diabetes mellitus ibrahim sales, pharm.d. assistant professor of clinical pharmacy king saud...
TRANSCRIPT

Diabetes Mellitus
Ibrahim Sales, Pharm.D.Assistant Professor of Clinical Pharmacy
King Saud [email protected]

2
Non-pharmacologic Therapy
• Diet– Medical nutrition therapy is recommended for all
persons with DM • Physical activity
– Aerobic exercise– Goal: at least 150 minutes/week of moderate
(50%–70% maximal heart rate) intensity exercise– Resistance training at least twice weekly

Benefits of Modest Weight Loss in Type 2 DM
• Loss of 20lb (10%) in obese subjects reduced FBG by 29mg/dL and A1C by 1.1%
• Loss of 10lb (5%) reduced DBP by 5%• Loss of 6lb (3%) in obese men decreased
– Total cholesterol by 17%– LDL-C by 9%– Triglycerides by 35%
Arch Intern Med. 1987;147:1748 Diabet Med. 1990;7:228Arch Intern Med. 1997;157:169Metabolism. 1999;5:641

Medical Nutrition Therapy in Type 2 DM Management

Oral Medications
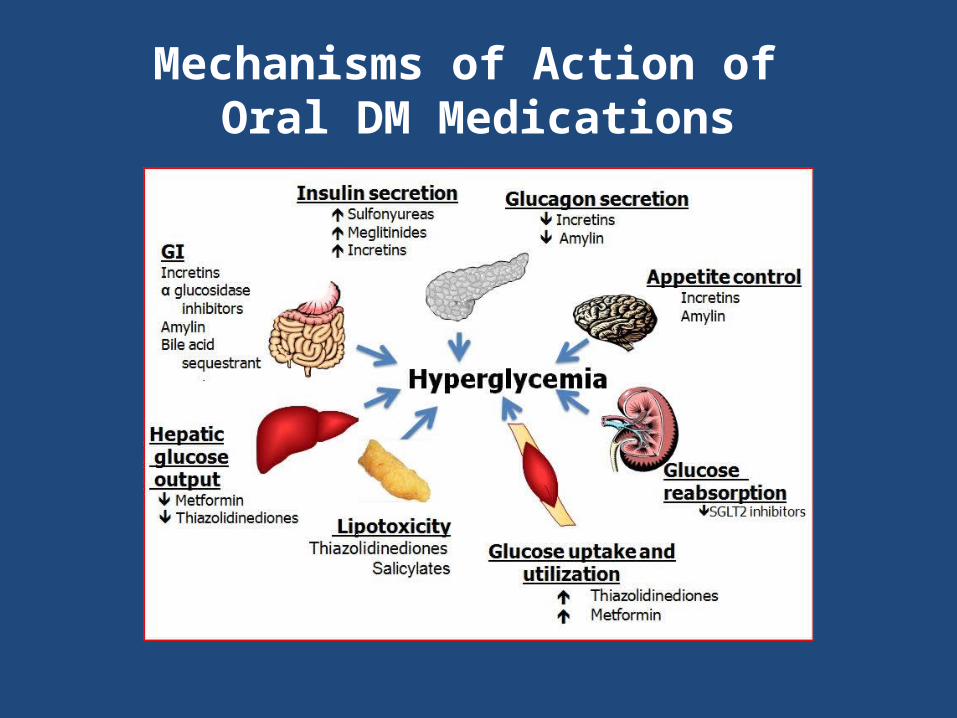
Mechanisms of Action of Oral DM Medications
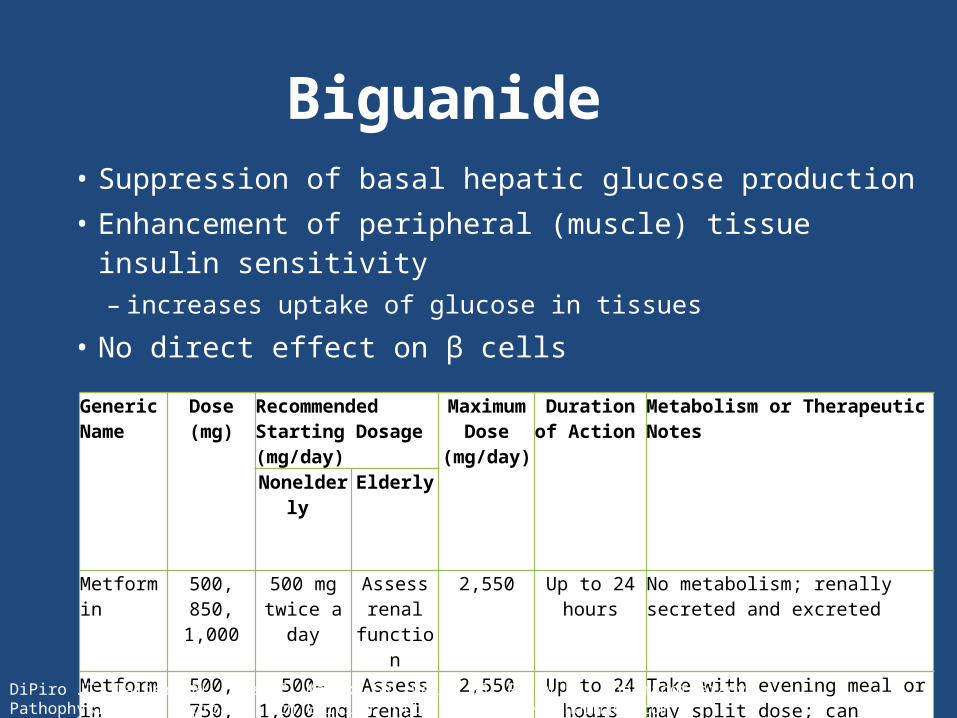
Biguanide
Generic Name
Dose (mg) Recommended Starting Dosage (mg/day)
Maximum Dose
(mg/day)
Duration of Action
Metabolism or Therapeutic Notes
Nonelderly Elderly
Metformin 500, 850, 1,000
500 mg twice a day
Assess renal
function
2,550 Up to 24 hours
No metabolism; renally secreted and excreted
Metformin extended- release
500, 750, 1,000
500–1,000 mg with evening
meal
Assess renal
function
2,550 Up to 24 hours
Take with evening meal or may split dose; can consider trial if intolerant to immediate-release
• Suppression of basal hepatic glucose production• Enhancement of peripheral (muscle) tissue insulin
sensitivity– increases uptake of glucose in tissues
• No direct effect on β cells
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th Edition: http://www.accesspharmacy.com

