otto zuhr wound closure and wound healing. suture ...a wide range of different suture materials are...
TRANSCRIPT

VOLUME 48 • NUMBER 8 • SEPTEMBER 2017 647
Q U I N T E S S E N C E I N T E R N AT I O N A L
Wound closure and wound healing. Suture techniques
in contemporary periodontal and implant surgery:
Interactions, requirements, and practical considerations
Otto Zuhr, Dr med Dent1/Dodji Lukas Akakpo2/Markus Hürzeler, Prof Dr Med Dent3
In contemporary reconstructive periodontal and implant sur-gery, attaining uncomplicated wound healing in the early post-operative healing phase is the key to achieving a successful treatment outcome and is of central interest, from the clinical as well as the scientific perspective. The realization of primary wound healing is the central challenge in most cases. Two of the evidence-based factors that affect postoperative wound healing can be influenced by the surgeon: the blood supply to the surgi-cal site and postoperative wound stability. The surgical suture is a key determinant of whether adequate wound stability is achieved in this context without complicating the course of
wound healing by exerting unnecessary trauma or excessive tensile strain on the wound edges. Therefore, the inclusion of anchors in the suturing process that make it possible to achieve the best wound stability possible is often an important key to success. This article provides an overview of the principles of successful wound closure that are relevant to postoperative wound healing in order to equip dentists with the tools needed for the correct, indication-specific selection and performance of surgical suturing techniques in daily practice. (Quintessence Int 2017;48: 647–660; originally published (in German) in Implantologie 2016;24:281–294; doi: 10.3290/j.qi.a38706)
Key words: microsurgery, suture anchoring, suture material, suturing technique, wound closure, wound healing
ORAL SURGERY
Otto Zuhr
the key to success is to achieve fast and uncomplicated
wound healing. The successful integration of graft and
augmentation materials commonly used in this context
depends on a range of factors, such as, and in particu-
lar, the good blood supply to the surgical site, the pre-
vention of bacterial infections, and the achievement of
maximal wound stability. The realization of primary
wound healing is therefore the measure of all things in
the majority of these cases.1,2 From a biologic perspec-
tive, wound healing by primary and secondary inten-
tion leads to the same result: wound closure. However,
the two processes differ significantly in terms of the
chronology of the different phases of wound healing
and the tissue quality at the end of the healing period.3
Reconstructive hard and soft tissue augmentation pro-
cedures in periodontal and dental implant surgery are
increasingly shaping the treatment spectrum of den-
tistry. More and more emerging evidence shows that
1 Private Practice, Hürzeler & Zuhr Joint Dental Practice, Munich, Germany; and Asso-
ciate Professor, Center for Dentistry, Oral and Maxillofacial Surgery (Carolinum),
Johann Wolfgang Goethe University, Polyclinic for Periodontology, Frankfurt,
Germany.
2 Dentist, Hürzeler & Zuhr Joint Dental Practice, Munich, Germany.
3 Private Practice, Hürzeler & Zuhr Joint Dental Practice, Munich, Germany; and
Associate Professor, Albert-Ludwigs University, Department of Conservative Den-
tistry and Periodontology, Freiburg University Hospital, Freiburg, Germany.
Correspondence: Dr med dent Otto Zuhr, Hürzeler & Zuhr Dental Practice, Rosenkavalierplatz 18, 81925 Munich, Germany. Email: [email protected]

VOLUME 48 • NUMBER 8 • SEPTEMBER 2017648
Q U I N T E S S E N C E I N T E R N AT I O N A L
Zuhr et al
From a surgical point of view, smooth, well-vascu-
larized, tension-free, and precisely adapted wound
edges are the most important prerequisites for primary
intention healing. After primary wound closure in this
manner, a thin but stable blood clot forms between the
wound margins, and little to no local tissue ischemia
occurs. Consequently, it is virtually impossible for bac-
teria to infiltrate the wound, particularly the deep tissue
layers. The blood supply to the wound is rapidly
restored, and a provisional matrix quickly forms to
cover the wound. Under favorable conditions, a wound
can close within a few days of primary wound closure in
the absence of clinically detectable inflammation,
wound secretion, and granulation tissue. There is very
little to no scar tissue formation after wound healing by
primary intention. The outcome of primary wound
healing can thus be described as wound tissue regen-
eration in the sense of “restitutio ad integrum”, ie res-
toration of the tissue to more or less its original intact
condition.
Secondary wound healing, on the other hand, is
associated with the formation of repair tissue. To
quickly close the wound and restore the integrity of the
epithelial lining of the oral cavity, the body produces
low-grade scar tissue to bridge over the gap resulting
from tissue damage or removal. When suture closure
results in excessive tension on flap edges, or when
suture loosening occurs due to improper suture tying,
or a restricted local blood supply leads to wound edge
necrosis, healing by secondary intention often occurs in
spite of primary wound closure.4 Especially in the intra-
oral cavity, such wounds are associated with a high risk
of bacterial contamination. In many cases, this results in
a compromised treatment outcome characterized by
the development of volume defects, fibrotic tissue, and
hypertrophic scars.5
Against the background of this knowledge, it is
evident that the successful performance of any recon-
structive-surgical procedure requires a deep under-
standing of the importance of wound healing as well
as the identification and control of factors influencing
the wound healing process. From the clinical per-
spective, these are basic keys to success. Prognostic
factors associated with wound healing have been
investigated in research on the treatment of gingival
recession in the context of reconstructive periodontal
and implant surgery.6 Risk factors for failure can be
divided into three broad categories: patient-related,
defect-related, and technique-related. It seems feasi-
ble to transfer the knowledge gained in the context
of gingival recession treatment to other settings.
