. he method is grounded in social ettings and is based on the collection nd analysis of qualitative data eveloped by Glaser and Strauss (1967). lthough the method dates back to 1967,
ts use in Information Systems research s very recent. Useful summaries of the se of GT in IS research can be found in ughes and Howcroft (2000) and rquhart (2001). ccording to the method, conceptual roperties and categories may be discovered' or generated from ualitative data by following a number f guidelines and procedures where the im is to indicate the importance of the ctors in the social setting. T proceeds with two analytical
echniques - theoretical sampling and onstant comparison. The theoretical ampling in GT is theory-driven. Strauss nd Corbin (1998) emphasize that the rounds that determine which events, ctivities, or people require further data ollection are analytic grounds based on he emerging theory. As each new ncident or concept emerges, it needs to e compared against existing concepts nd categories for both similarities and ifferences. The research utilises heoretical sampling of a typical clinical cenario and undertakes comparative nalysis of emerging technologies and hallenges and provides an interpretation f a theory that forms the basis of an
(HICSS’03)

Proceedings 0-7695-187
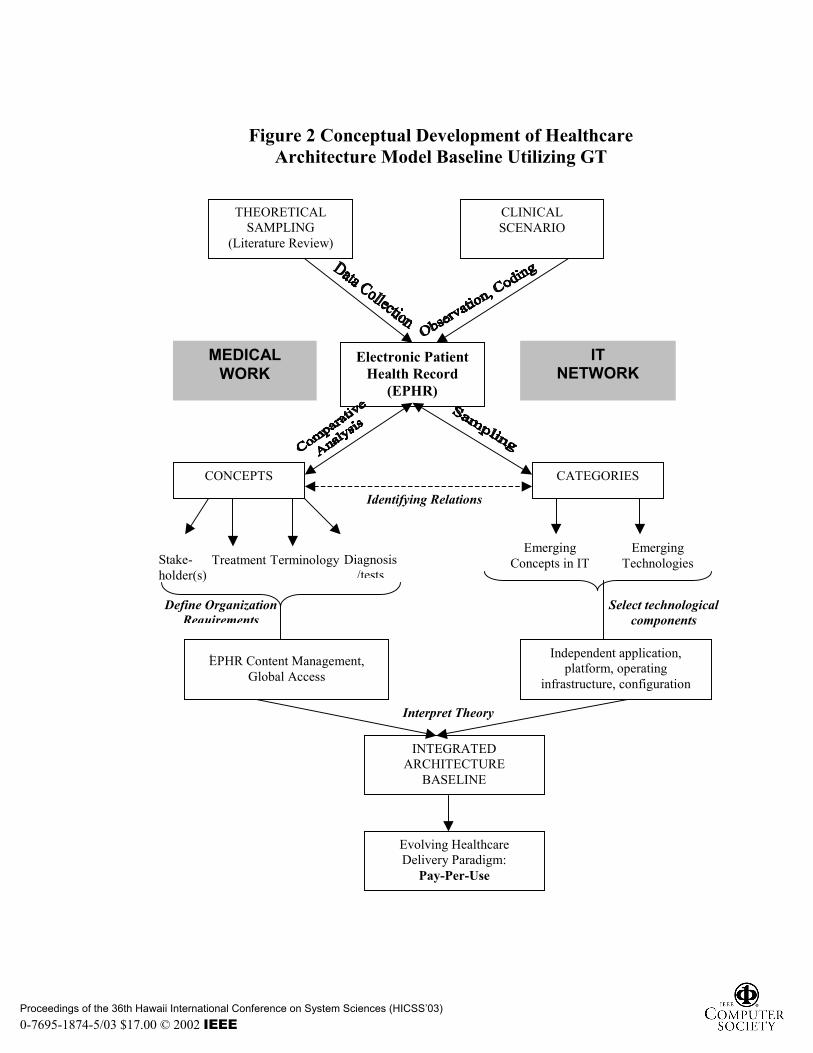
information architecture model suitable within the pay-per-use concept. The GT method enables understanding of the complexity of healthcare delivery and its relationships within the context of ‘sociality’. It implies a relationship view of health markets, which means that it is concerned with relationships between health institutions over time, rather than single exchange episode and transaction. Assuming such a relationships view to be an important empirical phenomenon in healthcare delivery system, Grounded Theory explicates these relationships by adopting a process perspective as opposed to a unit perspective. this is done by taking a social, psychological level of analysis and by defining the research problem from the perspective of the focal actor. It further leads to the assumption that that business takes place in a network setting where different business actors are linked to each other through direct and indirect relationships (as the definition of integrated delivery networks, systems (IDN / IDS). The network of relationships is the unit of analysis, not the individual firm (Forsgren and Johanson, 1992). Indeed the emphasis on connection is important because networks emerge and develop as a consequence of interactions. Relationships form the context in which interactions take place. Thus, grounded theory explicates these relationships by adopting a process perspective as opposed to a unit perspective. Refer to figure 2. for the whole process. 6. Pay-Per-Use Concept In the current rapidly moving technological environment, healthcare organizations that aspire to stay ahead of the technological curve, are in need of cost-effective and powerful applications that can improve the cost of care and overall enterprise performance without requiring huge capital investments. To
sicmtop‘tSFauucahrtoawmsabohiii 6IAsosacrmioaahtic
of the 36th Hawaii International Conference on System Sciences4-5/03 $17.00 © 2002 IEEE
erve that purpose, a new concept is ntroduced called ‘Pay-per-use’. This oncept, which will be of interest to ost healthcare organizations, is similar
