parkinson’s disease ibrahim sales, pharm.d. assistant professor of clinical pharmacy king saud...
TRANSCRIPT

Parkinson’s Disease
Ibrahim Sales, Pharm.D.Assistant Professor of Clinical Pharmacy
King Saud [email protected]

Learning Objectives
• Describe Parkinson’s Disease• List drugs used in the treatment of Parkinson’s
Disease• Describe the pharmacological management of
each drug used in the treatment of Parkinson’s Disease
• Describe the mechanism of action, toxicities, and pharmacokinetics of drugs used to treat Parkinson’s Disease

Parkinson’s Disease (PD)
• Second most common neurodegenerative disease
• Clinical symptoms are motor and nonmotor• Diagnosis based on motor symptoms• Etiology is unknown• No treatment can stop the progression of PD
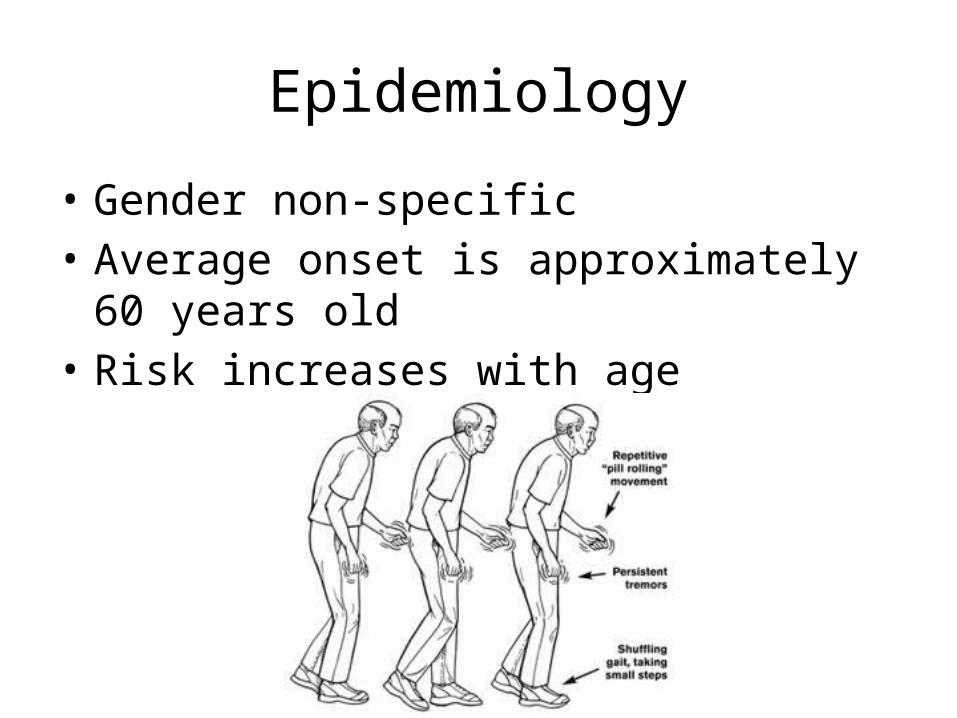
Epidemiology
• Gender non-specific• Average onset is approximately 60 years old• Risk increases with age

Clinical Presentation
• d

Pharmacological Management
• There is no treatment that can stop or reverse the loss of dopaminergic neurons
• Symptomatic relief• Strategies– Increase the amount of dopamine activity in the
brain– Decrease the amount of cholinergic brain activity– Both (dopamine and acetylcholine need to be in
balance for normal, balanced movement)

Therapeutic Goals
• Reduce the incidence and severity of motor and nonmotor symptoms
• Maintain quality of life• Improve activities of daily living• Minimize complications of drug therapy

Levodopa
• First introduced in the 1960s• Gold standard• Dopamine cannot cross the blood-brain
barrier• Levodopa (amino acid) precursor of dopamine• Carbidopa – decarboxylase inhibitor in
peripheral body tissues

Levodopa
• Ameliorates the motor symptoms• Improves QOL, lengthens independence and
decreases mortality rate• Effects last for several hours initially• Therapeutic response nears t½ eventually

Levodopa
• Rapidly absorbed from the small intestines• High-protein meals will delay absorption and
decrease peak plasma concentration• Peak plasma concentration: 0.5 to 2 hours• t ½ : 1 to 3 hours

Levodopa
• Contraindications:– Psychotic patients, closed-angle glaucoma, active
peptic ulcer (monitor closely), MAO inhibitor if taken within 14 days, undiagnosed skin lesion or history of melanoma
• Pregnancy risk factor C• Adverse effects: – Nausea, vomiting, anorexia; postural hypotension;
nightmares, agitation, confusion insomnia, depression, somnolence, anxiety

