pancreatic hormones & antidiabetic drugs shi-hong zhang 张世红 [email protected]
TRANSCRIPT

胰高血糖素胰岛素生长抑素

Overview of Glucose Regulation by Insulin
Amended from Dinneen SF. Diabetes Med. 1997;14(suppl 3):S19-24.
Insulin secretion
Glucose disposal ↑
Persistent hepatic glucose
output ↓
Glucose absorption
Lipogenesis↑
Lipolysis↓
Glycogenesis ↑
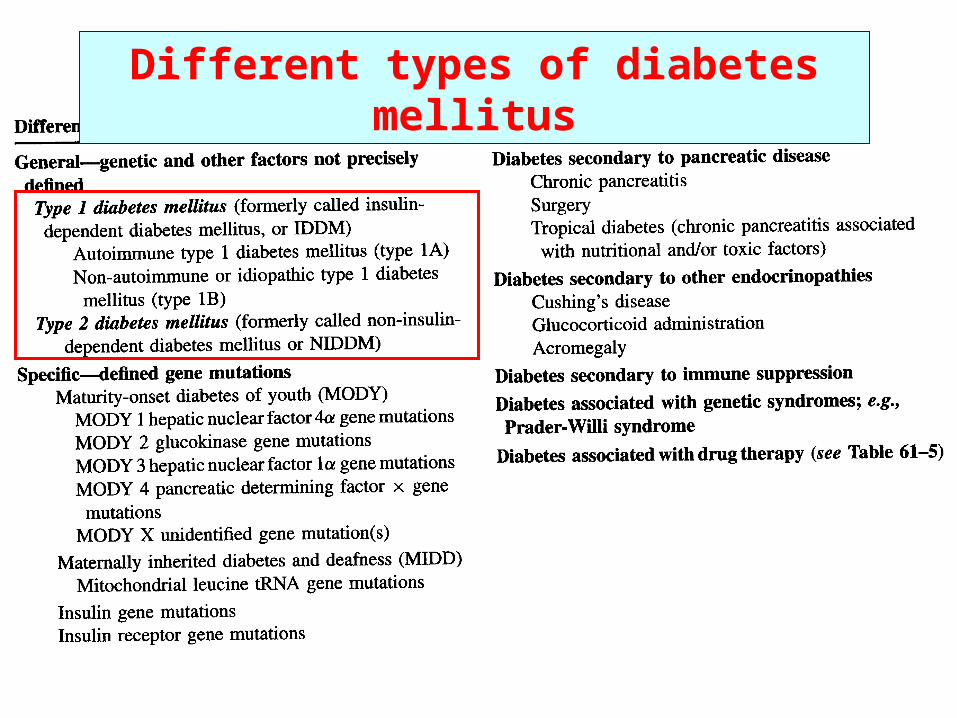
Different types of diabetes mellitus

“Beta-cell failure”
prediabetic metabolic syndrome

Symptoms
of diabetes

Complications of diabetes mellitus
• Acute complications– Diabetic ketoacidosis ( 酮症酸中毒 )
– Hyperosmotic nonketotic coma ( 高渗性非酮症性昏迷)
• Chronic complications– Cardiovascular diseases– Renal damage– Retinal damage– Nerve degeneration– Infection – Myopathy – etc.

Pharmacological therapy Insulin Oral hypoglycemic drugs
Insulin sensitizers 胰岛素增敏剂 :Biguanides 双胍类Thiazolidinediones (TDs,噻唑烷二酮类 )
Insulin secretagogues (促胰岛素分泌药 ):Sulfonylureas 磺酰脲类Meglitinides (Non-SU) 格列奈类GLP-1 agonists and DPP-4 inhibitors
α-glucosidase inhibitors α-葡萄糖苷酶抑制剂 Amylin analogue 胰淀粉样多肽类似物 Aldose reductase inhibitor 醛糖还原酶抑制剂

A.A. Insulin Insulin

Frederick Sanger (1918- 2013)

A. Insulin
1. Pharmacological effects(1) Carbohydrate metabolism: reduces blood glucose levels by
glycogenolysis , glycogen synthesis , gluconeogenesis , glucose transport .(2) Lipid metabolism: fat synthesis , lipolysis , plasma free
fatty acids , ketone bodies .(3) Protein metabolism: active transport of amino acids , incorporation of amino acids into protein , protein catabolism (4) Cardiac stimulation
(5) Promote cellular K+ uptake

