pathophysiology of lupus nephritis
TRANSCRIPT
Systemic lupus erythematosus
Dr. Mohit Mathur
14/10/14

Introduction
The term “lupus erythematosus” was introduced by 19th-century physicians to describe skin lesions, it took almost 100 years to realize that the disease is systemic and spares no organ and that it is caused by an aberrant autoimmune response.
In 1941, Klemperer, Pollack and Baehr first described systemic lupus erythematosus (SLE) as one of the CTD
Definition
Systemic lupus erythematosus (SLE) is an autoimmune disease in which organs and cells undergo damage mediated by tissue-binding autoantibodies and immune complexes
The prevalence ranges from 20 to 150 cases per 100,000 population, with the highest prevalence reported in Brazil.
Prevalance appears to be increasing as the disease is recognized more readily and survival is increasing.
The onset of disease peaks between 15 and 45 years of age, and more than 85% of patients are younger than 55 years of age.
The 10-year survival rate is about 70%.
Females outnumber males by about 10 to 1 Males with SLE have the same incidence of
renal disease as females.
SLE is more likely to be associated with severe nephritis in children and in males and is less likely in elderly individuals
Females outnumber males by about 10 to 1 Males with SLE have the same incidence of
renal disease as females.
SLE is more likely to be associated with severe nephritis in children and in males and is less likely in elderly individuals

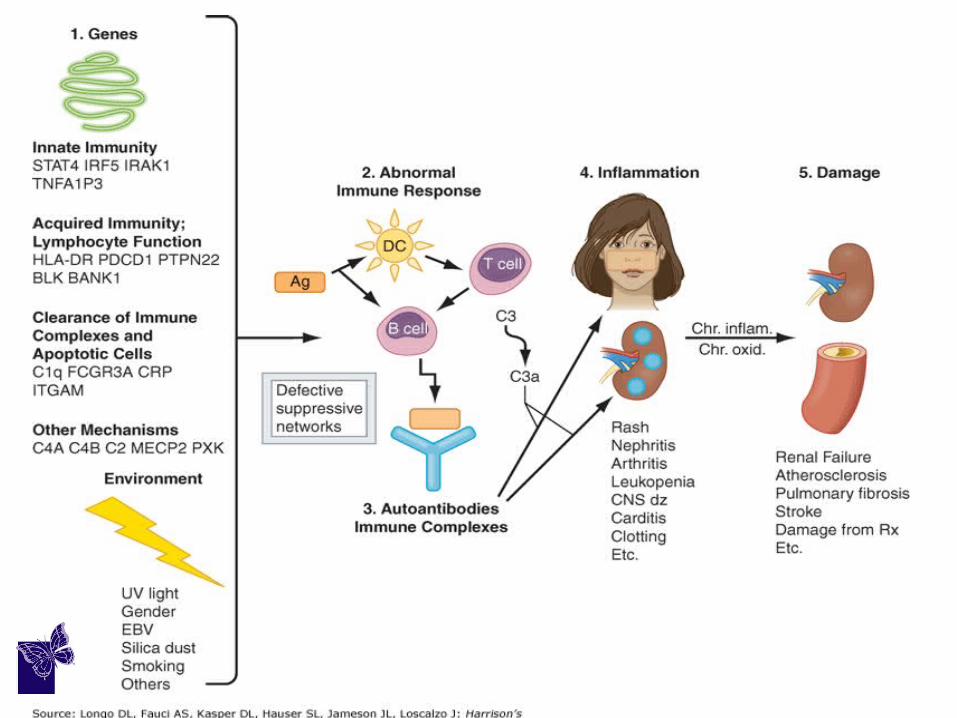
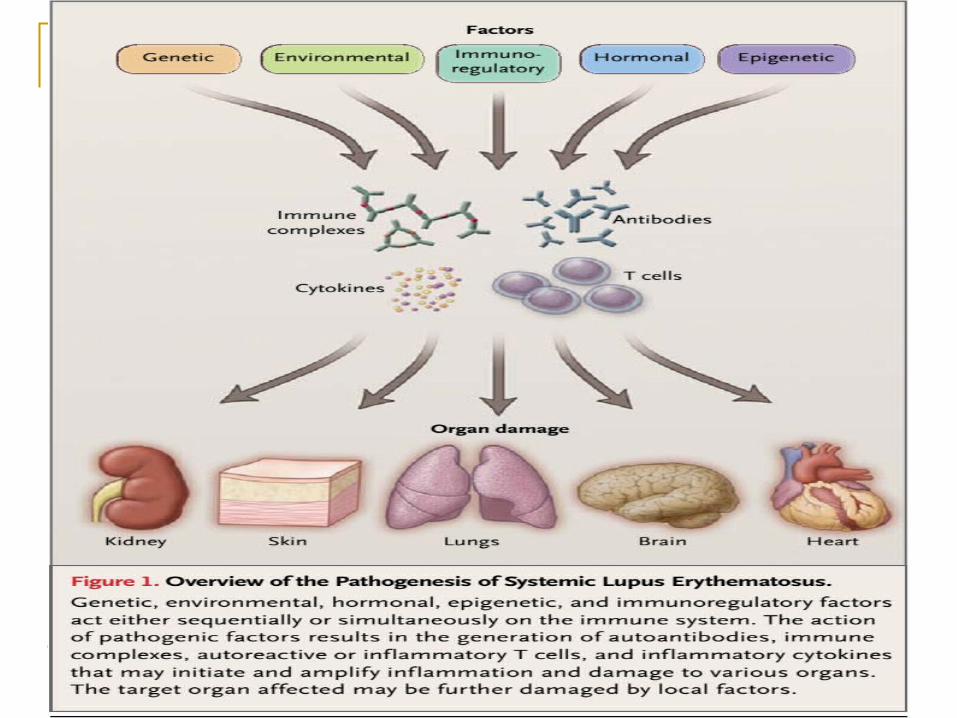
Pathogenesis and Etiology There are multiple susceptibility factors,
which result in abnormal immune responses, which vary among different patients.
These factors include: Genetic factors Environmental factors
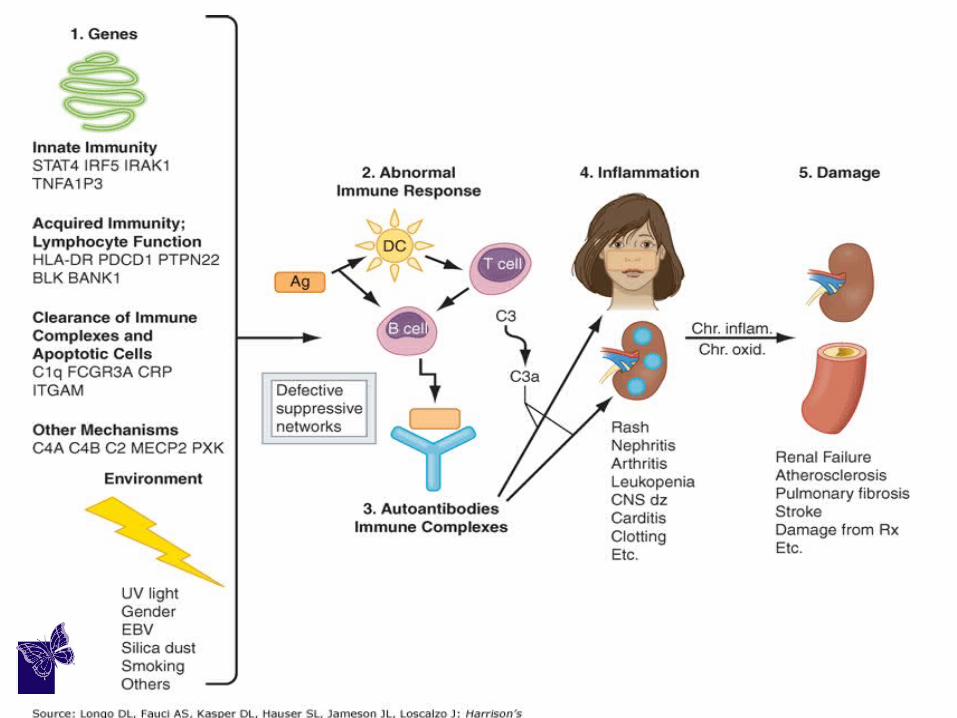
Abnormal immune responses Those responses may include:
(1) Activation of innate immunity
(dendritic cells,monocyte/macrophages) by CpG DNA, DNA in immune complexes, viral RNA, and RNA in RNA/protein self-antigens;
(2) Abnormal activation pathways in adaptive immunity cells (T and B lymphocytes);
(3) Ineffective regulatory CD4+ and CD8+ T cells;
(4) Reduced clearance of immune complexes and of apoptotic cells.
Pathogenesis Self-antigens (nucleosomal DNA/protein;
RNA/protein in Sm, Ro, and La; phospholipids) are available for recognition by the immune system in surface blebs of apoptotic cells;

