optimal timing of resumption of warfarin after...
TRANSCRIPT

Optimal Timing of Resumption of Warfarin AfterIntracranial Hemorrhage
Ammar Majeed, MD; Yang-Ki Kim, MD; Robin S. Roberts, PhD;Margareta Holmstrom, MD, PhD; Sam Schulman, MD, PhD
Background and Purpose—The optimum timing of resumption of anticoagulation after warfarin-related intracranialhemorrhage in patients with indication for continued anticoagulation is uncertain. We performed a large retrospectivecohort study to obtain more precise risk estimates.
Methods—We reviewed charts of 2869 consecutive patients with objectively verified intracranial hemorrhage over 6 yearsat 3 tertiary centers. We calculated the daily risk of intracranial hemorrhage or ischemic stroke with and withoutresumption of warfarin; we focused on patients who survived the first week and had cardiac indication foranticoagulation or previous stroke. Using a Cox model, we estimated rates for these 2 adverse events in relation todifferent time points of resumed anticoagulation. The combined risk of either a new intracranial hemorrhage or anischemic stroke was calculated for a range of warfarin resumption times.
Results—We identified warfarin-associated intracranial hemorrhage in 234 patients (8.2%), of whom 177 patients (76%)survived the first week and had follow-up information available; the median follow-up time was 69 weeks (interquartilerange [IQR] 19–144). Fifty-nine patients resumed warfarin after a median of 5.6 weeks (IQR 2.6–17). The hazard ratiofor recurrent intracranial hemorrhage with resumption of warfarin was 5.6 (95% CI, 1.8–17.2), and for ischemic strokeit was 0.11 (95% CI, 0.014–0.89). The combined risk of recurrent intracranial hemorrhage or ischemic stroke reacheda nadir if warfarin was resumed after approximately 10 to 30 weeks.
Conclusion—The optimal timing for resumption of warfarin therapy appears to be between 10 and 30 weeks afterwarfarin-related intracranial hemorrhage. (Stroke. 2010;41:2860-2866.)
Key Words: intracranial hemorrhage � anticoagulation � ischemic stroke � management
Intracranial hemorrhage is the most feared complication oftreatment with vitamin K antagonists. The incidence of this
hemorrhage is approximately 0.2% per year of treatment.1
Despite the underlying risk of a thromboembolic event inpatients requiring long-term prophylaxis, an intracranial hem-orrhage necessitates temporary discontinuation of a vitaminK antagonist. Depending on the indication for prophylaxis,the withdrawal of anticoagulation exposes the patient to asubstantial risk of thromboembolic complications. Annualrates of 12% to 22% have been reported in patients with St.Jude’s Medical bileaflet heart valves,2 4% to 18% in patientswith atrial fibrillation and additional risk factors for stroke,3
and 10% for patients with recurrent venous thromboembo-lism.4 The decision about when to resume anticoagulationrequires the physician to balance the risk of an additionalbleeding event (particularly of recurrent intracranial hemor-rhage, the risk of which is likely high shortly after the index
bleed, although poorly studied) with the risk of thromboem-bolism in the absence of anticoagulation.
A limited number of observational studies have addressedthe question posed in this study.5–12 These studies generallyincluded few patients who were followed at a single centerand had limited follow-up. Several of the authors and theAmerican Stroke Association13 suggest restarting anticoagu-lation after a period of 7 to 14 days following intracranialhemorrhage. A recent systematic review of studies in patientswith mechanical heart valves reached the same conclusionbased on only 2 recurrent hemorrhages and 4 strokes.14 Sevenexperts expressed the opinion that warfarin could be restartedin stable patients 3 to 10 days after intracranial hemorrhage.15
We performed this study to address the timing of resump-tion of warfarin after intracranial hemorrhage and assess therisks and benefits both in patients who restarted warfarin andthose who did not. To our knowledge, this is the first
Received June 9, 2010; accepted September 13, 2010.From the Department of Hematology (A.M., M.H., S.S.), Karolinska University Hospital and Karolinska Institute, Stockholm, Sweden; Department
of Medicine (A.M.), Malar Hospital, Eskilstuna, Sweden; Department of Medicine (Y.-K.K.), Soonchunhyang University, Seoul, Korea; Department ofClinical Epidemiology and Biostatistics (R.S.R.) and Department of Medicine (Y.-K.K., S.S.), McMaster University and Thrombosis AtherosclerosisResearch Institute (R.S.R., S.S.), Hamilton, ON, Canada.
S.S. planned and supervised the study. M.H. contributed to the implementation of the study at the Swedish sites. A.M. and Y.-K.K. performed the chartreview. R.S.R. and S.S. performed the statistical analyses. A.M. and S.S. wrote the manuscript, and all the other authors critically reviewed the manuscript.
Correspondence to Sam Schulman, MD, Thrombosis Service, HHS-General Hospital, 237 Barton Street East, Hamilton, ON L8L 2X2, Canada. [email protected]
© 2010 American Heart Association, Inc.
Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.110.593087
2860
by guest on July 3, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on July 3, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on July 3, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on July 3, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on July 3, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on July 3, 2018http://stroke.ahajournals.org/
Dow
nloaded from

multicenter study with analysis of the optimal timing ofresumption of anticoagulation performed by calculating haz-ards of recurrent hemorrhage and of ischemic stroke, with orwithout warfarin.
MethodsThe study was conducted at 3 tertiary care hospitals: KarolinskaUniversity Hospital in Solna-Stockholm, and Karolinska UniversityHospital in Huddinge-Stockholm, both in Sweden; and at HamiltonHealth Sciences-General Hospital, Ontario, Canada. One investiga-tor in each country (A.M. in Sweden and Y.-K.K. in Canada)reviewed the charts of all patients admitted between January 2002and December 2007 in Canada, and between January 2004 andDecember 2008 in Sweden, who had a diagnosis of intracranialhemorrhage (ICD-10 diagnosis code I600-I629). Data from patientswith warfarin-associated intracranial hemorrhage underwent a finalreview by a third investigator (S.S.).