Mechanism of insulin actions: Interact with insulin receptors

2. Clinical uses(1) Type I diabetic mellitus
(2) Type II diabetic mellitus : extreme high blood
glucose or after failure to other drugs
(3) Diabetic complications: diabetic ketoacidosis ( 酮症酸中毒 ), hyperosmotic nonketotic coma (高渗性非酮症性昏迷) (4) Critical situations of diabetic patients: fever,
severe infection, pregnancy, trauma, operation
(5) Promotion of K+ uptake into the cells
A. Insulin

3. Preparations
Fast-acting insulin
Regular insulin 正规胰岛素Monocomponent insulin 单组分胰岛素
• High solubility• Can be given intravenously• Start working 0.5-1h after injection, reach peak 2-4h,
and last 5-7h.
A. Insulin
3. PreparationsFast-acting insulin analogs
Insulin aspart 门冬胰岛素 ( B28 脯氨酸变为门冬氨酸)Insulin lispro 赖脯胰岛素(颠倒 B28 、 29 脯赖顺序)
•Start working 5-15 minutes after injection, reach peak at
1h, and last ~4 hours. • Used for IDDM and NIDDM with high postmeal glucose.
A. Insulin

3. Preparations
Intermediate-acting insulin (lente)
Neutral protamine hagedorn (NPH, isophane insulin )
中性(低)精蛋白锌胰岛素Globin zinc insulin 珠蛋白锌胰岛素
• Start working 1-1.5h after injection, reach peak 8-12h,
and last 24h.
A. Insulin

3. PreparationsLong-acting insulin (ultralente)
Protamine zinc insulin (PZI) 精蛋白锌胰岛素
• Start working 4-8h after s.c. injection, reach peak 14-
20h, and last 24-36h.
A. Insulin
3. Preparations
Super-long acting insulin analogsInsulin glargine 甘精胰岛素( B 链 C 端加两个精氨酸, A21 甘氨酸替代门冬酰
胺)
Insulin detemir 地特胰岛素(去除 B30 苏氨酸, B29 赖氨酸加脂肪酸侧链)
•Less soluble than native human insulin at physiological pH,
and precipitates in skin following subcutaneous injection,
resulting in delayed absorption.
•Onset 1-2 h after injection and continues to work for as long
as 24 hours.
• Used to treat type 1 or type 2 diabetes mellitus.
A. Insulin

3. PreparationsMixed insulin
Human insulin isophane 低精蛋白锌胰岛素 +
Human insulin 人胰岛素
• Start working 0.5h after injection, reach peak 2-12h,
and last 16-24h.
A. Insulin


• For patients who eat meals out, may consider use of an insulin pen.
• Most insulins now available as pen

Insulin Pump and Glucose Monitoring
Insulin Pump – “Open Loop”Patient sets basal infusion rate and superimposedboluses
Continuous Glucose Monitor
“Closed Loop” insulin pump system is ultimate goal: infusion rate adjusted based on input from continuous glucose monitor.

4. Adverse effects
(1) Hypoglycemia: adrenaline secretion (sweating,
hunger, weakness, tachycardia, blurred vision, headache,
etc.), treated with 50% glucose.
(2) Hypersensitivity: treated with H1 antagonists,
glucocorticoids
(3) Insulin resistance: acute, chronic
(4) Lipoatrophy 脂肪萎缩 and lipohypertrophy 脂肪增生(5) Others: weight gain, refractive errors ( 屈光不正 ), edema
A. Insulin

B. Oral hypoglycemic drugs Insulin action enhancers 胰岛素增敏剂 :
Biguanides 双胍类Thiazolidinediones (TDs ,噻唑烷二酮类 )
Insulin secretagogues (促胰岛素分泌药) :Sulfonylureas 磺酰脲类Meglitinides (Non-SU) 格列奈类 ( 苯丙胺酸衍生物 )GLP-1 agonists and DPP-4 inhibitors
α-glucosidase inhibitors α- 葡萄糖苷酶抑制剂 Amylin analogue 胰淀粉样多肽类似物 Aldose reductase inhibitor 醛糖还原酶抑制剂

