nyulmc neurological surgery - nyu langone health...neurosurgery, functional neurosurgery, peripheral...
TRANSCRIPT
1
ProgramManual
NYULMC
NEUROLOGICALSURGERY2016-2017
ADEPARTMENTALGUIDEFORRESIDENTSANDFACULTYCANBEVIEWEDONLINEON
NEWINNOVATIONSANDNEUROSURGERYWEBSITE:Dateupdated:Fall/2016
2
TableofContents
ProgramManual..........................................................................................................................1OverviewoftheNeurosurgeryResidencyTrainingProgram...............................................4ProgramDirector,AssociateDirector,&AdministrativeStaff.........................................................5Facilities...................................................................................................................................................................6CoreFaculty............................................................................................................................................................8
CoreFacultybySections.....................................................................................................................8BrainTumors&SkullBaseNeurosurgery....................................................................................8Spinal&PeripheralNerveNeurosurgery......................................................................................8CerebrovascularNeurosurgery.......................................................................................................8CenterforNeuromodulation(DeepBrainStimulationandNeurostimulationforPainandHeadache).......................................................................................................................................9Epilepsy....................................................................................................................................................9PediatricNeurosurgery.......................................................................................................................9Research..................................................................................................................................................9BellevueHospital..................................................................................................................................9VeteransAffairsMedicalCenter.....................................................................................................10TrainingProgramCurriculum........................................................................................................11TrainingProgramSchedules..........................................................................................................14Conferences.........................................................................................................................................................17
ConferenceSchedule..........................................................................................................................17ConferenceDescriptions/Topics...................................................................................................17DidacticResidentEducation........................................................................................................................20
Goals&Objectives–Overall............................................................................................................21Goals&Objectives–BySite,RotationANDClinicalyear................................................................22
Policies...................................................................................................................................................85BLS/ACLS/PALS/NRP/ATLStrainingPolicy........................................................................................89CaseLogPolicy&Procedure........................................................................................................................92ChiefResidentorFellowPolicy..................................................................................................................95ConcernsandComplaintsPolicy................................................................................................................98CorrectiveActionandDisciplinaryPolicy............................................................................................102DisasterPolicy..................................................................................................................................................115DutyHourPolicy.............................................................................................................................................120
HowToReportDutyHourViolationsatNYU:..............................................................................122HowToReportDutyHourViolationsatBellevue:.............................................................122
EvaluationPolicy.............................................................................................................................................131FatigueMitigationPolicy.............................................................................................................................136ImpairmentPolicy..........................................................................................................................................139MoonlightingPolicy.......................................................................................................................................143On-callPolicy....................................................................................................................................................144Out-rotation/ElectivePolicy......................................................................................................................146ProfessionalismPolicy..................................................................................................................................152RecruitmentandSelectionPolicy............................................................................................................156SupervisionandScopeofPracticePolicy(includingEscalation)..............................................158
3
TermsandConditionsofEmploymentPolicy....................................................................................164Time-offandEffectofTakingLOAPolicy..................................Error!Bookmarknotdefined.TransitionsofCare.........................................................................................................................................172
NEUROSURGERYPROGRAMTRANSITIONSOFCAREPOLICY.............................................172Book&ConferenceFund...................................................................................................................................178PatientSafety/QualityImprovementResources,Expectations&Curriculum..........................183EducationandScholarlyActivitiesforTrainees.....................................................................................185EducationandScholarlyActivitiesforFaculty........................................................................................186ClinicalCompetencyCommitteeDescription(CCC)..............................................................................188ProgramEvaluationCommitteeDescription(PEC)....................................................................189Evaluationoftheresident/fellowbythefaculty(byeachlearningexperience)................190
Evaluationforeachlearningexperienceinareaofsub-specialtytraining....Error!Bookmarknotdefined.
Evaluationofthefacultybytheresident/fellow...............................................................................206Semi-AnnualEvaluation(bytheProgramDirector).......................................................................211SummativeEvaluation(bytheProgramDirector)...........................................................................214Evaluationoftheprogrambytheresident/fellow...........................................................................215Evaluationoftheprogrambythefaculty.............................................................................................218
Examinations,Licensure&Certificate......................................................................................219HouseStaffWellbeing....................................................................................................................223MandatedOnlinemodulesforHouseStaff..............................................................................230NYULMCMedicalLibrary...............................................................................................................231OnCallRooms...................................................................................................................................232CommitteeParticipationforHouseStaff.................................................................................234AdditionalInformation..................................................................................................................236UsefulLinks&Resources..............................................................................................................238

4
OverviewoftheNeurosurgeryResidencyTrainingProgram
TheNeurologicalSurgeryResidencyTrainingProgramsponsoredbyNYUSchoolofMedicineattheNYULangoneMedicalCenterisaseven-yearprogramdesignedtoprovideresidentswithincreasingclinicalandsurgicalresponsibilityoverthecourseoftheirtraining,inordertopreparegraduatesforanacademicneurosurgicalcareer;ahigh-qualitypracticeintheprivatesector;orfurthertraininginasub-specialtyfellowship.
TheoverallgoaloftheDepartmentofNeurologicalSurgerytrainingprogramatNewYorkUniversity(NYU)SchoolofMedicineistotrainhighlymotivated,Confident,andclinically excellent neurological surgeonswho are not onlyskilled in the technicalaspectsof the specialtybut alsoappreciate the humanistic sideof thepracticeofmedicine and the collegiality of their peers. TheNYUNeurological SurgeryDepartmentisorganizedintosub-specialtyteamsthatspanacrosstheparticipatinginstitutionswith each individual faculty member focused in an area of clinical andresearchexpertise including: vascular/endovascularNeurosurgery, tumorandskullbaseneurosurgery,complexreconstructiveandminimallyinvasivespinalsurgery,pediatricneurosurgery,functionalneurosurgery,peripheralnervesurgery,adultandpediatricepilepsysurgery,stereotacticradiosurgery,andneurotrauma.Affiliatedfacultymembersfromothersubspecialtiesalsoparticipateinresidentteachinginendovascularneurosurgery(InterventionalNeuroradiology),skullbasesurgery(Neuro-otology),andNeuro-oncology.
5
ProgramDirector,AssociateDirector,&AdministrativeStaff
ChairmanJohnG.Golfinos,MDDepartmentofNeurosurgeryJohn.Golfinos@nyumc.org212-263-2950ViceChairmanandProgramDirectorHowardRiina,MDHoward.Riina@nyumc.org212-263-0094AssociateProgramDirectorDavidHarter,[email protected]
ProgramManagerEducationandAcademicAffairsIvonneMonterreyIvonne.Monterrey@nyumc.org212-263-6415ProgramAdministrativeAssistantLaverneCummingsLaverne.Cummings@nyumc.org212-263-6413ProgramAdministrativeAssistantAllisonGeorge-LucasAllison.George-Lucas@nyumc.org212-263-6416BusinessManagerJoeMarinoJoseph.Marino@[email protected]
6
FacilitiesOurresidency-trainingprograminclinicalneurosurgeryutilizesthreemedicalinstitutions,alllocatedinclosegeographicalproximitytoeachotherontheEastSideofManhattanbetween23rdand34thStreet.• NYULangoneMedicalCenter(TischHospital).LocatedonNYULangone’smaincampus,TischHospitalhousesafull-service,state-of-the-artacutecareneurosurgicalfacilitythatperformsapproximately1,800neurosurgicalprocedureseachyear.AtTischHospital resources inc lude: 5stateof theartneurosurgical suitesareavailabledaily.TheseOR’shavefullmicrosurgicalcapabilities.ThereisalsoadedicatedcombinedOR/angiography suite.Additionally, a 2-roomdigitalneuroangiographysuiteisavailabletoneurosurgerydailyintheneuroradiologysuite.WehaveaddedanewGammaKnife®PERFEXIONunitwhichhasenhancedourcapabilities in Stereotactic radiosurgery.We have also added five newBrainLabSystems,aStrykerNavigationsystem,andaStealthO-ARMsystemthatenhance our frame based and framelessStereotactic surgery and spinalnavigation capabilities. Ourstate-of-the-artneurosurgicalintensivecare/postoperativeunithastenbedsandisadjacenttoourneurosurgicalfloor,whichcontainsanother18beds.Inaddition,therenownedRuskInstituteofRehabilitationMedicinealsopartofNYULangoneMedicalCenterisoftenusedforthesubacuteneurosurgicalrehabilitationofourpatients.
• BellevueHospitalCenter.ThisworldfamouscityhospitalandAmerica’soldestpublichospitalandaregionalLevel1TraumaCenter,isaflagshipoftheNYCHealthandHospitalcorporationandtheheartandsouloftheNYULMCNeurosurgeryprogram.ItsmissionistoprovidethebestavailablemedicalcaretotheresidentsofNYCresidentsofNYCregardlessofincomeorsocioeconomicstatus.Bellevueprovidescomprehensiveneurosurgicalcareinfacilitiesthatincludeabrand-newsix-bedneurosurgicalICU,and24bedsontheneurosurgery/neurologyfloor.Inadditiontotrauma,BellevueHospitalCenterprovidesauniqueclinicalexperiencewithintheNYULangoneneurosurgicalresidencytrainingprogram.At Bellevue hospitalthereis1dedicatedstateoftheartneurosurgicalsuite withfull microsurgical capabilities available to the Neurosurgical service onscheduledORdaysandforneurosurgicalemergencycases.
• VANewYorkHarborHealthcareSystem(formerlytheManhattanVeterans
AdministrationMedicalCenter).TheVANewYorkHarborHealthcareSystemistheprimaryveteransneurosurgicalreferralcenterforNewYorkCityandsurroundingareas.Ithas1dedicatedstateof

7
theartneurosurgicalsuite with full microsurgical capabilities available to theneurosurgical service.CurrentlyunderconstructionisNYULangone’snewKimmelPavilion,astate-of-the-artclinicalfacilityscheduledtoopenin2018,whichwillbeoneofthemostadvancedneurosurgicalfacilitiesinthecountry.Itwillcontainadedicatedneurosurgicaloperatingsuitecomprisedof8stateofthe art OR’s (2 withintraoperative MRI capabilities, and 2 dedicated combinedOR/angiographysuites(hybridoperatingrooms),comprisingthesecondflooroftheKimmelPavilion.Thisfacilitywillalsoincludeabrandnewneurologicalintensivecareunit,neurologicalcarestep-downunit,patientroomsaswellasapediatrichospitalwithinahospitalwithadditionaldedicatedpediatricneurosurgicalspace.
8
CoreFaculty
CoreFacultybySections
BrainTumors&SkullBaseNeurosurgery
JohnG.Golfinos,MD–ChairmanoftheDepartmentofNeurosurgery/Co-Director,BrainTumorsCenter
ChandranathSen,MD–Professor/Director,SkullBase
DouglasKondziolka,MD,MSc–Professor/Director,CenterforAdvancedRadiosurgeryatNYULangoneMedicalCenter
DimitrisPlacantonakis,MD,PhD–AssistantProfessor
JafarJafar,MD–Professor/Director,CerebrovascularSurgery,Neurosurgeon-in-Chief
DavidGordon,MD–AssistantProfessor
Spinal&PeripheralNerveNeurosurgery
AnthonyFrempong-Boadu,MD–AssociateProfessor/Director,SpinalSurgery/Co-Director,SpineCenter
NoelPerin,MD–AssociateProfessor/Director,MinimallyInvasiveSpinalSurgery
MichaelSmith,MD–AssistantProfessor
DonatoPacione,MD–AssistantProfessor
RameshBabu,MD–AssociateProfessor
ErichAnderer,MD–AssistantProfessor
CerebrovascularNeurosurgery
HowardA.Riina,MD–Professor/Director,EndovascularSurgery
JafarJafar,MD–Professor/Director,CerebrovascularSurgery,Neurosurgeon-in-Chief
PaulHuang,MD–AssistantProfessor
9
DavidGordon,MD–AssistantProfessor
CenterforNeuromodulation(DeepBrainStimulationandNeurostimulationforPainandHeadache)
AlonMogilner,MD,PhD–AssociateProfessor/Director,CenterforNeuromodulation
DouglasKondziolka,MD,MSc–Professor/Director,CenterforAdvancedRadiosurgeryatNYULangoneMedicalCenter
MichaelPourfar,MD–AssociateProfessor
EpilepsyWernerDoyle,MD–AssociateProfessor
AdultHydrocephalusProgram
JamesB.Golomb,MD–AssistantProfessor
PediatricNeurosurgery
JeffreyWisoff,MD–Professor/Director
DavidHarter,MD–AssistantProfessor/AssociateDirector,NeurosurgeryResidencyTrainingProgram
AmandaYaun,MD–AssistantProfessor
E.TeresaHidalgo,MD–ClinicalInstructor
Research
MitchellChesler,MD–Professor/ViceChair,Research
DouglasKondziolka,MD,MSc–Professor/ViceChair,ClinicalResearch
MargaretRice,PhD–Professor
DimitrisPlacantonakis,MD,PhD–AssistantProfessor
10
Hae-RiSong,MD–AssistantProfessor
BELLEVUEHospitalPaulHuang,MD–AssistantProfessor/ChiefBellevueNeurosurgeryServiceStephenRussell,MD–AssistantProfessor
NYULutheranMedicalCenter
ErichAnderer,MD–AsistantProfessor/Chief
DavidGordon,MD–AssistantProfessor
VANYHarborHealthcareSystem,ManhattanCampus
JamesStone,MD–Professor/Chief
11
TrainingProgramCurriculumCHRONOLOGICALROTATIONS,TRAININGSTRUCTUREANDCURRICULUMAllrotationsarerequiredYear1:InternshipInthefirstpostgraduateyear(PGY-1)residentsarerequiredtoparticipateinaneurosurgicalinternshipatNewYorkUniversity.TheinternyearconsistsofaNeuroscienceblockthatincludes3monthsofNeurologyandonemontheachofneuropathology,neuroradiology,andneurosurgery(atBellevueHospitalandTischHospital).TheNeurosurgeryrotationallowsthenewresidentstobecomefamiliarwiththeday-to-dayoperationoftheNYUneurosurgicalservicethusallowingthemtogaininsightintowhatwillberequiredofthemastheyprogressthroughtheneurosurgicalresidencytrainingprogram.TheinternshipalsoincludesaGeneralSurgeryexperiencethatincludesadultgeneralsurgery,ICU/Criticalcare,andtraumasurgery.Mostoftheserotationshavemajorcriticalcareexperiencesaspartoftheoverallinternshipexperience.Year2:ClinicalNeurosurgery,Neuropathology,andNeuroradiologyInthesecondyearofneurosurgeryresidency(PGY-2),theresidentshavefourthreemonthrotationsonfourdistinctNYUNeurosurgicalServices:TischHospitalTeam1(TumorVascular/SkullBase/Functional/EpilepsyService),TischTeam2(Spine/PeripheralNerveServices),BellevueHospitalCenter,andNewYorkHarborHealthCareSystem(VA).Therotationsprovideneurosurgicalward,neurosurgicalclinicandcriticalcareexperiencesinvariedneurosurgicalpracticeenvironments.Withclosesupervision,theresidentsareintroducedtobasicwardandoperativeproceduresincludingtraumacraniotomy,CSFdiversion(ventriculostomiesandshunts),lumbarpunctures,tractionforspinetrauma,basicspineprocedures,peripheralnerveproceduresandintracranialpressuremonitoring.Residentsarealsointroducedtointerventionalneuroradiologyproceduresincludingbasicangiography.Year3:ClinicalNeurosurgery,Neuropathology,andNeuroradiologywithGraduatedResponsibilitiesInthethirdyearofneurosurgeryresidency(PGY-3),theresidentsrotatewithincreasedlevelsofward,clinic,ICUandoperativeresponsibilitiesthroughthesamefourthreemonthrotationstheydidasaPGY2year-TischHospitalTeam1(TumorVascular/SkullBase/Functional/EpilepsyService),TischTeam2(Spine/PeripheralNerveServices),BellevueHospitalCenter,andNewYorkHarborHealthCareSystem(VA).Therotationscontinuetoprovideneurosurgicalward,clinicandcriticalcareexperiencesinvariedneurosurgicalpracticeenvironments.Withclosesupervisionfromthechiefresidentsandfaculty,theresidentsareintroducedtoincreasinglycomplexwardandoperativeprocedures,andoutpatientclinicsatBHCandtheVA(oneday/wk),andmanagementofneurosurgicalemergenciesintheBHandtheNICU.Thisincludesbothincreasedresponsibilityforoperativeandnon-operativepatientcare.spinetraction,simplespineprocedures,peripheralnerveproceduresandintracranialpressuremonitoring.InterventionalNeuroradiologyrotationsatboth
12
BellevueandTischintroducetheresidentstointerventionsincludinganeurysmtreatment,managementofvasospasmandtumorembolization.ResidentsalsoareintroducedtoGammaKniferadiosurgeryincludingheadframeapplicationandlesiontreatmentplanning.Year4:Pediatrics/Epilepsy/TraumaInthefourthyearofneurosurgeryresidency(PGY-4),isdividedbetweensixmonthsastheseniorresidentonthepediatricneurosurgeryserviceatNYULangone’sTischHospitalandsixmonthsastheseniorresidentontheneurosurgicaltraumaserviceatBellevueHospital.Theserotationsprovidegraduatedclinicalandoperativeresponsibilitywithadefinedpatientpopulation.Thesix-monthrotationperiodaschiefresidentonthePediatricNeurosurgeryservicewithDrs.WisoffandHarterallowsforain-depthexposuretothesub-disciplineofpediatricneurosurgery.Residentexperienceacontinuityofcarelearningexperiencebyparticipatinginthemedicalaswellassurgicalmanagementofthesepatients.Patientsseepatientsintheclinicandfollowthemthrutheirpre-operative,operativeandpostoperativecare.Duringthesesixmonths,thechiefisexposedtothefullrangeofoperativepediatricneurosurgicaldisorders,includinganextensiveexperiencewithpediatricbraintumors,epilepsyandcranialendoscopy.ThedivisionhascollaborativeeffortswiththeDepartmentofPlasticSurgeryinthetreatmentofcraniofacialdisorders.ThetraumaexperienceattheBellevueHospitalrepresentsauniqueneurosurgicalexperienceatoneofthebusiestlevel1traumacentersinNewYorkCity.Year5:Research/ElectiveThefifthneurosurgeryyear(PGY-5)isentirelydevotedtoahypothesis-drivenbasicscienceresearchprojectinordertoestablishthefoundationforanacademicorotherinnovativeneurosurgicalcareerorunderspecialcircumstances,adedicatedyearlongsubspecialtyclinicalelective.Inthepast,residentshavechosenfocusedclinicalelectivesinFunctionalNeurosurgery,EndovascularNeurosurgery,Radiosurgery,andComplexSpineSurgery.ThePGY5residenttakesnightcallastheprimaryemergencyconsultresidentandfirstassistantfortheBellevueHospitalChiefResidentinemergency/traumacaseswithgraduatedlevelsofoperativeresponsibility.ResidentscontinuetoattendneurosurgicaldidacticconferencesandothermajorDepartmentaleventsduringthisyear.TheNeurologicalSurgerydepartment’seffortandcommitmenttoresearchforHouseStaffwillnowincludetheIntensiveTraininginResearchStatistics,Ethics,andProtocolInformaticsandDesign(INTREPID)SummerIntensiveProgramforeachandeveryresidentstartingtheirfifthorresearchyear.
Year6:ClinicalNeurosurgery(ChiefResidentYear#1)Thesixthneurosurgeryyear(PGY-6)isdividedbetweentwo6-monthsenior/servicechiefresidentrotationsontheTischHospitalNeurosurgeryservices:Team1(Tumor/Vascular/SkullBase/Functional/EpilepsyService),andTeam2(SpinalandPeripheralNerveServices). Theserotationsprovide theopportunity tomanageaclinical service with directed supervision and

13
educational responsibility for juniorresidentsandrotatingmedicalstudents.UnderthesupervisionoftheNeurosurgicalFaculty, theresidentassumesincreasingoperativeandnon-operativepatientcareresponsibility.Thisincludesgreaterparticipationinthecrucialportionofneurosurgicaloperativeprocedures.Year7:ClinicalNeurosurgery(ChiefResidentYear#)Theseventhneurosurgeryyear(PGY-7)isdevotedto6monthsofChiefResidencyeachatBellevueHospitalCenterandattheNewYorkHarborHealthCareSystem.TheBellevuechiefresidentalsoservesasadministrativechiefresidentfortheNYUNeurosurgery Residency Program. With appropriatesupervision, these rotationsprovide the residentswithanopportunity toessentially completelydirecta clinicalservicewithlongitudinalfollow-upofallpatientsfrominitialconsultation(intheclinicsorER)throughtopostoperativefollow-up.TheNewYorkHarborHealthCareSystemistheregionalVANeurosurgicalreferralcenterforthetri-stateregionandBellevue Hospital is abusy Level -1 trauma center and the mainfacility of the publichospitalsystem(HHCsystem)inNewYorkCity.
14
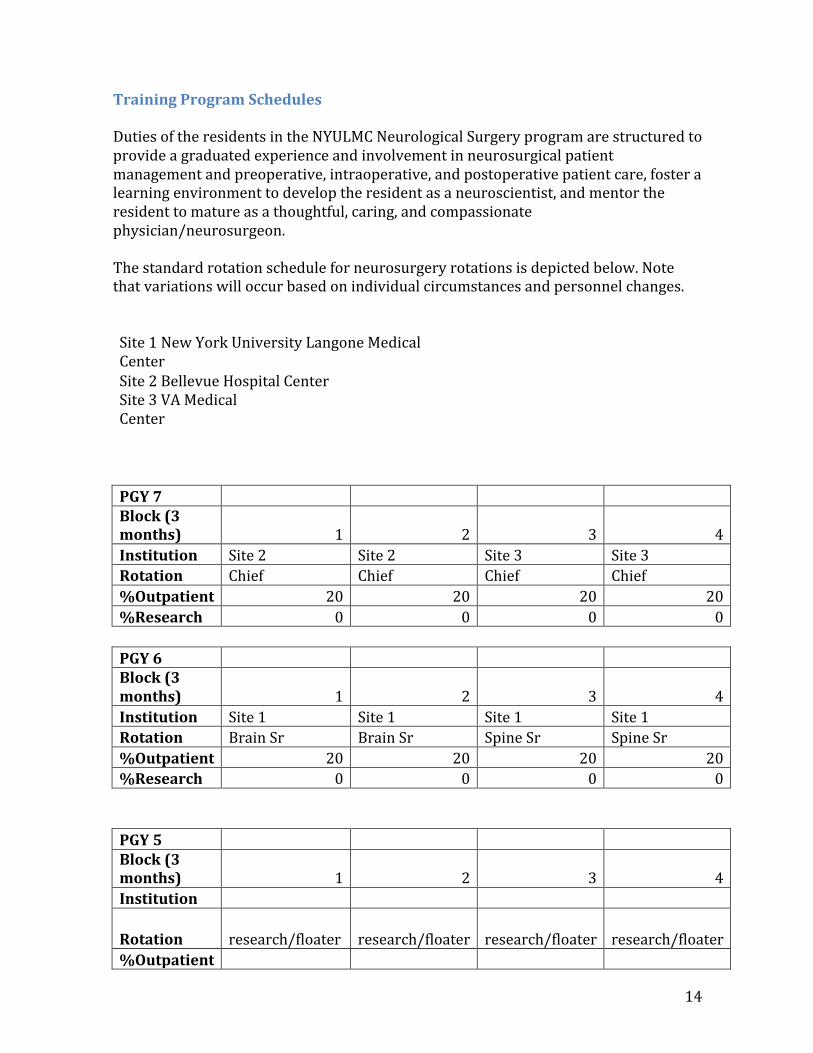
TrainingProgramSchedulesDutiesoftheresidentsintheNYULMCNeurologicalSurgeryprogramarestructuredtoprovideagraduatedexperienceandinvolvementinneurosurgicalpatientmanagementandpreoperative,intraoperative,andpostoperativepatientcare,fosteralearningenvironmenttodeveloptheresidentasaneuroscientist,andmentortheresidenttomatureasathoughtful,caring,andcompassionatephysician/neurosurgeon.Thestandardrotationscheduleforneurosurgeryrotationsisdepictedbelow.Notethatvariationswilloccurbasedonindividualcircumstancesandpersonnelchanges.
Site1NewYorkUniversityLangoneMedicalCenterSite2BellevueHospitalCenter Site3VAMedicalCenter PGY7 Block(3months) 1 2 3 4 Institution Site2 Site2 Site3 Site3 Rotation Chief Chief Chief Chief %Outpatient 20 20 20 20 %Research 0 0 0 0 PGY6 Block(3months) 1 2 3 4 Institution Site1 Site1 Site1 Site1 Rotation BrainSr BrainSr SpineSr SpineSr %Outpatient 20 20 20 20 %Research 0 0 0 0 PGY5 Block(3months) 1 2 3 4 Institution
Rotation research/floater research/floater research/floater research/floater %Outpatient
15
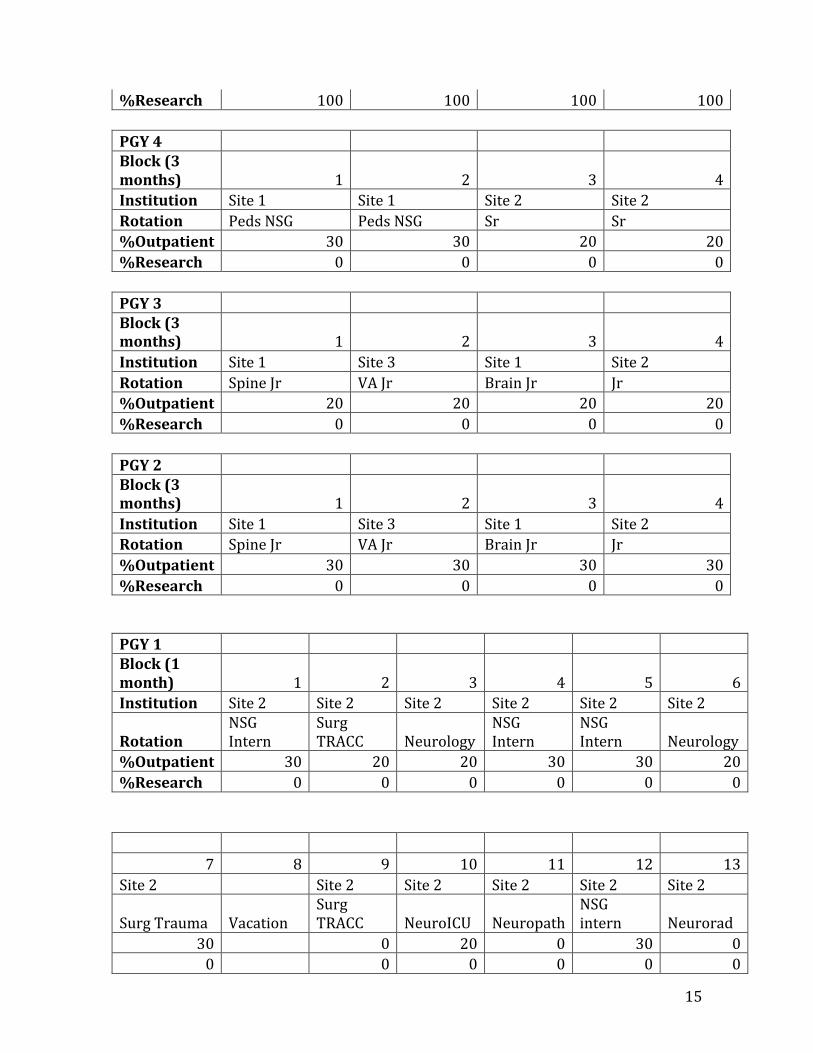
%Research 100 100 100 100 PGY4 Block(3months) 1 2 3 4 Institution Site1 Site1 Site2 Site2 Rotation PedsNSG PedsNSG Sr Sr %Outpatient 30 30 20 20 %Research 0 0 0 0 PGY3 Block(3months) 1 2 3 4 Institution Site1 Site3 Site1 Site2 Rotation SpineJr VAJr BrainJr Jr %Outpatient 20 20 20 20 %Research 0 0 0 0 PGY2 Block(3months) 1 2 3 4 Institution Site1 Site3 Site1 Site2 Rotation SpineJr VAJr BrainJr Jr %Outpatient 30 30 30 30 %Research 0 0 0 0 PGY1 Block(1month) 1 2 3 4 5 6Institution Site2 Site2 Site2 Site2 Site2 Site2
RotationNSGIntern
SurgTRACC Neurology
NSGIntern
NSGIntern Neurology
%Outpatient 30 20 20 30 30 20%Research 0 0 0 0 0 0
7 8 9 10 11 12 13Site2 Site2 Site2 Site2 Site2 Site2
SurgTrauma VacationSurgTRACC NeuroICU Neuropath
NSGintern Neurorad
30 0 20 0 30 00 0 0 0 0 0

16
17
ConferencesNeurosurgeryDepartmentConferencesTheconferencesoccurduringablockoftimeprotectedfromelectiveclinicalactivity.Residentsarerequiredtoattendatleast75%ofallmandatoryresidentconferences.Conferenceattendance,punctualityandparticipationwillbereviewedanddiscussedattheMilestoneEvaluationCommitteeandwithindividualresidentsattheirsemi-annualreview.Designatedfacultyareassignedtooverseeeachconference.Allfacultymembersareinadditionencouragedtoattendallconferencesandarerequiredtoattendselectedconferences.TheNeurosurgeryDepartmentholdsintra-andinterdepartmentalteachingconferencesthroughouttheweek,withFridaysdevotedtoconferencesfrom7:30a.m.to3:00p.m.asanacademicday.Electivesurgerymaybeperformedbutwithoutdedicatedresidentcoverage.Conferencesarestructuredwithanemphasisonresidenteducation,astraineespresentclinicalproblemsandarequestionedinordertosharpentheirdecision-makingskills.Theformatandtopicsorsubjectmatterismodeledaftertheoralneurosurgicalboardexamination.GrandRoundsguestpresenters/visitingprofessorsareselectedbasedontheirareasofclinicalandresearchexpertise.Followinggrandroundspresentations,visitingprofessorsspendadditionaltimewiththeresidentsdiscussingcomplexcases,issuesinacademicneurosurgeryandcareerchoices.
ConferenceScheduleMonday9:00amCraniofacialConferenceMonday3:30pmEpilepsyCaseConferenceWednesday7:30amCerebrovascularConferenceThursday7:30amPituitaryConference(SecondThursdaysofthemonth)Friday:7:30amSpineandPeripheralNerveConference8:00amNeurosurgeryGrandRounds,(Speakers,Unknowns,MorbidityandMortality)9:30amNeuro-OncologyTumorBoard12:00pmPediatricNeurosurgeryCaseConference1:00pmChairmanRounds
ConferenceDescriptions/TopicsCraniofacialConference:HeldweeklyinconjunctionwiththeDepartmentofPlasticSurgery,thisinternationallyrecognizedclinic-conferencefocusesonchildrenwithcomplicatedcraniofacialabnormalities.
18
EpilepsyCaseConference:Thisisamultidisciplinaryconferenceheldtodiscusssurgicalmanagementofpatientswithtreatmentresistantepilepsy.Location:TheconferenceroomattheNYUComprehensiveEpilepsyCenter,223E.34thSt.inManhattan.Forinformation,contactMargieHernandezat646-558-0801orElizabethOdewaleat646-558-0802.CerebrovascularConference:Thisconferenceisacombinedneurosurgeryandinterventionalneuroradiologycasemanagementconference.Interestinganddifficultcasesarereviewedanddecisionsaremaderegardingthemostappropriatemanagementstrategies.PituitaryConference(secondThursdayofeachmonth):Thisisamulti-institutionalandmulti-disciplinaryconferenceofthedepartmentsofNeurosurgery,Endocrinology,Neuro-OphthamologyandRadiationOncology.Interestingcasesanddifficultclinicalproblemsarepresentedandtheirmanagementdiscussed.SpineandPeripheralNerveConference:ThisconferenceisheldeveryFridaythroughouttheyearunderthedirectionofDr.AnthonyFrempongofNeurosurgery.Pre-andpostoperativecasesarepresented,andresidentsareaskedtointerpretimagingstudiesanddiscussmanagementstrategiesandtechnicalaspectsofsurgicalprocedures.Inadditiontospinecases,oneperipheralnervecaseisreviewedeachweek.NeurosurgeryGrandRounds:ThisconferenceisheldeveryFridayduringthemonthsofSeptemberthroughJune.GrandRoundsisattendedbyNeurosurgeryfaculty,residents,andinterestedcommunityneurosurgeons.Duringthefirsthour,alecturerelatedtotheneurosciencesisgivenbymedicalschoolfacultyorvisitingprofessors(aboutfiveperyear).Thesecondhourisdevotedtopresentationofinterestingcasesbyresidents,followedbydiscussionoftheirmanagementbyresidentsandfaculty.TheGrandRoundsonthefirstFridayofeachmonthisdevotedtoadiscussionofmorbidityandmortalityoccurringatourthreeteachinghospitalsduringthepriormonth.Onlymedicalprofessionalsandtraineesareallowedtoattend.Neuro-OncologyTumorBoard:Thisisamulti-disciplinaryconferenceofNeurosurgery,Neuro-Oncology,andNeuropathology.Intheconference,braintumorcasesofthepriorweekarepresented,imagingstudiesarereviewed,andmanagementstrategiesareplanned.PediatricNeurosurgeryCaseConference:Thisconference,whichtakesplaceoverlunch,isledbyDr.JeffreyWisoff,andDr.DavidHarterofPediatricNeurosurgeryandaNeuroradiologyattending.Intheconference,managementstrategiesfor

19
patientsscheduledforsurgeryintheupcomingweekarediscussedwithactiveresidentparticipation.Chair’sRounds:ThisconferenceisheldeveryFridayexceptduringthemonthsofJulyandAugust.Duringtheconference,residentspresentinterestingandproblemcasesfromBellevueHospitalandtheVeteransAffairsMedicalCentertoNeurosurgeryDepartmentChairDr.JohnGolfinosfordiscussionofimagingfindings,management,andsurgicalstrategies.
20
DidacticResidentEducationJournalClub:Recentjournalarticlesarepresentedandreviewedindepthbyaresidentandthendiscussedbyfacultyandhousestaff.Bothresidentsandfacultyattendthislateafternoonmeetingoverdinner.PGY5–residentsonresearchdelegatearticlestotheotherresidentsandfacultyforreviewanddiscussion.Studentsdoingelectiverotationsalsohaveopportunitytopresentcaseworkorresearchatthismeeting.Forreviewarticles,ananalysisofthequalityofthearticleshouldbepresentedcriticallybytheresident.Facultyinattendancewilljudgeboththequalityofthechoiceofarticle,theanalysisandpresentation.JournalClubmeetsonamonthlybasis.ResidentCadaverDissectionCourse–occuratleasttwotothreetimesayearandcoverareasofsub-specialtyoranatomicalinterest.TheyaretypicallyonFridays,aftermorningconferencesandrunfortheentireday.Thesecoursesaredesignedandcoordinatedbysenior/servicechiefandchiefresidentswithinputfromtheotherhousestaff.Summerlectures–occurthroughoutthemonthsofJulyandAugustweeklyonFridaysat12pm.Lecturetopicsarechosenbyfacultymembersandareaofspecialty.
AdditionalEducationalResourcesSANSCourseThemeTextSubscriptionBookandConferenceAllowanceMeetingstopresenttoAttributeNeurosurgeryBootCampWoodsHole(RUNN)iDevelopLearningModules
21
Goals&Objectives–OverallOverallProgramGoals,Objectives,andGraduationRequirementsTheoverallgoaloftheresidencyprogramistodevelopinourgraduatingresidentsaproficiencylevelappropriateforanewandindependentpractitionerinthesixcorecompetenciesasoutlinedbytheACGME.WefollowthestandardsputforthbytheNeurosurgeryRRCoftheACGMEinthemilestonesproject.GraduationisconsistentwithattainmentofaLevel4acrossallofthesemilestones.TheseguidelinescanbeseenatACGMEMilestonesProject.Themilestonesreflect:
•Patientcarethatiscompassionate,appropriate,andeffectiveforthetreatmentofhealthproblemsandthepromotionofhealth.•Medicalknowledgeabouttheestablishedandevolvingbiomedical,clinicalandcognatesciencesandtheapplicationofthisknowledgetopatientcare.•Practicebasedlearningandimprovement,whichinvolvesinvestigationandevaluationofpatientcare,theappraisalandassimilationofscientificevidence,followedbyimprovementinpatientcare.•Interpersonalandcommunicationskillsresultingineffectiveinformationexchangewithpatients,theirfamilies,andotherhealthprofessionals.•Professionalismmanifestedthroughacommitmenttocarryoutprofessionalresponsibilities,adherencetoethicalprinciples,andsensitivitytoadiversepatientpopulation.•Systems-basedpracticeasmanifestedbyactionsthatdemonstrateanawarenessofandresponsivenesstothelargercontextinsystemsofhealthcareandtheabilitytoeffectivelymobilizesystemresourcestoprovidecarethatisofoptimumvalue.
Eachrotationisdesignedwiththeseoverallgoalsinmind.Inordertodirectprogress,goalsandobjectiveshavebeenformulatedforeachrotationandapprovedbythePEC(ProgramEvaluationCommittee).Uniqueaspectsofeachrotationareoutlinedinthishandbook,andthespecificgoalsandobjectivesforeachrotationaredelineatedintheappendix.Assessmenttoolsaredesignedtodemonstrateprogresstowardstheseobjectivesbydirectlymappingtothemilestonesrequirementsusingacommonformat.
22
Goals&Objectives–BySite,RotationANDClinicalyearProgressiveResponsibilityOfResidentsInEachYearAndInEachRotation
NeurosurgeryPGY-1-(ResidentsrotateasNeurosurgeryInterns)ThegoaloftheneurosurgeryinternshipatNewYorkUniversityistoprovideresidentswithanin-depthfoundationintheprinciplesandpracticeofneurosurgeryandintheclinicalneurosciencesthatareoffundamentalimportancetoneurosurgery.ResidentswhohavematchedinNeurologicalSurgeryintheNewYorkUniversityprogramarerequiredtoparticipateinaneurosurgicalinternshipatNewYorkUniversity.Thisinternshipyearconsistsofrotationsunderthedirectionoftheneurologicalsurgery-trainingprograminneuroradiology,clinicalneurosurgeryandneurology.Inaddition,residentsrotateinandgainadditionalexperienceinadultgeneralsurgery,ICU/Criticalcare,andtraumasurgeryallwithmajorcriticalcareexperienceaspartoftheinternshipexperience.BytheendoftheinternshipyearthePGY-1residentshouldmasterthefollowing:
1. PatientCarea. Performanddocumentahistoryandphysicalexaminationinatimely
mannerb. Generateadifferentialdiagnosisc. Presentsynthesizedandcoherentclinicalinformationtomoresenior
membersofthemedicalteamd. Learntoprioritizeclinicalcaree. Recognizewhenmoreseniorhelpisneededandreadilyaskfor
assistancef. Interactwithpatientsandfamiliesg. Becomefamiliarandcomfortablewithoperatingroomenvironmenth. Learntoperformathoroughneurologicalexami. Becomecompetentwithbasicprocedures/skills
2. MedicalKnowledge
a. Expandknowledgeoffundamentalsofneurologyi. Specificreadingsii. DepartmentofNeurologydidacticlectureseries
b. Expandknowledgeoffundamentalsofneuroradiologyi. Specificreadingsii. Neuroradiologylecture/conferences
c. Expandknowledgeoffundamentalsofneuro-ophthalmologyi. Specificreadings
d. Expandknowledgeoffundamentalsofneuropathologyi. Specificreadingsii. Neuropathologylecture/conferences
e. Expandknowledgeoffundamentalsofneuroanatomyandneurophysiology
i. Specificreadings
23
ii. Caseconferencesf. Expandknowledgeoffundamentalsofcriticalcare
i. Specificreadingsii. Recognizemedicalemergenciesiii. Basicventilatormanagementiv. Invasivemonitoring
3. Practice-basedLearningandImprovement
a. Developabilitytolearnfromerrorsb. Learntoapplyknowledgebasetopatientmanagement
4. InterpersonalandCommunicationSkillsa. Learntobeaproductivememberofsurgicalserviceb. Understandhierarchyofmedicalpersonnelandchainofcommandc. Developgoodrecordkeepingskillsandhabitsd. Presentcomplexcasessuccinctlye. Communicateeffectivelywithpatients
5. Professionalisma. Treatotherswithrespectandsensitivityb. Acceptresponsibilityc. Demonstratereliability
6. System-basedPracticea. Developearlyawarenessofneedtopracticeinanefficientandcost-
effectivemanner
GeneralSurgeryRotations(3months)
ThegeneralsurgeryrotationsareunderthedirectionofDr.RussellBerman,ResidencyProgramDirectorfortheNewYorkUniversityDepartmentofSurgeryinclosecoordinationwiththeNeurosurgicalProgramDirector.AllneurosurgeryinternschedulesincluderotationsinTraumaCriticalCare,andTraumasurgery.Theserotationsareofgreateducationalvaluetothefutureneurosurgeon.Thegeneralsurgeryrotationsprovideeachneurosurgeryresidentwithgenerousexposuretobasicsurgicalandtraumacriticalcareskillset.Uponcompletionofthegeneralsurgeryblock,eachresidentisexpectedtohavecompletedtheGoalsandObjectivesofthespecificR1generalsurgeryrotationsasfollows:TraumaCriticalCare-RotationGoalsandObjectives
Rotation:(R1)Length:4weeks,twoseparateblocksSummary:ThemaingoalofthisrotationistoprovidetheR1Residentanorganizedexperienceto
24
enablehim/hertoacquirethebasicknowledgeandskillsintheevaluationandmanagementofpatientsintheintensivecaresetting.OBJECTIVES:Theobjectivesoftheserotationsareforresidentstodevelopknowledgeandskillsin:
1. Theperformanceofathoroughandcompletebasicevaluationincludinghistoryandphysicalexaminsurgicalcriticalcarepatients.
2. Thepreoperativeevaluationandpreparation.3. Themanagementofallpostoperativecareincludingcriticalcare
managementinhighriskpatientsandthoseundergoingextensivesurgicalproceduresrequiringsuchcare.
4. Formulationofadiagnosticandtreatmentplanforemergencyroomandinpatientconsultations.
5. Introductoryleveloperativeskills.6. Optimalpatientcare.7. Professionalandcompassionatecommunicationandinteractiveskillswith
patients,colleaguesandfamilies.8. Practice-basedlearningandimprovement.9. Systems-basedpractice.
