parturition and foal neonatal care lacp pg. 163. average 335-340 days. variable- breed, season, sex...
TRANSCRIPT

Parturition and FoalNeonatal Care
LACP pg. 163
Average 335-340 days.
Variable- breed, season, sex of foal, plane of nutrition, fetal genotype
Gestation Length

Equine Gestation HormonesProgesterone/Progestogens
Progesterone initially rises, followed by a slight ↓ then ↑ to a peak at d 80, then gradually ↓ to 1-2 ng/ml during mid-late gestation (d 150).
Second ↑ associated with formation of accessory & secondary CL. Late gestation progesterone rises (last month of pregnancy)
Once embryo enters uterus, it migrates throughout the uterine body and both horns until 16-17d (becomes to big to pass through horn.
This migrations signals the dam that she is pregnant. (contacts endometrial surface repeatedly) FIXATION
Embryo – 40d Fetus – after 40d

60d-7 months- fetus develops slowly
(fetal organ development) 8 months- increase in size to about 60% of its
weight in the last 3 months.
Placenta
Placenta takes over progesterone production ~d 100 until foaling.
Complete placental formation is done at 150 days.
DAY 150 - Firm placental attachment

Placenta Attachment of placenta to endometrium begins
around day 40 of gestation and not complete until 120d.
Endometrial cups (day 25) fetal in orgin, form from girdle cells, and invade the dam’s endometrium . Forms horseshoe like ring of white cups. Produce ECG that stimulates CL to produce progesterone. Cups degenerate at day 70.
Loss after day 40- no return to heat for 3-4 months.

Epitheliochorial and noninvasive (materanal and fetal epithelium contact)
Attachement- diffuse in that the membranes are attached to all portions of the uterus with the exception of the cervix- no attachement
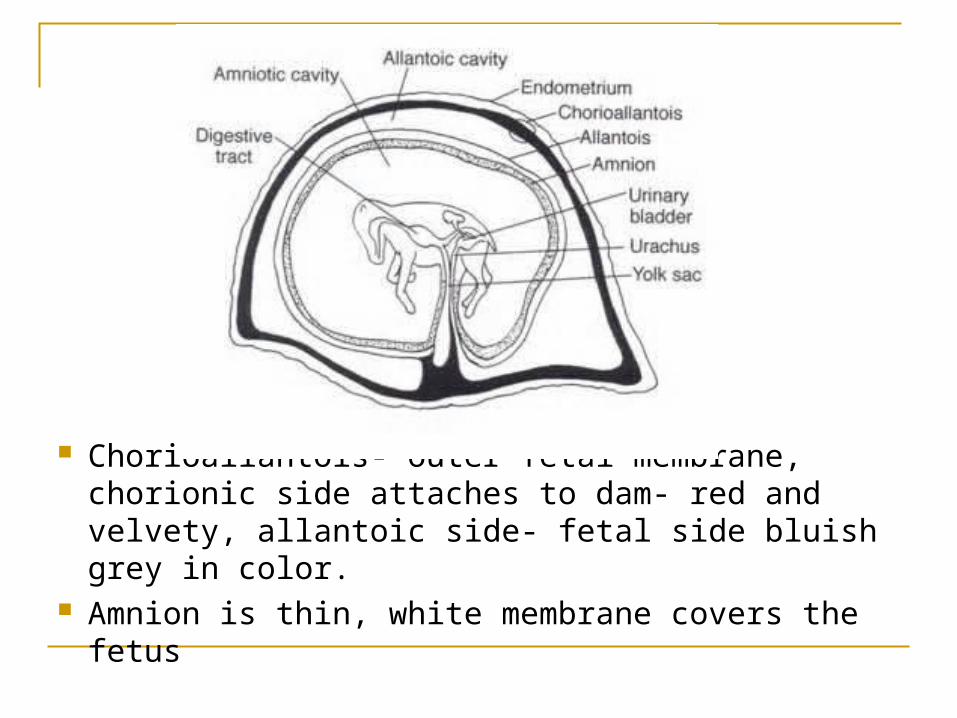
Chorioallantois- outer fetal membrane, chorionic side attaches to dam- red and velvety, allantoic side- fetal side bluish grey in color.
Amnion is thin, white membrane covers the fetus
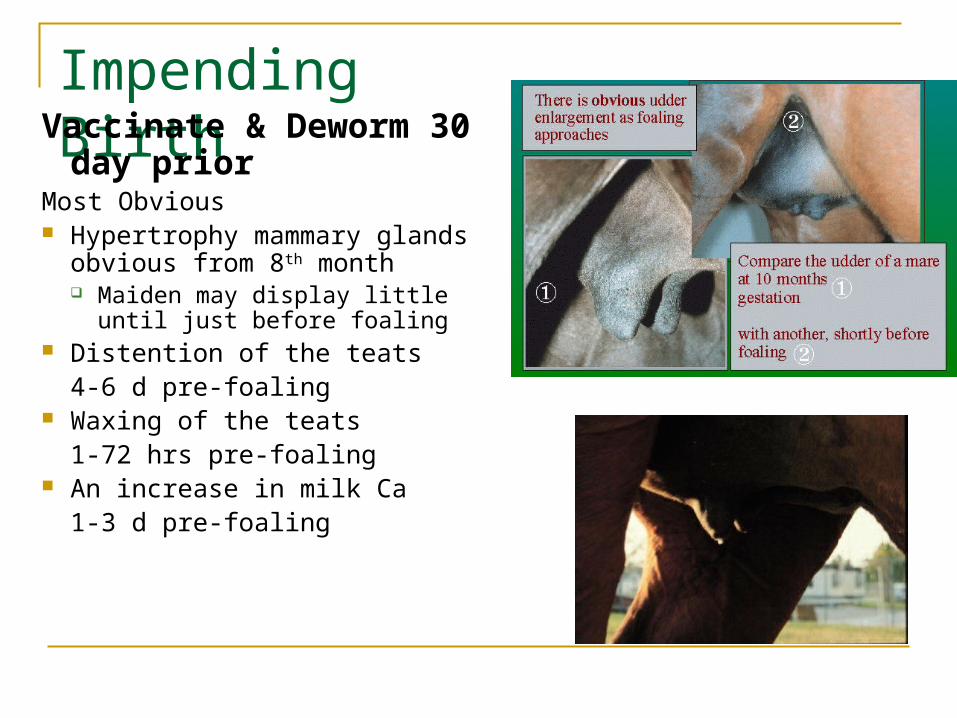
Impending BirthVaccinate & Deworm 30 day prior
Most Obvious Hypertrophy mammary
glands obvious from 8th month Maiden may display little until
just before foaling Distention of the teats
4-6 d pre-foaling Waxing of the teats
1-72 hrs pre-foaling An increase in milk Ca
1-3 d pre-foaling