…pathogenesis
Immune cell activation is accompanied by increased secretion of multiple cytokines and inflammatory mediators like:
a) Type 1 and 2 interferons (IFNs), b) Tumor necrosis factor c) Interleukin (IL)-17 and IL-10. d) B cell–maturation/survival cytokines B lymphocyte stimulator
(BLyS/BAFF)Note: These cytokines produce fever, malaise, myalgia, weight loss etc
(Similar to viral infections) Decreased production of other cytokines also contributes
to SLE: Lupus T and natural killer (NK) cells fail to produce enough IL-2
and transforming growth factor to induce and sustain regulatory CD4+ and CD8+ T cells.
…pathogenesis
The result of these abnormalities is sustained production of autoantibodies and immune complexes;
…pathogenesis
Due to the defects listed above antigens, autoantibodies, and immune complexes persist for prolonged periods of time, allowing inflammation and disease to develop.
Pathogenic antibodies/immunecomplex bind target tissues, with activation of complement, leading to release of cytokines, chemokines, vasoactive peptides, oxidants, and destructive enzymes.
This is accompanied by influx into target tissues of T cells, monocyte/macrophages, and dendritic cells, activation of resident macrophages and dendritic cells.
In the setting of chronic inflammation, accumulation of growth factors and products of chronic oxidation contribute to irreversible tissue damage, including fibrosis/sclerosis, in glomeruli, arteries, brain, lungs, and other tissues.
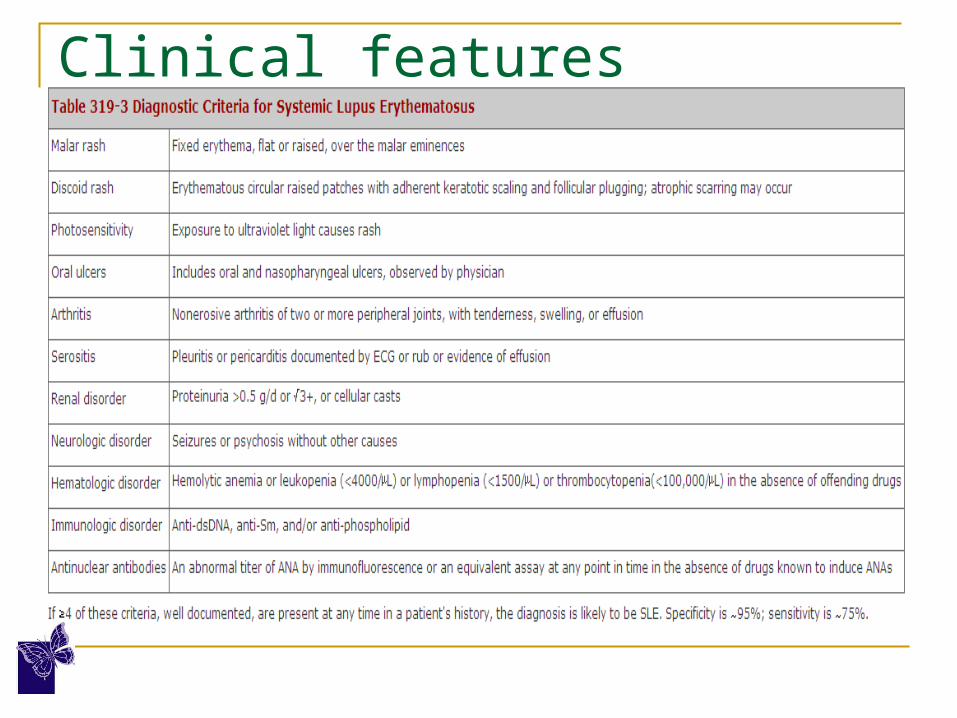
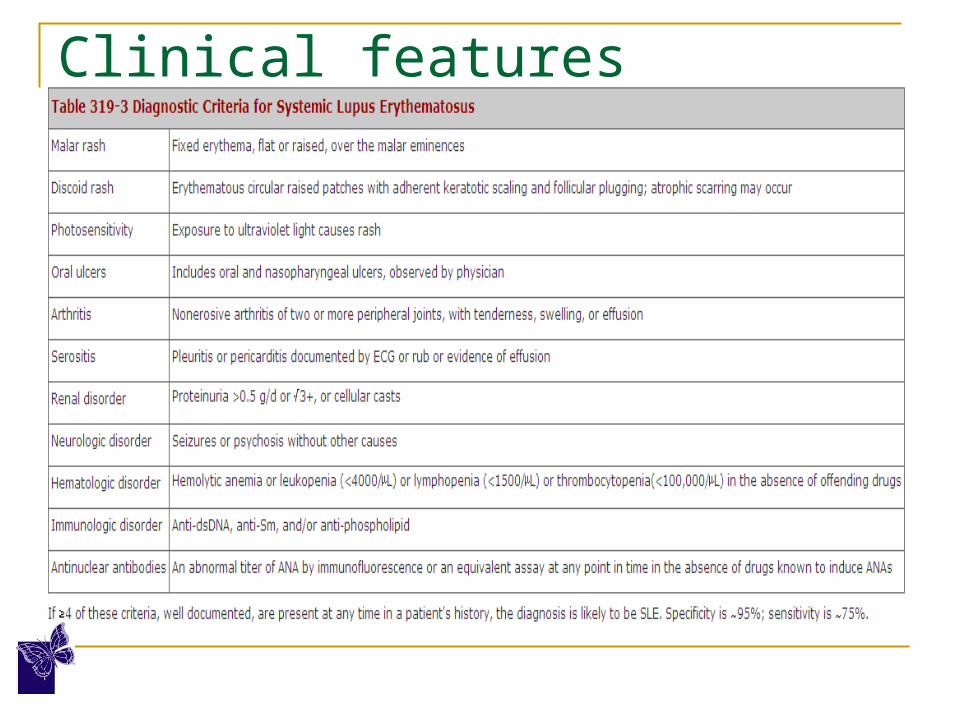
Clinical features
The clinical heterogeneity of the disease led to the establishment of 11 criteria with 4 needed for the formal diagnosis of systemic lupus erythematosus (SLE).
Clinical features

As early as the 13th century, medical writings by Rogerius (c. 1230) and Paracelsus (c. 1500) proposed the Latin term lupus, meaning wolf, to describe the erythematous ulcerative lesions affecting the skin of the cheeks
Clinical features