The Institutional Ethics Committees in both countries approvedthis retrospective study and waived the need for consent frompatients. Patients who were being treated with warfarin at the time ofdiagnosis of intracranial hemorrhage, and who had an internationalnormalized ratio of �1.5 at the time the bleeding occurred, wereincluded in the study. The diagnosis had to be radiologicallyconfirmed. Any combination of intracerebral hemorrhage with sub-dural or subarachnoid hemorrhage was classified as intracerebral.We excluded from our analysis patients with hemorrhage caused bysevere accidents, with multi-trauma, or those with hemorrhagictransformation of ischemic stroke.
Data regarding patient characteristics, indication for warfarintreatment, risk score for stroke in patients with atrial fibrillation,3
additional antithrombotic treatment, international normalized ratio atpresentation, cause of bleeding (spontaneous or traumatic), locationof bleeding according to radiological investigations, and neurosur-gical intervention were collected. From the follow-up period afterintracranial hemorrhage, we collected data on resumption of warfa-rin, recurrent intracranial bleeding, ischemic stroke, systemic embo-lism, transitory ischemic attacks, heart valve thrombosis, venousthromboembolism, death, and the timing of these events in relationto the index intracranial hemorrhage. The data were retrieved fromelectronic hospital charts and by contacting each patient’s familyphysician.
Our aim was to describe the occurrences of recurrent bleeding,thromboembolic complications, and death in patients surviving thefirst week after the index intracranial hemorrhage. The reason forthis focus was that resumption of anticoagulation with vitamin Kantagonists during the first week has rarely been recommended.Furthermore, patients with such short survival are usually very illand are not considered for anticoagulant therapy during this limitedperiod. In addition, we focused the analysis on patients who were ata moderate-to-high risk of ischemic stroke, including those withatrial fibrillation, mechanical heart valves, left ventricle thrombus, orprevious ischemic stroke.
Binomial data were analyzed with the �2 test, and continuousvariables were analyzed with Student t-test or Mann–Whitney forskewed distributions. Median value and interquartile range (IQR)were used to describe these skewed distributions. Cumulative riskswere estimated with Kaplan–Meier analysis. A Cox model was fittedfor recurrent intracranial hemorrhage and separately for ischemiccerebral events, with a time-dependent variable indicating the time atwhich warfarin was resumed (if at all). The assumption in the Coxmodel was that from the time of resumption, warfarin exerts aconstant proportional effect on the risk of recurrent intracranialhemorrhage, and exerts a constant proportional reduction of the riskof ischemic events. The software for calculations was SAS7STAT 9(SAS Institute Inc.). The results of the Cox models yielded estimatesof the risks per day (hazards) of intracranial hemorrhage or ofthromboembolic event, with and without warfarin treatment, overtime since the qualifying event. Based on these estimates, wecomputed the cumulative risks over treatment horizons between 3
and 6 years, and with warfarin resumption commencing between 1and 50 weeks after the index intracranial hemorrhage.
ResultsDemographicsWe identified and reviewed retrospectively the records of all3287 admissions for 2869 consecutive patients diagnosedwith intracranial hemorrhage at the 3 centers. Two hundredthirty-four patients (8.2%) fulfilled the criteria for inclusionin the study. The baseline characteristics of the patients aredescribed in Table 1. Few patients were identified withintracranial pathology as secondary cause of intracerebralhemorrhage: 4 patients with aneurysms, 4 patients withamyloid angiopathy, 2 patients with tumors, and 1 patientwith a ruptured colloid cyst. The number of patients whowere reviewed, included in the study, and had resumption ofanticoagulation at the 3 sites of investigation is shown inTable 2.
MortalityWe had access to follow-up information on the 234 patientsregarding major clinical events for a median of 34 weeks(IQR 1–115). For the 177 patients who survived the firstweek, the median follow-up duration was 69 weeks (IQR19–144). Overall, 113 patients (48%) died during the follow-up, corresponding to a median survival of 4.5 years. Fifty-seven patients (24%) died within the first week: 54 patientsbecause of progression of bleeding and/or herniation (1patient also had massive pulmonary embolism), 2 patientsfrom ischemic stroke, and 1 patient from myocardial infarc-tion. Fatal outcome within the first week occurred in 47 of allpatients (36%) with intracerebral hemorrhage, 3 patients(14%) with subarachnoid hemorrhage, and 7 patients (8%)with subdural hematoma. During the entire follow-up, mor-tality among those with intracerebral hemorrhage was 59%,compared with 32% after subdural hematoma (Kaplan–Meieranalysis, P�0.001). Recurrent intracranial hemorrhage wasfatal in 4 of 18 patients (22%). In contrast, with the 21patients (12%) who experienced a subsequent arterial throm-boembolic event, none of those events were fatal.
Resumption of WarfarinFifty-nine patients (33%) resumed warfarin. The patients forwhom warfarin was restarted were younger and had a longerfollow-up than did the remainder (Table 1). Warfarin wasrestarted in 22 of the patients with atrial fibrillation (22%), 8of the patients with venous thromboembolism (27%), 15 ofthe patients with mechanical aortic valve (79%), and 7 of thepatients with mechanical mitral valve (77%). There was ahighly significant difference between the proportions ofrestarted patients among those with mechanical valves com-pared with those of the remainder (P�0.001). Warfarin wasresumed in 23 of all first-week survivors after intracerebralhemorrhage (28%), in 7 patients with subarachnoid hemorrhage(39%), and in 29 patients with subdural hematoma (38%).Resumption occurred after a median of 4.4 weeks (IQR 2.3–14)in patients with intracerebral hemorrhage, compared with 6.4weeks (IQR 3.6–26) after subdural hematoma.
Majeed et al Warfarin Resumption After Intracranial Hemorrhage 2861
by guest on July 3, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Finally, warfarin was restarted in 10 of those with previousstroke (31%) versus 49 of those without (34%). There wereno statistically significant differences in any of thoseproportions.