Fescue Toxicity
Pull mare off fescue at least 1 month before foaling.
(endophyte-infected)
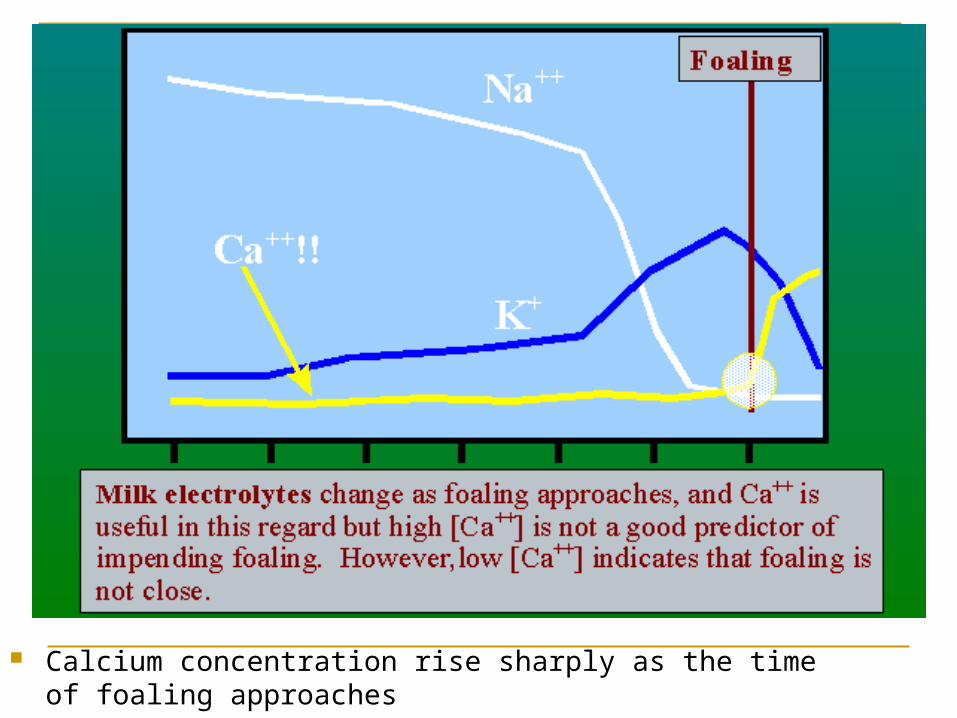
Calcium concentration rise sharply as the time of foaling approaches
Foaling Facilities Stall-
14x14 for light mares
Disinfect between foaling
Good air circulation
Safe, solid construction
Straw bedding Paddock-
“clean” grassy paddock
Safe, good fencing
Other horses?
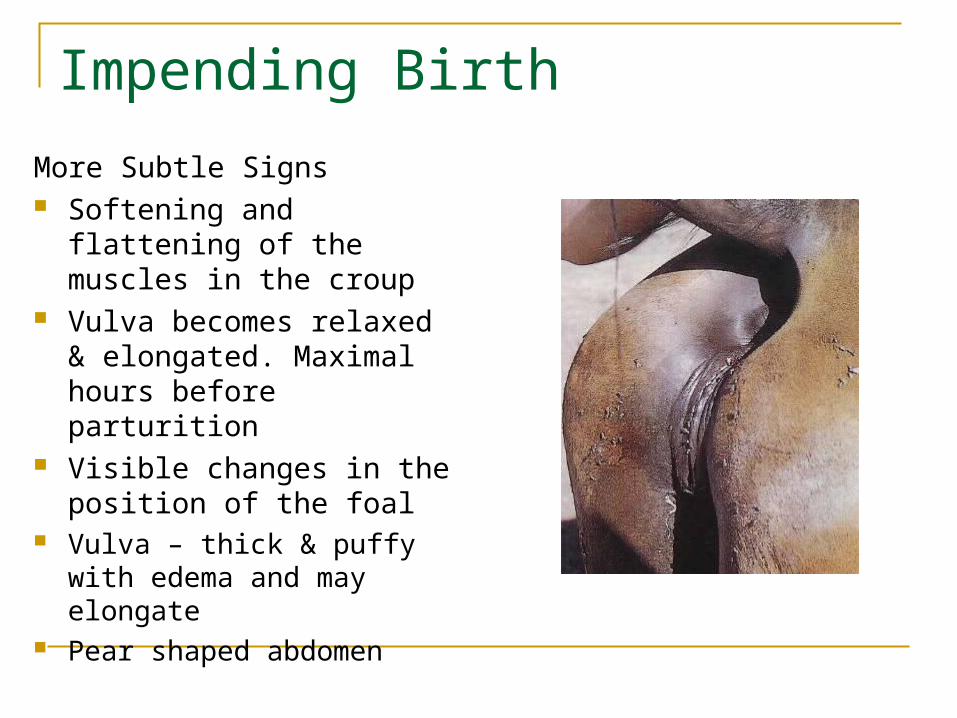
Impending Birth
More Subtle Signs Softening and flattening of
the muscles in the croup Vulva becomes relaxed &
elongated. Maximal hours before parturition
Visible changes in the position of the foal
Vulva – thick & puffy with edema and may elongate
Pear shaped abdomen
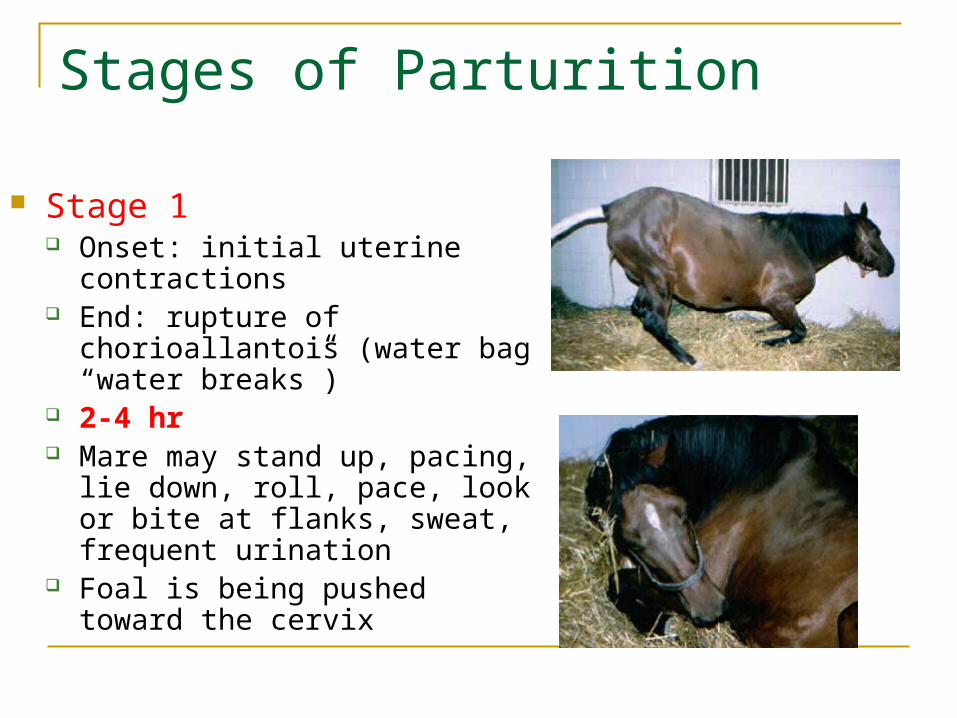
Stages of Parturition
Stage 1 Onset: initial uterine contractions End: rupture of chorioallantois
(water bag “water breaks”) 2-4 hr Mare may stand up, pacing, lie
down, roll, pace, look or bite at flanks, sweat, frequent urination
Foal is being pushed toward the cervix

