on corneal thickness and intraocular pressure : a clinical study on the thickness of the cornea in...
TRANSCRIPT

ACTA OPHTHALMOLOGICA VOL. 4 5 1967
The Department of Ophthalmology, Rigshospitalet, University of Copenhagen, Copenhagen, Denmark
ON CORNEAL THICKNESS AND INTRAOCULAR PRESSURE
A clinical study on the thickness of the cornea in eyes with retinal detachment")
BY
N . Ehlers and D . Riise
In vitro, the intraocular pressure (IOP) exerts a reducing effect on the swelling of the cornea (Ehlers 1967) and, accordingly, it would be expected that the thickness of the cornea in man was influenced by the intraocular pressure. In vitro, the hydration of the monkey cornea was reduced considerably even at low IOP, whereas an increase in pressure to values above normal IOP produced a further slight reduction only in the hydration (Ehlers 1966). Therefore, any influence on the corneal thickness in man, exerted by the IOP, would be ex- pected in particular in the form of increased thickness at a low IOP. In the case of retinal detachment, reduced IOP is often found, in particular if the detach- ment has been present for some period of time (Linne'i 1966). In such eyes Schepens (1965) described the finding of marked swelling of the sclera. In these patients, the opposite, non-affected eyes would serve as an ideal control material. Furthermore, by examining cases of detachment without reduction in IOP, it would be possible to determine whether a change in thickness is caused by a change in the IOP and not by other unknown factors related to the detach- ment.
The literature contains only few reports on the correlation between corneal thickness and IOP, and these have resulted in contradictory conclusions (Sbordone 1953, Ytteborg & Dohlman 1965).
I t is not the purpose of the present study to decide upon the absolute thick- ness of the cornea, which has been~ determined by uon Bahr (1948, 1956) and Maurice & Giardini (1951).
") Received April 26th 1967.
809

METHODS
Patient niutcrinl. All patients included in this study suffered from unilateral retinal detachment. Both eyes were examined and, if signs of corneal disease were present, the case was discarded. Cases piesenting slight anterior chamber reaction in the af- fected eye were accepted, since this occurred both with and without reduction in IOP. Furthermore a few cases had to be excluded because the vision of the affected eye was so reduced that the patient could not fix the slit lamp during the thickness measure- ment. Measuring techriiqzce. The corneal thickness was measured in accordance with the method of jaeger (1953), using the attachment I to the Haag-Streit slit-lamp model 900. The IOP was measured with the Goldmann applanation tonometer, attached to the Haag-Streit slit-lamp model 900.
The corneal thickness was measured five times in each eye and the result was given as the arithmetic mean. The IOP was not determined until these measurements had been made, so that, when the thickness was measured, the observer did not know whether the two eyes presented any difference in pressure (see later). At least two readings of the pressure were made in each eye, and in most cases the pressure was determined several times during the days before and after the measurement of the thickness.
The centering on the cornea is of the utmost importance for the thickness measure- ments. With the instrument applied this is usually ensured by making the patient look directly on the light in the slit-lamp and by projecting the light directly on to the centre of the pupil. Therefore, as far as possible the measurements were made with a non-dilated pupil. The angle kappa was not measured, but in none of the patients was strabismus noted. Statisticnl calculations. When differences between the two eyes are studied, it is im- portant to take into consideration that the data obtained are not independent. The values recorded in the two eyes of a person are inherently paired. In order to make a significance test, it must, therefore. be ascertained whether the mean of the diffe- rences between the paired values differs significantly from zero. In the present cal- culations, the t-distribution was used to test the significance of the differences. The following formula was used (Croxton 1953):
- X,) - 0
t = (\'D)i
- N?:-'l) Nr (N-1)
where D is the difference between two paired values, XI, the arithmetic mean of the differences and N the number of differences.
