pathophysiology, diagnosis, and treatment amitabh k...
TRANSCRIPT

arcoidosis
Amitabh
K. Bharadwaj, Harvard Medical School, Year-IVGillian Lieberman, MD
Pathophysiology, Diagnosis, and Treatment
September 2000Amitabh K. BharadwajGillian B. Lieberman, MD
2
Fever of Unknown Etiology
• M. S. is a 52 yo white F with a history of scleroderma and cholelithiasis who presented with dry cough, shaking chills, and fevers to 102 F despite being put on amp/gent/flagyl
Amitabh K. BharadwajGillian B. Lieberman, MD

3
Chest film• There were no
abnormalities identified
BIDMC
Amitabh K. BharadwajGillian B. Lieberman, MD

4
In view of her significant presentation, a chest and abdominal CT were ordered.
• A chest CT showed mediastinal lymphadenopathy, and an interstitial reticulo nodular pattern predominantly in the upper lobes.
Mediastinal adenopathy
Interstitial markings Nodules
Chest CT
Amitabh K. BharadwajGillian B. Lieberman, MD
5
Ddx Upper Lobe Interstitial Process
• Silicosis• Sarcoid• Atypical PCP• Hypersensitivity Pneumonitis• Ankylosing spondylitis• Langerhans cell histiocytosis
Amitabh K. BharadwajGillian B. Lieberman, MD

6
Patient’s Abdominal CT
Abdominal CT showed: • 1.8 cm gallstone
without signs of cholecystitis.
• Multiple low- attenuation splenic lesions
BIDMC Low-attenuated splenic lesions8mm hepatic cyst(incidental finding)
Amitabh K. BharadwajGillian B. Lieberman, MD

7
Lung and spleen findings suggest Sarcoidosis. Splenic and lung
biopsies were obtained and showed non caseating
granulomata confirming the diagnosis of Sarcoidosis
Amitabh K. BharadwajGillian B. Lieberman, MD

8
The patient underwent a laporoscopic cholecystectomy
and splenectomy. Her fever and night sweats abated and she was
discharged without further treatment.
Amitabh K. BharadwajGillian B. Lieberman, MD

9
Follow up Chest X-ray• 4 mo later she came
back for outpatient f/u and her CXR showed she had developed hilar adenopathy
BIDMC
Bilateral hilar adenopathy
Amitabh K. BharadwajGillian B. Lieberman, MD

10
Repeat Chest CT• Mediastinal windows
showed:Hilar and mediastinal lymph node enlargement
Mediastinal(subcarinal)adenopathy
Hilar adenopathy
BIDMC
Amitabh K. BharadwajGillian B. Lieberman, MD

11
Repeat Chest CTLung windows showed:Numerous small sub-cm lungnodules bilaterally
Lung nodules
BIDMC
Amitabh K. BharadwajGillian B. Lieberman, MD

12
Chest findings are compatible with progression of stage 11
sarcoidosis
Amitabh K. BharadwajGillian B. Lieberman, MD

13
Sarcoidosis• F > M, 20-40 yo• United States: black > white 10:1 – 17:1• Europe: disease affects mostly whites• Chronic multisystem disorder of unknown etiology • Noncaseating granulomas in affected organs:
T lymphocytes and macrophages • Most frequently symptomatic organs:
– Lung 90%– Lymph nodes 75-90%– Skin/eye/liver 25% each– Bone marrow/spleen 15-40%– CNS/MS/heart 5% each
Amitabh K. BharadwajGillian B. Lieberman, MD

14
Disease Presentation• Most patients have some respiratory symptoms• Subacute sarcoidosis: 20-40%
– Fever, malaise, anorexia, or weight loss– +/- Dry cough, dyspnea, retrosternal chest
discomfort– Often self-limited
• Chronic sarcoidosis: 40-70%– Dry cough, dyspnea, or retrosternal chest
discomfort– +/- Fever, malaise, anorexia, weight loss– May progress to permanent lung and secondary
organ damage
Amitabh K. BharadwajGillian B. Lieberman, MD

15
Diagnosis
Required for diagnosis:• History / Physical exam• Negative blood tests and positive
pulmonary function tests• CXR indicative of sarcoidosis• Biopsy evidence of noncaseating
granulomatous process– lung parenchyma (usual site, via bronchoscopy)– hilar nodes, skin, conjunctiva, lip
Amitabh K. BharadwajGillian B. Lieberman, MD