Biguanides (双胍类) Metformin 二甲双胍Thiazolidinediones (TZDs) 噻唑烷酮类化合物 Rosiglitazone 罗格列酮 Pioglitazone 吡格列酮
Insulin action enhancers

Increases insulin
sensitivity, enhances
glucose uptake in fat
tissues and anaerobic
glycolysis in skeletal
muscles;
Decreases glucose
absorption in gut and
glucagon release,
inhibits hepatic
gluconeogenesis
Metformin
1. Pharmacologicla effects

2. Clinical uses First line drug for type II diabetes, esp. patients with obesity;
polycystic ovary syndrome
Major advantages: lack of weight gain, absence of
hypoglycemia, decrease in risk of CV events, low cost with
generic prep.
3. Adverse effects
GI reactions, severe lactic acidosis, malabsorption of vitamin
B12 and folic acid
Metformin

1. Pharmacological effects Selective agonists for nuclear peroxisome proliferator
activated receptor- (PPAR , 过氧化物酶增殖体激活受体 ),
increase glucose transport into muscle and adipose
tissue.
(1) Lower insulin resistance
(2) Lipid metabolism regulation: TG, free fatty acid
(3) Prevent diabetic complications: anti-platelet, renal
protection, anti-atherosclerosis
(4) Improve cell function
Thiazolidinediones


2. Clinical uses•Used for treatment of insulin-resistant diabetic
patients or type 2 patients;•Delayed onset of action – takes 8-12 weeks to
achieve maximal effect;•Absence of hypoglycemia when used as
monotherapy;•No reliance on renal excretion
Thiazolidinediones

3. Adverse effects Edema: at higher doses and used with insulin, in older
patients, patients with multiple medical problems, patients
with underlying CAD or CHF
Increased risk of cardiac events
Headache
Myalgia ( 肌痛 )
GI reactions
Hepatic damage (troglitazone).
Contraindicated with Class III or IV heart failure or significant
liver disease.
Thiazolidinediones

Tolbutamide (D860) 甲苯磺丁脲Chlorpropamide 氯磺丙脲Gliburide 格列本脲 (优降糖)Glipizide 格列吡嗪(美吡达)Gliclazide 格列齐特 (达美康)Glimepiride 格列美脲(亚莫利)
Sulfonylureas (磺酰脲类)

1. Pharmacological effects 1) Increase insulin release: block ATP sensitive K+
channel, Ca2+ inflow
Sulfonylureas

1. Pharmacological effects 2) Increase receptor affinity to insulin (long-
term use)
3) Promote glucose uses (促进合成糖原和脂肪) 4) Increase sensitivity of β cells to glucose
5) Anti-uretic effect ( 格 列 本 脲 / 氯磺 丙脲 ) :ADH 6) Anti-platelet effect ( 格列齐特 )
Sulfonylureas

2. Clinical uses
(1) Type II diabetic mellitus: first line oral
hypoglycemic drug, alone or combined with
insulin
(2) Diabetes insipidus ( 尿崩症 ): 氯磺丙脲
Sulfonylureas

3. Adverse effects
(1) GI reactions
(2) CNS reactions (嗜睡、眩晕)(3) Hypoglycemia: especially in elderly, with hepatic or renal insufficiencies
(4) Others: leukopenia ( 白细胞减少 ), cholestatic jaundice ( 胆汁郁积性黄疸 ), hepatic damage
Sulfonylureas
• Act by binding to SUR1 on beta cells to promote insulin
secretion. • Repaglinide ( 瑞格列奈 ) and Nateglinide ( 那格列奈 ) are
currently available agents. • Efficacy of repaglinide appears to be similar to SU’s• Major advantage is rapid onset and offset, can dose just
prior to meals with better postmeal control.• Lower risk to induce hypoglycemia than SUs.• Are additive with metformin (二甲双胍 ).• Used for type 2 patients.
Non-SU Insulin Secretagogues

• Hepatic metabolism permits use in patients with
impaired renal function.
• Many drug interactions. Most concerning is gemfibrozil
(吉非罗齐 ) which increases repaglinide concentration
and may result in prolonged effect.
• Cost may be an issue (1 or 2 mg tabs: $122.09/month
at drugstore.com)
Non-SU Insulin Secretagogues

