outpatient opioid treatment center –...
TRANSCRIPT

Outpatient Opioid Treatment Center – 101

§ Opioids are drugs that act on the nervous system to relieve pain. Continued use and abuse can lead to physical dependence and withdrawal symptoms. Examples of opioids are painkillers such as; morphine, methadone, Buprenorphine, hydrocodone, and oxycodone. Heroin is also an opioid and is illegal.
§ Opioid drugs sold under brand names include: OxyContin®, Percocet®, Vicodin®, Percodan®, Tylox® and Demerol® among others.
§ The most abused form of opiates is heroin. Heroin is processed from morphine. Heroin is typically sold as a white or brownish powder or as the black sticky substance known as "Black Tar Heroin."
§ Opiates are part of the agonist family of drugs. An agonist is a chemical that binds to a specific receptor and produces either excitation or inhibition of action potentials.


Other drug names and information to be aware of: § Black Tar Heroin § Pinky § Carfentanil § Benzodiazepines

§ In just a year, overdose deaths from opioid painkillers and heroin jumped 14%, hitting record levels in 2014, according to a new Centers for Disease Control and Prevention report. Between 2000 and 2014, nearly half a million Americans died from overdoses involving these drugs.
§ The most commonly prescribed opioid painkillers — like oxycodone and hydrocodone — were involved in more overdose deaths than any other type of the drug. Those deaths rose by 9%.
§ According to the report, two main shifts are driving the tragic trend:
§ More Americans are using opiate painkillers: Research suggests that one of the reasons that abusing opiates can make people more susceptible to future heroin abuse is because the drugs act similarly in the brain . A report released in July found that people who abused opiate painkillers were 40 times as likely to abuse heroin.
§ Inexpensive heroin has become more widely available: Heroin costs about one-fifth as much as most prescription opioids.

§ When someone injects, snorts, or smokes heroin, the brain converts it into morphine. Morphine binds to molecules on cells located throughout the brain and body called opioid receptors, which affect how we perceive pain and rewards.
§ This explains the surging sense of euphoria that many people feel when they inject the drug straight into the bloodstream. After the initial "rush," the skin gets flushed and warm, the arms and legs start to feel heavy, and thinking slows.
§ Because we also have opioid receptors in our brain stem — the body's main control center that is in charge of automatic processes such as blood pressure and breathing — overdosing on heroin can slow and even stop breathing, leading to brain damage or coma.



Short Term
§ A feeling of a "rush" - intensity if a function of how much drug is taken and how rapidly the drug enters the brain and binds to the natural opiod receptor.
§ Accompanying the rush are warm flushing of the skin, dry mouth, and a heavy feeling in the extremities, nausea, vomiting, and severe itching
§ Drowsiness
§ Slowing of cardiac function and breathing
§ Clouded mental state
§ Suppression of pain
§ Spontaneous abortion
Long Term § Addiction
§ Infectious diseases, for example HIV/AIDS
§ and Hepatitis B and C
§ Collapsed veins
§ Bacterial infections
§ Abscesses
§ Infection of the lining and heart valves


§ Opioid painkillers can have effects similar to heroin and morphine, especially when taken in ways other than prescribed by a doctor.
§ When prescription painkillers act on our brain's pleasure and reward centers, they can make us feel good. More importantly, though, they can work to reinforce behavior, which in some people can trigger a repeated desire to use.
§ You may also feel sleepy. Opioids act on multiple brain regions, but when they go to work in the locus ceruleus, a brain region involved in alertness, they can make us sleepy. Why? The drugs essentially put the brakes on the production of a chemical called norepinephrine, which plays a role in arousal.
§ You'll begin to feel their effects 10 to 90 minutes after use, depending on whether they're taken as directed or used in more dangerous ways Some drugmakers design versions of their medications to deter abuse. Extended-release forms of oxycodone, for example, are designed to release slowly when taken as directed. But crushing, snorting, or injecting the drugs can hasten their effects. It can also be deadly. Depending on the method used, the effect can last anywhere from four to 12 hours.
§ For severe pain, doctors typically prescribe opioid painkillers like morphine for a period of four to 12 hours, according to the Mayo Clinic. Because of their risks, it's important to take prescription painkillers only according to your physician's specific instructions.
Effects

§ Suddenly stopping the drugs can result in withdrawal symptoms like shakiness, vomiting, and diarrhea.
§ Taking prescription painkillers for an extended period increases the likelihood that your brain will adapt to them by making less of its own natural opioids. So when you stop taking the drugs, you can feel pretty miserable. For most people, this is uncomfortable but temporary.
§ But in people who are vulnerable to addiction, it can be dangerous because it can spurn repeated use.
§ "From a clinical standpoint, opioid withdrawal is one of the most powerful factors driving opioid dependence and addictive behaviors," Yale psychiatrists Thomas Kosten and Tony George write in a 2002 paperin the Journal of Addiction Science & Clinical Practice.