16
Presentation of Pulmonary Sarcoid on Chest XRay
Amitabh K. BharadwajGillian B. Lieberman, MD
17
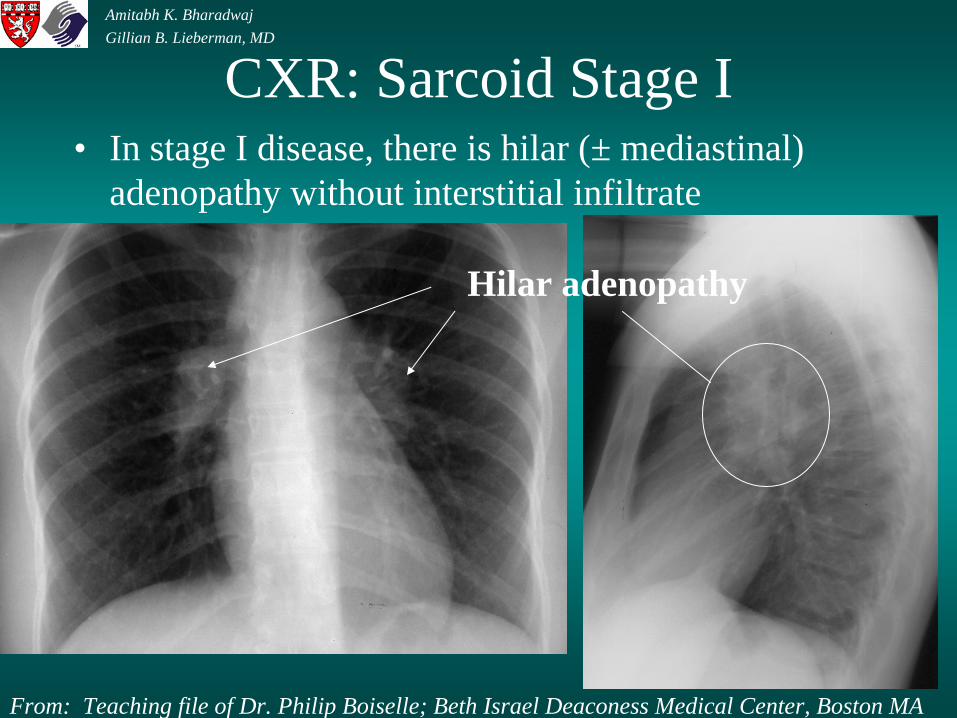
CXR: Sarcoid Stage I• In stage I disease, there is hilar (± mediastinal)
adenopathy without interstitial infiltrate
Hilar adenopathy
From: Teaching file of Dr. Philip Boiselle; Beth Israel Deaconess Medical Center, Boston MA
Amitabh K. BharadwajGillian B. Lieberman, MD

18
Differential for Hilar Adenopathy
• Tb - usually unilateral• Sarcoid - usually bilateral, symmetric• Fungal infection• Metastatic disease - especially renal, thyroid• Lymphoma/leukemia• Benign lymph node hyperplasia
(Castleman’s disease)
Amitabh K. BharadwajGillian B. Lieberman, MD

19
CXR: Sarcoid Stage II
• In stage II disease, hilar adenopathy is accompanied by interstitial infiltrate, which tends to be more prominent at the apices as in this patient
Apicalinfiltrate
Hilar adenopathy
From: Teaching file of Dr. Philip Boiselle; Beth Israel Deaconess Medical Center, Boston MA
Amitabh K. BharadwajGillian B. Lieberman, MD

20
CXR: Sarcoid Stage III• In stage III disease, hilar
LAN has disappeared and diffuse interstitial infiltrates remain
• Differential includes: CHF, lymphangitic spread of CA, infection (viral, mycoplasma), sarcoid, pneumoconiosis, collagen vascular disease
Diffuse interstitialinfiltrates
From: Teaching file of Dr. Philip Boiselle; Beth Israel Deaconess Medical Center, Boston MA
Amitabh K. BharadwajGillian B. Lieberman, MD