Biguanide
• Most common adverse effects: GI – abdominal discomfort, stomach upset, diarrhea
• Weight loss can occur– anorexia– stomach fullness
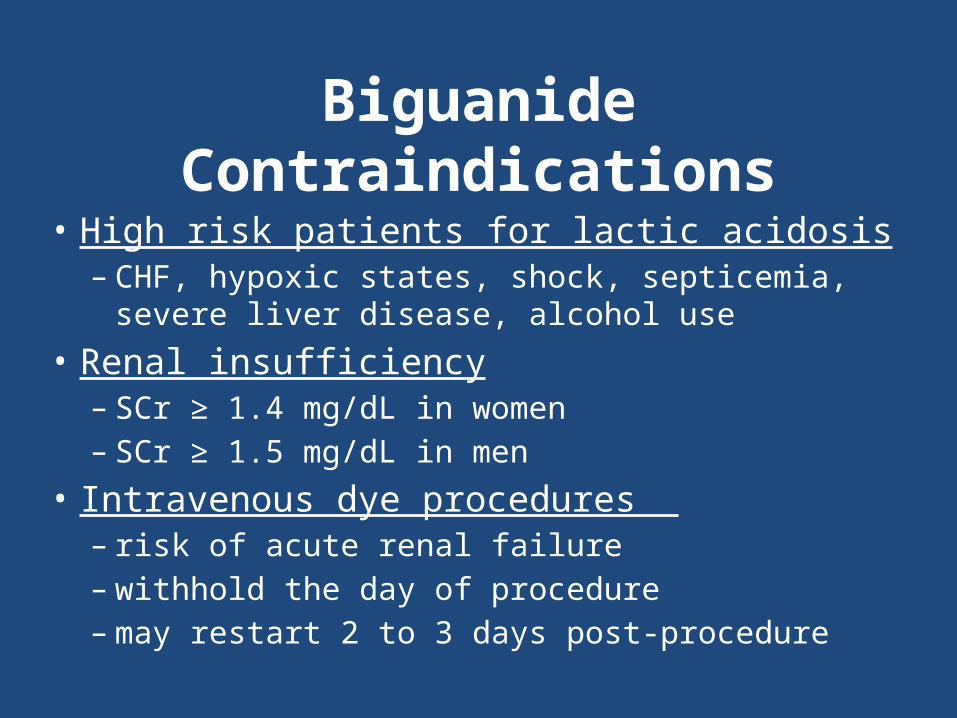
Biguanide Contraindications• High risk patients for lactic acidosis
– CHF, hypoxic states, shock, septicemia, severe liver disease, alcohol use
• Renal insufficiency– SCr ≥ 1.4 mg/dL in women– SCr ≥ 1.5 mg/dL in men
• Intravenous dye procedures – risk of acute renal failure– withhold the day of procedure– may restart 2 to 3 days post-procedure

Biguanide
• Average HbA1c reduction: 1.5 to 2.0%• FBG reduction: 60 to 80 mg/dL• Reduce FBG levels when > 300 mg/dL• Decrease plasma triglycerides & LDL-C by ~8 to
15%• Increases HDL-C: 2%

