access to pharmacotherapy of opioid dependence 29-30.02
TRANSCRIPT

Access to pharmacotherapy of opioid dependence
29-30.02.2008, Riga
Ave Talu
National Institute for Health Development
Estonian Drug Monitoring Centre
e-mail: [email protected]
http://eusk.tai.ee
http://www.tai.ee

2
1. Availability of drug treatment for injecting drug users (IDUs) in Estonia
2. Results of and conclusions drawn from an assessment survey (funded by UNODC) on the quality of methadone maintenance treatment and on the demand for services in Estonia
3. Available data for planning substitution treatment for IDUs and possible activities to be implemented on the framework of UNODC project in Estonia

3
Availability of drug treatment (1)
The majority of health care institutions providing addiction treatment engage in
outpatient care (five of the treatment institutions funded by the NIHD provides only
outpatient care and one outpatient as well as inpatient care).
In 2007 drug treatment was funded from the financial resources of the Global Fund,
HIV/AIDS prevention strategy and of local governments. A person can also seek
treatment, funding it from his own financial means.
According to the HIV/AIDS 2007 prevention strategy and the Global Fund report, the
number of persons undergoing methadone substitution treatment increased over the
years.
Alternative substitution treatment with buprenorphine for IDUs was not funded
According to experts the availability of drug (substitution) treatment for injecting drug
users (IDUs) is insufficient in Estonia (Drew et al, 2008).

4
Availability of drug treatment (2)
673 methadone substitution treatment places funded by the Global Fund and HIV/AIDS prevention strategy were filled in six treatment centres in 2007 (National Institute for Health Development, 2008).
A total of 1030 clients received methadone substitution treatment in 2007of whom 35% (357 clients) stopped the treatment.
As for local governments, in 2007 only Tallinn funded the treatment of 104 adult clients in addition to the state funding of methadone substitution treatment.
In 2007 a total of 777 methadone substitution treatment places were funded from various sources (covers 5.6% of IDUs)

5
Availability of drug treatment (3)
356,689 euros of state funds were used for the provision of substitution treatment service, which ensured treatment for less than one-tenth (4.9%; N=673) of injecting drug addicts
On the average 346 euros were spent on the substitution treatment of one opiate addict in 2007.
Drug treatment (detoxification and substitution treatment) is very limited in prisons and lacking in detention houses and due to the limited number of treatment places drug addicts under probation supervision have very linited access to drug treatment.
It is known that best substitution treatment results are achieved when treatment is consistent, support services are provided and adequate amounts of medications are used

6
Availability of drug treatment (4)
Experts responsible for the drafting of the Development Plan for Drug Treatment found that more emphasis should be laid on referring injecting drug users to treatment and on introducing treatment options
They also found that there is a need to pay attention to the development of an early intervention, addiction diagnostics and referral to treatment system for minors (e.g. innovative options, such as peer-driven intervention for involving IDUs in drug treatment)
Such target groups as amphetamine and opiate injectors, under-age drug addicts, drug addicts under probation supervision, inmates, persons in detention, etc., have limited access to suitable treatment options.

7
Availability of methadone substitution treatment for IDUS in 2007.
1,030673356,6895,580,976Total
1485,88092,000Western Tallinn Central Hospital
1287543,951687,690AS Wismari Haigla
16911752,681824,284OÜ Elulootus
23013072,8161,139,317OÜ Narva Sõltuvusravi Keskus
386274144,4102,259,526OÜ Corrigo
1046936,951578,159OÜ Aasa Kliinik
Number of
clients in a year
(incl. stopped persons)
Filled treat-ment
places a year
Funds allocated
(EUR)
Funds allocated
(EEK)
Health care institution
Source: National Institution for Health Development, Department of the Prevention of Infectious diseases and Drug Addiction, 2007; National HIV/AIDS strategy 2007 report.

8
Characteristics of persons seeking for drug treatment in 2008
(NIHD, Drug Treatment Database 2009)
In 2008 in total 824 of drug treatment case notices were enetred to the Drug
Treatment Database of which 228 were treatment discontinuation notices.
77.5% of persons starting the drug treatment were male, close to 70% were 20-
29 years old, 86% were Russian speaking.
More than half of persons (56%) seeking for drug treatment live in Ida-Viru
County and 36% in Tallinn
96% of persons seeking for drug treatment were IDUs with opioid dependency
56% of clients in treatment injected fentanyl or 3-methylfentanyl (TMF) and 25%
heroin as a main drug.