While both patient-related factors (eg, general
health) and defect-related factors (eg, the defect con-
figuration) are primarily controlled by appropriate
patient selection, it is mainly via technique-related
factors that the clinician can have a positive influence
on wound healing and, thus, a direct effect on the
outcome of treatment. Surgical soft tissue manage-
ment is therefore a key determinant of the success or
failure of treatment. Careful preoperative planning of
all parts of the procedure (from the first incision to
flap elevation to wound closure) is needed to ensure
optimal wound stability and an optimal blood supply
to the surgical site.7,8 Surgical suturing techniques
play an important role in this context.9
The aim of this article is therefore to equip practic-
ing dentists with the tools needed to correctly select
and perform the various suturing techniques used in
oral surgery in an indication-specific manner. Clinical
examples are provided to illustrate a range of aspects,
from the indication-specific selection of appropriate
suture materials and suturing techniques and practical
tips on how to perform them. It is our hope that this
will contribute to a better understanding of the impor-
tance of achieving wound closure based on biologically
sound principles for successful wound healing in the
oral cavity.
MACRO OR MICROSURGERY?
Thanks to the availability of optical magnification and
special microsurgical instrument kits, it is now possi-
ble to perform surgical procedures in the oral cavity
with relatively little trauma and high precision. More
and more scientific evidence is emerging to support
the clinical observation that the consistent use of a

VOLUME 48 • NUMBER 8 • SEPTEMBER 2017 649
Q U I N T E S S E N C E I N T E R N AT I O N A L
Zuhr et al
microsurgical approach not only leads to superior early
wound healing with significantly less morbidity, but
also significantly improves the clinical results of oral
surgery.10-12 Microsurgical approaches to reconstructive
periodontal and implant surgery were originally intro-
duced in the early 1990s,13,14 and the ensuing develop-
ment of suitable microsurgical instruments and suture
materials has been a decisive driver of advances in this
field.
In contrast to the classic microsurgery disciplines
such as neurosurgery or ophthalmic surgery, the micro-
surgical techniques used in periodontal and implant
surgery must be adapted to meet the very special
requirements of the oral cavity: they must be delicate
enough to ensure the atraumatic and precise adapta-
tion of sometimes very fragile oral mucosa under opti-
cal magnification yet sturdy enough to withstand high
mechanical stresses, especially in the gingiva or palatal
masticatory mucosa.
Regarding the suture materials, it has proven to be
advantageous to use needles of sufficient length and
stability. Ideally, the needle should be sturdy enough to
penetrate the intraoral tissues smoothly and without
bending, long enough to cross the interdental space in
a single pass, and fine enough to be combined with
fine sutures.
In light of these instrument requirements, it does
not seem absolutely necessary to use an operating
microscope. Loupes with 4.5- to 6-fold magnification
have proved to be an adequate and easy-to-use alter-
native. In terms of the range of optical magnification
and instruments used today, microsurgical interven-
tions in the oral cavity fall somewhere between the
realms of classic microscopic surgery and traditional
macroscopic surgery. This development increasingly
raises two reasonable questions:
• Will strict differentiation between macro- and
microsurgery still be useful in the future?
• Should surgical interventions in the oral cavity gen-
erally be performed via a microsurgical approach
with adequate magnification, using instruments
and suture materials developed specifically for this
purpose?
BIOLOGIC AND PHYSICAL REQUIREMENTS OF SUTURE MATERIALS
A wide range of different suture materials are available
for oral surgery today. Sutures may be classified on the
basis of their structural and physical properties.15 Struc-
turally, sutures are defined in terms of their size (diam-
eter), number of filaments (monofilament vs multifila-
ment/braided), and surface texture (smooth vs rough).
In terms of their physical properties, suture materials
are classified based on their biodegradability (absorb-
able vs nonabsorbable), stiffness, tensile strength, and
knot security.
The ability of a suture to withstand mechanical stress
depends on its combination of physical and structural
properties.16 Equipped with a wide base of knowledge
about the specific properties of different suture mater-
ials, surgeons can not only correctly choose an appropri-
ate suture for a specific case, but are also able to enhance
the healing process to a certain extent. There are very
high requirements that an “ideal” suture material must
meet.17-19 Regarding factors related to the manufacturing
process, the ideal suture material should be easily steril-
izable and precision-fabricated so as to ensure a uniform
and consistent thread size. High tear and tensile
strength, good handling properties, and high knot secu-
rity are other requirements it should meet. Moreover, the
ideal suture material should cause minimal trauma
during tissue passage and minimal immunologic tissue
reactivity with no capillarity tendencies associated with
the so-called “wick effect.” Capillarity is a process by
which fluids and microorganisms are drawn into the
wound via the filaments of sutures, multifilament mater-
ials in particular, which act like the wick of a candle due
to their rough and braided surface.20 The tendency for
biofilm formation and the risk of patients injuring them-
selves on stiff suture edges during the healing phase
should be as low as possible, and the duration of func-
tion of absorbable sutures must be clearly defined. Last
but not least, manufacturing costs should be low
enough to ensure a reasonable sales price appropriate
for the large volume of sutures used in daily practice.

VOLUME 48 • NUMBER 8 • SEPTEMBER 2017650
Q U I N T E S S E N C E I N T E R N AT I O N A L
Zuhr et al
Absorbable and nonabsorbable sutures are classi-
fied on the basis of their in-vivo biodegradability.