Resumption of warfarin occurred after a median durationof 5.6 weeks (IQR 2.6–17) for all first-week survivors, after9.2 weeks (IQR 5.6–34) for patients with atrial fibrillation,after 4.6 weeks (IQR 2.3–15) for patients with mechanical
Table 1. Characteristics of the Patients at Baseline
CharacteristicTotal
PatientsFirst-WeekSurvivors
With Cardiac Indication*
WarfarinResumed
WarfarinNot Resumed
n 234 177 45 87
Age, median (IQR) 76 (67–81) 75 (65–80) 70 (63–77) 78 (70.5–72)†
Male sex, n (%) 142 (61) 112 (63) 31 (69) 56 (64)
Indication for anticoagulation, n (%)‡
Atrial fibrillation 135 (58) 102 (58) 22 (49) 79 (91)
Risk score CHADS2�0 1 (1) 1 (1) 0 (0) 1 (1)
Risk score CHADS2�1 23 (17) 20 (20) 6 (27) 14 (18)
Risk score CHADS2�2 44 (33) 34 (33) 6 (27) 28 (35)
Risk score CHADS2�3 23 (17) 18 (18) 4 (18) 13 (16)
Risk score CHADS2�4 25 (19) 19 (19) 4 (18) 15 (19)
Risk score CHADS2�5 14 (11) 7 (7) 2 (9) 5 (6)
Risk score CHADS2�6 1 (1) 1 (1) 0 (0) 1 (1)
Unknown 4 (3) 2 (2) 0 (0) 2 (3)
Venous thromboembolism 37 (16) 30 (17) 0 (0) 0 (0)
Mechanical aortic valve 24 (10) 19 (11) 15 (33) 4 (5)
Mechanical mitral valve 11 (5) 9 (5) 7 (16) 2 (2)
Other 27 (11) 17 (10) 1 (2) 2 (2)
Additional antithrombotic treatment, n (%)
None 205 (88) 158 (89) 40 (89) 78 (90)
Aspirin 23 (10) 14 (8) 3 (7) 8 (9)
Clopidogrel 1 (0.4) 1 (0.5) 0 0
Aspirin and clopidogrel 5 (2) 4 (2) 2 (4) 1 (1)
Triggering factor, n (%)
Spontaneous§ 154 (66) 111 (63) 26 (58) 56 (64)
Fall or moderate trauma 51 (22) 44 (25) 13 (29) 25 (29)
Poorly controlled hypertension 11 (5) 10 (5) 3 (7) 3 (3)
Amyloid angiopathy 4 (2) 4 (2) 0 3 (3)
Unknown 14 (6) 8 (5) 3 (7) 0
INR on admission, median (IQR) 2.65 (2.2–3.5) 2.6 (2.1–3.4) 2.5 (2.0–3.4) 2.6 (2.2–3.4)
Type of intracranial hemorrhage, n (%)
Intracerebral 130 (55) 83 (47) 18 (40) 44 (51)
Lobar 54 (42) 48 (58) 10 (56) 27 (61)
Deep hemispheric 53 (41) 29 (35) 7 (39) 15 (34)
Brainstem 15 (12) 3 (4) 0 1 (2)
Unclear 8 (6) 3 (4) 1 (6) 1 (2)
Subdural 83 (36) 76 (43) 22 (49) 35 (40)
Subarachnoid 21 (9) 18 (10) 5 (11) 8 (9)
Evacuation of hematoma, n (%) 81 (35) 73 (41) 20 (44) 32 (37)
Follow-up, weeks, median (IQR) 34 (1–115) 69 (19–144) 140 (69–207) 49 (4.3–100)†
INR, international normalized ratio.*These 132 patients are the basis for the risk modeling.†P�0.001 (Mann–Whitney test) in the comparison of those who resumed warfarin or did not.‡P�0.001 (Pearson �2 test for multiple groups, followed by 2-group comparison of mechanical valves vs other
indications using Fisher exact test) in the comparison of those who resumed warfarin or did not.§In this subset, there are 4 patients with aneurysm/arterio-venous malformation, 2 with tumors, and 1 with
ruptured colloid cyst.
2862 Stroke December 2010
by guest on July 3, 2018http://stroke.ahajournals.org/
Dow
nloaded from

aortic valve, after 3.1 weeks (IQR 2.2–14) for patients withmechanical mitral valve, and after 2.3 weeks (IQR 1.7–19)for patients with venous thromboembolism.
Recurrent Intracranial HemorrhageRecurrent intracranial hemorrhage was observed in 18 pa-tients (10%); 8 of those patients restarted warfarin and 10 ofthose patients did not, although 2 of the latter patientssubsequently resumed warfarin treatment. Twelve patientswith subdural hematoma (16%; 4 had resumed warfarin and8 patients had not) and 6 patients with intracerebral hemor-rhage (7%; 4 had resumed warfarin and 2 patients had not)developed recurrent intracranial hemorrhage, versus none ofthose with subarachnoid hemorrhage (P�0.1). Kaplan–Meieranalysis showed a trend toward higher risk of recurrence inpatients with subdural hematoma (16%) compared with thosewith intracerebral hemorrhage (8.4%); (P�0.07). Among thepatients with intracerebral hemorrhage, it recurred in 4patients with lobar localization and in 1 patient each withdeep hemispheric or brain stem localization. The type ofrecurrence was generally the same as it was in the indexbleeding, except for 1 patient with initial intracerebral hem-orrhage in which it recurred as subdural, and another patientwith the opposite sequence. The cumulative risk of recurrentintracranial hemorrhage without restarted anticoagulation orfrom the time point of resumption of anticoagulation is shownin Figure 1A and 1B, respectively.