Stages of Parturition Stage 2
Onset: rupture of chorioallantois (8-20L)
End: delivery of fetus- cord is broken
Timeline 20-30 min Contractions occur in groups
of 3-4 followed by a rest period of 3 to 5 minutes
Forefeet visable, soles pointing down
Oxytocin release, uterine contractions reinforced


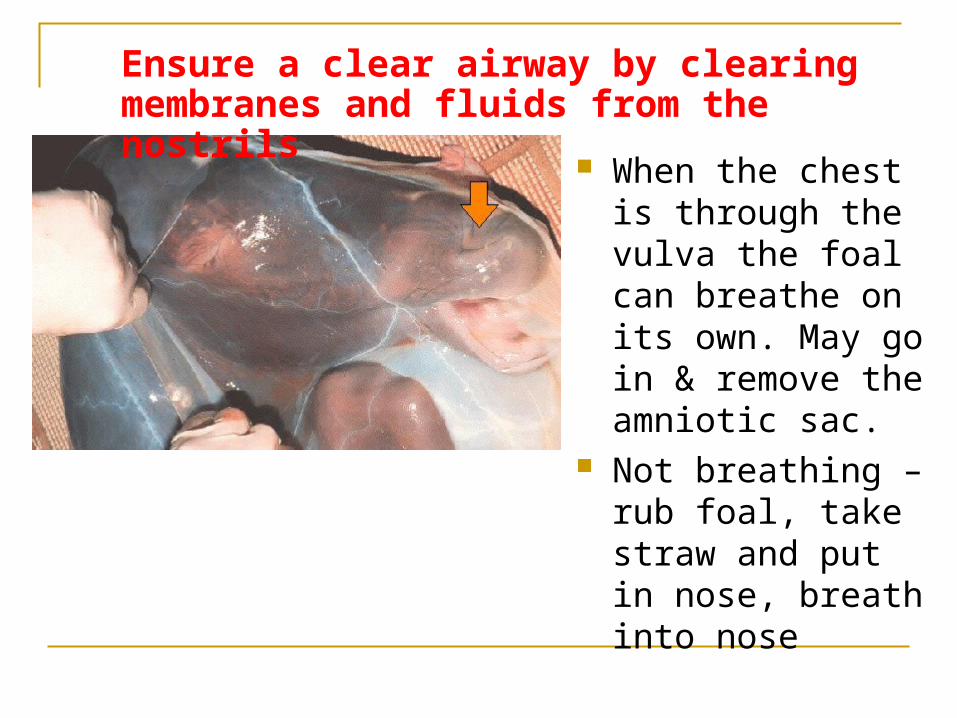
When the chest is through the vulva the foal can breathe on its own. May go in & remove the amniotic sac.
Not breathing – rub foal, take straw and put in nose, breath into nose
Ensure a clear airway by clearing membranes and fluids from the nostrils
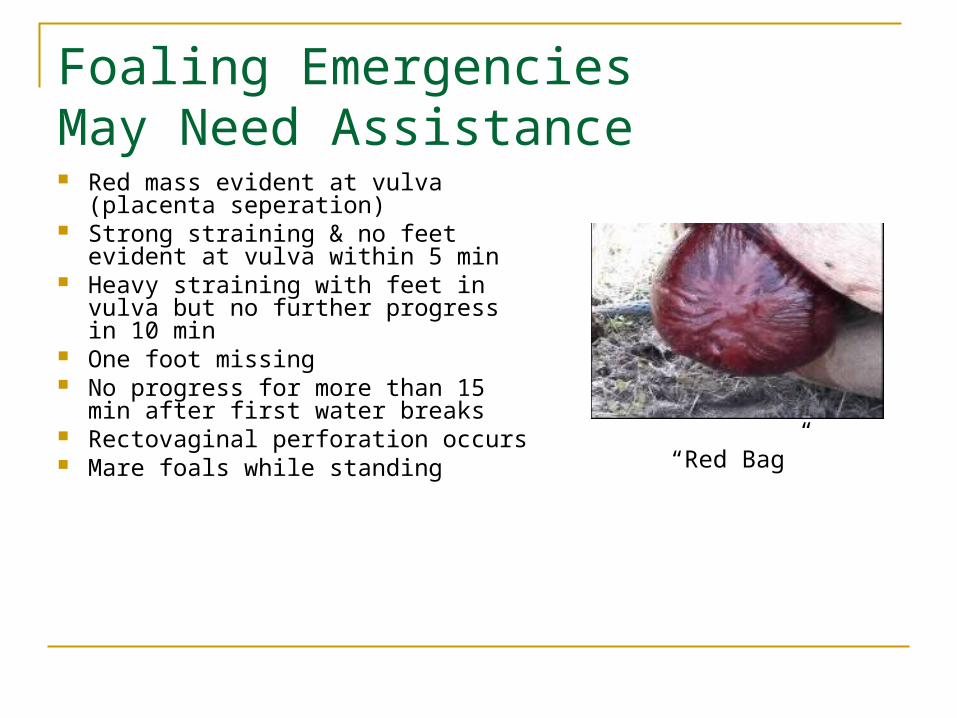
Foaling EmergenciesMay Need Assistance Red mass evident at vulva (placenta
seperation) Strong straining & no feet evident at
vulva within 5 min Heavy straining with feet in vulva
but no further progress in 10 min One foot missing No progress for more than 15 min
after first water breaks Rectovaginal perforation occurs Mare foals while standing
“Red Bag”