Absorbable sutures may be either natural or synthetic
in origin.15 Natural absorbable sutures are broken down
by proteolytic enzymes, while synthetic absorbable
sutures are degraded by hydrolysis. The degradation
process by which sutures are absorbed triggers an
inflammatory reaction in the surrounding tissues.21,22
Therefore, it seems advisable to limit the use of absorb-
able sutures to deep tissue layers that are no longer
accessible after wound closure and healing. Because
natural sutures generally elicit a greater degree of tis-
sue reaction than synthetic sutures,23,24 they are no
longer recommended for use in oral surgery. The
inflammatory response associated with the absorption
of polyglycolic acid (PGA)-based synthetic sutures is
relatively small.25 PGA sutures are absorbed over a
period of 60 to 90 days.26 However, they appear to have
a maximum of 50% of their original tensile strength
after an implantation period of 60 days.26
Synthetic nonabsorbable sutures made of poly-
amide polymer, polyolefin, polypropylene, or poly-
vinylidene fluoride feature outstanding tissue compat-
ibility.2,27 These monofilament sutures have a much
lower degree of capillarity than multifilament sutures.28
In line with this, there is evidence suggesting that
monofilament sutures are associated with a lower risk
of wound infection.29-31 This advantage, however, is
offset by certain disadvantages: monofilament sutures
are somewhat stiff and inflexible, which results in
poorer handling properties and knot security.23
For the surgeon, the challenge is to choose a suture
material that provides an optimum balance between
the advantages of monofilament and multifilament
sutures.
Smooth polyvinylidene fluoride-based synthetic
monofilament sutures appear to be the suture materials
that offer the best compromise at present.32 Evidence
suggests that the aforementioned disadvantages with
respect to handling properties and knot security no lon-
ger apply from a suture size of 6-0 and 7-0.33 However,
precise knot-tying technique is still needed to achieve
secure wound closure with monofilament sutures.
Expanded polytetrafluoroethylene (ePTFE) is a spe-
cial type of nonabsorbable synthetic suture material.
Expanded PTFE fibers form monofilament sutures with
“pockets of air” incorporated in the material. They have
excellent tissue compatibility, but their porosity (air
content of 50% to 60%) and porosity-related swelling
capacity result in increased bacterial biofilm coloniza-
tion of the thread surface. These are major drawbacks,
but ePTFE also offers some great advantages, such as
excellent glide characteristics. Therefore, ePTFE suture
material can now be recommended as a standard ma-
terial for macrosurgical sutures in oral surgery. How-
ever, because of their porous surface, ePTFE sutures
should not be used in cases where the suture material
must be left in place for long periods of time.2
Proper surgical needle selection is not only import-
ant for successful wound closure, but also for prevent-
ing additional tissue trauma. Surgical needles must
have high flexural strength: they must be rigid enough
to resist bending when passed through tough tissues,
yet ductile enough to keep from breaking as soon as
they encounter resistance. Furthermore, a good surgi-
cal needle must be sterilizable and corrosion-resistant.
The material that best meets these requirements is
high-quality stainless steel, which is usually nickel- or
chrome-plated to make it easier to polish.
Curved needles are easier to control in confined
spaces. They guide the path of the thread through the
tissue such that pulling on the free ends of the suture
brings the edges of the wound into apposition with
slight eversion. Straight needles, on the other hand,
result in inversion of the wound edges, which gener-
ally should be avoided in periodontal surgery. When
making interdental sutures, it should be possible to
insert the needle through the interdental space in a
single pass. This requires the use of longer needles,
especially in the molar region. Needles with a ⅜ or ½
curve and an arc length of 8 to 15 mm are preferen-
tially used in periodontal and dental implant surgery
for this reason. Needles with a triangular cutting blade
have proved effective in periodontal microsurgery.
Only the front third (tip) of the needle should be
sharp, and the middle third (shaft) should be flattened

VOLUME 48 • NUMBER 8 • SEPTEMBER 2017 651
Q U I N T E S S E N C E I N T E R N AT I O N A L
Zuhr et al
for better retention in the needle holder. A polished
surface enhances the ability of the needle to glide
through tissues. Round-bodied needles are not recom-
mended because they bend more easily and are more
difficult to pass through periodontal tissues. The junc-
tion between the needle and the thread is another
important factor. Eyed needles are reusable. The eye
of the needle and the doubled strand of thread in that
region produce in a relatively broad suture footprint,
which causes substantial tissue trauma. Atraumatic
suture needles were developed for this reason. Unlike
eyed needles, the suture thread is glued or welded to
the blunt end of the eyeless atraumatic suture needle,
creating a smooth junction (swage) between the
needle and the thread. Because these are disposable
needles designed for single use only, they are always
new and sharp. Consequently, atraumatic suture nee-
dles results in a tremendous reduction of tissue
trauma. All of these are good reasons why atraumatic
suture needles should be used in oral surgery in gen-
eral and oral microsurgery in particular.
PRINCIPLES OF SUTURE CLOSURE
Because complete immobilization of wounds in the oral
cavity during the postsurgical period is rarely possible,
precise and stable suture closure is crucial to successful
wound healing following oral surgery. The surgeon
should always keep the goal of suturing in mind: Surgi-
cal sutures must passively secure the flap in the pos-
ition established during surgery, keep the edges of the
wound in intimate contact (this is especially important
for grafts depending on initial nutrition by diffusion),
and stabilize the wound during the early healing phase.