§ Scarred and/or collapsed veins
§ Bacterial infections of the blood vessels and heart valves
§ Abscesses (boils) and other soft-tissue infections
§ Liver or kidney disease
§ Lung complications resulting from the overall poor health of the abuser
§ Clogging in the blood vessels.
§ Arthritis or other rhematologic problems.
§ Hepatitis B and C
§ HIV
§ Other blood borne pathogens

§ Benzodiazepines in Combination with Opioid Pain Relievers or Alcohol: Greater Risk of More Serious ED Visit Outcomes
§ Benzodiazepines, such as alprazolam (Xanax®), diazepam (Valium®), clonazepam (Klonopin®), and lorazepam (Ativan®), depress central nervous system (CNS) activity and are used to relieve symptoms of anxiety, panic attacks, and seizures.1,2 They have been deemed safe and effective when taken as prescribed and directed. However, when combined with other drugs that depress CNS activity, such as alcohol or opioid pain relievers like oxycodone (OxyContin®), hydrocodone (Vicodin®), hydromorphone (Dilaudid®), or morphine, benzodiazepines may present serious or even life-threatening problems.
Benzodiazepines

§ Overdosing can stop breathing and cause brain damage, coma, or even death. Combining them with alcohol or other drugs — even when taken according to the directions — can be especially deadly. Since they slow breathing, combining opioid painkillers with other drugs (benzodiazepines) with similar effects can drastically raise the chances of accidental overdose and death. "Unfortunately, too many patients are still co-prescribed opioid pain relievers and benzodiazepines [tranquilizers]," the institute said.
§ Abusing opioid painkillers has been linked with abusing similar drugs, like heroin.
§ A CDC report found that people who'd abused opioid painkillers were 40 times as likely to abuse heroin compared with people who'd never abused them. The National Institute on Drug Abuse says that close to half of young people surveyed in three recent studies who'd injected heroin said they'd abused prescription painkillers before they started using heroin.
§ You may also develop a tolerance for the drugs so that you need more to get the same effect over time.
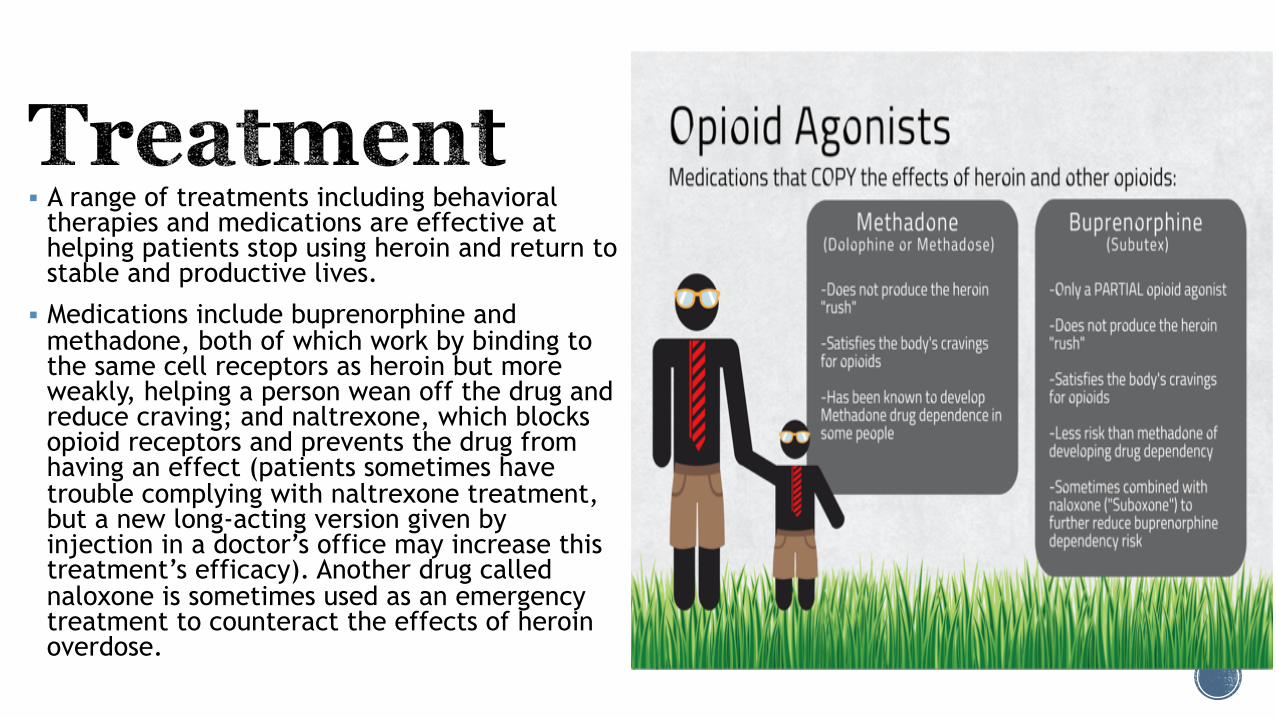
§ A range of treatments including behavioral therapies and medications are effective at helping patients stop using heroin and return to stable and productive lives.
§ Medications include buprenorphine and methadone, both of which work by binding to the same cell receptors as heroin but more weakly, helping a person wean off the drug and reduce craving; and naltrexone, which blocks opioid receptors and prevents the drug from having an effect (patients sometimes have trouble complying with naltrexone treatment, but a new long-acting version given by injection in a doctor’s office may increase this treatment’s efficacy). Another drug called naloxone is sometimes used as an emergency treatment to counteract the effects of heroin overdose.