Foaling EmergenciesMay Need Assistance
If the chorioallantois does not break and the velvety-red surface of the chorioallantois is presented at the vulva, it should be immediately ruptured because this indicates that the placenta is separating from the endometrium and that fetal oxygenation will be impaired
- cut placenta and pull foal (fescue toxicity)
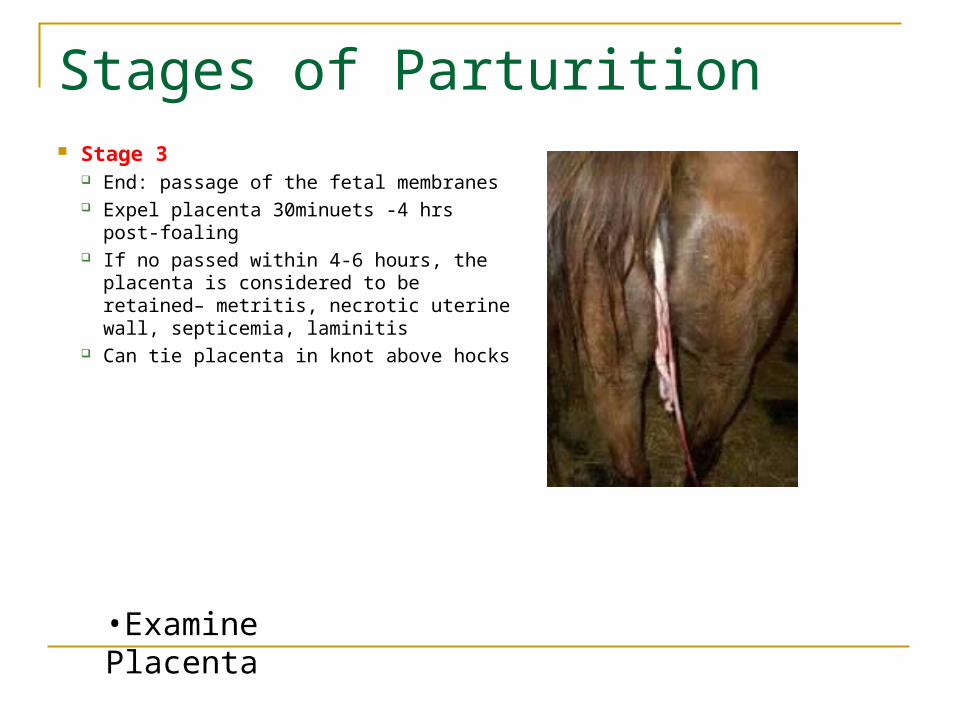
Stages of Parturition Stage 3
End: passage of the fetal membranes Expel placenta 30minuets -4 hrs post-
foaling If no passed within 4-6 hours, the placenta
is considered to be retained– metritis, necrotic uterine wall, septicemia, laminitis
Can tie placenta in knot above hocks
•Examine Placenta
http://video.google.com/videosearch?q=horse+breeding&hl=en&emb=0&aq=f#q=foaling&hl=en&emb=0

•Arrange the membranes in a capital "F" position, with the pregnant horn uppermost and the body forming the vertical bar of the "F"•Tip of the nonpregnant horn is the most likely part of the placenta to be retained•Placenta Examination
•Weight •Length of umbilical cord & location•Appearance of gross lesions, missing pieces
Placenta Examination

Retained Placenta: Treatment After 2 hrs Oxytocin Infusion of fluid into allantoic cavity Antibiotics Non-sterioidal anti-inflammatory drugs Frog support pads Deeply bedded stall

Abortions
No common, greater in mares over 14yrs Twins- 90% abort, Abortion in mid to later gestation may occur
in single horse, or many “abortion storm” (viral or bacterial)
If this happens fetus should be placed on ice and examined by vet within 12 hours.
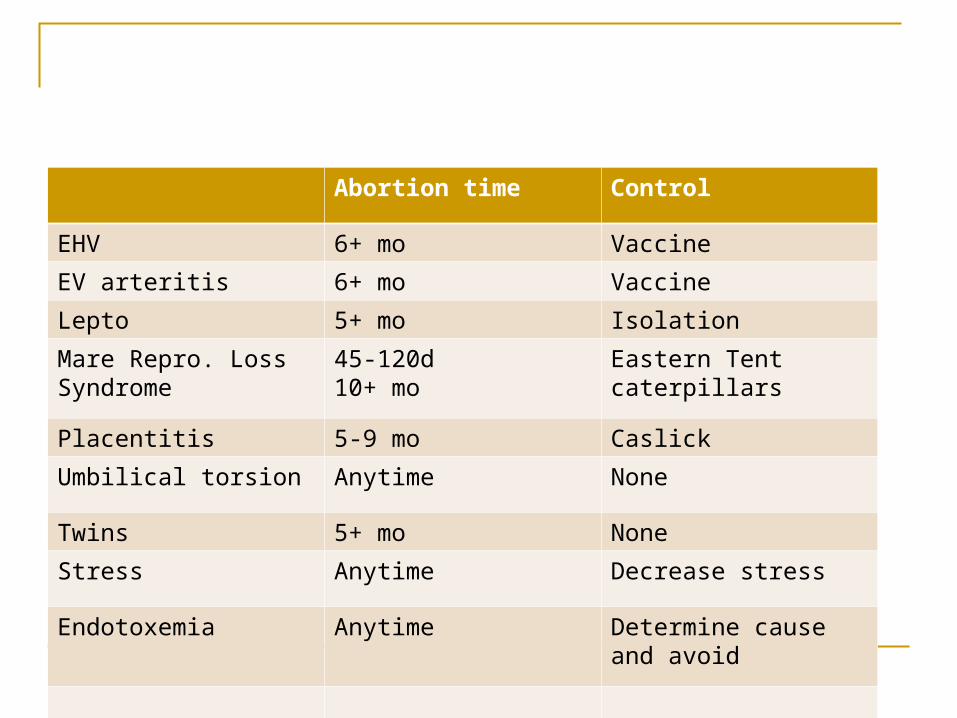
Abortion time Control
EHV 6+ mo Vaccine
EV arteritis 6+ mo Vaccine
Lepto 5+ mo Isolation
Mare Repro. Loss Syndrome
45-120d10+ mo
Eastern Tent caterpillars
Placentitis 5-9 mo Caslick
Umbilical torsion Anytime None
Twins 5+ mo None
Stress Anytime Decrease stress
Endotoxemia Anytime Determine cause and avoid
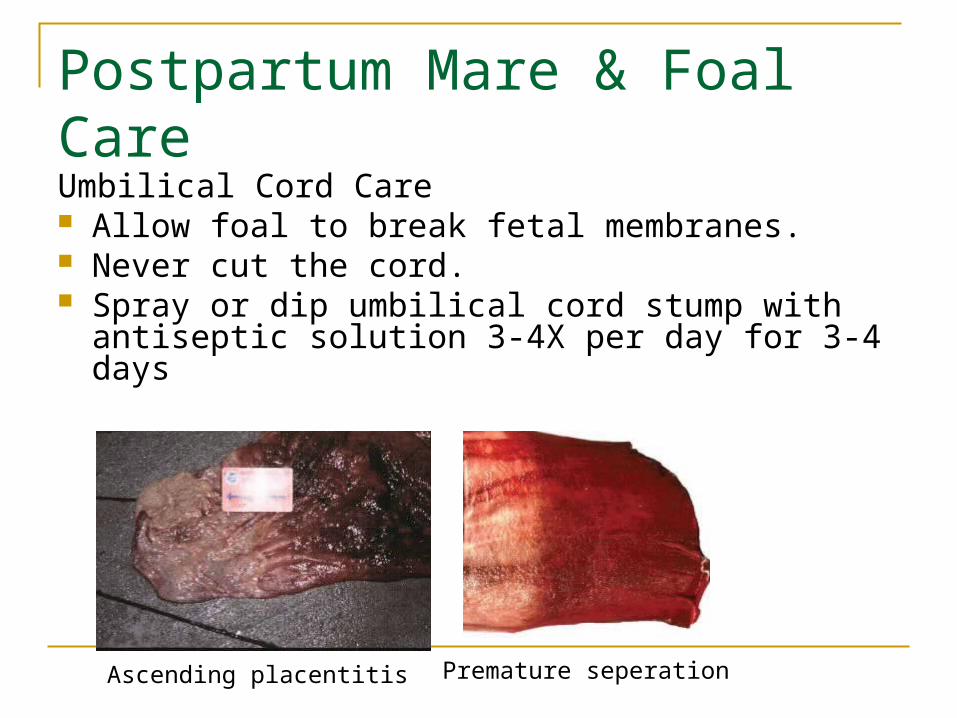
Postpartum Mare & Foal CareUmbilical Cord Care Allow foal to break fetal membranes. Never cut the cord. Spray or dip umbilical cord stump with antiseptic
solution 3-4X per day for 3-4 days
Ascending placentitis Premature seperation