COMPETENCYBASEDGOALS
1. PatientCareTheR1willbegintolearntoprovidepatientcarethatiscompassionate,appropriateandeffectiveforthetreatmentofhealthproblemsandthepromotionofhealth,knowledgeofacidosis/alkalosisandhowtodrawandinterpretanarterialbloodgas..Attheendoftherotation,theR1willbeknowledgeableinandbeabletoperform:
CriticalCareandManagementofShock• Differentiatetypesofshock(hemorrhagic,cardiogenic,septic,neurologic)
andinitiateappropriatetherapy• Insertcentralvenousandarterialcathetersandobtainhemodynamicdata;
interpretdataandinitiatetherapy• Recognizeclinicpresentationofapneumothoraxandinsertchesttube• Recognizetheindicationsforbloodcomponenttherapyandinitiatetherapy• Recognizeatransfusionreactionandinitiatemanagement• InstitutemeasurestopreventupperGIbleedingincriticallyillpatientsCoagulationandAnticoagulation• Choosetheappropriatetestsfordiagnosisofacoagulopathy,andhavea
workingknowledgeoffactoranalysis• ApplyeffectivepreventivemeasuresforDVTandPE• Initiateandmonitortherapeuticanticoagulationanditscomplications• Diagnoseandmanageacutedeepvenousthrombosis• Acutelymanageapatientwithasuspectedacutepulmonaryembolus,and
provideadifferentialdiagnosis
25
AppliedCardiacPhysiology• Recognizerhythmdisturbances,myocardialischemiaonEKG• Assess,formulateadifferentialdiagnosisandinitiatetherapyfor
hypotension• Knowandapplyappropriatetreatmentforsupraventriculartachycardia• Treatcongestivefailureandacutepulmonaryedema• Managehypertensioninasurgicalpatient.Understandmultidrugtherapy
andthetoxicandsideeffectsofantihypertensivedrugs.AppliedRenalPhysiology• Knowthepathophysiologyofthedevelopmentofacuterenalfailure;the
differentiationofprerenal,renalobstructivetypesofrenalfailure;andthegeneralconceptsofpreventionandtreatmentofARF
• Recognizeandtreatsimpleelectrolytedisturbances• UnderstandappropriatefluidreplacementandbalanceAppliedPulmonaryPhysiology• Knowthemanifestations–clinicalandbylaboratorytesting–of
obstructivepulmonarydiseaseandpulmonaryinsufficiency,andtheirsurgicalperioperativemanagement
• Recognizebronchoconstrictivedisordersandtheirperioperativemanagement
AppliedNutrition
• Learntomanagethenutritionalneedsofacriticallyillpatient• PlacementofnasogastrictubeandDobhofffeedingtube
SurgicalSkills
• DevelopsurgicalskillsinCPR,CVCplacement,arterialcatheterplacement,andchesttubeplacement
• Performfirstassistantinbedsidebronchoscopy,pulmonarylavage,andtracheotomy
• Obtainoropharyngealcontrolofairway,provideAmbuventilationandperformorotrachealintubation
2. MedicalKnowledge
TheR1willbegintodemonstrateknowledgeofestablishedandevolvingbiomedical,clinical,epidemiologicalandsocial-behavioralsciences,acidoses/alkalosisstatesandabginterpretation,aswellastheapplicationofthisknowledgetopatientcare.Attheendoftherotation,theR1willbeknowledgeablein:• Understandandutilizebasicprinciplesofmechanicalventilation• Recognizeclinicpresentationofapneumothorax• Recognizetheindicationsforbloodcomponenttherapyandinitiatetherapy• Recognizeatransfusionreactionandinitiatemanagement• Recognizerhythmdisturbances,myocardialischemiaonEKG
26
• Assess,formulateadifferentialdiagnosisandinitiatetherapyforhypotension• Knowandapplyappropriatetreatmentforsupraventriculartachycardia• Knowthepathophysiologyofthedevelopmentofacuterenalfailure;the
differentiationofprerenal,renalobstructivetypesofrenalfailure;andthegeneralconceptsofpreventionandtreatmentofARF
• Knowthemanifestations–clinicalandbylaboratorytesting–ofobstructivepulmonarydiseaseandpulmonaryinsufficiency,andtheirsurgicalperioperativemanagement
• Recognizeandtreatsimpleelectrolytedisturbances• Pathology• Currentliterature
3. Practice-BasedLearningandImprovement
TheR1willbegintoattaintheabilitytoinvestigateandevaluatehis/hercareofpatients,toappraiseandassimilatescientificevidenceandtocontinuouslyimprovepatientcare.R1residentswill:1. Self-monitortoidentifystrengthsandweaknessesandsetgoalsforlearning2. Incorporatefeedbackfrompeers,faculty,patientsandancillarystaffforself-
improvement3. Useinformationtechnologyinpatientcare4. Analyzepracticeandimplementimprovements
4. InterpersonalandCommunicationSkills
R1residentsmustbegintodemonstrateinterpersonalandcommunicationskillsthatfacilitatetheflowofinformationbetweenpatients,theirfamiliesandhealthprofessionals.R1residentswill:1. Communicateeffectivelywithpatientsandfamiliesacrossallsocioeconomic
andculturalbackgrounds2. Communicateeffectivelywithphysicians,otherhealthprofessionalsandhealth
agencies3. Workeffectivelyinahealthcareteam4. Actasaconsultant5. Maintaincomprehensive,timelyandlegiblemedicalrecords
5. Professionalism
TheR1residentwillbegintodemonstrateacommitmenttocarryingoutprofessionalresponsibilitiesandanadherencetoethicalprinciplesbyshowing:1. Compassion,integrityandrespecttoothersnotwithstandingrace,religion,
age,genderordisabilities2. Responsivenesstopatentneedsthatsupersedesself-interestandrespectsthe
patient’sprivacyandautonomy3. Accountabilitytopatients,societyandtheprofession
6. Systems-BasedPracticeTheR1residentmustbegintodemonstrateanawarenessofandresponsivenesstothelargercontextandsystemofhealthcarebyhavingtheabilitytocalluponappropriateresourcesinthesystemtooptimizehealthcare.Theresidentwill:
27
1. Workeffectivelyinvarioussettingsandsystems2. Coordinatepatientcarewithinthehealthcaresystemconsideringcostsand
risk-benefitanalysis3. Advocateforqualitycarewithininterprofessionalteamstoenhancesafety
andimprovequality4. Identifysystemerrorsandformulatesolutions5. Befamiliarwithethical,socioeconomicandmedicallegalissues6. Interactwithsocialworkers,atattendsocialworkmeetingstolearnwhere
patientsneedtogoandhowtogetthemthere
TraumaSurgery-RotationGoalsandObjectivesSummary:The overall goal of rotations on the Bellevue Hospital trauma service is to attain athorough understanding of the pathophysiology of injury; to gain knowledge andexperience in all phases of care of the trauma patient including resuscitation,operativejudgmentandtechnique,criticalcare,andrehabilitation.
Rotation:BellevueHospital(R1)Length:4weeksOBJECTIVES:Theobjectivesofthisrotationaretoforresidentstodevelopknowledgeandskillsin:
1. Participateasamemberofthesurgicalandemergencymedicineteamintheinitialresuscitationoftheinjuredpatientandinthesubsequentmanagementofthetraumapatientduringtheoperativeandpost-operativephases.
2. Attainproficiencyindiagnosticandtherapeuticprocedures.3. Formulationofadiagnosticandtreatmentplanforemergencyroomand
inpatientconsultations.4. Provideoptimalpatientcare.5. Professionalandcompassionatecommunicationandinteractiveskillswith
patients,colleaguesandfamilies.6. Practice-basedlearningandimprovement.7. Systems-basedpractice,particularlywithintheprivatehospitalsetting.
COMPETENCY-BASEDGOALSMedicalKnowledgeAtthecompletionoftheserotationsresidentsshould:
1. Understandemergencyairwaymanagementincludingendotrachealintubation,peripheralandcentralvenousaccess,Swan-Ganzcatheterinsertion,closedtubethoracotomy,diagnosticperitoneallavage,woundmanagement,andperformanceoftraumaultrasonography(FAST).
2. Manageresponsibilitiessuchaswoundcare,nutritionalandfluidmanagementandchartdocumentation.
3. Knowledgeofpost-injurycare.4. Beabletointerpretradiographicfindings,EKGs.
28
5. Learnthefundamentalstepsofoperativemanagementoftrauma.Skills:R1shouldbeabletohavethebelowspecificskillsattheendofthisrotation:
1. Understandtheprinciplesandlimitationsoftheultrasound(FAST)anddiagnosticperitoneallavage.
2. Beabletoinitiatemaneuverstopreventhypothermiaintheinjuredpatient.3. Performbasicwoundmanagement,simplesuturerepair,compressionand
antibioticprophylaxis.4. Interpretbloodgasesandunderstandtheimportanceofbasedeficit.
PatientCareAtthecompletionoftheserotationsresidentsshould:
1. Haveanunderstandingofandbeabletodelivercompassionatecaretopediatricpatients.
2. Gainexperienceindeliveringinformationtopatients’familymemberswhenappropriate,particularinthepediatricpopulation.
3. Beabletouseknowledgeandskillslearnedtoenhancecareofpatients.Practice-BasedLearningandImprovementAtthecompletionoftheserotationsresidentsshould:
• Havegainedinsightintohowtolocateinformationrelevanttoaparticularpatient’sclinicalsituationandbeabletoapplythatinformationtopatientcare.
• Haveaworkingknowledgeofhowtoaccessscientificinformationrelevanttoaparticularpatientandbeabletoassimilatethatinformationandapplytoitpatientcare.
• Beadeptatusingtheavailabletechnologytoaccesspatientinformation.InterpersonalandCommunicationSkillsAtthecompletionoftheserotationsresidentsshould:
• Understandtheimportanceofeffectivecommunicationtopatients,ancillarystaffandcolleagues.
• Developskillstocommunicatemedicalinformationtoparentsandfamilymembersofapediatricpatient.
• Developskillstocommunicatewithco-workersandcolleaguestoallowforoptimumpatientcare.
ProfessionalismAtthecompletionoftheserotationsresidentsshould:• Understandtheimportanceofathroughcommitmenttocarryingoutprofessional
responsibilities.• Demonstrateadherencetoethicalprincipals.• Showsensitivitytodiversepatientpopulations.
System-BasedPracticeAtthecompletionoftheserotationsresidentsshould:
29
A. Understandtheimportanceofworkingeffectivelyinthehealthcaredelivery,particularlyintheprivatehospitalsetting.
B. Understandtheimportanceofcoordinationofpatientcarewithinthehealthcaresystemanddemonstrateaworkingknowledgeofthis.
Neurology,Neuroradiology,Neuropathology,NeurosurgeryTheneurologicrotationsareunderthedirectionofDr.SaranJonas,ChiefoftheNeurologyServiceatBellevueHospital,Drs.AjaxGeorgeseniorneuroradiologistattheNewYorkUniversityDivisionofNeuroradiologyandWendyHotsonChiefoftheNeuroradiologyServiceatBellevueHospital,Dr.ZagZag,DirectorofNeuropathologyfortheNewYorkUniversityDivisionofNeuropathology,Dr.PeterKimNelson,DirectorofInterventionalNeuroradiologyandDr.PaulHuang,ChiefoftheNeurosurgeryServiceatBellevueHospitalinclosecoordinationwithDr.HowardRiina,NeurosurgicalProgramDirector.Theserotationsprovidetheneurosurgeryinternswithanindepthexposuretobasicneurologicaldiagnosisandpatientcare.Theygainexperiencewithawiderangeofneurologicaldisorders,includingcerebrovasculardisease,neurodegenerativeconditions,epilepsy,movementdisorders,neuromusculardisorders,providesexposuretoelectroencephalography,electromyography,basicsofneuropathology,andneurotrauma.GoalsandobjectivesspecifictotheNeurologyrotationinclude:Uponcompletionofthe2-monthneurologyblock,eachresidentisexpectedtohavecompletedtheGoalsandObjectivesoftheneurologyrotationsasfollows:
1. Understandingthecausalmechanismsofawidevarietyofadultneurologicaldiseases
2. Managementofacuteandchronicneurologicdiseases3. Comprehensiveexposuretooutpatientmanagementofpatientswith
neurologicaldisease4. Introductiontopediatricneurology5. Interpretationofelectroencephalograms(EEGs),electromyograms(EMGs),
andnerveconductionandotherelectrophysiologicalstudies6. Interpretationofcerebrospinalfluid(CSF),LPsandserologicaltestsfor
neurologicalconditions7. Introductiontonerveandmusclebiopsiesandtheirinterpretationinthe
diagnosisofcomplexneuropathiesandmyopathies8. Refinementofneurologicalexaminationandhistory-takingskills9. Acquireabasicunderstandingoftheneuropathologythatunderlies
neurologicaldisease10. Exposuretoneurologicresearchtopics
Neuroradiology/InterventionalNeuroradiologyNeuroradiology/InterventionalNeuroradiology(1month):Thisrotationprovidesanoutstandingdidacticexperienceinafieldthatisessentialto
30
thepracticeofneurosurgery.Residentsworkcloselywiththemembersoftheinterventionalneuroradiologyfaculty.TheneurosurgeryresidentmeetstheNYUinterventioalneuroradiologyfacultyintheINRsuiteeachmorningtoparticipateinallintervnetionalNeuroradiologyproceduresastheyoccurduringtheday.Theresidentwillobserveandparticipateintheperformanceofcerebralangiogramsandembolizationprocedureswiththeinterventionalneuroradiologyfaculty.Theresidentisalsorequiredtocompleteassignedreadingsininterventionalneuroradiologythatwillgreatlyenhancethisexperience.GoalsandobjectivesNeuroradiologyrotation:
1. Understandthefundamentalprinciplesofcurrentneuroradiologicalimaging
techniquesincludingMRI,CT,PET,functionalMRI,MRperfusion,CTangiography,CTperfusionanddigitalsubtractionangiography
2. Understandtheappropriate,efficient,andcosteffectiveuseofimagingstudies3. BecomeadeptinbasicinterpretationofneuroradiologicalstudiesincludingCT,
MRI,MRA,CTA,MRP,CTPanddigitalsubtractionangiography4. Understandtheroleofinterventionalneuroradiologyindiagnosisand
treatmentofneurologicaldisease,includingendovascularmanagementofneurovascularproblems
5. Becomefamiliarwiththerelationshipbetweenimagingstudiesandneuropathologicalmaterial
NeuropathologyNeuropathology(1month):Thisrotationprovidesanoutstandingdidacticexperienceinafieldthatisessentialtothepracticeofneurosurgery.Residentsworkcloselywiththemembersoftheneuropathologyfaculty.TheneurosurgeryresidentmeetstheNYUneuropathologyfacultyinthereadingroomeachmorningtoparticipateinthereadingofallneuropathologyspecimensobtainedduringthepreviousdayandastheyoccurduringthedayincludingpreparingandreadingfrozenspecimens.Theresidentwillobserveandparticipateintheinterpretationofallpathologicspecimenwiththeneuropathologyfaculty.TheresidentisalsorequiredtocompleteassignedreadingsinneuropathologyandattendadultandpediatricTumorboardthatwillgreatlyenhancethisexperience.GoalsandobjectivesNeuropathologyrotation:
A. UnderstandpracticalapplicationofneuropathologytoclinicalpracticeB. Understandthefundamentalprinciplesofcurrentneuropathologicalstaining
techniquesC. Understandtheappropriate,efficient,andcosteffectiveuseofathology
modalitiesincludingEMandspecialstainsD. BecomeadeptinbasicinterpretationofneuropathologicalslidesE. Understandtheroleofneuropathologyinthediagnosis,treatmentand
prognosisofneurologicaldisease
31
F. Becomefamiliarwiththerelationshipbetweenimagingstudiesandneuropathologicalmaterial
G. ExpandknowledgeoffundamentalsofneuroanatomyandneurophysiologyH. Acquireabasicunderstandingoftheneuropathologythatunderlies
neurologicaldiseaseI. Gainexposuretoneurologicresearchtopics
NeurosurgeryNeurosurgery(2monthsBellevueHospital,1monthTischHospital):Thethree-monthNeurosurgeryrotationallowsthenewresidentstobecomefamiliarwiththeday-to-dayoperationoftheNYUneurosurgicalservicethusallowingthemtogaininsightintowhatwillberequiredofthemastheyprogressthroughtheneurosurgicalresidency.TheinternwillobserveandparticipateintheneurosurgicalcaseswiththechiefresidentandtheNeurosurgicalfacultyatbothTischandBellevueHospitals.TheywillalsobeintroducedtooutpatientneurosurgerybyattendingandparticipatingintheneurosurgeryclinicatBellevueHospital.ThePGY2’salsocovertheVAclinicoccasionally.TheresidentisalsorequiredtoattendtheSNS(SocietyofNeurologicalSurgery)basicneurosurgicalskillsresidentbootcamp,completeassignedreadingsinneurosurgeryandattendallneurosurgerydidacticconferences.GoalsandobjectivesofinternNeurosurgeryrotation:
o Performanddocumentahistoryandphysicalexaminationinatimelymannero Generateadifferentialdiagnosiso Presentsynthesizedandcoherentclinicalinformationtomoreseniormembersofthe
medicalteamo Learntoprioritizeclinicalcareo Recognizewhenmoreseniorhelpisneededandreadilyaskforassistanceo Interactwithpatientsandfamilieso Becomefamiliarandcomfortablewithoperatingroomenvironmento Learntoperformathoroughneurologicalexamo Becomefamiliarwithneurosurgicalstandardofcareanditsscientificunderpinningso Becomecompetentwithbasicprocedures/skills
o InvasiveICPmonitoringo ShuntTapso LumbarPunctures
o Recognizeneurosurgicalemergencieso
NeurosurgeryPGY-2-(ResidentsrotateasJuniorResidentsatBellevueHospital
Center)• Neurosurgery R1 residents must have successfully completed an accredited
NeurosurgeryinternshipatNYUinaccordancewithNeurosurgeryRRCguidelines.They must demonstrate competence in all of the general medical and surgicalprinciples of patient care, medical knowledge, interpersonal & communicationskills, and professionalism at each stage throughout the training program. They
32
mustalsodemonstrateknowledgeofpoliciespertaining topatientrights,HIPPA,appropriate use of restraints and seclusion, recognizing fatigue, recognizingphysician impairment, and those pertaining to patient safety, all in accordancewith Bellevue Hospital Center policy and similar policies at Tisch Hospital,including completion of corresponding modules in the idevelop system. Theresidency program provides graduated levels of responsibility in patientevaluation, neurological disease management and neurological surgery, asresidentsrotatethroughthevariousneurosurgicalservicesatthemedicalcenter.Junior level residents work directly with the Neurosurgical Faculty and chiefresidents at Bellevue Hospital Center and Tisch Hospitals neurosurgical traumaandelectiveservices.Duringtheserotationstheresidentsassumemoreandmoredirect responsibility and surgical opportunities in the care of patients. Surgicaltechniques are learned and standards of care adopted. By the end of the PGY 2Neurosurgeryyeartheresidentshouldmasterthefollowing:
PATIENTCARE:• Theresidentswilllearnhowtotakeaneurologicalhistory,performaneurological
examinationandderiveadifferentialdiagnosis• Residentswilllearntorapidlyidentifypotentialsurgicalriskspreoperativelyand
learnmethodstominimizethoserisks.• With appropriate supervision, residents will learn to competently perform the
followingprocedures:Procedures
HistoryPhysicalNeurologicalExaminationInsertionnasogastrictubeLumbarpunctureArterialpunctureInsertionIVlinesRemovalofsuturesInsertionofFoleycatheterEKGIncision/drainageofsuperficialabscessSuturingoflacerationsWounddebridementDressingchangesInsertioncentralvenouscatheterInsertionSwan-GanzEmergencytracheotomyAspirateshuntreservoirInsertionlumbarsubarachnoidcatheterTwistdrillcraniotomyforICPmonitorBurrholefortraumaBurrhole/twistdrillventriculostomyTwistdrillforSEPSdrainageofsubduralhematomasApplication/insertioncervicaltraction
33
Suturesimplelacerationscalp/backSuturecomplexlacerationscalp/backOpeningandclosurecraniotomyincisionsExternalizeshunts
MEDICALKNOWLEDGE:• Theresidentswilllearntheneurodiagnosticstudiesavailablefortheevaluationof
patients. They will learn the importance of correlative neuroanatomy ininterpretingthesestudies.
• Theresidentswilllearn:o Theanatomyofthebrain,spine,peripheralnervesandthebonycoverings
ofeach.o Thephysiologyofnormalbrainandnormalvasculature.
• The residents will develop competence in the interpretation of neurodiagnosticexaminations in disease states. These include: conventional radiographs, cranialandspinalcomputedtomography,cranialandspinalmagneticresonanceimaging,MRangiography,CTangiographyandvenograms,cerebralandspinalangiography.
• They will learn critical interpretation and correlation of clinical andneurodiagnostic (imaging) examinations based on a sound knowledge ofneurologyandneuropathology.Theywilldiscuss:
• Thedefinitionofmild,moderate, and severebrain injuryand identify theindividualcomponentsandscoresoftheGlasgowComaScaleandGlasgowOutcomeScale.
• Theclinicalandradiologicpathwaysforclearanceofthespine• The difference between complete and incomplete spinal injury and
demonstrate the ability to accurately complete detailedASIA grading andcategoryassignment,andtheprognosisofneurologicrecoveryforeach.
• Themajorpatternsofspinalinjury(complete,centralcord,Brown-Sequard,cauda equina, etc). Whatmechanisms of injury and spinal column injuryare most commonly associated with each? What is the prognosis forrecoveryforeach?
• Thepathophysiologyofcraniocervicalinjuriesinadults.• Thepathophysiologyofsub-axialspinalcolumnandspinalcordinjuriesin
adults.• Fundamentalmanagementofpatientswithheadinjuries,including
intracranialpressure(ICP)monitoring• Stabilizationandmanagementoftraumatothespine,andspinalcordinjury• FundamentalICUcare,particularlyformultisystem-injuredpatients• FundamentalERcareofacuteneurologicalinjuries,includingbluntand
penetratinginjuriesandsubarachnoidhemorrhage• Outpatientmanagementofnewandfollow-uppatients• Exposuretopediatricneurosurgicalmanagementwhileoncall
• Residents will discuss the indications and potential complications for allneurosurgicalprocedures.Thiswillbeacquiredfromdiscussionswithfaculty,byparticipating in conferences and by reading textbooks and the correspondingliterature.These skillswill be evaluated indidactic case conferences, in residentevaluationsandinthemilestonecommitteemeetings.
34
• They will learn how to write appropriate admission and medication orders forward,ICU,andpost-operativepatients.
• TheywilldiscussspecificJCAHOhospitalsafetyregulations.• Theywill discuss the importance of timely and accuratemedical record keeping
includingmedicationreconciliation.• Knowledge of general medicine and surgical principles as well as the
pathophysiology of neurosurgical diseases will be acquired with experience,readingandobservationof thepracticehabitsofseniorneurosurgeonsandnon-surgicalconsultants,andindidacticcaseconferences.
INTERPERSONALCOMMUNICATIONSKILLS:• They will learn how to communicate the pertinent positives and negatives of a
generalmedical and neurological examination to senior residents, neurosurgicalattendings,andconsultingphysiciansinanaccurateandtimelyfashion.
• They will learn how to communicate critical interpretation and correlation ofclinicalandneurodiagnostic(imaging)examinationsbasedonasoundknowledgeof neurology and neuropathology to senior residents, neurosurgical attendings,andconsultingphysiciansinanaccurateandtimelyfashion.
• They will learn to be competent in communicating with team members in thehand-overprocessinordertominimizeerrorsduringtransitionsofcare.
• Theywilllearntocommunicateclearlyandpromptlywiththenursingandsupportstaffinordertoobtainthebestpatientcare.
• They will learn to communicate patient information, care plans, and prognosiseffectivelyandcompassionatelywithpatientsandtheirfamilies.
• TheywillalsolearntopresentinweeklydidacticcaseconferencesandatJournalClub.
SYSTEMSBASEDPACTICE:• Residentswill learn thatpatientcare isa teameffortwhereeachmemberof the
team is equally important in attaining satisfactory patient outcomes. The teamincludes all members of the healthcare delivery system including: floor nurses,nurse practitioners, operating room personnel, social workers, case managers,rehabilitation specialists, consultants and house staff from other services, otherneurosurgicalresidentsandmedicalstudentsandconsultantneurosurgeons.
• Theywilllearntocoordinateandmanagecommunicationbetweenservicesonco-managedpatients.
• Theywill interact and coordinate the longitudinal care of neurosurgical patientsthrough discussions with Neurosurgical NP’s, Physician Assistants, Physiatrists,PhysicalTherapists,SocialWorkers,andDischargePlanningnurses.
• Theywilldiscusstheregulatoryissuesinvolvedinreportingbraindeathandnon-accidentalneurologicinjury(especiallyinthepediatricpopulation).
PRACTICE-BASEDLEARNING:• The resident will learn to analyze his or her own practice for needed
improvements.• Theywillalsolearntouseevidencefromscientificstudiestoguidetheirmedical
decision-making.
35
• Theywilldiscusstheapplicationofresearchandstatisticalmethods.• They will participate in clinical research projects, where appropriate, including
participatingintheIRBandconsentprocess.• ResidentswillattendtheWood’sHoleNeurosurgicalResearchCourse.PROFESSIONALISM:• Trainees will learn constructive collegiality with faculty, their fellow residents,
consultants andhouse staff fromother specialties and services, andwithnursesandparamedicalpersonnel.
• Residentswilllearnhowtodealwithpatientsandfamiliesinacompassionateandhumanisticway.
• Maintain professional rapport and comportment with patient families, nurses,otherphysicianteamsandotherhospitalpersonnel.
• Demonstraterespectforpatientsandcolleaguesfromdiversecultural,ethnicandreligiousbackgrounds.
• Demonstratehonestyinallprofessionalinteractions.• Residentswillmaintaintimelyandaccuratemedicalrecords.• Residentswillalso:
o Attendallrequiredconferencesinatimelyfashion.o Pre-roundonICUpatientsandpresenttimely,accuratedatatotheteam.o Participate in discussion of ethical dilemmas related to care delivery,
consent,andlifesupportinseverelyinjuredpatients.o ProvideconsultationtotheEDandotherservicesintimelyfashion.o Demonstrate dress, grooming and behavior consistent with institutional
anddepartmentalguidelines.o Comply with all GME and Departmental regulations regarding duty hour
restrictionsandreportpersonalscheduleintimelyandaccuratefashion.o Appear for duty appropriately rested and fit to provide the services
requiredbytheirpatients.o Accurately self-report fatigue in situations that may compromise safety
and/orpatientcare.o Mustbecommittedtoandresponsibleforpromotingpatientsafety.o Must demonstrate responsiveness to patient needs that supersedes self-
interest.o Must recognize thatundercertaincircumstances, thebest interestsof the
patient may be served by transitioning that patient’s care to anotherqualifiedandrestedprovider.
METHODSOFEVALUATION:• Resident fundofmedical knowledgewill be evaluated annually beginning in the
PGY2yearbysittingforthewrittenportionoftheABNSprimaryexamination.o They are required to obtain a passing grade on this examination prior to
completing their PGY6 year of residency training, andprior to becomingchiefresident.
o They are also expected to improve their percentile performance on theABNSprimaryexaminationeachyear.
36
• Resident will also attend weekly didactic conferences and the monthly JournalClub.
• Conferenceattendanceandparticipationwillbereviewedanddiscussedwiththeresident. They are required to attend at least 75% of all mandatory residentconferences.
• The senior residents who report directly to the attending surgeons will alsoevaluatethejuniorresidents.
• TheNeurosurgeryAttendingStaffreviewsResidentMedicalDocumentation.• Resident academic productivity regarding published abstracts, meeting
presentations,andpublishedmanuscripts,awards,etc.arealsoreviewed.• Residentsarerequiredtopublish2articleseachyear.Thiscanbeintheformofa
peerreviewedarticle,abookchapter,peerreviewbasicscienceresearchpaperorpublishededitorial.
• The resident will also be evaluated on their attainment of these goals andobjectives as well as on their performance in conferences on a biannual basisthroughwritten evaluation of all 6 competencies (see resident evaluations) andverbalfeedbackfromtheChairmanandProgramDirector.
• Facultymembers,aseniorresident(asisappropriate),andtheNeurosurgicalNP’sevaluate all residents after each rotation and during milestone evaluationmeetings. They are evaluated on all 6 competencies (see resident evaluations).Theirattendanceandperformanceindidacticteachingconferencesandtheircaselogs are also reviewed. The Chairman and Program Director review theseevaluations and give verbal andwritten feedback to the residents on a biannualbasis.
• Residents are promoted each year based on demonstration of competentperformanceofallmilestonerequirementsasoutlinedabove.
NeurosurgeryPGY-2-(ResidentsrotateasJuniorResidentsonTischteams1&2)• Neurosurgery PGY-2 residents must have successfully completed an accredited
PGY-1yearneurosurgicalinternship.Theymustdemonstratecompetenceinallofthe general medical and surgical principles of patient care, medical knowledge,interpersonal & communication skills, and professionalism at each stagethroughout the training program. They must also demonstrate knowledge ofpatientrights,includingHIPPAandtheappropriateuseofrestraintsandseclusion.Residentphysiciansarepermittedtoconductface-to-faceevaluationofpatientsinrestraintsorseclusionandtoorderpatientrestraintsandseclusioninaccordancewithNewYorkUniversityHospitalsCenterPolicyonRestraintsandSeclusion.Theresidency program provides graduated levels of responsibility in patientevaluation, management and surgery as residents rotate through the variousneurosurgical services in the medical center. Junior and intermediate levelresidentsworkwithmasterneurosurgeonsontwodistinctadultservicesatTischHospital: (Tumor/Vascular/Skull Base/Functional/Epilepsy Service)(Spinal/Peripheral Services). They also rotate through the Pediatric/PediatricEpilepsy services at TischHospital. During these rotations the residents assumemore and more direct responsibility and surgical opportunities in the carepatients. Surgical techniques are learned and standards of care adopted. In
37
addition to mastering the procedures outlined below, by the end of the PGY 2Neurosurgeryyeartheresidentshouldbeabletomasterthefollowing:
PATIENTCARE:• Theresidentswilllearnhowtotakeaneurologicalhistory,performaneurological
examinationandderiveadifferentialdiagnosis• Residentswilllearntorapidlyidentifypotentialsurgicalriskspreoperativelyand
discussmethodstominimizethoserisks.• With appropriate supervision, residents will learn to competently perform the
followingprocedures:Procedures
HistoryPhysicalNeurologicalExaminationInsertionnasogastrictubeLumbarpunctureArterialpunctureInsertionIVlinesRemovalofsuturesInsertionofFoleycatheterEKGIncision/drainageofsuperficialabscessSuturingoflacerationsWounddebridementDressingchangesInsertioncentralvenouscatheterInsertionSwan-GanzEmergencytracheotomyAspirateshuntreservoirInsertionlumbarsubarachnoidcatheterTwistdrillcraniostomyforICPmonitorBurrholefortraumaBurrhole/twistdrillventriculostomyTwistdrillforSEPSdrainageofsubduralhematomasApplication/insertioncervicaltractionSuturesimplelacerationscalp/backSuturecomplexlacerationscalp/backOpenandclosurecraniotomyincisionsExternalizeshunts
MEDICALKNOWLEDGE:• The residents will learn neurodiagnostic studies available for the evaluation of
patients. They will learn the importance of correlative neuroanatomy ininterpretingthesestudies
• Theresidentswilldiscuss:o Theanatomyofthebrain,spine,peripheralnervesandthebonycoverings
ofeach.
38
o Thephysiologyofnormalbrainandnormalvasculature.• The residents will develop competence in the interpretation of neurodiagnostic
examinations in disease states. These include: conventional radiographs, carotidultrasonography, cranial and spinal computed tomography, cranial and spinalmagnetic resonance imaging, MR angiography, CT angiography and venograms,cerebralandspinalangiography.
• They will learn critical interpretation and correlation of clinical andneurodiagnostic (imaging) examinations based on a sound knowledge ofneurologyandneuropathology.Theywilldiscuss:
o Thedefinitionofmild,moderate, and severebrain injuryand identify theindividualcomponentsandscoresoftheGlasgowComaScaleandGlasgowOutcomeScale.
o Theclinicalandradiologicpathwaysforclearanceofthespineo The difference between complete and incomplete spinal injury and
demonstrate the ability to accurately complete detailedASIA grading andcategoryassignment,andtheprognosisofneurologicrecoveryforeach.
o Themajorpatternsofspinalinjury(complete,centralcord,Brown-Sequard,cauda equina, etc). Whatmechanisms of injury and spinal column injuryare most commonly associated with each? What is the prognosis forrecoveryforeach?
o Thepathophysiologyofcraniocervicalinjuriesinadults.o Thepathophysiologyofsub-axialspinalcolumnandspinalcordinjuriesin
adults.• Residents will discuss the indications and potential complications for all
neurosurgicalprocedures.Thiswillbeacquiredfromdiscussionswithfacultyandby reading textbooksand the literature. Itwill alsobeevaluated indidactic caseconferences.
• They will learn how to write appropriate admission and medication orders forward,ICU,andpost-operativepatients.
• TheywilldiscussspecificJCAHOhospitalsafetyregulations.• They will learn the importance of timely and accurate medical record keeping
includingmedicationreconciliation.• Knowledge of general medicine and surgical principles as well as the
pathophysiology of neurosurgical diseases will be acquired with experience,readingandobservationof thepracticehabitsofseniorneurosurgeonsandnon-surgicalconsultants,andindidacticcaseconferences.
INTERPERSONALCOMMUNICATIONSKILLS:• They will learn how to communicate the pertinent positives and negatives of a
generalmedical and neurological examination to senior residents, neurosurgicalattendings,andconsultingphysiciansinanaccurateandtimelyfashion.
• They will learn how to communicate critical interpretation and correlation ofclinicalandneurodiagnostic(imaging)examinationsbasedonasoundknowledgeof neurology and neuropathology to senior residents, neurosurgical attendings,andconsultingphysiciansinanaccurateandtimelyfashion.
• They will learn to be competent in communicating with team members in thehand-overprocessinordertominimizeerrorsduringtransitionsofcare.
39
• Theywilllearntocommunicateclearlyandpromptlywiththenursingandsupportstaffinordertoobtainthebestpatientcare.
• They will learn to communicate patient information, care plans, and prognosiseffectivelyandcompassionatelywithpatientsandtheirfamilies.
• TheywillalsolearntopresentinweeklydidacticcaseconferencesandatJournalClub
SYSTEMSBASEDPACTICE:• Residentswill learn thatpatientcare isa teameffortwhereeachmemberof the
team is equally important in attaining satisfactory patient outcomes. The teamincludes all members of the healthcare delivery system including: floor nurses,nurse practitioners, operating room personnel, social workers, case managers,rehabilitation specialists, consultants and house staff from other services, otherneurosurgicalresidentsandmedicalstudentsandconsultantneurosurgeons.
• Theywilllearntocoordinateandmanagecommunicationbetweenservicesonco-managedpatients.
• Theywill interact and coordinate the longitudinal care of neurosurgical patientsthrough discussions with Neurosurgical NP’s, Physiatrists, Physical Therapists,SocialWorkers,andDischargePlanningnurses.
• Theywilldiscusstheregulatoryissuesinvolvedinreportingbraindeathandnon-accidentalneurologicinjury(especiallyinthepediatricpopulation).
PRACTICE-BASEDLEARNING:• The resident will learn to analyze his or her own practice for needed
improvements.• Theywillalsolearntouseevidencefromscientificstudiestoguidetheirmedical
decision-making.• Theywilldiscusstheapplicationofresearchandstatisticalmethods.• They will participate in clinical research projects where appropriate including
participatingintheIRBandconsentprocess.• ResidentswillattendtheWood’sHoleNeurosurgicalResearchCourse.PROFESSIONALISM:• Trainees will learn constructive collegiality with faculty, their fellow residents,
consultants and house staff from other specialties and services, but also withnursesandparamedicalpersonnel.
• Residentswilllearnhowtodealwithpatientsandfamiliesinacompassionateandhumanisticway.
• Maintain professional rapport and comportment with patient families, nurses,otherphysicianteamsandotherhospitalpersonnel.Demonstraterespectforpatientsandcolleaguesfromdiversecultural,ethnicandreligiousbackgrounds.
• Demonstratehonestyinallprofessionalinteractions.• Residentswillmaintaintimelyandaccuratemedicalrecords.• Residentswillalso:
o Attendallrequiredconferencesinatimelyfashion.o Participate in discussion of ethical dilemmas related to care delivery,
40
consent,andlifesupportinseverelyinjuredpatients.o ProvideconsultationtotheED(emergencydepartment)andotherservices
intimelyfashion.o Demonstrate dress, grooming and behavior consistent with institutional
anddepartmentalguidelines.o Comply with all GME and Departmental regulations regarding duty hour
restrictionsandreportpersonalscheduleintimelyandaccuratefashion.o Appear for duty appropriately rested and fit to provide the services
requiredbytheirpatients.o Accurately self-report fatigue in situations that may compromise safety
and/orpatientcare.o Mustbecommittedtoandresponsibleforpromotingpatientsafety.o Must demonstrate responsiveness to patient needs that supersedes self-
interest.o Must recognize thatundercertaincircumstances, thebest interestsof the
patient may be served by transitioning that patient’s care to anotherqualifiedandrestedprovider.
METHODSOFEVALUATION:• Resident fundofmedicalknowledgewillbeevaluatedannuallybysitting for the
writtenportionoftheABNSprimaryexamination.o Residentsarerequiredtoobtainapassinggradeonthisexaminationprior
tocompletingtheirPGY6yearofresidencytrainingandpriortobecomingchiefresident.
o They are also expected to improve their percentile performance on theABNSprimaryexaminationeachyear.
• Resident will also attend weekly didactic conferences and the monthly JournalClub.
• Conferenceattendanceandparticipationwillbereviewedanddiscussedwiththeresident. They are required to attend at least 75% of all mandatory residentconferences.
• The senior residents who report directly to the attending surgeons will alsoevaluatethejuniorresidents.
• TheNeurosurgeryAttendingStaffreviewsResidentMedicalDocumentation.• Resident academic productivity regarding published abstracts, meeting
presentations,andpublishedmanuscripts,awards,etc.arealsoreviewed• The resident will also be evaluated on their attainment of these goals and
objectives as well as on their performance in conferences on a quarterly basisthroughwritten evaluation of all 6 competencies (see resident evaluations) andverbalfeedbackfromtheChairmanandProgramDirector.
• Facultymembers,aseniorresident(asisappropriate),andtheNeurosurgicalNP’sevaluateallresidentsaftereachrotation.Theyareevaluatedonall6competencies(seeresidentevaluations).Theirattendanceandperformanceindidacticteachingconferences and their case logs are also reviewed. The Chairman and Program
41
Directorreviewtheseevaluationsandgiveverbal feedback to theresidentsonaquarterlybasis.
• Residents are promoted each year based on demonstration of competentperformanceofallrequirementsasoutlinedabove.
NeurosurgeryPGY-2-(ResidentsrotateasJuniorResidentsatNewYorkHarborHealthCareSystem)• Neurosurgery PGY2 residents must have successfully completed an accredited
neurosurgeryinternship.Theymustdemonstratecompetenceinallofthegeneralmedicalandsurgicalprinciplesofpatientcare,medicalknowledge, interpersonal&communicationskills,andprofessionalismateachstagethroughoutthetrainingprogram. They must also demonstrate knowledge of patient rights, includingHIPPAandtheappropriateuseofrestrainsandseclusion.Residentphysiciansarepermitted to conduct face-to-face evaluationofpatients in restrainsor seclusionand to order patient restraints and seclusion in accordancewithManhattan VAHospitals Center Policy on Restraints and Seclusion. The residency programprovidesgraduatedlevelsofresponsibilityinpatientevaluation,managementandsurgery as residents rotate through the various neurosurgical services in themedical center. Junior, intermediate level and senior residents work withattending neurosurgeons at the Neurosurgical Service at the Manhattan VAMedicalCenter.Duringtheserotationstheresidentsassumemoreandmoredirectresponsibilityandsurgicalopportunities inthecarepatients.Surgical techniquesare learned and standards of care adopted. In addition to mastering theprocedures outlined below, by the end of the PGY 2 Neurosurgery year theresidentshouldbeabletomasterthefollowing:
PATIENTCARE:• Theresidentswilllearnhowtotakeaneurologicalhistory,performaneurological
examinationandderiveadifferentialdiagnosis• Residentswilllearntorapidlyidentifypotentialsurgicalriskspreoperativelyand
discussmethodstominimizethoserisks.• With appropriate supervision, residents will learn to competently perform the
followingprocedures:Procedures
HistoryPhysicalNeurologicalExaminationInsertionnasogastrictubeLumbarpunctureArterialpunctureInsertionIVlinesRemovalofsuturesInsertionofFoleycatheterEKGIncision/drainageofsuperficialabscessSuturingoflacerationsWounddebridement
42
DressingchangesInsertioncentralvenouscatheterInsertionSwan-GanzEmergencytracheotomyAspirateshuntreservoirInsertionlumbarsubarachnoidcatheterTwistdrillcraniotomyforICPmonitorTwistdrillforSEPSdrainageofsubduralhematomasBurrholefortraumaBurrhole/twistdrillventriculostomyApplication/insertioncervicaltractionSuturesimplelacerationscalp/backSuturecomplexlacerationscalp/backOpenandclosurecraniotomyincisionsExternalizeshunts
MEDICALKNOWLEDGE:• Theresidentswilllearntheneurodiagnosticstudiesavailablefortheevaluationof
patients. They will discuss the importance of correlative neuroanatomy ininterpretingthesestudies
• Theresidentswilldiscuss:o Theanatomyofthebrain,spine,peripheralnervesandthebonycoverings
ofeach.o Thephysiologyofnormalbrainandnormalvasculature.
• The residents will develop competence in the interpretation of neurodiagnosticexaminations in disease states. These include: conventional radiographs, carotidultrasonography, cranial and spinal computed tomography, cranial and spinalmagnetic resonance imaging, MR angiography, CT angiography and venograms,cerebralandspinalangiography.