§ Both behavioral and pharmacological (medications) approaches help to restore a degree of normalcy to brain function and behavior, resulting in increased employment rates and lower risk of HIV and other diseases and criminal behavior. Although behavioral and pharmacologic treatments can be extremely useful when utilized alone, research shows that for some people, integrating both types of treatments is the most effective approach.
§ Pharmacological Treatment (Medications) Scientific research has established that pharmacological treatment of opioid addiction increases retention in treatment programs and decreases drug use, infectious disease transmission, and criminal activity. When people addicted to opioids first quit, they undergo withdrawal symptoms (pain, diarrhea, nausea, and vomiting), which may be severe. Medications can be helpful in this detoxification stage to ease craving and other physical symptoms, which often prompt a person to relapse.
§ While not a treatment for addiction itself, detoxification is a useful first step when it is followed by some form of evidence-based treatment. Medications developed to treat opioid addiction work through the same opioid receptors as the addictive drug, but are safer and less likely to produce the harmful behaviors that characterize addiction.

§ Three types of medications include: (1) agonists, which activate opioid receptors; (2) partial agonists, which also activate opioid receptors but produce a smaller response; and (3) antagonists, which block the receptor and interfere with the rewarding effects of opioids. A particular medication is used based on a patient’s specific medical needs and other factors. Effective medications include:

§ Methadone is a slow-acting opioid agonist. Methadone is taken orally so that it reaches the brain slowly, dampening the “high” that occurs with other routes of administration while preventing withdrawal symptoms.
§ Methadone has been used since the 1960s to treat heroin addiction and is still an excellent treatment option, particularly for patients who do not respond well to other medications.
§ Methadone is only available through approved outpatient treatment programs, where it is dispensed to patients on a daily basis.

§ Buprenorphine (Subutex®) is a partial opioid agonist. Buprenorphine relieves drug cravings without producing the “high” or dangerous side effects of other opioids.
§ Suboxone® is a novel formulation of buprenorphine that is taken orally or sublingually and contains naloxone (an opioid antagonist) to prevent attempts to get high by injecting the medication.
§ If an addicted patient were to inject Suboxone, the naloxone would induce withdrawal symptoms, which are averted when taken orally as prescribed. FDA approved buprenorphine in 2002, making it the first medication eligible to be prescribed by certified physicians through the Drug Addiction Treatment Act. This approval eliminates the need to visit specialized treatment clinics, thereby expanding access to treatment for many who need it.

§ “A Methadone patient is monitored more closely than a paroled murder.”
§ Dr. Edwin A Salsitz, of Beth Israel Hospital in NYC
§ In a comprehensive review of methadone effectiveness, published in Psychiatric Services in 2013, the authors conclude:
§ “Overall, there is a high level of evidence for the effectiveness of MMT in improving treatment retention and decreasing illicit opioid use.”
§ In a comprehensive review of buprenorphine effectiveness published in Psychiatric Services in 2014 the authors conclude:
§ “Overall, a high level of evidence was found for the effectiveness of BMT in improving treatment retention and decreasing illicit opioid use.”

§ Numerous studies over the last 50 years, comparing methadone maintenance to tapering, have consistently demonstrated that relapse is the rule. Relapse rates reported are generally in the 80—100% range over time.
§ Similar rates of relapse are now reported comparing buprenorphine maintenance to tapering.
§ Of particular note was the decrease in HIV seropositivity in patients on methadone maintenance versus patients who had discontinued maintenance and relapsed to IVDU in the early 1980’s.

§ The term opioid substitution treatment (OST) is widely used in Europe, Australia, and elsewhere. Terminology is important, and this term is misleading to many patients, and particularly significant others.
§ Methadone and Buprenorphine Maintenance are treatments for opioid use disorder. A clear distinction should be made between physical dependence and addiction.
§ Methadone and buprenorphine maintained patients, with negative UDT’s, and no other criteria for opioid use disorder, are physically dependent, but not addicted to the medication.