Thromboembolic EventsAmong the 21 patients who suffered a subsequent arterialthromboembolic event, 2 patients had systemic embolism(brachial artery and femoral artery), 1 patient had a transientischemic attack, and 18 patients suffered an ischemic stroke.Strokes occurred in 12 patients (12%) with atrial fibrillation,in 4 patients (14%) with mechanical heart valves, in 1 patient(3%) with venous thromboembolism, and in 1 patient (6%)with another indication for warfarin. Kaplan–Meier analysisshowed a significantly higher risk of arterial thromboembo-lism in patients with previous stroke (28%) compared withthose without (8.6%); (P�0.004). The cumulative risk ofischemic events without restarted anticoagulation or from thetime point of resumption of anticoagulation is shown inFigure 1A and 1B, respectively.
Eleven patients (5%) developed symptomatic venousthromboembolism following warfarin cessation, after a me-dian of 2 weeks (IQR, 1.5–5) from the intracranial hemor-rhage; in 4 of these patients, the initial indication for warfarinwas venous thromboembolism.
Risk ModelingThe modeling of risk for recurrent intracranial hemorrhageversus ischemic stroke in patients with or without resumptionof warfarin therapy is based on the population with cardiacindication for anticoagulation and/or with previous ischemicstroke and who had survived the first week without arecurrent event (n�132; Table 1).
As might be expected, fitting separate Cox models with atime-dependent variable to indicate the point at which war-farin was restarted revealed strong effects of anticoagulationresumption. Restarting warfarin increased the risk of recur-rent intracranial hemorrhage by more than a factor of 5 (HR5.57; 95% CI, 1.80–17.25; P�0.0029), whereas the risk of athromboembolic event was reduced by almost 90% (HR 0.11;95% CI, 0.14–0.87; P�0.036). These model-based estimatesare apparent in the raw data displayed in the top panel ofTable 3. There, time is divided into periods with reasonablyconstant risk, which differ somewhat among recurrent hem-orrhage and ischemic stroke, as these have independentnatural courses. Within each time period, we show theobserved number of events and the number of days at risk,separately for days when patients are receiving versus not
Table 2. Distribution of Patients at the 3 Sites of Investigation
HamiltonHealth
Sciences,General Site
KarolinskaUniversityHospital,
Solna
KarolinskaUniversityHospital,Huddinge
TotalPatients
Admissions* for intracranialhemorrhage, n
1397 1105 785 3287
Patients with intracranialhemorrhage, n
1371 895 603 2869
Warfarin-associatedintracranial hemorrhage,n (%)
117 (8.5) 59 (6.6) 58 (9.6) 234 (8.2)
Patients restarted onwarfarin, n (%)
33 (28) 11 (19) 15 (26) 59 (25)
*Some patients had �1 admission.
TIME SINCE QUALIFYING ICH (WEEKS)
CU
MU
LA
TIV
E R
ISK
(%
)
0 50 100 150
0
5
10
15
20
25
30
ATRISK
ICH 177 56 35 16IE 177 54 34 15
ICH
IE
TIME SINCE WARFARIN START (WEEKS)
CU
MU
LA
TIV
E R
ISK
(%
)0 50 100 150
0
5
10
15
20
25
30
ATRISK
ICHIE
59 42 29 2259 47 32 24
IE
ICH
A
B
Figure 1. Cumulative risk of recurrent intracranial hemorrhage(ICH) and ischemic event (IE) without resumption of warfarin (A)and from the time point of resuming warfarin (B).
Majeed et al Warfarin Resumption After Intracranial Hemorrhage 2863
by guest on July 3, 2018http://stroke.ahajournals.org/
Dow
nloaded from
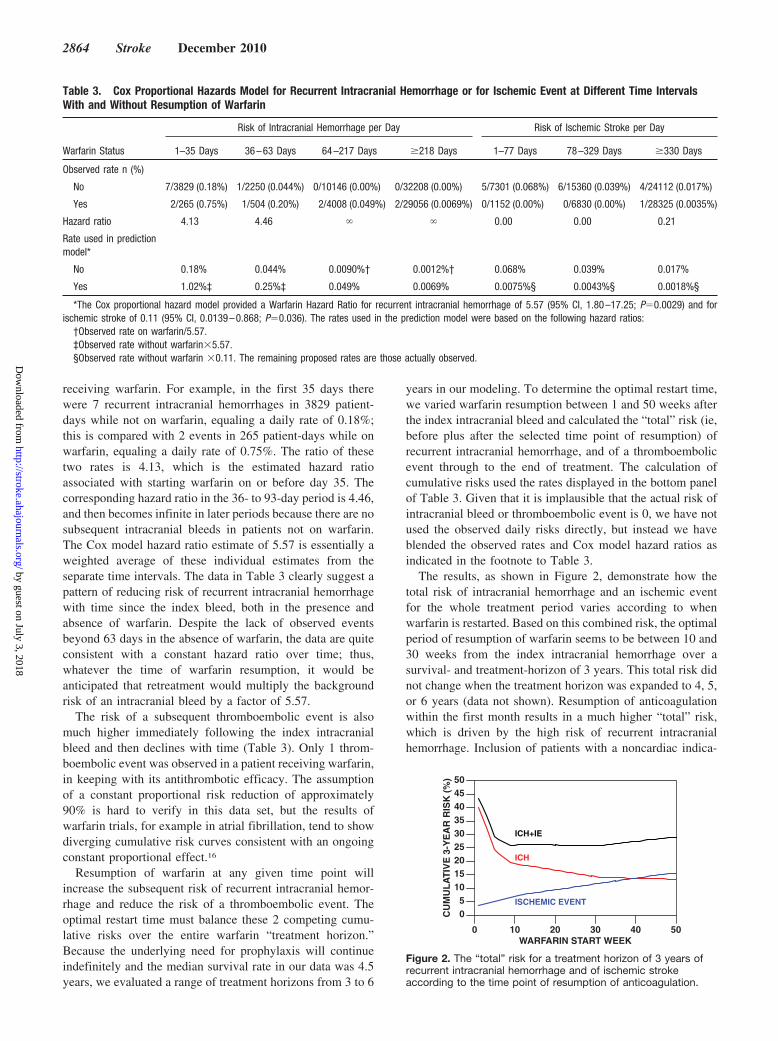
receiving warfarin. For example, in the first 35 days therewere 7 recurrent intracranial hemorrhages in 3829 patient-days while not on warfarin, equaling a daily rate of 0.18%;this is compared with 2 events in 265 patient-days while onwarfarin, equaling a daily rate of 0.75%. The ratio of thesetwo rates is 4.13, which is the estimated hazard ratioassociated with starting warfarin on or before day 35. Thecorresponding hazard ratio in the 36- to 93-day period is 4.46,and then becomes infinite in later periods because there are nosubsequent intracranial bleeds in patients not on warfarin.The Cox model hazard ratio estimate of 5.57 is essentially aweighted average of these individual estimates from theseparate time intervals. The data in Table 3 clearly suggest apattern of reducing risk of recurrent intracranial hemorrhagewith time since the index bleed, both in the presence andabsence of warfarin. Despite the lack of observed eventsbeyond 63 days in the absence of warfarin, the data are quiteconsistent with a constant hazard ratio over time; thus,whatever the time of warfarin resumption, it would beanticipated that retreatment would multiply the backgroundrisk of an intracranial bleed by a factor of 5.57.