Biguanide
• Weight loss: 2 to 3 kg• Use in all type 2 DM patients
– If tolerated & not contraindicated– Only oral antidiabetic agent proven to reduce
mortality risk • UKPDS shows metformin is best suited for
obese type 2 DM patients; reduces mortality

Biguanide SummaryMedication (A1C reduction)
Mechanism of Action Comments
Metformin(1.5% to 2%)
• Decreases hepatic glucose production
• Improves insulin sensitivity (Increases peripheral glucose uptake and utilization)
• Decreases intestinal absorption of glucose
• Modest weight loss is common
• Contraindicated in patients with renal impairment (CrCl < 60 mL/min)
• Gastrointestinal side effects are most common
• Low risk of hypoglycemia

Case 2: Medication-Induced Hypoglycemia
TY is a 44 y/o male with Type 2 DM. This is his first visit with you. He is only taking Metformin 1000mg twice daily. Last week he was exercising and halfway through, he stopped because he was feeling extremely weak and was sweating profusely. He took his blood glucose and it was 68. He wants to know if this is a common symptom because of his medication.

Sulfonylureas
• Enhance insulin secretion – bind SUR receptors on pancreatic β cells– results in suppressed hepatic glucose production
• Classification: 1st & 2nd generation – differences in potency, adverse effects– no therapeutic superiority among agents
• Glyburide– requires adjustment for renal dysfunction; higher risk
of hypoglycemia

SulfonylureasIn
suli n
Ef fe
c t
B L D HS B
Type 2 DM
Sulfonylurea

SulfonylureasGeneric Name Dose
(mg)Recommended Starting Dosage
(mg/day)
Equivalent Therapeutic Dose (mg)
Maximum Dose
(mg/day)
Duration of Action
Metabolism or Therapeutic Notes
Nonelderly Elderly
1st Generation
Acetohexamide 250, 500 250 125–250 500 1,500 Up to 16 hours
Metabolized in liver; metabolite potency equal to parent compound; renally eliminated
Chlorpropamide 100, 250 250 100 250 500 Up to 72 hours
Metabolized in liver; also excreted unchanged renally
Tolazamide 100, 250, 500
100–250 100 250 1,000 Up to 24 hours
Metabolized in liver; metabolite less active than parent compound; renally eliminated
Tolbutamide 250, 500 1,000–2,000 500–1,000
1,000 3,000 Up to 12 hours
Metabolized in liver to inactive metabolites that are renally excreted
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th Edition: http://www.accesspharmacy.com

SulfonylureasGeneric Name Dose
(mg)Recommended Starting Dosage
(mg/day)
Equivalent Therapeutic Dose (mg)
Maximum Dose
(mg/day)
Duration of Action
Metabolism or Therapeutic Notes
Nonelderly Elderly
2nd Generation
Glipizide 5, 10 5 2.5–5 5 40 Up to 20 hours
Metabolized in liver to inactive metabolites
Glipizide 2.5, 5, 10, 20
5 2.5–5 5 20 24 hours Slow-release form; do not cut tablet
Glyburide 1.25, 2.5, 5
5 1.25–2.5 5 20 Up to 24 hours
Metabolized in liver; elimination ½ renal, ½ feces
Glyburide, micronized
1.5, 3, 6 3 1.5–3 3 12 Up to 24 hours
Equal control, but better absorption from micronized preparation
Glimepiride 1, 2, 4 1–2 0.5–1 2 8 24 hours Metabolized in liver to inactive metabolites
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th Edition: http://www.accesspharmacy.com

Sulfonylureas
• Most common side effect: hypoglycemia – Higher with chlorpropamide & glyburide – High risk patients require lower doses
• elderly• renal/hepatic disease• patients that skip meals• vigorous exercise • substantial weight loss
• Weight gain also common (~3kg)• Less common adverse effects: rash, GI upset

Sulfonylureas
• Titrate sulfonylureas doses every 1 to 2 weeks• Maximal effective dose ~60 to 75% stated max
dose• At equipotent doses, all sulfonylureas equally
effective at lowering blood glucose

Sulfonylureas
• Average HbA1c reduction: 1.5 to 2%• FBG reduction: 60 to 70 mg/dL• Most patients do not reach glycemic goal with
monotherapy– 1˚ failure: < 30 mg/dL drop in FBG
• low C-peptide • high (> 250 mg/dL) FBG
– 2˚failure: good initial response, but insufficient to reach or maintain glycemic goal
• 5 to 7% per year failure rate

Sulfonylureas SummaryMedication(A1C reduction)
Mechanism of Action Comments
Glyburide; Glibenclamide
Glipizide
Glimepiride
Gliclazide
(1.5% to 2%)
Stimulates insulin release from the β-cells of the pancreas
May cause weight gain
High propensity for hypoglycemic episodes