Levodopa
• Patients may develop myoclonus or dystonia when medication is at its peak concentration
• Dyskinesia is not disabling if mild; only severe• “On-off phenomenon”– Initial responders
• Decreased absorption/effect:– Oral iron salts (except iron sucrose, ferumoxytol, iron
dextran complex and ferric gluconate); sapropterin, metoclopramide, phenytoin, pyridoxine, kava kava; methylphenidate can increase levodopa toxicity

Levodopa
• Usually prescribed with carbidopa• IR tablet: carbidopa 25mg/levodopa 100mg
TID– Increase dose by one tab every other day
• Carbidopa 25mg/levodopa 250mg– Increase dose by ½ tab every 1 to 2 days
• Max number of tablets is 8 or 200mg carbidopa and 2000mg levodopa

Levodopa
• Sustained release• Carbidopa 50mg/levodopa 200mg BID at least
6 hours apart– Increase dose every 3 days
• Max number of tablets per day is 8• Initial dose for elderly is carbidopa
25mg/levodopa 100mg two tablets daily

Dopamine Agonists
• Directly stimulate dopamine receptors• Ergot dopamine agonists (bromocriptine)• Non-ergot dopamine agonists (pramipexole and ropinirole)
– Stimulate the D3 and D2 receptors• Ineffective in patients that do not respond to levodopa• Monotherapy or in combination with carbidopa/levodopa
– Can postpone levodopa use• Improves tremor, bradykinesia, and rigidity• Dopamine agonists last therapeutically longer than levodopa• Minimize fluctuations in dopamine blood concentrations,
allow for levodopa dose reduction, improve ADLs

Bromocriptine
• Partial dopamine agonist• Ergot derived• Ergot derived side effects:
Pulmonary/cardiofibrosis infiltrates• Dosing: 1.25 mg BID– Increase at 2 to 4 weeks by 2.5mg/day– Average dose: 20-40mg daily in TID or QID doses– Max dose: 90mg/day

Rotigotine
• Transdermal Patch– Daily patch formulation– Start at 2mg/24 hours; max 6mg/24 hours– Do not discontinue abruptly• Neuroleptic malignant syndrome like• Akinetic crisis

Pramipexole
• Stimulates the D3 receptors• May be prescribed for mild cases of PD;
especially effective for treating patients experiencing the “on-off phenonmenon”– Reduces the “off” time

Pramipexole
• Rapidly absorbed from the GI tract• Plasma concentration peaks in 2 hours for the
IR form; peaks in 6 hours for the extended release form
• t ½ is 8.5 hours; 12 hours for the elderly• Excreted in the urine, 90% unchanged

Pramipexole
• Initial dose for the IR form is 0.375mg daily divided into 3 doses– Titrate dose every 5 to 7 days to minimize adverse effects– Maximum dose 4.5mg daily
• Initial dose for the ER for is also 0.375mg daily– Titrate dose by 0.75mg a day every 5 to 7 days– Maximum dose is 4.5mg a day– CrCl 30 – 50 mL/min, dose every other day up to 2.25mg daily
CrCl (mL/min) >60 35 to 59 15 to 34
Initial dose 0.125mg TID 0.125mg BID 0.125mg daily
Maximum dose
1.5mg TID 1.5mg BID 1.5mg daily

Pramipexole
• If discontinuing, taper over one week– Risk of developing a disorder resembling
neuroleptic malignant syndrome• Pregnancy risk factor C
Ropinirole
• Stimulates the D2 receptor and is effective in mild cases
• Effective in patients in an advanced stage who have “on-off phenomenon”
• Absorbed in the GI tract; unaffected by food• Plasma concentration peaks at 1 to 2 hours for IR
form; 6 to 10 hours for ER form• t ½ 6 hours• Excreted in the urine; clearance is decreased from 15
to 30% in patients over 65 years old

Ropinirole
• Initial dose for the IR tablet for the first week is 0.25mg TID– Titrate slowly to avoid toxic effects– Week 2: 0.5mg TID– Week 3: 0.75mg TID– Week 4: 1mg TID– Can increase by 1.5mg a day on a weekly basis up to
a total dose of 9mg a day– Can raise dose by 3mg a day on a weekly basis up to a
total of 24mg a day

Ropinirole
• If discontinuing, gradually taper over a 7 day period– Frequency should be decreased to BID for the first
4 days then lowered to once daily for the remaining 3 days

Ropinirole
• The initial dose for the ER tablet is 2 mg once daily for the first 1 or 2 weeks
• The dose can be increased by 2 mg a day on a weekly basis with the maximum dosage as 24mg daily
• Taper in the same manner as the IR tablet