21
CXR: Sarcoid Stage IV
• Presents with fibrosis as in this radiograph
From: Loyola University - www.lumen.luc.edu/lumen/MedEd/Radio/Sarc/introxry.htm
Fibrotic bands
Amitabh K. BharadwajGillian B. Lieberman, MD
22
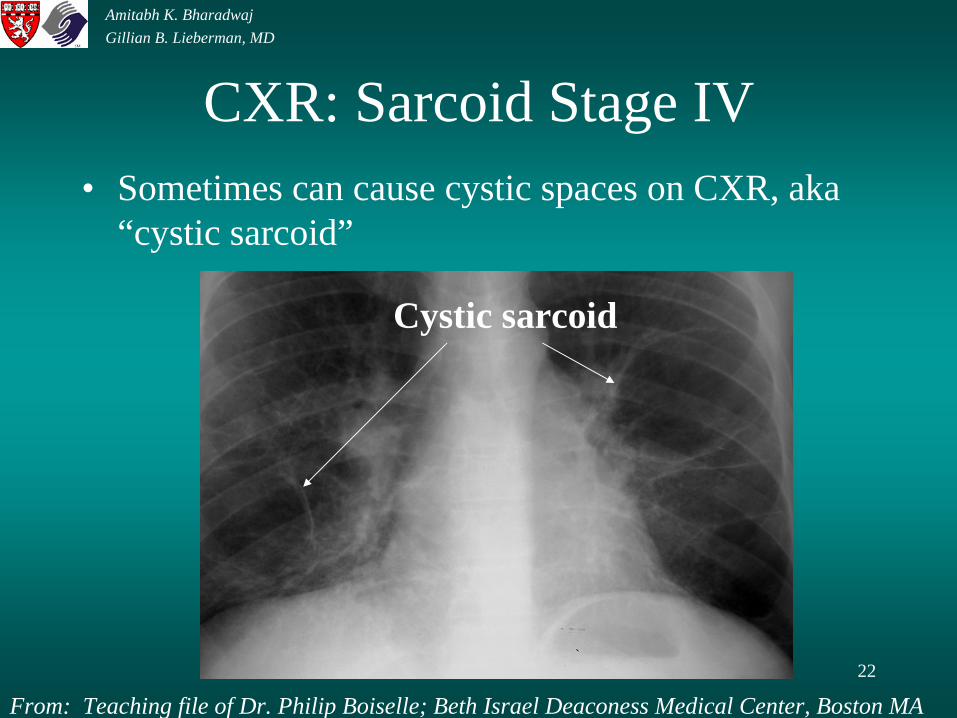
CXR: Sarcoid Stage IV• Sometimes can cause cystic spaces on CXR, aka
“cystic sarcoid”
Cystic sarcoid
From: Teaching file of Dr. Philip Boiselle; Beth Israel Deaconess Medical Center, Boston MA
Amitabh K. BharadwajGillian B. Lieberman, MD

23
Differential for fibrosis
• Collagen vascular disease (RA, scleroderma)• Sarcoid stage IV• Silicosis• Asbestosis• Hypersensitivity pneumonitis• Idiopathic fibrosis• Drug/radiation toxicity
Amitabh K. BharadwajGillian B. Lieberman, MD

24
Pulmonary Sarcoid on Chest CT
Amitabh K. BharadwajGillian B. Lieberman, MD
25
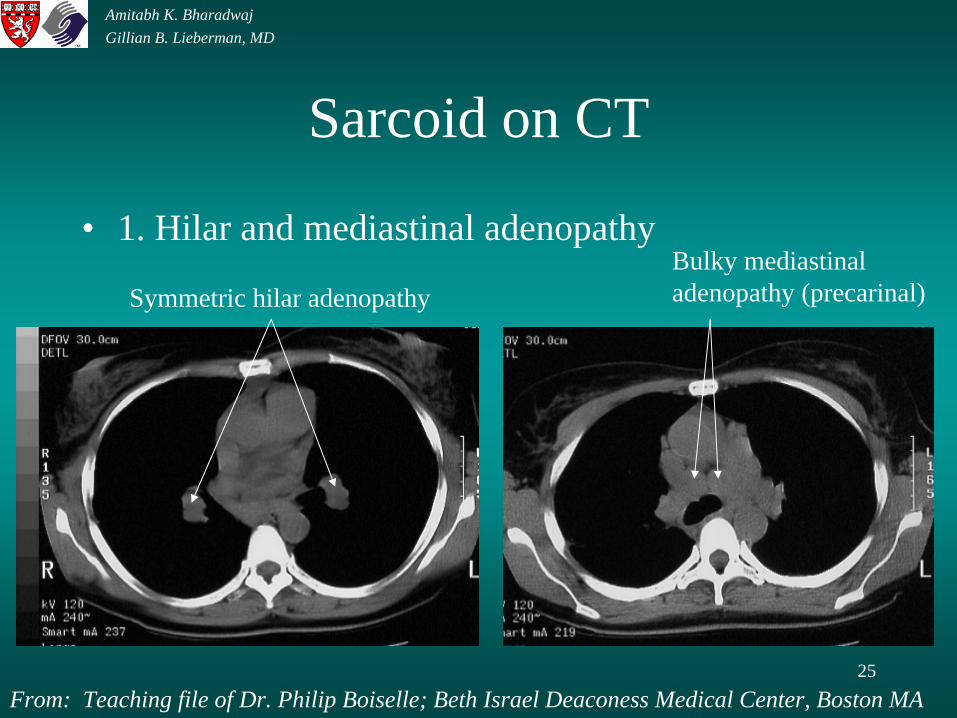
Sarcoid on CT
• 1. Hilar and mediastinal adenopathy
Symmetric hilar adenopathyBulky mediastinaladenopathy (precarinal)
From: Teaching file of Dr. Philip Boiselle; Beth Israel Deaconess Medical Center, Boston MA
Amitabh K. BharadwajGillian B. Lieberman, MD