Diagnosis Autoantibody testing
In 1948 Malcom Hargrave, Helen Richmond and the medical resident Robert Morton noted the presence of previously unknown cells in the bone marrow of a patient with SLE.
They called these LE cells and described them as mature polymorphonuclear leukocytes which had phagocytosed the liberated nuclear material of another leukocyte
This extremely important discovery laid the foundation of research for ANA.
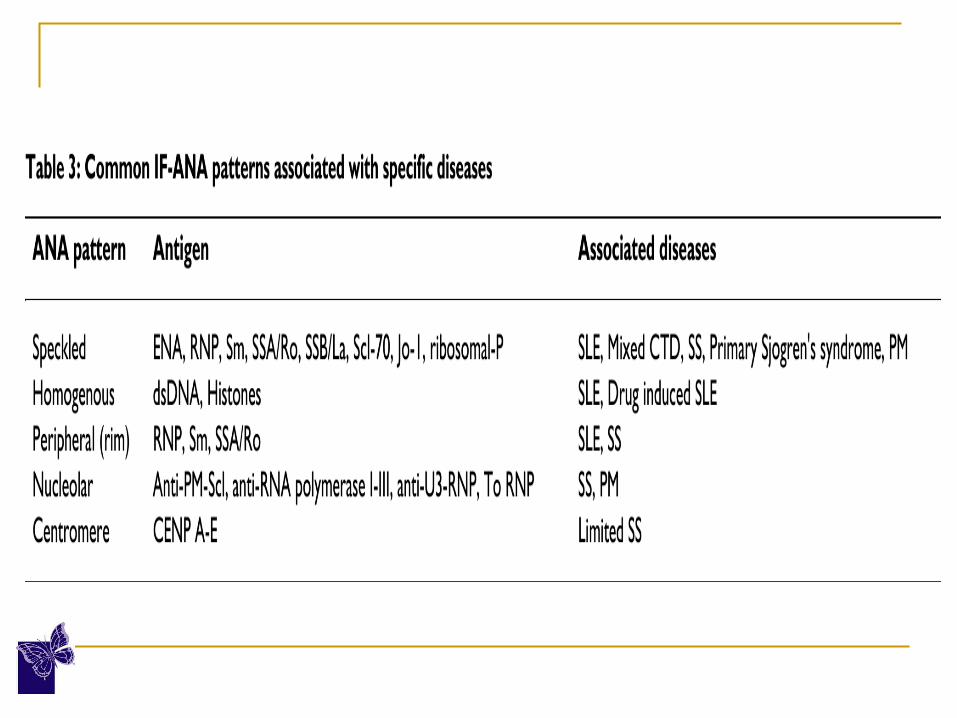
Presently the ANA have been categorized in to 2 main groups:
Autoantibodies to DNA and histones
These include antibodies against single/doublestranded DNA (dsDNA) and histones
Autoantibodies to extractable nuclear antigens (ENA).
i. These nuclear antigens were named ENA as they are extracted from the nuclei with saline.
ii. Autoantibody to Smith antigen (Sm), ribonucleoproteins (RNP), SSA/Ro, or SSB/La, Scl-70, Jo-1 and PM1.
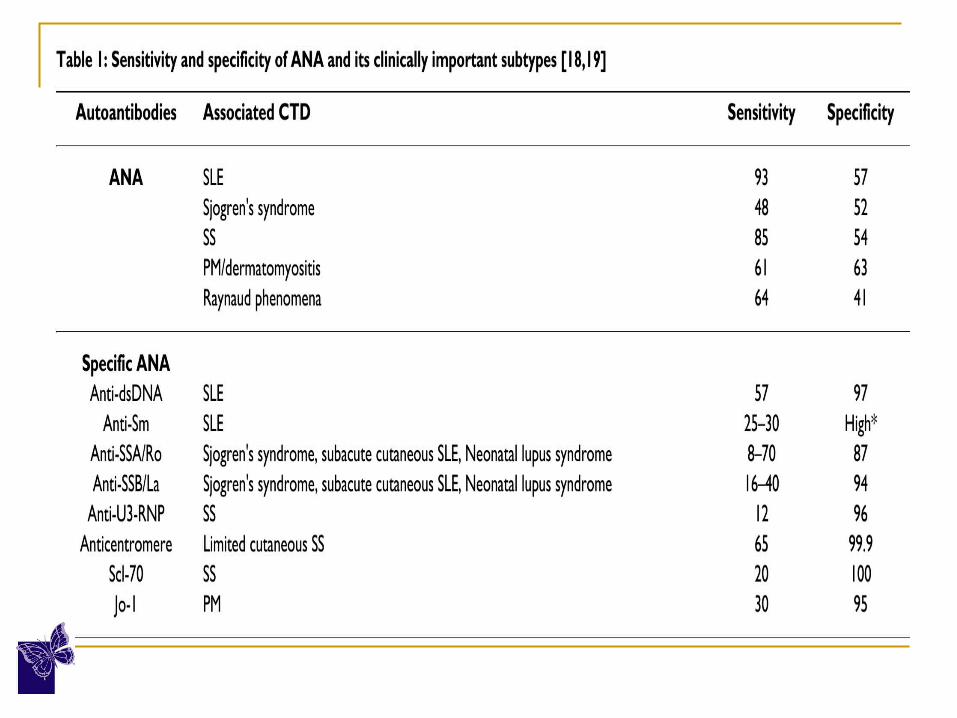
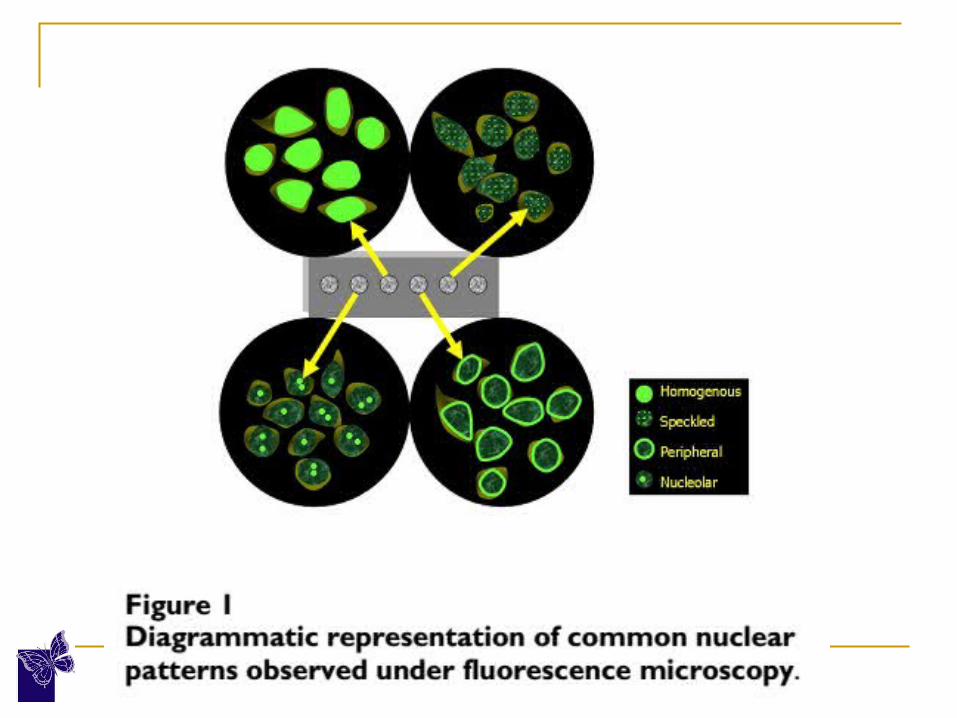
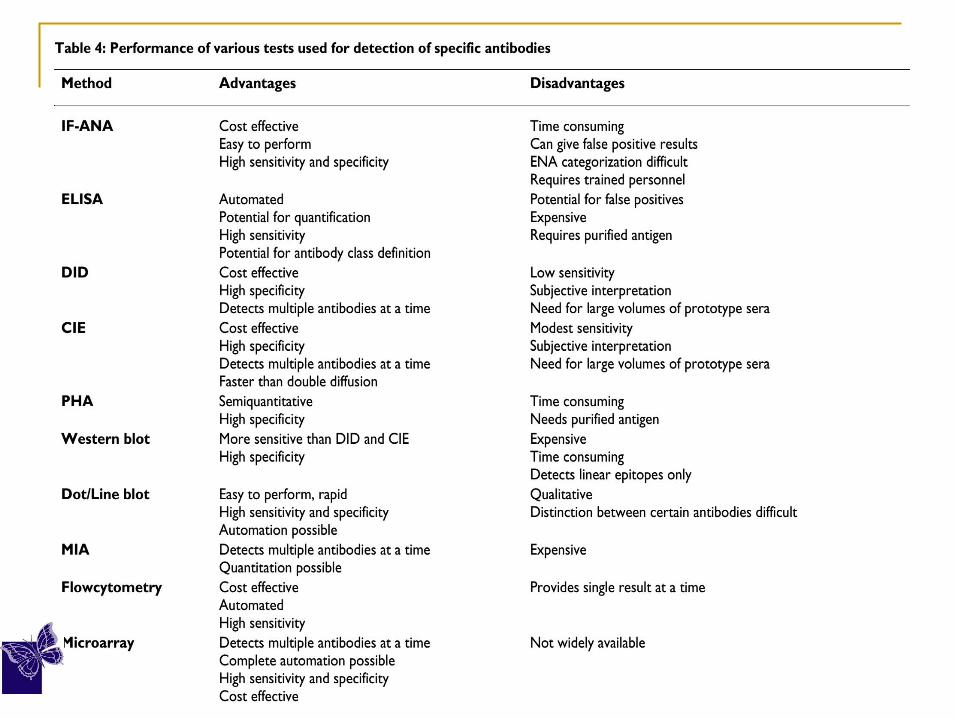
ANA – the two broad subtypes


Techniques for ANA detection Indirect immunofluorescence antinuclear
antibody test (IF-ANA) Enzyme immunoassay (EIA)/enzyme linked
immunosorbent assay (ELISA)
IF-ANA: The standard ANA testing technique It is inexpensive and easy to perform, with
high sensitivity and specificity The test detects the presence of ANA in the
blood of the patient which adhere to HEp-2 cell substrate, forming distinct fluorescence patterns.
ANA titer
It is directly proportional to antibody concentration and expressed with a quantitative scale of values.
Its evaluation is crucial as low titer is less significant, and may be seen even in healthy individuals.
A titer of 1:160 is taken as significant.
ELISA
ELISA is both highly specific and sensitive and substantially decreases the time involved when screening large numbers of patient samples.
The test is simple to perform, can be automated and does not require highly trained operators who can recognize microscopic patterns.
The EIA/ELISA is therefore becoming the most widely used method not only for routine screening but also for detection of specific ANA.
Complement Levels Levels of total hemolytic complement (CH50) and
complement components are usually decreased during active SLE and especially active LN.
Levels of C4 and C3 often decline before a clinical flare of SLE.
Serial monitoring of complement levels, with a decline in levels predicting a flare, is considered more useful clinically than an isolated depressedC3 or C4 value.
Normalization of depressed serum complement levels is often associated with improved outcomes.
Pathogenesis of Lupus Nephritis
DISEASE PATHOMECHANISMS AT THE KIDNEY LEVEL
IgG, IgM, IgA deposition and complement activation via classical pathway.
(a) Glomerulus:
Mesangial compartment (glomerular inflammation, class I and II);
Sub-endothelial compartment (vascular inflammation, class III and IV);
Subepithelial compartment (podocyte injury,class V).
(b) Tub.-Int: Peritubular vascular injury.
Disease patho-mechanism at the kidney level Fc, Toll-like, and complement receptor
activation. Increased, local expression of cytokines,
chemokines and adhesion molecules.
(a) Glomerulus: Activation of glomerular parenchymal cells and infiltrating leukocytes.
(b) Tub.-Int: Activation of peritubular endothelial cells and tubular epithelial cells.
Cont…
Recruitment of leukocytes with pro-inflammatory effector functions.
(a) Glomerulus: Amplification of inflammation via release of cytokines and cytotoxic factors.
(b) Tub.-Int: Similar to glomerulus, tertiary lymphoid organ formation, specifically local immunoglobulin production.
Programmed death of renal parenchymal cells – reparative hyperproliferation.
(a) Glomerulus: Mesangio-proliferative glomerulonephritis (GN), endocapillary GN, podocyte loss, parietal cell hyperproliferation and cellular crescent formation.
(b) Tub.-Int: Tubular atrophy, loss of peritubular vasculature causing hypoxia.