Apomorphine
• Stimulates D2, D3, D4, and D5 receptors• “Rescue therapy” for a patient who has severe
“off” period and is not responding to other medication
• Subcutaneously injected• Therapeutic benefit begins in 10 minutes and
lasts for 2 hours• Plasma concentration peak in 20 minutes• t ½ is 40 minutes

Apomorphine
• Contraindications– Hypersensitivity to apomorphine or ingredients;
administration IV; concomitant use with serotinin antagonists (loss of consciousness and extreme hypotension)
– Toxic effects include hypotension, chest pain, dyskinesia, sweating, drowsiness, falls, abnormal EKG (QT prolongation), nausea and vomiting (pre and post anti-emetics )• Trimethobenzamide at 300mg TID should be started 3 days before
the patient receives the first dose and continued at least for the first 2 months
• Ondansetron is a serotonin antagonist and should not be used
Apomorphine
• Three days before initial dose, administer trimethobenzamide 300mg TID; continue for 2 months then assess
• Initial dose is a test dose of 2mg given during an “off” period
• If patient tolerates the test dose, start at 2mg– May increase dose by 1mg every few days
• Max dose is 6mg

Apomorphine
• Patients tolerating the test dose, but not therapeutically responding– 2nd test dose of 4mg administered– If responds, starting dose is 3mg– Increase dose every few days; max is 6mg
• Patients who don’t tolerate the test dose of 4mg– 3rd test dose of 3mg can be given– If tolerated, the start dosage is 2mg– 2mg dose may be increased by 1mg to a max of 3mg
Apomorphine
• If not administered for more than 1 week, the start dose is 2mg; the dosage must gradually be increased
• Standing and supine BP must be checked before administering a test dose– Both pressures must be checked 20, 40, and 60
minutes after the test dose– If additional test dosed are needed, there must be a
2-hour wait before the next test dose which should be only given during an “off” period

Apomorphine
• Use cautiously in patients with mild to moderate impairment of the liver
• The test dose and starting dose should be 1mg for patients with mild to moderate renal impairment
• Pregnancy risk factor C

Dopamine Agonists ADEs
• Nausea, vomiting, dyskinesias, somnolence, sedation, hallucinations, nightmares, confusion, and postural hypotension
• Obsessive-compulsive disorder and impulse-control disorder
• Excessive daytime sleepiness– Modafinil 200 – 400mg daily

MAO-B Inhibitors
• Monoamine oxidase type B is an enzyme which metabolizes dopamine to homovanillic acid in the striatum
• Selegiline and rasagiline interfere with dopamine metabolism, thereby increasing the concentration of dopamine at the neuronal synapse

MAO-B Inhibitors
• They provide some therapeutic benefit when used as monotherapy in early or mild symptomatic PD
• May decrease the effects of the “off” period when administered with levodopa and prolong its effects, allowing the dosage of levodopa to be reduced

Pharmacokinetics
• Selegiline– Effects start within 1 hour and last for 24-72 h– T ½ is 10 h for the tablet, but 18 to 25 for the
transdermal form• Rasagiline– Effects start within 1 hour and last for 1 week– T ½ is 1.3 to 3 h

Selegiline and Rasagiline
• Dyskinesias may increase if administered with levodopa, but can be controlled by lowering the levodopa dose
• Potential for serotonin syndrome• Pregnancy risk factor C• Adverse effects– Selegiline: nausea, confusion, hallucinations, insomnia,
headache, jitteriness, orthostatic hypotension, dyskinesias– Rasagilinie: diarrhea, weight loss, hallucinations, rash– Tyramine – hypertensive crisis

Dosing
• Selegiline– 5mg BID at breakfast and lunch (insomnia)– Initial dose for ODT is 1.25mg daily x 6 weeks• May increase to max dose of 2.5mg daily
• Rasagiline– 1mg daily if needed and tolerated– Lower levodopa dose 9 to 13% (dyskinesias)– Mild hepatic impairment dose: 0.5mg daily• Avoid in moderate to severe hepatic impairment

COMT Inhibitors
• The enzyme catechol-o-methyltransferase (COMT) metabolizes dopamine to homovanillic acid
• Levodopa is mainly metabolized by COMT• COMT inhibitors increase the levodopa half-life
and allow more levodopa to cross the BBB• COMT administered with levodopa decreases
the “off” period and increases the “on” period• Possible lowering of the levodopa dosage

COMT Inhibitors
• Entacapone– Quickly absorbed; quick onset of action– Peak effect at 1 hour– T ½ is 2 hours
• Tolcapone– Rapidly absorbed– T ½ is 2-3 hours– Peak plasma concentration in 2 hours