o a rental service, in which rganizations pay for what they use for a eriod of time via the Internet. This Pay-per-use’ is accessed by users as per heir needs, to accomplish a given task. o, it has several value added benefits. irst, healthcare organizations that ccess applications through ‘Pay-per-se’ typically pay only for what they se, not for unused time. There are no ostly software contracts to maintain, nd upfront costs associated with large ardware and software deployments are educed. As ‘Pay-per-use’ will act as the echnical services department of an rganization, the need for experienced nd highly paid technical staff to deal ith installing, operating and aintaining applications is diminished
ignificantly. The concept will assist the dministrative processes and prove eneficial to healthcare organisations. In rder to implement the concept, the ealthcare delivery industry requires an nfrastructure that is ‘investment-ndependent’ with respect to the EPHR nformation asset management.
.1 Independent Information nfrastructure n independent information infra-
tructure allows a healthcare rganization to procure all the relevant ervices viz., the technology, pplication, data storage and ommunication services from the espective vendors with relatively inimal capital investment. This
nfrastructure would facilitate the rganization to procure these services on ‘pay-per-use’ basis. Today, the internet rchitecture and the Word Wide Web ave laid the foundations for enabling he ‘investment-independent’ nformation infrastructure for the health are industry. Distributed database and
(HICSS’03)

Proceedings o0-7695-1874
data management services are available from service providers. These applications also use the software technology, like Java, that can run on all hardware platforms under various operating systems. This enables ‘platform-independence’ for the health care organizations. The applications also share data among various distributed databases using the database connectivity standards, like ODBC, IIOP, and CORBA etc. All these applications are now available to run from a simple ‘web browser’ from anywhere on a personal computer that connects to the Internet. Communica-tion and Internet services are available on subscription basis. This provides the basis for ‘database independence’ and ‘communication technology indepen-dence’. The vendors for the ‘enabling software’ and applications are now supporting ‘application-independent’ data formats (XML). Industry standards have been set to define this ‘application-independent’ data definition and manipulation needs. With this, an application for a specific purpose, from vendor X, will be able to read/write data in a common format and exchange data. Organizations now are inclined to switch their vendors for applications according to their business needs. Healthcare service is now not bound by the application system and its vendor but is driven by competition among ‘applica-tion system developers’ and service providers for better information management. 7. Health Information Architecture Having provided a comparative analysis of concepts and categories within medical scenarios, the GT method enables interpretation of the model architecture for use within pay-per-use. The scenario-derived elements which focus on EPHR content management are: patients, healthcare service providers, healthcare delivery organiza-
tesdeto,mdthdhc Ssa(facit‘dai(usafceasfppdiabpms
f the 36th Hawaii International Conference on System Sciences -5/03 $17.00 © 2002 IEEE
ions, healthcare sponsors (Government .g. Ministry of Health) as well as events uch as patient visits, health problems, iagnoses, orders for tests or operations tc, references to other specialists, reatment, test results from service rders. Additionally, Images, audio video clips, multi-media attachments,
edical fields (Paediatrics, Orthopae-ics, Radiology etc.) that have unique erminology and vocabulary used in ealth record management for problems, iagnosis, results, inference, treatment ave significant relevance and ontributions to EPHR.