Insufficient regeneration and scarring
(a) Glomerulus: Focal segmental glomerulosclerosis, fibrocellular crescents, global glomerulosclerosis, i.e. nephron loss (class VI).
(b) Tub.-Int: Tubular atrophy and nephron loss, interstitial fibrosis.
When to biopsy?
Renal biopsy is generally indicated in a patient with any combination of:
a) Acute increase in serum creatinine, b) Proteinuria >500 mg/24 h, c) Hematuria in presence of any level of
proteinuria. d) Active sediment/cellular casts e) To detect class switch/transformation in
an established case of LN

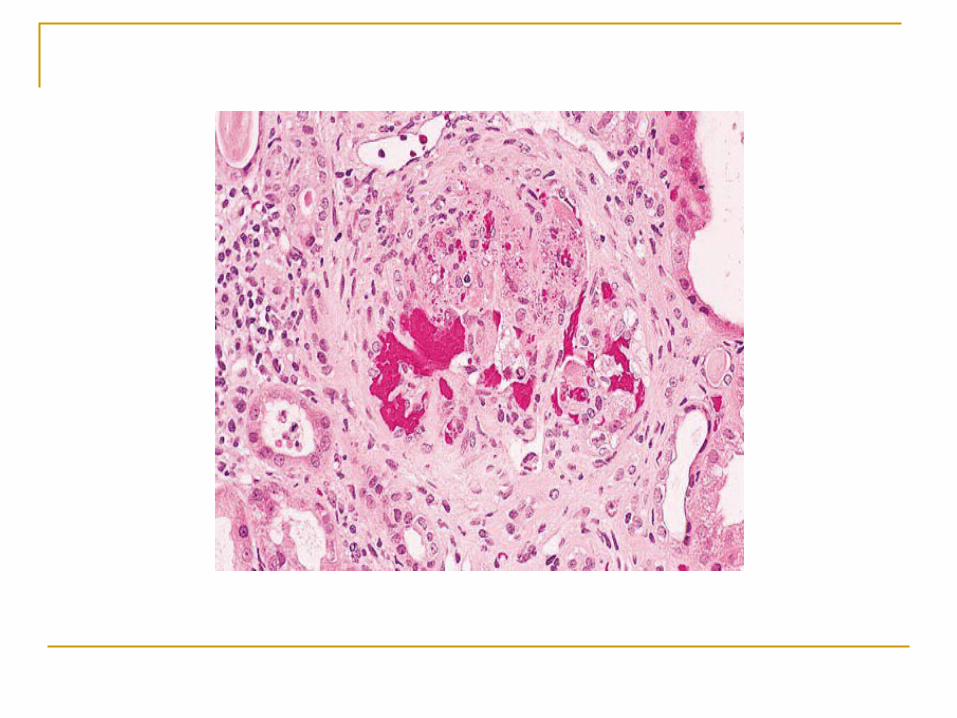
Role of renal biopsy Glomerulonephritis (GN) is the most common form
of renal disease in patients with SLE, but is frequently accompanied by tubulointerstitial and/or vascular lesions (such as thrombosis secondary to antiphospholipid syndrome).
A variety of other nephropathies have also been described like
a) Renal amyloidosis, b) Focal segmental glomerulosclerosis, c) Minimal-change disease, d) IgA and IgM nephropathy, e) Necrotizing glomerulitis, f) Sarcoidal and NSAID-induced tubulointerstitial
nephritis
Clinico-pathological correlation Several studies have focused on the
discrepancy between clinical presentation and pathologic findings at renal biopsy in patients with SLE.
Silent LN has been reported not only in class II but also in class IV.
Even patients with low-level proteinuria (<1g/24h) have demonstrated significant renal involvement with proliferative LN (classes III or IV)
Glomerular pathology Terminology
The major histologic abnormalities of the glomerulus in lupus nephritis include immune deposits, glomerular proliferation, influx of leukocytes, glomerular necrosis, and scarring.