Umbilical cord is made of
Umbilical vein, 2 umbilical arteries, and urachus
Vein becomes the falciform ligament
Arteries become the round ligaments of the bladder
Best to let the cord rupture naturally
Neonatal Care
The neonatal period is the period following birth, which most clinicians consider the first 4 to 5 days
This period is one of susceptibility to many diseases and conditions that can be threatening to the immediate and long-term health of the foal
Good neonatal care is a combination of sound management practices and recognition of normal and abnormal conditions

Foal FactsFoal Facts
Newborn foal should exhibit a suckle reflex at 20 minutes after birth, stand within 30-60 min.and nurse within 60 to 180 min.
The first urination occurs within 10 hours and the meconium should be passed by 24 hours after parturition. (Meconium is the first fecal material that the newborn foal normally evacuates. It appears in pelleted form, brown to black in coloration. They must pass this or become impacted.)
LACP pg. 165
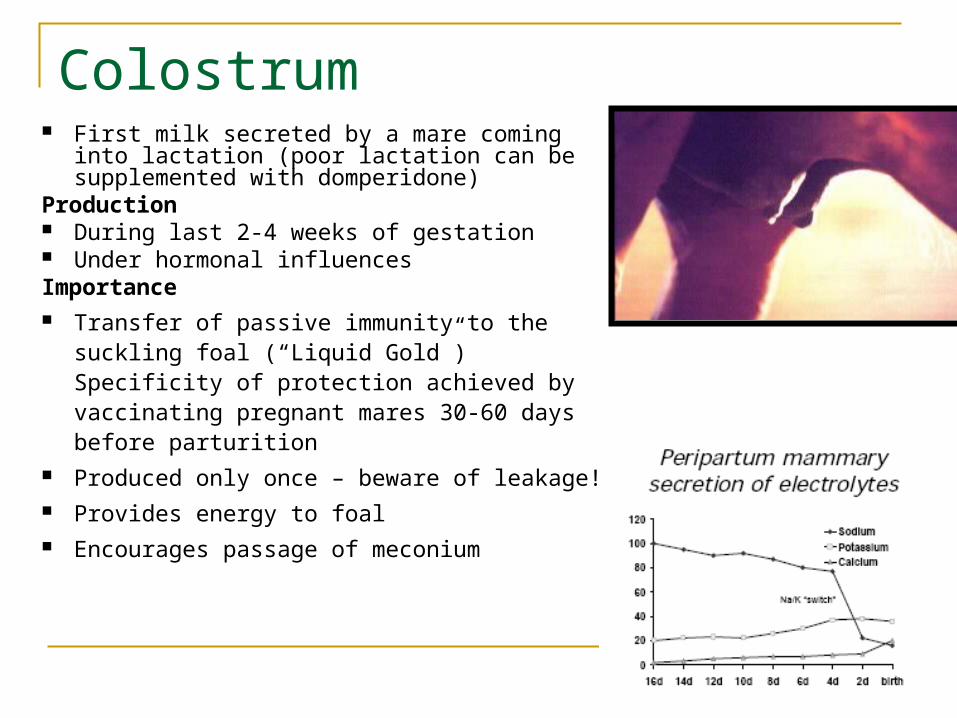
Colostrum First milk secreted by a mare coming into
lactation (poor lactation can be supplemented with domperidone)
Production During last 2-4 weeks of gestation Under hormonal influencesImportance Transfer of passive immunity to the suckling
foal (“Liquid Gold”) Specificity of protection achieved by vaccinating pregnant mares 30-60 days before parturition
Produced only once – beware of leakage! Provides energy to foal Encourages passage of meconium

Colostrum
Quality Relates directly to antibody content Good quality:
≥ 50 (70) g/L IgG and specific gravity > 1.060 Thick, sticky, yellow secretion All foals should have IgG measured between 8-24 hours