ocial theory also enables the setting of tandard requirements for global EPHR ccess, namely, functional independence different record management featured or different medical fields); the pplication chosen to manage data ontent for patient health record (PHR) n a field; the choice of ‘best-of-breed’ echnology (by sponsor) to promote application - independence’; universal ata manipulation formats used by pplications to facilitate ‘data - ndependence’; data storage definitions the choice to store data anywhere) to be sed by applications to promote ‘data torage independence’ (able to store data t locations of choice). The stated eatures promote ‘platform, onfiguration, machine independence’; nable application access definitions to llow authorised persons to access ecure data of a patient health record rom all storage locations; data resentation to healthcare service roviders (HSPs) to access and record ata in different relevant formats (text, mages, audio, video, charts, numbers in ccessible formats) using simple, thin rowser clients; and the merging of atient health data (PHD) from various edical centres, stored in distributed
torage locations.
(HICSS’03)
Proceeding0-7695-18
The baseline for a model health information architecture is described as follows:
• For health care organizations (sponsors), healthcare delivery is the ‘core’ paradigm business and ‘not’ healthcare systems development, maintenance. Hence, health organizations demand application investment-independence.
• Easy-to-use patient health record management software in each specific healthcare area is deployed in a ‘Pay-per-use’ model.
• Processed health record data is stored at an information service provider’s facility in a ‘portable format’ on a ‘Pay-per-data storage’ basis and accessible always.
• Health service providers access and manage patient health records using a simple workstation with a browser.
• Health care sponsors select the application software to be used for each area.
• Health care sponsors defines a ‘portal’ through which authorised health care service providers can manage patient health records .
• The Portal authenticates each user access, deploys all ‘applications’ currently in use for various medical disciplines.
• When an authorised practitioner accesses the portal and (s)he is directed automatically to use the relevant software to record, access, store patient health record information.
• The selected application aided by the portal provides a single logical collection of all components of the patient health record covering medical history by visit and allows additional
s of the 36th Hawaii International Conference on System Sciences74-5/03 $17.00 © 2002 IEEE
updates to the patient's health record.
• The selected application software saves the patient health record (PHR) details in a universal format (e.g. XML) in storage areas directed by the set up established by the healthcare sponsor(HCS). This establishes the ‘Data Independence’ and ‘Data Storage or Configuration Independence’ (a vision for the future).