The risk of a subsequent thromboembolic event is alsomuch higher immediately following the index intracranialbleed and then declines with time (Table 3). Only 1 throm-boembolic event was observed in a patient receiving warfarin,in keeping with its antithrombotic efficacy. The assumptionof a constant proportional risk reduction of approximately90% is hard to verify in this data set, but the results ofwarfarin trials, for example in atrial fibrillation, tend to showdiverging cumulative risk curves consistent with an ongoingconstant proportional effect.16
Resumption of warfarin at any given time point willincrease the subsequent risk of recurrent intracranial hemor-rhage and reduce the risk of a thromboembolic event. Theoptimal restart time must balance these 2 competing cumu-lative risks over the entire warfarin “treatment horizon.”Because the underlying need for prophylaxis will continueindefinitely and the median survival rate in our data was 4.5years, we evaluated a range of treatment horizons from 3 to 6
years in our modeling. To determine the optimal restart time,we varied warfarin resumption between 1 and 50 weeks afterthe index intracranial bleed and calculated the “total” risk (ie,before plus after the selected time point of resumption) ofrecurrent intracranial hemorrhage, and of a thromboembolicevent through to the end of treatment. The calculation ofcumulative risks used the rates displayed in the bottom panelof Table 3. Given that it is implausible that the actual risk ofintracranial bleed or thromboembolic event is 0, we have notused the observed daily risks directly, but instead we haveblended the observed rates and Cox model hazard ratios asindicated in the footnote to Table 3.
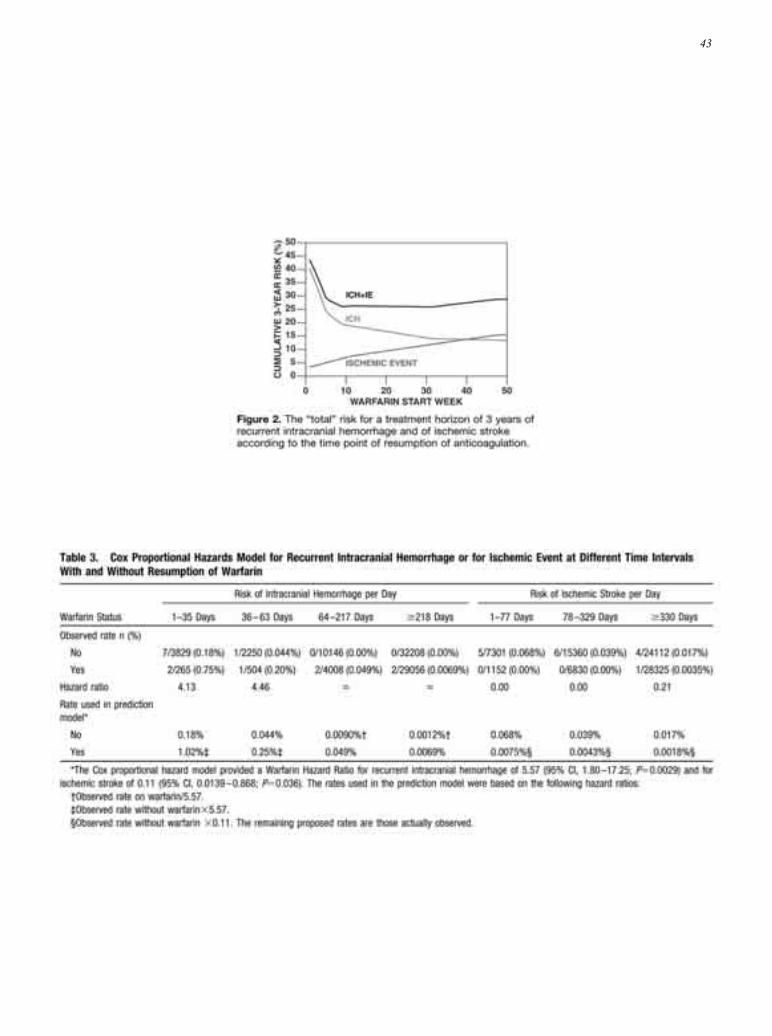
The results, as shown in Figure 2, demonstrate how thetotal risk of intracranial hemorrhage and an ischemic eventfor the whole treatment period varies according to whenwarfarin is restarted. Based on this combined risk, the optimalperiod of resumption of warfarin seems to be between 10 and30 weeks from the index intracranial hemorrhage over asurvival- and treatment-horizon of 3 years. This total risk didnot change when the treatment horizon was expanded to 4, 5,or 6 years (data not shown). Resumption of anticoagulationwithin the first month results in a much higher “total” risk,which is driven by the high risk of recurrent intracranialhemorrhage. Inclusion of patients with a noncardiac indica-
Table 3. Cox Proportional Hazards Model for Recurrent Intracranial Hemorrhage or for Ischemic Event at Different Time IntervalsWith and Without Resumption of Warfarin
Warfarin Status
Risk of Intracranial Hemorrhage per Day Risk of Ischemic Stroke per Day
1–35 Days 36–63 Days 64–217 Days �218 Days 1–77 Days 78–329 Days �330 Days
Observed rate n (%)
No 7/3829 (0.18%) 1/2250 (0.044%) 0/10146 (0.00%) 0/32208 (0.00%) 5/7301 (0.068%) 6/15360 (0.039%) 4/24112 (0.017%)
Yes 2/265 (0.75%) 1/504 (0.20%) 2/4008 (0.049%) 2/29056 (0.0069%) 0/1152 (0.00%) 0/6830 (0.00%) 1/28325 (0.0035%)
Hazard ratio 4.13 4.46 � � 0.00 0.00 0.21
Rate used in predictionmodel*
No 0.18% 0.044% 0.0090%† 0.0012%† 0.068% 0.039% 0.017%
Yes 1.02%‡ 0.25%‡ 0.049% 0.0069% 0.0075%§ 0.0043%§ 0.0018%§
*The Cox proportional hazard model provided a Warfarin Hazard Ratio for recurrent intracranial hemorrhage of 5.57 (95% CI, 1.80–17.25; P�0.0029) and forischemic stroke of 0.11 (95% CI, 0.0139–0.868; P�0.036). The rates used in the prediction model were based on the following hazard ratios:
†Observed rate on warfarin/5.57.‡Observed rate without warfarin�5.57.§Observed rate without warfarin �0.11. The remaining proposed rates are those actually observed.