Colostrum Evaluating Colostrum QualityWhen? Assess before foal sucklesHow? Physical appearance
Thick, sticky, yellow secretion indicates good quality Dilute, white or translucent secretion indicates poor quality
Stall Side Tests
Banking of Colostrum
Only good quality colostrum
Storage at - 20ºC:
IgG concentration stable for 12 months
Other immune components (complement, etc) and nutritional
components decrease significantly
Storage at -70ºC:
Permanent maintenance of all components
Colostrum
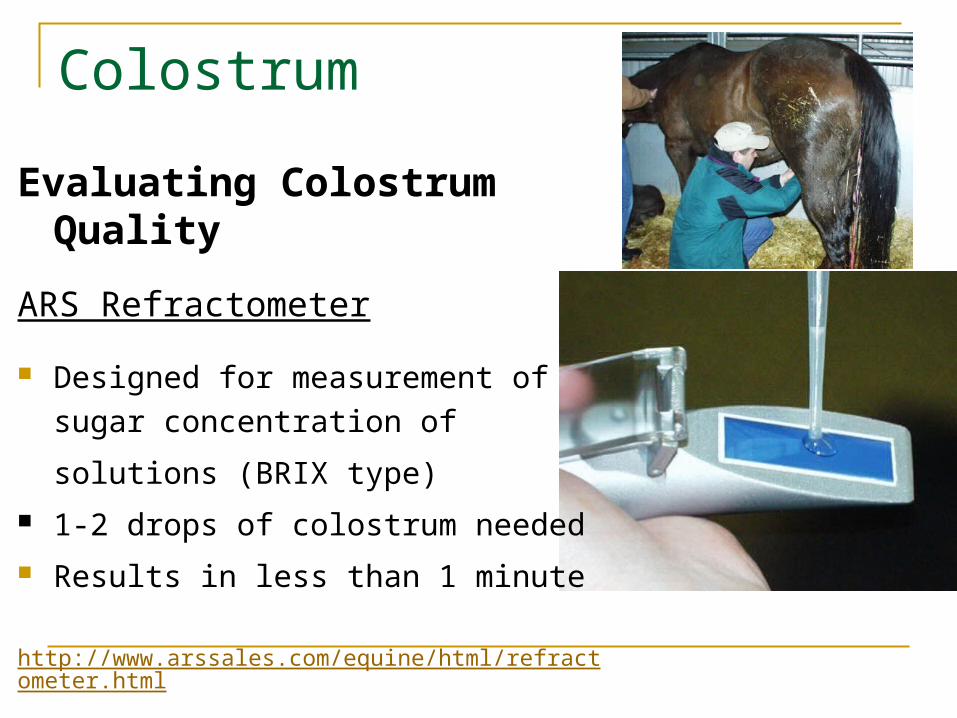
Evaluating Colostrum Quality
ARS Refractometer
Designed for measurement of sugar
concentration of
solutions (BRIX type)
1-2 drops of colostrum needed
Results in less than 1 minute
http://www.arssales.com/equine/html/refractometer.html

Colostrum
ARS Refractometer - Results
Evaluating Colostrum Quality

Foal Immune Status
Evaluation of serum IgG status
When? Typically at 12-24 h after birth
Peak serum levels of IgG achieved by 18h Absorption of immunoglobulins from small intestine essentially
complete If failure of passive transfer: treat with IV plasma
Can measure early at 6-12 h IgG first detected in foal’s serum at 6 h of age If no IgG or very low level at 6-12 h: can give colostrum to
increase levels

Foal Immune Status
Evaluation of serum IgG statusSnap Foal IgG Test ELISA Use whole blood, serum, or plasma Calibrator spots indicate IgG
levels of 400 and 800 mg/dl Sample color is proportional to
IgG content Results in 10-15 min. Expensive but convenient

Foal Aftercare: within 1st 24 hours
Give enema to prevent Meconium impaction
Give Tetanus antitoxin Check for presence of suckle reflex Check for any malformations or
deformities Take blood sample from foal. Perform a physical
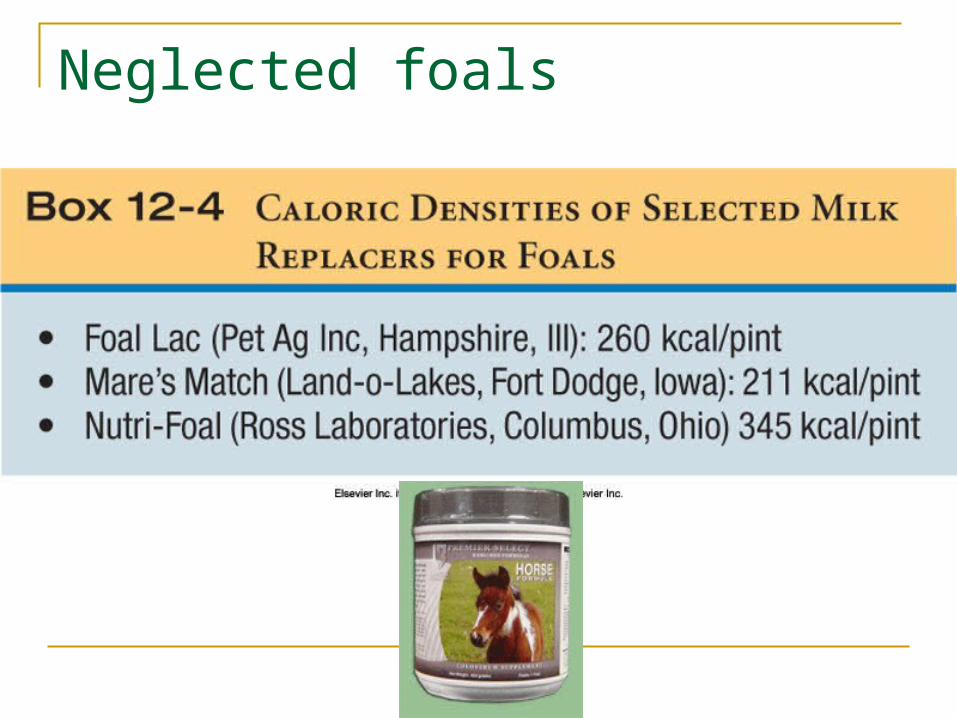
Neglected foals
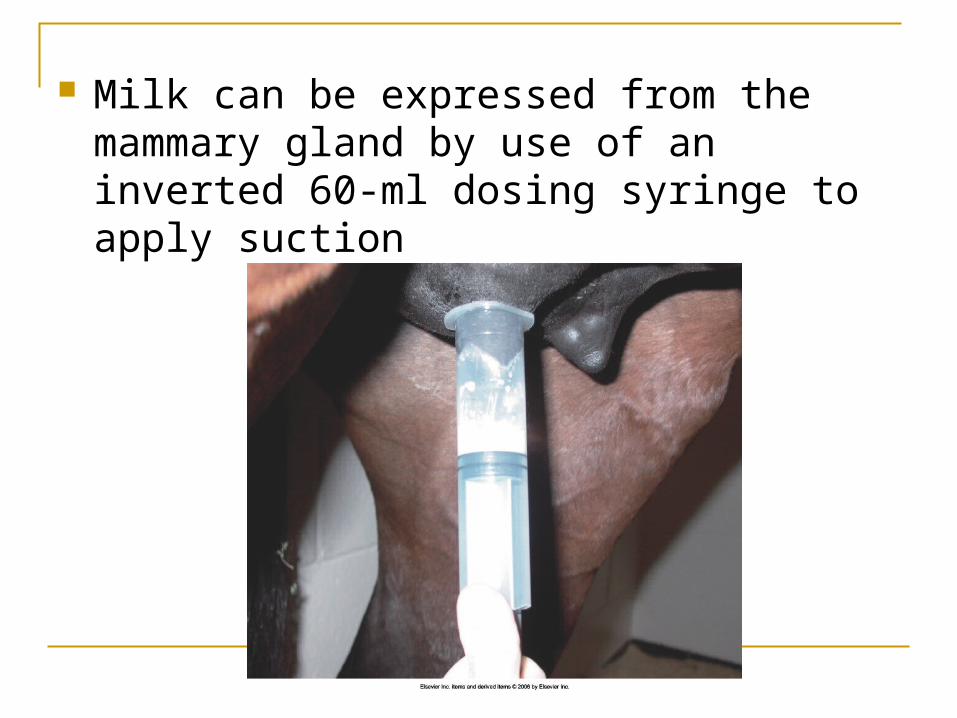
Milk can be expressed from the mammary gland by use of an inverted 60-ml dosing syringe to apply suction