• They will learn critical interpretation and correlation of clinical andneurodiagnostic (imaging) examinations based on a sound knowledge ofneurologyandneuropathology.Theywilllearn:
o Thedefinitionofmild,moderate, and severebrain injuryand identify theindividualcomponentsandscoresoftheGlasgowComaScaleandGlasgowOutcomeScale.
o Theclinicalandradiologicpathwaysforclearanceofthespineo The difference between complete and incomplete spinal injury and
demonstrate the ability to accurately complete detailedASIA grading andcategoryassignment,andtheprognosisofneurologicrecoveryforeach.
o Themajorpatternsofspinalinjury(complete,centralcord,Brown-Sequard,cauda equina, etc). Whatmechanisms of injury and spinal column injuryare most commonly associated with each? What is the prognosis forrecoveryforeach?
o Thepathophysiologyofcraniocervicalinjuriesinadults.o Thepathophysiologyofsub-axialspinalcolumnandspinalcordinjuriesin
adults.
43
• Residents will discuss the indications and potential complications for allneurosurgicalprocedures.Thiswillbeacquiredfromdiscussionswithfacultyandby reading textbooksand the literature. Itwill alsobeevaluated indidactic caseconferences.
• They will learn how to write appropriate admission and medication orders forward,ICU,andpost-operativepatients.
• TheywilldiscussspecificJCAHOhospitalsafetyregulations.• They will learn the importance of timely and accurate medical record keeping
includingmedicationreconciliation.• Knowledge of general medicine and surgical principles as well as the
pathophysiology of neurosurgical diseases will be acquired with experience,readingandobservationof thepracticehabitsofseniorneurosurgeonsandnon-surgicalconsultants,andindidacticcaseconferences.
INTERPERSONALCOMMUNICATIONSKILLS:• They will learn how to communicate the pertinent positives and negatives of a
generalmedical and neurological examination to senior residents, neurosurgicalattendings,andconsultingphysiciansinanaccurateandtimelyfashion.
• They will learn how to communicate critical interpretation and correlation ofclinicalandneurodiagnostic(imaging)examinationsbasedonasoundknowledgeof neurology and neuropathology to senior residents, neurosurgical attendings,andconsultingphysiciansinanaccurateandtimelyfashion.
• They will learn to be competent in communicating with team members in thehand-overprocessinordertominimizeerrorsduringtransitionsofcare.
• Theywilllearntocommunicateclearlyandpromptlywiththenursingandsupportstaffinordertoobtainthebestpatientcare.
• They will learn to communicate patient information, care plans, and prognosiseffectivelyandcompassionatelywithpatientsandtheirfamilies.
• TheywillalsolearntopresentinweeklydidacticcaseconferencesandatJournalClub
SYSTEMSBASEDPACTICE:• Residentswill learn thatpatientcare isa teameffortwhereeachmemberof the
team is equally important in attaining satisfactory patient outcomes. The teamincludes floor nurses, nurse practitioners, operating room personnel, socialworkers,rehabilitationspecialists,consultantsandhousestafffromotherservices,otherneurosurgicalresidentsandmedicalstudentsandconsultantneurosurgeons.
• Theywilllearntocoordinateandmanagecommunicationbetweenservicesonco-managedpatients.
• Theywill interact and coordinate the longitudinal care of neurosurgical patientsthrough discussions with Neurosurgical NP’s, Physiatrists, Physical Therapists,SocialWorkers,anddischargeplanningnurses.
• Theywill learn the regulatory issues involved in reportingbraindeathandnon-accidentalneurologicinjury(especiallyinthepediatricpopulation).
PRACTICE-BASEDLEARNING:
44
• The resident will learn to analyze his or her own practice for neededimprovements.
• Theywillalsolearntouseevidencefromscientificstudiestoguidetheirmedicaldecisionmaking
• Theywilllearntheapplicationofresearchandstatisticalmethods.• They will participate in clinical research projects where appropriate including
participatingintheIRBandconsentprocess.• ResidentswillattendtheWood’sHoleNeurosurgicalResearchCoursePROFESSIONALISM:• Trainees will learn constructive collegiality with faculty, their fellow residents,
consultants and house staff from other specialties and services, but also withnursesandparamedicalpersonnel.
• Residentswilllearnhowtodealwithpatientsandfamiliesinacompassionateandhumanisticway.
• Maintainprofessionalrapportandcomportmentwithpa• Demonstraterespectforpatientsandcolleaguesfromdiversecultural,ethnicand
religious backgrounds, patient families, nurses, other physician teams and otherhospitalpersonnel.
• Demonstratehonestyinallprofessionalinteractions.• Residentswillmaintaintimelyandaccuratemedicalrecords.• Residentswillalso:
o Attendallrequiredconferencesinatimelyfashion.o Pre-roundonICUpatientsandpresenttimely,accuratedatatoteam.o Participate in discussion of ethical dilemmas related to care delivery,
consent,andlifesupportinseverelyinjuredpatients.o ProvideconsultationtotheEDandotherservicesintimelyfashion.o Demonstrate dress, grooming and behavior consistent with institutional
anddepartmentalguidelines.o Comply with all GME and Departmental regulations regarding duty hour
restrictionsandreportpersonalscheduleintimelyandaccuratefashion.o Appear for duty appropriately rested and fit to provide the services
requiredbytheirpatients.o Accurately self-report fatigue in situations that may compromise safety
and/orpatientcare.o Mustbecommittedtoandresponsibleforpromotingpatientsafety.o Must demonstrate responsiveness to patient needs that supersedes self-
interest.o Must recognize thatundercertaincircumstances, thebest interestsof the
patient may be served by transitioning that patient’s care to anotherqualifiedandrestedprovider.
METHODSOFEVALUATION:• Resident fundofmedicalknowledgewillbeevaluatedannuallybysitting for the
writtenportionoftheABNSprimaryexamination.o They are required to obtain a passing grade on this examination prior to
completingtheirresidencytrainingandbecomingchiefresident(PGY7).
45
o They are also expected to improve their percentile performance on theABNSprimaryexaminationeachyear.
• Resident will also attend weekly didactic conferences and the monthly JournalClub.
• Conferenceattendanceandparticipationwillbereviewedanddiscussedwiththeresident. They are required to attend at least 75% of all mandatory residentconferences.
• The senior residents who report directly to the attending surgeons will alsoevaluatethejuniorresidents.
• TheNeurosurgeryAttendingStaffreviewsResidentMedicalDocumentation.• Resident academic productivity regarding published abstracts, meeting
presentations,andpublishedmanuscripts,awards,etc.arealsoreviewed• The resident will also be evaluated on their attainment of these goals and
objectives as well as on their performance in conferences on a quarterly basisthroughwritten evaluation of all 6 competencies (see resident evaluations) andverbalfeedbackfromtheChairmanandProgramDirector.
• Facultymembers,aseniorresident(asisappropriate),andtheNeurosurgicalNP’sevaluateallresidentsaftereachrotation.Theyareevaluatedonall6competencies(seeresidentevaluations).Theirattendanceandperformanceindidacticteachingconferences and their case logs are also reviewed. The Chairman and ProgramDirectorreviewtheseevaluationsandgiveverbal feedback to theresidentsonaquarterlybasis.
• Residents are promoted each year based on demonstration of competentperformanceofallrequirementsasoutlinedabove.
NeurosurgeryPGY3 - (Residents rotate as Intermediate level JuniorResidentsonTischTeams1&2)Neurosurgery PGY3 residents must demonstrate competence in all principles ofpatient care, medical knowledge, interpersonal & communication skills, andprofessionalism, as well as, in all procedures required of a Neurosurgery PGY2resident prior to progressing to the Neurosurgery PGY3 year. During this year, theresident’s clinical responsibility increases. The resident will become adept withneurosurgical instruments, operating microscope, navigation systems, and patientpositioning. An attending physician supervises all Operating Room proceduresperformedbyresidents.PATIENTCARE:
• Residentswill learnimportantdetailssuchaspatientpositioningandoptimalsurgicalapproachesforeachprocedure.ThiswillbelearnedfromexperiencedsupervisingseniorneurosurgeryhousestaffandtheNeurosurgicalfaculty.
• Theywilllearnthetechnicalaspectsoftheoperationsandwillbeevaluatedbysupervising senior neurosurgical house staff and attending staff in theoperativetheater.
• Theyare responsible for thebasic functionof theNeurosurgery services andurgent daytime neurosurgery consultations in the Hospital and in theEmergencyDepartment.
• They must demonstrate with the appropriate supervision the ability torecognizeandtreatneurosurgicalemergencies:
46
o Statusepilepticso Unstablespineandspinalcordinjuryo Acuteshuntmalfunctiono CerebralHerniation/Increasedintracranialpressureo Acuteintracranialhemorrhageo CNSinfectiono Sub-arachnoidhemorrhage/Vasospasmo MetabolicDisorders/intoxication/withdrawal(EtOHandNarcotic)
• Theywilllearntoobtainandevaluateproperdiagnosticradiologicalstudies.MEDICALKNOWLEDGE:
• Residents will learn the necessary elements for a good surgical outcome:properpatientselection, identificationandpreoperativestabilizationofotherdiseaseprocesseswhichcancauseproblemsinthepostoperativeperiodsuchas hypertension, cardiovascular disease, pulmonary insufficiency, diabetes,alcoholism, clotting disorders, renal insufficiency, atherosclerosis andendocrinologicdysfunction.
o Theresidentswillbetaughttoidentifyandmanageemergencysituations:epiduralhematoma,cerebralherniation,postoperativehematoma,traumaticspinalcordinjury,obstructivehydrocephalus,cerebralischemia,spinalcordcompression,statusepilepticusandothers.Theywillalsolearnthepreoperativeselectionofendovascularneurosurgerycandidatesaswellasthepreoperativecounseling,preoperativeand,postoperativecareofendovascularneurosurgerypatients.
• They learnthis throughextensiveclinicalexposureanddidacticquestionandanswersessions in themultipleconferencesoffered throughout theacademicyear.
• Withappropriatesupervision,residentswilllearntocompetentlyperformthefollowingprocedures:
ProceduresAllNeurosurgeryPGY2proceduresIncision,burrholesandremovalofboneflapforcraniotomyIncision,burrholesandremovalofboneflapforsub-occipitalcraniotomyVentriculo-peritionealshuntVentriculo-pleuralshuntVentriculo-atrialshuntClosurelaminectomywoundsClosureanteriorcervicalfusionwoundsLaminectomyforlumbardiscLumbarlaminectomyforstenosisCSFshuntlumbarCarpaltunnelreleaseUlnarnervereleaseLumbarpediclescrewplacementLateralmassscrewplacementFundamentalcerebralandspinalangiography
47
INTERPERSONALandCOMMUNICATIONSKILLS:• They will learn how to communicate the pertinent positives and negatives of a
generalmedical and neurological examination to senior residents, neurosurgicalattendings,andconsultingphysiciansinanaccurateandtimelyfashion.
• They will learn how to communicate critical interpretation and correlation ofclinicalandneurodiagnostic(imaging)examinationsbasedonasoundknowledgeof neurology and neuropathology to senior residents, neurosurgical attendings,andconsultingphysiciansinanaccurateandtimelyfashion.
• They will learn to be competent in communicating with team members in thehand-overprocessinordertominimizeerrorsduringtransitionsofcare.
• Theywilllearntocommunicateclearlyandpromptlywiththenursingandsupportstaffinordertoobtainthebestpatientcare.
• They will learn to communicate patient information, care plans, and prognosiseffectivelyandcompassionatelywithpatientsandtheirfamilies.
• TheywillalsolearntopresentinweeklydidacticcaseconferencesandatJournalClub
SYSTEMS-BASEDPRACTICE:
• In addition to skillsmastered in the PGY2 year, traineeswill learnwhat thedelivery of health care costs (daily hospitalization costs, the costs of imagingproceduresandlaboratorytests,surgicalfees,anesthesiacharges,etc.).
• Theywillbetaughttopracticecost-effectivemedicinewithoutsacrificinggoodclinicaloutcomes.
• The resident will discuss JACHO patient safety standards regarding patientidentification, medication order writing, surgical site preparation (includinghairremoval),peri-operativeantibioticadministration,thepre-operativetimeout site and operative identification procedure, and peri- operative DVTprophylaxisalgorithm.
• They will learn effective interaction with the peri-operative nursing andanesthesia personnel in delivering appropriate operative patient careincluding:
o Siteidentification,confirmationandpreparation(asabove).o Communication of need for modification of anesthetic technique (i.e.
neurophysiologicmonitoring).o Availabilityofcellsaver/bloodproducts.o Alertnursingstaffofpotentialforfrozensection.o Reviewandcorrectionofperi-operativeriskfactorsandco-morbidities
prior to starting procedure (i.e. Alerting electrophysiology of need tointerrogatepacemakerorplaceamagnet).
PRACTICE-BASEDLEARNING:
• Residents will learn to critically analyze the literature and presentations atmeetings.Journalarticlesandconferencepresentationsarediscussedbetweenresidents and faculty in formal “JournalClubs”, in conferences and inday-to-daydiscussionswithfacultymembers.
• Resident fundofmedical knowledgewill be evaluatedannuallyby sitting forthe written portion of the ABNS primary examination. They are required to
48
obtainapassinggradeonthisexaminationpriortocompletingtheirresidencytrainingandbecomingchiefresident(PGY7).
• TheywillparticipateinclinicalresearchprojectswhereappropriateincludingparticipatingintheIRBandconsentprocess.
PROFESSIONALISM:• Traineeswilllearnconstructivecollegialitywithfaculty,theirfellowresidents,
consultantsandhousestafffromotherspecialtiesandservices,andwithnursesandparamedicalpersonnel.
• Residentswilllearnhowtodealwithpatientsandfamiliesinacompassionateandhumanisticway.
• Maintainprofessionalrapportandcomportmentwithpatientfamilies,nurses,otherphysicianteamsandotherhospitalpersonnel.
• Demonstraterespectforpatientsandcolleaguesfromdiversecultural,ethnicandreligiousbackgrounds.
• Demonstratehonestyinallprofessionalinteractions.• Residentswillmaintaintimelyandaccuratemedicalrecords.• Residentswillalso:
o Attendallrequiredconferencesinatimelyfashion.o Pre-round on ICU patients and present timely, accurate data to
neurosurgeryteam.o Participate in discussion of ethical dilemmas related to care delivery,
consent,andlifesupportinseverelyinjuredpatients.o ProvideconsultationtotheEDandotherservicesintimelyfashion.o Demonstrate dress, grooming and behavior consistent with institutional
anddepartmentalguidelines.o Comply with all GME and Departmental regulations regarding duty hour
restrictionsandreportpersonalscheduleintimelyandaccuratefashion.o Appear for duty appropriately rested and fit to provide the services
requiredbytheirpatients.o Accurately self-report fatigue in situations that may compromise safety
and/orpatientcare.o Mustbecommittedtoandresponsibleforpromotingpatientsafety.o Must demonstrate responsiveness to patient needs that supersedes self-
interest.o Must recognize thatundercertaincircumstances, thebest interestsof the
patient may be served by transitioning that patient’s care to anotherqualifiedandrestedprovider.
METHODOFEVALUATION:• Resident fundofmedicalknowledgewillbeevaluatedannuallybysitting for the
writtenportionoftheABNSprimaryexamination.o They are required to obtain a passing grade on this examination prior to
completingtheirresidencytraining.o TheyarealsoexpectedtoimprovetheirpercentileperformanceontheABNSprimaryexaminationeachyear.
49
• Resident will also attend weekly didactic conferences and the monthly JournalClub.
• Conferenceattendanceandparticipationwillbereviewedanddiscussedwiththeresident. They are required to attend at least 75% of all mandatory residentconferences.
• The senior residents who report directly to the attending surgeons will alsoevaluatethejuniorresidents.
• TheNeurosurgeryAttendingStaffreviewsResidentMedicalDocumentation.• Resident academic productivity regarding published abstracts, meeting
presentations,andpublishedmanuscripts,awards,etc.arealsoreviewed• The resident will also be evaluated on their attainment of these goals and
objectives as well as on their performance in conferences on a quarterly basisthroughwritten evaluation of all 6 competencies (see resident evaluations) andverbalfeedbackfromtheChairmanandProgramDirector.
• Facultymembers,aseniorresident(asisappropriate),andtheNeurosurgicalNP’sevaluateallresidentsaftereachrotation.Theyareevaluatedonall6competencies(seeresidentevaluations).Theirattendanceandperformanceindidacticteachingconferences and their case logs are also reviewed. The Chairman and ProgramDirectorreviewtheseevaluationsandgiveverbal feedback to theresidentsonaquarterlybasis.
• Residents are promoted each year based on demonstration of competentperformanceofallrequirementsasoutlinedabove.
NeurosurgeryPGY3-(ResidentsrotateasIntermediatelevelJuniorResidentsatBellevueHospitalCenter)NeurosurgeryPGY3residentsmustdemonstratecompetenceinallprinciplesofpatientcare,medicalknowledge,interpersonal&communicationskills,andprofessionalismaswellasinallproceduresrequiredofaNeurosurgeryPGY2residentpriortoprogressingtotheNeurosurgeryPGY3year.Duringthisyear,theresidents’clinicalresponsibilityincreases.Theresidentwillbecomeadeptwithneurosurgicalinstruments,operatingmicroscope,navigationsystems,andpatientpostioning.AnattendingphysiciansupervisesallOperatingRoomproceduresperformedbyresidents.Inadditiontomasteringtheproceduresoutlinedbelow,theNeurosurgeryPGY3residentmustmaster:PATIENTCARE:
• Residents will discuss important details such as patient positioning andoptimal surgical approaches for each procedure. This will be learned fromexperienced supervising senior neurosurgery house staff and theNeurosurgicalfaculty.
• Theywilllearnthetechnicalaspectsoftheoperationsandwillbeevaluatedbysupervising senior neurosurgical house staff and attending staff in theoperativetheater.
• Theyare responsible for thebasic functionof theNeurosurgery services andurgent daytime neurosurgery consultations in the Hospital and in theEmergencyDepartment.
50
• They must demonstrate with the appropriate supervision the ability torecognizeandtreatneurosurgicalemergencies:
o Statusepilepticuso Unstablespineandspinalcordinjuryo Acuteshuntmalfunctiono CerebralHerniation/Increasedintracranialpressureo Acuteintracranialhemorrhageo CNSinfectiono Sub-arachnoidhemorrhage/Vasospasmo MetabolicDisorders/intoxication/withdrawal(EtOHandNarcotic)
• Theywilllearntoobtainandevaluateproperdiagnosticradiologicalstudies.MEDICALKNOWLEDGE:
• Residents will learn the necessary elements for a good surgical outcome:properpatientselection, identificationandpreoperativestabilizationofotherdiseaseprocesseswhichcancauseproblemsinthepostoperativeperiodsuchas hypertension, cardiovascular disease, pulmonary insufficiency, diabetes,alcoholism, clotting disorders, renal insufficiency, atherosclerosis andendocrinologicdysfunction.
• The residents will be taught to identify and manage emergency situations:epidural hematoma, cerebral herniation, postoperative clot, traumatic spinalcord injury, obstructive hydrocephalus, cerebral ischemia, spinal cordcompression, statusepilepticusandothers.They learn this throughextensiveclinical exposure and didactic question and answer sessions in the multipleconferencesofferedthroughouttheacademicyear.
• Withappropriatesupervision,residentswilllearntocompetentlyperformthefollowingprocedures:
ProceduresAllNeurosurgeryPGY2proceduresIncision,burrholesandremovalofboneflapforcraniotomyIncision,burrholesandremovalofboneflapforsub-occipitalcraniotomyVentriculo-peritionealshuntVentriculo-pleuralshuntVentriculo-atrialshuntClosurelaminectomywoundsClosureanteriorcervicalfusionwoundsLaminectomyforlumbardiscLumbarlaminectomyforstenosisCSFshuntlumbarCarpaltunnelreleaseUlnarnervereleaseLumbarpediclescrewplacementLateralmassscrewplacement
INTERPERSONALandCOMMUNICATIONSKILLS:
51
• They will learn how to communicate the pertinent positives and negatives of ageneralmedical and neurological examination to senior residents, neurosurgicalattendings,andconsultingphysiciansinanaccurateandtimelyfashion.
• They will learn how to communicate critical interpretation and correlation ofclinicalandneurodiagnostic(imaging)examinationsbasedonasoundknowledgeof neurology and neuropathology to senior residents, neurosurgical attendings,andconsultingphysiciansinanaccurateandtimelyfashion.
• They will learn to be competent in communicating with team members in thehand-overprocessinordertominimizeerrorsduringtransitionsofcare.
• Theywilllearntocommunicateclearlyandpromptlywiththenursingandsupportstaffinordertoobtainthebestpatientcare.
• They will learn to communicate patient information, care plans, and prognosiseffectivelyandcompassionatelywithpatientsandtheirfamilies.
• TheywillalsolearntopresentinweeklydidacticcaseconferencesandatJournalClub
SYSTEMS-BASEDPRACTICE:
• In addition to skillsmastered in the PGY3 year, traineeswill learnwhat thedelivery of health care costs (daily hospitalization costs, the costs of imagingproceduresandlaboratorytests,surgicalfees,anesthesiacharges,etc.).
• Theywillbetaughttopracticecost-effectivemedicinewithoutsacrificinggoodclinicaloutcomes.
• The resident will discuss JACHO patient safety standards regarding patientidentification, medication order writing, surgical site preparation (includinghairremoval),peri-operativeantibioticadministration,thepre-operativetimeout site and operative identification procedure, and peri-operative DVTprophylaxisalgorithm.
• They will learn effective interaction with the peri-operative nursing andanesthesia personnel in delivering appropriate operative patient careincluding:
o Siteidentificationandpreparation(asabove).o Communication of need for modification of anesthetic technique (i.e.
neurophysiologicmonitoring).o Availabilityofcellsaver/bloodproducts.o Alertnursingstaffofpotentialforfrozensection.o Reviewandcorrectionofperi-operativeriskfactorsandco-morbidities
prior to starting procedure (i.e. Alerting electrophysiology of need tointerrogatepacemakerorplaceamagnet).
PRACTICE-BASEDLEARNING:
• Residents will learn to critically analyze the literature and presentations atmeetings.Journalarticlesandconferencepresentationsarediscussedbetweenresidents and faculty in formal “JournalClubs”, in conferences and inday-to-daydiscussionswithfacultymembers.
• Resident fundofmedical knowledgewill be evaluatedannuallyby sitting forthe written portion of the ABNS primary examination. They are required to
52
obtainapassinggradeonthisexaminationpriortocompletingtheirresidencytraining.
• TheywillparticipateinclinicalresearchprojectswhereappropriateincludingparticipatingintheIRBandconsentprocess.
PROFESSIONALISM:• Trainees will learn constructive collegiality with faculty, their fellow residents,
consultants andhouse staff fromother specialties and services, andwithnursesandparamedicalpersonnel.
• Residentswilllearnhowtodealwithpatientsandfamiliesinacompassionateandhumanisticway.
• Maintain professional rapport and comportment with patient families, nurses,otherphysicianteamsandotherhospitalpersonnel.
• Demonstraterespectforpatientsandcolleaguesfromdiversecultural,ethnicandreligiousbackgrounds.
• Demonstratehonestyinallprofessionalinteractions.• Residentswillmaintaintimelyandaccuratemedicalrecords.• Residentswillalso:
o Attendallrequiredconferencesinatimelyfashion.o Pre-roundonICUpatientsandpresenttimely,accuratedatatoteam.o Participate in discussion of ethical dilemmas related to care delivery,
consent,andlifesupportinseverelyinjuredpatients.o ProvideconsultationtotheEDandotherservicesintimelyfashion.o Demonstrate dress, grooming and behavior consistent with institutional
anddepartmentalguidelines.o Comply with all GME and Departmental regulations regarding duty hour
restrictionsandreportpersonalscheduleintimelyandaccuratefashion.o Appear for duty appropriately rested and fit to provide the services
requiredbytheirpatients.o Accurately self-report fatigue in situations that may compromise safety
and/orpatientcare.o Mustbecommittedtoandresponsibleforpromotingpatientsafety.o Must demonstrate responsiveness to patient needs that supersedes self-
interest.o Must recognize thatundercertaincircumstances, thebest interestsof the
patient may be served by transitioning that patient’s care to anotherqualifiedandrestedprovider.
METHODOFEVALUATION:• Resident fundofmedicalknowledgewillbeevaluatedannuallybysitting for the
writtenportionoftheABNSprimaryexamination.o They are required to obtain a passing grade on this examination prior to
completingtheirresidencytraining.o TheyarealsoexpectedtoimprovetheirpercentileperformanceontheABNSprimaryexaminationeachyear.
• Resident will also attend weekly didactic conferences and the monthly JournalClub.
53
• Conferenceattendanceandparticipationwillbereviewedanddiscussedwiththeresident. They are required to attend at least 75% of all mandatory residentconferences.
• The senior residents who report directly to the attending surgeons will alsoevaluatethejuniorresidents.
• TheNeurosurgeryAttendingStaffreviewsResidentMedicalDocumentation.• Resident academic productivity regarding published abstracts, meeting
presentations,andpublishedmanuscripts,awards,etc.arealsoreviewed• The resident will also be evaluated on their attainment of these goals and
objectives as well as on their performance in conferences on a quarterly basisthroughwritten evaluation of all 6 competencies (see resident evaluations) andverbalfeedbackfromtheChairmanandProgramDirector.
• Facultymembers,aseniorresident(asisappropriate),andtheNeurosurgicalNP’sevaluateallresidentsaftereachrotation.Theyareevaluatedonall6competencies(seeresidentevaluations).Theirattendanceandperformanceindidacticteachingconferences and their case logs are also reviewed. The Chairman and ProgramDirectorreviewtheseevaluationsandgiveverbal feedback to theresidentsonaquarterlybasis.
• Residents are promoted each year based on demonstration of competentperformanceofallrequirementsasoutlinedabove.
NeurosurgeryPGY3-(ResidentsrotateasIntermediatelevelJuniorResidentsatNewYorkHarborHealthCareSystem(VA)Neurosurgery PGY3 residents must demonstrate competence in all principles ofpatient care, medical knowledge, interpersonal & communication skills, andprofessionalismaswellasinallproceduresrequiredofaNeurosurgeryPGY2residentprior toprogressing to theNeurosurgeryPGY3year.During this year, the residentsclinical responsibility increases. The residentwill become adeptwith neurosurgicalinstruments, operating microscope, navigation systems, and patient postioning. Anattending physician supervises all Operating Room procedures performed byresidents. Inadditiontomasteringtheproceduresoutlinedbelow,theNeurosurgeryPGY3residentmustmaster:PATIENTCARE:
• Residentswill learnimportantdetailssuchaspatientpositioningandoptimalsurgicalapproachesforeachprocedure.ThiswillbelearnedfromexperiencedsupervisingseniorneurosurgeryhousestaffandtheNeurosurgicalfaculty.
• Theywilllearnthetechnicalaspectsoftheoperationsandwillbeevaluatedbysupervising senior neurosurgical house staff and attending staff in theoperativetheater.
• Theyare responsible for thebasic functionof theNeurosurgery services andurgent daytime neurosurgery consultations in the Hospital and in theEmergencyDepartment.
• They must demonstrate with the appropriate supervision the ability torecognizeandtreatneurosurgicalemergencies:
o Statusepilepticuso Unstablespineandspinalcordinjury
54
o Acuteshuntmalfunctiono CerebralHerniation/Increasedintracranialpressureo Acuteintracranialhemorrhageo CNSinfectiono Sub-arachnoidhemorrhage/Vasospasmo MetabolicDisorders/intoxication/withdrawal(EtOHandNarcotic)
• Theywilllearntoobtainandevaluateproperdiagnosticradiologicalstudies.MEDICALKNOWLEDGE:
• Residents will learn the necessary elements for a good surgical outcome:properpatientselection, identificationandpreoperativestabilizationofotherdiseaseprocesseswhichcancauseproblemsinthepostoperativeperiodsuchas hypertension, cardiovascular disease, pulmonary insufficiency, diabetes,alcoholism, clotting disorders, renal insufficiency, atherosclerosis andendocrinologicdysfunction.
• The residents will be taught to identify and manage emergency situations:epidural hematoma, cerebral herniation, postoperative clot, traumatic spinalcord injury, obstructive hydrocephalus, cerebral ischemia, spinal cordcompression, statusepilepticusandothers.They learn this throughextensiveclinical exposure and didactic question and answer sessions in the multipleconferencesofferedthroughouttheacademicyear.
• Withappropriatesupervision,residentswilllearntocompetentlyperformthefollowingprocedures:
ProceduresAllNeurosurgeryPGY2proceduresIncision,burrholesandremovalofboneflapforcraniotomyIncision,burrholesandremovalofboneflapforsub-occipitalcraniotomyVentriculo-peritionealshuntVentriculo-pleuralshuntVentriculo-atrialshuntClosurelaminectomywoundsClosureanteriorcervicalfusionwoundsLaminectomyforlumbardiscLumbarlaminectomyforstenosisCSFshuntlumbarCarpaltunnelreleaseUlnarnervereleaseLumbarpediclescrewplacementLateralmassscrewplacement
INTERPERSONALandCOMMUNICATIONSKILLS:• They will learn how to communicate the pertinent positives and negatives of a
generalmedical and neurological examination to senior residents, neurosurgicalattendings,andconsultingphysiciansinanaccurateandtimelyfashion.
• They will learn how to communicate critical interpretation and correlation ofclinicalandneurodiagnostic(imaging)examinationsbasedonasoundknowledge
55
of neurology and neuropathology to senior residents, neurosurgical attendings,andconsultingphysiciansinanaccurateandtimelyfashion.
• They will learn to be competent in communicating with team members in thehand-overprocessinordertominimizeerrorsduringtransitionsofcare.
• Theywilllearntocommunicateclearlyandpromptlywiththenursingandsupportstaffinordertoobtainthebestpatientcare.
• They will learn to communicate patient information, care plans, and prognosiseffectivelyandcompassionatelywithpatientsandtheirfamilies.
• TheywillalsolearntopresentinweeklydidacticcaseconferencesandatJournalClub
SYSTEMS-BASEDPRACTICE:
• In addition to skills mastered in the R1 year, trainees will learn what thedelivery of health care costs (daily hospitalization costs, the costs of imagingproceduresandlaboratorytests,surgicalfees,anesthesiacharges,etc.).
• Theywillbetaughttopracticecost-effectivemedicinewithoutsacrificinggoodclinicaloutcomes.
• The resident will discuss JACHO patient safety standards regarding patientidentification, medication order writing, surgical site preparation (includinghairremoval),peri-operativeantibioticadministration,thepre-operativetimeout site and operative identification procedure, and peri- operative DVTprophylaxisalgorithm.
• They will learn effective interaction with the peri-operative nursing andanesthesia personnel in delivering appropriate operative patient careincluding:
o Siteidentificationandpreparation(asabove).o Communication of need for modification of anesthetic technique (i.e.
neurophysiologicmonitoring).o Availabilityofcellsaver/bloodproducts.o Alertnursingstaffofpotentialforfrozensection.o Reviewandcorrectionofperi-operativeriskfactorsandco-morbidities
prior to starting procedure (i.e. Alerting electrophysiology of need tointerrogatepacemakerorplaceamagnet).
PRACTICE-BASEDLEARNING:
• Residents will learn to critically analyze the literature and presentations atmeetings.Journalarticlesandconferencepresentationsarediscussedbetweenresidents and faculty in formal “JournalClubs”, in conferences and inday-to-daydiscussionswithfacultymembers.
• ResidentswillattendtheChicagoNeurosurgicalReviewCourse.• Resident fundofmedical knowledgewill be evaluatedannuallyby sitting for
the written portion of the ABNS primary examination. They are required toobtainapassinggradeonthisexaminationpriortocompletingtheirresidencytraining.
• TheywillparticipateinclinicalresearchprojectswhereappropriateincludingparticipatingintheIRBandconsentprocess.
56
PROFESSIONALISM:• Trainees will learn constructive collegiality with faculty, their fellow residents,
consultants andhouse staff fromother specialties and services, andwithnursesandparamedicalpersonnel.
• Residentswilllearnhowtodealwithpatientsandfamiliesinacompassionateandhumanisticway.
• Maintain professional rapport and comportment with patient families, nurses,otherphysicianteamsandotherhospitalpersonnel.
• Demonstraterespectforpatientsandcolleaguesfromdiversecultural,ethnicandreligiousbackgrounds.
• Demonstratehonestyinallprofessionalinteractions.• Residentswillmaintaintimelyandaccuratemedicalrecords.• Residentswillalso:
o Attendallrequiredconferencesinatimelyfashion.o Pre-roundonICUpatientsandpresenttimely,accuratedatatoteam.o Participate in discussion of ethical dilemmas related to care delivery,
consent,andlifesupportinseverelyinjuredpatients.o ProvideconsultationtotheEDandotherservicesintimelyfashion.o Demonstrate dress, grooming and behavior consistent with institutional
anddepartmentalguidelines.o Comply with all GME and Departmental regulations regarding duty hour
restrictionsandreportpersonalscheduleintimelyandaccuratefashion.o Appear for duty appropriately rested and fit to provide the services
requiredbytheirpatients.o Accurately self-report fatigue in situations that may compromise safety
and/orpatientcare.o Mustbecommittedtoandresponsibleforpromotingpatientsafety.o Must demonstrate responsiveness to patient needs that supersedes self-
interest.o Must recognize thatundercertaincircumstances, thebest interestsof the
patient may be served by transitioning that patient’s care to anotherqualifiedandrestedprovider.
METHODOFEVALUATION:• Resident fundofmedicalknowledgewillbeevaluatedannuallybysitting for the
writtenportionoftheABNSprimaryexamination.o They are required to obtain a passing grade on this examination prior to
completingtheirresidencytraining.o TheyarealsoexpectedtoimprovetheirpercentileperformanceontheABNSprimaryexaminationeachyear.
• Resident will also attend weekly didactic conferences and the monthly JournalClub.
• Conferenceattendanceandparticipationwillbereviewedanddiscussedwiththeresident. They are required to attend at least 75% of all mandatory residentconferences.
• The senior residents who report directly to the attending surgeons will alsoevaluatethejuniorresidents.
57
• TheNeurosurgeryAttendingStaffreviewsResidentMedicalDocumentation.• Resident academic productivity regarding published abstracts, meeting
presentations,andpublishedmanuscripts,awards,etc.arealsoreviewed• The resident will also be evaluated on their attainment of these goals and
objectives as well as on their performance in conferences on a quarterly basisthroughwritten evaluation of all 6 competencies (see resident evaluations) andverbalfeedbackfromtheChairmanandProgramDirector.
• Facultymembers,aseniorresident(asisappropriate),andtheNeurosurgicalNP’sevaluateallresidentsaftereachrotation.Theyareevaluatedonall6competencies(seeresidentevaluations).Theirattendanceandperformanceindidacticteachingconferences and their case logs are also reviewed. The Chairman and ProgramDirectorreviewtheseevaluationsandgiveverbal feedback to theresidentsonaquarterlybasis.
• Residents are promoted each year based on demonstration of competentperformanceofallrequirementsasoutlinedabove.
NeurosurgeryPGY4-(ResidentsrotateasSeniorResidentsonPediatricNeurosurgeryandEpilepsy/FunctionalNeurosurgery)Neurosurgery PGY4 residentsmust demonstrate competence in all the competencybasedprinciplesofpatientcare,medicalknowledge, interpersonal&communicationskills, and professionalism as well as in all procedures required of a NeurosurgeryPGY3 resident prior to progressing to the Neurosurgery PGY4 year. An attendingphysician supervises all Operating Room procedures performed by residents andsupervisesallpatientcontact.Inadditiontomasteringtheproceduresoutlinedbelow,theNeurosurgeryPGY4residentmustmaster:PEDIATRICSPATIENTCAREPEDIATRICS:• Perform all of the diagnostic, procedural and communicative skills and
competency-basedrequirementsoutlinedinthepreviousyears,andapplythosetothepediatricandthefunctional/epilepsypatientpopulation.
• With appropriate supervision, residents will learn to competently perform thefollowingproceduresinthepediatricpatientpopulation:PediatricNeurosurgicalProcedures
Incision,burrholesandremovalofboneflapforcraniotomyIncision,burrholesandremovalofboneflapforsub-occipitalcraniotomyVentriculo-peritionealshuntVentriculo-pleuralshuntVentriculo-atrialshuntClosurelaminectomywoundsLaminectomyforlumbardiscCraniotomyfortraumaCraniotomyforcraniofacialrepairCranioplastyVentriculoendoscopicproceduresandequipment–fiberopticandrodlensscopesandcameras,endoscopicthirdventriculostomy,tumorbiopsyandresection,cystfenestration
58
LaminectomylumbarLaminectomythoracic/cervicalPeripheralnerverepair/decompressionCraniotomy/microsurgicaltechniquefortumorCraniotomy/microsurgicaltechniqueforvascularlesionDemonstrate the ability to position, prepare and drape pediatric patients,includinginfants,forinsertionofCNSimplanteddevices(includingCSFshunt)Demonstrate appropriate placement of cranial immobilization devices,includingMayfieldandSugitapins,inyoungchildrenConsiderations for wound closure in pediatric patients, suture material andcranialplatingoptions.Collect,editandpresenthighqualityintraoperativephotographsandvideoforuseinconferencesandpublication.
MEDICALKNOWLEDGEPEDIATRICS:• DiscusstheembryologyofcongenitalCNSmalformation.• Demonstrate the proper performance of a complete and a targeted neurological
examinationindifferentagegroupsandcircumstances:o Infanto Childo Adolescento Developmentallydelayedpatient.
• Demonstrate the ability to obtain and evaluate proper radiological studies inchildren:
o MRIbrainandspineo CineMRICSFflowstudyo MRA/MRVo CTbrainandspineo 3DCTskullforsynostosiso CSFshuntandbaclofenpumpx-rayserieso VNSx-rayserieso NuclearMedicineShuntPatencystudy
• Demonstrate ability to recognize, understand and manage, with supervision,
neurosurgicalemergenciesinchildren:o Statusepilepticus(thisismanagedbyneurology)o Cerebralherniationo CNSinfectiono Unstablespineo SevereCNSmetabolicabnormalityo SevereCSFshuntmalfunction.
• DemonstratetheabilitytoevaluatepatientsforCSFshuntinfectionand/orfailure.• Demonstratetheabilitytoevaluatepediatricneurotraumapatients.• DemonstratetheabilitytoperformbasicbedsideandICUproceduresinchildren:
o CSFshunttapo ICPmonitor
59
o Ventriculostomyo Lumbarpuncture/Lumbardrainplacement.
• Discuss the intra- and peri-operative physiology of the premature infant, infantandchild.
• Discuss the pathophysiology and management of congenital, post-hemorrhagic,post-infectious, post-traumatic, oncologic, and myelomeningocele associatedhydrocephalus.
• DiscussthetumorbiologyofCNSmalignancyinchildren.• Discussmanagementofmyelomeningocelepatients inpre-natal, infant,childand
adultagegroups.• Discuss the pathophysiology of childhood epilepsies, cortical dysplasia and
heterotopia.• Discuss the appropriate medical, surgical and endoscopic management of
obstructiveandcommunicatinghydrocephalus.• Discuss primary and secondary management of tethered spinal cord, including
diagnosisofsecondarytethering.• DiscussICUmanagementofseveretraumaticbraininjuryinchildren• Discuss the diagnosis and management of non-accidental trauma including
notificationoftheappropriateauthorities.• Discusstheroleofsurgeryinmedicallyrefractoryepilepsytreatmentinchildren,
includingresectivesurgeryandVNS.• Discussintra-operativeandpost-operativestrategiesforresectionandadjunctive
therapy in medulloblastoma, cerebellar astrocytoma and hypothalamicastrocytoma.
• Discuss appropriate post-traumatic and peri-operative narcotic orders in infantsandchildren.
• Discussappropriatepainmanagement,sedationagents,dosesandtheregulatorylimitsonsupervisedsedationinpediatricpatients.
• Discusstheprinciplesofmedicalandsurgicalmanagementofspinalcordinjuriescommontochildhood:SCIWORAandcraniocervicalinjury.
• DiscussanddemonstratetheappropriatemanagementforspinalcordandcolumninjuryininfantsandchildrenincludingICUcare,bracing,andsurgery.
• Discuss the treatment of Chiari Imalformation and syringomyelia, including thedifferential diagnosis of and various direct and indirect surgical treatments forsyringomyelia.
• Discussthemanagementofcongenitalbirthpalsies.• Discuss the medical and surgical management options in severe spasticity and
dystoniarelatedtocerebralpalsy.• Discuss the medical and surgical management principles in patients with
neurocutaneousdisorders, includingneurofibromatosis types Iand II,hereditaryhemorrhagictelangiectasia,andtuberoussclerosis.
• Discuss the medical and surgical management of patients with intracranial andintraspinalcysts.
• Discussthemedicalandsurgicalmanagementofpediatricpatientswithintracerebralhemorrhage,includingthatrelatedtoarteriovenousmalformations
• Discuss the medical and surgical management of CNS infections and parasitic
60
infection.• BeabletodiscussandwritePICUandpost-opordersappropriateforapremature
infant,infant,child,andadolescent.• Demonstrate the ability to participate in the multi-disciplinary management of
craniosynostosispatients,includingperi-operativeplanningandmanagement,andpostoperativecare.
• Recognizedifferentshuntvalves,mechanismsandprogrammingofprogrammablevalves
• Understandthediagnosticatreatmentparadigmsfornormalpressurehydrocephalus.
• Discussthepathophysiologyofcraniofacialdisorders,sporadicandsyndromic,commonmanifestationsandassociations.
• INTERPERSONALandCOMMUNICATIONSKILLS:• They will learn how to communicate the pertinent positives and negatives of a
general medical and neurological examination to neurosurgical attendings, andconsultingphysicians.
• They will learn how to communicate critical interpretation and correlation ofclinicalandneurodiagnostic(imaging)examinationsbasedonasoundknowledgeof neurology and neuropathology to senior residents, neurosurgical attendings,andconsultingphysicians.
• TheywillpresentinweeklydidacticcaseconferencesandatJournalClub• Provideaccuratedetailedsignoutforallcoveringresidents.• They will learn to be competent in communicating with team members in the
hand-overprocessinordertominimizeerrorsduringtransitionsofcare.• Communicate treatment plans effectively with the pediatric house staff, nurse
practitionersandnurses.• They will learn to communicate patient information, care plans, and prognosis
effectively and compassionately with parents and with the patient as isappropriate.
• Theywilllearntocommunicateoperativeinformationregardingrisksbenefitandalternatives to parents and patient (as is appropriate) in an effective andcompassionatefashioninordertoobtaininterventionorsurgicalconsent.
SYSTEMS-BASEDPRACTICE:
• Traineeswilllearnwhatthedeliveryofhealthcarecosts(dailyhospitalizationcosts, the costs of imaging procedures and laboratory tests, surgical fees,anesthesiacharges,etc.).
• Theywillbetaughttopracticecost-effectivemedicinewithoutsacrificinggoodclinicaloutcomes.