Adverse Reactions
• Entacapone– Diarrhea, brown-orange colored urine from the
accumulation of metabolites, dyskinesia, nausea and vomiting• Dyskinesia and nausea can be decreased or avoided by
lowering the dose of levodopa by 20 to 30% in the first 48 hours of administering entacapone

Adverse Reactions
• Tolcapone– Same as entacapone– Dyskinesia and nausea can be decreased by lowering
the levodopa dose, but the diarrhea can be so severe that 5 to 10% of patients d/c
– Dizziness, hallucinations, somnolence, postural hypotension; hepatic toxicity (some fatal cases)• Administer if no other treatment is available or
responsive; patients must sign a consent form; liver enzymes must be monitored every two weeks for the first year

Dosing
• Entacapone– With every dose of levodopa/carbidopa, 200mg is
prescribed– Max frequency is 8x daily; max dose is 1600mg daily
• Tolcapone– More potent; advanced patients– 100mg TID; can be increased to 200mg TID– If no improvement in 3 weeks, d/c– If hepatic impairment develops, d/c
• Both medications are pregnancy risk factor C

Anticholinergics
• Antimuscarinic anticholinergic medications lower the actions of the cholinergic neurons in the striatum; basis for therapeutic effects is not understood
• Due to the toxicity of the other PD medications, if the patient is in early stages of PD, not elderly and the main symptom is tremor, may prescribe

Anticholinergics
• Benefits:– Rest tremor– Urinary frequency– Excess sweating– Drooling
• Less effective for bradykinesia, rigidity, or gait problems

Anticholinergics
• Elderly concerns– Increased risk of confusion, cognitive problems,
hallucinations– Dementia
• 2.5-fold increase in amyloid plaque and neurofibrillary tangle densities
• Baseline cognition evaluation, psychiatric history, and blood pressure
• Monitor for typical symptoms; decreased gastric acid secretion; decreased gastric emptying

Anticholinergics
• Trihexyphenidyl– t ½ or 33 hours– Plasma concentration peaks in 1.3 hours
• Benztropine– Effects start in 1 hour and lasts for 6 to 48 hours

Adverse Reactions
• Constipation, urinary retention, mydriasis, blurred vision, tachycardia, confusion, hallucinations, nausea, vomiting, hyperthermia
• Use with caution in CV disease, renal impairment, hepatic impairment, glaucoma, and prostatic hyperplasia
• KCl can interact and lead to ulcers

Dosing
• Trihexyphenidyl– Initial dose is 1mg daily
• Increase by 2 mg every 3-5 days• Usual dose is 6-10mg daily in 3-4 doses• Some patients need 12-15mg daily• If prescribed with levodopa, dose is 3-6mg daily in divided doses
• Benztropine– Initial dose is 1 to 2 mg daily in 2-4 doses
• May increase dose by 0.5mg each week; max 6mg/daily
• Avoid in patients > 60 years of age• Pregnancy risk factor C

Amantadine
• Releases stored dopamine and inhibits the NMDA glutamate receptor (excitatory)
• Prescribed in early PD; primarily prescribed to decrease the dyskinesia, tremor and rigidity of the advanced stage
• May only be beneficial for a few weeks or months

Amantadine
• Well absorbed and takes effect within 48 hrs• t ½ from 9 to 31 hrs• Plasma concentration peak of 2 to 4 hrs
• Adverse effects– Nausea, dizziness, insomnia, livedo reticularis (benign
purple mottling of the skin of dependent extremities), peripheral edema, orthostatic hypotension, hallucinations, and confusion
– Its stimulant action may worsen insomnia and restlessness

Dosing
• Standard dose for monotherapy is 100mg BID– May be increased to 400mg daily in divided doses
• Patients taking high doses of other medications for PD– Initial dose is 100mg daily• Dose can be increased after 1 week or more to 100mg
BID
• Pregnancy risk factor C

Treatment Algorithm

Treatment Algorithm

Treatment Algorithm

Wearing off therapy
• If monotherapy with levodopa– Increase frequency of levodopa
• Change to SR/CR formulation
– Increase dose of levodopa– Add a dopamine agonist– Add COMT-I
• If monotherapy with dopamine agonists– Add carbidopa/levodopa
• Apomorphine – rescue therapy• Diet – Avoid high protein

On-Off Phenomena
• Rapid fluctuations from “on” to “off” motor states• Freezing gate• Occurs in patients with advanced disease– Have motor fluctuations– Dyskinesia– On chronic levodopa
• Increase the frequency of levodopa• Add dopamine agonist• Add COMT-I