The selected suture materials, suturing techniques, and
soft tissue management must ensure that suture knots
do not come undone and that both the suture mater-
ials and the soft tissues are able to resist the mechanical
stresses exerted upon them during the early healing
phase. All of these conditions must be met in order to
achieve healing by primary intention and, most impor-
tantly, good cosmetic results without scarring, espe-
cially in the esthetic zone.
Incisions should be placed in keratinized tissue
whenever possible because this makes it easier to
achieve precise suture closure. The selected incision
technique and flap design should ensure that the
edges of the flap are held in the desired position with-
out tension and that they can be coapted with sutures
without excessive pulling force. This is essential for
achieving the required stability of wound closure
without the sutures tearing out of the skin during
healing. If mobile and immobile flap components are
to be connected, then suturing should always be per-
formed from movable to non-movable tissue to pre-
vent the sutures from tearing through the edges of
the immobile flap. Gently mobilizing the edges of the
immobile flap can make it easier to achieve precise
suturing.
As a general rule, the needle should be inserted at a
90-degree angle to the tissue to minimize trauma. The
force used to guide the needle should always be
applied in the direction of the needle curvature. The
use of needle holders with a round handle cross-sec-
tion facilitates controlled and precise rotational move-
ment of the fingers. As a rule, the needle is held per-
pendicular to the incision line. The general rule is: the
fewer sutures needed to achieve precise and stable
approximation of the flap margins, the better.
The needle holder should be sturdy enough to
grasp fine needles of different sizes securely, yet small
enough to allow easy access into interdental spaces.
Needle holder jaws with a round cross-section prevent
damage to the sutures as well as trauma to the sur-
rounding tissues during suture placement. Needle
holders with a ratchet lock normally are not used in
conventional microsurgery, but have proven very help-
ful in periodontal and implant surgery. They are
designed to hold the needle securely and enable con-
trolled passage of the needle through the often coarse
periodontal soft tissues without excessive pressure on
the instrument handle.
To ensure sufficient knot security, each suture knot
consists of multiple loops. The first loop determines the
position and tension of the suture and, thus, the exact
position of the wound edges. The second loop (and

VOLUME 48 • NUMBER 8 • SEPTEMBER 2017652
Q U I N T E S S E N C E I N T E R N AT I O N A L
Zuhr et al
third loop, if necessary) serves to secure the position
of the first loop. Simple reverse-direction knots can be
tied using microsurgical suture materials of size 7-0
and smaller. First, a double loop is formed, followed
by a second single loop in the opposite direction. The
short end travels in the opposite direction. It should
be noted that once the second loop has been made, it
is not possible to tighten the first loop by pulling on
the second. Therefore, it is important to ensure that
the first loop is securely placed in precise position
before making the second. After making the first loop,
it can be helpful to turn the suture ends 180-degrees
before making the second loop. If it is not possible to
check loop position during suturing, a third single
loop should be made in the opposite direction. The
same rule applies when using size 6-0 microsurgical
suture material. Macrosurgical sutures made of ePTFE
should be tied using a square knot with an additional
third throw to ensure adequate knot security. This
knot is constructed with three consecutive single
loops, each in the opposite direction of the preceding
throw. Due to the excellent gliding capacity of ePTFE,
the first loop can still be tightened after the second
loops have been made. The third loop is needed to
ensure knot security.
To guarantee that the blood supply to the wound is
not impaired during healing, it is important to ensure
that the sutures are not pulled too tightly. The surgical
knot should be as small as possible, and the cut ends of
the knot should never be longer than 3 mm. To avoid
irritation of the wound edges and to minimize plaque
accumulation in the wound, knots should not be
placed on the incision line, but lateral to the wound
edges.
To prevent impairment of healing, the sutures
should be removed with sharp instruments, with as
little trauma as possible, 5 to 7 days after the pro-
cedure.
In oral surgery, sutures are tied either completely
with instruments (needle holder and forceps) or partly
with instruments (needle holder and fingers). Instru-
ment tying enables better control of loop position,
especially in poorly accessible sites.34,35
SUTURING TECHNIQUES AND THEIR CLINICAL APPLICATION
The main objective of the commonly used suturing
techniques described below is the constant clinical
challenge of achieving the most stable wound closure
possible without significantly affecting the blood sup-
ply to the surgical site. Clearly, sufficient wound stability
cannot be achieved if the suture only passes through
mobile tissue flaps alone. Therefore, the availability of
suitable anchors for the sutures is a decisive factor in
the successful selection and execution of a suturing
technique that meets the requirements of the specific
clinical situation. Natural structures (such as the teeth,
gingiva, masticatory mucosa of the hard palate, and
periosteum) as well as artificial structures (such as com-
posite resin anchors) can provide sufficient anchorage.
Single interrupted sutures
Optimal adaptation of two surgical flap edges is the
central focus of suturing. Compared with continuous
sutures, the advantage of interrupted sutures is that
the loss of an individual suture does not mean the com-
plete loss of suture closure. Although it can be assumed
that the use of as few sutures as possible has a benefi-
cial effect on wound healing in the oral cavity, inter-
rupted sutures are relatively time-consuming. This is a
major disadvantage, even if they are used sparingly. If
wound closure is performed using single interrupted
sutures, the distance between the incision line and the
needle entry and exit points (bite size) should be kept
as equal as possible. The closer to the surface the
suture passes through the tissue, the smaller the bite
size should be. However, the bite size should never be
less than 1 to 2 mm (minimum bite size). Ideally, the
suture should cross the incision line at right angles and
should only deviate from this course in selected cases
(Figs 1 to 3).