• Discuss specific JCAHO hospital safety regulations that are particularlyimportantinthemanagementofnon-verbal,veryyoung,andverylowweightpatients
• Discuss the appropriate notification procedures upon the diagnosis of non-accidentaltraumainthepediatricpopulation.
• Attendpediatriconcology,craniofacial,andspasticityconferences.
61
• ManagecommunicationbetweenthePediatricICUteamsandpediatriciansforco-managedpatients.
PRACTICE-BASEDLEARNING:
• Residents will learn to critically analyze the literature and presentations atmeetings.Journalarticlesandconferencepresentationsarediscussedbetweenresidents and faculty in formal “JournalClubs”, in conferences and inday-to-daydiscussionswithfacultymembers.
• Resident fundofmedical knowledgewill be evaluatedannuallyby sitting forthe written portion of the ABNS primary examination. They are required toobtainapassinggradeonthisexaminationpriortocompletingtheirresidencytraining.
• TheywillparticipateinclinicalresearchprojectswhereappropriateincludingparticipatingintheIRBandconsentprocess.
• The resident will present at pediatric tumor board and will present thepediatricM&M’sinthemonthlyM&Mconference.
• Residents will learn that their best teachers are their patients. Much can belearnedbystudyingtheirpatients’symptoms,whetherthesearerelievedbyasurgicalprocedureorothertherapy,whatbenefittheyderivefromproceduresandatwhatcostand,ofcourse,thelong-termfollow-up.
PROFESSIONALISM:• Trainees will learn constructive collegiality with faculty, their fellow residents,
consultants andhouse staff fromother specialties and services, andwithnursesandparamedicalpersonnel.
• Residentswilllearnhowtodealwithpatientsandfamiliesinacompassionateandhumanisticway.
• Maintain professional rapport and comportment with patient families, nurses,otherphysicianteamsandotherhospitalpersonnel.
• Demonstraterespectforpatientsandcolleaguesfromdiversecultural,ethnicandreligiousbackgrounds.
• Demonstratehonestyinallprofessionalinteractions,• Residentswillmaintaintimelyandaccuratemedicalrecords.• Residentswillalso:
o Attendallrequiredconferencesinatimelyfashion.o Pre-roundonICUpatientsandpresenttimely,accuratedatatoteam.o Participate in discussion of ethical dilemmas related to care delivery,
consent,andlifesupportinseverelyinjuredpatients.o ProvideconsultationtotheEDandotherservicesintimelyfashion.o Demonstrate dress, grooming and behavior consistent with institutional
anddepartmentalguidelines.o Comply with all GME and Departmental regulations regarding duty hour
restrictionsandreportpersonalscheduleintimelyandaccuratefashion.o Appear for duty appropriately rested and fit to provide the services
requiredbytheirpatients.o Accurately self-report fatigue in situations that may compromise safety
and/orpatientcare.
62
o Mustbecommittedtoandresponsibleforpromotingpatientsafety.o Must demonstrate responsiveness to patient needs that supersedes self-
interest.o Must recognize thatundercertaincircumstances, thebest interestsof the
patient may be served by transitioning that patient’s care to anotherqualifiedandrestedprovider.
METHODOFEVALUATION:• Resident fundofmedicalknowledgewillbeevaluatedannuallybysitting for the
writtenportionoftheABNSprimaryexamination.o They are required to obtain a passing grade on this examination prior to
completingtheirresidencytrainingandbecomingchiefresident(PGY7).o TheyarealsoexpectedtoimprovetheirpercentileperformanceontheABNSprimaryexaminationeachyear.
• Resident will also attend weekly didactic conferences and the monthly JournalClub.
• Conferenceattendanceandparticipationwillbereviewedanddiscussedwiththeresident. They are required to attend at least 75% of all mandatory residentconferences.
• The senior residents who report directly to the attending surgeons will alsoevaluatethejuniorresidents.
• TheNeurosurgeryAttendingStaffreviewsResidentMedicalDocumentation.• Resident academic productivity regarding published abstracts, meeting
presentations,andpublishedmanuscripts,awards,etc.arealsoreviewed.• The resident will also be evaluated on their attainment of these goals and
objectives as well as on their performance in conferences on a quarterly basisthroughwritten evaluation of all 6 competencies (see resident evaluations) andverbalfeedbackfromtheChairmanandProgramDirector.
• Facultymembers,aseniorresident(asisappropriate),andtheNeurosurgicalNP’sevaluateallresidentsaftereachrotation.Theyareevaluatedonall6competencies(seeresidentevaluations).Theirattendanceandperformanceindidacticteachingconferences and their case logs are also reviewed. The Chairman and ProgramDirectorreviewtheseevaluationsandgiveverbal feedback to theresidentsonaquarterlybasis.
• Residents are promoted each year based on demonstration of competentperformanceofallrequirementsasoutlinedabove.
EPILEPSYPATIENTCAREEPILEPSY:• Perform all of the diagnostic, procedural and communicative skills and
competency-basedrequirementsoutlinedinthepreviousyears,andapplythosetothepediatricandthefunctional/epilepsypatientpopulation.
63
• With appropriate supervision, residents will learn to competently perform thefollowingproceduresinthefunctional/epilepsypatientpopulation:
Epilepsy/FunctionalNeurosurgeryProcedures:
1. CraniotomyforGridPlacement–2. CraniotomyforFunctionalResection–3. CraniotomyforFunctionalBrainMapping–4. Awake Craniotomies: craniotomies under local anesthesia with unique
technicalconsiderationsfor“awake”craniotomies.5. BurrHolesforDeepBrainStimulation6. BurrHolesforPlacementoflinearelectrodearraysanddepthelectrodesusing
natural landmarks, frameless and stereotactic frame based techniques forlocalizationandtrajectoryplanning.
7. MultistageCorticalresectionformedicallyrefractoryepilepsy8. VagusNerveStimulatorImplantation
a. denovoimplantationb. removalandrevisionofthesystemc. rudimentaryprogrammingofthestimulationparameters.
9. Laminectomylumbar/thoracicforimplantationofSpinalCordStimulatorsa. percutaneousandlaminectomyimplantationb. denovoimplantationc. revisionsand,andremovald. rudimentaryprogramming
10. Performing laminectomy under local anesthesia for optimal electrodepositioning.
11. Laminectomylumbar/thoracicforimplantationofIntrathecalPumps12. DBSplacementformovementdisorders13. AllNeurosurgeryPGY3procedures
MEDICALKNOWLEDGEEPILEPSY:• Discuss the pathophysiology of childhood epilepsies, cortical dysplasia and
heterotopia, benign and low-grade neoplasms, and common syndromes that areassociatedwithepilepsysuchasTuberousSclerosis.
• Discuss the role of surgery in the treatment of medically refractory epilepsy inchildrenandadults.
• Discuss the role of vagus nerve stimulation related to intracranial surgery forepilepsymanagement.
• Discuss the roleof thevariousdiagnosticand therapeutic surgicalprocedures inlightofthevariouscharacteristicmedicallyresistantepilepsies.
• Torelatetheresectiveandaugmentativetechniquestotheevolvingunderstandingof epilepsy from a functional and physiologic rather than a purely anatomicproblem.
• Discuss the relationship of experimental options such as responsiveneurostimulation and deep brain stimulation to the current neurosurgicalunderstandingofepilepsymanagement.
• Discuss the role of and the interpretation in the epilepsy surgery evaluationprocessinformulatingasurgicalplanthatincludes:
64
o videoEEGmonitoringo Wadatestingo functionalimaging(fMRI,PET,SPECT,MEG)o neuropsychologicalevaluationandseizuresemiology
• Discuss the various surgical approaches, electrode designs and implantationoptionstobeabletosamplefromtheconvexityaswellashiddencorticalsurfaces.
• Discusspostimplantcarefortheimplantedpatient.• Discusselectroderemoval.• Discusscomplicaitonuniquetoelectrodes.• Discuss the options and considerations required for anatomic and functional
resectionsinlightoffunctionalneurologicconsequences.• Discuss how functional imaging relates to the use of intra-operative functional
study.• DiscusshowfunctionalimagingisusefulforbothforinvasiveEEGandfunctional
mapping• Discuss the common complications and risk avoidance issues in the setting for
epilepsysurgerybutalsoitsappropriatenessadaptedtospecialcasesofneoplasmassociatedwithseizuresoreloquentcortex.
• Discuss the limitations and design of the surgical implantation to maximizeefficacy.
• Discuss the theory, limitations, and interpretation of physiologic findings, of thediagnostic-therapeutic staged craniotomy epilepsy surgery, compared andcontrasted to the standard single stageprocedures suchas classic antero-medialtemporalloberesection.
• Discussproceduredesignhowspecificelectrodesarelocatedandusedtoanswerimportant physiologic questions to maximize epilepsy control and minimizefunctionaldeficitsfromreseciton.
• Design and discuss appropriate resective epilepsy surgical procedure based oninterpretationofdiagnosticmodalities.
• Discusstherelationshiptopercutaneous implantationofSpinalcordstimulators,the revisions and de novo implantation, and removal, and rudimentaryprogramming.
NeurosurgeryPGY5(ResidentsrotateasSeniorResidentsatallthreeInstitutionsoronelective/research)
The PGY 5 neurosurgery resident year is primarily an elective one in which theresident can choose to pursue neuroscience research or a directed intenseneurosurgical subspecialty experience. Past residents have had concentratedexperiences in Functional neurosurgery, Spinal neurosurgery, Endovascularneurosurgery,andRadiosurgery.Theresident isexpectedtopass theABNSprimaryexaminationduringthisyearandtoproduceatleastonemanuscriptforpresentationatanationalmeetingandeventualpublication.TheR4residenttakesnightcallasthe
65
primary emergency trauma consult resident and first assistant for the BellevueHospital Chief residents in emergency/trauma cases with graduated levels ofoperative responsibility. Neurosurgery PGY 5 residents must demonstratecompetence in all principles of patient care, medical knowledge, interpersonal &communicationskills, andprofessionalismaswellas inallprocedures requiredofaNeurosurgery PGY4 resident prior to progressing to the Neurosurgery PGY5 year.Surgicaltechniquesarelearnedandstandardsofcareadopted.Anattendingphysiciansupervises all Operating Room procedures performed by residents. In addition tomastering the procedures outlined below, the Neurosurgery PGY5 resident mustmaster:PATIENTCARE:
• Theywilldemonstratecompetenceinperformingoperativeproceduresneatlyandcarefully,respectingtissueplanesandpreservingnormalstructures.
• Residentswillmasterallprioritemsonthisgraduatedlevelofresponsibilitiesand program goals handout andwith appropriate supervision, residentswilllearntocompetentlyperformthefollowingprocedures:
Procedures
CraniotomyfortraumaCraniotomyfortumorCraniotomyforcraniofacialrepairCranioplastyStereotaticbiopsiesandresectionsLaminectomylumbarLaminectomythoracic/cervicalAnteriorcervicalapproachtospinePeripheralnerverepair/decompressionCarotidendarterectomyCraniotomy/microsurgicaltechniquefortumorCraniotomy/microsurgicaltechniqueforvascularlesionTranssphenoidalpituitarysurgerySkullbasecraniotomyfortumorExtracranial/IntracranialvascularbypasssurgeryTransthoracicdecompressionofthespineRetroperitonealdecompressionofthespineComplexspinalreconstructionfortumor/traumaAllNeurosurgeryR3procedures
MEDICALKNOWLEDGE:• Theresidentwillmastertheknowledgeapplicabletothechosenareaofresearch
andclinicalexpertiseduringthiselectiveyear.• The residentwill also demonstrate under appropriate supervision the ability to
master the evaluation and care of operative and non-operative neurosurgicalemergencies.
INTERPERSONALandCOMMUNICATIONSKILLS:
66
• They will learn how to communicate the pertinent positives and negatives of ageneralmedical and neurological examination to senior residents, neurosurgicalattendings,andconsultingphysiciansinanaccurateandtimelyfashion.
• They will learn how to communicate critical interpretation and correlation ofclinicalandneurodiagnostic(imaging)examinationsbasedonasoundknowledgeof neurology and neuropathology to senior residents, neurosurgical attendings,andconsultingphysiciansinanaccurateandtimelyfashion.
• They will learn to be competent in communicating with team members in thehand-overprocessinordertominimizeerrorsduringtransitionsofcare.
• Theywilllearntocommunicateclearlyandpromptlywiththenursingandsupportstaffinordertoobtainthebestpatientcare.
• They will learn to communicate patient information, care plans, and prognosiseffectivelyandcompassionatelywithpatientsandtheirfamilies.
• TheywillorganizeJournalClubincludingselectingandassigningthearticles.• Theywillalsolearntopresentinweeklydidacticcaseconferences.SYSTEMS-BASEDPRACTICE:
• Residentswillbepreparedfortheregulatoryandfinancialaspectsofaclinicalpracticewhentheyfinishtheirresidency.Residentswilllearnwhatitcoststorunapracticeandbecognizantofsuchinformationas:themechanicsofbillingandcollection,diagnosticandbillingcodes,MedicareandMedicaidregulations,etc.
• Astraineesbecomemoremature itwillbe important for themtorealize thatwehaveveryfewanswersinneurologicalsurgery.Therewillalwaysbebetterways of helping our patients: more efficient, less invasive, less morbidprocedures, alternative therapies, better instrumentation, translationalresearch, etc. In our programwe stress to residents, as they become youngneurosurgeonsthatduringtheirsubsequentcareerstheymuststriveleavethefieldbetter than they found it.During their residency theymustquestion thevalidity of every procedure we do, especially in terms of cost/benefit andpatientoutcome.Residentsareencouragedtobecreativeandusefacilitiesthatare available throughout the institution for development of instrumentation,softwaredevelopment,statisticalanalysisandbasicsciencecollaboration.
PRACTICE-BASEDLEARNING:
• Residents will learn to critically analyze the literature and presentations atmeetings. Journal articles and conference presentations are organized by thePGY5’sanddiscussedbetweenresidentsandfacultyinformal“JournalClubs”,inconferencesandinday-to-daydiscussionswithfacultymembers.
• TheywillparticipateinclinicalresearchprojectswhereappropriateincludingparticipatingintheIRBandconsentprocess.
• Residentswill be involved in clinicalprospective and retrospective follow-upstudiesandwilllearnthenecessarydataacquisitionandanalysistoolssothatthey can continue their investigations during their training and throughouttheircareers.
• Residentswilllearnthatneurosurgeryisnotinsular.Readingtheliteratureinourfieldaswellasotherdisciplineswillspawnideasforthe improvementof
67
our techniques and practices. Development of web pages and sharingknowledge with colleagues in other countries by means of the Internetincreasestheexcitementofandenrichesourfield.
• Participation at national meetings is encouraged. Post-residency fellowshipsoverseas are also encouraged and contacts made with foreign colleaguessupportthese.Traineeswillrealizeearlyonthatneurosurgeryisinternational.
• Seniorresidentswillteach,andmentorstudentsandtheirjuniorresidents,doclinical and basic science research throughout their residency and areencouragedtopursueanacademiccareeruponcompletionoftheirtraining.
• Residents will learn that their best teachers are their patients. Much can belearnedbystudyingtheirpatients’symptoms,whetherthesearerelievedbyasurgicalprocedureorothertherapy,whatbenefittheyderivefromproceduresandatwhatcostand,ofcourse,thelong-termfollow-up
PROFESSIONALISM:• Trainees will learn constructive collegiality with faculty, their fellow residents,
consultants and house staff from other specialties and services, but also withnursesandparamedicalpersonnel.
• Residentswilllearnhowtodealwithpatientsandfamiliesinacompassionateandhumanisticway.
• Maintain professional rapport and comportment with patient families, nurses,otherphysicianteamsandotherhospitalpersonnel.
• Demonstraterespectforpatientsandcolleaguesfromdiversecultural,ethnicandreligiousbackgrounds.
• Demonstratehonestyinallprofessionalinteractions.• Residentswillmaintaintimelyandaccuratemedicalrecords.• Residentswillalso:
o Attendallrequiredconferencesinatimelyfashion.o Pre-roundonICUpatientsandpresenttimely,accuratedatatoteam.o Participate in discussion of ethical dilemmas related to care delivery,
consent,andlifesupportinseverelyinjuredpatients.o ProvideconsultationtotheEDandotherservicesintimelyfashion.o Demonstrate dress, grooming and behavior consistent with institutional
anddepartmentalguidelines.o Comply with all GME and Departmental regulations regarding duty hour
restrictionsandreportpersonalscheduleintimelyandaccuratefashion.o Appear for duty appropriately rested and fit to provide the services
requiredbytheirpatients.o Accurately self-report fatigue in situations that may compromise safety
and/orpatientcare.o Mustbecommittedtoandresponsibleforpromotingpatientsafety.o Must demonstrate responsiveness to patient needs that supersedes self-
interest.o Must recognize thatundercertaincircumstances, thebest interestsof the
patient may be served by transitioning that patient’s care to anotherqualifiedandrestedprovider.
68
METHODOFEVALUATION:• Resident fundofmedicalknowledgewillbeevaluatedannuallybysitting for the
writtenportionoftheABNSprimaryexamination.o Theyarerequiredtoobtainapassinggradeonthisexaminationduringthis
yearoftheirresidencytrainingandbecomingchiefresident(PGY7).o They are also expected to improve their percentile performance on the
ABNSprimaryexaminationeachyear.• Resident will also attend weekly didactic conferences and the monthly Journal
Club.• Conferenceattendanceandparticipationwillbereviewedanddiscussedwiththe
resident. They are required to attend at least 75% of all mandatory residentconferences.
• The senior residents who report directly to the attending surgeons will alsoevaluatethejuniorresidents.
• TheNeurosurgeryAttendingStaffreviewsResidentMedicalDocumentation.• Resident academic productivity regarding published abstracts, meeting
presentations,andpublishedmanuscripts,awards,etc.arealsoreviewed.• The resident will also be evaluated on their attainment of these goals and
objectives as well as on their performance in conferences on a quarterly basisthroughwritten evaluation of all 6 competencies (see resident evaluations) andverbalfeedbackfromtheChairmanandProgramDirector.
• Facultymembers,aseniorresident(asisappropriate),andtheNeurosurgicalNP’sevaluateallresidentsaftereachrotation.Theyareevaluatedonall6competencies(seeresidentevaluations).Theirattendanceandperformanceindidacticteachingconferences and their case logs are also reviewed. The Chairman and ProgramDirectorreviewtheseevaluationsandgiveverbal feedback to theresidentsonaquarterlybasis.
• Residents are promoted each year based on demonstration of competentperformanceofallrequirementsasoutlinedabove.
ResearchAfterdiscussionwiththeProgramDirector,DepartmentChairmanandViceChairmanforResearch,residentsmayelecttospendayearinthelaboratoryworkingonapre-designed research project. All residents prior to reaching the PGY5 yearwill havedeveloped research and investigative interests and may have begun specializedprojects. Residents will have been assigned a research mentor and may identify aresearchprojectandlaboratoryinwhichtowork.NeurosurgeryPGY6(ResidentsrotateasSeniorResidentsatTischHospitalonTeams1&2)Neurosurgery PGY6 residents must demonstrate competence in all principles ofpatient care, medical knowledge, interpersonal & communication skills, andprofessionalismaswellasinallproceduresrequiredofaNeurosurgeryPGY5residentpriortoprogressingtotheNeurosurgeryPGY6year.ThePGY6residentworksdirectlyastheprimaryassistantfortheattendingneurosurgeonsonalloperationsperformed
69
attheTischHospital.ThePGY6residentisalsoprimarilyresponsible,withattendingsupervision, for the in-patientcareandevaluationofneurosurgicalpatientsatTischHospital.AtTischHospital,seniorlevelresidentsworkwithmasterneurosurgeonsontwodistinctadultservices;(Tumor/Vascular/SkullBase/Functional/EpilepsyService)(Spine/Peripheral Services). During these rotations the residents assumemore andmoredirect responsibility and surgical opportunities in the careofprivatepatients.Surgicaltechniquesarelearnedandstandardsofcareadopted.Anattendingphysiciansupervises all Operating Room procedures performed by residents. In addition tomastering the procedures outlined below, the Neurosurgery R6 residents mustmaster:PATIENTCARE:§ Theywilldemonstratecompetenceinperformingoperativeproceduresneatlyand
carefully,respectingtissueplanesandpreservingnormalstructures.Thewillmastertheuseofphysiologicmappingtechniquesandneuronavigation(framebasedandframeless)asadjunctstosurgery.• Residentswillmasterallprioritemsonthisgraduatedlevelofresponsibilities
and program goals handout andwith appropriate supervision, residentswilllearntocompetentlyperformthefollowingprocedures:
Procedures
CraniotomyfortraumaCraniotomyfortumorprimaryandmetastaticCraniotomyforcraniofacialrepairCranioplastyFrameBasedandFramelessStereotaticbiopsiesandresectionsDBSandmotiondisorderssurgeryCarotidendarterectomyCraniotomy/microsurgicaltechniquefortumorCraniotomy/microsurgicaltechniqueforvascularlesion(aneurysmandAVM)TranssphenoidalpituitarysurgeryEndoscopicsurgeryfortumorandCSFdiversion(3rdVentriculostomy)SkullbasecraniotomyfortumorCraniotomyforposteriorfossasurgeryExtracranial/IntracranialvascularbypasssurgeryServeasprimaryinterventionalistforallINRcases,includinghighlycomplexproceduresCarotidEndarterectomyFundamentalproceduresinInterventionalNeuroradiology(includingtreatmentofaneurysms,arteriovenousmalformationsandfistulas,cranialandspinaltumorembolizations,andcarotidocclusivedisease)CraniocervicaldecompressivesurgeryLaminectomylumbarfortumor(intraandextradural)Laminectomy thoracic/cervical for decompression and resection of tumors(intradural–inc.intramedullary-andextradural)Peripheralnerverepair/decompressionAnteriorcervicalapproachtospineinc.transoral
70
AnteriorspinalinstrumentationAnterolateralspinalinstrumentationTransthoracicdecompressionofthespineRetroperitonealdecompressionofthespineTranspedicularandextracavitarydecompressionofthespineCranio-cervicalreconstructionComplexspinalreconstructionfortumor/trauma/deformityAnteriorandposteriorspinalosteotomiesfordeformityPosteriorspinalinstrumentation(cranio-cervical-thoraclumbar-sacral-pelvic)AllNeurosurgeryR3procedures
MEDICALKNOWLEDGE:• Discuss the appropriatemanagement of low back pain and spondylosis prior to
surgicalconsideration,includingPT,epiduralsteroids,painmanagement,etc.• Discussappropriatepre-operativesmokingcessationprotocols.• Discuss ASA anesthetic risk classes and appropriate pre-operative anesthesia
evaluation.• Discusscardiacischemiariskassessmentandreductionpriortosurgery.• Listtheprincipalfactorsthatinfluencesuccessfulwoundhealing.• Discuss the appropriate use of bracing in the evaluation of lumbar
spondylolisthesis/instability.• Discuss management protocols for patients on either anti-platelet or anti-
coagulanttherapyforvariousindicationspriortospinalorcranialsurgery.• Review the signs, symptoms and pathophysiology of common syndromes of
degenerative spinal disorders such as radiculopathy,myelopathy, instability andneurogenicclaudication.
• Identifythecommonsyndromesofspinalcordinjury.• Discuss the biomechanics of the craniocervical junction, cervical and
thoracolumbarspine• Discussthedefinitionofspinalinstabilityandrecognizetheradiographicsignsof
congenital,degenerative,neoplasticandtraumaticspinalinstability.• Identifytheclassicalbrainstemischemicsyndromes.• Explain the concepts of cerebral blood flow, cerebral autoregulation, ischemic
thresholds,intracranialpressureandcerebralperfusionpressure.• Recognizethecommoncausesofbrainischemicstates.• Discusstheepidemiology,physiologyandunderlyingpathophysiologyofischemic
braininjury,includingconceptsofcriticaltherapeuticwindow.• Recognize the common causes of intracranial, subarachnoid and intraspinal
hemorrhage.• Recognize the typical clinical course of patients with ischemic and hemorrhagic
stroke,includingpeakriskintervalsforedema,vasospasmandre-bleeding.• DiscussthecuttingedgepracticeofInterventionalNeuroradiology.• Discussthedifferentialdiagnosisofring-enhancingintracranialmasses.• Discussthevarioustumorsthatmayariseinthecerebellopontineangle.• Discuss the classification schemes, anatomic location, cell of origin, clinical
presentation, age at presentation, molecular biology and natural history of
71
commonintrinsicbrainneoplasms.• DiscussthepathophysiologyofParkinson’sdiseaseandessentialtremor.• Discussthebenefitsandlimitationsofframe-basedstereotacticproceduresversus
framelessstereotacticprocedures.• Discusstheclassificationoftrigeminalfacialpainanditstherapeuticimplications.• Demonstrate anunderstandingof the anatomy, physiology, pathophysiology and
presentationofperipheralnervedisease.INTERPERSONALandCOMMUNICATIONSKILLS:• They will learn how to communicate the pertinent positives and negatives of a
generalmedical and neurological examination to senior residents, neurosurgicalattendings,andconsultingphysicians.
• They will learn how to communicate critical interpretation and correlation ofclinicalandneurodiagnostic(imaging)examinationsbasedonasoundknowledgeof neurology and neuropathology to senior residents, neurosurgical attendings,andconsultingphysicians.
• They will learn to be competent in communicating with team members in thehand-overprocessinordertominimizeerrorsduringtransitionsofcare.
• TheywillpresentinweeklydidacticcaseconferencesandatJournalClub.SYSTEMS-BASEDPRACTICE:
• Residentswillbepreparedfortheregulatoryandfinancialaspectsofaclinicalpracticewhentheyfinishtheirresidency.Residentswilllearnwhatitcoststorunapracticeandbecognizantofsuchinformationas:themechanicsofbillingandcollection,diagnosticandbillingcodes,MedicareandMedicaidregulations,etc.
• Astraineesbecomemoremature iswillbe important forthemtorealizethatwehaveveryfewanswersinneurologicalsurgery.Therewillalwaysbebetterways of helping our patients: more efficient, less invasive, less morbidprocedures, alternative therapies, better instrumentation, translationalresearch, etc. In our programwe stress to residents, as they become youngneurosurgeonsthatduringtheirsubsequentcareerstheymuststriveleavethefieldbetter than they found it.During their residency theymustquestion thevalidity of every procedure we do, especially in terms of cost/benefit andpatientoutcome.Residentsareencouragedtobecreativeandusefacilitiesthatare available throughout the institution for development of instrumentation,softwaredevelopment,statisticalanalysisandbasicsciencecollaboration.
PRACTICE-BASEDLEARNING:
• Residents will learn to critically analyze the literature and presentations atmeetings.Journalarticlesandconferencepresentationsarediscussedbetweenresidents and faculty in formal “JournalClubs”, in conferences and inday-to-daydiscussionswithfacultymembers.
• TheywillparticipateinclinicalresearchprojectswhereappropriateincludingparticipatingintheIRBandconsentprocess.
• Residentswill be involved in clinicalprospective and retrospective follow-upstudiesandwilllearnthenecessarydataacquisitionandanalysistoolssothat
72
they can continue their investigations during their training and throughouttheircareers.
• Residentswilllearnthatneurosurgeryisnotinsular.Readingtheliteratureinourfieldaswellasotherdisciplineswillspawnideasforthe improvementofour techniques and practices. Development of web pages and sharingknowledge with colleagues in other countries by means of the Internetincreasestheexcitementofandenrichesourfield.
• Participation at national meetings is encouraged. Post-residency fellowshipsoverseas are also encouraged and contacts made with foreign colleaguessupportthese.Traineeswillrealizeearlyonthatneurosurgeryisinternational.
• Seniorresidentswillteach,andmentorstudentsandtheirjuniorresidents,doclinical and basic science research throughout their residency and areencouragedtopursueanacademiccareeruponcompletionoftheirtraining.
• Residents will learn that their best teachers are their patients. Much can belearnedbystudyingtheirpatients’symptoms,whetherthesearerelievedbyasurgicalprocedureorothertherapy,whatbenefittheyderivefromproceduresandatwhatcostand,ofcourse,thelong-termfollow-up.
PROFESSIONALISM:• Trainees will learn constructive collegiality with faculty, their fellow residents,
consultants and house staff from other specialties and services, but also withnursesandparamedicalpersonnel.
• Residentswilllearnhowtodealwithpatientsandfamiliesinacompassionateandhumanisticway.
• Maintain professional rapport and comportment with patient families, nurses,otherphysicianteamsandotherhospitalpersonnel.
• Demonstraterespectforpatientsandcolleaguesfromdiversecultural,ethnicandreligiousbackgrounds.
• Demonstratehonestyinallprofessionalinteractions.• Residentswillmaintaintimelyandaccuratemedicalrecords.• Residentswillalso:
o Attendallrequiredconferencesinatimelyfashion.o Pre-roundonICUpatientsandpresenttimely,accuratedatatoteam.o Participate in discussion of ethical dilemmas related to care delivery,
consent,andlifesupportinseverelyinjuredpatients.o ProvideconsultationtotheEDandotherservicesintimelyfashion.o Demonstrate dress, grooming and behavior consistent with institutional
anddepartmentalguidelines.o Comply with all GME and Departmental regulations regarding duty hour
restrictionsandreportpersonalscheduleintimelyandaccuratefashion.o Appear for duty appropriately rested and fit to provide the services
requiredbytheirpatients.o Accurately self-report fatigue in situations that may compromise safety
and/orpatientcare.o Mustbecommittedtoandresponsibleforpromotingpatientsafety.o Must demonstrate responsiveness to patient needs that supersedes self-
interest.
73
o Must recognize thatundercertaincircumstances, thebest interestsof thepatient may be served by transitioning that patient’s care to anotherqualifiedandrestedprovider.
METHODOFEVALUATION:• ResidentwillpresentatweeklydidacticconferencesandthemonthlyJournalClub.• Conferenceattendanceandparticipationwillbereviewedanddiscussedwiththe
resident. They are required to attend at least 90% of all mandatory residentconferences.
• The senior residents who report directly to the attending surgeons will alsoevaluatethejuniorresidents.
• TheNeurosurgeryAttendingStaffreviewsResidentMedicalDocumentation.• Resident academic productivity regarding published abstracts, meeting
presentations,andpublishedmanuscripts,awards,etc.arealsoreviewed• The resident will also be evaluated on their attainment of these goals and
objectives as well as on their performance in conferences on a quarterly basisthroughwritten evaluation of all 6 competencies (see resident evaluations) andverbalfeedbackfromtheChairmanandProgramDirector.
• Facultymembers,aseniorresident(asisappropriate),andtheNeurosurgicalNP’sevaluateallresidentsaftereachrotation.Theyareevaluatedonall6competencies(seeresidentevaluations).Theirattendanceandperformanceindidacticteachingconferences and their case logs are also reviewed. The Chairman and ProgramDirectorreviewtheseevaluationsandgiveverbal feedback to theresidentsonaquarterlybasis.
• Residents are promoted each year based on demonstration of competentperformanceofallrequirementsasoutlinedabove.
NeurosurgeryPGY7)(ResidentrotatesasChiefResidentsatBellevueHospitalCenterfor6months)
Over the six previous years of the training program, residents progress fromsupervisedpatient careprovidersandsurgicalassistants tocompetentpractitionerswho can function and operate independently with faculty acting as back-up.Neurosurgery PGY7 residents must demonstrate competence in all principles ofpatient care, medical knowledge, interpersonal & communication skills, andprofessionalismaswellasinallproceduresrequiredofaNeurosurgeryPGY6residentpriortoprogressingtotheNeurosurgeryR6year.Anattendingphysiciansupervisesall Operating Room procedures performed by residents. The PGY7 neurosurgicalexperience offers the residents a unique experience that is duplicated in very fewprograms in the country. During this year the residents with strict attendingsupervisiongettheopportunitytorunverybusydiverseneurosurgicalpracticeswiththe emphasis placed on the evaluation and management of neurosurgical patientsfrom the “start to finish.” This includes an extensive outpatient practice where thePGY7residenthas theprimaryresponsibility toevaluateandmanagealloutpatientneurosurgicalproblems includingemergenciesandtransfers fromother institutions.This also includes the pediatric patient population. This year allows the residents aseamlesstransitionintotheworldofafullyindependentpracticingneurosurgeon.The
74
PGY7 resident sits in with the attendings at Bellevue hospital when purchasingdecisions aremade for the clinics and the operating room. They interfacewith theother services as theprimaryneurosurgical contact. These interactions are all donewith close attending supervision but it does allow for the sense of autonomousdecision-making.Inparticular;
TheBellevueHospital chief resident,who consultswith full time faculty, runsthe neurosurgical service and functions at the level of a fully trainedneurosurgeon in this primarily elective practice. The rotation allows theresidentmoreautonomyastheyruntheneurosurgicalserviceandperformsallsurgical procedures under close faculty supervision. Bellevue exposesresidentstooutpatient,emergencypatient,andtraumapatientmanagementinadditiontoalargeelectivecaseloadinalargecityhospital.ThechiefresidentwithattendingsupervisionemploysthemethodsandhighstandardslearnedatTischHospitalandgainsconfidence,enablingheorshetobecomeacompetentindependentneurosurgicalpractitioner.
PATIENTCARE:
• Chief residentwill teach, andmentor students and their junior residents, doclinical and basic science research throughout their residency and areencouragedtopursueanacademiccareeruponcompletionoftheirtraining.
• ChiefresidentwillmanageallICUandwardneurosurgicalpatientsandobtainconsultations.
• Formulatetreatmentplansforneurosurgicalpatientsutilizingthebestavailableevidencebasedstudies.
• Discuss the appropriate use of peri-operative and chronic anti-coagulation inpatientswithcerebrovasculardisease.
• Withappropriatesupervision,residentswilllearntocompetentlyperformthefollowingprocedures:
o Craniotomyforanteriorcirculationaneurysmo CraniotomyforAVMo Craniotomyfortumor:o Carotidendarterectomyo Transsphenoidalhypophysectomyo SkullbaserepairofCSFleako Combinedsurgeryforcranialbasetumorresectionsandreconstruction
• Demonstrate an understanding of indications for surgical intervention forneurologicaldiseases.
• Providein-patientneurosurgicalconsultationwithfacultysupervision.• ProvideoutpatientneurosurgicalcliniccareatBellevuewithfacultysupervision.• Independently perform all Neurosurgery PGY5 and PGY6 procedures with
appropriatefacultysupervision.• Demonstrate the ability to recognize and treat complications related to
neurosurgical diseases and procedures, including cerebral vasospasm, CSF leak,stroke,seizure,metabolicdisorder,etc.
• Determinedischargereadinessanddirectdischargeplanning.• By the end of this year, the Chief Resident will demonstrate competence in

75
independently performing (under faculty supervision) all of the commonneurosurgical procedures performed by contemporary neurological surgeons intheUnitedStates.
• The Chief Resident will master all items on the program goals handout anddemonstrate the ability to perform independently and competently as aneurologicalsurgeon.
MEDICALKNOWLEDGE:
8. Discusstherelevantsurgicalanatomyofthebrain,spine,peripheralnervesandthe bony coverings of each, particularly as they relate to diagnosis, surgicalapproaches,andtreatmentofneurosurgicaldiseases.
9. Discussthepathophysiologyofaneurysmalsubarachnoidhemorrhage,cerebralvasospasmandcommunicatinghydrocephalusafterSAH.
10. Discussanddiscussthebleedingriskaccordingtoaneurysmtype,location,andfamilyhistoryandHunt-Hessclassification.
11. Describe the pathophysiology, classification (typological, anatomical andsurgicalgrade)andbleedingriskofarteriovenousmalformations.
12. Discussanddiscussthepathophysiologyofcarotidstenosis,TIA,RIND,stroke,reperfusionsyndrome,andchroniccerebralischemia.
13. Identify threshold levels for flow-relatedcerebral ischemia ingrayandwhitematterforelectricaldysfunctionandirreversibleneuronaldeathanddescribethe various available methodologies for measuring or clinically estimatingcerebralbloodflow.
14. Discussanddiscussthepathophysiologyofneoplasticdiseasesofthenervoussystemanditscoverings.
15. Learnanddiscussthedifferentialdiagnosisofskullbasetumorspresentinginvarious locations/compartments and the associated clinical presentations(withparticularattentiontoassociatedcranialnervedeficits).
16. Learnanddiscusscurrenttheoryinadjunctiveneuro-oncologycare,17. Learn and discuss the physiology and pathophysiology of the hypothalamic-
pituitary endocrine axis and the associated diagnostic findings in pituitarytumorpatientsandpatientswithothersellarandsupra-sellarlesions.
• Resident fundofmedicalknowledgewillbeevaluatedannuallybysitting for thewrittenportionof theABNSprimaryexamination.Theyare required toobtainapassinggradeonthisexaminationpriortocompletingtheirresidencytraining.• Residentswillmasterall itemson thisgraduated levelof responsibilitiesand
programgoalshandoutprior tocompletingresidency training.Thusallowingthem to be competent independent practitioners of Neurosurgery. Thishandoutisgiventoallresidentsandreviewedwiththemannually.
INTERPERSONALandCOMMUNICATIONSKILLS:• They will learn how to communicate the pertinent positives and negatives of a
general medical and neurological examination neurosurgical attendings, andconsultingphysicians.
• Discuss how to evaluate, work up and treat patients in the out patient clinicsetting.
76
• Discusshowtoeffectivelycommunicatewithpatientsandtheirfamiliesregardingthe patient’s diagnosis, condition, need for intervention (or not), and the risks,benefits,andalternativesofit.
• Theywilldiscusshowtoeffectivelycommunicatewithpatientsandtheirfamiliesregardingbadnewsincludingpooroutcome,death,andbraindeath.
• Theywill discuss how to communicate critical interpretation and correlation ofclinicalandneurodiagnostic(imaging)examinationsbasedonasoundknowledgeof neurology and neuropathology to senior residents, neurosurgical attendings,andconsultingphysicians.
• They will learn to be competent in communicating with team members in thehand-overprocessinordertominimizeerrorsduringtransitionsofcare.
• TheywillpresentinweeklydidacticcaseconferencesandatJournalClub.• Theywillcommunicatewithsocialwork,rehabilitationspecialists,anddischarge
planningnursestocoordinatethefollow-upandlongtermcareoftheirpatients.• Communicatewithpost-operativepatientsintheoutpatientclinicsregardingtheir
progress,prognosis,activitylevel,andreturntoworkstatus.SYSTEMS-BASEDPRACTICE:
• Coordinatethepre-operativeclearanceandschedulingofallsurgicalpatients.• Schedule the appropriate consulting surgeons andOR equipment in order to
ensureabilitytoperformtheappropriateprocedure.• Present all outpatient clinic patients to the attendings during the weekly
outpatient teaching rounds including pertinent positives and negatives andtreatmentplan.
• Coordinatetheoutpatientworkupofallpotentialsurgicalpatientsandensureappropriatefollowupfornon-surgicalpatients.
• Residentswillbepreparedfortheregulatoryandfinancialaspectsofaclinicalpracticewhentheyfinishtheirresidency.Residentswilldiscusswhatitcoststorunapracticeandbecognizantofsuchinformationas:themechanicsofbillingandcollection,diagnosticandbillingcodes,MedicareandMedicaidregulations,etc.
• Astraineesbecomemoremature iswillbe important forthemtorealizethatwehaveveryfewanswersinneurologicalsurgery.Therewillalwaysbebetterways of helping our patients: more efficient, less invasive, less morbidprocedures, alternative therapies, better instrumentation, translationalresearch, etc. In our programwe stress to residents, as they become youngneurosurgeonsthatduringtheirsubsequentcareerstheymuststriveleavethefieldbetter than they found it.During their residency theymustquestion thevalidity of every procedure we do, especially in terms of cost/benefit andpatientoutcome.Residentsareencouragedtobecreativeandusefacilitiesthatare available throughout the institution for development of instrumentation,softwaredevelopment,statisticalanalysisandbasicsciencecollaboration.
PRACTICE-BASEDLEARNING:
• Residents will learn to critically analyze the literature and presentations atmeetings.Journalarticlesandconferencepresentationsarediscussedbetween
77
residents and faculty in formal “JournalClubs”, in conferences and inday-to-daydiscussionswithfacultymembers.
• Resident fundofmedical knowledgewill be evaluatedannuallyby sitting forthe written portion of the ABNS primary examination. They are required toobtainapassinggradeonthisexaminationpriortocompletingtheirresidencytraining.
• TheywillparticipateinclinicalresearchprojectswhereappropriateincludingparticipatingintheIRBandconsentprocess.
• Residentswill be involved in clinicalprospective and retrospective follow-upstudiesandwilllearnthenecessarydataacquisitionandanalysistoolssothatthey can continue their investigations during their training and throughouttheircareers.
• Residentswilllearnthatneurosurgeryisnotinsular.Readingtheliteratureinourfieldaswellasotherdisciplineswillspawnideasforthe improvementofour techniques and practices. Development of web pages and sharingknowledge with colleagues in other countries by means of the Internetincreasestheexcitementofandenrichesourfield.
• Participation at national meetings is encouraged. Post-residency fellowshipsoverseas are also encouraged and contacts made with foreign colleaguessupportthese.Traineeswillrealizeearlyonthatneurosurgeryisinternational.
• Seniorresidentswillteach,andmentorstudentsandtheirjuniorresidents,doclinical and basic science research throughout their residency and areencouragedtopursueanacademiccareeruponcompletionoftheirtraining.
• Residents will learn that their best teachers are their patients. Much can belearnedbystudyingtheirpatients’symptoms,whetherthesearerelievedbyasurgicalprocedureorothertherapy,whatbenefittheyderivefromproceduresandatwhatcostand,ofcourse,thelong-termfollow-up.
PROFESSIONALISM:• Trainees will learn constructive collegiality with faculty, their fellow residents,
consultants and house staff from other specialties and services, but also withnursesandparamedicalpersonnel.
• Residentswilllearnhowtodealwithpatientsandfamiliesinacompassionateandhumanisticway.
• Maintain professional rapport and comportment with patient families, nurses,otherphysicianteamsandotherhospitalpersonnel
• Demonstraterespectforpatientsandcolleaguesfromdiversecultural,ethnicandreligiousbackgrounds
• Demonstratehonestyinallprofessionalinteractions• Residentswillmaintaintimelyandaccuratemedicalrecords.• Residentswillalso:
o Attendallrequiredconferencesinatimelyfashiono Pre-roundonICUpatientsandpresenttimely,accuratedatatoteamo Participate in discussion of ethical dilemmas related to care delivery,
consent,andlifesupportinseverelyinjuredpatients.o ProvideconsultationtotheEDandotherservicesintimelyfashiono Demonstrate dress, grooming and behavior consistent with institutional
78
anddepartmentalguidelineso Comply with all GME and Departmental regulations regarding duty hour
restrictionsandreportpersonalscheduleintimelyandaccuratefashion.o Appear for duty appropriately rested and fit to provide the services
requiredbytheirpatients.o Accurately self-report fatigue in situations that may compromise safety
and/orpatientcare.o Mustbecommittedtoandresponsibleforpromotingpatientsafety.o Must demonstrate responsiveness to patient needs that supersedes self-
interest.o Must recognize thatundercertaincircumstances, thebest interestsof the
patient may be served by transitioning that patient’s care to anotherqualifiedandrestedprovider.