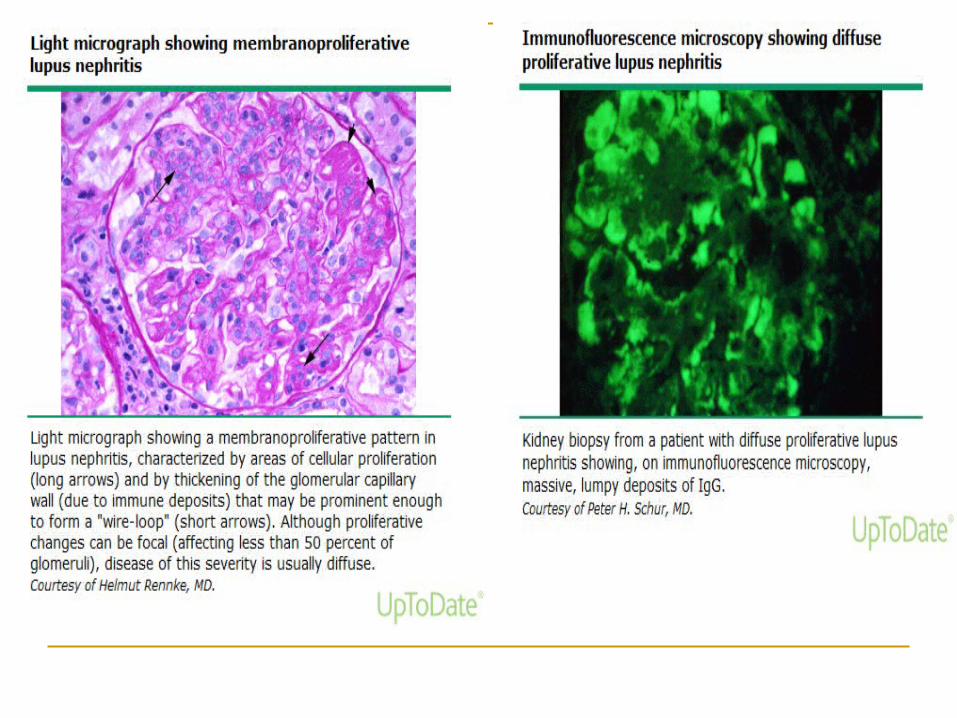
Wire loop Wire loops, a classic sign of active lupus
nephritis, are segmental areas of refractile, eosinophilic, thickening of the glomerular capillary seen by light microscopy in haematoxylin and eosin stained sections
They correspond to massive subendothelial electron-dense deposits on electron microscopy, that when large enough to completely involve the peripheral circumference of the glomerular capillary wall
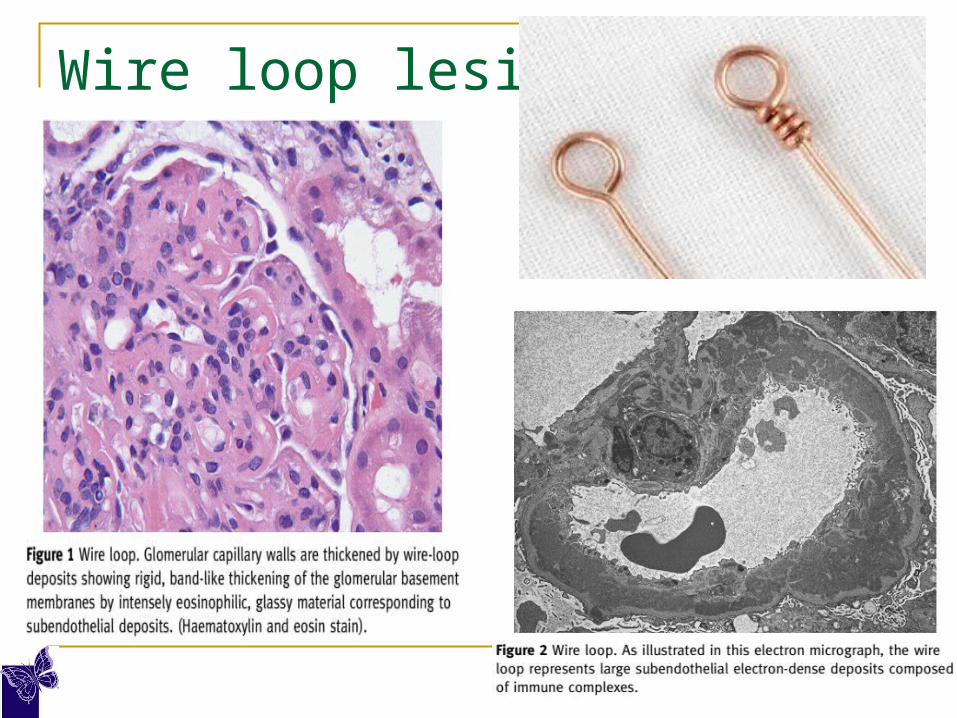
Wire loop lesions
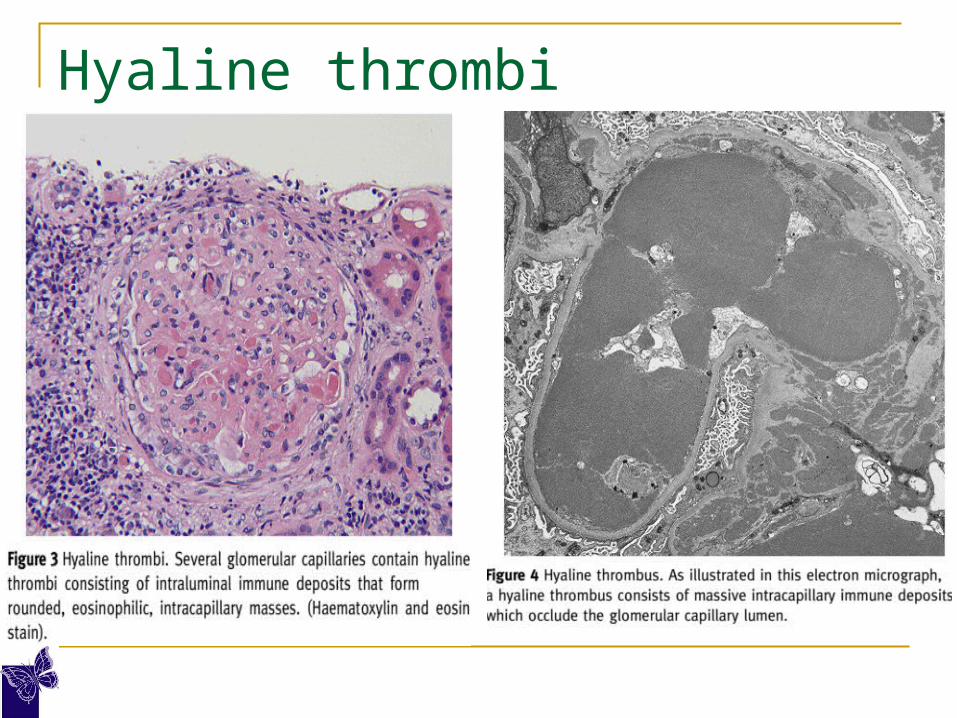
Hyaline thrombi
Hyaline thrombi are large, acellular, eosinophilic, intracapillary deposits that occlude the glomerular capillary lumens
The term is actually a misnomer because they do not represent true fibrin thrombi but are instead massive intracapillary immune deposits
Hyaline thrombi
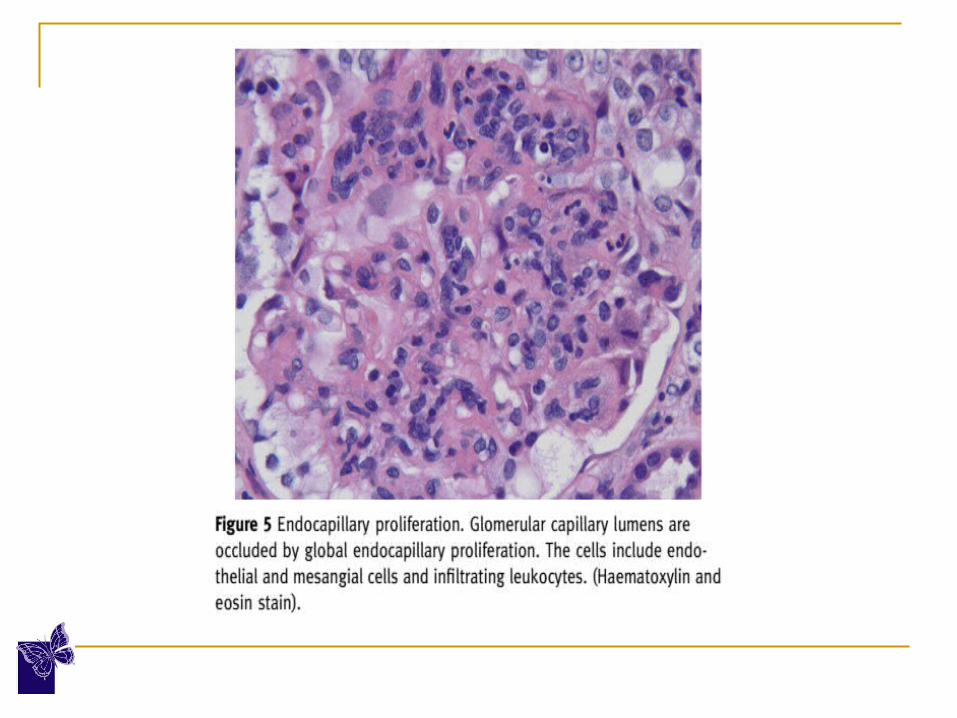
Hypercellularity
Proliferation of glomerular endothelial, mesangial, and epithelial cells and infiltration of leukocytes is the most frequent histological finding in lupus nephritis.
Mesangial hypercellularity and matrix expansion are the first observable responses to mesangial deposits.
The endocapillary hypercellularity results from the proliferation of glomerular endothelial and mesangial cells, as well as by leukocyte infiltration that occludes the glomerular capillary
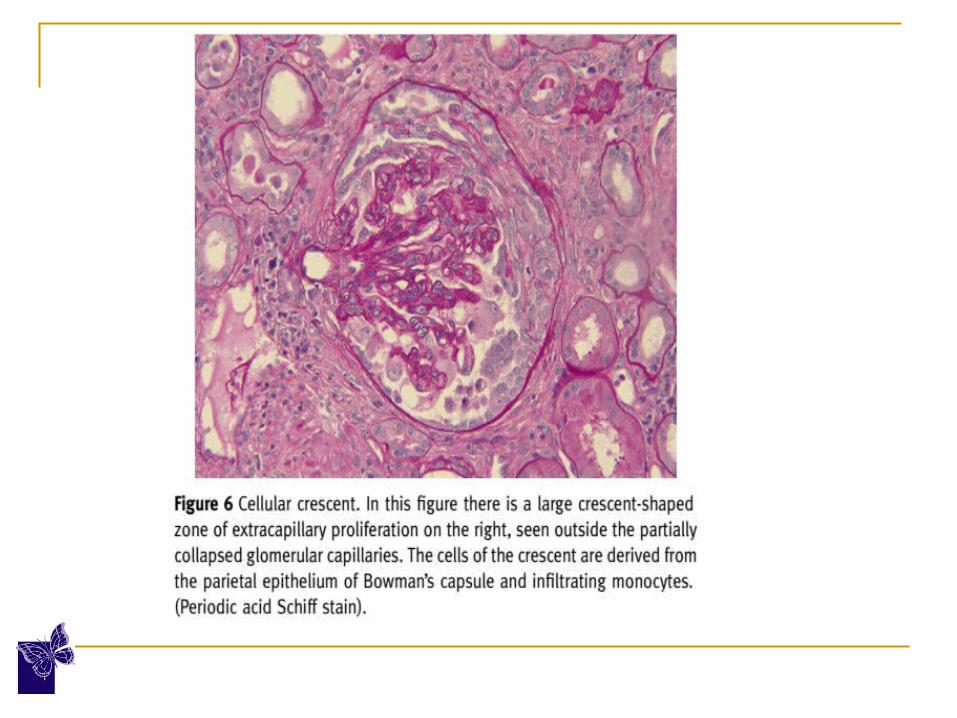
Crescents
Cellular crescents are a feature of active lupus nephritis.
Cellular crescents commonly overlie necrosis of the glomerular tuft, and are formed by proliferating parietal epithelial cells with infiltrating mononuclear cells (monocytes or macrophages).
The greater the proportion of glomerular involvement (i.e > 50%), the worse the prognosis.
With evolution of the glomerular injury, there is progressive scarring of cellular crescents, forming fibrocellular and fibrous crescents.
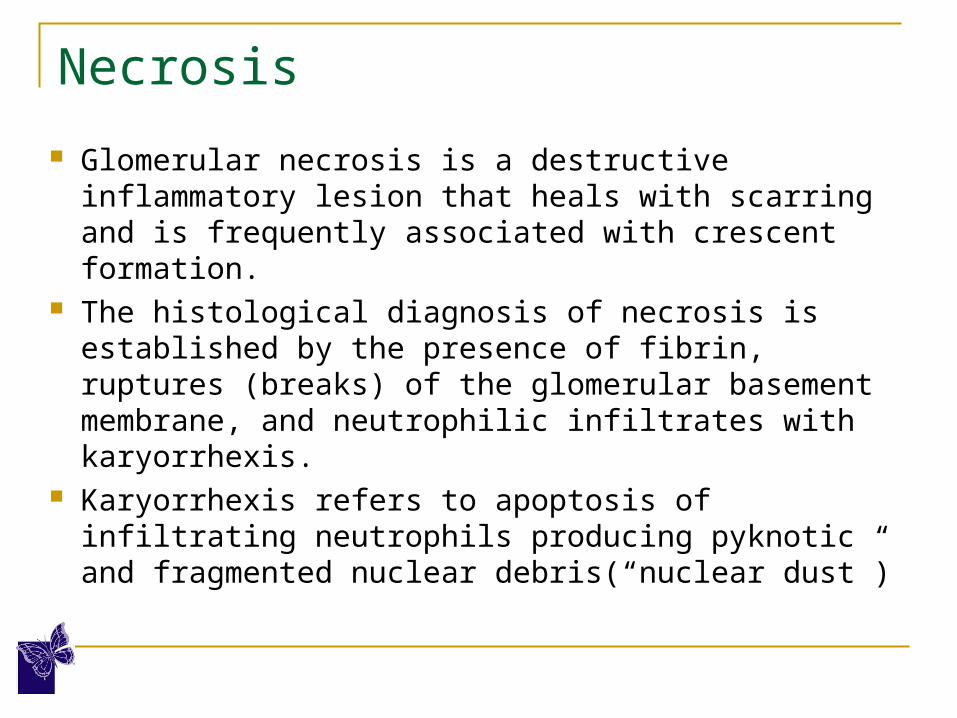
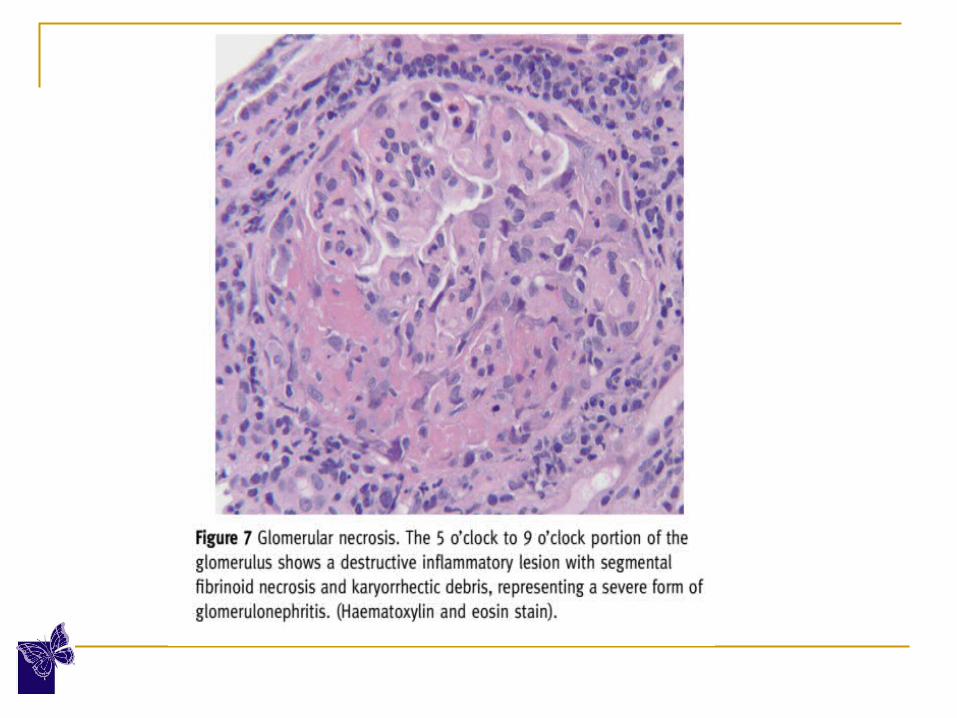
Necrosis
Glomerular necrosis is a destructive inflammatory lesion that heals with scarring and is frequently associated with crescent formation.
The histological diagnosis of necrosis is established by the presence of fibrin, ruptures (breaks) of the glomerular basement membrane, and neutrophilic infiltrates with karyorrhexis.
Karyorrhexis refers to apoptosis of infiltrating neutrophils producing pyknotic and fragmented nuclear debris(“nuclear dust”)
Classification of Lupus Nephritis The original World Health Organization
(WHO) classification of LN introduced in 1974 has evolved into the 2003 International Society of Nephrology (ISN)/Renal Pathology Society (RPS) classification
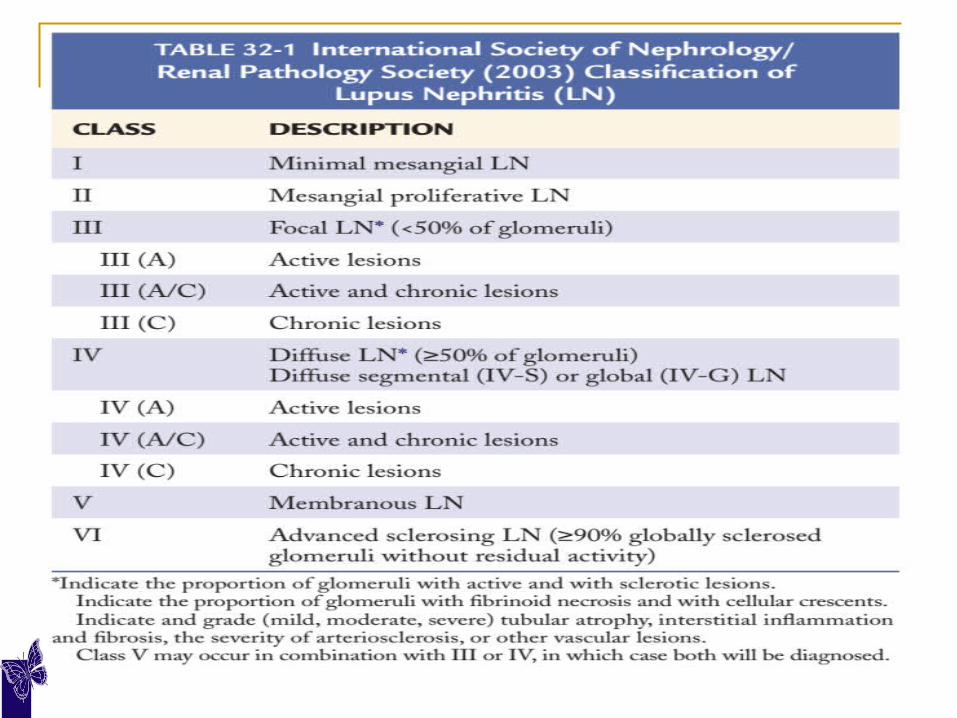