Tension-relieving sutures
Tension-relieving sutures are always used in combina-
tion with closing sutures to achieve tension-free adap-
tation of the flap edges before the actual suture closure.

VOLUME 48 • NUMBER 8 • SEPTEMBER 2017 653
Q U I N T E S S E N C E I N T E R N AT I O N A L
Zuhr et al
The use of closing sutures alone leads to punctiform
flap adaptation, whereas the combination of closing
and tension-relieving sutures results in broader and
intimate adaptation between the flap edges. This
enhances the precision and mechanical stability of
wound closure, which is particularly important in cases
where increased wound tension or mechanical stress
during the postoperative healing phase is likely to
occur due to postoperative edema or to talking and
chewing movements. Tension-relieving sutures are
placed before closing sutures. They may have a crossed
or parallel suture pattern and can be positioned hori-
zontal or vertical to the incision line. Tension-relieving
sutures may be placed externally or internally, above or
below the incision line.2 The internal horizontal mat-
tress suture is the most commonly used tension-reliev-
ing suture in periodontal and implant surgery. It may
run parallel to or cross over the incision line (Figs 4 to 6).
Bite-Size Bite-Size
Fig 1 Schematic illustration of “bite size.”
Fig 2 Suture closure of a vertical relieving incision in conjunc-tion with a coronally advanced flap (suture material: Seralene Blue 7/0 DS-12).
Fig 3 Schematic representation of a single interrupted suture used for flap stabilization (arrow): the suture passes from the mobile flap to the stationary anchor point, in this case, the gingiva in the immobile part of the second flap (A, anchor; MF, mobile flap).
A MF

VOLUME 48 • NUMBER 8 • SEPTEMBER 2017654
Q U I N T E S S E N C E I N T E R N AT I O N A L
Zuhr et al
Single sling sutures
Regenerative periodontal therapy for deep infra-alveolar
bone defects often requires the simplified papilla preser-
vation technique in interdental spaces, which runs
obliquely through the papilla, from buccal to lingual.36 As
the interdental space generally does not provide enough
access for correct single interrupted suture placement,
the single sling suture is a useful tool for achieving pre-
cise flap adaptation in these cases (Figs 7 to 9).
MBF
A
MPF
Fig 4 Clinical example: An internal hori-zontal mattress suture was used for wound closure after a subepithelial connective tis-sue graft was harvested from the lateral palate for soft tissue ridge augmentation (suture material: Seralene Blue 6/0 DS-15).
Fig 5 Schematic representation of an internal horizontal mat-tress suture (occlusal view).
Fig 6 Schematic diagram demonstrating the use of an internal horizontal mattress suture for flap stabilization (arrow): the palatal masticatory mucosa is used for anchorage (A, anchor; MBF, mobile buccal flap; MPF, mobile palatal flap).

VOLUME 48 • NUMBER 8 • SEPTEMBER 2017 655
Q U I N T E S S E N C E I N T E R N AT I O N A L
Zuhr et al
Double sling sutures
The double sling suture, a combination of single
interrupted suture and tension-relieving suture,
makes it possible to achieve very good and stable
flap adaptation with relatively little time and effort.37
The first part of the suture achieves tension-free clo-
sure of deeper tissues while providing wound edge
eversion. This facilitates the second part of the
suture to ensure precise wound closure. The double
sling suture is passed through the palatal mastica-
Fig 7 Single sling suture used to close a microsurgical access flap after regenerative periodontal therapy in the maxillary anter-ior region (suture material: Seralene Blue 7/0 DS-15).
MBFA
MPF
Fig 8 Schematic representation of a single sling suture (sagittal view).
Fig 9 Schematic representation of the single sling suture tech-nique for flap stabilization (arrow): the palatal masticatory muco-sa (included in the second pass of the suture) is used for anchorage (A, anchor; MBF, mobile buccal flap; MPF, mobile palatal flap).

VOLUME 48 • NUMBER 8 • SEPTEMBER 2017656
Q U I N T E S S E N C E I N T E R N AT I O N A L
Zuhr et al
tory mucosa or the gingiva of the lingual mucosa to
stabilize the wound (Figs 10 to 13).
Suspension sutures
Suspension sutures are used with repositioned flaps to
secure the surgically established flap position if in cases
where the periosteum or attached gingiva does not allow
for sufficient wound stabilization. The teeth or artificially
created retention areas serve as anchors, eg for horizon-
tal or vertical double-crossed sutures, respectively.
The double-crossed suture is a commonly used sus-
pension suture.38 As its name implies, it crosses the
interdental space twice. Horizontal double-crossed
sutures use the circumference of the tooth as an anchor
MBFA
MPF
Figs 10 and 11 Use of two double sling sutures for suture closure after implant placement in the maxillary anterior region (suture material: Seralene Blue 6/0 DS-15), with three additional single interrupted sutures (Seralene Blue 7/0 DS-12).
Fig 12 Schematic representation of a double sling suture tech-nique (sagittal view).
Fig 13 Schematic representation of the double sling suture technique of flap stabilization (arrow): the palatal masticatory mucosa, which was included in the first pass of the suture but was not mobilized, is used for anchorage (A, anchor; MBF, mobile buccal flap; MPF, mobile palatal flap).

VOLUME 48 • NUMBER 8 • SEPTEMBER 2017 657
Q U I N T E S S E N C E I N T E R N AT I O N A L
Zuhr et al
point. It is used, for example, for donor site closure after
harvesting a free connective tissue graft from the lateral
palate. Additional anchorage of the suture to the pala-
tal masticatory mucosa apical to the harvest site results
in simultaneous wound compression (Figs 14 to 16).