§ All opioids share common adverse or side effects: most common are constipation, increased sweating, and pruritus. All opioids may decrease testosterone levels.
§ Opioids, however, do not result in organ damage, as compared to alcohol, tobacco, and cocaine. The common side effects should be monitored and appropriately treated.
§ Methadone does prolong the QTc interval at clinically relevant doses. EKG’s will detect this problem ♣ Opioids do decrease salivary flow and may have some effect on osteoclast/osteoblast function, but the myth that methadone “rots teeth and bones,” although very prevalent, is a myth.

§ Many addiction treatment providers insist on total abstinence, including properly prescribed medications, as a criterion for “recovery.” This issue often becomes one of ideology rather than science.
§ A methadone or buprenorphine maintained patient, with no use of illicit or non-prescribed drugs, negative UDT’s, attending to personal, family, work, and community responsibilities, should be considered to be in “recovery” or remission.*
§ There are patient groups, such as the National Alliance of Methadone Advocates, who advocate and educate on Medication Assisted Recovery.
§ Recovery is a personal term, best left to each patient to define for themselves.

§ All Treatments Work for Some Patients, No One Treatment Works for All Patients. Treatment decisions should not be ideologically driven.
§ Addiction is a chronic disease. For some patients indefinite pharmacologic treatment will provide the best outcome. This is no different from other common chronic disorders such as hypertension.
§ Paradoxically, it is precisely the patients who have done well on treatment with methadone, who feel the most stigmatized, and are asked repeatedly: “When and why don’t you “get off” this stuff?”

§ When a patient misunderstands the directions for use, accidentally takes an extra dose, or deliberately misuses a prescription opioid or an illicit drug like heroin
§ If a person takes opioid medications prescribed for someone else
§ If a person mixes opioids with other medications, alcohol, or over-the-counter drugs
§ Opioid overdose is life-threatening and requires immediate emergency attention. Recognizing the signs of opioid overdose is essential to saving lives. Learn more about opioid overdose.

§ Overdose is a dangerous and deadly consequence of heroin use. A large dose of heroin depresses heart rate and breathing to such an extent that a user cannot survive without medical help. Naloxone (e.g., Narcan®) is an opioid receptor antagonist medication that can eliminate all signs of opioid intoxication to reverse an opioid overdose. It works by rapidly binding to opioid receptors, preventing heroin from activating them.
§ Because of the huge increase in overdose deaths from prescription opioid abuse, there has been greater demand for opioid overdose prevention services. Naloxone that can be used by nonmedical personnel has been shown to be cost-effective and save lives.
§ In April 2014, the U.S. Food and Drug Administration (FDA) approved a naloxone hand-held auto-injector called Evzio, which rapidly delivers a single dose of naloxone into the muscle or under the skin, buying time until medical assistance can arrive. Since Evzio can be used by family members or caregivers, it greatly expands access to naloxone.

§ Naloxone is a medication approved by the Food and Drug Administration (FDA) to prevent overdose by opioids such as heroin, morphine, and oxycodone. It blocks opioid receptor sites, reversing the toxic effects of the overdose. Naloxone is administered when a patient is showing signs of opioid overdose. The medication can be given by intranasal spray, intramuscular (into the muscle), subcutaneous (under the skin), or intravenous injection.
§ Naloxone is also added to buprenorphine to decrease the likelihood of diversion and misuse of the combination drug product. Learn more about buprenorphine.
§ A doctor can prescribe naloxone to patients who are in medication-assisted treatment (MAT), especially if the patient is taking medications used in MAT or considered a risk for opioid overdose.
§ Patients given an automatic injection device or nasal spray should keep the item available at all times. Medication should be replaced when the expiration date passes.
§ Naloxone is effective if opioids are misused in combination with other sedatives or stimulants. It is not effective in treating overdoses of benzodiazepines or stimulant overdoses involving cocaine and amphetamines.

§ In an effort to save more lives from opioid overdose, SAMHSA published the Opioid Overdose Prevention Toolkit – 2014. The Toolkit equips communities and local governments with material to develop policies and practices to help prevent opioid-related overdoses and deaths. It also serves as a foundation for educating and training:
§ Communities
§ Prescribers of opioid pain medications
§ First responders
§ Patients who are prescribed opioid medications
§ Individuals and family members who have experienced an opioid overdose

§ Importance of behavioral therapy § One on one coaching § W.R.A.P. (Wellness Recovery Action Plan) § Counseling § Group Discussions § Peer to Peer § Family Support Group § Additional Self Help Classes

§ SAMHSA – Substance Abuse and Mental Health Services Administration
§ CDC – Center for Disease Control and Prevention
§ NIH – National Institute on Drug Abuse
§ ASAM – American Society of Addiction Medication
§ DEA – Drug Enforcement Administration
§ EVZIO.com