9
Assessment survey on the quality of methadone substitution treatment
and on the demand of services (NIHD & UNODC, 2009) (1)
The survey was funded from the resources of the XEE/J20 project of the UN
Office on Drugs and Crime (UNODC) “HIV/AIDS Prevention among Injecting
Addicts and in Prisons in Estonia, Latvia and Lithuania 2006-2010”.
The assessment survey includes substitution treatment centres of six service
providers and their 54 clients.
The survey point to various problems in opiate substitution treatment that require
quick solutions.
The findings of this survey are similar to those of a quick assessment of
methadone maintenance treatment conducted in June 2007 on the framework of
UNODC project in Estonia by Dr. E. Subata
Five of the sampled service providers offer only methadone substituton
treatment and one methadone as well as buprenorphine treatment.

10
Assessment survey on the quality of methadone substitution treatment
and on the demand of services (NIHD & UNODC, 2009) (2)
Different sets of questions were used in order to obtain an overview of the political and
organisational context of opiate maintenance treatment, to assess how satisfied
clients are with the provided treatment service, to study the management of work and
service quality in health care institutions providing maintenance treatment and their
cooperation with other social and health care institutions.
In addition a supplementary questionnaire was composed for opiate-injecting addicts
not undergoing treatment in order to gain information on their attitudes and opinion on
methadone maintenance treatment.
The past years the focus of opiate substitution treatment in Estonia has been rather on
damage reduction or motivational enhancement treatment than on individual
substitution treatment
It could be concluded that substitution treatment is a highly fragmentised field lacking
an integral approach and distribution of responsibility.

11
Assessment survey on the quality of methadone substitution treatment
and on the demand of services (NIHD & UNODC, 2009) (3)
Uniform understanding of the essence and goals of treatment across service
planners and providers varies considerably.
The lack of support services is a major weakness of substitution treatment; many
refer to the absence of psycho-social additional services and counselling.
Cooperation between service planners and service providers is weak.
The main issues are as follows: weak general concept and management system,
shortcomings in the organisation of work in treatment centres, limited support
services, lack of cooperation with other institutions and the negative image of
methadone maintenance treatment among injecting drug addicts as well as service
providers.

12
Assessment survey on the quality of methadone substitution treatment
and on the demand of services (NIHD & UNODC, 2009) (4)
The lack of a unified framework and guidelines calls for setting national standards
of substitution treatment, a fixed treatment structure and development trends,
distributing responsibility and for political will to develop the field.
Various parties of the survey offered as one solution the authorisation of new
treatment guidelines for opiate addiction on a higher level so as to avoid their
turning into a document of an advisory nature.
The next step after setting the general framework for opiate addiction treatment is
the enhancement of the organisation of work in treatment centres.
Responses of employees providing methadone maintenance treatment revealed
that first and foremost it is the in-house organisation of work that is problematic.

13
Assessment survey on the quality of methadone substitution treatment
and and on the demand of services (NIHD & UNODC, 2009) (5)
It would be useful to compile specific education plans for various professional
groups and find funding possibilities for organising training events.
Substitution treatment centres could also perform the function of connecting
clients to other services of health and social care institutions.
According to the staff of treatment centres such cooperation between different
institutions could be facilitated by a case manager working for a treatment
centre.
Organising round-table meetings and making mutual cooperation contracts
should contribute to effective cooperation between different institutions
14
Assessment survey on the quality of methadone substitution treatment
and on the demand of services (NIHD & UNODC, 2009) (6)
Giving take-away methadone doses to clients is quite a common practice in
Estonia.
Regarding take-away doses it is important to note that clients have to
“deserve” such a privilege.
According to clients the period after which they can apply for take-away
methadone varies among treatment centres from three weeks to two years.
The frequency of taking urine samples (used as a check-up mechanism) in
treatment centres remains elusive.
In the current situation it would be practical to further structure the
requirements for take-away methadone and establish a more efficient
system for check-up urine samples.