The changes introduced in the new ISN/RPS classification include:
a) The “normal” category of LN was eliminated from the previous WHO classifications, and mesangial LN was thus divided into two categories to maintain the relevant number designation of other classes.
b) ISN/RPS classification has more detailed definitions of specific categories, and this has resulted in improved reproducibility.
ISN/RPS Class I Minimal mesangial lupus nephritis Class I is characterized by normal glomeruli
by light microscopy. Purely mesangial immune deposits identified
by immunofluorescence. This is the mildest form of lupus nephritis, Class I patients have minimal clinical renal
disease

ISN/RPS Class II The glomeruli in Class II may
have any degree of mesangial proliferation by light microscopy, associated with mesangial immune deposits by immunofluorescence.
Mesangial hypercellularity is defined as greater than three cells in mesangial regions distant from the vascular pole in 3-μm–thick sections.
Any active or inactive lesion or significant subendothelial deposits (wire loops) disqualify the biopsy from this class.
The clinical renal manifestations of Class II patients are mild and the prognosis is excellent.
ISN/RPS Class III ISN/RPS class III, focal LN, is defined as focal
(< 50% Gloms) - segmental or global endocapillary or extracapillary GN..
Endocapillary and extracapillary proliferation. Class III biopsies may have active (proliferative),
inactive (sclerosing), or active and inactive lesions subclassified as A, C, or A/C, respectively.
Active lesions may display cellular crescents, fibrinoid necrosis, nuclear pyknosis or karyorrhexis, wireloop lesions, hyaline bodies and rupture of the glomerular basement membrane (GBM).
Hematoxylin bodies, swollen basophilic nuclear material acted upon by antinuclear antibodies, are occasionally found within the necrotizing lesions (Specific Lesion)
In class III biopsies, glomeruli adjacent to those with severe histologic changes may show only mesangial abnormalities by LM.
In class III, diffuse mesangial and focal and segmental subendothelial immune deposits are typically identified by IF and EM.
ISN/RPS class IV ISN/RPS class IV or Diffuse proliferative
LN, has qualitatively similar glomerular endocapillary proliferation as class III, but the proliferation involves more than 50% of the glomeruli
ISN/RPS class IV is subdivided into: i) Diffuse segmental proliferation (class IV-S)
More than 50% of affected glomeruli have segmental lesions
ii) Diffuse global proliferation (class IV-G) More than 50% of affected glomeruli have global
lesions.