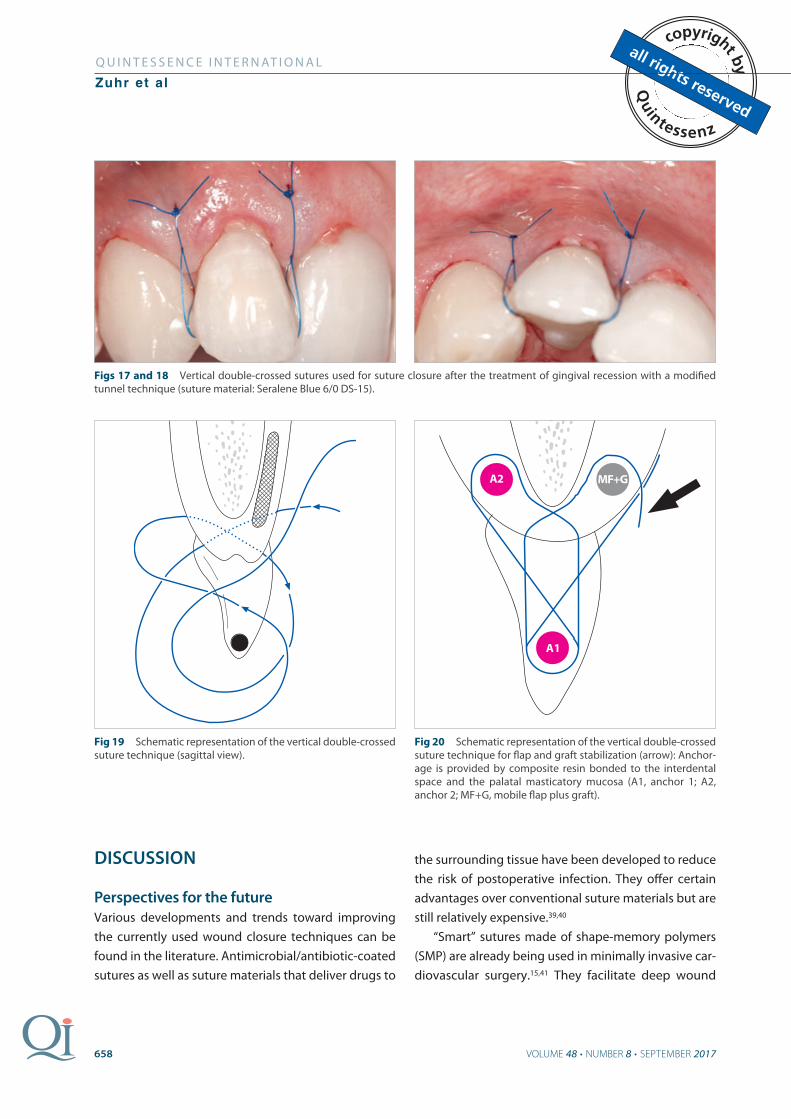
Vertical double-crossed sutures are anchored by
composite resin bonded to the interdental space, coro-
nal to the wound. They are used, for example, after
plastic reconstructive surgery performed by tunneling
technique and entirely without superficial buccal inci-
sions. Vertical double-crossed suture placement allows
for ideal coronal stabilization of augmented tissue as
well as for compression and stabilization of the wound
(Figs 17 to 20).
Fig 14 Horizontal double-crossed sutures used for wound clo-sure after harvesting a subepithelial connective tissue graft from the lateral palate (suture material: Gore-Tex CV5).
Fig 15 Schematic representation of a parallel and a crossed horizontal double-crossed suture (occlusal view).
MF
A1
A2
Fig 16 Schematic representation of a parallel and a crossed horizontal double-crossed suture used for flap stabilization (arrow): a tooth and the palatal masticatory mucosa serve as anchors (A1, anchor 1; A2, anchor 2; MF, mobile flap).
VOLUME 48 • NUMBER 8 • SEPTEMBER 2017658
Q U I N T E S S E N C E I N T E R N AT I O N A L
Zuhr et al
DISCUSSION
Perspectives for the future
Various developments and trends toward improving
the currently used wound closure techniques can be
found in the literature. Antimicrobial/antibiotic-coated
sutures as well as suture materials that deliver drugs to
the surrounding tissue have been developed to reduce
the risk of postoperative infection. They offer certain
advantages over conventional suture materials but are
still relatively expensive.39,40
“Smart” sutures made of shape-memory polymers
(SMP) are already being used in minimally invasive car-
diovascular surgery.15,41 They facilitate deep wound
Figs 17 and 18 Vertical double-crossed sutures used for suture closure after the treatment of gingival recession with a modified tunnel technique (suture material: Seralene Blue 6/0 DS-15).
Fig 19 Schematic representation of the vertical double-crossed suture technique (sagittal view).
MF+G
A1
A2
Fig 20 Schematic representation of the vertical double-crossed suture technique for flap and graft stabilization (arrow): Anchor-age is provided by composite resin bonded to the interdental space and the palatal masticatory mucosa (A1, anchor 1; A2, anchor 2; MF+G, mobile flap plus graft).

VOLUME 48 • NUMBER 8 • SEPTEMBER 2017 659
Q U I N T E S S E N C E I N T E R N AT I O N A L
Zuhr et al
closure because they shrink up to form self-tightening
knots when external energy is applied.