15
Assessment survey on the quality of methadone substitution treatment
and on the demand of services (NIHD & UNODC, 2009) (7)
Tests used for identifying opiates in urine have a low-sensitivity for synthetic
opiates, such as fentanyl (Berens at al., 2002; Heit et al, 2004).
The specific ELISA testing procedure needs to be applied to determine the use of
fentanyl – highly widespread in Estonia – among substitution treatment clients.
The hours of work of treatment centres should be carefully considered, taking into
account clients’ preferences, the surroundings, public transport schedules and the
capabilities of centre’s employees.
Some centres in the sample were open from 8.00 to 18.00 providing clients with
quite a large window for obtaining their daily dose. Others were open in the
morning or in the evening, depending on the day of the week.
Client responses reveal a certain degree of discontent with centres' working
hours. Weekends were regarded as especially difficult periods.

16
Assessment survey on the quality of methadone substitution treatment
and on the demand of services (NIHD & UNODC, 2009) (8)
According to employees’ estimates an average dose ranged 25-80 ml.
This estimate indicates that differences between methadone doses provided in
various centres are relatively large.
Also, the client satisfaction survey backs up this guess: according to the survey a daily
methadone dose remains in the range of 9-205 ml.
A positive change that new treatment guidelines for opiate addiction establish
recommended methadone doses and instructions for administration. The approval of
treatment guidelines on a higher level is required for the development of a unified
standard and common practice.
More than half of clients have friends who do not attend substitution treatment
because they do not believe in it or consider it to be harmful. The unpopularity of
methadone substitution treatment is also manifested in the lack of treatment queues in
most of the centres.

17
Assessment survey on the quality of methadone substitution treatment
and on the demand of services (NIHD & UNODC, 2009) (9)
The factors currently reducing demand for methadone substitution treatment are the
lack of adequate information and the dubious quality of the treatment.
On the basis of survey results it can be assumed that the rise in the quality of the
treatment experienced firsthand by clients and the distribution of adequate
information via appropriate channels should increase demand for the treatment.
The survey indicates that IDUs regard as the most reliable source of information
fellow addicts and employees of syringe exchange points. Planned approaches
should be conducted through the aforementioned information sources in order to
distribute adequate information and direct addicts to the drug treatment service.
It is vital to improve the image of substitution treatment in the general population in
order to create competition in providing the treatment service and a stronger sense
of self-esteem among the staff.

18
Assessment survey on the quality of methadone substitution treatment
and on the demand of services (NIHD & UNODC, 2009) (10)
Raising the quality of the substitution treatment service contributes to improving the
reputation of methadone maintenance treatment in the general public and to
increasing its coverage.
One of the positive findings of the survey that a number of clients manifested a
favourable attitude toward substitution treatment and stated that treatment has
brought about positive behavioural changes and improved their psychological
situation.
A number of clients claimed that their health as well as psychological and social
situation has improved thanks to undergoing the treatment. Some respondents say
that they have completely quit substance use and criminal behaviour.
Rise in treatment quality and the development of psycho-social support services in
substitution treatment programmes guarantees better observation of treatment
routine and higher efficiency (McLellan et al, 1993).

19
Characteristics of IDUs in Estonia
Differences in the structure of the local illegal drug market are probably accountable
for variations in injected narcotic substances.
Earlier surveys indicate that injecting drug addicts in Estonia inject primarily
amphetamine and fentanyl (Platt et al, 2006; Uusküla et al, 2008).
Cross-sectional surveys conducted in 2007 among injecting drug users in two
regions (Tallinn (N=350) and Kohtla-Järve (N=350) suggest a similar trend.
According to the risk behaviour survey of injecting drug users conducted by the
National Institute for Health Development in 2006 and 2007 respectively, 53.3% and
48.6% of the drug addicts using the syringe exchange service had injected
amphetamine and 9% and 12%, respectively fentanyl in the last month (Lõhmus et
al., 2007, Lõhmus et al., 2008).
In terms of the regional prevalence of drugs the percentage of injectors was higher
in Tallinn (64%) than in Ida-Viru County (47%).

20
Primary injected drug over the course of the last four weeks among IDUs in
Tallinn and Kohtla-Järve in 2007(NIHD & University of Tartu, 2008)
1.10.4-7.56.7Other
1.40-2.30.6Sudafed
8.95.2-15.69.8Heroin
57.641.7-57.049.5Poppy liquid
12.910.7-22.316.2Amphetamine
1612.3-24.718.2Fentanyl
Studied IDUs in Kohtla-Järve
0.30-1.10,3Sudafed
1.10-1.60.6Heroin
25.723.1-44.133.5Amphetamine
71.153.7-74.464.2Fentanyl
Studied IDUs Tallinn
%95% CI%
SPP**EPP*
* EPP Estimated Population Proportion; **SPP Sample Population Proportion

