opioid analgesics
TRANSCRIPT
Opioid Analgesics Sameen Rashid M.Phil. Pharmacology

Analgesics
Analgesics, or pain killers, that bind to opioid receptors which are found principally in the:CNSGastrointestinal tract
Classification:Natural opiatesSemi-synthetic OpiatesFully synthetic opioidsEndogenous opioid peptides

• Actions•
Full agonists - Morphine• partial agonists - Codeine• Antagonists - Nalbuphine

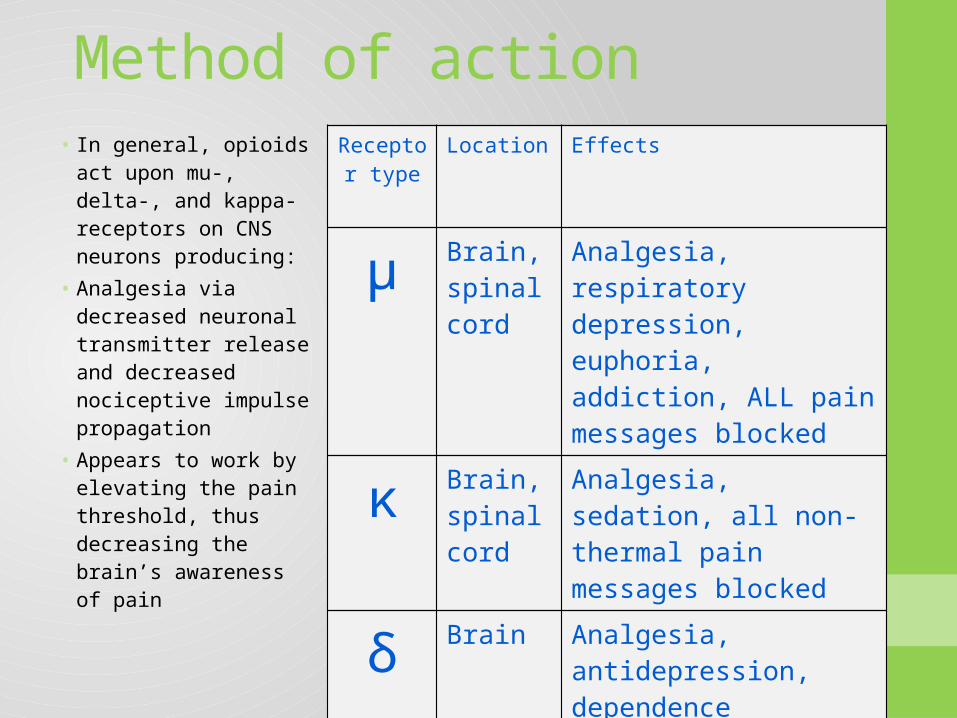
Method of actionReceptor
typeLocation Effects
μ Brain, spinal cord
Analgesia, respiratory depression, euphoria, addiction, ALL pain messages blocked
κ Brain, spinal cord
Analgesia, sedation, all non-thermal pain messages blocked
δ Brain Analgesia, antidepression, dependence
• In general, opioids act upon mu-, delta-, and kappa-receptors on CNS neurons producing:
• Analgesia via decreased neuronal transmitter release and decreased nociceptive impulse propagation
• Appears to work by elevating the pain threshold, thus decreasing the brain’s awareness of pain

Pharmacokinetics

Absorption
• Most opioid analgesics are well absorbed when given by subcutaneous, intramuscular, and oral routes
• Other routes of opioid administration include oral mucosa via lozenges, and transdermal via transdermal patches.
• Recently an iontophoretic transdermal system has been introduced, allowing needle-free delivery of fentanyl for patient-controlled analgesia.

Distribution
• All opioids bind to plasma proteins with varying affinity.
• the drugs rapidly leave the blood compartment and localize in highest concentrations in tissues.
• Drug concentrations in skeletal muscle may be much lower, but this tissue serves as the main reservoir because of its greater bulk.

Metabolism • The opioids are converted in large part to polar
metabolites.• Morphine is metabolized to M3G and M6G.• M3G, a compound with neuroexcitatory
properties and M6G, an active metabolite with analgesic property.
• Esters (e.g, heroin, remifentanil) are rapidly hydrolyzed by common tissue esterases.
• Heroin (diacetylmorphine) is hydrolyzed to monoacetylmorphine and finally to morphine, which is then conjugated with glucuronic acid.