Meglitinides
Generic Name
Dose (mg)
Recommended Starting Dosage
(mg/day)
Maximum Dose
(mg/day)
Duration of Action
Metabolism or Therapeutic Notes
Nonelderly Elderly
Nateglinide 60, 120 120 with meals
120 with meals
120 mg three times a day
Up to 4 hours
Metabolized by cytochrome P450 (CYP450), CYP2C9, and CYP3A4 to weakly active metabolites; renally eliminated
Repaglinide 0.5, 1, 2 0.5–1 with meals
0.5–1 with meals
16 Up to 4 hours
Metabolized by CYP3A4 to inactive metabolites; excreted in bile
• Stimulate insulin secretion from pancreatic β cells– require presence of glucose
• Similar mechanism to sulfonylureas– faster onset, shorter duration
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th Edition: http://www.accesspharmacy.com

MeglitinidesIn
suli n
Ef fe
c t
B L D HS B
Type 2 DM
Meglitinide

Meglitinides• Most common adverse effect: hypoglycemia
– less than with sulfonylureas• Weight gain may occur
– repaglinide: 2 to 3 kg– nateglinide: < 1 kg
• CYP3A4 inducers or inhibitors may interact with repaglinide
• May use in patients with renal insufficiency• Use with caution in severe hepatic impairment

Meglitinides• May be used as monotherapy or in combination with
metformin or TZDs in Type 2 DM• Dose up to 30 min prior to each meal
– dose can be skipped if a meal is skipped– meals low in carbohydrates may not need a dose
• Average HbA1c reduction < 1%– Reduces FBG by ~60mg/dL
• Useful in reducing postprandial glucose excursions in patients close to glycemic goals
• Patients having a poor response to sulfonylurea therapy are not likely to respond if these drugs are added

Repaglinide vs. Nateglinide Monotherapy
Diabetes Care 2004;27:1265-1270

Meglitinides SummaryMedication(A1C reduction)
Mechanism of Action Comments
Repaglinide
Nateglinide
(0.5% to 1%)
Stimulates the release of insulin from the β-cells of the pancreas
• Shorter acting than the SUs
• Taken with meals • The dose should be
skipped if the meal is skipped
• Lower risk of hypoglycemia than with SUs
• May cause weight gain

α-Glucosidase Inhibitors• Competitively inhibit enzymes in the small intestine
– delay sucrose & complex carbohydrate breakdown
• Absorption of glucose is delayed to the distal portion of the small intestine resulting in a reduction of “peak” postprandial blood glucose concentrations
• Reduce postprandial hyperglycemia
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th Edition: http://www.accesspharmacy.com
Generic Name
Dose (mg) Recommended Starting Dosage (mg/day)
Maximum Dose (mg/day)
Duration of Action
Metabolism or Therapeutic Notes
Nonelderly Elderly
Acarbose 25, 50, 100 25 mg one to three times a day
25 mg one to three times a day
25–100 mg three times a day
1–3 hours Eliminated in bile
Miglitol 25, 50, 100 25 mg one to three times a day
25 mg one to three times a day
25–100 mg three times a day
1–3 hours Eliminated renally
28

Without Pharmacotherapy
α-Glucosidase InhibitorsWith
Pharmacotherapy

α-Glucosidase InhibitorsPostprandial Blood Glucose in Human Volunteers
0 30 60 90 120 150 180
Time (Min.)
(mg/
dl)
Without Precose With Precose

31
α-Glucosidase Inhibitors
• Adverse effect:– GI side effects most common
• flatulence, bloating, abdominal discomfort, diarrhea
– May elevate serum aminotransferase • Contraindications:
– IBD– colonic ulceration– intestinal obstruction– cirrhosis

32
α-Glucosidase Inhibitors
Efficacy– Reduce postprandial glucose 40 to 50 mg/dL– FBG relatively unchanged (~10% reduction)– Average HbA1c reduction: 0.3 to 1%– Beneficial in patients close to target HbA1c with
near-normal FBG but high postprandial levels– Do not affect the absorption of simple sugars such
as glucose and lactose

33
α-Glucosidase Inhibitor
• May be monotherapy or used with metformin, sulfonylureas, insulin
• Initiate with very low dose – 25 mg with one meal a day
• Increase gradually to maximum dose– 50 mg TID patients ≤ 60 kg– 100 mg TID patients > 60 kg
• Take with 1st bite of a meal

Alpha-glucosidase InhibitorsMedication(A1C reduction)
Mechanism of Action Comments
Acarbose
Miglitol
(0.3% to 1%)
• Delays the breakdown of complex carbohydrates into glucose
• The absorption of glucose is delayed in the distal portion of the small intestine
• Can cause flatulence, abdominal pain, diarrhea
• Not as effective as the other oral agents
• Considered 2nd or 3rd line therapy