• GLP-1: glucogons-like protein-1
• Exenatide (依可那肽 ): GLP-1
agonist , stimulates insulin secretion, only
available as injection.
• Sitagliptin (西他列汀 ), vildagliptin (维格列汀 ): DPP-4(二肽基肽酶Ⅳ) inhibitor.
GLP-1 agonists and DPP-4 inhibitors


Acarbose-Precose 阿卡波糖 Miglitol-Glyset 米格列醇 Voglibose 伏格列波糖
Alpha-Glucosidase inhibitors

Alpha-Glucosidase inhibitors
• Acarbose (阿卡波糖 ) is an oligosaccharide (低聚糖 ),
hardly absorbed• Miglitol (米格列醇 ) resembles a monosaccharide, fairly
well-absorbed. • Reducing intestinal absorption of starch (淀粉 ), dextrin (糊
精 ), and disaccharides (二糖 ) by inhibiting the action of
intestinal brush border -glucosidase(葡萄糖苷酶) .• Acarbose also blocks pancreatic alpha-amylase (淀粉酶 ).• Used for diabetes mellitus type 2, particularly with regard to
postprandial餐后的 hyperglycemia.

• Must be taken at the start of main meals to have maximal
effect. • Efficacy will depend on the amount of complex
carbohydrates in the meal.• Absence of hypoglycemia when used as monotherapy. • Side effects: gastrointestinal side effects such as flatulence
and diarrhea; voglibose (伏格列波糖 ), in contrast to
acarbose, has less of GI side effects and more economical.
Alpha-Glucosidase inhibitors

Amylin analogues淀粉样多肽类似物
• Mechanism of action: – Inhibits glucagon secretion, thereby reducing hepatic glucose
production– Slows gastric emptying– Promotes satiety reduces caloric intake
• Pramlintide (Symlin普兰林肽 ) is the only amylin analog on
the market• As adjunct therapy for patients with type 1 or 2 diabetes to
control postprandial glucose• Increases the risk of severe hypoglycemia • The other main side effect is nausea.
Riddle and Drucker. Diabetes Care 2006; 29:435-49.

Alsose reductase inhibitors醛糖还原酶抑制剂
– Rational: aldose reductase activity increases in
those tissues that are not insulin sensitive,
including lenses, peripheral nerves and
glomerulus, may be involved in diabetic
complications.– Epalrestat (依帕司他 ) inhibits aldose reductase,
delay the progression of diabetic neuropathy
and ameliorate the associated symptoms of the
disease.


中国 2 型糖尿病防治指南( 2013 年版)

Case report
• A 45-year-old man first consulted his physician because of nocturia
(夜尿 ), mild thirst, and some fatigue. At the time, he was somewhat
overweight and sedentary (久坐 ) in his habits. Laboratory tests
showed an elevated fasting blood glucose level of 15 mmol/L,
glucose but no ketones in the urine. Diabetes was diagnosed and
he was placed on diabetic diet low in free sugar and fat. Two
months later, he was found to have higher fasting blood glucose, 2-
hr postlunch glucose, glycosylated hemoglobin (HbA1C). Therefore,
He was started on glyburide 5mg before breakfast and 5 mg before
dinner, but the blood glucose remained elevated. The dosage was
therefore raised to 10 mg twice daily, and this achieved a good
result.

Case report
• After 3 years, he developed unstable angina pectoris, and the blood
glucose and HbA1C levels were again found to be elevated. Addition of
metformin to his treatment produced some improvement, but his cardiac
symptoms gradually worsened over the next 3 years. He showed
intermittent glycosuria and proteinuria. His weight had fallen to a normal
level. His physician therefore decided to transfer him to insulin therapy,
started on a regimen of 22 units of Lente insulin and 12 units of regular
insulin every morning before breakfast. The dosage was gradually raised
to 35 units according to the glucose level in the blood and urine. During
the next year he had three mild hypoglycemic reactions. He was found
to have stable background retinopathy, mild nephropathy and mild
numbness and tingling in both feet, but the blood pressure remained
normal.