Common Foal Diseases
Sepsis Perinatal Asphyxia Prematurity Neonatal Diarrhea Respiratory Disease

Sepsis
Common in foals Fever, elevated heart rate, or respiratory rate
Causes: improper umbilical care, failure of passive transfer, poor sanitation, maternal illness such as placentitis
Treatment: intensive nursing care, immunoglobulin therapy, antimicrobial treatment

Perinatal Asphyxia
Lack of oxygen “dummy foal syndrome” cerebral edema and
ischemia and necrosis of the brain
48 hours after birth foal my lose the affinity for the mare, become unable to suckle, wander aimlessly, and potential for seizures.
Prognosis is good if there are no seizures

Prematurity
Equal to or less then 320 days
Low birth wt, weakness, short hair coat, increased joint motion, rear limb flexural laxity, take longer to stand, suckle reflex may lack vigor, domed forehead, floppy ears
Survival depends on degree of complication

Diarrhea Common Frequency of diarrhea, suckling of foal,
weather other foals are affected
Cause: Foal heat diarrhea, rotavirus, coronavirus, septicemia, salmonella, clostridium, Strondyloides westeri, lactose intolerance.
Iv fluid therapy, probiotics, analgesics, plasma

Respiratory Disease Can be hard to diagnose: restlessness and
agitation, increased respiratory rate or distress.
Diagnosis- thoracic radiograph, arterial blood gas, pulse ox, ultrasound
Cough is rarely seen, nasal discharge uncommon, respiratory rate and rhythm can be unreliable, mucous membrane won’t reflect mild to moderate pulmonary disease, Thoracic auscultation can be misleading

Bacterial pneumonia Viral pneumonia Fungal pneumonia Milk aspiration Acute respiratory distress syndrome Persistent pulmonary hypertension Fractured rib Pneumothorax Pleural effusion

Examination of the inner ear reveals petechiation

The critically ill neonatal foal should be placed on a warm, well-padded surface in semisternal recumbency

The jugular groove is widely clipped and prepared with sterile solutions before intravenous catheter placement

Proper restraint of the foal is achieved by gently cradling one hand under the neck and grasping the base of the tail with the other hand.


Limb Deformities
Angular- Varus, Valgus, Windswept Axial- off set knees Rotational- muscular Spiral- toed in Flexor – week or contracted flexors
Most are congenital, premature, dietary, blunt trauma to the growth plate, uneven hoof balance

Angular
Valgus
Varus
Windswept
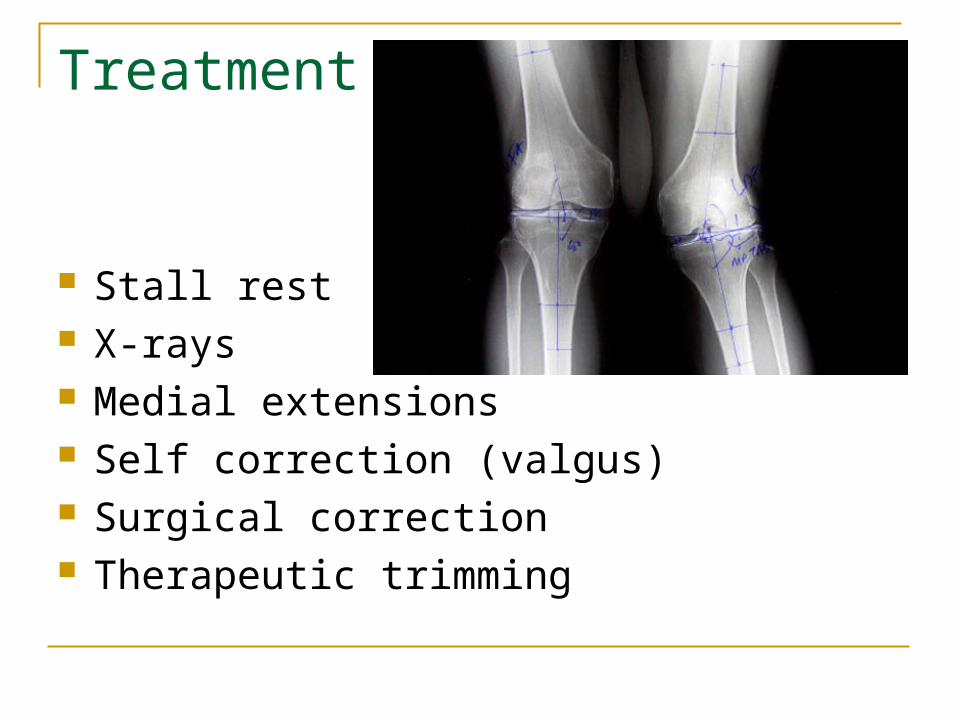
Treatment
Stall rest X-rays Medial extensions Self correction (valgus) Surgical correction Therapeutic trimming