8. Discussion This paper focuses on social process in medical work and IT network to explicate the investment-independent theory within pay-per-use concept. It delineates a model of standards for healthcare information, network and communication while maintaining that the proposed concept is a theoretical development, in view of an evolving technological environment in modern times. The ‘open’ information system is itself an evolving concept for evolving problems in healthcare delivery and is subject to further studies and development. The ‘sociality problem’ in the information architecture model in the healthcare delivery system stems from its interdisciplinary roots. Indeed, when we consider the numerous interdependent links such as technology, knowledge, social relations, administra-tive routines and systems and legal ties, components from different disciplines are difficult to integrate because they come encumbered by values, meanings and associations that often remain immiscible. Grounded theorists’ distinction between process and unit is that researching units are generally concerned with developing static descriptions, whereas processes are conceptually developed to account for behaviour as it occurs over time. Hence,
(HICSS’03)

Proceeding0-7695-18
in assuming a process orientation dynamic, cross-contextual properties of behaviour can be uncovered. The complexity and interdependency of business relationships can be understood and explained by taking processes as the unit of analysis. The grounded theory approach provides a specific and systematic approach to the study of process. This notion of a generic process orientation addresses the ‘sociality problem’. The problem of attempting to integrate components from other disciplines is not a problem for the grounded theory method, as those concepts are only allowed as data and if they do not 'fit' the emerging codes and categories they are rejected. Grounded theorists claim that the key to their method is that the data should fit the theory, not the other way around. Finally, the GT methodology incorporates the assumption that the actors under study have their own perspectives, are able to interpret these and those of others and they get incorporated into the researcher's own interpretation. The theory evolves through a continuous interplay between analysis and data collection; however, this redefining involves interpretative work and grounded theorists accept responsibility for their interpretative role. While multiple prospective are systematically sought during the research process, the emerging theory are interpretations made of the data and all interpretations are temporarily limited judgements that can be made about the soundness or probable usefulness of the theory (Strauss and Corbin, 1994, 1998). Since the nineties, Kuwait like many other states has made tremendous progress in the field of IT. The growth of internet technology has been very rapid and has taken a place of dominion in most work places. Similarly, the health sector has also shown several transitions that have brought about useful
s of the 36th Hawaii International Conference on System Sciences 74-5/03 $17.00 © 2002 IEEE
transformation in administrative tasks, such as the increased use of computer records for management purposes. However, high rise in the demand for quantity and quality of health services and the costs of implementing IT utilities have posed problems in the health sector with difficulties in providing sufficient local resources and experience with knowledge to invest in IT. Based on an empirical research, Khalfan et al (2001) pointed out that shortages of IT skills in Kuwait, as an example of a developing country, has always been problematic (Khalfan and Gough, 2001). IT skills are an important ingredient for IT diffusions and assimilation. To overcome such ‘serious’ problems different organisations tend to adopt different strategies. This paper proposes ‘pay-per-use’ concept as an alternative option that can prove to be beneficial for a small country like the State of Kuwait. 9. Conclusion ‘Pay-per-serve’ concepts open for us a ‘investment-independent technology’ theory. The phenomena of technology evolution will no longer frighten healthcare authorities from investing in technology that may become obsolete. If health informatics is really to serve people and their health, attention needs to be given to deploy a National Patient Health Information System. Only then will shared information and record system linkage become super highway of knowledge between patient and their supporting professionals. The relationship between concepts and categories will be a template for any healthcare institution having lack of expertise to develop such system and a constrained budget. Mapping the complex everyday reality of the area under investigation into the scenario domain will result in well-constructed model or framework. One of the features of Grounded Theory is that it represents the complex everyday reality of the area
(HICSS’03)

Proceedings 0-7695-187
under investigation (Strauss and Corbin, 1990). References: Anderson, R. J. (1996), “Security in Clinical Information Systems”, BMA, London.
Ball, M. J and Collen, M (1992), Aspects of the computer-based patient record. New York: Springer.
Berry, R. M (1997), “The Genetic Revolution and the Physician's Duty of Confidentiality. The role of the old Hippocratic Virtues in the Regulation of the New Genetic Intimacy”, J. Leg. Med., Vol. 18(4): pp: 401-441, PMID: 9433035.
Bleich, H. L and Lawrence, L (1993), “Weed and the Problem -Oriented Medical Record.” M. D. Computing, vol. 10, pp: 69-71
Bourka, A., Polemi, N. and Koutsouris, D. (2001), “An Overview in Healthcare Information System Security”, In: Patel, V. L., Rogers, R. and Haux, R (eds.) Proceedings of the Tenth World Congress on Medical Informatics (MEDINFO '2001), IMIA Canada
Carroll, J. M. (1999), Five reasons for scenario-based design. In Proceedings of the 32rd Annual Hawaii International Conference on Systems Sciences Los Alamitos, CA: IEEE Computer Society Press.
Clancey, W. L (1995) “The Learning Process in the Epistemology of Medical Information”. Methods of Information in Medicine. vol 34, pp: 122-130.