WARFARIN START WEEK
CU
MU
LA
TIV
E 3
-YE
AR
RIS
K (
%)
0 10 20 30 40 50
05
101520253035404550
ICH
ISCHEMIC EVENT
ICH+IE
Figure 2. The “total” risk for a treatment horizon of 3 years ofrecurrent intracranial hemorrhage and of ischemic strokeaccording to the time point of resumption of anticoagulation.
2864 Stroke December 2010
by guest on July 3, 2018http://stroke.ahajournals.org/
Dow
nloaded from

tion for warfarin or without previous stroke in this analysisdid not change the outcome (data not shown).
DiscussionWe are reporting results from a large cohort of patients withwarfarin-induced intracranial hemorrhage. Our analysis ofpatients with a high risk for arterial thromboembolic compli-cations and the extended follow-up enabled us to estimate theoptimal time interval for resumption of warfarin, taking intoaccount the risk for recurrent intracranial hemorrhage as wellas for ischemic stroke. In contradiction to previous studies,our data suggest that warfarin resumption should be delayedat least a month from the index event. With 100 patientsresuming anticoagulation 2 weeks, 5 weeks, or 10 weeks afterwarfarin-associated hemorrhage, there would, according toour modeling, be during a 3-year treatment horizon 36, 24, or19 recurrent intracranial hemorrhages versus 4, 5, or 7ischemic events, respectively.
The ideal design would have been a randomization be-tween early and late resumption of anticoagulation, but thisposes substantial logistical challenges. We needed approxi-mately 5 years of consecutive cases from 3 tertiary referralcenters to collect sufficient data for our analysis. We chose toanalyze only recurrent major bleeds that were intracranialbecause of the clinical burden and the high risk of chronicsequel and death. The only thromboembolic complication ofsimilar severity is ischemic stroke, and we therefore excludedtransitory ischemic attacks and systemic embolism from ouranalysis. Our hazards model was focused on patients with acardiac indication for anticoagulation or with previous strokebecause when untreated, these conditions confer a moderate-to-high risk of ischemic stroke. Clinicians are usually lesshesitant about permanent discontinuation of anticoagulationif the initial indication was venous thromboembolism.
In a systematic review of 6 retrospective studies, whichincluded 120 patients with mechanical heart valves and intra-cranial hemorrhage, the authors concluded that it wassafe to resume warfarin within 2 weeks.14 All 6 studies wereeither small or had a very limited follow-up, and only 2recurrent intracranial hemorrhages and 4 ischemic strokeswere reported. These studies did not include patients withatrial fibrillation and additional risk factors for stroke, orpatients with myocardial infarction and intramural thrombus;both groups are also of interest due to high risk of stroke. Arecently published systematic review with 492 patients con-cluded that anticoagulation may be resumed after 72 hours.17
This review included a large number of single-case reportswith a high risk for bias toward successful cases, and theauthors considered all anticoagulants of any dose together.The hitherto largest cohort included 141 patients, of whom 35patients resumed warfarin; however, the follow-up was only30 days, which may explain why no recurrent intracranialhemorrhage was observed.10 The second-largest cohort had52 patients, of whom 23 patients resumed warfarin, reported3 recurrent intracranial hemorrhages and 3 ischemic strokesduring a mean follow-up of 43 months.9 These small numbersof events do not allow statistical analysis of the optimal timeof resumption of anticoagulation. Eckman et al addressed thisquestion by using a Markov model, and concluded that
patients with deep hemispheric location of the hemorrhage(which had a reported low risk of recurrence) would qualifyfor resumption of anticoagulation, provided that the risk ofischemic stroke was high.18 Conversely, patients with lobarhemorrhage, which appears to carry a higher risk of recur-rence, should never be restarted on anticoagulation. Thisanalysis focused on patients who had atrial fibrillation and anaverage risk of stroke of 4.5% per year. We had too-smallnumbers of each of the subtypes of intracerebral hemorrhagewith recurrence to confirm those assumptions. Furthermore,the risk for ischemic stroke varies widely, and for a patientwith a previous stroke, the risk of recurrence (28% in ourmaterial) may justify resumption of anticoagulation for apatient with lobar hemorrhage as well.