RESULTS
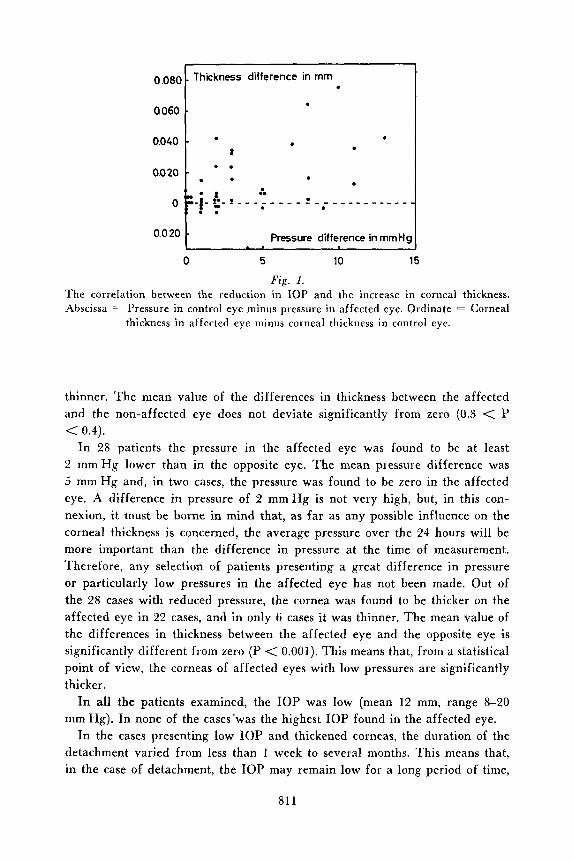
The results of measurements in 45 patients suffering from retinal detachment are plotted in Fig. 1 .
In 1 7 patients the difference in IOP between the two eyes was less than 2 mm Hg. In 4 cases identical corneal thicknesses were measured in the two eyes, in 7 cases the cornea was thicker in the affected eye, and in 6 cases it was
810
0.08C
a060
0.040
0.0 20
0
0.0 20
Thickness difference in rnm
.
Pressure difference in rnrnH!
0 5 10 15
Fig. 1. The correlation between the reduction in IOP and the increase in corneal thickness. Abscissa = Pressure in control eye minus pressure in affected eye. Ordinate = Corneal
thickness in affected eye minus corneal thickness in control eye.
thinner. The mean value of the differences in thickness between the affected and the non-affected eye does not deviate significantly from zero (0.3 < P < 0.4).
I n 28 patients the pressure in the affected eye was found to be at least 2 m m H g lower than in the opposite eye. The mean pressure difference was 5 mm Hg and, in two cases, the pressure was found to be zero in the affected eye. A difference in pressure of 2 m m H g is not very high, but, in this con- nexion, it must be borne in mind that, as far as any possible influence on the corneal thickness is concerned, the average pressure over the 24 hours will be more important than the difference in pressure at the time of measurement. Therefore, any selection of patients presenting a great difference in pressure or particularly low pressures in the affected eye has not been made. Out of the 28 cases with reduced pressure, the cornea was found to be thicker on the affected eye in 22 cases, and in only 6 cases it was thinner. The mean value of the differences in thickness between the affected eye and the opposite eye is significantly different from zero (P < 0.001). This means that, from a statistical point of view, the corneas of affected eyes with low pressures are significantly thicker.
In all the patients examined, the IOP was low (mean 12 mm, range 8-20 mm Hg). I n none of the cases’was the highest IOP found in the affected eye.
In the cases presenting low IOP and thickened corneas, the duration of the detachment varied from less than 1 week to several months. This means that, in the case of detachment, the IOP may remain low for a long period of time,
811
and that as regards the thickness of the cornea no compensatory mechanisms seem to be active.
With respect to an elucidation of the influence of the IOP on the corneal thickness, examination of patients representing extremely low IOP before operation and normalized IOP after operation appears immediately to be ideal. In compliance with clinical experience that, from a prognostic viewpoint, the finding of a low IOP is unfavourable, no such cases were found. A case in which identical IOP and corneal thickness in the two eyes were found imme- diately after the development of retinal detachment, appears informative. After a few days, the pressure in the affected eye decreased and then the cornea was found to be thicker in this eye.