“Barbed sutures” with sharp projections (barbs) on
the material surface are currently used in plastic sur-
gery for closure of deeper tissue layers.42-44 They allow
for knotless wound closure after minimally invasive
surgery; the omission of knots eliminates friction and
thus helps to prevent wound irritation.45 Because these
sutures have a relatively strong tendency to develop
large biofilms when left in place for long periods of
time, they seem to be unsuitable for surgical proced-
ures in the oral cavity.40
In cases where immediate hemostasis is not
needed, wound closure with surgical staples is a
time-saving alternative to suture closure.46 Surgical
staples are still mainly used to close macrosurgical
wounds outside the facial region, and the quality of
wound closure is strongly dependent on the nature of
the tissue involved.39
The use of thrombin, fibrin, and cyanoacrylate glues
that cure on contact with weakly basic fluids, such as
water or blood, is an extremely atraumatic and
time-saving method of wound closure.47 Fibrin glues
are now mainly used in general medicine for endo-
scopic procedures; one of their main advantages is
elimination of the need for postoperative suture
removal.48,49 As evidence suggests that glues do not
result in any significant increase in the tensile strength
of closure,50 their hemostatic effect is clearly the main
emphasis. However, tissue adhesives are rarely used in
periodontal and implant surgery today.
The described developmental approaches show
that current and future surgical suture materials devel-
opment tends to be aimed at making simple and
time-saving wound closure possible, even under diffi-
cult conditions, and at accelerating the pace of healing
more actively than in the past. It remains to be seen
which of these new developments will play a role in
reconstructive periodontal and implant surgery in the
future and will translate into clinical applications that
benefit patients.
REFERENCES 1. Burkhardt R, Lang NP. Fundamental principles in periodontal plastic surgery
and mucosal augmentation: a narrative review. J Clin Periodontol 2014;
41(Suppl 15): S98–S107.
2. Burkhardt R, Lang NP. Influence of suturing on wound healing. Periodontol
2000 2015;68: 270–281.
3. Wong ME, Hollinger JO, Pinero GJ. Integrated processes responsible for soft
tissue healing. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1996;82:
475–492.
4. Wikesjo UM, Nilveus R. Periodontal repair in dogs: effect of wound stabiliza-
tion on healing. J Periodontol 1990;61: 719–724.
5. Bhattacharya R, Xu F, Dong G, et al. Effect of bacteria on the wound healing
behavior of oral epithelial cells. PLoS One 2014;9:e89475.
6. Cortellini P, Pini Prato G. Coronally advanced flap and combination therapy for
root coverage. Clinical strategies based on scientific evidence and clinical
experience. Periodontol 2000 2012;59: 158–184.
7. Mormann W, Ciancio SG. Blood supply of human gingiva following periodon-
tal surgery. A fluorescein angiographic study. J Periodontol 1977;48: 681–692.
8. Sculean A, Gruber R, Bosshardt DD. Soft tissue wound healing around teeth
and dental implants. J Clin Periodontol 2014;41(Suppl 15): S6–S22.
9. Burkhardt R, Lang NP. Role of flap tension in primary wound closure of muco-
periosteal flaps: a prospective cohort study. Clin Oral Implants Res 2010;21:
50–54.
10. Bittencourt S, Del Peloso Ribeiro E, Sallum EA, Nociti FH Jr, Casati MZ. Surgical
microscope may enhance root coverage with subepithelial connective tissue
graft: a randomized-controlled clinical trial. J Periodontol 2012;83: 721–730.
11. Burkhardt R, Lang NP. Coverage of localized gingival recessions: comparison
of micro- and macrosurgical techniques. J Clin Periodontol 2005;32: 287–293.
12. Nizam N, Bengisu O, Sonmez S. Micro- and macrosurgical techniques in the
coverage of gingival recession using connective tissue graft: 2 years fol-
low-up. J Esthet Restor Dent 2015;27: 71–83.
13. Shanelec DA. Current trends in soft tissue. J Calif Dent Assoc 1991;19: 57–60.
14. Tibbetts LS, Shanelec DA. An overview of periodontal microsurgery. Curr Opin
Periodontol 1994: 187–193.
15. Dennis C, Sethu S, Nayak S, Mohan L, Morsi YY, Manivasagam G. Suture ma-
terials: Current and emerging trends. J Biomed Mater Res A 2016;104:
1544–1559.
16. Marturello DM, McFadden MS, Bennett RA, Ragetly GR, Horn G. Knot security
and tensile strength of suture materials. Vet Surg 2014;43: 73–79.
17. Brunius U, Zederfeldt B. Suture materials in general surgery. A comment. Prog
Surg 1970;8: 38–44.
18. Gabrielli F, Potenza C, Puddu P, Sera F, Masini C, Abeni D. Suture materials and
other factors associated with tissue reactivity, infection, and wound dehis-
cence among plastic surgery outpatients. Plast Reconstr Surg 2001;107:
38–45.
19. Postlethwait RW, Schauble JF, Dillon ML, Morgan J. Wound healing. II. An
evaluation of surgical suture material. Surg Gynecol Obstet 1959;108:
555–566.
20. Tabanella G. Oral tissue reactions to suture materials: a review. J West Soc
Periodontol Periodontal Abstr 2004;52: 37–44.
21. Meyer RD, Antonini CJ. A review of suture materials, Part I. Compendium
1989;10: 260–262,264–265.
22. Meyer RD, Antonini CJ. A review of suture materials, Part II. Compendium
1989;10: 360–362,364,366–368.
23. Salthouse TN. Biologic response to sutures. Otolaryngol Head Neck Surg
(1979) 1980;88: 658–664.