Axial- off set knees
No treatment, undesirable in race horses, can lead to unsoundness
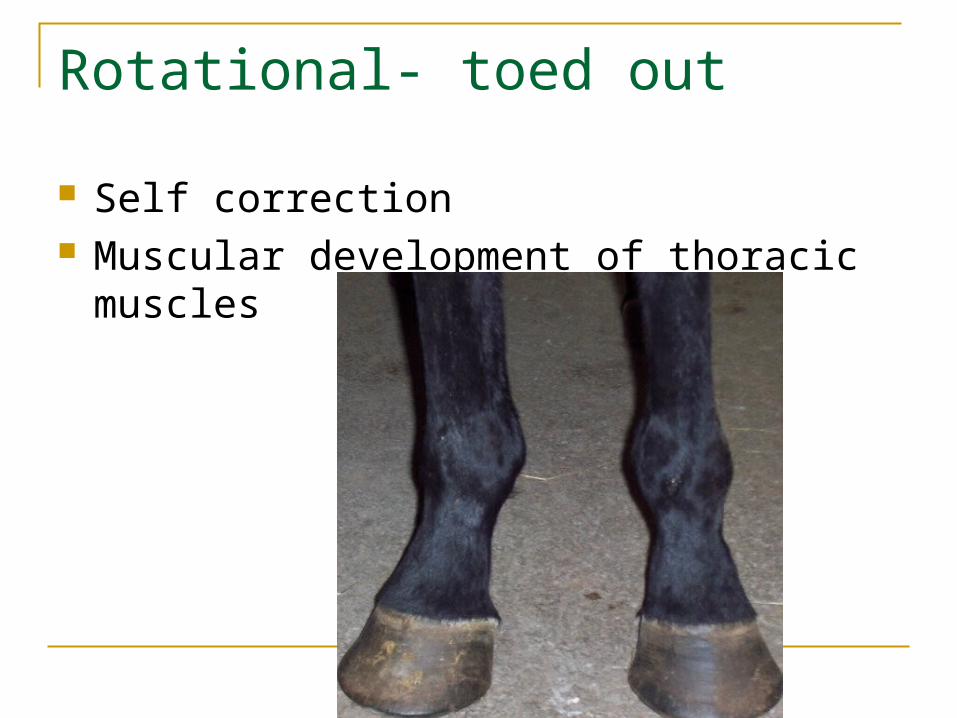
Rotational- toed out
Self correction Muscular development of thoracic muscles

Spiral – toed in
Fetlock is in normal
alignment
No treatment, corrective
shoeing masks problem
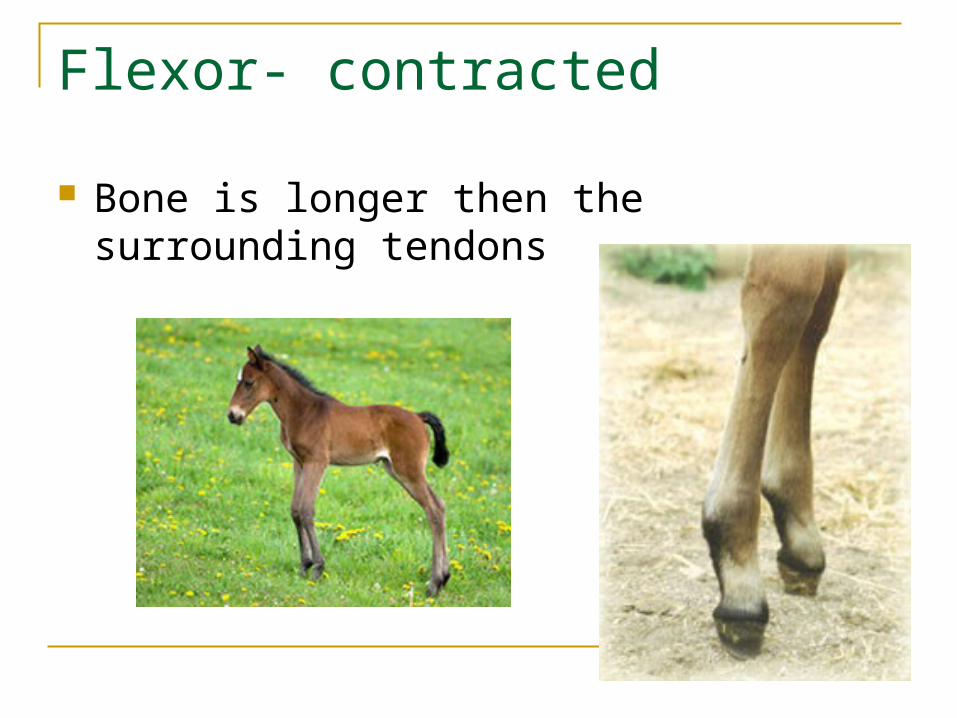
Flexor- contracted
Bone is longer then the surrounding tendons

treatment
Tetraclycine- shown to relax the muscle/tendon unit
Bandaging Passive extension stretching Air splints PVC splints surgery
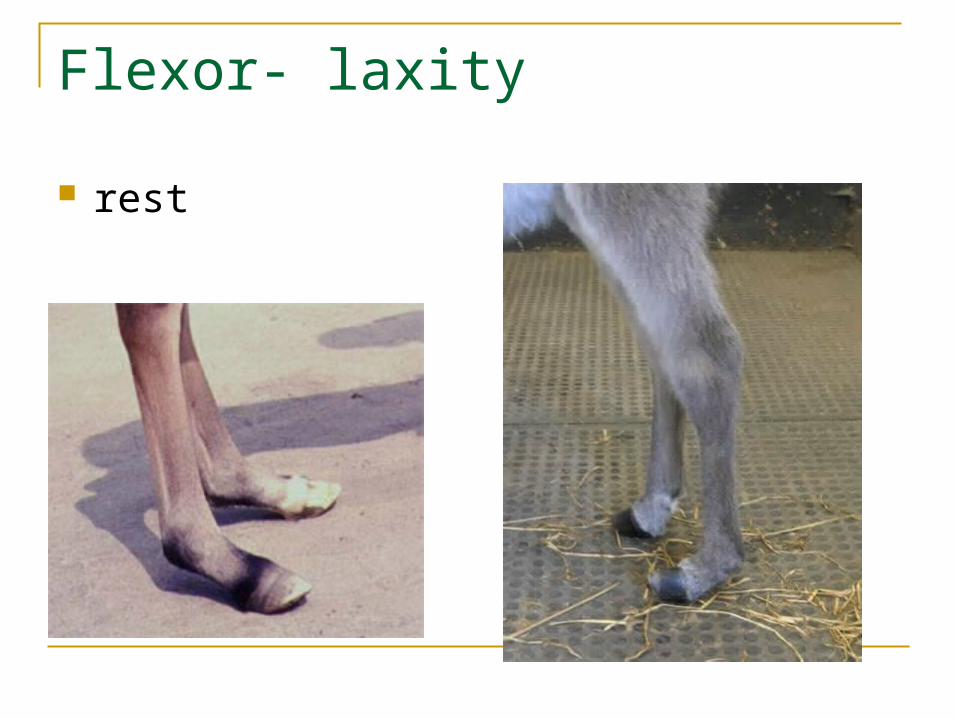
Flexor- laxity
rest

Bone growth catches up with tendons Swimming Care for soft tissues if damaged