TZDs: Thiazolidinediones • May be used in type 2 DM therapy• Enhance insulin sensitivity at muscle, liver, fat tissues• Decrease hepatic glucose production• Requires presence of insulin
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th Edition: http://www.accesspharmacy.com
Generic Name
Dose (mg) Recommended Starting Dosage (mg/day)
Maximum Dose
(mg/day)
Duration of Action
Metabolism or Therapeutic Notes
Nonelderly Elderly
Pioglitazone 15, 30, 45 15 15 45 24 hours Metabolized by CYP2C8 and CYP3A4; two metabolites have longer half-lives than parent compound
Rosiglitazone
2, 4, 8 2–4 2 8 mg/day or 4 mg twice a
day
24 hours Metabolized by CYP2C8 and CYP2C9 to inactive metabolites that are renally excreted
35

Thiazolidinediones
• Usual reduction in HbA1c of 1.5% - 2.5%• Decreases in blood glucose can be seen within 2-4
weeks• Maximum glucose lowering effects may take up to 12
weeks• Demonstrated perseverance of effect for up to 1-2
years
37
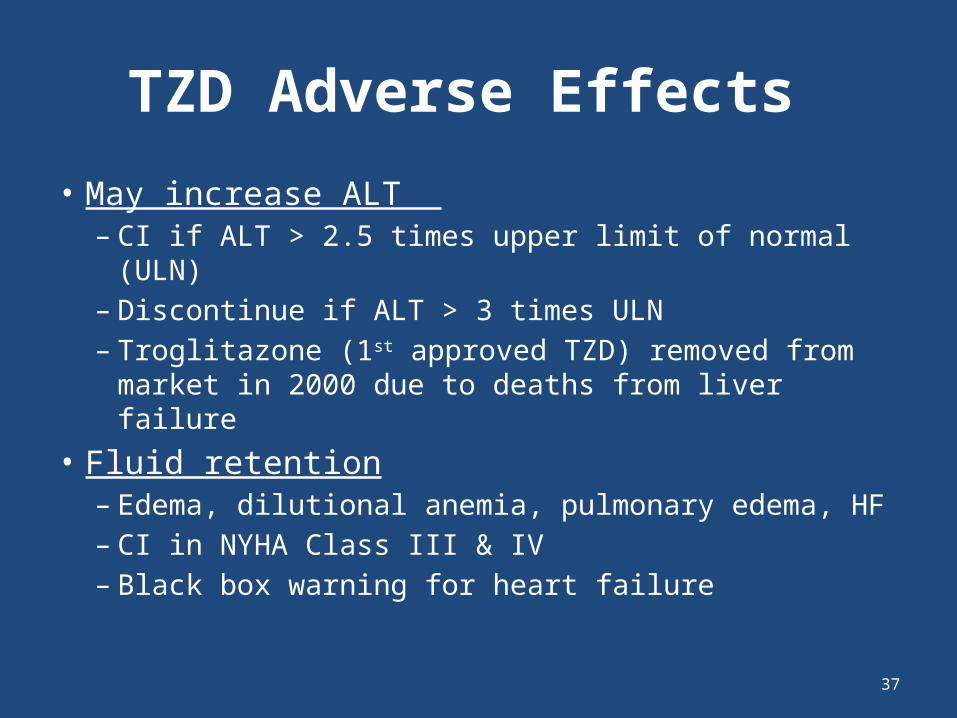
TZD Adverse Effects
• May increase ALT – CI if ALT > 2.5 times upper limit of normal (ULN)– Discontinue if ALT > 3 times ULN– Troglitazone (1st approved TZD) removed from
market in 2000 due to deaths from liver failure• Fluid retention
– Edema, dilutional anemia, pulmonary edema, HF– CI in NYHA Class III & IV– Black box warning for heart failure

38
TZD Adverse Effects
• Weight Gain– 1.5 to 6 kg – Fluid retention & fat accumulation
• Increased fracture risk – upper & lower limbs of postmenopausal women
• Ovulation– aovulatory patients can resume ovulation – pregnancy & contraception precautions required– pregnancy category C

39
TZDs
• Average HbA1c reduction ~1.5%• FBG reduction: 60 to 70 mg/dL at max doses• Maximal glycemic-lowering effects after 3 to 4 months• Triglycerides:
– pioglitazone: 10 to 20% decrease– rosiglitazone: neutral effect
• LDL: – pioglitazone: no significant increase– rosiglitazone: 5 to 15% increase
• HDL: both increase 3 to 9 mg/dL
39

Thiazolidinediones SummaryMedication(A1C reduction)
Mechanism of Action Comments
Rosiglitazone
Pioglitazone
(1.5% to 2.5%)
• Improves insulin sensitivity in skeletal muscle and adipose tissue
• Decreases hepatic glucose output
• FDA-imposed restricted use of rosiglitazone due to cardiovascular ischemic risk
• Risk of bladder cancer with pioglitazone
• Long onset and prolonged effects after discontinuation
• Can cause weight gain, edema, and worsen CHF