Excretion
• Polar metabolites, including glucuronide conjugates of opioid analgesics, are excreted mainly in the urine.
• Small amounts of unchanged drug may also be found in the urine.
• Glucuronide conjugates are found in the bile.• Enterohepatic circulation represents only a small
portion of the excretory process.
Pharmacodynamics

Mechanism of Action
• Opioid drug bind to opioid receptor widely distributed in CNS and other tissues.
• A part of family of G- protein complex receptors.• Open K+ Channels.• Prevent opening of Ca2+ channels.• Inhibit the release of other neurotransmitters.






Properties of Morphine
• Good for treating dull, constant pain rather than sharp, periodic pain
• Unfortunately, it also has a large number of side effects including:
• Depression of the respiratory centre• Constipation• Excitation• Euphoria• Nausea• Pupil constriction• Tolerance and dependence

Clinical Uses
• Analgesia • Acute Pulmonary Edema • Cough Suppression • Diarrhea • Severe cute shooting visceral pain.• MI.• Shivering • Terminal stages of malignancy.• Severe crush injuries.• Postoperative pain.• Applications in Anesthesia

Side effects• Tolerance• Dependence• Addiction• Death• Confusion• Constipation• Dizziness• Respiratory depression• Hallucination• Hypotension• Itching• Nausea• Sedation• Rash

Withdrawal symptoms • Anorexia• Weight loss• Pupil dilation• Chills• Excessive sweating• Abdominal cramps• Muscle spasms• Hyperirritability• Lacrimation• Tremor• Increased heart rate• Increased blood pressure
Overdose
• A study was done in W. Virginia to evaluate persons dying of unintentional pharmaceutical overdose, the types of drugs involved and role of drug abuse in the deaths.
• Opioid analgesics were taken by 93.2% (275/295) of all people who died of pharmaceutical overdoses in W. Virginia in 2006.
• Only 44.4% (122/275) of those people had ever been prescribed these drugs.
• The majority of overdose deaths in West Virginia in 2006 were associated with nonmedical use and diversion of pharmaceuticals, primarily opioid analgesics.

Treatment of Opioid Overdosage
• Intravenous injection of naloxone dramatically reverses coma due to opioid overdose but not that due to other CNS depressants. Use of the antagonist should not, of course, delay the institution of other therapeutic measures, especially respiratory support.
Treatment for addiction
• Several treatments and treatment strategies exist for opioid addiction. They are
• The Cold Turkey Approach• Traditional Opioid Drug Treatment• Rapid Detoxification

The Cold Turkey Method• About eight to twelve hours after the last heroin use, an
addict's eyes begin to tear and he/she starts to experience flu-like symptoms: sneezing, weakness, depression, muscle cramps, nausea, vomiting, diarrhea. The symptoms increase in severity over two to three days.
• Within a week to 10 days the illness is over. • The phrase 'cold turkey' probably comes from the appearance
of goose bumps all over the body, which resembles a plucked turkey. Muscle spasms in the legs produce kicking movements, and this may be the derivation of the expression 'kick the habit.'

The Cold Turkey Method- Withdrawal Symptoms

Traditional Drug Based Treatments- Methadone
• Methadone has traditionally been provided to the addiction population
• Numerous clinics start addicts at 30mg and raise the dosage 10mg a day until the addict feels they are at a comfortable level of dosage.
• At proper dosing, methadone usually reduces the appetite for and need to take heroin.
• Many factors determine the treatment dose schedule, and some follow the philosophy that methadone maintenance treatment is not curative for heroin addiction

Rapid Detoxification• The process involves intubation and external ventilation of the
patient coupled with the administration of opioid receptor antagonists (blockers) while the patient is under general anesthesia.
• The most often used drugs are Naloxone and Naltrexone.• Naloxone is a powerful Mu opioid receptor antagonist that is
capable of rapidly displacing other opioids from the opioid receptors.
• As a result, massive withdrawal symptoms are triggered but are attenuated by the fact that the patient is under anesthesia.

Patient undergoing Rapid Detox

OPIOID ANTAGONISTS
• The pure opioid antagonist drugs are• Naloxone • Naltrexone • Nalmefene

Clinical Use
• Treatment of acute opioid overdose.• Treatment of opioid addiction.• Analgesic.• Used to reverse the effects of narcotic drugs
used during surgery or to treat pain.

Brands available
Generic Name Brand Namebuprenorphine Buprenexbutorphanol Stadolcodeine Tylenol with codeinefentanyl Duragesichydrocodone Vicodinhydromorphine Dilaudidmethadone Dolophinemorphine Astramorphoxycodone OxyContinporpoxyphene Darvon