24. Tajirian AL, Goldberg DJ. A review of sutures and other skin closure materials.
J Cosmet Laser Ther 2010;12: 296–302.
25. Balamurugan R, Mohamed M, Pandey V, Katikaneni HK, Kumar KR. Clinical and
histological comparison of polyglycolic acid suture with black silk suture after
minor oral surgical procedure. J Contemp Dent Pract 2012;13: 521–527.

VOLUME 48 • NUMBER 8 • SEPTEMBER 2017660
Q U I N T E S S E N C E I N T E R N AT I O N A L
Zuhr et al
26. Ethicon. Suture characteristics. Wound closure manual. Available at: http://
www.uphs.upenn.edu/surgery/Education/facilities/measey/Wound_Clo-
sure_Manual.pdf. Accessed 15 June 2016.
27. Lambertz A, Schroder KM, Schob DS, et al. Polyvinylidene fluoride as a suture
material: evaluation of comet tail-like infiltrate and foreign body granuloma.
Eur Surg Res 2015;55: 1–11.
28. Osterberg B, Blomstedt B. Effect of suture materials on bacterial survival in
infected wounds. An experimental study. Acta Chir Scand 1979;145: 431–434.
29. Blomstedt B, Osterberg B, Bergstrand A. Suture material and bacterial trans-
port. An experimental study. Acta Chir Scand 1977;143: 71–73.
30. Haaf U, Breuninger H. [Resorbable suture material in the human skin: tissue
reaction and modified suture technic]. Hautarzt 1988;39: 23–27.
31. Osterberg B. Enclosure of bacteria within capillary multifilament sutures as
protection against leukocytes. Acta Chir Scand 1983;149: 663–668.
32. Wada A, Kubota H, Hatanaka H, Miura H, Iwamoto Y. Comparison of mechan-
ical properties of polyvinylidene fluoride and polypropylene monofilament
sutures used for flexor tendon repair. J Hand Surg Br 2001;26: 212–216.
33. Burkhardt R, Preiss A, Joss A, Lang NP. Influence of suture tension to the
tearing characteristics of the soft tissues: an in vitro experiment. Clin Oral
Implants Res 2008;19: 314–319.
34. Zuhr O, Hürzeler MB (eds). Plastic esthetic periodontal and implant surgery.
Berlin: Quintessence Publishing, 2012: 36–67.
35. Zuhr O, Hürzeler MB (eds). Plastic esthetic periodontal and implant surgery.
Berlin: Quintessence Publishing, 2012: 84–117.
36. Cortellini P, Prato GP, Tonetti MS. The simplified papilla preservation flap. A
novel surgical approach for the management of soft tissues in regenerative
procedures. Int J Periodontics Restorative Dent 1999;19: 589–599.
37. Wachtel H, Fickl S, Zuhr O, Hurzeler MB. The double-sling suture: a modified
technique for primary wound closure. Eur J Esthet Dent 2006;1: 314–324.
38. Zuhr O, Rebele SF, Thalmair T, Fickl S, Hurzeler MB. A modified suture tech-
nique for plastic periodontal and implant surgery: the double-crossed suture.
Eur J Esthet Dent 2009;4: 338–347.
39. Hemming K, Pinkney T, Futaba K, Pennant M, Morton DG, Lilford RJ. A system-
atic review of systematic reviews and panoramic meta-analysis: staples versus
sutures for surgical procedures. PLoS One 2013;8:e75132.
40. Dhom J, Bloes DA, Peschel A, Hofmann UK. Bacterial adhesion to suture ma-
terial in a contaminated wound model: comparison of monofilament, braid-
ed, and barbed sutures. J Orthop Res 2017;35: 925–933.
41. Lendlein A, Langer R. Biodegradable, elastic shape-memory polymers for
potential biomedical applications. Science 2002;296(5573): 1673–1676.
42. Ingle NP, King MW. Optimizing the tissue anchoring performance of barbed
sutures in skin and tendon tissues. J Biomech 2010;43: 302–309.
43. Ingle NP, King MW, Zikry MA. Finite element analysis of barbed sutures in skin
and tendon tissues. J Biomech 2010;43: 879–886.
44. Matarasso A. Introduction to the barbed sutures supplement: the expanding
applications of barbed sutures. Aesthet Surg J 2013;33(3 Suppl):7S–11S.
45. Greenberg JA, Clark RM. Advances in suture material for obstetric and gyne-
cologic surgery. Rev Obstet Gynecol 2009;2: 146–158.
46. Ethicon. Suture characteristics. Wound closure manual. Available at: http://
www.uphs.upenn.edu/surgery/Education/facilities/measey/Wound_Clo-
sure_Manual.pdf. Accessed 15 June 2016.
47. Seewald S, Sriram PV, Naga M, et al. Cyanoacrylate glue in gastric variceal
bleeding. Endoscopy 2002;34: 926–932.
48. Committee AT, Bhat YM, Banerjee S, et al. Tissue adhesives: cyanoacrylate
glue and fibrin sealant. Gastrointest Endosc 2013;78: 209–215.
49. Gogulanathan M, Elavenil P, Gnanam A, Raja VB. Evaluation of fibrin sealant as
a wound closure agent in mandibular third molar surgery: a prospective,
randomized controlled clinical trial. Int J Oral Maxillofac Surg 2015;44:
871–875.
50. Myer CMt, Johnson CM, Postma GN, Weinberger PM. Comparison of tensile
strength of fibrin glue and suture in microflap closure. Laryngoscope
2015;125: 167–170.