“Incretin Effect”
Normal Weight: Non-Diabetic Subjects Normal Weight: Diabetic Subjects
Plasma Insulin Responses to Oral and Intravenous Glucose
Oral GlucoseIntravenous Glucose
Non-Diabetic Subjects (glucose range 3.9-6.7 mmol/L)Diabetic Subjects (glucose range 4.7-12.2 mmol/L)
Oral GlucoseIntravenous Glucose
Data from: Perley M, et al. J Clin Invest 1967; 46:1954-1962
60
Pla
sma
Insu
lin
(U
/mL
)
30
0
0 60 120 18030 90 150 0 60 120 18030 90 150
90
Pla
sma
Insu
lin
(U
/mL
)
60
30
0
90
Time (min)Time (min)

Incretins
•Peptide hormones secreted byenteroendocrine cells in the GI tract
•Modulate pancreatic islet secretions
•Other effects on nutrient homeostasis
•Two major incretins that affect glucose metabolism
– GLP-1: glucagon-like peptide-1
– GIP: glucose-dependent insulinotropicpolypeptide

GLP-1•Produced by intestinal L-cells, which are locatedpredominately in the ileum and colon (distalportion of the gut)
•Potent insulinotropic hormone
•Plasma levels increase rapidly in response tomeals (carbohydrate & lipid)
•Once secreted it is rapidly inactivated by dipeptidyl peptidase IV (DPP-IV) t1/2 ~ 2 min
•Type 2 DM & Impaired Glucose Tolerance (IGT)present with lower plasma GLP-1 compared tohealthy controls

GLP-1 Secretion and Metabolism
Mixed Meal
Intestinal GLP-1 Release
Plasma
GLP-1 (7-36)Active
DPP-IV
GLP-1(9-36)Inactive
GLP-1 Actions
Rapid Inactivation
(>80% of pool)
Renal Clearance
DPP-IV = Dipeptidyl peptidase-IVDeacon CF, et al. Diabetes. 1995;44:1126-1131.

GLP-1 Modes of Action in Humans
GLP-1 is secretedfrom the L-cellsin the intestine
This in turn…
• Stimulates glucose-dependent insulin secretion
• Suppresses glucagonsecretion
• Slows gastric emptying
Long term effectsdemonstrated in animals…
• Increases beta-cell mass and maintains beta-cell efficiency
• Reduces food intake
Upon ingestion of food…
Drucker DJ. Curr Pharm Des 2001; 7:1399-1412Drucker DJ. Mol Endocrinol 2003; 17:161-171

Strategies to Enhance Incretin Action in Diabetes
• Glucagon-like peptide-1 (GLP-1) analogues*
• Exenatide (synthetic Exendin-4)*
• Dipeptidyl peptidase-IV (DPP-IV) inhibitors
* Incretin mimetic agents

DPP-IV Inhibitors
Mixed Meal
Intestinal GLP-1 Release
Plasma
GLP-1 (7-36)Active
DPP-IV
GLP-1(9-36)Inactive
GLP-1 Actions
Rapid Inactivation
(>80% of pool)
Renal Clearance
DPP-IV = Dipeptidyl peptidase-IVDeacon CF, et al. Diabetes. 1995;44:1126-1131.
↑ Activity
Incretin Enhancement

DPP-IV Inhibitors
• Inhibit DPP-IV which degrades GLP-1– prolongs GLP-1 t½ – GLP-1 deficient in type 2 DM
• Partially reduces elevated postprandial glucagon • Stimulates glucose-dependent insulin secretion
48

49
DPP-IV Inhibitors
• May be used as monotherapy or in combination therapy
• Average HbA1c reduction 0.7 to 1.0% • Mild hypoglycemia may occur• Postmarking reports of serious hypersensitivity
reactions – anaphylaxis– angioedema– exfoliative skin conditions (Stevens-Johnson syndrome)

Dipeptidyl peptidase-4 (DPP-4) Inhibitors Summary
Medication(A1C reduction)
Mechanism of Action Comments
Linagliptin
Saxagliptin
Sitagliptin
Vildagliptin
(0.7% to 1%)
• Inhibits the degradation of endogenous incretins which increases insulin secretion
• Decreases glucagon secretion
• Weight neutral• Rare instances of
hypoglycemia• Considered 2nd line
therapy• Reports of acute
pancreatitis

Non-insulin Injectable Medications

0 3 6 9 12
0
100000
200000
300000
400000
Time After Meal (h)
Pla
sma
Exe
nd
in-4
Co
nce
ntr
atio
n (
pg
/mL
)
Exendin-4 in the Gila Monster
• Exendin-4 was originallyisolated from thesalivary secretions ofthe Gila monster
• Exendin-4 wassubsequently found tocirculate as a meal-related peptide in this animal
• Exendin-4 has possibleendocrine function in thelizard Heloderma suspectum(Gila monster)
Data from: Young AA. Glucagon-like peptide-1, exendin and insulin sensitivity. In Hansen B, Shafrir E, Editors. Insulin Resistance and Insulin Resistance Syndrome. 1st ed. Harwood Academic Press; 2002, 235-262
4 mice1 rat