DISCUSSION
As stated above, it was not the purpose of the present study to determine the absolute thickness of the cornea, but only differences in thickness between the two eyes. When only differences are used in the statistical calculations, the influence of individual variations is reduced.
The relationship between IOP and corneal thickness in acute and chronic glaucoma was studied by Sbordone (1953). In two cases of acute glaucoma, the corneal thickness was increased considerably. In 12 cases of long-lasting pres- sure difference (chronic glaucoma), the cornea of the eye with the higher pres- sure was thinner in 9 cases and thicker in 3 cases. On an average, the cornea was thinner in the eye with the higher pressure.
Ytteborg & Dohlman (1965) noted no significant difference in corneal thick- ness among patients having an IOP below 40 mmHg. In a group having IQP higher than 40 mm Hg, the corneal thickness was significantly increased.
Among 8 patients with unilateral retinal detachment and lowered IOP, no difference in thickness was found in 5 , whereas in 3 cases the low-pressure eye had the thicker cornea. In their sbatistical calculation, Ytteborg & Dohlman ignored correlation between the corneal thickness of the two eyes of the same person. I t was concluded that no significant difference was present between the corneal thickness in eye with low and normal IOP and a P-value of 0.05 was given. If a correlation between the right and the left eye is taken into conside- ration, a value of 0.1 < P < 0.2 is found.
As regards the effects of high IOP on corneal thickness, Ytteborg & Dohlrnan listed 17 cases, in 11 of which the cornea was thicker in the eye with higher pressure, and in 5 cases no difference was observed. If all the 1 7 patients had simple chronic glaucoma, this result is directly opposed to that found by Sbordone (1953), as mentioned above, and the solution of the problem relating to corneal thickness in eyes with raised IOP must await further studies.
It seems reasonable to conclude that an increase in the thickness of the
812

cornea will occur if the IOP is reduced. The present study reveals a statistically significant increase, and the cases reported by Ytteborg & Dohlman (1965) do not contradict this finding.
S U M M A R Y
The effect of the intraocular pressure on the corneal thickness was studied in 45 patients with unilateral retinal detachment. When no difference in intra- ocular pressure was present, no difference in thickness was observed. When the intraocular pressure was reduced, the corneal thickness was increased.
REFERENCES
von Bahr, G. (1948) Measurements of the thickness of the cornea. Acta ophthal., Kbh.
von Bahr, G. (1956) Corneal Thickness. Its measurement and changes. Amer. J. Ophthal.
Croxton, F. E. (1953) Elementary statistics with applications in medicine and the biolo-
Ehlers, N . (1966) The fibrillary texture and the hydration of the cornea. Acta ophthal.,
Ehlers, N . (1967) Mechanical factors in the maintenance of normal corneal detur-
jaeger, W. (1953) Tiefmessung der menschlichen Vorderkammer mit planparallelen
Linnkr, E. (1966) Intra-ocular pressure in retinal detachment. Acta Ophthal., Kbh.
Maurice, D. M . & Giardini, A . A . (1951) A simple optical apparatus for measuring the corneal thickness and the average thickness of the human cornea. - Brit. J. Ophthal.
Schepens, C . L. (1965) in Schepens & Regan. Controversial aspects of the management
Sbordone, G. (1953) Richerche sullo spessore della cornea in occhi glaucomatosi. - Rass.
Ytteborg, /. & Dohlman, C . H . (1965) Corneal edema and intraocular pressure. Arch.
26: 247-266.
42: 251-263.
gical sciences. Dover pulb. Inc., New York, p. 240.
Kbh. 44: 620-630.
gescence. Acta ophthal., Kbh. 45: 658-672.
Platten (Zusatzgerat zur Spaltlampe) - Graefes Arch. Ophthal. 153: 120-131.
SUPPI. 84. p. 101-106.
35: 169-177.
of retinal detachment. Little, Brown & Co, Boston. p. 74.
ital. Ottal. 22: 262-268.
Ophthal., Chicago 74: 477-484.
813 Acta Ophthalmol. 45, VI