objectives not to be a nephrologist to understand lupus nephritis as a primary care physician. not...
TRANSCRIPT

OBJECTIVES
• NOT TO BE A NEPHROLOGIST
• TO UNDERSTAND LUPUS NEPHRITIS AS A PRIMARY CARE PHYSICIAN .

OBJECTIVES
• Define nephrotic syndrome and glomerulonephritis
• Identify the Diagnostic criteria for SLE • Antibodies markers in SLE• Prognostic markers in SLE• Classification of lupus nephritis • Indications and contraindications of renal biopsy• Common side effects of medicine used in lupus
nephritis

GLOMERULAR DISEASE
NEPHRITIC
FOCAL NEPHRITIC
DIFFUSE NEPHRITIC
NEPHROTIC Heavy protienuria (>3.5gm/day)
LipiduriaEdema
Hyperlipidemia

FOCAL NEPHRITIC
• URINALYSIS Red cells ( usually
dysmorphic ) Red cell cast Mild proteinuria (<1.5gm
/day)• Findings of more severe
disease are usually absent
DIFFUSE NEPHRITIC
• URINALYSIS Similar to focal disease but
heavy proteinuria (which may be in nephrotic range)
Edema Hypertension + Renal Insufficiency


Why Dr Reed’s Top Differential was Lupus ?



Why did he order anti-dsDNA and anti-SM antibody?
What is the role of complement level in lupus nephritis?

Serologic test
• ANA's are a highly sensitive screen for SLE, being found in more than 90% of untreated patients, but they are not specific for SLE.
• anti-dsDNA are a more specific but less sensitive marker of SLE and are found in almost three fourths of untreated patients with active SLE(97% specificity).
• Titers of anti-dsDNA antibodies often fluctuate with disease activity.
• Anti-Sm antibodies, although very specific for SLE are found in only about 25% of lupus patients.

MONITORING CLINICAL DISEASE
• There is controversy regarding the value of a declining C3 and C4 level and a rising anti-DNA antibody titer in predicting a clinical flare of SLE or active renal disease.clearly these are the most widely used serologic tests to monitor SLE activity.
• Nonspecific:ESR /CRP

• SO IF A PATIENT HAS POSITIVE SEROLOGIC MARKERS FOR LUPUS WHICH CORRELATE
WITH CLINICAL FINDINGS DO THEY STILL NEED A RENAL BIOPSY ? AND WHY?

CLASSIFICATION OF LUPUS NEPHRITIS
• CLASS I (Minimal Mesangial lupus Nephritis)
• CLASS II(Mesangial Proliferative Lupus Nephritis)• CLASS III(focal lupus nephritis)• CLASS IV (diffuse Lupus Nephritis )• CLASS V (membranous lupus nephritis )• CLASSVI (Advanced sclerosing lupus nephritis)
International Society of Nephrology/Renal Pathology Society (2003) Classification of Lupus Nephritis
• Class I Minimal mesangial LN
• Class II Mesangial proliferative LN
• Class III Focal LN* (<50% of glomeruli) • III (A): Active lesions
III (A/C): Active and chronic lesions III (C): Chronic lesions
• Class IV Diffuse LN* (≥50% of glomeruli) Diffuse segmental (IV-S) or global (IV-γ) LN IV (A): Active lesions IV (A/C): Active and chronic lesions IV (C): Chronic lesions
• Class V[†] Membranous LN• Class VI Advanced sclerosing LN (≥90% globally sclerosed glomeruli without
residual activity) .
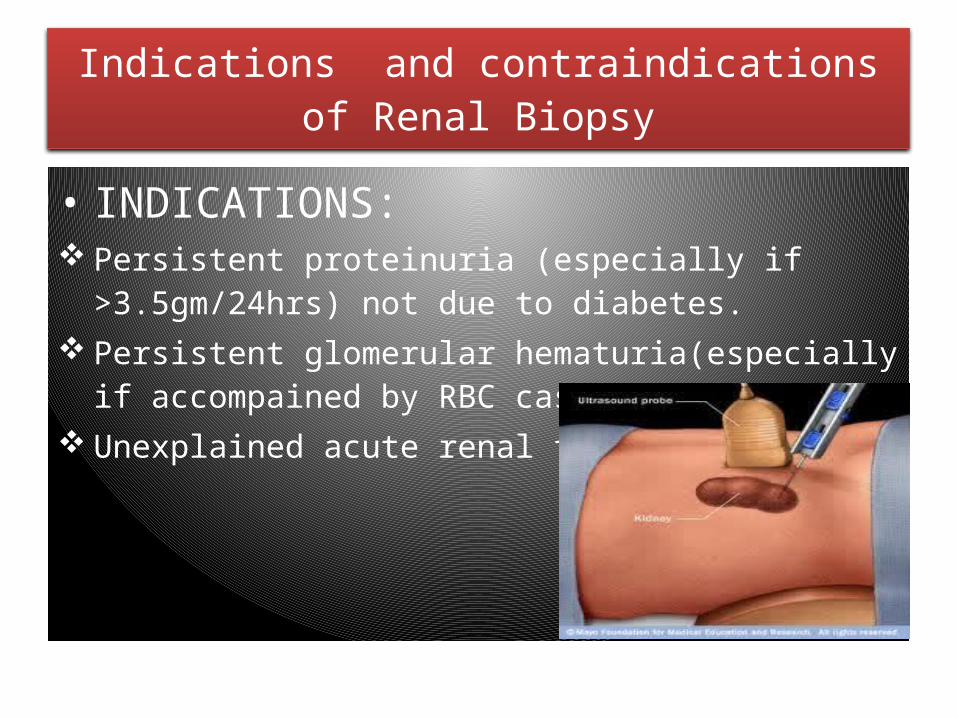
Indications and contraindications of Renal Biopsy
• INDICATIONS: Persistent proteinuria (especially if >3.5gm/24hrs) not due to
diabetes. Persistent glomerular hematuria(especially if accompained by
RBC cast) Unexplained acute renal failure

RENAL BIOPSY
• CONTRAINDICATIONS: Coagulation Disorders Thrombocytopenia Uremic Platelet Dysfunction(relative contraindication) Uncontrolled hypertension(relative risk, maintain B.P<140/90) Solitary Kidney (open biopsy is procedure of choice) Advanced age and Pregnancy are NOT a contraindication

RENAL BIOPSY
• COMPLICATIONS:Intrarenal Renal and perinephric
Hematomas(60-80%)Bleeding causing hypotension(1-2%),requiring
transfusion (6%)AV fistula (4-18%)Perirenal Soft Tissue Infection(0.2%).

Treatment of Lupus Nephritis
• IMMUNOSUPPRESIVE THERAPY:
Cyclophosphamide
PREDNISONE
Mycophenolate mofetil (MMF)
Other Drugs Azathioprine Cyclosporine Rituximab

Side effects of medication .
• Cyclophosphamide: Pancytopenia (to check cbc every two weeks) Predispose to infection by bonemarrow depression Premature amenorrhea,Permanent infertility Increases the risk of malignancy Bladder toxicity Hyponatremia due to SIADH

• Mycophenolate mofetil (MMF)It is substantially more expensive then other
drugsCytopenias: cbc first 2 weeks then every 6
weeksAssociation with developing CNS lymphoma.Antacids and Iron Supplements decrease
absorption of MMF

• AZATHIOPRINE :• Bone Marrow Suppression • Infection• Malignancy