21
Drug injecting during the last 4 weeks in Tallinn in 2007 (NIHD & University of
Tartu, 2008) (1)
* EPP Estimated Population Proportion; **SPP Sample Population Proportion
0.60-2.80.9Other
2.30.3-4.01.8Ecstasy
0.30-0.30.1Ephedrine
0.90-4.31.4Sudafed
0.90-6.62.2Cocaine
2.90.2-2.41.2Heroin
0.30-1.30.8Poppy liquid
4638.0-57.347.6amphetamine
79.462.4-81.371.9Fentanyl
Studied IDUs in Tallinn
%
95% confidence interval%
SPPEPP

22
Drug injecting during the last 4 weeks in Kohtla-Järve in 2007 (NIHD &
University of Tartu, 2008) (2)
* EPP Estimated Population Proportion; **SPP Sample Population Proportion
8.65.1-13.38.9Other
0.30-0.50.2Ecstasy
0.30-0.30.1Ephedrine
1.70-2.70.9Sudafed
24.614.4-25.219.5Heroin
66.249.0-65.157.3Poppy liquid
21.817.6-31.124.2Amphetamine
36.426.8-40.533.4Fentanyl
Studied IDUs in Kohtla-Järve
%
95% confidence
interval%
SPPEPP

23
Male (82%), Russian-speaking (in Tallinn 81% and in Kohta-Järve
92%)
More than 40% of the studied persons in both regions were in the age
group 25-29
Half of studied IDUs had passed no more than 9 grades at school
Close to half of the studied persons had health insurance
Background information on the studied IDUs in Tallinn and Kohtla-Järve in 2007 (NIHD & University of Tartu, 2008)

24
Average age in initiation of injecting drug use (NIHD &
University of Tartu, 2008)
13-3019,813-4019,7Sudafed
15-2821,516-3321,7Cocaine
13-3318,910-3118,6Home-made poppy liquid (MAK)
13-3019,211-4419,3Amphetamine
15-4022,313-4922,5Fentanyl
15-3019,311-4219,8Heroin
RangeAverage age
RangeAverage age
Drug
Kohtla-JärveTallinn

25
Prevalence of HIV, HBV, HCV and latent TB among studied
injecting drug users in 2007 (NIHD & University of Tartu, 2008)
4.40-30.86.4Kohtla-Järve (181 IDUs were tested)
10.12.5-14.07.6Tallinn (208 IDUs were tested)
Latent TB
72.553.3-68.359.5Kohtla-Järve
76.862.7-79.471.4Tallinn
HBV antibody
82.869.1-82.775.9Kohtla-Järve
94.382.2-95.789.8Tallinn
HCV
69.951.1-68.059.4Kohtla-Järve
55.139.2-56.047.5Tallinn
HIV
%95%CI%
SPPEPP

26
Riski behaviour of new vs old IDUs (Uusküla et al., 2008) (1)
The comparison of new and long-time injectors (Uusküla et al, 2008) as based
on cross-sectional surveys on the prevalence of HIV and risk behaviour
conducted in Tallinn in 2004 (Uusküla et al, 2007b) and 2005 (Platt et al, 2006)
demonstrates that new as well as long-time injecting drug users have similarly
risky injecting and sexual behaviour.
The majority of new and long-time injectors included in the 2004 and 2005
surveys were mostly Russian-speaking (in 2004 new injectors 96 % versus
long-time injectors 92%, in 2005 respectively 78% and 89%).
Half of the new as well as long-time injectors studied in the 2005 survey
injected drugs every single day.
New injectors were less probably daily injectors than long-time injectors (21.9%
versus 42.2%).

27
Riski behaviour of new vs old IDUs (Uusküla et al., 2008) (2)
According to the 2004 survey 43% of the new and 30% of the long-time IDUs reported receptive needle sharing during the last 90 days
According to the 2005 survey about one-third of the new and long-time users reported receptive needle sharing during the last 28 days.
Both studies (2004 versus 2005) show that the sexual risk behaviour of new and long-time IDUs (more than 1 sexual partner during the last 12 months) was similarly very risky (the 2004 survey: 45.8% versus 47.9%; the 2005 survey: 55.6% versus 59.6%).
The prevalence of HIV is very high among new and long-time IDUs. 2004. The HIV pevalence among new injectors was 50% in 2004 and 34% in 2005
and among long-time injectors 56% in 2004 and 34% 2005.