• Residentswilllearnhowto“run”anoperatingroomincludinginstructingstaffandanesthesiacolleaguesinaneffectiveandprofessionalmanner.
METHODOFEVALUATION:• ResidentwillpresentatweeklydidacticconferencesandthemonthlyJournalClub.• Conferenceattendanceandparticipationwillbereviewedanddiscussedwiththe
resident. They are required to attend at least 90% of all mandatory residentconferences.
• TheNeurosurgeryAttendingStaffreviewstheresidentsMedicalDocumentation.• Resident academic productivity regarding published abstracts, meeting
presentations,andpublishedmanuscripts,awards,etc.arealsoreviewed• The resident will also be evaluated on their attainment of these goals and
objectives as well as on their performance in conferences on a quarterly basisthrough written evaluation of all 6 ACGME competencies (see residentevaluations)andverbalfeedbackfromtheChairmanandProgramDirector.
• Faculty members, and the Neurosurgical NP’s evaluate the residents after eachrotation. They are evaluated on all 6 competencies (see resident evaluations).Theirattendanceandperformanceindidacticteachingconferencesandtheircaselogs are also reviewed. The Chairman and Program Director review theseevaluationsandgiveverbalfeedbacktotheresidentsonaquarterlybasis.
• Residents are graduated at the end of this year based on demonstration ofcompetentperformanceofallrequirementsasoutlinedaboveandbasedonacleardemonstration that they have become competent independent practitioners ofNeurosurgery.
NeurosurgeryPGY7(ResidentsrotateasChiefResidentsattheNewYork
HarborHealthCareSystem(VA)for6months)Over the six previous years of the training program, residents progress fromsupervisedpatient careprovidersandsurgicalassistants tocompetentpractitionerswho can function and operate independently with faculty acting as back-up.Neurosurgery PGY7 residents must demonstrate competence in all principles ofpatient care, medical knowledge, interpersonal & communication skills, andprofessionalismaswellasinallproceduresrequiredofaNeurosurgeryPGY6residentprior to progressing to the Neurosurgery PGY7 year. An attending physician
79
supervises all Operating Room procedures performed by residents. The PGY7neurosurgicalexperienceofferstheresidentsauniqueexperiencethatisduplicatedinveryfewprogramsinthecountry.Duringthisyeartheresidentswithstrictattendingsupervisiongettheopportunitytorunverybusydiverseneurosurgicalpracticeswiththe emphasis placed on the evaluation and management of neurosurgical patientsfrom the “start to finish.” This includes an extensive outpatient practice where thePGY7residenthas theprimaryresponsibility toevaluateandmanagealloutpatientneurosurgicalproblems includingemergenciesandtransfers fromother institutions.This also includes the pediatric patient population. This year allows the residents aseamlesstransitionintotheworldofafullyindependentpracticingneurosurgeon.ThePGY7 resident sits inwith the attendings at theVeterans hospitalwhenpurchasingdecisions aremade for the clinics and the operating room. They interfacewith theother services as theprimaryneurosurgical contact. These interactions are all donewith close attending supervision but it does allow for the sense of autonomousdecision-making.Inparticular;
The Chief resident consults with full time faculty, runs the neurosurgicalservice at the New York Harbor Health Care System (VA) in this primarilyelectivepractice.At theVA, the chief resident supervises andmentors juniorresident, and medical students. The rotation allows the resident moreautonomy as they run the neurosurgical service and perform all surgicalproceduresunderclose faculty supervision. Theygainexposureat theVA toout patient, emergency patient management in addition to a large electivecaseloadataregionalNeurosurgicalreferralhospital.ThechiefresidentwithattendingsupervisionemploythemethodsandhighstandardslearnedatTischHospitalandgainconfidence,enablingthemtobecomecompetentindependentneurosurgicalpractitioners.
PATIENTCARE:
• Chief residentswill teach,andmentorstudentsand their junior residents,doclinical and basic science research throughout their residency and areencouragedtopursueanacademiccareeruponcompletionoftheirtraining.
• ChiefresidentswillmanageallICUandwardneurosurgicalpatientsandobtainconsultation.
• Formulatetreatmentplansforneurosurgicalpatientsutilizingthebestavailableevidencebasedstudies.
• Discuss the appropriate use of peri-operative and chronic anti-coagulation inpatientswithcerebrovasculardisease.
• Withappropriatesupervision,residentswilllearntocompetentlyperformthefollowingprocedures:
o Craniotomyforanteriorcirculationaneurysmo CraniotomyforAVMo Craniotomyfortumor:o Carotidendarterectomyo Transphenoidalhypophysectomyo SkullbaserepairofCSFleako Combinedsurgeryforcranialbasetumorresectionsandreconstruction
80
• Demonstrate an understanding of indications for surgical intervention forneurologicaldiseases.
• Providein-patientneurosurgicalconsultationwithfacultysupervision.• Provideoutpatientneurosurgicalcliniccareat theNewYorkHarborHealthCare
Systemwithfacultysupervision.• Independently perform all Neurosurgery PGY5 and PGY6 procedures with
appropriatefacultysupervision.• Demonstrate the ability to recognize and treat complications related to
neurosurgical diseases and procedures, including cerebral vasospasm, CSF leak,stroke,seizure,metabolicdisorder,etc.
• Determinedischargereadinessanddirectdischargeplanning.• By the end of this year, the Chief Resident will demonstrate competence in
independently performing (under faculty supervision) all of the commonneurosurgical procedures performed by contemporary neurological surgeons intheUnitedStates.
• The Chief Resident will master all items on the program goals handout anddemonstrate the ability to perform independently and competently as aneurologicalsurgeon.
MEDICALKNOWLEDGE:18. Discusstherelevantsurgicalanatomyofthebrain,spine,peripheralnervesand
the bony coverings of each, particularly as they relate to diagnosis, surgicalapproaches,andtreatmentofneurosurgicaldiseases.
19. Discuss the pathophysiology of aneurysmal subarachnoid hemorrhage,cerebralvasospasmandcommunicatinghydrocephalusafterSAH.
20. Discussanddiscussthebleedingriskaccordingtoaneurysmtype,location,andfamilyhistoryandHunt-Hessclassification.
21. Describe the pathophysiology, classification (typological, anatomical andsurgicalgrade)andbleedingriskofarteriovenousmalformations.
22. Learn anddiscuss thepathophysiologyof carotid stenosis, TIA,RIND, stroke,reperfusionsyndrome,andchroniccerebralischemia.
23. Identify threshold levels for flow-relatedcerebral ischemia ingrayandwhitematterforelectricaldysfunctionandirreversibleneuronaldeathanddescribethe various available methodologies for measuring or clinically estimatingcerebralbloodflow.
24. Learn and discuss the pathophysiology of neoplastic diseases of the nervoussystemanditscoverings.
25. Learnanddiscussthedifferentialdiagnosisofskullbasetumorspresentinginvarious locations/compartments and the associated clinical presentations(withparticularattentiontoassociatedcranialnervedeficits).
26. Learnanddiscusscurrenttheoryinadjunctiveneuro-oncologycare,27. Learn and discuss the physiology and pathophysiology of the hypothalamic-
pituitary endocrine axis and the associated diagnostic findings in pituitarytumorpatientsandpatientswithothersellarandsupra-sellarlesions.
• Residentswillmasterall itemson thisgraduated levelof responsibilitiesandprogramgoalshandoutprior tocompletingresidency training.Thusallowing
81
them to be competent independent practitioners of Neurosurgery. Thishandoutisgiventoallresidentsandreviewedwiththemannually.
INTERPERSONALandCOMMUNICATIONSKILLS:• They will learn how to communicate the pertinent positives and negatives of a
general medical and neurological examination neurosurgical attendings, andconsultingphysicians.
• Theywill discusshow to evaluate,workupand treatpatients in theoutpatientclinicsetting.
• Theywilldiscusshowtoeffectivelycommunicatewithpatientsandtheirfamiliesregardingthepatient’sdiagnosis,condition,needforintervention(ornot),andtherisks,benefits,andalternativesofit.
• They will also discuss how to effectively communicate with patients and theirfamiliesregardingbadnewsincludingpooroutcome,death,andbraindeath.
• Theywill discuss how to communicate critical interpretation and correlation ofclinicalandneurodiagnostic(imaging)examinationsbasedonasoundknowledgeof neurology and neuropathology to senior residents, neurosurgical attendings,andconsultingphysicians.
• They will learn to be competent in communicating with team members in thehand-overprocessinordertominimizeerrorsduringtransitionsofcare.
• TheywillpresentinweeklydidacticcaseconferencesandatJournalClub.• Theywillcommunicatewithsocialwork,rehabilitationspecialists,anddischarge
planningnursestocoordinatethefollow-upandlongtermcareoftheirpatients.• Communicatewithpost-operativepatientsintheoutpatientclinicsregardingtheir
progress,prognosis,activitylevel,andreturntoworkstatus.SYSTEMS-BASEDPRACTICE:
• Coordinatethepre-operativeclearanceandschedulingofallsurgicalpatients.• Schedule the appropriate consulting surgeons andOR equipment in order to
ensureabilitytoperformtheappropriateprocedure.• Present all outpatient clinic patients to the attendings during the weekly
outpatient teaching rounds including pertinent positives and negatives andtreatmentplan.
• Coordinatetheoutpatientworkupofallpotentialsurgicalpatientsandensureappropriatefollowupfornon-surgicalpatients.
• Residentswillbepreparedfortheregulatoryandfinancialaspectsofaclinicalpracticewhentheyfinishtheirresidency.Residentswilldiscusswhatitcoststorunapracticeandbecognizantofsuchinformationas:themechanicsofbillingandcollection,diagnosticandbillingcodes,MedicareandMedicaidregulations,etc.
• Astraineesbecomemoremature iswillbe important forthemtorealizethatwehaveveryfewanswersinneurologicalsurgery.Therewillalwaysbebetterways of helping our patients: more efficient, less invasive, less morbidprocedures, alternative therapies, better instrumentation, translationalresearch, etc. In our programwe stress to residents, as they become youngneurosurgeonsthatduringtheirsubsequentcareerstheymuststriveleavethefieldbetterthantheyfoundit.
82
• Duringtheirresidencytheymustquestionthevalidityofeveryprocedurewedo, especially in terms of cost/benefit and patient outcome. Residents areencouraged tobe creativeanduse facilities that areavailable throughout theinstitution for development of instrumentation, software development,statisticalanalysisandbasicsciencecollaboration.
PRACTICE-BASEDLEARNING:
• Residents will learn to critically analyze the literature and presentations atmeetings.Journalarticlesandconferencepresentationsarediscussedbetweenresidents and faculty in formal “JournalClubs”, in conferences and inday-to-daydiscussionswithfacultymembers.
• Resident fundofmedical knowledgewill be evaluatedannuallyby sitting forthe written portion of the ABNS primary examination. They are required toobtainapassinggradeonthisexaminationpriortocompletingtheirresidencytraining.
• TheywillparticipateinclinicalresearchprojectswhereappropriateincludingparticipatingintheIRBandconsentprocess.
• Residentswill be involved in clinicalprospective and retrospective follow-upstudiesandwilllearnthenecessarydataacquisitionandanalysistoolssothatthey can continue their investigations during their training and throughouttheircareers.
• Residentswilllearnthatneurosurgeryisnotinsular.Readingtheliteratureinourfieldaswellasotherdisciplineswillspawnideasforthe improvementofour techniques and practices. Development of web pages and sharingknowledge with colleagues in other countries by means of the Internetincreasestheexcitementofandenrichesourfield.
• Participation at national meetings is encouraged. Post-residency fellowshipsoverseas are also encouraged and contacts made with foreign colleaguessupportthese.Traineeswillrealizeearlyonthatneurosurgeryisinternational.
• Seniorresidentswillteach,andmentorstudentsandtheirjuniorresidents,doclinical and basic science research throughout their residency and areencouragedtopursueanacademiccareeruponcompletionoftheirtraining.
• Residents will learn that their best teachers are their patients. Much can belearnedbystudyingtheirpatients’symptoms,whetherthesearerelievedbyasurgicalprocedureorothertherapy,whatbenefittheyderivefromproceduresandatwhatcostand,ofcourse,thelong-termfollow-up.
PROFESSIONALISM:• Trainees will learn constructive collegiality with faculty, their fellow residents,
consultants and house staff from other specialties and services, but also withnursesandparamedicalpersonnel.
• Residentswilllearnhowtodealwithpatientsandfamiliesinacompassionateandhumanisticway.
• Maintain professional rapport and comportment with patient families, nurses,otherphysicianteamsandotherhospitalpersonnel.
• Demonstraterespectforpatientsandcolleaguesfromdiversecultural,ethnicandreligiousbackgrounds.
83
• Demonstratehonestyinallprofessionalinteractions.• Residentswillmaintaintimelyandaccuratemedicalrecords.• Residentswillalso:
o Attendallrequiredconferencesinatimelyfashion.o Pre-roundonICUpatientsandpresenttimely,accuratedatatoteam.o Participate in discussion of ethical dilemmas related to care delivery,
consent,andlifesupportinseverelyinjuredpatients.o ProvideconsultationtotheEDandotherservicesintimelyfashion.o Demonstrate dress, grooming and behavior consistent with institutional
anddepartmentalguidelines.o Comply with all GME and Departmental regulations regarding duty hour
restrictionsandreportpersonalscheduleintimelyandaccuratefashion.o Appear for duty appropriately rested and fit to provide the services
requiredbytheirpatients.o Accurately self-report fatigue in situations that may compromise safety
and/orpatientcare.o Mustbecommittedtoandresponsibleforpromotingpatientsafety.o Must demonstrate responsiveness to patient needs that supersedes self-
interest.o Must recognize thatundercertaincircumstances, thebest interestsof the
patient may be served by transitioning that patient’s care to anotherqualifiedandrestedprovider.
• Residentswilllearnhowto“run”anoperatingroomincludinginstructingstaffandanesthesiacolleaguesinaneffectiveandprofessionalmanner.
METHODOFEVALUATION:• ResidentwillpresentatweeklydidacticconferencesandthemonthlyJournalClub.• Conferenceattendanceandparticipationwillbereviewedanddiscussedwiththe
resident. They are required to attend at least 90% of all mandatory residentconferences.
• TheNeurosurgeryAttendingStaffreviewstheresidentsMedicalDocumentation.• Resident academic productivity regarding published abstracts, meeting
presentations,andpublishedmanuscripts,awards,etc.arealsoreviewed• The resident will also be evaluated on their attainment of these goals and
objectives as well as on their performance in conferences on a quarterly basisthrough written evaluation of all 6 ACGME competencies (see residentevaluations)andverbalfeedbackfromtheChairmanandProgramDirector.
• Faculty members, and the Neurosurgical NP’s evaluate the residents after eachrotation. They are evaluated on all 6 competencies (see resident evaluations).Theirattendanceandperformanceindidacticteachingconferencesandtheircaselogs are also reviewed. The Chairman and Program Director review theseevaluationsandgiveverbalfeedbacktotheresidentsonaquarterlybasis.
• Residents are graduated at the end of this year based on demonstration ofcompetentperformanceofallrequirementsasoutlinedaboveandbasedonacleardemonstration that they have become competent independent practitioners ofNeurosurgery.

84
85
PoliciesAllGMEPoliciescanbefoundherehttps://nyumc.ellucid.com/homeAdvancementPolicyAdvancementintheprogramrequires:
1. Completionofallscheduledrotationswithsupportingevaluationsinallcompetencies.GraduationisatthediscretionoftheProgramDirectorandtheClinicalCompetencyCommittee,typicallybasedupondemonstratedimprovement,and/orongoingcompliancewitharemediationorprobationplan.
2. AdvancementalongtheMilestonestothesatisfactionoftheCCCandProgramDirector.
3. R4residentsshouldtaketheABNSPrimaryExaminationforcreditduringorinspecialcircumstancespriortothatyear.
4. Completeandaccurateprocedurelogstosubstantiatefuturecredentialing.5. Completion/fulfillmentofall“credentialing”requirementswiththeseveral
hospitalsandsignoffbytheOfficeofGraduateMedicalEducation.NYUSchoolofMedicineIssuingDepartment:GraduateMedicalEducationEffectiveDate:06/10/2014ReissueDate:01/01/2016AdvancementPolicyforHouseStaffOfficersI.SummaryofPolicyNYULMCiscommittedtomeaningfulandenrichingeducationalexperiencesforitsHouseStaffOfficers.ThisincludesassurancethattheseHouseStaffOfficershavetheappropriatecredentialstoworkinaclinicalsettingandremaingainfullyemployedwhileassuringmeaningfuleducation,personalhealthandsafetyforpatients.InordertoupholdthesestandardstheNYUOfficeofGMEhascreatedtheAdvancementPolicyforHouseStaffOfficersinACGMEAccreditedandNon-ACGMEAccreditedProgramswhichoutlinesthepromotionrequirementsforeachHouseStaffOfficertoadvancetothenextprogressivelyhighertraininglevel.II.Definitions(ifapplicable)
C. House Staff Officer - a physician who is enrolled in an accredited or non-accredited NYUSoM Training Program for a clinical specialty or subspecialtythisincludesallResidentsandClinicalFellows.
D. ACGME–AccreditationCouncilforGraduateMedicalEducation
86
E. AOA–AmericanOsteopathicAssociation
F. CPME–CouncilonPodiatricMedicalEducation
G. SponsoringInstitution–NYUSchoolofMedicineandNYUHospitalsCenter
H. OfficeofGME–OfficeofGraduateMedicalEducationI. AdministrativeLOA-administrativeleaveofabsenceentailsnocreditfor
trainingandnocompensationastheResidentorFellowisnotpermittedtoworkduringthisLeaveofAbsence.
J. HouseStaffOfficer–Traineesinspecialtyandsubspecialtyprograms,
whetherornotACGME-accredited.
K. USMLESTEP3–TheUnitedStatesMedicalLicensingExaminationisathree-stepexaminationformedicallicensureintheUnitedStatesandissponsoredbytheFederationofStateMedicalBoards(FSMB)andtheNationalBoardofMedicalExaminers(NBME).TheCompositeCommittee,appointedbytheFSMBandNBME,establishespoliciesfortheUSMLEprogram.MembershipincludesrepresentativesfromtheFSMB,NBME,EducationCommissionforForeignMedicalGraduates(ECFMG),andtheAmericanpublic.
L. COMLEX-USAExam-DevelopedbytheNationalBoardofOsteopathicMedical
Examiners,COMLEX-USAisthenewsequentialthree-levelexaminationprocessforosteopathicmedicallicensureintheUnitedStates.Theexaminationprocessisinterdisciplinaryandhighlyclinical,withevenbasicsciencecomponentstestedwithinaclinicalcontext.
III.PolicyA. AdvancingHouseStaffOfficerReappointmentCriteria1. Evaluation:AdvancingHouseStaffOfficerReappointment isdependentupon
satisfactorydemonstrationof clinical competence andprofessional standardsasdeterminedbyverbalandwrittenevaluationbytheFaculty.Unsatisfactoryhouse staff officer evaluations can result in remediation, probation, andsuspensionfromdutiesorterminationofappointmentasahousestaffofficer.A full description of NYULMC’s ‘Evaluation for Residents and Fellows Policy’and‘CorrectiveActionandDisciplinaryPolicyforHouseStaff’canbeviewedatontheGMEwebsite,1underthe“PoliciesandProcedures”section.
2. Advancement Checklist: Each Advancing House Staff Officer eligible to bepromoted to the next progressively higher training level or transferring toanother training program within NYULMC will receive an electronic
87
Advancement Checklist in New Innovations prior to their respectiveadvancement date. House Staff Officers are required to complete theAdvancement Checklist before they will be allowed to advance to the nexttraining level. The requirements for advancement include completion of thefollowingitems:
a. E-LearningComplianceModulesb. HouseStaffContract
3. USMLE Step 3 or COMLEX-USA Exam: All House Staff Officers in ACGME-
accreditedprogramswithM.D.degreesmusttakeUSMLEStep3Exampriortoadvancing to their final year of residency. HouseOfficerswith aD.O. degreemaytakeeithertheUSMLEexams(Steps1,2&3)ortheCOMLEX-USAexams(Levels 1, 2 & 3) – i.e. Medicine residents must take USMLE Step 3 beforeadvancing to their third (3rd) year of residency; Surgery residents beforeadvancing to their fifth (5th) year of residency. A full description of NYULicensure Policy and USMLE requirements can be viewed at on the GMEwebsite, under the “Policies and Procedures” section. Foreign NationalGraduatesarerequiredtotakeandpassUSMLEStep3tobeeligibleforanH1BVisa.AllHouseStaffOfficersinAOA-accreditedprogramsmusttakeandpassCOMLEX3orUSMLEStep3bytheendofthePGY2yeartocontinuetraining.
4. Licensure: A valid New York Statemedical license is required for all housestaffinanon-accreditedtrainingprogram(orlimitedpermitiftheFellowisnoteligible foraLicense). (Note:Failure to takeand/orpassUSMLEStep3doesnot determine “eligibility.” See “Licensure Requirements for House Staff,”SectionsVandVI.)Thislicensemustbeobtainedbeforetrainingcanbeginandmust remain valid throughout the duration of the training program. TheResidentagreestoabidebyNYU’sLicensurePolicyinadditiontotheNewYorkStatelicensurerequirementsforphysiciansintraining,whichcanbefoundat:http://www.op/nysed.gov.NYU’s policy on licensure ismore restrictive thanthat of New York State. A full description of NYU Licensure Policy can beviewedatontheGMEwebsite,underthe“PoliciesandProcedures”section.
IV. PolicyEnforcement
J. Failuretoreceivesatisfactoryevaluations.IfaHouseStaffOfficerreceivesunsatisfactoryevaluationsandfailstoremediate,theymaybesubjecttoadelayedadvancementdateandcorrectiveand/ordisciplinaryactionmaybetakenasoutlinedinthe‘CorrectiveActionandDisciplinaryPolicyforHouseStaff’whichcanbeviewedatontheGMEwebsite,underthe“PoliciesandProcedures”section.
88
K. FailuretocompletetheAdvancementChecklist.TheOfficeofGMEwilltrackthesubmissionofalldocumentsandcompletionofallprocessestoobtainthestatusofHouseStaffOfficeradvancementandsatisfactionofallchecklistitems.IfaHouseStaffOfficerfailstocompleteallrequirementsoftheadvancementchecklistbythesetduedate,theywillberequiredtopetitiontheGMEofficeforanextensionofthedeadline,withthesupportoftheprogramdirector,inordertocontinuetrainingwithoutinterruption.
L. FailuretotakeULMLEStep3orCOMLEX-USAExam.
IfaHouseStaffOfficerfailstotakeUSMLEStep3orCOMLEX-3priortoadvancingtothelastyearofhis/herresidency,theywillbeplacedonanAdministrativeLOA.AHouseStaffOfficerplacedonanunpaidAdministrativeLOAisnotpermittedtotrainandthereforecannotreceivetrainingcreditorbepaidforthetimeoutonleave.HouseStaffOfficersinAOAAccreditedprogramswhofailtotakeUSMLEStep3orCOMLEXbytheendoftheirPGY-2yeararesubjecttonon-renewalofcontractforthePGY-3year.
M. FailuretopassUSMLEStep3orCOMLEX–USA.
IfaHouseStaffOfficerinanACGME-accreditedprogramtakestheexamandfails,he/sheshouldbeplacedonRemediation;however,theymaybepromotedandcontinuetraining.IfaHouseStaffOfficerinanAOA-accreditedprogramtakestheexamandfails,he/shewillnotbeabletoadvancetothePGY3yearandmaybesubjecttonon-renewalofcontractforthePGY-3year.
N. FailuretoObtainorRenewaLicense(Non-ACGMEandNon-AOA
AccreditedPrograms).AresidentorfellowwhofailstomaintainavalidNYSLicense(orlimitedpermit)maynotcontinuetraining.AresidentorfellowwhodoesnotrenewthevalidNYSLicense(orlimitedpermit)willbeplacedonanAdministrativeLOA.ThereareNOEXCEPTIONS.
89
BLS/ACLS/PALS/NRP/ATLStrainingPolicyNYUSchoolofMedicineIssuingDepartment:GraduateMedicalEducationEffectiveDate:07/01/2013ReissueDate:01/01/2016BLS/ACLS/PALS/NRP/ATLSTrainingPolicyforHouseStaffOfficersI.ApplicabilityofthePolicyNYUHospitalCentersBLS/ACLS/PALS/NRP/ATLScertificationrequirementsforallHouseStaffOfficersinACGMEandnon-ACGME-accreditedspecialtyandsubspecialtyprograms.II.Definitions(ifapplicable)
B. BLS–BasicLifeSupport
C. ACLS–AdvancedCardiacLifeSupport
D. PALS–PediatricAdvancedLifeSupportE. NRP-NeonatalResuscitationProgramF. ATLS–AdvancedTraumaLifeSupportG. ACGME–AccreditationCouncilforGraduateMedicalEducationH. Director – The House Staff Officer’s NYU Director of Residency or Fellowship
TrainingI. NYULMC–NYUanditsaffiliatedhospitalsJ. House Staff Officer – In this document, all references to House Staff Officers
include trainees in specialtyandsubspecialtyprograms,whetherornotACGME-accredited.
K. OfficeofGME–OfficeofGraduateMedicalEducationIII.Policy
1. TheNYUOffice of GraduateMedical Education requires the certification andmaintenanceofacurrentBLS,ACLS,PALSandNRPforallhousestaffofficersinfollowing training programs in accordance with the ACGME ProgramRequirements.
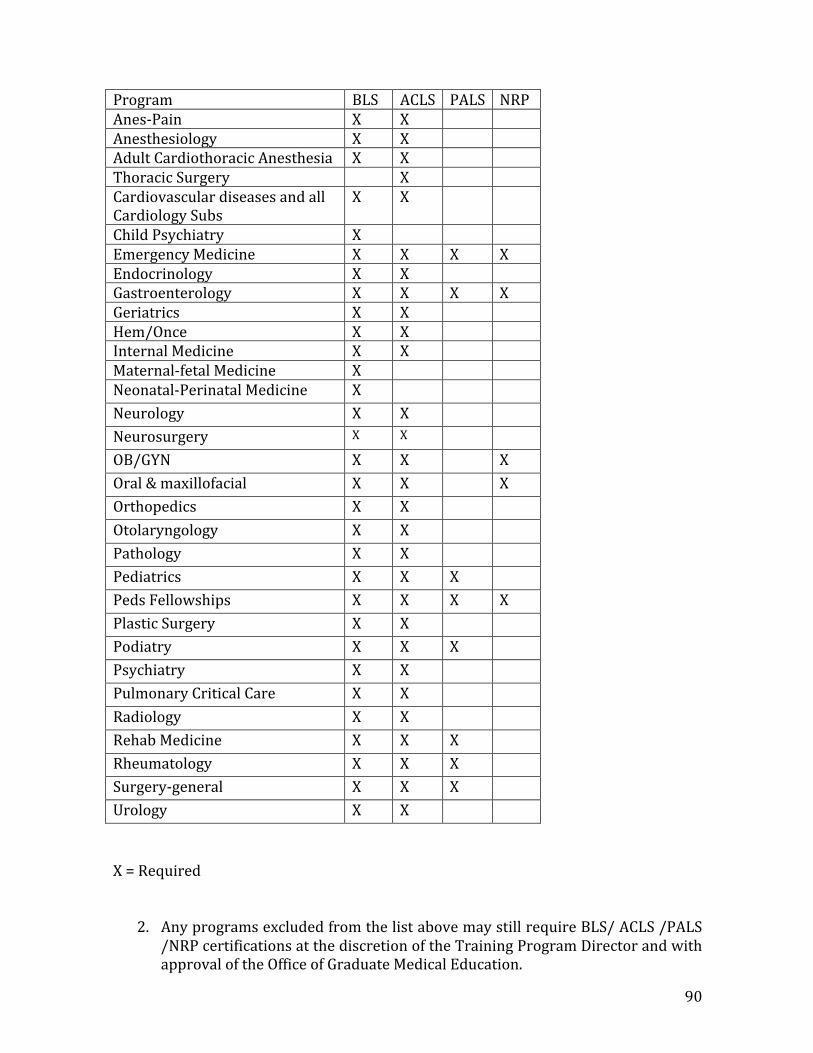
90
Program BLS ACLS PALS NRPAnes-Pain X X Anesthesiology X X AdultCardiothoracicAnesthesia X X ThoracicSurgery X CardiovasculardiseasesandallCardiologySubs
X X
ChildPsychiatry X EmergencyMedicine X X X XEndocrinology X X Gastroenterology X X X XGeriatrics X X Hem/Once X X InternalMedicine X X Maternal-fetalMedicine X Neonatal-PerinatalMedicine X Neurology X X Neurosurgery X X
OB/GYN X X XOral&maxillofacial X X XOrthopedics X X Otolaryngology X X Pathology X X Pediatrics X X X PedsFellowships X X X XPlasticSurgery X X Podiatry X X X Psychiatry X X PulmonaryCriticalCare X X Radiology X X RehabMedicine X X X Rheumatology X X X Surgery-general X X X Urology X X
X=Required
2. AnyprogramsexcludedfromthelistabovemaystillrequireBLS/ACLS/PALS/NRPcertificationsatthediscretionoftheTrainingProgramDirectorandwithapprovaloftheOfficeofGraduateMedicalEducation.
91
3. AllsurgeryresidentsmustmaintainATLScertificationinaccordancewiththe
NewYorkStateTraumaProgram.
4. All certifications and record keeping is the responsibility of each trainingprogram, and must be made available to the Office of Graduate MedicalEducationuponrequest.
5. Whenre-certificationisrequiredaspartoftheresidencyorfellowshiptraining
program, the Office of Graduate Medical Education will provide the trainingwithout cost to the Resident/Fellow. BLS/ ACLS /PALS /NRP courses areavailable free of charge for all trainees excluding those in their final year oftrainingthroughtheNYUDepartmentEmergencyMedicineTrainingDivision.
6. EachTrainingProgram is responsible for registering theirhouse staff for the
BLS/ACLS/ PALS/NRP courses. TheNYUDepartment EmergencyMedicineTraining Division will not accept registration requests submitted by housestaff.
7. Ifahousestaffofficerdoesnotattendacoursetheyhavebeenregisteredfor,
theywillbemarked,asa‘noshow’fortheclassandtheTrainingProgramwillberesponsibleforreimbursingtheOfficeofGraduateMedicalEducationforthecostofthecourse.
92
CaseLogPolicy&ProcedureWeadheretotheCaselogguidelinesoftheReviewCommitteeforNeurologicalSurgeryasfollows:AllACGMEneurologicalsurgeryresidentsarerequiredtologtheiractivitywiththeACGMEontheResidentCaseLogsystemonlineonaregularbasis.TheClinicalCompetencyCommitteereviewsthecaselogreportsonasemi-annualbasistoensurethattheresidentsaremeetingpredeterminedminimumprocedurerequirements.ResidentRole:ResidentsurgicalproceduresmustbeenteredintotheACGMECaseLogSystem.Residentsmustindicatetheirmajorroleineachcase:AssistantResidentSurgeon,SeniorResidentSurgeon,orLeadResidentSurgeon.Thedefinitionsfortheserolesare:
• Assistantresidentsurgeon:includespositioning,sterilepreparation,placementofmonitoringdevices,microscopepreparation,participationintheinitial(opening)orfinal(closing)portionsofthecase,and/orassistingtheresidentorstaffsurgeon(s)
• Seniorresidentsurgeon:mayincludeaspectsoftheabove,andmustinclude
participationinthesurgicalprocedurebetweenopeningandclosing
• Leadresidentsurgeon:mayincludeaspectsoftheabove,andmustincludeparticipationinthecriticalportionofthecase
To claim a case, a residentmust scrub in for the procedure (i.e., scrub hands, usesterile gloves,withorwithoutgown).Therecanbeseveral residentspercase,buteachresidentmayclaimonlyonerolepercase(Assistant,Senior,orLead).TherecanbeonlyoneLeadResidentSurgeonpercase,buttheAssistantandSeniorResidentrolesarenot limitedinnumberpercase.OnlythosecasescompletedintheroleofSeniorResidentSurgeonorLeadResidentSurgeonwillcounttowardstherequiredminimumCaseLognumbers.However,theReviewCommitteeexpectsthattheCaseLogdatawilldemonstrateincreasingparticipationandprogressiveresponsibility.Credit:EachresidentmayenteroneormoreCPTcodespercase,butmayclaimcreditforonlyoneCPTcodepercase.Ifmorethanoneresidentparticipatedinthesamecase,eachresidentmayclaimthesameCPTcodeforcreditforthatcaseasappropriate,aslongastheclaimedrolesarenotthesame,exceptfortheAssistantResidentSurgeonrole.Forexample,oneAssistantResidentSurgeonmayclaimaCPTcodeforcreditwhenparticipatingintheinitial(opening)portionofthecase,whileanotherAssistantResidentSurgeonmayclaimthesameCPTcodeforcreditwhenparticipatinginthefinal(closing)portionofthesamecase.Seecriticalcareguidelinesbelowforfurtherinformation.
93
PatientType:
• TheReviewCommitteedefinesapediatricpatientasonewhoislessthan18yearsoldatthetimeoftheprocedure.
• Anadultpatientisdefinedasonewhois18yearsorolderatthetimeoftheprocedure.
• Apediatricpatientwhois18yearsorolderatthetimeofafollow-upproceduremustbeloggedasanadultpatient.
SpecificCodingGuidelines:
• AirwayManagement:Therequirementfor10proceduresinthisdefinedcasecategorycanbemetbymultipleprocedures,includingintubation,tracheostomy,thoracentesis,tubethoracostomy,andbronchoscopy.BundlingofCPTcodesoccasionallypreventsagranulardescriptionofaprocedurethatisofinteresttotheReviewCommitteeandcentraltoneurologicalsurgeryeducation.Simpleintubation,nowbundledwithanesthesiaorcriticalcareprovision,isanexample.ResidentsshouldsearchunderDC26(airwaymanagement)forthefollowingcode:31575(laryngoscopy,flexiblefiberoptic;diagnostic)Thoughdirectlaryngoscopyisonlyacomponentofintubationandmaynotbeperformedfiber-optically,codingintubationinthismannerwillensureappropriatecredit.
• CriticalCare:Residentsarerequiredtolog90carecriticalprocedures.
Residentscanpaironeormoreoftheseminorprocedurecodeswiththeprimarycodeforamajorprocedureforaparticularpatientcareepisode.Forexample,ifaresidentintubatesapatient,placesacentralline,andparticipatesinalumbarfusion,heorshemaylogaprimarycodeforairwaymanagementasonecase,aprimarycodeforcentrallineplacementasaseparatecase,andaprimarycodeforthelumbarfusionasathirdcase.Otherelementsofthespinesurgerymuststillbeincludedassecondarycodeswithinthelumbarsuffusioncase.
ReviewCommitteeExpectations:Residentsgraduatingin2014-2015areexpectedtodemonstratecompliancewithallminimumnumbers,exceptforthecriticalcare(DC20-28)andendovascular(DC3b)procedures.Beginningwiththe2015-2016academicyear,allprogramgraduatesareexpectedtodemonstratecompliancewithallminimumnumberswithoutexception.
MonitoringofCaseLogs:Programsmustmonitortheaccurateandtimelyentryofcasesintothesystem.
Aspartofmonitoringresidentprogresstowardsdevelopingcompetenceinsurgicalskills,cumulativeoperativeexperiencereportsshouldbegeneratedfromtheCaseLogSystemandreviewedwitheachresidentaspartofhisorhersemiannualreview.ProgramAdministrationcompletesmonitoringofallresidentCaseLogsonamonthlybasis.Reportsaregatheredandsentto

94
ProgramDirectoronanasneededbasis.ProgramAdministrationalsomonitorsCaseLogMinimumRequirementsnotifiesProgramDirectorofanyconcernsorareaswhereresidentmayneedfulfillorbeontracktofulfillingrequirements.
95
ChiefResidentorFellowPolicyNYUHospitalsCenterIssuingDepartment:GraduateMedicalEducationEffectiveDate:07/20/2011ReissueDate:01/01/2016ChiefResidentorFellowPolicyI.SummaryofPolicyThispolicydescribestheappointmentanddutiesofaChiefResidentorFellowthatareinadditiontothoseregularlyperformedbyotherresidentsinhisorherdepartmentandpost-graduateyear.II.ApplicabilityofthePolicyAppliestoAllNYUSchoolofMedicineandNYUHospitalsCentertraineesandForeignNationalPhysiciansinACGMEandAOAaccreditedspecialtyandsubspecialtyprograms.III.Definitions(ifapplicable)
A. Chief Resident/Fellow – a senior-level resident or fellow who has beenassigned administrative and training responsibilitieswithin the residencytrainingprogram.
B. Director–medicaldirectoroftheresidency-trainingprogram.
C. ACGME–AccreditationCouncilforGraduateMedicalEducation
D. AOA–AmericanOsteopathicAssociation
E. SponsoringInstitutions–NYUSchoolofMedicineandNYUHospitalsCenter
IV.Policy
A. AChiefResidentorFellowisappointedbyhisorherDirectorandisgenerallyinhisorherfinalyearofResidencyorFellowship(e.g.,Surgery)orisworkingforanadditionalyearafterresidencyiscompleted(e.g.,InternalMedicineandPediatrics). Somepost-graduate trainingprograms require that each residentserveasChiefResidentinthelastornexttolastyearoftraining.TheDirectormaygivethetitleofChiefResidentorFellowtoasmanyresidentsinhisorherprogram as available chief differentials and perform Chief Resident duties.ProgramswithoutChiefdifferentialsarenotallowedtogivethesedutiestothehousestaff.Suchdutiesfrequentlyinclude:
96
a. supervisingandtrainingjuniorresidents;
b. developing rotation, conference, journal club, lecture, and on-call
schedules;
c. actingasaresidentliaison;
d. providingformalmedicalstudenteducation;
e. monitoringandrecordingattendance;
f. reassigningresidentsasnecessaryforcoverageissueswhenunplannedabsencesoccur(duetoillness,etc.);
g. makingdecisionsonbehalfofhisorherdepartment;and
h. performing other administrative duties as assigned by his or herDirectorofTraining(“Director”).
i. ExtraYearChiefResidentsmust complete applications for andwill beappointed to the Medical Staff at each institution (except the VA, inwhichcasetheywillremainhousestaff.)
V.Compensation
A. Eachtrainingprogramisauthorizedtoawardadditionalcompensationabovethe PGY compensation for one FTE Chief Resident per year, at the rate of$4,000 for NYU, $2,500 for NYU Lutheran and $4,162 for Bellevue(“differential”). Any program that has 10 residents ormore is authorized toaward the differential to additional Chief Residents, on the basis of one FTEdifferentialforeach10residentsinthetrainingprogram,nottoexceedatotalof10ChiefResidentsinasingleprogram.
B. In the event the number of FTE Chiefs exceeds the number of allotteddifferentials,theprogramdifferentialwillbepooledanddividedequallyamongtheChiefs. At thediscretionof theDirector, thedifferentialmaybeproratedamongChiefswhenthedurationofaChiefResident’stermofappointmentasChiefResidentislessthanoneyear.
C. TheDirectormustobtainapprovalfromtheOfficeofGMEbeforethenumberof
compensatedChiefResidentsmaybeincreasedbeyondthetotalestablishedfortheprogram.
D. Directors have the discretion to develop ChiefAppointmentpolicies for their
respectivetrainingprogramsthatismorerestrictivethanthispolicy.

97
98
ConcernsandComplaintsPolicyProgramPolicyonResidentConcernsandComplaints
Aconcernisanissue,care,trouble,ordistressthatsomeonehasaboutaresidencyorfellowshipprogramand/oritssponsoringinstitutionthatcreatesuncertaintyandapprehension.Examplesinclude:inabilitytoaccessone’sfile;fearand/orintimidationwithintheprogramorinstitution;residentwell-beingissues;untimelyverificationofresidency/fellowshipeducation;inabilitytoobtainadateforagrievancehearing;abusesofpowerordiscretion.
TheNeurologicalResidencyTrainingProgrammaintainsapolicythatmakesdiscussionregardingitsfunctioningasopenaspossibleforResidentstovoicetheirconcerns.Throughtheevaluationprocess,Residentsareabletoindicatetheiropinions,concernsandobservationsregardingtheirtraininginaconfidentialfashion.Wewillalsostrivetomaintaintheconfidentialityoftheindividualwhosubmitsaconcern.TheProgramDirector,AssociateProgramDirectorsandSiteDirectorsareallreadilyavailableandwillingtodiscussanyconcernsatanytime.IntheeventthattheResidentpreferstodiscussmatterswithsomeoneelse,facultymembersinthedivisionarereadilyavailableaswell.AnotheravenueofcommunicationisthroughyourChiefResidentsand/orProgramManagerwhocandirectyoutotheproperindividual(s)or,withyourpermissioncantransmityourconcerntotheProgramadministration.Inaddition,theAssociateDeanforGraduateMedicalEducationisalsoreadilyavailable.TheDIOisthepersoninourinstitution’sgraduatemedicaleducation(GME)officewhohasoversightoveralloftheprogramsattheinstitution.Wehaveastrictpolicyofnon-retaliationforthereportingofanyconcerns/and/orcomplaints.AnymemberoftheFacultyorthestaffwhoengagesinsuchbehaviorissubjecttodisciplinaryaction.NYUSchoolofMedicineIssuingDepartment:GraduateMedicalEducationEffectiveDate:09/16/2011ReissueDate:01/01/2016HouseStaffOfficerConcernsorComplaintsI.SummaryofPolicyTheNYUSchoolofMedicineiscommittedtomaintaininganenvironmentthatissupportiveandconducivetolearninginwhichResidents/Fellowshavetheopportunitytoraiseconcernsandprovidefeedbackwithoutintimidationor
99
retaliationandinaconfidentialmannerasappropriate.Assuch,opencommunicationwithHouseStaffOfficersisofutmostimportance.Intheeventthatanindividualwouldliketodiscussorreportaconcernorcomplaint,therearenumerousopportunitiesforresidentstodoso,eitherdirectlyoranonymously.II.ApplicabilityofthePolicyThispolicyappliestoallHouseStaffOfficersinGMEresidencyorfellowshiptrainingprogramsatNYU.III.Definitions(ifapplicable)
A. GME–OfficeofGraduateMedicalEducation
B. GMEC–GraduateMedicalEducationCommittee
C. CIR–CommitteeofInternsandResidents-BellevueHospital
D. DIO–DesignatedInstitutionalOfficial
E. Program Director – Medical director of GME specialty or sub-specialtytrainingprogram
F. HSLC-HouseStaffLeadershipCouncil
G. HSPSC–HouseStaffPatientSafetyCouncil
IV.Procedure
A. House Staff Leadership Council (HSLC) The ACGME InstitutionalRequirementsstate that theSponsoringInstitutionand itsprogramsmustprovide an environment inwhich residentsmay raise and resolve issueswithout fear of intimidation or retaliation. One forum that is required toprovide thisenvironment isanorganizationand/or forumforHouseStaffOfficers to communicate, exchange information, and discuss and addressHouse Staff Officer issues. The House Staff Leadership Council providessuch a forum, and is comprised of representatives from each trainingprogram. The Council meets monthly, and all House Staff Officers areinvitedtoattend,orareencouragedtoexpresstheircommentsorconcernstotheHouseStaffLeadershipCouncilrepresentativefromhis/herprogramto speak on his/her behalf. House Staff Leadership Council is in regularcontactwiththeDIO,andthroughhim,theViceDeanandDean/CEO.