The main limitation of our study is the retrospective designwith resumption of anticoagulation occurring at different timepoints. The choice of time point might have been biased bythe fear of the clinician of recurrent bleeding or of ischemicstroke; this seems to have been the case for patients withmechanical valves who were restarted on warfarin morefrequently than for other subsets. However, those with pre-vious stroke were treated in a similar manner to thosewithout, despite higher risk for new ischemic events. Amongpatients with subdural hematoma and a high risk for recurrenthemorrhage, the rate of resumption was as high as it was forother patients. Although warfarin was resumed more fre-quently in younger patients, we did not observe a differencein the risk for recurrent intracranial hemorrhage or ischemicevents depending on age (data not shown). Another limitationof our study is the significantly shorter follow-up of patientswho were not restarted on warfarin. However, with a medianof 39 weeks of observation in this subset, the period with thehighest event rate should have been covered.
We acknowledge that our conclusions are based on rela-tively few clinical events. However, our study includes moreevents than does any previous study or systematic review. Wehave shown that the initial risk for recurrent intracranialhemorrhage increases 5-fold when warfarin is resumed, andthat the risk of recurrent bleeding with resumed warfarin ishigher than is the risk of ischemic events without anticoag-ulation. Resumption of warfarin can therefore be delayed bymore than 1 month after the index event. In fact, the optimalperiod for resumption of anticoagulation seems to occurbetween week 10 and week 30 after warfarin-associatedintracranial hemorrhage, when the risk for recurrent intracra-nial hemorrhage and the risk for ischemic stroke are takeninto account. Our findings contradict the recommendationsmade in previous studies and expert opinion. The largernumber of patients included in this study, the longer follow-up, and the modeling we performed have allowed for a moreprecise description of the total risk for serious events inrelation to the timing of resumed anticoagulation. The span ofthis interval of 20 weeks may be helpful to select whenpatients with a perceived high risk for bleeding versus highrisk for stroke should be restarted.
Sources of FundingNo external funding was obtained for this study. Y.-K.K. receivedsalary support from Soonchunhyang University while performing the
Majeed et al Warfarin Resumption After Intracranial Hemorrhage 2865
by guest on July 3, 2018http://stroke.ahajournals.org/
Dow
nloaded from

study at McMaster University. A.M. received PhD-student supportfrom the Research and Development center, Eskilstuna, Sweden.
DisclosuresS.S. has received consulting fees from Astra-Zeneca, Bayer Health-Care, Boehringer Ingelheim, GlaxoSmith-Kline, Octapharma, andSanofi-Aventis; lecture fees from LEO Pharma, Sanofi-Aventis, andBoehringer Ingelheim; and grant support from Bayer HealthCare.M.H. has received lecture fees from Baxter Medical, CSL Behring,Leo-Pharma, and Nycomed, and travel support from Leo Pharma andSwedish Orphan. A.M., R.R., and Y.-K.K. have no potential con-flicts of interest to declare.
References1. Schulman S, Beyth RJ, Kearon C, Levine MN. Hemorrhagic compli-
cations of anticoagulant and thrombolytic treatment: American college ofchest physicians evidence-based clinical practice guidelines (8th edition).Chest. 2008;133:257S–298S.
2. Salem DN, O’Gara PT, Madias C, Pauker SG. Valvular and structuralheart disease: American college of chest physicians evidence-basedclinical practice guidelines (8th edition). Chest. 2008;133:593S–629S.
3. Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, RadfordMJ. Validation of clinical classification schemes for predicting stroke:Results from the national registry of atrial fibrillation. JAMA. 2001;285:2864–2870.
4. Kearon C, Kahn SR, Agnelli G, Goldhaber S, Raskob GE, Comerota AJ.Antithrombotic therapy for venous thromboembolic disease: Americancollege of chest physicians evidence-based clinical practice guidelines(8th edition). Chest. 2008;133:454S–545S.
5. Ananthasubramaniam K, Beattie JN, Rosman HS, Jayam V, Borzak S.How safely and for how long can warfarin therapy be withheld inprosthetic heart valve patients hospitalized with a major hemorrhage?Chest. 2001;119:478–484.
6. Babikian VL, Kase CS, Pessin MS, Caplan LR, Gorelick PB. Resumptionof anticoagulation after intracranial bleeding in patients with prostheticheart valves. Stroke. 1988;19:407–408.
7. Bertram M, Bonsanto M, Hacke W, Schwab S. Managing the therapeuticdilemma: Patients with spontaneous intracerebral hemorrhage and urgentneed for anticoagulation. J Neurol. 2000;247:209–214.
8. Butler AC, Tait RC. Restarting anticoagulation in prosthetic heart valvepatients after intracranial haemorrhage: A 2-year follow-up. Br JHaematol. 1998;103:1064–1066.
9. Claassen DO, Kazemi N, Zubkov AY, Wijdicks EF, Rabinstein AA.Restarting anticoagulation therapy after warfarin-associated intracerebralhemorrhage. Arch Neurol. 2008;65:1313–1318.
10. Phan TG, Koh M, Wijdicks EF. Safety of discontinuation of anticoagu-lation in patients with intracranial hemorrhage at high thromboembolicrisk. Arch Neurol. 2000;57:1710–1713.
11. Punthakee X, Doobay J, Anand SS. Oral-anticoagulant-related intracere-bral hemorrhage. Thromb Res. 2002;108:31–36.
12. Wijdicks EF, Schievink WI, Brown RD, Mullany CJ. The dilemma ofdiscontinuation of anticoagulation therapy for patients with intracranialhemorrhage and mechanical heart valves. Neurosurg. 1998;42:769–773.
13. Broderick J, Connolly S, Feldmann E, Hanley D, Kase C, Krieger D,Mayberg M, Morgenstern L, Ogilvy CS, Vespa P, Zuccarello M.Guidelines for the management of spontaneous intracerebral hemorrhagein adults: 2007 update: A guideline from the american heart association/american stroke association stroke council, high blood pressure researchcouncil, and the quality of care and outcomes in research interdisciplinaryworking group. Circ. 2007;116:e391–e413.