The most controversial of these changes in the ISN/RPS classification system is the subdivision of class IV into diffuse global and diffuse segmental LN.
The Lupus Nephritis Collaborative Study Group showed the Class IV-S biopsies had more extensive fibrinoid necrosis and less prominent immune deposits, and despite similar treatment, Class IV-S had a worse prognosis than Class IV-G.
However, several studies have shown that suggest lupus nephritis Class IV-G has a similar or worse outcome than lupus nephritis Class IV-S
ISN/RPS class IV All of the active features described for class
III may be encountered in ISN/RPS class IV LN.
There is more extensive peripheral capillary wall subendothelial immune deposition and extracapillary proliferation in the form of crescents is common.
Occasionaly MPGN pattern or Necrotising vasculitis may also be seen
Class IV patients usually have evidence of active systemic disease and have the most severe and active clinical renal presentation.
Proteinuria is universal, haematuria occurs to variable degrees in 80% - 90% of patients, and renal insufficiency is detected in more than 50% of patients.
These patients have the worst prognosis despite optimal treatment
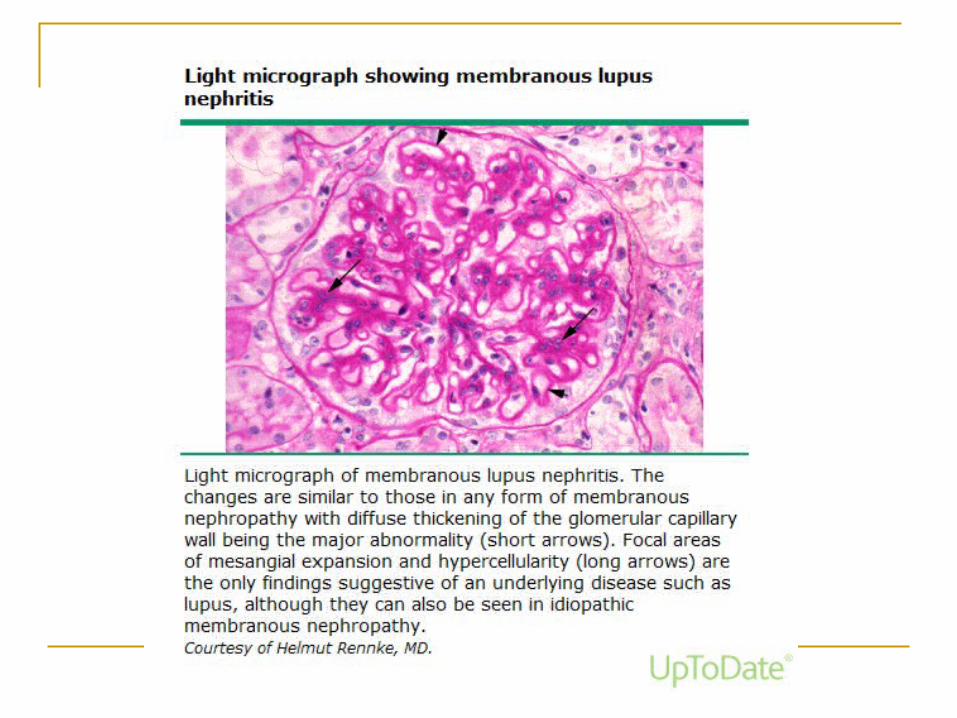
ISN/RPS class V Defined by regular subepithelial immune deposits producing a
membranous pattern The coexistence of mesangial immune deposits and mesangial
hypercellularity helps to distinguish membranous LN from primary membranous glomerulopathy.
There is typically thickening of the glomerular capillary walls and “spike” formation between the subepithelial deposits.
When the membranous alterations are accompanied by focal or diffuse endocapillary proliferative lesions and subendothelial immune complex deposition, they are classified as class V + III and V + IV, respectively.
Because sparse subepithelial deposits may also be encountered in other classes (III or IV) of LN, a diagnosis of pure lupus membranous LN should be reserved only for cases in which the membranous pattern predominates.
ISN/RPS class VI
ISN/RPS class VI, advanced sclerosing LN or end-stage LN, is reserved for biopsies with more than 90% of the glomeruli sclerotic.
There are no active lesions, and it may be difficult to even establish the diagnosis of LN without the identification of residual glomerular immune deposits by IF and EM.

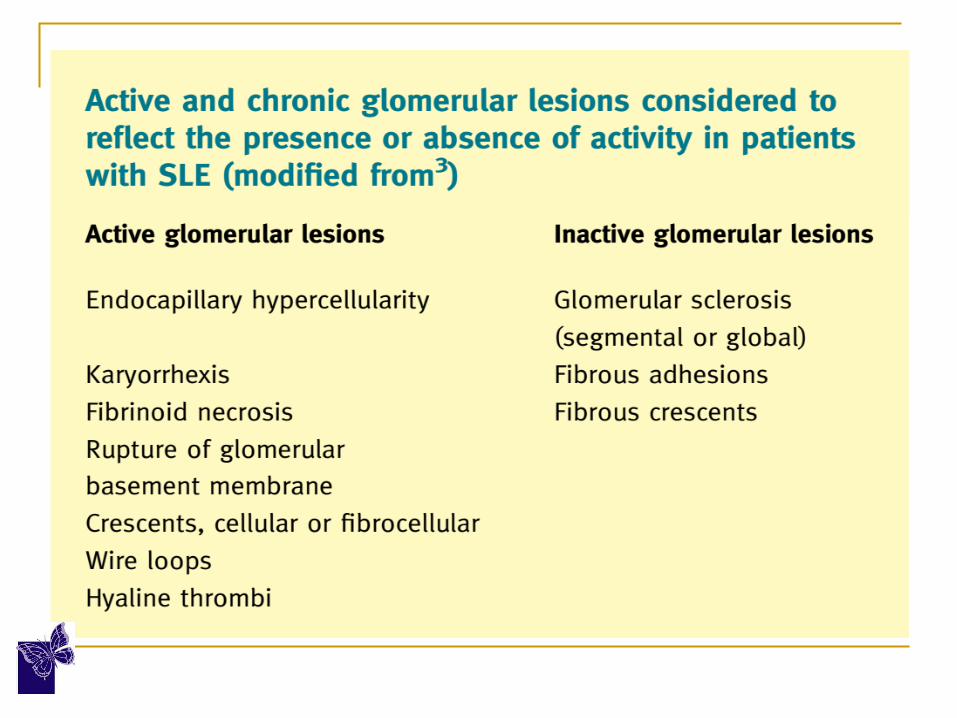
Activity and chronicity Index The biopsy is graded on a scale of 0 to 3+ for each
of six histologic features. The severe lesions of crescents, and fibrinoid
necrosis are assigned double weight. The sum of the individual components yields a total
histologic activity index score of from 0 to 24. Likewise, a chronicity index of 0 to 12 is
derived. High activity index (>12) and especially a high
chronicity index (>4) have a poor 10-year renal survival.
However, in several large studies, neither the activity index nor the chronicity index correlated well with long-term prognosis.