100
B. House Staff Patient Safety Council –Any issues or concerns related toqualityand/orpatientsafetycanalsobebroughttotheHouseStaffPatientSafetyCouncil(HSPSC).TheHSPSCiscomprisedofNYUHouseStaffOfficerswhohaveaninterestinqualityandsafety.HouseStaffOfficersarewelcometobringconcernsaboutpatientsafetyorquality issues to thiscouncil,or,can ask the HSPSC representative from his/her program to speak onhis/her behalf. To contact the House Staff Patient Safety Council, pleasecontacttheOfficeofGME.
C. AnnualProgramReview –TheAnnualProgramReview,requiredby the
ACGMEandperformedannuallybyProgramleadershipmustincludeHouseStaff Officer representation from the program and must also include areviewofwritten evaluationsof theprogram,by theHouseStaffOfficers.The Annual Program Review provides time for House Staff Officers toreport any issues or concerns they may have with the training programand/orfaculty.TheseissuesorconcernswillsubsequentlybereviewedbytheAssociateDeanforGMEandtheSeniorDirectoroftheOfficeofGME.
D. ComplianceHotline(NYUHC/TischHospital)–AComplianceHotline(1-
866-NYU-1212) isalsoavailable toallmembersof the institutiontoallowfortheconfidential,anonymousreportingofactivitiesthatarecontrarytohospitalandSchoolofMedicineregulationsandpoliciessuchasviolationsof resident duty hours, and form of harassment, HIPAA violations, etc.ResidentsareremindedofandencouragedtousethisHotlineonaregularbasis.
E. Compliance Hotline (Bellevue Hospital Center) – A Medical Resident
Hotline is also available through Bellevue Hospital Center intranet(http://intranet.bellevue.org/) Click directly on Resident Hotline OnlineIssues Form. The submission form will be forwarded to pertinentdepartmentAdministrators,Chief’sofService,MedicalDirectorandothersinanefforttofacilitatetheresolutionoftheissues.
F. Incident/Error Reporting: House Staff Officers should report sentinel
events, adverse events, and/or close calls. Reporting such events is theresponsibility of all House Staff Officers, and will increase the focus onimproving patient safety, help develop changes that result in improvedoutcomes,andincreaseourreportingofadverseeventsandourawarenessofpatientsafetyissues.
a. At NYULMC: House Staff Officers are encouraged to use the Patient
SafetyIntelligence(PSI)whenworkingatanNYULMCfacility.ThePSIisweb-basedapplicationthatallowsuserstoelectronicallyreportevents.Anyone can enter an event using the PSI, and these events can bereported anonymously. The PSI Icon can be found on every clinical
101
desktop, or it canbe accessbynavigating toTheLink,2selecting “webapplications”on therighthandsideof thescreen,andclickingon“PSIforfrontlinereporter.”
b. At theManhattanVA: House Staff Officers can report events using a
web-basedreportingsystem,calledElectronicPatientEventReporting(ePER).
c. AtBellevue:Toreportevents,pleasegototheBellevueHospitalCenter
(BHC) Intranet, and click on the “Patient Safety Hotline” link on theright-handsideofthescreen.Pleasefollowallprompts.
d. AtNYULutheran:HouseStaffOfficerscanreporteventsusingMIDAS.
G. ResidentsonBellevuePayroll–WhenresidentsrotateontotheBellevue
Hospital pay line, they are also representedby aunion, theCIR,3that hasadditional avenues for the redress of grievances within its policiesdevelopedthroughcollectivebargaining.
H. ProgramDirectorand/orDIO–ResidentsmayalsocontacttheirProgram
Director,DIO/AssociateDean forGraduateMedical Education, and/or theOfficeofGraduateMedicalEducationtodiscussanyissuesofconcern.
102
CorrectiveActionandDisciplinaryPolicyNYUHospitalsCenterIssuingDepartment:GraduateMedicalEducationEffectiveDate:08/01/2013ReissueDate:01/01/2016CorrectiveActionandDisciplinaryPolicyforHouseStaffI.SummaryofPolicyThe Accreditation Council for Graduate Medical Education (ACGME) requires awritten set of policies and procedures for House Staff Officer evaluation andfor implementing corrective and/or disciplinary action when a House StaffOfficer’s performance fails to meet required standards. This includes thecriteriaforanyadverseaction,suchasplacingaresident/fellowon probationorterminating a House Staff Officer whose performance is unsatisfactory. Theprocedures are designed to be fair to House Staff Officer, patients under care,and the training program and are applicable to all House Staff Officers intraining at New York University School of Medicine (“NYU”) or any affiliatedtrainingsites.
AllfurtherreferencesinthisdocumenttoHouseStaffOfficershallincluderesidentsandfellows.
II.ApplicabilityofthePolicyThispolicyapplies toallHouseStaffOfficers, including those inACGMEandnon-ACGME- accreditedspecialtyandsubspecialtyprograms
III.Definitions
ACGME–AccreditationCouncilforGraduateMedicalEducationAOA–AmericanOsteopathicAssociation
CCC(forACGMEAccreditedPrograms)–ClinicalCompetencyCommittee,whichiscomposedofatleastthreemembersof the Program faculty andmay include faculty from other programs and non-physician membersof the health care team. For each Program, there must be a writtendescription of its CCC responsibilities, including: (a) review all residentevaluationssemi-annually;(b) prepare and assure the reporting of Milestones evaluations of eachresident semi- annually to ACGME; and (c) advise the program directorregarding resident progress, including promotion, remediation, anddismissal.
CPH – Committee on Physicians’ Health of the Medical Society of theState ofNew York
103
Director–DirectorofResidencyorFellowshiptrainingprogram
GME–OfficeofGraduateMedicalEducation
NYU–NewYorkUniversitySchoolofMedicine
OPMC–NYSOfficeofProfessionalMedicalConductOPTI-OsteopathicPostdoctoralTrainingInstitutionPTRC-ProgramandTraineeReviewCouncilattheNYULutheransiteSponsoringInstitutions-NYUSchoolofMedicineandNYUHospitalsCenter
IV.Policy
A. PerformanceDeficiencies
Upon receipt of satisfactory evaluations and compliance with all othertermsoftheHouse StaffPoliciesandProcedures,eachHouseStaffOfficershould expect to continue to the next level of training to programcompletion. If, however, a House Staff Officer’s performance isunsatisfactory, as determined by the CCC (or similar educationcommittee for non-ACGME programs), the Director shall notify theHouse Staff Officer of that conclusion, both verbally and in writing, assoon as it is determined and initiate appropriate corrective and/ordisciplinary action, as provided in Section IV.A.1., Remediation. In theordinary course, corrective and/or disciplinary action should beimposed progressively, beginning with a plan for remediation andproceeding to probation anddismissal from the program ifperformancedoes not improve. In some cases, as outlined in SectionIV.A.3, summarysuspensionmaybe appropriate. Prior to initiating any corrective and/ordisciplinary action, the Director must consult with the Associate Deanfor Graduate Medical Education and the Senior Administrative Directorfor NYU GME. In addition, the Director must inform all relevantHospital Medical Directors of any disciplinary action initiated againsttheHouseStaffOfficerunderthisSectionIV.
1. Remediation:In theevent thataHouseStaffOfficer’s performance is
unsatisfactory and summary suspension is not appropriate, theDirector, after consultation with the NYU GME, shall issue aremediation letter to the House Staff Officer, which must include adetailedplan for remediation.Copiesof the remediation letterand all subsequent administrative documentation relating to thiscorrective action shall be maintained in the Director’s and the NYUGMEfiles.
104
a. The remediation letter may include documentary evidence,
such as letters of complaint, attendance logs, reports from thelicensureboard,andother relevantdocumentsandmaterials.
b. Theremediationperiodmustbedefinedintheremediationplan.
c. The plan for remediation must include directives for
additional supervision and specific instructions with clearmeasurable educational goals and performanceexpectations.
d. TheplanshouldprovideforregularfeedbackfromtheDirector
(orDirector’s designee)totheHouseStaffOfficer.
e. In determining the appropriate plan of remediation, theDirector shall decide which action to take based on numerousfactors,suchasthenatureandseverity of the deficiency givingrise to the need for corrective action, the potential impact onpatient health or safety, the impact of the House StaffOfficer’s conduct on the program or the facility, the likelihoodthat thedeficiencycanor shall be successfully remediated, andthe degree of notice and opportunity to cure that the HouseStaffOfficerhaspreviouslyreceived.
f. Attheendoftheremediationperiod,thefollowingmayoccur:
i. Conclusion of remediation, with a statement provided
to the House StaffOfficer stating that the conditions ofremediation were satisfactorily resolved and there isno present need for further correctiveaction.Copiesofsuch statement shall be maintained in the Director’sandtheNYUGMEfiles;
ii. Continuation of remediation, provided the HouseStaff Officer has performed satisfactorily on asignificant portion of his/her plan of remediation andthe Director agrees to the assignment of an additionalterm of remediation. Continued remediation shall beapproved for a specified period of time, with aredefinition of the problems and procedures to befollowed in order to satisfy this additional term ofremediationinaccordancewiththisSectionIV;or
ii. Imposition of a term of probation as specified under
Section IV.A.2,Probation.
105
2. Probation - Following a summary suspension or the unsuccessful
completion of a plan of remediation or as deemed necessary due toone or more recurring performance deficiencies after priorremediationperiods, theDirectororhis/her designee shall place theHouse Staff Officer on probation, provided the House Staff Officer’scontinuation in the program does not constitute a serious threat tothe welfare or safety of patients, employees, or other staffmembersortotheintegrityof theprogram,asfollows:
a. TheDirectororhis/herdesigneeshallmeetwiththeHouse
StaffOfficerand presentawrittennotice,draftedinconjunctionwiththeNYUGME,stating:
i. thetermofprobation(ordinarilynottoexceedsix
months);
ii. the reasons for probation (i.e., the House StaffOfficer's specific actions or deficiencies that led tothe recommendation for probation);and
iii. the conditions of probation (i.e., what the HouseStaffOfficer shall be expected to do differently andthe specific measures the department will take toprovide the House Staff Officer the opportunity toachieve these goals). Copies of the written noticeand all subsequent administrative documentationrelating to this disciplinary action shall bemaintained in the NYU GME files. Copies of thewritten instance also shall be forwarded to allrelevant Hospital Medical Directors. The writtennotice shall advisetheHouseStaffOfficeroftherightto appeal the decision of probation as provided inSectionIV.B.,Appeals.
b. Attheendoftheprobationaryperiod,thefollowingmayoccur:
i. Termination of probation, with notice provided to
theHouseStaff Officer stating that the conditionsofprobation were satisfactorily resolved and there isno present need for further probation. Copies ofsuch statement shall be maintained in theDirector’s and the NYU GME files and forwarded toall relevant HospitalMedical Directors;
ii. Continuation of probation for an additional
specified period of timewith awritten redefinition
106
of the problems and procedures to be followed inorder to satisfy this additional term of probation inaccordancewiththisSectionIV.A.2.;or
iii. Termination of the House Staff Officer’s
participation in the residency or fellowshipprogram in accordance with Section IVA.5.,Dismissal.
c. AdecisiontoplaceaHouseStaffOfficeronprobationmay
requirereporting totheappropriateStateagency,asdiscussedinSectionIV.C.,Reporting.
3.Summary Suspension -AHouse StaffOfficermaybe summarilysuspended from participation in the residency/fellowship trainingprogrambytheDirector, the DepartmentChair,aHospitalMedicalDirector,ortheDeanoftheSchoolof Medicineorhis/herdesigneea)iftheHouseStaffOfficer’sactionsorhis/her continuedparticipationintheprogrammayconstituteathreattothewelfareorsafety ofpatients,employees,orotherstaffmembersortotheintegrityoftheprogram;orb)ifhis/herlicenseorpermitissuspendedorrevoked.WhenaHouseStaffOfficeris summarilysuspendedfromtheprogram,thefollowingproceduresshallbefollowed:
a. The Director, in conjunctionwith the NYU GME, shall provide
the House Staff Officer with written confirmation of his/hersuspension. The notice shall specify the deficiencies that gaverise to the suspension, the term of the suspension, and anyconditions that might be imposed for resuming participationin the residency/fellowship program after the period ofsuspension. Copies of this notice shall be maintained in theDirector’s and the NYU GME files. Copies shall also beforwarded to all relevant Hospital Medical Directors. Creditfor GME training shall not be given to a House Staff Officerduring a period of suspension.No compensation is earned orpaid to a House Officer during a period of suspension, buthealth insurance and professional liability insurance coverageismaintained.
b. TheHouseStaffOfficer shall be advised inwritingof the right
toappealthe suspensionasprovidedinSectionIV.B.,Appeals.
c. The House Staff Officer shall be advised in writing regardingthe program’s policy with respect to whether, upon returnfrom suspension, any academic or clinical work and/oradditional time will need to be made up, and /or completionoftrainingextendedduetothesuspensionperiod.
107
d. At the end of the suspension period, the Director, in
conjunction with the NYU GME, shall notify the House StaffOfficer in writing as to what further action, if any, is to betaken. Copies of this notice shall be maintained in theDirector’s and the NYU GME files. Copies shall also beforwarded to all relevant Hospital Medical Directors. One ofthefollowingmayoccur:
i. Termination of suspension, with a statement provided
to the House Staff Officer stating that suchsuspension occurred and there is no present need foradditionaldisciplinaryaction;
ii. Terminationof suspensionandplacementof theHouseStaffOfficer onprobationasspecifiedunderSectionIV.A.2,Probation;or
iii. TerminationoftheHouseStaffOfficer'sparticipationin
theresidency orfellowshipprogram,inaccordancewithSectionIV.A.5.,Dismissal.
d. A decision to suspend requires reporting to the appropriate
Stateagency, as discussedinSectionIV.C.,Reporting.4.DenialofAcademicCredit:
If a House Staff Officer fails to make up work missed during asummarysuspension; doesnotsatisfactorilycompleteremedialworkduring a probationary period;misses a significant component of theacademic program during leave from the program; or has otherwisefailed tomakesufficient academicprogress, theDirectormayrequiretheHouseStaffOfficerrepeatallorpartoftheacademicyear'swork.
5.Dismissal:
a. The Director shall recommend the House Staff Officer’s dismissal fromthe program to the Department Chair or Dean or his/her designee, iftheHouse StaffOfficerhas:
i. Misrepresented credentials upon which s/he had
been accepted into the program, which will not besubjecttotheappealsprocess;
ii. Engaged in conduct that threatens the welfare or
safetyofpatients, employees,orotherstaffmembersor the integrity of the residency or fellowship
108
training program, or if his/her license or limitedpermitisrevokedorsuspended;
b.Failedtomeetstandardsforacademic,clinical,orprofessionalconduct/performance, as set forth in the NYU Office of GME“EvaluationPolicyforGraduateMedicalEducation,”aftersummarysuspension o r probation.
i. The process of dismissal shall be initiated by
recommendation of the Director to the DepartmentChair after consultation with the NYU GME. TheDepartment Chair shall make the final decision todismiss in consultation with the Director and/or theDean or his/her designee and shall record therecommendationand the reasons thereofinwriting.
ii. TheHouse StaffOfficer shall receivenotice of dismissal
from the Department Chair with a copy of therecommendation for dismissal and the reasons thereof.S/healsoshall receivenoticeof his/herright toappeal,as provided in Section IV.B., Appeals. Notice of therecommendation for dismissal and all subsequentadministrative documentation relating to thisdisciplinary action shall bemaintained in theDirector’sand the NYU GME files. A copy of the notice ofdismissal shall be forwarded to all relevant HospitalMedicalDirectors.
iii. If the House Staff Officer does not request a hearing,
the recommendation for dismissal shall be final andeffective as of the date of receipt by the House StaffOfficer, and the decision to dismiss shall not besubject to further review, in accordance with SectionIV.B.,Appeals.
iv. If a House Staff Officer is dismissed before the
completion of his/her academic year, theDirector shalldetermine the number of month’s credit to be giventheHouseStaffOfficer for that academicyear.
v. A decision to dismiss requires reporting to the
appropriate State agency, as provided in Section IV.C.,Reporting.
6. TrainingExtensions
109
a. ForACGMEprograms:TheProgramhastheauthoritytoextendthehousestaffofficer’scontractforaperiodofupto1monthforleaveorillnesspurposeswithoutrequestingapprovalfromtheRRC.AllextensionsbeyondonemonthneedtobeapprovedbytheRRC.
b. ForAOAprograms:TheProgramhastheauthoritytoextendthehousestaffofficer’scontractforaperiodofupto3monthsforleaveorillnesspurposeswithoutrequestingapprovalforoverlapfromtheSpecialtyCollegeand/orPTRC.ThereisnoneedtorequesttemporaryincreaseincomplementfromthePTRCforextensionupto3months.Ifaremediationplanresultsintheextensionoftraininginexcessof3months,advancedapprovalmustbeobtainedandreportedtotheAOADivisionofPostdoctoralTraining,specialtyCollegeandOPTI.Acopymustbemaintainedinthehousestaffofficer’sfile.
B.Appeals
1. NeitherthedecisiontoplaceaHouseStaffOfficeronaplanofremediationnor theplanofremediationitselfisappealable.
2. Thedecisiontosummarilysuspend,placeonprobation,not
advance,denyacademiccredit,ordismissaHouseStaffOfficerisappealable,asfollows:
a. TheHouseStaffOfficermustsubmitawrittenrequest for
a hearing to his/her Department Chair within sevencalendardaysafterhis/herreceipt ofwrittennoticeofanappealable adverse decision or recommendation. If norequest is submitted within such seven-day period, theDirector's decision shall become final and not subject tofurtherreview.
b. The Dean or his/her designee in consultation with the
Department Chair shall appoint an ad hoc AppealsCommittee. The Appeals Committee shall consist of twoattending physicians, each of whom hold facultyappointments in the New York University School ofMedicine, and two House Staff Officers, none of whomhave had prior direct involvement in the proceedingswithrespecttotheHouseStaffOfficer.
c. The Appeals Committee shall be charged to review and
make a recommendation to theDeanorhis/herdesigneeonthefollowingissues:
110
i. Was the decision of the department or divisionmade substantially in compliance with theprocedures set forth in the Corrective Action andDisciplinaryPolicyforHouseStaffOfficers?
ii. Was the decision of the department or division
made arbitrarily and capriciously or in bad faith orin violation of anti- discrimination or other laws orregulations?
iii. It is not the role of the Appeals Committee to
substitute its academic judgment for the academicjudgment of the department or division. If theAppeals Committee determines the answer to i) isyes and the answer to ii) is no, the AppealsCommittee should uphold the decision of thedepartment or division. If the Appeals Committeedetermines that the department has failed tosubstantially comply with the procedures of theCorrective Action and Disciplinary Policy for HouseStaffOfficersor that the decision of the departmentwas made arbitrarily and capriciously or in badfaith or in violation of anti-discrimination or otherlaws or regulations, the Appeals Committee shallmakeanappropriate recommendationforremedyorreversal.
d. The Appeals Committee shall hold a hearing in a timely
fashion. The House Staff Officer shall receive at leastthree calendar days’ prior notice of the hearing. Suchnotice shall include a statement of reasons(s) for thedepartment or division’s decision to summarily suspend,placeon probation,not advance,denyacademic credit ordismiss the House Staff Officer. The Director, the NYUGME, and all relevant Hospital Medical Directors shallreceivecopiesofthenotice.
e. The Appeals Committee shall make rules it deems
necessary to assure prompt, fair, and expeditioushandling of the appeal. The Committee shall bepermitted to have legal counsel present during thehearing. The rules of law relating to the examination ofwitnesses or presentation of evidence shall not apply.Any relevant matter upon which responsible personsmay rely on the conduct of serious affairs may beconsidered.
111
f.TheAppealsCommitteeshallconductinterviewsandreviewdocuments, including medical records, as the AppealsCommittee deems necessary or helpful in its conduct of theinvestigation. A recording of all interviews shall be made.The Appeals Committee may require a physical and/ormental evaluation of the House Staff Officer in any casewhere the Appeals Committee has reason to consider thephysical or mental competency of the House Staff Officer.Appropriate consultants shall carry out such evaluation, anda report of the evaluation shall be forwarded to the HouseStaff Officer aswell as to the Appeals Committee.
g.TheAppealsCommitteeshallbeauthorizedtorecommendthatthe charges or proposed disciplinary action raisedagainst the House Staff Officerbemodified.
h. The physical presence of the House Staff Officer for whom
the hearing has been scheduled shall be required. Failureto appear without good cause shall bedeemed awaiver oftheHouseStaffOfficer’srighttothehearingprovidedinthissection, shall be considered an acceptance of an adversedecision,andisfinal.
i. At the hearing the House Staff Officer may elect to be
accompanied or represented by an attorney or otherpersonsofhisorherchoice.Therole of this representativeshall be limited to providing advice and counsel to theHouse Staff Officer; and addressing the members of theAppeals Committee. The role of the representative shallnot include the questioning of witnesses. The AppealsCommitteemay, in its discretion, furtherdefine, expand, orlimittheroleofanysuchrepresentative.
j. TheHouseStaffOfficer(orhis/herrepresentative)shallhavetheright
to present the House Staff Officer's position to the AppealsCommittee, together with such other documentation as the HouseStaff Officer may wish. The House Staff Officer may suggestwitnesses who have information relevant to the issueunderappeal.It shall be within the sole discretion of the Appeals Committee todetermineif thewitnesseswill beinterviewed.
k. Following the hearing, the Appeals Committee shallsubmit to theDean or his/her designee a written reportand recommendation, which may include arecommendation that the proposed charges ordisciplinary action be modified. The House Staff Officer
112
and theDirector, theNYU GME,andall relevantHospitalMedical Directors shall receive copies of the report fortheirfiles.
l. The Appeals Committee shall forward the record of itsproceedings and interviews to the Dean. The proceedings andrecords of the Appeals Committee and the Dean's decisionshall be, so far as possible, confidential,but shallbe retainedasaninstitutionalrecord.
TheDeanorhis/herdesigneeshallissueafinalwrittendecisionwithin seven(7)calendardaysafterreceiptoftheAppealsCommittee'sreport. TheHouseStaffOfficerandtheDirector,theNYUGME,andall relevantHospitalMedicalDirectorsshallreceivecopiesofthedecision fortheirfiles.
a. Thedecisionof theDeanorhis/herdesignee is final and,therefore,not subjecttofurtherappeal.
C.Reporting
1. Whenever the Director takes any action underSubsections IV.A.2, 3, 4 or 5, PerformanceDeficiencies,s/he shall notify the Associate Dean for GraduateMedical Education, the Senior Administrative Directorfor NYU GME, and all relevant Hospital MedicalDirectors of the action taken and the circumstancessurroundingit,aswellastheultimatedispositionofthematter.
2. Hospitals are required, under § 405.3 (e), Codes,Rules
and Regulations of New York State, to report to theOPMC any denial, suspension, restriction, termination,or curtailment of training, employment, association, orprofessional privileges or the denial of certification ofcompletion of training of any physician licensed orregistered by the New York State Department ofEducation forreasonsrelated in anywaytoanyofthefollowing
a. Alleged mental or physical impairment, incompetence,
malpractice, misconduct, or endangerment of patientsafetyorwelfare;
b. Voluntary or involuntary resignation or withdrawal of
association or of privilegeswith theHospital to avoid theimpositionofdisciplinarymeasures;and
c. The receipt of information concerning a conviction of a
113
misdemeanor or felony. The report must be made inwriting to OPMC, with a copy to the appropriate areaadministrator of the New York State Office of HealthSystems Management, within 30 days after the taking ofsuch action, andmustinclude:
1. Thenameandaddressoftheindividual;2. Theprofessionandlicensenumber;3. ThedateoftheHospital'saction;4. Adescriptionoftheactiontaken;and5. The reason for the Hospital's action or the
nature of the action or conduct which ledto the resignation or withdrawal and thedate thereof.
3. In cases involving unlicensed physicians practicing under alimited permit or serving inaclinical fellowshiporresidency, theHospitalmustreporttotheNew YorkStateEducationDepartmentOfficeofProfessionalDiscipline.
4.All licensed health professionals, including physicians, arerequiredbystatelaw toreportcolleagueswhomtheysuspectmaybeguiltyofmisconductasdefined in New York State law. Failureto report suspected instances of misconduct is, in itself,misconduct.ForphysiciansandHouseStaffOfficersaffiliatedwithahospital, the report can be made to the hospital’s Chief MedicalOfficer, whowill then inform OPMC; in the case of a House StaffOfficer,thereportmaybemade to theProgramDirector, theDIO,the Senior Administrative Director for NYU GME, and/or allrelevant Hospital Medical Directors. If the colleague is notaffiliated with a hospital, a report can be made to the countymedical society, which will be responsible for reporting toOPMC. If a health professional is uncertain whether specificactions or behaviors constitute misconduct, s/he may requestadvice fromOPMCwithoutrevealingthenameof thepractitioner.Once adviceisprovided,thehealthprofessionalwhorequestedtheadviceisrequiredto followit.
5.Practitionerssuspectedofhavingproblemswithalcohol,drugs,ormental illness,
butwhoseabilitytopracticeisnotimpaired,maybe reported to theCommitteeon Physicians’ Health of the Medical Society of the State of New York (CPH).All calls are confidential. CPH identifies, refers to treatment and monitorsimpaired physicians. The program is voluntary and participation isconfidential. The names of physicians participating in the program are notsharedwithOPMC without aparticipant’s approvalunless there is a failure tocomply with treatment recommendations. A physician whose medicalperformance may be impaired, however, alsomust be reported toOPMC.The
114
law does not exempt physicians from their duty to report colleaguespracticing with a suspected impairment to OPMCbecause theyhave reportedtoCPH.
6.Nothing in this policy relieves the institution of its obligations toreport incidents of possible professional misconduct under applicablelawsandregulations. The resultsofdrugoralcoholtestingandmattersrelated thereto shall bekept confidentialexcepttotheextentnecessarytoimplementthispolicy.
7.APlanforRemediationneednotbereported.
115
DisasterPolicyNYUSchoolofMedicineIssuingDepartment:GraduateMedicalEducationEffectiveDate:05/16/08ReissueDate:01/01/2016DisasterPolicyI.PolicyPurposeTo define the basic procedures and assigned responsibilities to efficiently andeffectivelyreconstitute and restructure the resident training experiencefollowing a disaster or a set ofsignificant events, and/or interruption inpatientcare.NYU SoM strives to provide a stableeducationalenvironmentforHouseStaffOfficersandtoprovideguidelinesforadministrativecontinuityandmaintenanceofthecriticalteachingmissionoftheNYUSoM.
When disasters occur elsewhere we will attempt to take on displaced residentsfrom otherprogramswhen feasible. Inorder to credentialHouseStaffdisplaceddue tonaturalorotherdisasters. TheGMEmayaccept amodified list ofcredentials, agreeduponby theDIO, theDirector, and the SeniorAdministrativeDirector of GME of the host institution.Under allcircumstances,itistheresponsibilityoftheGMEtocredentialdisplacedHouseStaff.
II.ApplicabilityofthePolicyAllTrainees,includingthoseinACGMEandnon-ACGMEaccreditedspecialtyandsub-specialtyprogram.III.Definitions(ifapplicable)A.NYUHC–NYUHospitalsCenterB.NYUSoM–NewYorkUniversitySchoolofMedicineC.GMEC–GraduateMedicalEducationCommitteeD.GME–OfficeofGraduateMedicalEducationE.ACGME–AccreditationCouncilforGraduateMedicalEducationF.DIO–ACGMEDesignatedInstitutionalOfficialG.IRIS–MedicareGMEReimbursementSystem–Intern&ResidentInformationSystemH.Disaster–Aneventorsetofeventscausingsignificantalterationtotheresidencyexperienceatoneormoreresidencyprograms.I.Director–MedicalDirectoroftheACGME-accreditedornon-accreditedspecialtyorsub-specialtyprogram.J.HouseStaffOfficer–Traineesinspecialtyandsubspecialtyprograms,whetherornotACGME-accredited.V.Responsibilities
116
A.GMEC’sResponsibilities
1.TheGMEC is responsible for assuring that all graduatemedicaleducationprogramsandDirectorsareawareofandcomplywith thispolicyand formonitoringprogram-specificcontingencyplanningforadisasterorinterruptioninpatientcare.
B.NYUSoM’sResponsibilities
1.AllNYUSoMsponsoredgraduatemedicaleducationDirectorsareresponsibleforimplementing this policy as it pertains to program-specific disastercontingencyplanningandtocommunicationwiththeOfficeofGraduateMedicalEducation,ACGME,andHouseStaffOfficersregardingtemporaryand/orpermanenttransfers.
C.DIOandGMEResponsibilities
1.The N Y U SoM Designated Institutional Official to the ACGME andthe N Y U SoMGraduateMedical Education Program staff are responsiblefor working withdisaster-affectedprograms and Directors to reconstituteor reconfigure the educationalexperience forresidentsandclinicalfellows.
IV.Procedure
1.Priortoanyexpectedemergencyplanningforananticipatedemergency(i.e.ahurricaneorstorm)theDIOwillestablishcommunicationwithallprogramsandprovideongoingcommunicationandinstructions.
2.Immediately after a disaster or interruption in patient care, eachgraduatemedicaleducation program affected by the disaster orinterruption, under thedirectionof itsDirector,andincollaborationwiththeDIOandtheOfficeofGraduateMedicalEducation,willundertakeall reasonablemeasures toascertain thewhereaboutsof itstrainees and ensure their safety. If trainees are in immediatedanger, theDirector, incollaborationwiththeDIOandOfficeofGME,willcoordinateallreasonablemeasuresavailabletotheNYUSoMtoremovetraineesfromharmandreturnthemtosafety.
3.Communication: Consistent with the NYU Emergency Operations Plan,informationconcerning disaster operations can be found atwww.med.nyu.edu.TheOffice ofGraduateMedicalEducationwillserveasacommandcenterforHouseStaffOfficersandProgramDirectorsduringadisaster.IntheeventthattheNYUwebsiteoremailisnotavailable,alternatemeansofcommunicationsuchascellphones,personalemailsmaybeused,includingsocialmedia.NYUSOM/HospitalmayalsouseSendWordNow(SWN)asameansofemergencycommunicationtocellphonesusingtext,voiceandemailmessaging.Tohelpensuretheeffectivenessoftheircommunications,allHouseStaffarestronglyencouragedtoupdatetheir
117
emergencycontactcellphonenumbersinPeopleSoft.
4.Assoonaspossibleafterthedisasterorinterruptioninpatientcare,theDIOwillnotifytheACGMEofthenatureanddetailsofthedisasterortheinterruption.TheExecutiveDirectorofACGMEwithconsultationof theACGMEExecutiveCommitteeand theChairoftheInstitutionalReviewCommitteewilldecideifthedisasterreportwarrantsadeclarationofdisasterbytheACGME.ShouldtheACGMEdeclareadisaster,anoticewillbe posted on the ACGME website, with informationrelating to theACGMEresponsetothedisaster.TheDIOwillmonitorthisinformationandmaintainongoingcommunicationswiththeACGME.
5.Following declaration of a disaster or an interruption in patient care,the DIO,andOfficeofGraduateMedicalEducation,workingwiththeGMEC,andotherNYUSoMadministrationwillworktorestructure,reconfigureorreconstitutetheeducationalexperience for traineesenrolled in N Y U SoM sponsored graduate medicaleducationprogramsaffectedbythedisasterorinterruption,asquicklyaspossible.6.Within tendays after a declaration of disaster is issuedby theACGME,theDIOorhis/her designeewill contact theACGME to discuss the duedates that theACGMEwillestablishforeachaffectedprogramto:SubmitproposedprogramreconfigurationsforreviewbytheACGMEInformeachHouseStaffOfficerofatransferdecision
7.Transfera.If the DIO determines that the N Y U SoM sponsored graduate medicaleducationprogram(s) affectedby thedisaster or interruption in patient care cannot berestructuredorreconstitutedtoprovideanadequateeducationalexperienceforHouseStaffOfficers,oriftheprogramcannotberestructuredorreconstitutedwithinanappropriate time frame toallowHouseStaffOfficers tocomplete their trainingprogramrequirementswithinthestandardtimerequiredforcertificationwithintheirspecialty,thentheDIOworkingincollaborationwiththeDirector(s),theOfficeofGraduateMedicalEducation,andNYUSoMadministrationwill:
i. Arrangetemporarytransferstootherprograms/institutionsuntilsuchtimeasthetrainingprogramcanprovideanadequateeducationalexperienceforeachofitsHouseStaffOfficers.
ii. Cooperate in and facilitate temporary/permanent transfers tootherprograms/institutions.Programs/institutionswillmakethekeep/transferdecisionexpeditiously so as to maximize the likelihood thateach resident will timelycompletethetrainingyear.
iii. AMemorandumofUnderstanding(MOU)willbecreatedforeachrotating
118
Institutiontowhichourtraineesarebeingdisplaced.
b.Informeachtransferredtraineeoftheminimumdurationofhis/hertemporarytransfer,andcontinuetokeepeachtraineeinformedoftheminimumduration.Ifandwhenaprogramdecidesthatatemporarytransferwillcontinuetoand/orthroughtheendofatrainingyear,itmustsoinformeachsuchtransferredtrainee.
c.During the period of time thatNYU trainees spend in temporary transferat thehostprogram,NYUandaffiliateswillcontinuetoprovidesalary,travel,andbenefitstothetrainee,consistentwithapplicablelaw.
8.NYUSoMtrainees,who,asaresultofthedisasterorinterruptioninpatientcare,temporarilytransfertoothertrainingprograms,willbeprovidedbytheirDirectorswithabestestimate of the duration of time that relocation tothe host programwillbenecessary.Shouldthetimeatthehostprogramneedtobeextended,theHouseStaffOfficerswillbenotifiedby theirDirector(s)usingwrittenorelectronicmeans, indicating theestimateddurationoftheextension.
9.TheDIOwillbetheprimaryinstitutionalcontactwiththeACGMEandtheInstitutionalReviewCommitteeExecutiveDirector regardingdisasterplanimplementationandcommunication regarding specific graduatemedicaleducationneedswithin N YU SoM. TheDIOwillcalloremailtheInstitutionalReviewCommitteeExecutiveDirectorwithinformation and/or requests forinformation as specified intheACGME Policies andProceduremanual.Communications fromDirectors to theACGMEwillbedirectedbyphone oremail to the appropriate ReviewCommittee Executive Director.Communicationsfromresidents/clinical fellowstotheACGMEalsowillbedirectedtotheappropriateReviewCommitteeExecutiveDirector.
10.IndividualNYUsponsoredgraduatemedicaleducationprogramswilltakeresponsibilityfor establishing contingency plans and procedures to addresscontinuationof programleadership, evacuation planning, relocation,programrecovery,maintenance ofcommunicationandworkingwithaffiliates in the eventofadisasteror interruption inpatientcareandcoordinateallplansthroughtheGraduateMedicalEducationOffice.
11.IndividualNYUsponsoredgraduatemedicaleducationprogramswill,totheextentpermittedbyavailableresourcesandprogrampersonnel,protecttheacademicandtrainingfilesofresidentsorclinicalfellowsfromlossordestructionbydisaster.
12.AdministrativeSupport
a.All temporary Disaster Relief rotations to other institutionsmust bemaintained in
NewInnovations.
119
b.Intheeventofadisaster,communicationbetweentheSeniorAdministrativeDirectorof Graduate Medical Education, the DIO, ChiefMedical Officers ofNYUTischHospitalandtheaffiliateinstitutions,GeneralCounsel,andtheViceDeanofHumanResourceswillbe initiated tomobilizeHouseStaff. DuringadisasterHouseStaffcanobtaincurrentinformationontheNYUEmergencyManagementwebsite:http://central.nyumc.org/clin/admin/E-MGMT/Pages/home.aspxaswellastheEmployeeEmergencyInformationHotline:212-263-2002.CommunicationsmayalsobesenttoallHouseStaffusingSendWordNow(SWN),viatext,voiceoremailmessaging.
13.DisplacedResidentsFromOtherPrograms
a.Ifsalaryandsupportwillcontinuetobeprovidedbyhomeinstitution,thentheHouse
Staffwillonlyneedtosubmitthefollowing:i. In-ElectiveForm,Request,andAgreementii. HouseStaffApplicationiii. ProofofapprovalofDirector&DIOfromhostinstitution
b.IftheHouseStaffistobeemployedinadditiontotheabove,thenecessaryemploymentpaperworkmustbe submitted, following thecredentialingchecklist ofNYUSoM.
c.IfthedisplacedHouseStaffwasintheaccreditedprogramattheirhomeinstitution,the corresponding accreditedprogramatNYUSoMand NYU Lu theran Med i ca l c en ter must requestACGMEpermission totemporarilyhostdisplacedHouseStaff.
14.RecordKeeping
a. DocumentationofalltemporaryassignmentsmustbemaintainedforGMEreimbursementpurposes.
b. RotationassignmentsforalltraineesmustbeenteredandtrackedinNewInnovationstoappropriatelycapturetheFTEdataforIRIS.
120
NeurosurgeryDutyHourPolicyItisthepolicyoftheDepartmentofNeurologicalSurgerytofullycompllywithboth405regulations,i.e.NewYorkStateregulations(whichareineffectforNewYorkUniversityHospitalsCenterandBellevueHospitalCenter),aswellasACGMEregulations,i.e.nationalregulations(whichareineffectfortheNewYorkCampusoftheDepartmentofVeteransAffairsNewYorkHarborHealthcareSystem).TheProgramDirectordiscussesdutyhourregulationswiththeResidentsnumeroustimesthroughoutthedurationofthetrainingProgram,startingwithorientation,andateachofsemiannualindividualmeetingswitheachresident.HealsoreviewstheseregulationswithfacultymembersatfacultyandProgrammeetingsandduringhisday-to-dayrunningoftheProgram.Thisisalsodoneinthecontextofteachingabouttheadverseeffectsoffatigue.Theprogramdirector,sitedirectors,andclinicalservicechiefsareaccountableforensuringstrictcompliancewithallworkhourspolicies..ThefacultyareaskedtoassessdutyhourcomplianceandfatiguewitheachResidentrotatingonallclinicalservicesTheGMECommitteereceivesperiodicreportsonworkhourcompliance as part ofthe QA process. Duty hours are defined as all clinical andacademicactivitiesrelatedtotheeducationalprogram:patientcare,bothinpatientandoutpatient,administrative duties related to patient care, the provision for transfer ofpatientcare,timespentin-houseduringcallactivities,timespentoffsiteengaginginathomecallactivities,andscheduledacademicactivitiessuchasconferences.Dutyhoursdonotincludereadingandpreparationtimespentawayfromthedutysite.TheNYU-DepartmentofNeurologicalSurgeryfullysupportstheResidentWorkHourLimitationsestablishedbyNewYorkState405Regulations, theNeurologicalSurgeryResidencyReviewCommitteeandtheACGME.Moonlighting isstrictlyprohibitedby theNYUDepartmentofNeurologicalSurgery.MinimumTimeOffbetweenScheduledDutyPeriodsisasfollows:
o PGY-1 residents should have 10 hours, and must have eight hours, free of
dutybetweenscheduleddutyperiods.
o Intermediate-level residents (PGY 2-5) should have 10 hours free of duty,andmusthaveeighthoursbetweenscheduleddutyperiods.Theymusthaveatleast14hoursfreeofdutyafter24hoursofin-houseduty.
o Residentsinthefinalyearsofeducation(PGY6-7)mustbepreparedtoenter
the unsupervised practice of medicine and care for patients over irregularorextendedperiods.
o This preparation must occur within the context of the 80- hour,
121
maximum duty period length, and one-day-off-in- seven standards.While it is desirable that residents in their final years of educationhave eighthours freeofdutybetweenscheduleddutyperiods, theremay be circumstances when these residents must stay on duty tocare for theirpatientsorreturntothehospitalwithfewerthaneighthours free of duty. The site directors and the program directorstrictly monitor circumstances of return-to-hospital activities withfewer than eight hours away from thehospitalbyresidents in theirfinalyearsofeducation.
MaximumFrequencyofIn-HouseNightFloat:
NYU Department of Neurological Surgery does not participate in in-HouseNightFloat
MaximumIn-HouseOn-CallFrequency
PGY-2residentsandabovemustbescheduledforin-housecallnomore
frequentlythanevery-third-night(whenaveragedoverafour-weekperiod).
At-HomeCallo Timespentinthehospitalbyresidentsonat-homecallmustcounttowardsthe
80- hourmaximumweekly hour limit. The frequency of at-home call is notsubject tothe every-third-night limitation, butmust satisfy the requirementforone-day-in-sevenfreeofduty,whenaveragedoverfourweeks.
o At-home call must not be so frequent or taxing as to preclude rest or
reasonablepersonaltimeforeachresident.
o Residents are permitted to return to the hospital while on at-home call tocarefor
o neworestablishedpatients.Eachepisodeofthistypeofcare,whileitmust
beincludedinthe80-hourweeklymaximum,willnotinitiateanew“off-dutyperiod”.
o Verbal inquiresaremadeby the, sitedirectors,andclinical servicechiefs,or
by The program director regarding if the At-home call was so taxing as topreclude rest or reasonable personal time for the resident. If this is thecase resident is instructed to return home (car fare is provided) and not toreturn until the next schedule duty period at which point they are re-evaluated.