14. Romualdi E, Micieli E, Ageno W, Squizzato A. Oral anticoagulanttherapy in patients with mechanical heart valve and intracranial haemor-rhage. A systematic review. Thromb Haemost. 2009;101:290–297.
15. Aguilar MI, Hart RG, Kase CS, Freeman WD, Hoeben BJ, Garcia RC,Ansell JE, Mayer SA, Norrving B, Rosand J, Steiner T, Wijdicks EF,Yamaguchi T, Yasaka M. Treatment of warfarin-associated intracerebralhemorrhage: Literature review and expert opinion. Mayo Clin Proc.2007;82:82–92.
16. van Walraven C, Hart RG, Singer DE, Laupacis A, Connolly S, PetersenP, Koudstaal PJ, Chang Y, Hellemons B. Oral anticoagulants vs aspirin innonvalvular atrial fibrillation: An individual patient meta-analysis. JAMA.2002;288:2441–2448.
17. Hawryluk GW, Austin JW, Furlan JC, Lee JB, O’Kelly C, Fehlings MG.Management of anticoagulation following central nervous system hem-orrhage in patients with high thromboembolic risk. J Thromb Haemost.2010;8:1500–1508.
18. Eckman MH, Rosand J, Knudsen KA, Singer DE, Greenberg SM. Canpatients be anticoagulated after intracerebral hemorrhage? A decisionanalysis. Stroke. 2003;34:1710–1716.
2866 Stroke December 2010
by guest on July 3, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Ammar Majeed, Yang-Ki Kim, Robin S. Roberts, Margareta Holmström and Sam SchulmanOptimal Timing of Resumption of Warfarin After Intracranial Hemorrhage
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 2010 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/STROKEAHA.110.593087
2010;41:2860-2866; originally published online October 28, 2010;Stroke.
http://stroke.ahajournals.org/content/41/12/2860World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org/content/suppl/2013/10/02/STROKEAHA.110.593087.DC2 http://stroke.ahajournals.org/content/suppl/2012/03/12/STROKEAHA.110.593087.DC1
Data Supplement (unedited) at:
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOnce the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Strokein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on July 3, 2018http://stroke.ahajournals.org/
Dow
nloaded from

42 Stroke Vol. 4, No. 1
Abstract 14
43

Stroke 日本語版 Vol. 5, No. 424
頭蓋内出血後のワルファリン再開の最適時期Optimal Timing of Resumption of Warfarin After Intracranial Hemorrhage
Ammar Majeed, MD1,2; Yang-Ki Kim, MD3,5; Robin S. Roberts, PhD4,6; Margareta Holmström, MD, PhD1; Sam Schulman, MD, PhD1,5,6
1 Department of Hematology, Karolinska University Hospital and Karolinska Institute, Stockholm, Sweden; 2 Departmentof Medicine, Mälar Hospital, Eskilstuna, Sweden; 3 Department of Medicine, Soonchunhyang University, Seoul, Korea; 4 Department of Clinical Epidemiology and Biostatistics and 5 Department of Medicine, McMaster University and 6 Thrombosis Atherosclerosis Research Institute, Hamilton, ON, Canada.
Abstract
背景および目的:継続的な抗凝固療法の適応患者がワルファリン投与に伴い頭蓋内出血を発症した場合の,出血後の抗凝固療法再開の最適時期は明確ではない。より正確なリスク推定値を得るために,大規模な後ろ向きコホート研究を実施した。方法:3 つの三次医療施設において,6年間に頭蓋内出血が客観的に確認された 2,869 例の病歴を連続的に検討した。ワルファリンを再開した場合と再開しなかった場合の1日あたりの頭蓋内出血または虚血性脳卒中のリスクを算出した。本研究では,最初の頭蓋内出血から 1週間以上生存し,心疾患により抗凝固療法が適応であるか,または脳卒中の既往のある患者に焦点をあてた。Coxモデルを用い,抗凝固療法再開(または非再開)後の各時点における頭蓋内出血と虚血性脳卒中の発現率を推定した。ある一定のワ
ルファリン再開時期範囲における新たな頭蓋内出血または虚血性脳卒中の複合リスクを算出した。結果:ワルファリンに伴う頭蓋内出血が 234 例(8.2%)に認められ,このうち 1週間以上生存した 177 例(76%)注)
から追跡調査データが得られた。追跡調査期間の中央値は69週であった[四分位範囲(IQR):19~ 144]。59例が 5.6週(中央値,IQR:2.6 ~ 17)後にワルファリンを再開した。ワルファリン再開による頭蓋内出血再発のハザード比は5.6(95% CI:1.8 ~ 17.2),虚血性脳卒中のハザード比は0.11(95% CI:0.014 ~ 0.89)であった。頭蓋内出血再発または虚血性脳卒中の複合リスクが最も低かったのは,約10 ~ 30 週後にワルファリンを再開した場合であった。結論:ワルファリン治療再開の最適時期は,ワルファリン投与に伴う頭蓋内出血から10~30週後であると思われる。
Stroke 2010; 41: 2860-2866
図1 ワルファリンを再開しなかった場合(A)とワルファリン再開後(B)の頭蓋内出血(ICH)再発および虚血性イベント(IE)の累積リスク。
ICH
IE
累積リスク(%)
A
ICH 確認後の経過時間(週)0 50 100 150
30
25
20
15
10
5
0
リスク患者 ICH 177 56 35 16
IE 177 54 34 15
IE
ICH
累積リスク(%)
B 30
25
20
15
10
5
00 50 100 150
ワルファリン再開後の経過時間(週)
リスク患者 ICH 59 42 29 22
IE 59 47 32 24
ICH
ICHIE
IE
注: 177 例の内訳は脳内出血 83例,硬膜下血腫 76例,くも膜下出血 18例であり,全体の 44例で転倒または中等度の外傷が誘因とされた(詳細は英文誌表 1を参照)。
������� �� � � ��� �������� ��