Exenatide: Clinical Pharmacology
Adverse Effects:• Nausea• Jittery• Dyspepsia
• Vomiting• Dizziness• Hypoglycemia (with sulfyl use)
• Diarrhea• Headache• Weight Loss
Dosage:• 5 μg BID within a 60-minute period before the morning and evening meals
• Based on clinical response dosage may be increased to 10 μg BID after 1 month of therapy
Storage:• Exenatide should be refrigerated (at all times) at 36º F to 46º F, protected
from light
• Pen should be discarded 30 days after first use, even if some drug remains in the pen

54
Exenatide
• Average HbA1c reduction ~0.9%• Significantly decreases postprandial glucose
excursions• Modest effects on FBG• Average weight loss in studies: 1 to 2 kg over 30
weeks – long-term, open-labeled trials show continued weight
loss for at least 2.5 years with 10 mcg BID dose• Improvements in triglycerides & HDL seen with
exenatide 10 mcg BID54

Nausea Is Dose-dependent and Decreases Over Time
Buse JB, et al. Diabetes Care. 2004;27:2628-2635.
0
5
10
15
20
25
30
0-4 >4-8 >8-12 >12-16 >16-20 >20-24 >24-28 >28
Treatment (wk)
Inci
den
ce o
f N
ause
a (%
IT
T S
ub
ject
s)
10 µg5 µgPlacebo
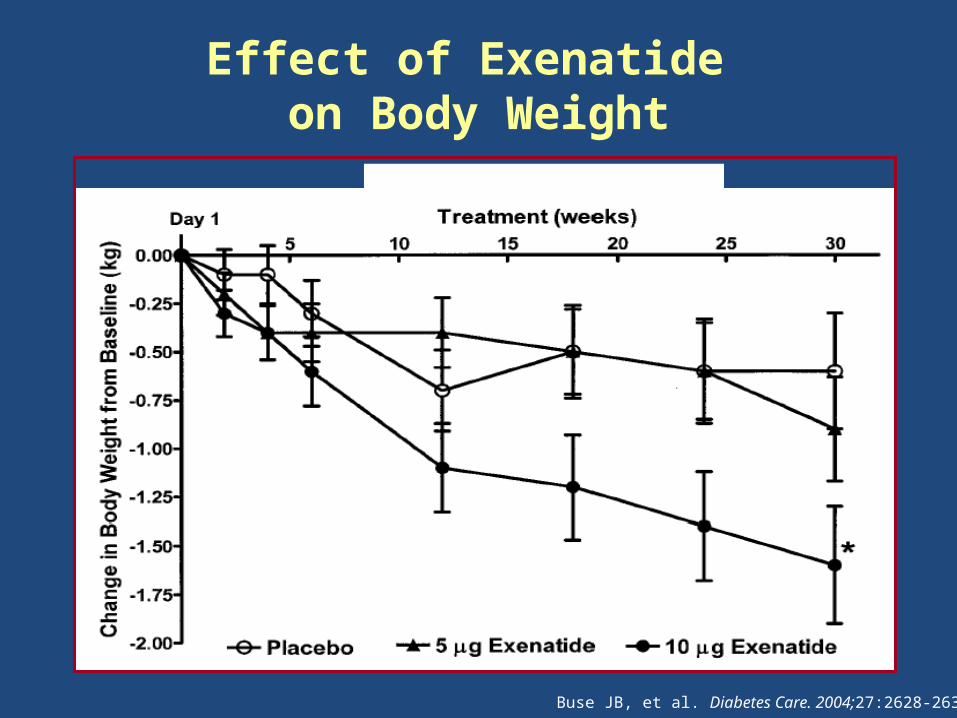
Effect of Exenatide on Body Weight
Buse JB, et al. Diabetes Care. 2004;27:2628-2635.

Once-daily injection of Liraglutide covers 24-h BG profile in type 2 diabetes
Adapted from: Degn et al. Diabetes 2004;53: 1187-1194.
24-h glucose AUC(mmol/l/h, mean ± SE)
232.3 ± 21.9 187.5 ± 14.0 (p = 0.01)
Pla
sma g
luco
se (
mm
ol/l)
Injection (08.00)
Time after injection (hours)
00 4 8 12 16 20 24
6
8
10
12
14Placebo
Liraglutide (6 µg/kg OD)
n=13

Liraglutide Effect on FBG and Weight
Fasting serum glucose
Weight change
1
0
-1
-2
-3
0
-1
-2
-3
-4
mM %
p<0.0001
p<0.015
Key observations:• Observations from
liraglutide and metformin versus metformin and a sulfonylurea
• Effect observed in the absence of hypoglycaemia
• 1mM = 20 mg/dLLiraglutide and metforminGlimepiride and metformin