Ourdepartmentinaccordancehasimplementedprocedurestorelieveapostgraduatetraineeduetofatigue(seeFatiguePolicy).Stressandfatiguecanbeeitherself-reportedorobservedbyother trainees, or responsibleattending staff.All of our residentsandfacultyarerequiredtotakeonlinetrainingmodulestoenablethemtorecognizeunduestressorfatigueinthemselvesorothers.Adequatebackupthroughqualifiedphysicianextenders or supervising attending
122
physicians is always available and is utilized asneeded toassure thatpatientcare isnot jeopardizedby resident stressor fatigue.Astressedorfatiguedresidentisinstructedtoreturnhome(carfareisprovided)andnottoreturnuntilthenextscheduledutyperiodatwhichpointtheyarere-evaluated.ThefacilitiesaffordedtheresidentsatNYUaretheretoensureanappropriateenvironment for learning and providing patient care. This includes food servicecapabilities during assigned duty hours and suitable on-call rooms suitable foreachresidentonnightdutyinthehospital.Dutyhoursaresubmitted for institutional reviewonabi-annualbasis(forthemonthsofAprilandOctober)withplansofcorrectioninstitutedforanyviolations.Theyarereviewedasacomponentoftheresident’sprofessionalismduringtheresidentsemi-annualreviews.Theprogramexpects100%compliancefromallHouseStaff.All duty hours violations should be reported immediately to the site directors,program director,ChiefResidentorprogrammanager. If need be, they can bereported anonymously to the compliancehotlinesasbelow:
HowToReportDutyHourViolationsatNYU:AnanonymousNYULMCComplianceHotlinehasbeenestablishedandisavailable24
hoursaday7daysaweek.Forquestionsorconcerns,facultyandstaffcancallthemultilingualhotlineandobtainatrackingnumber.IssuesandconcernsareforwardedtotheOfficeofComplianceforfollow-up.TheComplianceHotlinenumberis(866)-NYU-1212.
HowToReportDutyHourViolationsatBellevue:TheBellevueResidentHotlinecanbefoundontheBellevueIntranetHomePage.Thishotlineiscompletelyanonymous.Onthelefthandside:
1. Select“PatientSafetHotline”2. Then,gotothe“blue”section3. Selecteitheroneofthe
following:“Patientrelatedissues”“Residentrelatedissue”“Supplyrelatedissue”“Other”
4. fillinthefieldsAself-selectedpassword isrequiredsoyoucan follow-upontheresponse toyourcomplaint.
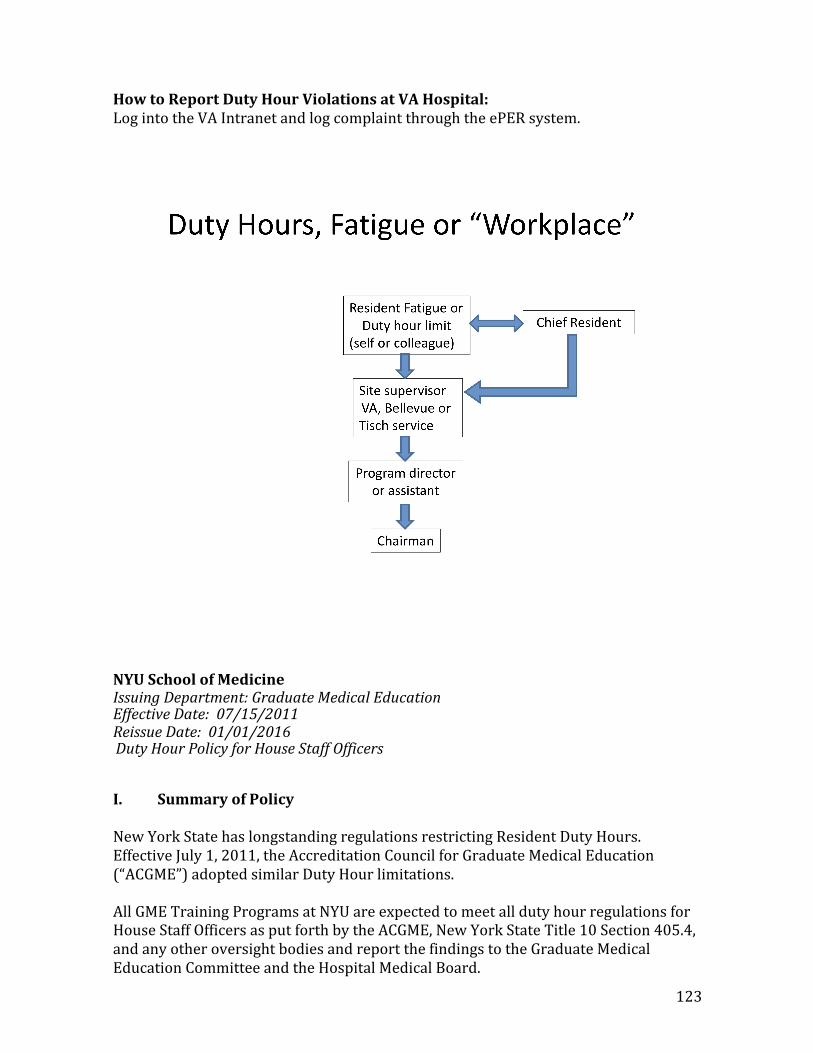
123
HowtoReportDutyHourViolationsatVAHospital:LogintotheVAIntranetandlogcomplaintthroughtheePERsystem.
NYUSchoolofMedicineIssuingDepartment:GraduateMedicalEducationEffectiveDate:07/15/2011ReissueDate:01/01/2016DutyHourPolicyforHouseStaffOfficersI.SummaryofPolicyNewYorkStatehaslongstandingregulationsrestrictingResidentDutyHours.EffectiveJuly1,2011,theAccreditationCouncilforGraduateMedicalEducation(“ACGME”)adoptedsimilarDutyHourlimitations.AllGMETrainingProgramsatNYUareexpectedtomeetalldutyhourregulationsforHouseStaffOfficersasputforthbytheACGME,NewYorkStateTitle10Section405.4,andanyotheroversightbodiesandreportthefindingstotheGraduateMedicalEducationCommitteeandtheHospitalMedicalBoard.
124
Initspolicyrequirements,theACGMEstates:4
Programsandsponsoringinstitutionsmusteducateresidentsandfacultymembersconcerningtheprofessionalresponsibilitiesofphysicianstoappearfordutyappropriatelyrestedandfittoprovidetheservicesrequiredbytheirpatients.Theprogrammustbecommittedtoandresponsibleforpromotingpatientsafetyandresidentwellbeinginasupportiveeducationalenvironment.Theprogramdirectormustensurethatresidentsareintegratedandactivelyparticipateininterdisciplinaryclinicalqualityimprovementandpatientsafetyprograms.Thelearningobjectivesoftheprogrammust:
beaccomplishedthroughanappropriateblendofsupervisedpatientcareresponsibilities,clinicalteaching,anddidacticeducationalevents;and,notbecompromisedbyexcessiverelianceonresidentstofulfillnon-physicianserviceobligations.
Theprogramdirectorandinstitutionmustensureacultureofprofessionalismthatsupportspatientsafetyandpersonalresponsibility.Residentsandfacultymembersmustdemonstrateanunderstandingandacceptanceoftheirpersonalroleinthefollowing:
a. assuranceofthesafetyandwelfareofpatientsentrustedtotheircare;
b. provisionofpatient-andfamily-centeredcare;
c. assuranceoftheirfitnessforduty;
d. managementoftheirtimebefore,during,andafterclinicalassignments;
e. recognitionofimpairment,includingillnessandfatigue,inthemselvesand
intheirpeers;
f. attentiontolifelonglearning;
g. themonitoringoftheirpatientcareperformanceimprovementindicators;
and,
h. honest and accurate reporting of duty hours, patient outcomes, and
clinicalexperiencedata.
4 https://www.acgme.org/acgmeweb/GraduateMedicalEducation/DutyHours.aspx
125
Allresidentsandfacultymembersmustdemonstrateresponsivenesstopatientneedsthatsupersedesself-interest.Physiciansmustrecognizethatundercertaincircumstances,thebestinterestsofthepatientmaybeservedbytransitioningthatpatient’scaretoanotherqualifiedandrestedprovider.
Inthisdocument,allreferencestoHouseStaffOfficersarelimitedtotraineesinACGME,AOA,andCPMEaccreditedspecialtyandsub-specialtyprograms.II.ApplicabilityofthePolicyThispolicyappliestoHouseStaffOfficersenrolledinallNYUHospitalsCenterspecialtyandsub-specialtytrainingprograms.III.Definitions(ifapplicable)
A. ACGME–AccreditationCouncilforGraduateMedicalEducation
B. AOA–AmericanOsteopathicAssociation
C. Call– a) At-Home Call (or pager call) is call taken from outside the assigned
institution;b) In-House Call is comprised of Duty Hours beyond the normal workday,
whenHouseStaffOfficersare required tobe immediatelyavailable in theassignedinstitution.
D. CPME-CouncilonPodiatricMedicalEducationE. ProgramDirector–DirectorofResidencyorFellowshipTraining
F. DutyHours– Includeall clinical andacademicactivitiesof theResident; i.e.,patient care (both inpatient and outpatient), administrative duties related topatient care, transfer of patient care, time spent in-house on-call, scheduledacademicactivitiessuchasconferences,andanymoonlightingactivities.DutyHoursdonotincludereadingandpreparationtimespentawayfromthedutysite.
G. NYULMC–NewYorkUniversitySchoolofMedicineandNYUHospitalsCenterH. Residents orHouse Staff Officers – All trainees enrolled in NYU Hospitals
CenterACGME,AOA,orCPME-accreditedspecialtyandsub-specialtytrainingprogramsthatinvolveclinicalduties.
126
I. FatigueManagement – Recognition by either a resident or supervisor of alevelofresidentfatiguethatmayadverselyaffectpatientsafetyandenactmentofasolutiontomitigatethefatigue.
J. Strategic napping – Short sleep periods, taken as a component of fatigue
management,whichcanmitigatetheadverseeffectsofsleeploss.
K. External Moonlighting – Voluntary, compensated, medically-related workperformedoutsidetheinstitutionwheretheresidentisintrainingoratanyofitsrelatedparticipatingsites.
IV.Policy
A. Monitoring and Reporting Procedures - Duty hours must be entered intoNew Innovations for aminimum of four weeks, twice over the course of anacademicyear(AprilandOctober).Allprogramsmusttrackdutyhoursduringtheserequiredtrackingtimes.Programscanindividuallyrequiremoretrackingbecompletedwithintheirprograminadditiontothesesetperiodsoftime.
1. Eachresidentisresponsiblefordirectentryofhonestandaccuratereporting of their own duty hour information into the NewInnovations(NI)system.
2. New Innovations will allow programs the option to establish anautomatedemailannouncementtobesenttoallresidentswhohavenot completed their duty hour calendar for the specified period oftime.
3. A global set of duty hour types are available to all programs toensurereporteddataisconsistentacrossprograms.
4. Programs should appropriately remediate any residents or fellowswhodonotenterDutyHoursintoNewInnovations
5. Program Directors are responsible for reviewing all duty hourviolationsreportedduringthetworequiredmonitoringperiods.TheProgramDirectorwill“sign-off”onallviolationswherethisoptionisavailable.
6. The Program Director should review all violations, and makeadjustments to program schedules or processes when recurrentviolationsarenoted.
7. Consecutivereportingperiodswillgeneratearequired‘PerformanceImprovementPlan’ tocorrect thedeficiency tobesubmitted to theDIOandreportedtotheGMECbytheProgramDirector.
8. TheGMEOfficeutilizesastandardreport fromNewInnovationstotrack data relating to both reporting compliance and duty hourviolationsandreporttotheGMEC,andtheGMECwillreporttotheHospitalMedicalBoardsforthetworequiredmonitoringperiods.
127
B. Regulations-NewYorkCodes,RulesandRegulations(NYCRR),Title10,Section405.4, and ACGME Final Requirements, “Resident Duty Hours Language,”promulgate Duty Hour restrictions in order that theworking conditions andhours of House Staff Officers promote the provision of quality medical care.TheregulationsestablishthefollowinglimitsonResidentDutyHours:
C. MaximumHoursofWorkperWeek–Dutyhoursmustbelimitedto80hoursper week, averaged over a four week period, inclusive of all in-house callactivitiesandallmoonlighting
D. DutyHourExceptions–AlthoughaReviewCommitteemaygrantexceptionsfor up to 10% or a maximum of 88 hours, the GMEC has determined theycannotapproveanyrequestssincetheywouldbeinconflictwiththeNYSDutyHourRegulations.
i. Moonlighting
1. Moonlightingmustnotinterferewiththeabilityoftheresidenttoachievethegoalsandobjectivesoftheeducationalprogram.
2. Time spent by House Staff Officers in Internal and ExternalMoonlighting must be counted towards the 80-hour MaximumWeeklyHourLimit.
3. PGY-1HouseStaffOfficersarenotpermittedtomoonlight.
4. HouseStaffOfficersonJ-1Visas.
ii. MandatoryTimeFreeofDuty–HouseStaffOfficersmustbescheduledforaminimumofonedayfreeofdutyeveryweek(whenaveragedoverfourweeks). At-homecall cannotbeassignedon these freedays.HouseStaffOfficersmayonlyworkatotalof12consecutivedays.
iii. MaximumDutyPeriodLength
1. Duty periods of PGY-1 House Staff Officers must not exceed 16hoursinduration.
2. Duty periods of PGY-2 House Staff Officers and above may bescheduled to a maximum of 24 hours of continuous duty in thehospital. Programs must encourage House Staff Officers to usealertness management strategies in the context of patient careresponsibilities. Strategic napping, especially after 16 hours ofcontinuous duty and between the hours of 10:00 p.m. and 8:00a.m.,isstronglysuggested.
a. It is essential for patient safety and House Staff Officerseducation effective transitions in care occur. House StaffOfficers may be allowed to remain on-site in order toaccomplishthesetasks;however, thisperiod,referredtoas
128
transitionaltime,mustbenolongerthananadditionalthreehours.
b. HouseStaffOfficersmustnotbeassignedadditionalclinicalresponsibilitiesafter24hoursofcontinuousin-houseduty.
c. Inunusualcircumstances,HouseStaffOfficers,ontheirowninitiative,mayremainbeyondtheirscheduledperiodofdutytocontinuetoprovidecaretoasinglepatient.Justificationsforsuchextensionsofdutyarelimitedtoreasonsofrequiredcontinuity for a severely ill or unstable patient, academicimportance of the events transpiring, or humanisticattentiontotheneedsofapatientorfamily
i. Under those circumstances, the House Staff Officermust:
a. Appropriately hand over the care of all otherpatients to the team responsible for theircontinuingcare;and,
b. Document the reasons for remaining to care forthe patient in question and submit thatdocumentation in every circumstance to theprogramdirector.
iv. MinimumTimeOffbetweenScheduledDutyPeriods
1. PGY-1House Staff Officers should have 10 hours, andmust haveeighthours,freeofdutybetweenscheduleddutyperiods.
2. Intermediate-levelHouseStaffOfficers [asdefinedby theReviewCommittee]shouldhave10hoursfreeofduty,andmusthaveeighthoursbetweenscheduleddutyperiods.Theymusthaveatleast14hoursfreeofdutyafter24hoursofin-houseduty.
3. House StaffworkingER shiftsmustnot exceed12hours of duty,must have 12 hours off between shifts. Transitional time is notallowed.
4. HouseStaffOfficers in the finalyearsofeducation [asdefinedbythe Review Committee] must be prepared to enter theunsupervised practice of medicine and care for patients overirregularorextendedperiods.
a. Thispreparationmustoccurwithinthecontextofthe80-hour, maximum duty period length, and one-day-off-in-seven standards. While it is desirable thatHouse Staff Officers in their final years of education
129
haveeighthoursfreeofdutybetweenscheduleddutyperiods,theremaybecircumstances[asdefinedbytheReview Committee] when these House Staff Officersmuststayonduty tocare for theirpatientsorreturnto the hospital with fewer than eight hours free ofduty.
v. MaximumFrequencyofIn-HouseNightFloat
1. House Staff Officers must not be scheduled for more than sixconsecutivenightsofnightfloat.
2. [Themaximumnumber of consecutiveweeks of night floats, andmaximumnumberofmonthsofnightfloatperyearmaybefurtherspecifiedbytheReviewCommittee.]
vi. MaximumIn-HouseOn-CallFrequency
1. PGY-2 House Staff Officers and above must be scheduled for in-house call no more frequently than every-third-night (whenaveragedoverafour-weekperiod).
vii. At-HomeCall
1. TimespentinthehospitalbyHouseStaffOfficersonat-homecallmustcounttowardsthe80-hourmaximumweeklyhourlimit.Thefrequency of at-home call is not subject to the every-third-nightlimitation, butmust satisfy the requirement for one-day-in-sevenfreeofduty,whenaveragedoverfourweeks.
i. At-homecallmustnotbesofrequentortaxingastoprecluderestorreasonablepersonaltimeforeachresident.
2. HouseStaffOfficersarepermitted to return to thehospitalwhileon at-home call to care for new or established patients. Eachepisode of this type of care,while itmust be included in the 80-hourweeklymaximum,willnotinitiateanew“off-dutyperiod”.
V. PolicyEnforcement
A. Violation ofDutyHour Limitations -Noncompliancewith NYCRR, Title10, Section 405.4, and/or ACGME requirements for Duty Hours in theLearning and Working Environment is a breach of policy that couldjeopardize the accreditation status of the Resident’s program and subjectNYUtoconsiderablefinancialpenalties.
130
B. Disciplinary Action - Refer to the NYU GME “Corrective Action andDisciplinary Policy for House Staff” for relevant disciplinary action policyandprocedureforcompliance.
VI.RelatedPolicies(ifapplicable)
A. CorrectiveActionandDisciplinaryPolicyforHouseStaffB. AlertnessManagement/FatigueMitigation
VII.LegalAuthority/References(ifapplicable)
A. NYCRR,Title10,Section405.4B. ACGME Requirements for Duty Hours in the Learning and Working
Environment
131
EvaluationPolicyTheNYUDepartmentofNeurosurgeryResidencyProgramevaluatesallfacultyandtraineesusinganobjectiveassessmentofcompetenceinthe6ACGMEcompetenciesofpatientcare,medicalknowledge,practice-basedlearningandimprovement,interpersonalandcommunicationskills,professionalism,andsystems-basedpractice.OurevaluationsareperformedusingtheNewInnovationssystem.TimelyevaluationsareassuredthroughtheNIsystem,whichautomaticallysendsreminderstoevaluatorsuntilevaluationsarecompleted,whichiscurrentlysetonaquarterlybasis.AllresidentsareprovidedaccesstoevaluationsviaNIinade-identifiedformatandfeedbackdiscussedatbothsemi-annualreviewmeetings.TheClinicalCompetencyCommitteereceivesfeedbackonasemi-annualizedbasisduringfacultyreviewmeetingsconductedwiththeChairoftheDepartment.NYUSchoolofMedicineIssuingDepartment:GraduateMedicalEducationEffectiveDate:07/01/2013ReissueDate:01/01/2016EvaluationforResidentsandFellowsI.SummaryofPolicyTheAccreditationCouncilforGraduateMedicalEducation(ACGMEandtheAmericanOsteopathicAssociation(AOA)requireawrittensetofpoliciesandproceduresforresidentandfellowevaluation.Theproceduresaredesignedtobefairtoresidents/fellows,patientsundercare,andthetrainingprogramandareapplicabletoallresidents/fellowsintrainingatNewYorkUniversitySchoolofMedicine/NYUHospitalsCenter(“NYU”).Allresidentsandfellowsmustbeevaluatedatleastsemi-annually.Aresidentwhoseperformanceisdeemedlessthansatisfactoryshouldbenotifiedofthatconclusion,bothverballyandinwriting,assoonasitisdetermined,inaccordancewiththeprovisionsoftheCorrectiveActionandDisciplinaryPolicyforHouseStaff.Allfurtherreferencesinthisdocument,toresidentsshallincludefellows.II.Definitions
A. ACGME–AccreditationCouncilforGraduateMedicalEducation
B. Director–DirectorofResidencyorFellowshiptraining
C. GME–NYUGraduateMedicalEducationOffice
D. NYU–NYUHospitalsCenter
E. AOA–AmericanOsteopathicAssociation
132
F. Sponsoring Institutions- NYU School of Medicine and NYU Hospitals
Center
III.Evaluation
TheprogramdirectormustappointtheClinicalCompetencyCommittee(CCC)fortheACGMEprogramortheMedicalEducationCommittee(MEC)forAOAprograms.
• At a minimum the Clinical Competency Committee or MedicalEducation Committee must be composed of three members of theprogramfaculty.
• Others eligible for appointment to the committee include faculty from other
programsandnon-physicianmembersofthehealthcareteam.
TheremustbeawrittendescriptionoftheresponsibilitiesoftheClinicalCompetencyCommittee.TheClinicalCompetencyCommitteeshould:
• Reviewallresidentevaluationssemi-annually;
o PrepareandassurethereportingofMilestonesevaluationsofeachresidentsemi-annuallytoACGME;and,• Advisetheprogramdirectorregardingresidentprogress,including
promotion,remediation,anddismissal.FormativeEvaluationTheFacultymustevaluateresidentperformanceinatimelymannerduringeachrotationorsimilareducationalassignment,anddocumentthisevaluationatcompletionoftheassignment.Theprogrammust:
• Provideobjectiveassessmentsofcompetenceinpatientcareandproceduralskills,medicalknowledge,practice-basedlearningandimprovement,interpersonalandcommunicationskills,professionalism,andsystems-basedpracticebasedonthespecialty-specificMilestones;
• Usemultipleevaluators(e.g.,faculty,peers,patients,self,andother
professionalstaff);
133
• Document progressive resident performance improvement appropriate toeducationallevel;and
• Provideeachresidentwithdocumentedsemiannualevaluationof
performancewithfeedback,ormorefrequentlybasedonACGMEprogramrequirements.AOAaccreditedprogramsmustalsodocumentformativefeedbacktointernsonaquarterlybasis.
• Theevaluationsofresidentperformancemustbeaccessibleforreviewbythe
resident,inaccordancewithinstitutionalpolicy.
SummativeEvaluation
• The specialty-specificMilestonesmust beused as one of the tools to ensureresidentsareable topracticecoreprofessionalactivitieswithoutsupervisionuponcompletionoftheprogram.
• Theprogramdirectormustprovideasummativeevaluationforeach
residentuponcompletionoftheprogram.Thisevaluationmust:
• Becomepartoftheresident’spermanentrecordmaintainedbythe
institution,andmustbeaccessibleforreviewbytheresidentinaccordancewithinstitutionalpolicy
• Documenttheresident’sperformanceduringthefinalperiodof
education;and,
• Verifythattheresidenthasdemonstratedsufficientcompetencetoenterpracticewithoutdirectsupervision.
Residents’Rights-Evaluationsmaintainedintheresident’sdepartmentfilemustbeaccessibletotheresident.Ifaresidentdisagreeswithorelectstocommentonstatementsincludedinawrittenevaluationinhis/herfile,theresidenthastherighttosubmitawrittenresponse,whichshallbecomepartoftheresident’sdepartmentfile.BasisforEvaluations-Eachresidentshallbeevaluatedbasedonwrittenandoralfeedbackfromfaculty,peers,patients,self,andotherprofessionalstaffatNYULMCandallaffiliatedsites.Evaluationsshallbebasedonthewrittengoalsandobjectivesoftheresidency/fellowshipprogramandontheassessmentofaresident'sspecificknowledge,skills,andattitudesineachofthefollowingareas:
I. Professionalcompetence,clinicalperformance,andjudgmentincluding,butnotlimitedto:
134
a)PatientcareandProceduralskills–Residentsmustbeabletoprovidepatientcarethatiscompassionate,appropriate,andeffectiveforthetreatmentofhealthproblemsandthepromotionofhealth.b)Medicalknowledge-Residentsmustdemonstrateknowledgeofestablishedandevolvingbiomedical,clinical,epidemiologicalandsocial-behavioralsciences,aswellastheapplicationofthisknowledgetopatientcare c)Practice-basedlearningandimprovement-Residentsmustdemonstratetheabilitytoinvestigateandevaluatetheircareofpatients,toappraiseandassimilatescientificevidence,andtocontinuouslyimprovepatientcarebasedonconstantself-evaluationandlife-longlearning d)Interpersonalandcommunication-Residentsmustdemonstrateinterpersonalandcommunicationskillsthatresultintheeffectiveexchangeofinformationandcollaborationwithpatients,theirfamilies,andhealthprofessionals.e)Professionalism-Residentsmustdemonstrateacommitmenttocarryingoutprofessionalresponsibilitiesandanadherencetoethicalprinciples.f.)Systems-basedpractice-Residentsmustdemonstrateanawarenessofandresponsivenesstothelargercontextandsystemofhealthcare,aswellastheabilitytocalleffectivelyonotherresourcesinthesystemtoprovideoptimalhealthcare.g.)OsteopathicPhilosophy,PrinciplesandManipulativeTreatment(AOAProgramsONLY)-AOAresidentsareexpectedtounderstandandapplytheosteopathicprinciples(OPP)appropriatetothecareofpatients.
Compliancewithestablishedpractices,rules,regulations,procedures,andpoliciesofNYU.
1.Completionandverificationofeducationalandtrainingrequirements.
a. CompliancewithstandardsofprofessionalconductassetforthinNewYorkStatelawand/orapplicablecodesofprofessionalethics.
b. Inaddition,theresidentshould:
135
• Developapersonalprogramoflearningtofostercontinuedprofessionalgrowthwithguidancefromtheteachingstaff;
• Participatefullyintheeducationalandscholarlyactivitiesoftheirprogram
• and,asrequired,assumeresponsibilityforteachingandsupervisingotherresidentsandstudents;
2. Participateinappropriateinstitutionalcommitteesandcouncilswhoseactions
affecttheireducationand/orpatientcare;
3. Submittotheprogramdirectorortoadesignatedinstitutionalofficialat• leastannually,confidentialwrittenevaluationsofthe
facultyandoftheeducationalexperiences.• Eachresidentalsomustparticipateactivelyinscholarly
activity.Scholarshipisdefinedasoneofthefollowing:Thescholarshipofdiscovery,asevidencedbypeer-reviewedfundingor publicationoforiginalresearchinpeer-reviewedjournals.
4. Thescholarshipofdissemination,asevidencedandinaccordancewiththe
following:
Allresidentsarerequiredtohavesubmittedforpublicationsatleast2articles:annually:Thismayincludepeerreviewarticles,editorialarticles,researchrelatedarticles,and/orbookchapters
Residentpresentationatregional,ornationalprofessionalandscientificsocietymeetings(e.g.cases,reportsorclinicalseries)isencouraged.
5. Activeparticipationinclinicaldiscussions,rounds,journalclubs,andresearch
conferencesinamannerthatpromotesaspiritofinquiryandscholarship;theofferingofguidanceandtechnicalsupport(e.g.,research
• design,statisticalanalysis)forresidentsinvolvedinresearch;andtheprovisionofsupportforresidentparticipation,asappropriate,inscholarlyactivities.
136
FatigueMitigationPolicyNew York University Neurosurgery Program, in compliance with the New YorkState Department of Health Regulations and ACGME program requirements,requiresthatallresidentsbemonitoredforsignsoffatigue.ItistheresponsibilityoftheProgramDirector, site directors, and clinical service chiefs tomonitor the on-callandassignmentschedulesofallpostgraduatetraineestoensurethatresidentsarereceivingampletimefor rest, in compliance with NYS and ACGME duty hourregulations. Our programeducatesall ofour facultyand residents about the signsand symptoms of fatigue and methods of fatigue mitigation to manage thepotential negative effects of fatigue on patient care and learning by using theSleep, Alertness, and Fatigue Education in Residency [SAFER] on lineeducational resources found on the NYU GME website Sleep, Alertness, andFatigueEducationinResidency(SAFER).Any post-graduate trainee who is experiencing fatigue should immediately notifyhis/herprogram of his/her state of fatigue. Likewise, when a program director,site directors, or clinical service chiefs, or chief residents determine or identifythat a resident is too fatigued to perform his/her duties effectively, the programdirectorwillarrangefortheresidenttobetemporarilyrelievedfromallon-callandclinical duties. Adequate backup through qualified physician extenders orsupervising attending physicians is always available and is utilized as needed toassure that patient care is not jeopardized by resident stress or fatigue and toensure continuity of patient care in the event that a resident may be unable toperform his/her patient care duties. Adequate sleep facilities options areprovided for fatigued residents but, in general a stressed or fatigued resident isinstructed to return home (car fare is provided) and not to return until the nextscheduleduty period atwhich point they are re-evaluated. It is the responsibilityof the Program Director / designee to notify the appropriate individuals of thechangeintheon-callandclinicalassignmentschedule.As stated in the duty hours policy, all duty hours violations should be reportedimmediatelytothesitedirectors,programdirector,ChiefResident,and/orprogrammanager.Ifneedbe,theycanbereportedanonymouslytothecompliancehotlinesaslistedabove.PleasenotethisisthedepartmentalpolicywhichissupplementaltotheinstitutionalpolicylistedbelowNYUSchoolofMedicineIssuingDepartment:GraduateMedicalEducationEffectiveDate:09/16/2011ReissueDate:10/31/2014AlertnessManagement/FatigueMitigationI.PolicyPurpose
137
In2010,theAccreditationCouncilforGraduateMedicalEducation(ACGME)setnewstandardsforHouseStaffOfficerwell-beingbasedonrecommendationsmadebytheInstituteofMedicine(IOM).Oneofthenewstandardswastheneedtosetmorespecificrequirementsforalertnessmanagementandfatiguemitigationstrategiesdesignedtoensurecontinuityinbothpatientcareandresidentsafety.II.ApplicabilityofthePolicyAppliestoHouseStaffOfficersenrolledinallNYUHospitalsCenterspecialtyandsub-specialtytrainingprograms.III.Definitions(ifapplicable)A. GME–OfficeofGraduateMedicalEducationB. ACGME–AccreditationCouncilforGraduateMedicalEducationC. IOM-InstituteofMedicineIV.Policy
A. TheGMETrainingProgrammust:a. Educate all facultymembers andHouse Staff Officers to recognize the
signsoffatigueandsleepdeprivationi. This educationmust be given to all program faculty and housestaff officers via the Sleep Alertness and Fatigue Education inResidency(SAFER)module.ThiswillpartiallysatisfytheACGMErequirements.
b. Educate all faculty members and House Staff Officers in alertnessmanagementandfatiguemitigationprocesses;
ii. AllHouseStaffofficersandProgramFaculty,mustcompletetheSAFER online tutorial on Sleep Alertness and FatigueManagementonIDevelop.
c. Adopt fatigue mitigation processes to manage the potential negativeeffectsof fatigueonpatientcareandlearning,suchasnapsorback-upcall schedules.
B. EachprogrammusthaveaformalprocesstoensurecontinuityofpatientcareintheeventthataHouseStaffOfficermaybeunabletoperformhis/herpatientcareduties.Thisprocessmustbecommunicatedtoprogramtraineesandfaculty.
C. Thesponsoring institutionmustprovideadequate sleep facilitiesand/or safetransportation options for House Staff Officers who may be too fatigued tosafelyreturnhome.

138
139
ImpairmentPolicyNYUHospitalsCenterIssuing Department:Graduate MedicalEducationEffectiveDate:09/01/2013Policy Name: ImpairmentPolicyforResidentsandFellowsI. SummaryofPolicyThe AccreditationCouncil for Graduate Medical Education (ACGME) requires awritten policyandprocedure foraddressing resident and fellow impairment. Theprocedures aredesigned tobe fair toresidents/fellows, patients under care,andthe training program andareapplicable toallresidents/fellows intrainingatNewYorkUniversitySchoolofMedicine(“NYU”).Allfurtherreferences inthisdocument, toresidentsshallincludefellows.II.DefinitionsACGME–AccreditationCouncilforGraduateMedicalEducationCPH–CommitteeonPhysicians’HealthoftheMedicalSocietyoftheStateofNewYorkDirector–DirectorofResidencyorFellowship trainingprogramGME–OfficeofGraduateMedical
Education
NYU–NewYorkUniversitySchoolof
MedicineOPMC–NYSOfficeof
ProfessionalMedicalConduct
HouseStaffOfficer -aphysicianwho isenrolled inanaccredited ornon-accredited NYUSoMTraining Program foraclinical specialty orsubspecialty thisincludes allResidents andClinicalFellows.III.PhysicianImpairmentIf, at anytime,the Directorhasreasonablecauseto suspectthata resident’sbehaviorisaltered because of aphysical ormental impairment or the use ofdrugs, narcotics, or alcohol,theresidentshall,attheDirector’s request, submittoaphysicaland/ormentalexaminationbyanursepractitioner and/orphysician(s)
140
acceptable totheNYUHospitalsCenterEmployeeHealthService.Reasonablecauseshallinclude,butnotbelimitedto:• unsatisfactory, excessive,ordeterioratingattendancerecord;• unexplainedabsences;• missedappointments,• decliningproductivityorotherunsatisfactoryperformance,
• accosting,striking,orassaultinganemployee,patient,orvisitorother
thaninself-defense;• returningto work followingparticipationin a drug or alcohol
rehabilitationprogramorleaveofabsence;• unkemptappearance,poorhygiene;trembling,slurredspeech;bloodshotor
blearyeyes;• complaints orallegations ofimpairment byanyone interactingwiththe
housestaffofficer;• arguments,bizarrebehavior;• irritability,depression,moodswings,irresponsibility;• poormemory,poorconcentration;• unexplainedaccidentsorinjuriestoself;• neglectoffamily,isolationfromfriends;• DWIarrest,DUIviolations,oranyotherarrestinvolvingdrugsoralcohol;• financialand/orlegalproblems;• unavailabilitybypager,phoneoremail;• unexplainedroundingatirregulartimes;• lossofinterestinprofessionalactivities,socialorcommunityaffairs;• neglect of patients, incomplete charting, or neglect of other clinical
oracademicresponsibilities;• inappropriate treatmentordangerousorders;• excessiveprescriptionwriting;• unusuallyhighdosesorwastagenotedindruglogs;• noticeabledependencyonalcoholordrugstorelievestress;• intoxicationatsocialeventsorodorofalcoholonbreathwhileonduty;or• any other behavior which suggests that the employee may be unfit for
work orwhichmaybereasonablyattributable totheuseofdrugs,narcotics,oralcohol.
TheDirectorshall,priortomakingsuchrequest,consultwiththeNYUGME.Thepurposeoftheexamination(s) shallbetodetermine iftheresident is free fromhealthimpairments whichposepotentialrisktopatientsorpersonnelorwhichmayinterferewiththeperformanceoftheresident’s clinical duties. Theexaminationshall include, but not be limited to, a breathalyzer,urinalysis,blood,and/orothersimilarteststodetermine ifdrugs,narcotics, and/oralcoholareintheresident’s system.Uponrequesting afitness fordutyexamination, the
141
Directormustexplaintothe housestaff officerthat failureto undergosuchexaminationwhen requestedshall begrounds for immediatesuspensionand/or dismissal from the training program in accordancewith theprovisionsofCorrective Action andDisciplinary Policy Section IV.A.4, SummarySuspension, andSectionIV.A.5,Dismissal.Pending and following medical evaluation, the resident may be placed on amedical leave ofabsence,administrativelyreferredfor further evaluationandrecommendedtreatment,and/orsubjecttodisciplinary actionuptoandincluding termination oftheresidency inaccordancewithThe CorrectiveActionand DisciplinaryPolicy. The Director shall consult with the NYU GMEprior toany decisionsregardingmedicalleaveof absence,treatmentreferralordisciplinaryaction.IV.ReportingHospitals are required to report to theNewYork State Office ofProfessionalMedical Conduct(OPMC)wheneverany of the followingactionsare taken forreasonsrelatedin any way toallegedmentalorphysical impairment:denial, suspension, restriction, termination, orcurtailment of,orvoluntary orinvoluntary resignation orwithdrawal from, training, employment,association,orprofessionalprivileges,orthedenialofcertificationofcompletionoftraining.Alllicensedhealthprofessionals, includingphysicians, arerequiredbystatelawtoreportcolleagues whom they suspect may be practicing while impaired.Failure to report is, in itself,professionalmisconduct.For attendingphysicians,the report can be made to the hospital’schief medical officer, who must theninform OPMC; in the case of residents and fellows, thereport should bemadeto the Program Director or the Senior AdministrativeDirector for NYUGME,whomusttheninformOPMC.Physicianssuspectedofhavingproblemswithalcohol,drugs,ormentalillness,butwhoseability to practice is not impaired, may be reported to theCommittee on Physicians’ Health oftheMedical Society of the State ofNew York(CPH). All calls are confidential. CPH identifies,referstotreatment,andmonitorsimpairedphysicians.Theprogramisvoluntaryandparticipationisconfidential.Thenamesofphysiciansparticipating intheprogramarenotsharedwith OPMC without a participant’s approval unless there is a failure to complywith treatmentrecommendations. AreferraltoCPHdoesnotexemptphysiciansfromtheirdutytoreportcolleaguespracticingwithasuspectedimpairment toOPMC.Nothingin this policyrelievesthe institutionof its obligationsto reportincidentsof possibleprofessional misconduct under applicable lawsandregulations.The results ofdrugoralcoholtesting andmatters related theretoshall bekept confidential except to theextent necessary toimplementthispolicy.

142

143
NeurosurgeryMoonlightingPolicyTheNYUSOMResidencyPrograminNeurologicalSurgeryDOESNOTallowmoonlightingunderanycircumstances.
144
On-callPolicyEveryresidentisexpectedtotakeassignedcallassetforthbyschedulesavailableonAMIONandthroughtheChiefNeurosurgeryResidents.Pagerswillbewornatalltimesduringcallandpageswillbeansweredinatimelyfashion.Theobjectiveofon-callactivitiesistoprovideresidentswithcontinuityofpatientcareexperiencesthroughouta24-hourperiod.In-housecallisdefinedasthosedutyhoursbeyondthenormalworkdaywhenresidentsarerequiredtobeimmediatelyavailableintheassignedinstitution.
ThecallscheduleforeachhospitalisprimarilytheresponsibilityofthePGY5resident.Problemswith,andchangesintheschedulemustbeapprovedbytheChiefResident.Patientcareandeducationalobjectivesmustbemonitored.On-callroomsareavailableatBellevueHospitalandTischHospitalforresidentuse.Residentworkhoursshouldbemonitoredbythechiefresidentonanon-goingbasis,withtheaimofmodifyingcallpoliciesandmanpowerdecisionstoinsurecontinuedfullcompliancewiththeACGMErequirements.NYU Department of Neurological Surgery does not participate in in-HouseNightFloatMaximumIn-HouseOn-CallFrequencyPGY-2residentsandabovemustbescheduledforin-housecallnomorefrequently
thanevery-third-night(whenaveragedoverafour-weekperiod).At-HomeCall
o Time spent in thehospital by residents on at-home callmust count towardsthe80-hourmaximumweekly hour limit. The frequency of at-home call isnot subject to the every-third-night limitation, but must satisfy therequirement for one-day-in- seven free of duty, when averaged over fourweeks.
o At-home call must not be so frequent or taxing as to preclude rest or
reasonablepersonaltimeforeachresident.
o Residentsarepermittedtoreturntothehospitalwhileonat-homecalltocareforneworestablishedpatients.Eachepisodeofthistypeofcare,whileitmustbeincludedinthe80-hourweeklymaximum,willnotinitiateanew“off-dutyperiod”.
o Verbal inquiresaremadeby the, sitedirectors,andclinical servicechiefs,or
by The program director regarding if the At-home call was so taxing as topreclude rest or reasonable personal time for the resident. If this is thecaseresident isinstructed to returnhome (car fare isprovided) andnot to

145
return until the next schedule duty period at which point they are re-evaluated
Out-rotation/ElectivePolicyNYUSchoolofMedicineIssuingDepartment:GraduateMedicalEducationEffectiveDate:04/21/11ReissueDate:01/01/2016Out-ElectivePolicyandProcedureI.PolicyPurposeOverthecourseofaHouseStaffOfficer’spost-graduatetraining,s/hemaybepermittedaprogram-specificnumberofelectives.Accordingly,theResident/FellowmayrequestauthorizationtoexploreaclinicalorresearchexperiencenotavailablethroughtheNewYorkUniversitySchoolofMedicine(“NYUSoM”)/NYUHospitalsCenter(“NYUHC”)byseekingapprovalforanOut-Elective.II.ApplicabilityofthePolicyHouseStaffOfficer’senrolledinACGME-accredited,AOA-accredited,andCPMEaccreditedspecialtyandsub-specialtyprogramsIII.Definitions(ifapplicable)
A. ACGME–AccreditationCouncilforGraduateMedicalEducation
B. AOA–AmericanOsteopathicAssociation
C. CPME-CouncilonPodiatricMedicalEducation
D. Agreement–Out-ElectiveProgramLetterofAgreement
E. CPME-CouncilonPodiatricMedicalEducation
F. Director–NYUDirectorofResidencyTraining
G. HouseStaffOfficer-aphysicianwhoisenrolledinanAccreditedornon-Accredited
H. NYUSoM Training Program for a clinical specialty or subspecialty this includes allResidentsandClinicalFellows.
I. NYUHC-NYUHospitalsCenter
J. GME–OfficeofGraduateMedicalEducation
147
K. Host Institution - The site of approved clinical study undertakenoutside theNYUSystem. AHost Institution canbeahospital, aprivatepracticeoffice, or anyotherclinicalentity.
L. NYUSOM-NewYorkUniversitySchoolofMedicine
M. NYUHC-NYUHospitalsCenter
N. Out-Elective-Aprogramofstudythatisarrangedonanindividualbasisandhosted
byan institutionthat isoutsidetheNYUSystem(asdefinedinthisSectionII). Out-Electives must be authorized by the NYU GME and be consistent with ResidencyReviewCommitteerequirements.
O. Request–Out-ElectiveRequestForm
P. StandingRotation - A Standing Rotation is a required component of a residency-
training program that takes place at a hospital or other settingwhereNYU has aninstitutionalaffiliationagreement.ThispolicydoesnotpertaintoStandingRotations.