26
Sarcoid on CT• 2. Interstitial markings and perilymphatic nodules
Perilymphatic nodules
Interstitial markings
From: Teaching file of Dr. Philip Boiselle; Beth Israel Deaconess Medical Center, Boston MA
Amitabh K. BharadwajGillian B. Lieberman, MD

27
Sarcoid on CT• 3. Fibrosis (end-stage)• “Honey combing”
From: Webb WR, Brandt WE, Helms CA. 1998. Fundamentals of Body CT. W.B. Saunders Company.
Amitabh K. BharadwajGillian B. Lieberman, MD

28
HRCT Findings in Sarcoid
• 1. Perilymphatic nodules, 1-10 mm, often subpleural, may calcify
• 2. Patchy, often asymmetric, distribution• 3. Upper lobe predominance • 4. Hilar and mediastinal LAN (not always;
may calcify)• 5. Ground-glass opacity (uncommon),
indicating the presence of small granulomas
Amitabh K. BharadwajGillian B. Lieberman, MD
29
Treatment of Sarcoidosis• Treat early - Permanent organ derangements are
not responsive to glucocorticoids• Oral prednisone• Repeat treatment protocol for reactivations • Other considerations
– inhaled glucocorticoids not efficacious– mild ocular disease: local therapy– uveitis: systemic therapy
Amitabh K. BharadwajGillian B. Lieberman, MD
30
References
• BIDMC, BIDMC Patient Care Radiology Files. 2000. Beth Israel Deaconess Medical Center, Boston MA. SLIDE#3, 4, 5, 7, 8, 9
• Boiselle, P. 2000. Personal teaching file, Beth Israel Deaconess Medical Center, Boston MA. SLIDE#13, 15, 16, 18, 21, 22
• Freiman DG. Pathology of Sarcoidosis. 1985. Semin Roentgenol 20:356-375. • Isselbacher K et al. 1994. Harrison’s Principles of Internal Medicine. McGraw-
Hill Publishing.• Loyola University Medical Education Network. 2000. Website address:
www.lumen.luc.edu/lumen/MedEd/Radio/Sarc/introxry.htm. SLIDE#17 • Miller BH, Rosado-de-Christenson ML, McAdams HP, Fishback NF. 1995.
RadioGraphics: 15:421-437. • Sanguinetti CM, Montroni M, Balbi B, Prete M, Gasparini S, Ross FA. 1987. Does
activity of pulmonary sarcoidosis depend on disease duration: a correlation between bronchoalveolar lavage, scintigraph, radiologic, and physiologic parameters and time of onset of disease. Sarcoidosis 4:18-24.
• Webb WR, Brandt WE, Helms CA. 1998. Fundamentals of Body CT. W.B. Saunders Company. SLIDE#19, 20, 23
Amitabh K. BharadwajGillian B. Lieberman, MD

31
Acknowledgements
Phillip Boiselle for his generous contribution of cases.Beverlee Turner for her efforts in making the final touches.
Amitabh K. BharadwajGillian B. Lieberman, MD
32
The End
Amitabh K. BharadwajGillian B. Lieberman, MD