Immunofluoroscence In LN, immune deposits can be found in the
glomeruli, tubules, interstitium, and blood vessels. IgG is almost universal, with co-deposits of IgM
and IgA in most specimens. Both C3 and C1q are commonly identified. The presence of all three immunoglobulins, IgG,
IgA, and IgM,along with the two complement components, C1q and C3, is known as “full house” staining and is highly suggestive of LN.
Staining for fibrin-fibrinogen is common in the distribution of crescents and segmental necrotizing lesions.
Electron Microscopy The distribution of glomerular, tubulointerstitial, and vascular
deposits seen by EM correlates closely with that observed by IF. Deposits are typically electron dense and granular. Some exhibit focal organization with a “fingerprint” substructure
composed of curvilinear parallel arrays measuring 10 to 15 nm in diameter.
Tubuloreticular inclusions (TRIs), intracellular branching tubular structures measuring 24 nm in diameter located within dilated cisternae of the endoplasmic reticulum of glomerular and vascular endothelial cells, are commonly observed in SLE biopsies.
TRIs are inducible upon exposure to INF-α(so-called “INF footprints”) and are also present in biopsies of HIV-infected patients and those with some other viral infections
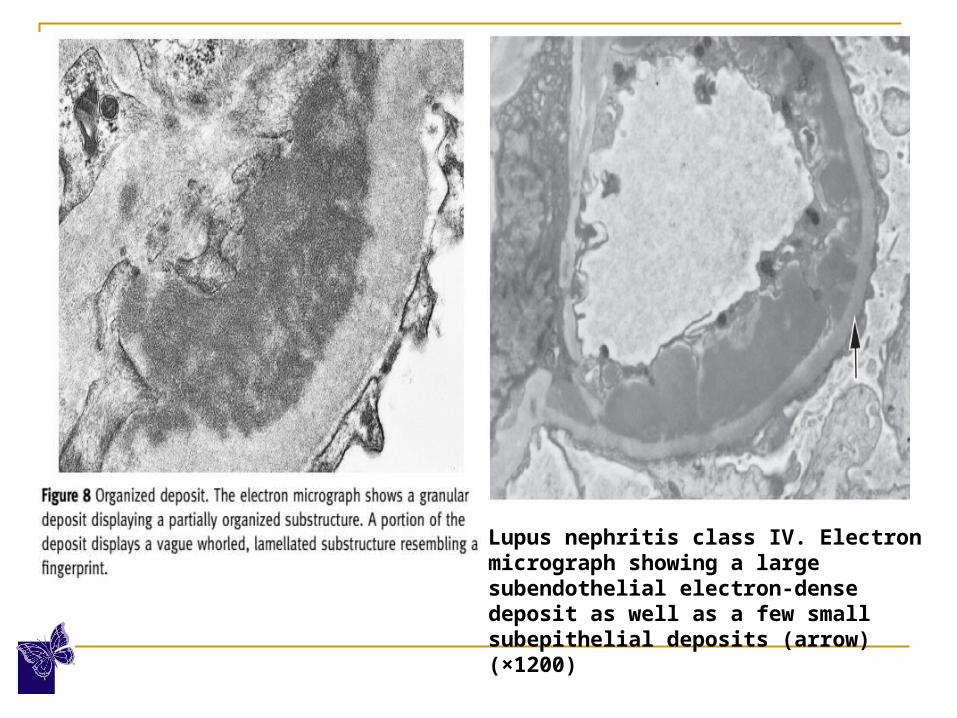
Lupus nephritis class IV. Electron micrograph showing a large subendothelial electron-dense deposit as well as a few small subepithelial deposits (arrow) (×1200)
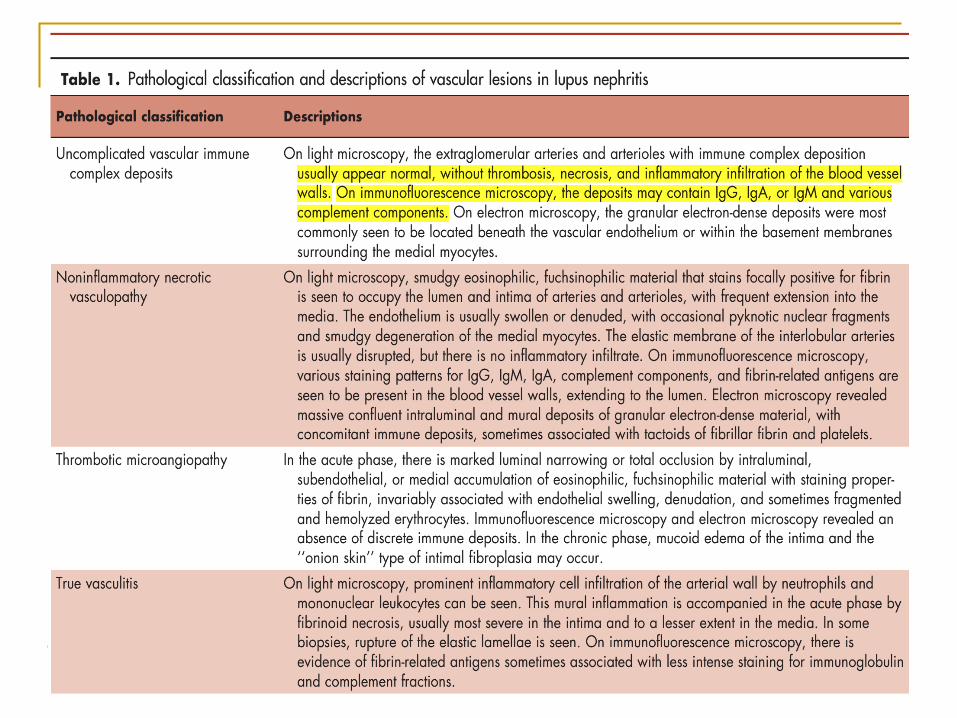
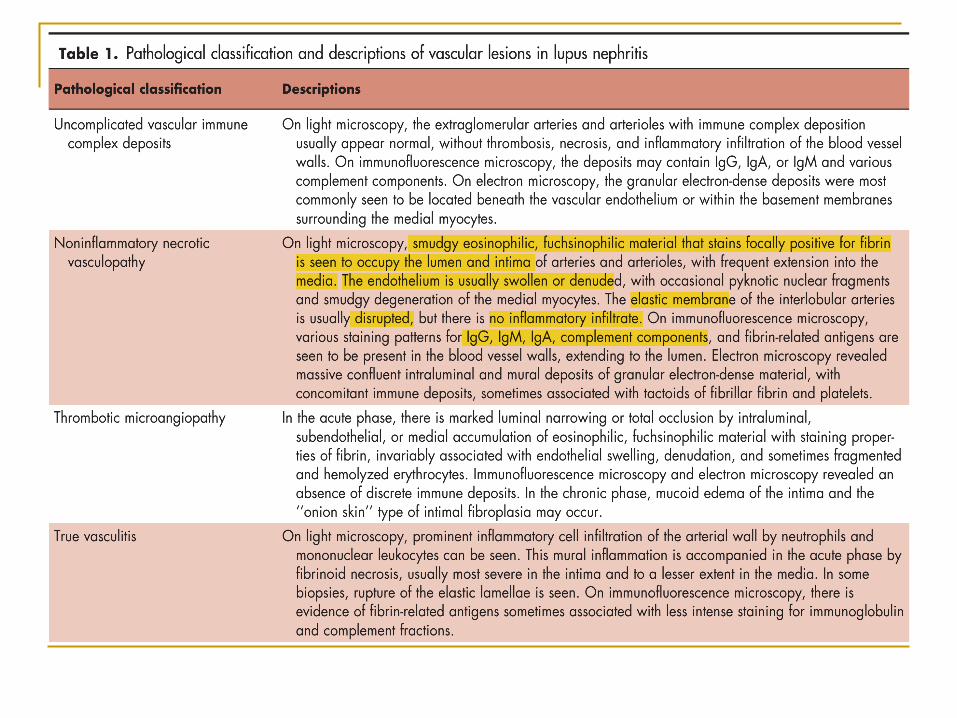
Prognostic Factors Not Addressed in the ISN/RPS classification – Tubulointerstitial and vascular involvement The ISN/RPS classification is based entirely on an
assessment of the glomerular alterations; Tubulointerstitial and vascular lesions were not
factored into the previous WHO classifications nor the 2003 ISN/RPS classification.
However, the 2003 ISN/RPS classification stipulates that the pathology report should include grading of the degree of tubular atrophy and interstitial fibrosis, interstitial inflammation and vascular disease.
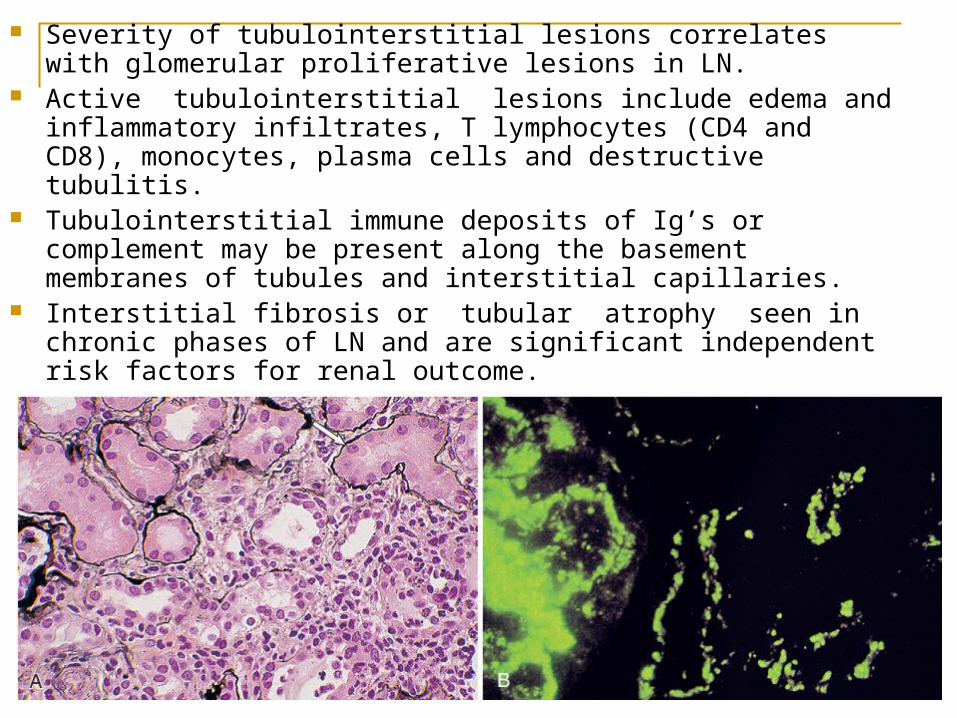
Severity of tubulointerstitial lesions correlates with glomerular proliferative lesions in LN.
Active tubulointerstitial lesions include edema and inflammatory infiltrates, T lymphocytes (CD4 and CD8), monocytes, plasma cells and destructive tubulitis.
Tubulointerstitial immune deposits of Ig’s or complement may be present along the basement membranes of tubules and interstitial capillaries.
Interstitial fibrosis or tubular atrophy seen in chronic phases of LN and are significant independent risk factors for renal outcome.


Biomarkers in detecting lupus activity Conventional markers of active renal disease are serum levels of
anti-dsDNA, anti-C1q antibody and complement levels have variable sensitivity between 50 and 75% for active renal disease.
Urinary biomarker candidates have included adhesion molecules, cytokines, chemokines, and their receptors, including VCAM-1, P-selectin, IL-6, IP-10, RANTES, MCP-1, CXCL16, CX3CL1, TWEAK, and TNFR1
Urinary proteomic approaches have been used to identify proteins like transferrin, ceruloplasmin, hepcidin 20, hepcidin 25, α1-acid-glycoprotein, lipocalintype prostaglandinD-synthetase, and neutrophil gelatinase associated lipocalin.
The utility of above biomarkers need independent confirmation in large scale prospective studies.
Conclusions Lupus nephritis can present as nephritic
and/or nephrotic syndrome with various combinations of edema, constitutional symptoms, proteinuria, hematuria, impaired renal function, abnormal lipid profile and hypertension.
Kidney biopsies remain the gold standard for establishing the diagnosis/prognosis/treatment of LN.

Thank you