Liraglutide: Effect on Weight
Note: Data from the double-blind, double-dummy, randomised, parallel group dose titration phase 2 study including a total of 144 patients with an average HbA1c of 9.4-9.5%. All changes are from baseline; that is, FSG of 13.0-13.2 mM and an average weight of 91-94 kg.
• Glimepiride and metformin
Mean
ch
an
ge in
bod
y w
eig
ht
from
base
line (
%)
Time (weeks)
-3
-2
-1
0
1
2
0 1 2 3 4 5
Continuing weight loss
• Liraglutide and metformin
Summary• A 24-hour pharmacodynamic profile
– Once-daily injection due to 12 hr half-life• Multiple anti-diabetic actions
– Increases insulin and lowers glucagon secretion– Rapid and sustained glycaemic effect– Weight control– -cell mass increased in animal models– -cell function improved in type 2 diabetes
• Strictly glucose-dependent actions– Very low hypoglycemia risk (no major and few minor events)– Counter-regulatory response to hypoglycaemia not impaired
• Well-tolerated– Mild, transient GI-symptoms; no antibodies (12-week data)

Glucagon-like, peptide-1 (GLP-1) Mimetic
Medication(A1C reduction)
Mechanism of Action Comments
Exenatide
Exenatide weekly
Liraglutide
(1% to 1.5%)
• Stimulates GLP-1 receptors which increases production of insulin in response to high blood glucose levels
• Inhibits post-prandial glucagon release
• Slows gastric emptying
• Injections• Promotes weight loss• Nausea and diarrhea
are common• Induces satiety
62
Pramlintide
• Adjunctive therapy for patients using insulin• Synthetic analog of amylin
– neurohormone co-secreted from β-cells with insulin
• Suppresses postprandial glucagon secretion• Reduces food intake• Slows gastric emptying

63
Pramlintide
• Subcutaneous injection in abdomen or thigh – variable absorption with arm injection
• Adverse effects:– GI most common– nausea, vomiting, anorexia– may decrease over time– dose-related, slowly titrate dose upwards
• May delay absorption of other medications; slow gastric emptying

64
Pramlintide
• Reduce preprandial insulin dose 30 to 50% at pramlintide initiation
• Basal insulin dose may be reduced if FBG close to goal
• Dosing– Type 2: 60 to 120 mcg prior to meals– Type 1: 15 to 60 mcg prior to meals
• 2.5 units on 100 units/ml insulin syringe = 15 mcg of pramlinitide
65
Pramlintide
• Average HbA1c reduction 0.4 to 0.6%• Decreases prandial glucose excursions• Little effect of FBG concentrations• Main advantage in type 1 DM is that it
stabilizes wide postprandial glycemic swings• Average weight loss in controlled trials: 1 to 2
kg

Warnings and Precautions

Case 3: Non-Insulin Injectables
YO is a 52 y/o female with Type 2 DM and central obesity. She was recently started on liraglutide and is now taking 1.8mg daily. She is nauseous after eating and states that this occurs even with her favorite #1 and #3 meal combos from McDonalds. She states that she knows that her diet is not good. How do you respond?

Treatment Algorithm
3rd Agent
2nd Agent
1st Agent Metformin
SU
TZD or DDP-4 or GLP-1 or
insulin
TZD
SU or DPP-4 or GLP-1 or
insulin
DPP-4 inhibitor
SU or TZD or insulin
GLP-1 agonist
SU or TZD or insulin
Insulin (usu. Basal)
TZD or DPP-4 or GLP-1

69
Drug Combination Change in HbA1c (%)
Number of Studies
Number of Subjects
Sulfonylurea + metformin –2.2 8 458
Sulfonylurea + insulin –1.9 17 88
Meglitinide + thiazolidinedione –1.7 1 434
Metformin + insulin –1.7 8 138
Sulfonylurea + α-glucosidase inhibitor –1.6 3 177
Metformin + meglitinide –1.4 3 226
Insulin + α-glucosidase inhibitor –1.2 1 20
Insulin + thiazolidinedione –1.2 7 850
Sulfonylurea + thiazolidinedione –1.1 12 1,315
Metformin + exenatide –0.8 2 1,070
Metformin + vildagliptin –0.7 1 416
Metformin + thiazolidinedione –0.9 3 284
Metformin + α-glucosidase inhibitor –0.4 3 173
Add-Ona Dual Therapy: Average HbA1c Reduction
aReductions are averages and do not imply superiority or inferiority of a combination.

Medication-specific TherapyHigh HbA1C, High FBG High HbA1C, Goal FBG, High PPBG
FASTING/BASAL POST-PRANDIAL
• Metformin• TZDs• Sulfonylureas• NPH Insulin• Long-acting insulins• Liraglutide
• Glinides• Α-glucosidase inhibitors• Colesevelam• DPP-4 inhibitors• Incretin mimetics
• (exenatide > liraglutide)• Fast/rapid acting insulins• Pramlintide

Diabetes Mellitus
Ibrahim Sales, Pharm.D.Assistant Professor of Clinical Pharmacy
King Saud [email protected]