Deluca, J. M (2000), “The Ethics of E-commerce”, Health Forum Journal, Vol. 43(3), pp: 28-35, San Francisco.
Deluca, J. M. and Enmark, R (2001), “The Latest Revolution” Health Forum Journal, Vol. 44(1), pp. 22-25, San Francisco.
Dick, R. S., Steen, E. B., and Detmer, D. E. 1997. The Computer-Based Patient
of the 36th Hawaii International Conference on System Sciences (4-5/03 $17.00 © 2002 IEEE
Record.. An Essential Technology For Health Care. Washington, D.C.: National Academy Press.
Drucker, P. (1999), “Management Challenges for the 21st Century”, Harper Business Press, New York.
Forsgren, M and J Johanson (1992), "Managing Internationalisation in Business Networks", in Managing Networks in International Business, p 1 - 15.
Glaser, B. G. and Strauss, A. (1967) The Discovery of Grounded Theory: Strategies for Qualitative Research, Aldine, New York.
Glaser, B. G. and Strauss, A. (1967) The Discovery of Grounded Theory: Strategies for Qualitative Research, Aldine, New York.
GMC (1995), “Confidentiality and Good Medical Practice”, London: General Medical Council.
Hughes, J. and Howcroft, D. A. (2000), “Grounded Theory: Never Knowingly Understood”, Information Systems Review, 4(1), pp:181-197.
Khalfan, A. and Gough, T.G. (2001), “Vender Selection Criteria and Post-implementation Evaluation Practices for IS/IT Outsourcing: A Case Study of a Developing Country”, Seventh European Conference on IT Evaluation, September, Dublin, Ireland.
Kim, W. (ed.) (1995), “Modern Database Systems: the Object Model, Interoperability, and Beyond”, ACM Press, New York, Addison-Wesley.
McDonald, C. J and Barnett, G. O (1990) “Medical-Record Systems”, In: Shortliffe, E. H and Perreault, L. E (eds). Medical Informatics. Computer Applications in Health Care. Reading, MA: Addison-Wesley; pp: 181-218.
Pronkin, M. A and Shifrin, M. A (1999), “Security for Electronic Patient Record System”, In: Kokol, P., Zupan, B., Stare,
HICSS’03)

Proceeding0-7695-18
J., Englbrecht, R. and Premik, M. (eds.) Medical Informatics Europe ‘99 Bridges of Knowledge, IOS press, Ohmsha.
Rector, A. L., Nowlan, W. A. and Kay, S (1991) “Foundations for an electronic medical record”. Methods Inf. Med. vol 30, pp: 179-86.
Rector, A. L., Nowlan, W. A., Kay, S., Goble, C. A.and Howkins, T. I (1993) “A framework for modelling the electronic medical record”. Methods Inf. Med., vol 32, pp: 109-19.
Shortliffe, E. H and Barnett, G. O (1990) “Medical data: Their Acquisition, Storage, and Use”, In: Shortliffe, E. H and Perreault, L. E (eds). Medical Informatics. Computer Applications in Health Care. Reading, MA: Addison-Wesley; pp: 37-69.
Sosa, M. and Levett, J. (1995), “The Information Society: Why Europe and Develop Countries should boost Partnership in Health Knowledge transfer”, Health Information society and developing countries, IOS Press, (Netherlands).
Sosa-ludiciss, M et al (eds.) (1998), “Internet, Telematics and Health” IOS Press, Ohmsha.
Strauss Anselm and Juliet Corbin (1994), Grounded Theory Methodology: An Overview, in N.K. Denzin and Y.S. Lincoln (eds.), Handbook of Qualitative Research, Sage Publications, London, 273-285.
Strauss, A. and Corbin, J. (1990), Basics of Qualitative Research: Grounded Theory Procedures and Techniques, California: SAGE Publications, Inc.
Strauss, A. and Corbin, J. (1998) Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory, Sage, London.
s of the 36th Hawaii International Conference on System Sciences74-5/03 $17.00 © 2002 IEEE
Urquhart, C. (2001) “An Encounter with Grounded Theory: Tackling the Practical and Philosophical Issues”, in: Trauth, E. (ed), Qualitative Research in Information Systems: Issues and Trends, Idea Group Publishing, London.