28
Drug-related deaths of IDUs (1)
117 IDUs died of fentanyl poisoning in 2005–2006, three of them in prison
(Ojanperä et al, 2008).
91% of the persons who died of fentanyl poisoning were male and their average age was 26.
In most cases the cause of death was incidental poisoning related to using fentanyl or fentanyl in combination with other drugs.
Three death related to 3-methyfentanyl were registered in prison.

29
Drug-related deaths of IDUs (2)
In 2007 in total of 107 IDUs died of fatal accidental poisoning of narcotic drugs and psychotropic substances (Female=7; Male=100). The vaste majority of died IDUs were young people (average age 26).
Results of comprehensive toxicological analysis
3Cocaine
22Opiates
25Methadone
25Amphetamine
49Bensidiazepines
98Fentanyl
30
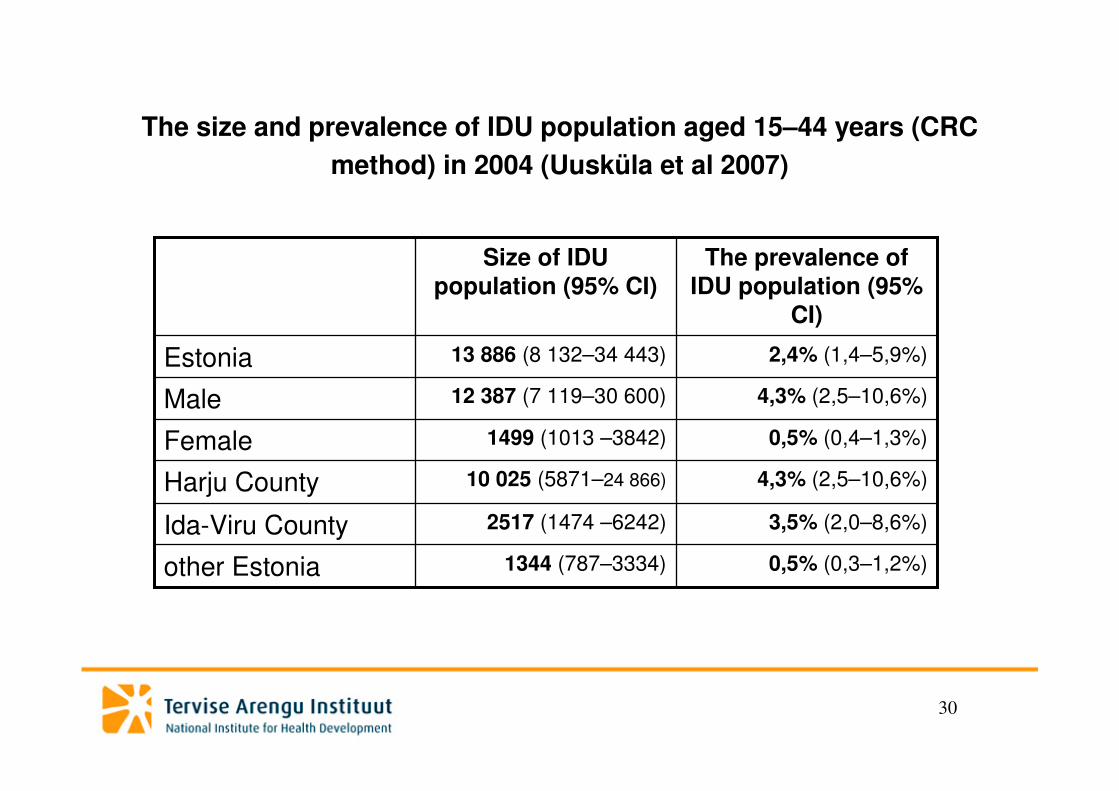
The size and prevalence of IDU population aged 15–44 years (CRC
method) in 2004 (Uusküla et al 2007)
0,5% (0,4–1,3%)1499 (1013 –3842)Female
0,5% (0,3–1,2%)1344 (787–3334)other Estonia
3,5% (2,0–8,6%)2517 (1474 –6242)Ida-Viru County
4,3% (2,5–10,6%)10 025 (5871–24 866)Harju County
4,3% (2,5–10,6%)12 387 (7 119–30 600)Male
2,4% (1,4–5,9%)13 886 (8 132–34 443)Estonia
The prevalence of IDU population (95%
CI)
Size of IDU population (95% CI)
31
http://eusk.tai.ee