Warner, David (1998), “The Globalization of Medical Care”, in Zarrilli, S. and Kinnon, C. (eds) International Trade in Health Services: A Development Perspective, UNCTAD and WHO, Geneva.
Wolvaardt, Gustaaf (1998), “Opportunities and Challenges for Developing Countries in Health Sector”, in Zarrilli, S. and Kinnon, C. (eds) International Trade in Health Services: A Development Perspective, UNCTAD and WHO, Geneva.
Yamazaki, S., Satomura, Y (2000) ‘Standard Method for Describing an Electronic Patient Record Template : Application of XML to Share Domain Knowledge,’ Method Inform Med, Vol.39 No.1 p50-55
Zelmer, J. L (1995), “Informatics and Health Care Reform”, In: Greenes, R. A., Peterson, H. E., and Protti, D. J. (eds.) Proceedings of the Eighth World Congress on Medical Informatics (MEDINFO '95), IMIA Canada.
(HICSS’03)

eedMAK HospitalVisit#4-Event#6
H URL:ceptionogram(
AK) Waheed
Dr.MusaVisit#4-Event#7
MOHURL:
Orthopaedics
ration
6
7
Operation Theatre
MOHURL:
Orthopaedics
Operations
Dr.MusaVisit#5-Event#8
8
MOHURL:
Orthopaedics
Dr.MusaVisit#5-Event#9
9
Pharmacy(Visit#6-Event10)
10
MOHURL:
Pharmacy
a
2
Proceedings0-7695-187
Figure1
Farwaniya clinic(Visit#1-Event#1)
Dr.John Sullivan(Visit#1-Event2)
Electronic Patient HealthRecord
MOH URL:ReceptionProgram
MOH URL:GeneralMedicine(Clinic)
Waheed Waheed WaheedRadiologist- Visit#2-Event#3
MOH URL:Radiology
Visit#1
Visit#1-Event2details
Visit#2-Event3detailswithXrayimage
MOH URL:ReceptionProgram
MOH URL:GeneralMedicine(Clinic)
Waheed Farwaniya clinic(Visit#3-Event#4)
Waheed
Visit#3
Dr.John Sullivan(Visit#3-Event5)
Visit#3-Event5details(referraltoOrthopaedic)
Wah
MORePr
M
Visit#4
Visit#4-Event7 Operequest
1 2 3
4 5
Operation detailsDr.MusaVisit#5-Event#8
Operation detailsDr.MusaVisit#5-Event#8
Pharmacy drugs (Visit#6-Event10)
Waheed
MAK Hospital(Visit#7-Event#11)
11
MOH URL:ReceptionProgram(M
AK)
Visit#7
Dr.MusVisit#7-Event#1
12
MOHURL:
Orthopaedics
Waheed is OK(Visit#7-Event#12)
Scenario forArchitecture
of the 36th Hawaii International Conference on System Sciences (HICSS’03) 4-5/03 $17.00 © 2002 IEEE
Proceedings o0-7695-1874
Figure 2 Conceptual Development of Healthcare Architecture Model Baseline Utilizing GT
THEORETICAL SAMPLING
(Literature Review)
CLINICAL SCENARIO
CONCEPTS CATEGORIES
Electronic Patient Health Record
(EPHR)
Stake- holder(s)
Diagnosis/tests
Treatment Terminology
Identifying Relations
Emerging Technologies
Emerging Concepts in IT
INTEGRATED ARCHITECTURE
BASELINE
MEDICAL WORK
IT NETWORK
Interpret Theory
Evolving Healthcare Delivery Paradigm:
Pay-Per-Use
EُPHR Content Management, Global Access
Define Organization Requirements
Select technological components
Independent application, platform, operating
infrastructure, configuration
f the 36th Hawaii International Conference on System Sciences (HICSS’03) -5/03 $17.00 © 2002 IEEE