Q. Supervisor–HostInstitutionfacultyresponsibleforthesupervisionandevaluation
ofanNYUResident/Fellow.IV.PolicyTheAccreditationCouncilforGraduateMedicalEducation(“ACGME”)requiresthatOut-Electivesa)bebasedonacleareducationalrationale;b)haveclearlystatedlearningobjectivesandactivities;andc)provideresourcesnototherwiseavailablewithintheHouseStaffOfficer’strainingprogram.Inaddition,Out-Electivesmustbeofsufficientlengthtoensureaqualityeducationalexperienceandshouldprovidesufficientopportunityforcontinuityofcare.ExceptionstothoserequirementsmustbejustifiedandapprovedbytheOut-ElectiveSubcommitteeoftheGMEC.Out-ElectivesmustbeselectedwiththeadviceandapprovaloftheHouseStaffOfficer’sNYUDirectorofResidencyTraining(“Director”),whowillbasehis/herrecommendationontheHouseStaffOfficer’sacademicstandingandfactorswhichincludewhetherornottheOut-Electiveexperience:
• IsavailablewithintheNYUHC;• Enriches,butnotreplaces,theResident/Fellow’scoreexperiences;
148
• Enhancestheresidencyexperience;and• ProvidessufficientandappropriatesupervisiontotheResident/Fellow.
WhenHouseStaffOfficer’seducationoccursoutsideNYU,NYUcontinuestohaveresponsibilityforthequalityofthateducationalexperienceandmustretainauthorityovertheHouseStaffOfficer’sactivities.Inthisdocument,referencestoResident/FellowsarelimitedtoNYUResident/Fellowsenrolledinspecialtyandsub-specialtyprogramsaccreditedbytheACGME,AOA,andCPME.
V.ProcedureL. InitialConsiderations-WhileitiswithintheDirector’sdiscretiontograntinitial
approvalforOut-ElectivestudytoaResident/Fellowinhis/herprogram,undernormalcircumstancesacceptablejustificationshouldincludeaffirmationthattheproposedtrainingexperienceisnotavailablewithinNYU.
M. AdditionalAcceptableJustification-TheDirectormay,however,considerrequeststhat:• ProvidedefinededucationalopportunitiesspecifictotheHouseStaffOfficer’scareer
goals;• AredeemedvaluabletoNYU;or• Arehumanitarianinnature.
N. Requirements.1. GoodAcademicStanding-AHouseStaffOfficermustbeingoodacademicstanding,
asevidencedbyhis/herperformanceevaluations.2. PGYYear.-AHouseStaffOfficermustbeaPGY-2orhighertobeeligibleforanOut-
Elective.
O. CompensationandMalpracticeInsuranceCoverage-ArrangementsfortheHouseStaffOfficer’scompensationandmalpracticeinsurancecoverageduringtheOut-Electivemustbeinplace(seeSectionsIV,MedicalLicensureandMalpracticeCoverage,andV,FinancialConsiderations,inthisdocument).
P. Program-SpecificGuidelines-TheDirectorwillestablishgeneralOut-Electiveguidelinesforhis/herprogramconsistentwiththisOut-ElectivePolicyandProcedure.
149
Q. SelectionofOut-Elective-AHouseStaffOfficerinterestedinpursuinganOut-Electivemustselectanareaofinterestandalocationforsuchtraining.TheHouseStaffOfficerthenmustcontactthesupervisingattendingphysicianattheprospectiveHostInstitutionandobtainaninformalpromiseofcommitmentfromhim/her.
R. CompletionoftheOutElectiveRequestForm.1. HouseStaffOfficer’sResponsibility.TheHouseStaffOfficermustinitiatethe
applicationprocessatNYUbycompletinganOut-ElectiveRequestForm,availableonlineattheGMEWebsiteunderPoliciesandProcedures.TheRequestformmustbesignedandapprovedbytheHostInstitutionSupervisor.TheHouseStaffOfficermustsubmitthecompletedformtohis/herDirectorforapprovalandsignature.
2. Director’sResponsibility.TheDirectormustapproveordenytheHouseStaffOfficer’sRequestinwriting:a. Denial.IftheDirectordeniestheHouseStaffOfficer’sRequest,theDirectorwill
returntheformtotheResident/Fellowsoindicating.AcopyofthedeniedRequestwillbemaintainedintheHouseStaffOfficer’sdepartmentfile.ThedecisionoftheDirectorisfinalandnotsubjecttoappeal.
b. Approval.IncaseswheretheDirectorapprovestheRequest,he/shewillcompletetheappropriateareaoftheform,initiateanOut-ElectiveProgramLetterofAgreement(“Agreement”),andsubmitasummarystatementsummarizingtheelectiveandaddressingthefollowingcriteria:
• Theeducationalvalueoftheexperience
• Uniquevaluetheexperienceprovidesc. Submission.SubmitalldocumentstotheNYUOfficeofGME(threemonthsprior
tothescheduledout-elective).TheelectivewillthenneedtheapprovaloftheOut-ElectiveSubcommitteeoftheGMEC,whichmeetsquarterly.
d. NYUGME’Responsibility.TheNYUOfficeofGMEwillforwardthecompletedandsignedRequestandAgreementtotheOut-ElectiveSubcommitteeforfinalexecution.
S. Notification-OncetheRequestandAgreementarefullyexecuted,theNYUOfficeofGMEwillnotifytheDirectorandtheResident/Fellowofthefinalapprovalinwriting.
T. Recordkeeping-CopiesoftheapprovedRequestandAgreementwillbesenttotheHouseStaffOfficerandmaintainedinthefilesoftheNYUOfficeofGME.TheoriginalRequestandAgreementwillbemaintainedintheResident/Fellow’sdepartmentfile.
150
U. Evaluation-TheDirectormustensurethatanevaluationoftheHouseStaffOfficer’sperformanceisobtainedfromtheSupervisororhis/herdesigneeattheendoftheOut-Elective.TheDirectororhis/herdesigneealsoshouldmeetwiththeResident/FellowattheconclusionoftheOut-Electivetodiscusstheexperienceandtheevaluationwithhim/her.
V. ContinuityExperience-Forthoseprogramsthathavecontinuityrequirements,continuityexperiencemustreceivepriorityoverotherresponsibilitiesandmaybeinterruptedonlyforvacationsandoutsiderotationslocatedattoogreatadistancetoallowResident/Fellowstoreturn.
VI. MedicalLicensureandMalpracticeCoverage
A. MedicalLicensure-It istheresponsibilityoftheHouseStaffOfficertounderstandand follow the applicable state licensure rules for House Staff Officer in GraduateMedical Education (“GME”) programs in the state in which s/he will be training.Many states require, atminimum,a training certificate tobe issuedby their state’smedicalboardpriortothecommencementofanyclinicalactivities;thisrequirementmayincludecertaininstitutionswithinNewYorkState.
B. MalpracticeCoverage-MalpracticecoverageprovidedtoHouseStaffOfficerbyNYU
is effective only within the standard clinical training program as defined withincurrent affiliation and/or program agreements; therefore, the Resident/Fellow hastheprimaryresponsibilityforensuringthatamalpracticepolicy,providedbyeithertheHostInstitutionorbytheNYUInsuranceOffice,isinforcetocoverhis/herOut-Electiveactivities.
ItisthepolicyofNYUSchoolofMedicinethatHouseStaffOfficerwhoelecttoparticipateinanout-electivecontacttheHostFacilitytoensurethattheHostFacilitywillprovideprofessionalliabilityinsurancethroughaqualifiedprofessionalliabilityinsurancecarrierorthroughselfinsurancetocovertheResident/FellowsasapplicableintheiractivitiesattheHostFacility.
IftheHostFacilityelectsnottocovertheHouseStaffOfficerandiftheout-electiveisneededtocompleteACGMErequirementsforthetrainingprogram,theResident/FellowmayrequestthattheNYUInsuranceOfficeauthorizemalpracticecoveragefortheout-elective.TheHouseStaffOfficerwillnotbecoveredbyNYUmalpracticeinsuranceduringanout-electiveintheabsenceofawrittenmalpracticeinsurancecoverageauthorizationfromthe
151
NYUInsuranceOffice.Inmostcases,thiswillresultinafeechangedtothedepartmentfortheextendedcoverage.
152
ProfessionalismPolicyNYUSchoolofMedicineIssuingDepartment:GraduateMedicalEducationEffectiveDate:04/08/2013ReissueDate:01/01/2016ProfessionalisminGraduateMedicalEducationI.SummaryofPolicyTheACGMECommonProgramRequirementsstatethefollowingwithregardtoprofessionalisminGraduateMedicalEducation:
Professionalism
Residentsmustdemonstrateacommitmenttocarryingoutprofessionalresponsibilitiesandanadherencetoethicalprinciples.Residentsareexpectedtodemonstrate:IV.A.5.e).(1)compassion,integrity,andrespectforothers;IV.A.5.e).(2)responsivenesstopatientneedsthatsupersedesselfinterest;IV.A.5.e).(3)respectforpatientprivacyandautonomy;IV.A.5.e).(4)accountabilitytopatients,societyandtheprofession;and,IV.A.5.e).(5)sensitivityandresponsivenesstoadiversepatientpopulation,includingbutnotlimitedtodiversityingender,age,culture,race,religion,disabilities,andsexualorientation.
II.PolicyPurposeInadditiontopoliciesandexpectationssetbyotherorganizationsandinstitutions(suchastheACGME,AOA,AAMC,JointCommission,andhospitalpolicies),thispolicysetstheprofessionalismexpectationsofHouseStaffOfficersandfacultyinGraduateMedicalEducationatNYULMC.III.ApplicabilityofthePolicyThispolicyappliestoallHouseStaffOfficersatNYULMC.Additionally,whenapplicable,thispolicysetsexpectationsforprogramdirectorsandfaculty.IV.Definitions(ifapplicable)

153
A. HouseStaffOfficer-aphysicianwhoisenrolledinanaccreditedornon-accreditedNYUSoM or NYUHC Training Program for a clinical specialty or subspecialty thisincludesallResidentsandClinicalFellows.
B. SponsoringInstitutions-NYUSchoolofMedicineandNYUHospitalsCenterV.Policy
A. Professionalism
a. Responsibilities:AllHouseStaffOfficersareexpectedto:i. Adhere to The NYULMC Code of Conduct and all policies of Office ofGME, NYULMC, HHC, VA, and any other policies that apply to HouseStaffOfficersortheinstitution/locationatwhichtheyareworking.
b. IntheCurriculum
i. In the Common Program Requirements, the ACGME states thatevaluation and teaching of professionalism “is most effective whendone in the context of patient care and related activities, (e.g.,conductingQIprojects,leadingateam,presentingM&M,reflectionsonpractice, conversation with mentor.” Program Directors and facultymustensuretheintegrationofprofessionalismintoallpossibleaspectsofthecurriculum.
ii. ProgramsmustincorporateeducationabouttheappropriatescenariosinwhichaHouseStaffOfficershouldaskforhelp.Eachprogrammustdetermine appropriate escalation procedures. These escalationproceduresmustbeprovidedtoHouseStaffOfficers.
iii. Programs must incorporate education about error reportingproceduresforalllocationsatwhichHouseStaffOfficerswillwork.
iv. HouseStaffOfficersmustbeappropriatelyeducatedaboutretaliation,howtorecognizeretaliatoryactions,andtheappropriatemethodsfordealingwithsuch.
c. EvaluationsandFeedback:Evaluationsmustbecompleted,asstipulatedinthe
ACGME requirements and the NYU Evaluation Policy for Graduate MedicalEducation.Inaddition:
i. Boththeevaluatorandthe individualbeingevaluatedareexpectedtorespectdiversityofopinion.
ii. House Staff Officers must be open to accepting evaluations andfeedbackontheirperformanceinallareasoftraining,andincorporateevaluationsandfeedbackintotheirpractice.
154
d. ErrorReporting,Concerns,andComplaints:HouseStaffOfficerareatthefront
lineofpatientcare,andareexpected toreportanyerrorsor incidentsusingtheappropriatemethods.Thispracticeisessentialtopatientcareandqualityimprovement,andshouldbeencouraged.Inaddition:
i. HouseStaffOfficersareexpectedtosubmitanyconcernsorcomplaintsasdefinedbythe“HouseStaffOfficerConcernsorComplaints”Policy.Theappropriatemechanisms for submitting such informationat eachinstitutionareavailableinthispolicy.
ii. If a situation or concern does not need to go through the formalprocesses listed above, House Staff Officers should approach theirsupervisor,thenexthighestrankingindividualiftheissueinvolvedthesupervisor, theOffice ofGME, and/or theAssociateDeanofGraduateMedicalEducation.
iii. Programsareresponsible foreducatingHouseStaffOfficersabouttheerror reporting methods at each hospital. Please refer to the “In theCurriculum”sectionofthispolicy.
iv. Programsmust ensure that error reportingmechanismsare availabletoHouseStaffOfficersatalltimes.
e. QualityImprovementandPatientSafety:HouseStaffOfficersareexpectedto:
i. Participate inquality improvement andpatient safetyprojectsduringtheirtimeoftraining.
ii. HouseStaffOfficersareexpected tobeawareofquality improvementinitiatives that are taking place at the hospitals in which they work.When possible and appropriate, House Staff Officers should activelyparticipateintheseinitiatives.
iii. Programs are responsible for providing the appropriate education toHouse Staff Officers about institutional/hospital quality improvementinitiatives.
B. Retaliationa. In order to provide all House Staff Officers with a culture of safety, and to
ensure that they feel comfortable reporting errors and providing feedback,askingforhelp,andreportinglapsesinprofessionalismbycolleagues,anyandallretaliatoryactionstakenagainstaHouseStaffOfficershouldbeescalatedtohis/hersupervisor,orthenexthighestrankingindividualintheeventthattheHouse Staff Officer’s supervisor is involved. Such incidents can also be
155
reported directly to the Office of GME, and the Associate Dean of GraduateMedicalEducation.
C. UnprofessionalBehaviorandRemediation
a. Any lapses in professionalism will be handled according to the “CorrectiveActionandDisciplinaryPolicyforHouseStaffOfficers.”
156
RecruitmentandSelectionPolicyRecruitment,selection,andappointmentofresidentsisperformedbyNeurosurgeryfaculty,theprogramdirector,associatedirectors,sitedirectors,andthedepartmentchair,undertheoversightoftheGraduateMedicalEducationCommittee(GMEC)andtheOfficeofGraduateMedicalEducation(OGME)inaccordancewiththeAccreditationCouncilforGraduateMedicalEducation(ACGME).TheapplicationreviewprocessensuresfairandconsistentconsiderationofallapplicantstotheNYUInternalMedicineResidencyTrainingProgram.RecruitmentandSelectionApplicationsforNYU’sNeurosurgeryResidencyTrainingProgramareprocessedthroughtheNationalResidencyMatchingProgram(NRMP)andtheElectronicResidencyApplicationService(ERAS).Acentralapplicationprocesshasallowedforastreamlinedapproachtosecuringaresidencyposition.
Writtenore-mailedapplicationswillnotbeconsidered.MoreinformationaboutERASmaybeobtainedbyvisitingtheAAMCwebsite.
AllrequesteddocumentswillbereviewedbytheDepartmentofNeurosurgeryHouseStaffSelectionCommittee,andselectedcandidateswillbeinvitedforaninterviewandtourofourmedicalcampus.DuetothelargenumberofapplicationsreceivedeachyearviaERAS,notallqualifiedcandidatescanbeaccommodatedwithinterviewsandtours.Weaskforyourunderstandinginthisregard.Interviewsgenerallytakeplaceinthelatterpartoftheyear,fromNovemberthroughJanuary.
AppointmentstotheneurosurgeryresidencyprogramaremadethroughtheNationalResidencyMatchingProgram(NRMP)andcommencebeforeJuly1ofeachacademicyear.Eligibility:
• Amedicaldegreepriortoresidencyprogramstartdatefromoneofthefollowing:• MedicalschoolsintheUnitedStatesandCanadaaccreditedbytheLiaisonCommittee
onMedicalEducation(LCME)• ApassingscoreonUSMLEStepI.• ThreelettersofRecommendationnotincludingDean’sLetter• CurrentCVandpersonalstatementonfile.
Non-U.S.citizensmustpossessaPermanentResidentCardoranappropriateeducationalvisapriortostartingapostgraduatemedicaleducationprogram.Pleasenotethatweaccept
157
applicationswithdocumentationofJ-1Visastatus,butcannotacceptanyothercategoryofvisas(e.g.H1B).
158
NeurosurgerySupervisionandScopeofPracticePolicy(includingEscalation)SupervisionofResidentsThetrainingprogramisstructuredtoencourageandpermitresidentstoassumeincreasinglevelsofresponsibilityappropriatewiththeirindividualprogress,experience,skill,knowledgeandjudgment.Intheclinicallearningenvironment,eachpatientmusthaveanidentifiable,appropriatelycredentialedandprivilegedattendingphysicianwhoisultimatelyresponsibleforthatpatient’scare.AtTischHospitalitistheadmittingfacultymember.AtBellevueHospitalandattheManhattanVAMedicalcenteritistheoncallfacultymember/admittingfacultymemberortheSiteDirector.Thisinformationshouldbeavailabletoresidents,facultymembers,consultingfacultyandresidents,thenursingstaff,andpatients.Residentsandfacultymembersmustinformpatientsoftheirrespectiverolesineachpatient’scare.LevelsofSupervisionTheprogrammustdemonstratethattheappropriatelevelofsupervisionisinplaceforallresidentswhocareforpatients.Supervisionmaybeexercisedthroughavarietyofmethods.Someactivitiesrequirethephysicalpresenceofthesupervisingfacultymember.Formanyaspectsofpatientcare,thesupervisingphysicianmaybeamoreadvancedresidentorfellow.Otherportionsofcareprovidedbytheresidentcanbeadequatelysupervisedbytheimmediateavailabilityofthesupervisingfacultymemberorresidentphysician,eitherintheinstitution,orbymeansoftelephonicand/orelectronicmodalities.Insomecircumstances,supervisionmayincludepost-hocreviewofresident-deliveredcarewithfeedbackastotheappropriatenessofthatcare.IntheseinstancestheClinicalCompetencyCommitteewillreviewofcaredeliveredoranyissuesthatarise.Toensureoversightofresidentsupervisionandgradedauthorityandresponsibility,theprogrammustusethefollowingclassificationandlevelsofsupervision:
• DirectSupervisionbyFaculty-facultyisphysicallypresentwiththeresidentbeingsupervised.
159
• DirectSupervisionbySeniorResidentsameasabovebutresidentisthedirectsupervisor.
• IndirectwithDirectSupervisionIMMEDIATELYAvailableFaculty–thesupervisingphysicianisphysicallypresentwithinthehospitalorothersiteofpatientcareandisimmediatelyavailabletoprovideDirectSupervision.
• IndirectwithDirectSupervisionIMMEDIATELYAvailableResidentsamebutdirectsupervisorisresident.
• IndirectwithDirectSupervisionAvailablethesupervisingphysicianisnotphysicallypresentwithinthehospitalorothersiteofpatientcare,butisimmediatelyavailablebymeansoftelephonicand/orelectronicmodalities,andisavailabletoprovideDirectSupervision.
• Oversight-Thesupervisingphysicianisavailabletoprovidereviewofprocedures/encounterswithfeedbackprovidedaftercareisdelivered.
Theprogramdirectorandfacultymembersassigntheprivilegeofprogressiveauthorityandresponsibility,conditionalindependence,andasupervisoryroleinpatientcaredelegatedtoeachresident.Theprogramdirectorevaluateseachresident’sabilitiesbasedonthespecificcriteriasetforthinthedepartmentsProgramGoalsandRotationalResponsibilitiesdocument.Whenavailable,evaluationshouldbeguidedbyspecificnationalstandards-basedcriteria.Facultymembersfunctioningassupervisingphysiciansshoulddelegateportionsofcaretoresidents,basedontheneedsofthepatientandtheskillsoftheresidents.Seniorresidentsorfellowsshouldserveinasupervisoryroleofjuniorresidentsinrecognitionoftheirprogresstowardindependence,basedontheneedsofeachpatientandtheskillsoftheindividualresidentorfellow.Theprogramprovidesguidelinesforcircumstancesandeventsinwhichresidentsmustcommunicatewithappropriatesupervisingfacultymembers,suchasthetransferofapatienttoanintensivecareunit,orend-of-lifedecisions(seethesupervisoryflowchartbelow).GuidelinesforResidentMandatoryCommunicationwithAttendingThefollowingsituationsrequiremandatorydirectcommunicationwiththefacultyresponsibleforpatientcare,duringroutineworkinghours,orafterhoursandweekends:1.Death2.Suicideattempt3.Violencerequiringphysicalrestraints
160
4.Pregnancy(initialnotification)5.Transferofcaretoanothermedicalorsurgicalservice6.Anyseriousadverseeventfrompharmacologicorpsychotherapeuticintervention7.AnycomplexdecisionmakingprocessthattheresidentdoesnotfeeladequatelyqualifiedtoundertakewithoutimmediateinputfromfacultyAnylapseinthisprocesswillbereportedtotheprogramdirector,whowillmonitorthereportingprocessandreviewmonthly.Eachresidentmustknowthelimitsofhis/herscopeofauthority,andthecircumstancesunderwhichhe/sheispermittedtoactwithconditionalindependence.Inparticular,PGY-1residentsshouldbesupervisedeitherdirectlyorindirectlywithdirectsupervisionimmediatelyavailable.Foreveryprogressioninlevel,curriculum,performanceandovertechnicalabilityareconsideredpriortochangeorrevisioninSOP.Facultysupervisionassignmentsshouldbeofsufficientdurationtoassesstheknowledgeandskillsofeachresidentanddelegatetohim/hertheappropriatelevelofpatientcareauthorityandresponsibilityandCompletionoftheSNSBootCampThespecificoverviewofresidentsupervisionandgradedauthorityandresponsibilityusingtheclassificationsofsupervisionisfoundinourdepartmentalScopeofPracticedocument(included),whichisavailableonlineonNewInnovations.ThisdocumentisreviewedandupdatedasrequiredbyinstitutionalpolicybyourClinicalCompetencyCommittee.Thesamplediagrambelowdetailsprocedureforescalationofissuesregardingsupervision,grievances,workhoursoranyotherresidentconcerns.
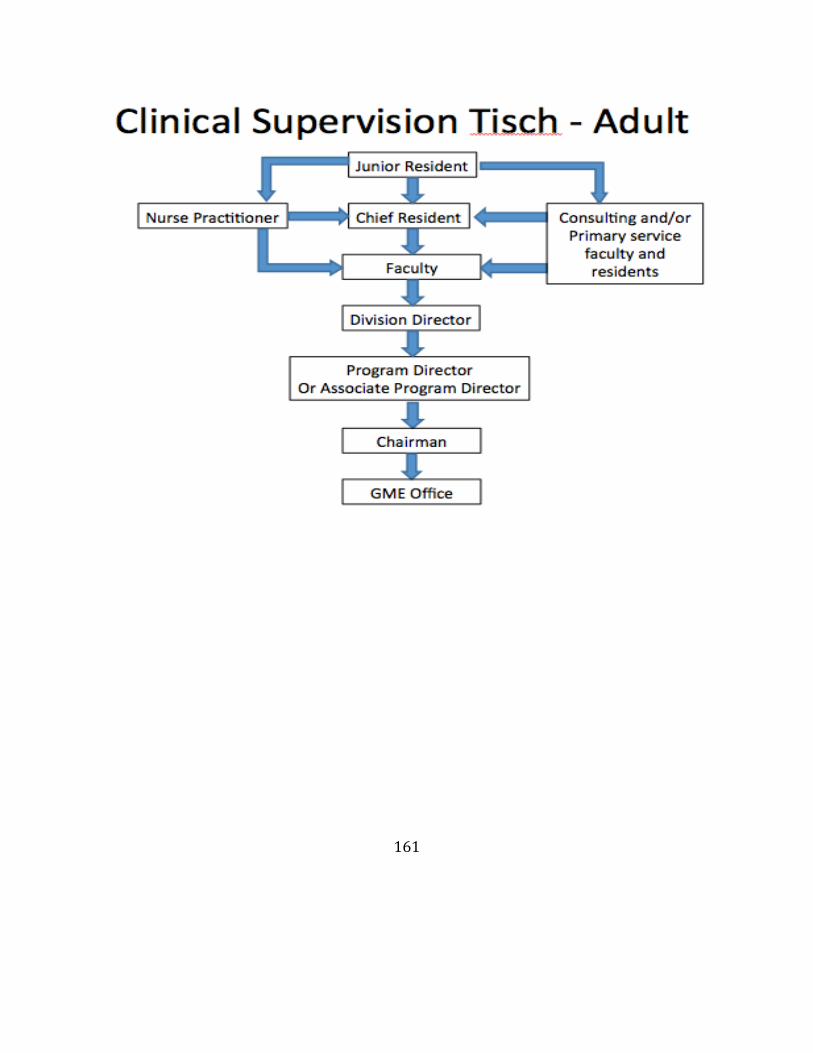
161
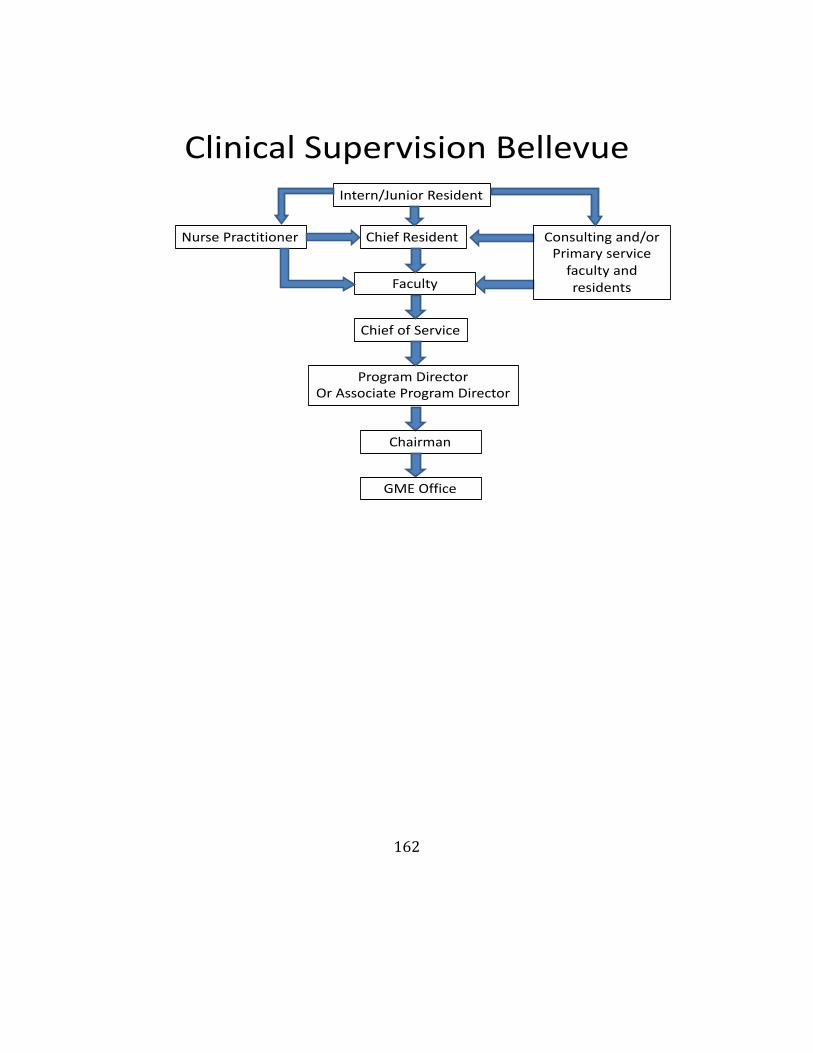
162
ClinicalSupervisionBellevue
ChiefResident
Faculty
ChiefofService
ProgramDirectorOrAssociateProgramDirector
NursePractitioner Consultingand/orPrimaryservicefacultyandresidents
Intern/JuniorResident
Chairman
GMEOffice
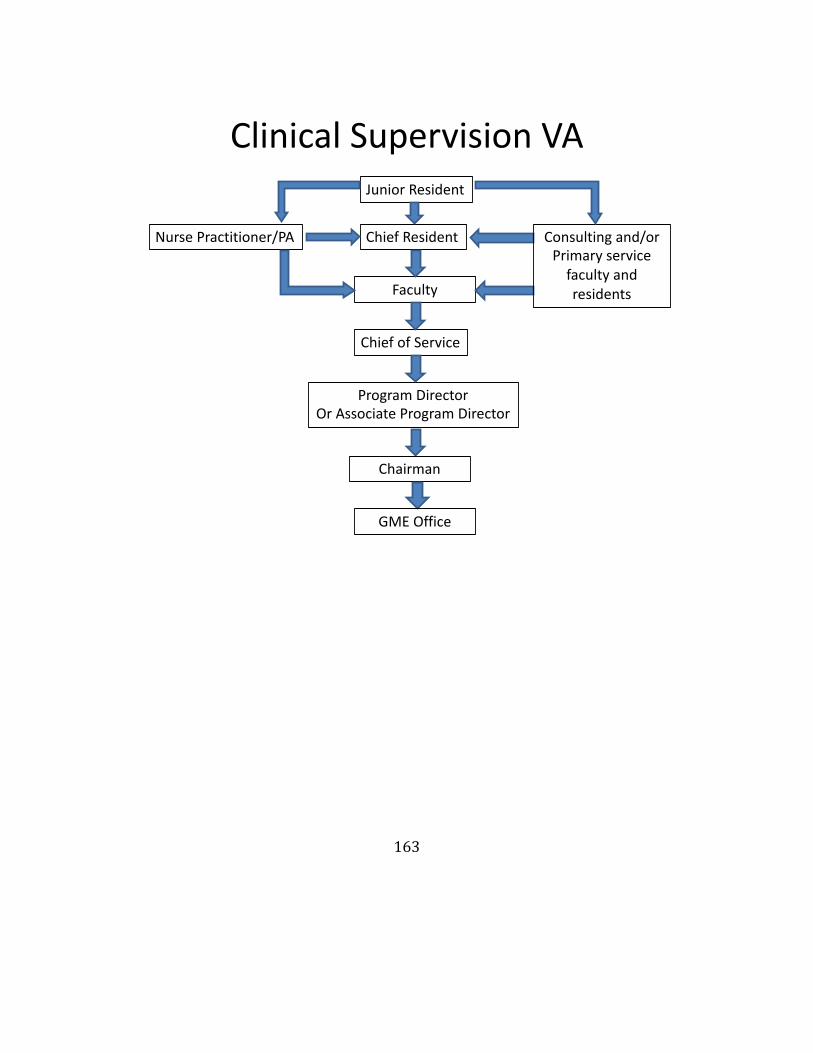
163
ClinicalSupervisionVA
ChiefResident
Faculty
ChiefofService
ProgramDirectorOrAssociateProgramDirector
NursePractitioner/PA Consultingand/orPrimaryservicefacultyandresidents
JuniorResident
Chairman
GMEOffice
164
TermsandConditionsofEmploymentPolicy
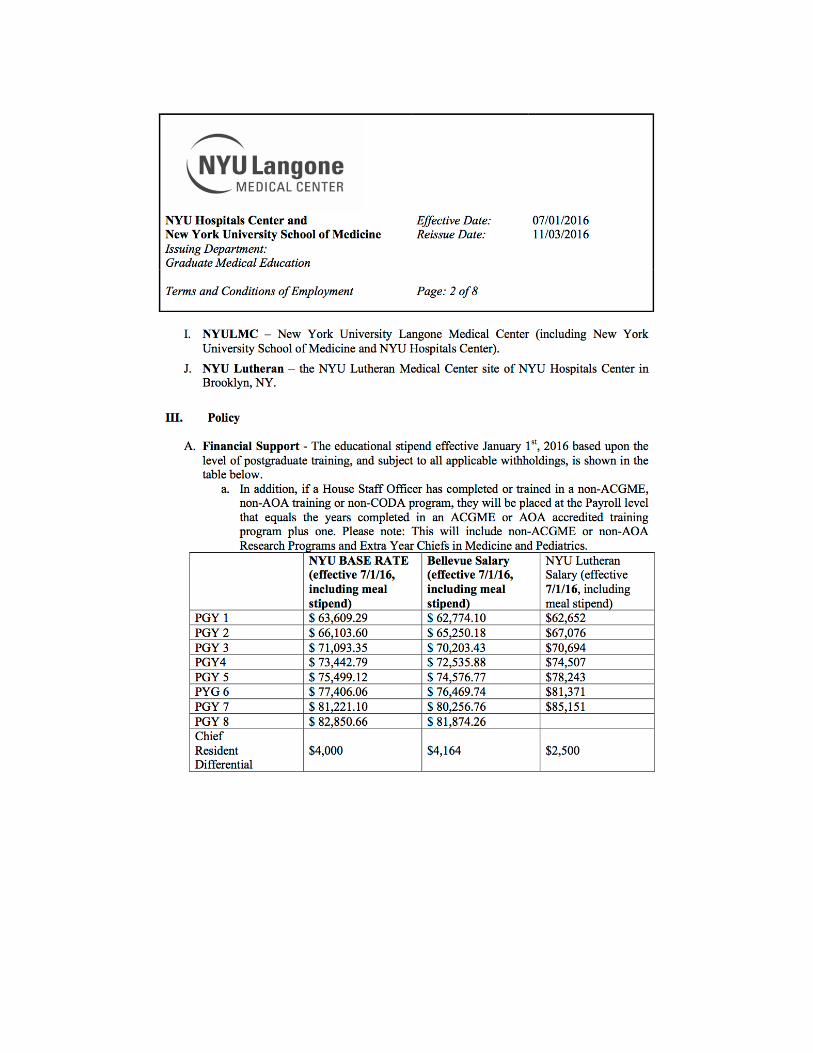
165
166
167
168
169
170
171
172
TransitionsofCare
NEUROSURGERYPROGRAMTRANSITIONSOFCAREPOLICYInaccordancewithinstitutionalpolicythatallprogramsmust design clinical assignmentstominimize the number of transitions inpatientcarethedepartmentofNeurosurgeryhasadoptedthefollowpolicyfortransitionsofcare.Weacknowledgethatthesponsoringinstitution and program must ensure and monitor effective,structuredhand-overprocessestofacilitatebothcontinuityofcareandpatientsafety.
1. Ourprogramwillensurethatresidentsarecompetentincommunicatingwithteam
membersinthehand-overprocess.2. The sponsoringinstitutionmustensure theavailabilityofschedulesthatinformall
membersofthehealthcareteamofattendingphysiciansandresidentscurrentlyresponsibleforeachpatient’scare.
3. Competenceoradherencetothispolicyinmonitoredduringeverysignouttoattendingorchiefresidentsupervising.Considerationsaredelineatedandtakenintoconsiderationduringformalevaluationperiodsoronaquarterlybasis.TheClinicalCompetencyCommitteealsoreservestherighttoreviewanyconcernsinadherencetotransitionofcare.
Allpatientorders, results,medications,progressandconsultnotesare located inourEMRsystemsatthevarioussitesandallpatientsmusthaveamedicationreconciliationwhentheyaretransferredbetweencaresettingsorservicesatallofourinstitutions.Thishelpstoalleviateopportunitiesforlossofinformationandcontinuityduringtransitionsofcare.Ultimately as is designated in our supervision policy the attending physician isresponsible for the care of any individual patient. We do however recognize thattransitionsofcareoccurbetweenhousestaffasthecomeonandoffshiftsinordertominimize the these effects our program encourages the following steps to minimizetransitions,errorsduringtransitions,andtomaximizepatientcare:Designateaquietspacewheretransitionsofcareoccur.Thisroomshould:o Includecomputerssoresidentscanaccessmedicalinformationusingthehospital
EMRo Allowforprivateuninterrupteddiscussionsabouteachindividualpatient
o AtLangoneMedicalCenter/TischHospitaltransitionofcarediscussionsshouldtakeplaceintheChiefsofficeorinthe12-floorconferenceroom.
o AtBellevueHospitaltransitionofcarediscussionsshouldtakeplaceinthe
173
residentofficeinsuite7S.o At theVAMedical Center transition of care discussions should takeplacein
theresidentoffice.Reduceinterruptionsduringtransitionofcare.
o The chief or senior resident on the service resident leads the transition of careprocess
o Residentstoavoiddistractionscausedbypagers,phonecalls,andothertaskso Ifaninterruptionoccurs,residentsshouldbeginthediscussionofthepatientover
again.Usecomputerizedtemplates(routesheets/lists)foralltransitionsofcare.
o TheseElectronictemplatesthataregeneratedfromthehospitalEMRsystemandhavepre-populatepatientinformation,suchas:
a. Patientnameb. Medicalrecordnumberc. Dateofbirthd. Roomnumbere. Dateofadmissionf. Primarydiagnosisg. Attendingphysicianofrecordh. Residentsshouldrevieweverypatientduringthetransitionofcare.
o Verballyidentifyeachpatiento Listthemajormedicalissuesandtheto-dolistthecoveringpractitionerneedsto
complete.o Avoidnonstandardabbreviations.o Statealloftheanticipatedproblemsthatmayarise.o Thereceivershouldbeanactivelistener,takenotes,andshouldverifyallofthe
itemsontheto-dolisttoensurethattheyunderstoodeverythingo Verifythattheyknowthecontactinformationoftheattendingphysicianofrecord
Identifysickpatientsupfront.o Ifthepatientissickortheteamisparticularlyconcerned,thegivershouldsaythatat
thebeginningofthepatient'stransitionofcareo Thishelpstoensurethatthephysicianreceivingtheinformationunderstandsthe
seriousnessofthesituationandaskstheappropriatequestions.o Ifappropriatetheteamshouldseethesepatientstogetherattheconclusionofthe
signoutdiscussions.Explaintherationale.Expectations:
o Residentshandingoffpatientstoanotherphysicianshouldexplaintheirrationaleforeachmanagementplan.
o Useif-thenscenariosduringtransitionsofcare.o Focusthediscussiononcontingencies(e.g., ifpatientreacts thisway,doX; if
patientreactsthatway,doY)o Givethereceivingphysiciansaclearunderstandingofwhattheyshouldconsider
doingduringtheirshift.o Empowergiversandreceivers.
174
o Bothpartiesshouldfeelcomfortableenoughtoasktheotherpractitionertoslowdownorelaborate
AllHouseStaffOfficerswillbeeducatedonhowtoperformappropriateandsafetransitions
ofcare.o AsaPGY1–includedinpartofprofessionalismcurriculumasafirstyearinthe
program,ResidentswillbeeducatedonproperTOCproceduresbyseniorresidentsandsupervisingattending’sateachsite.
o Theywillbeeducatedontheappropriatetimesofdaythatallhandoff’sshouldbecompletedbyandprovided.Listofpatientsonserviceshouldberunintheamandpmoratbeginningorendofashift.
o Servicechiefsonateachsitewillcommunicateanychangestothisschedule.o ListswillevaluatedbasedinclusionofabovecriteriainEMRtemplates.Theywillalso
evaluatedbasedontimelinessandaccuracyofinformation.o ItisanexpectationthatbycompetitionofPGY1year,alltraineeshavelearned
proceduresasstipulatedbythispolicy.Thisispartofatraineesprofessionalismscore.
Therequiredlevelofsupervisionfortransitionsofcarefordifferentlevelsoftrainees
and/orpatientcare.o AllPGY1andjuniorresidentswillhavedirectsupervisionfromservicechiefs.o ServiceChiefswillreportanyandallissuesthatarisefromTOCtosupervising
attendingonservice.o Thesitedirectors,servicechiefs,andprogramdirectorwillperiodicallymonitor,
observeandevaluatethesetransitionstoensurecompliancewiththeabove.o Evaluationwillalsotakeplaceaspartoftheirquarterlyevaluationsandasneededon
theflyevaluationsforaservice.CourseofActionintheeventthataHouseStaffOfficerviolatesthispolicy
o Intheeventthataresidentorfellowviolatesthispolicy,awrittenandorverbalwarningwillbeissuedbytheprogramdirectortoresident.
o Failuretoprovidetheexpectedtransitionofcarewillbedocumentedinresidentfileanddiscussedaspartofsemi-annualandmilestonereview
o Whereaconsistentproblemexists,theresidentorfellowwillheldtotheCorrectiveandDisciplinaryActionPolicyincludedinthismanual.
175
NYUSchoolofMedicineIssuingDepartment:GraduateMedicalEducationEffectiveDate:04/01/2013ReissueDate:10/31/2014TransitionsofCareandHandoffPolicyforHouseStaffOfficersI.SummaryofPolicyTheACGMECommonProgramRequirementsstate:
•Programs must design clinical assignments to minimize the number oftransitionsofpatientcare.•SponsoringInstitutionsandprogramsmustensureandmonitoreffective,structuredhand-overprocessestofacilitatebothcontinuityofcareandpatientsafety.•Programsmustensurethatresidentsarecompetentlyincommunicatingwithteammembersinthehand-overprocess.•Thesponsoringinstitutionmustensuretheavailabilityofschedulesthatinformallmembersof thehealthcare teamofattendingphysiciansandresidentscurrentlyresponsibleforeachpatient’scare.
II.PolicyPurposeThepurposeofthispolicyistoensurethatallHouseStaffOfficersandProgramDirectorsareawareof the importanceofsafeandeffective transitionsofcare.Thispolicyaimstomeet therequirementsoftheACGMEInstitutionalandCommonProgramRequirementswithrespecttotransitionsofcare.III.ApplicabilityofthePolicyThis policy applies to all House Staff Officers in ACGME accredited training programsatNYULMC.IV.PolicyTransitionsofCare/HandoffStandards–Thepoliciesthataredevelopedbyeachindividualprogrammustbesurethattransitionsofcareoccurinastandardizedfashion,
176
and include, atminimum,thefollowinginformation/components:a.Patientidentifiers:Name,medicalrecordnumber,dateofbirthb. Admission information: Admitting physician, date and time ofadmissionc.PatientSummary:examfindings,labresults,anyclinicalchangessinceadmission,includingchangesinlevelofpatientcareandseverityofissue(s)d. Activeissues:Currentdiagnosis,status,conditionofpatient,recentevents.e.Contingencyplans(“If…/…then”)f. Familycontactsg.Dischargeplans/instructions:Anydischargeinformationgiventopatient,
anticipateddischarge information.Thisshould includedischargeinstructionstootherfacilitiesorlevelsorcare.
h. Anticipatedaction/changes:Expectedtestsorprocedures.i. Anychangesinresponsibleattendingphysicianand/ornursej. “Check for Understanding”: All transitions of caremust be fortifiedwitha
“check-back”toensurethatthereceiverofinformationcorrectlyunderstandsallinformationthathasbeenprovided.
B.OfficeofGMEResponsibilities
a.The Sponsoring Institutionmustmonitor programs to ensure thateachprogram has a handoff/transitions of care policy that appliesspecificallytotheirspecialty.ThesepoliciesmustbesubmittedtotheOfficeofGMEatleastannuallyandwheneverrequested.
b. TheSponsoringInstitutionmusthavetheappropriatemechanismsin
placetoallowallappropriatepartiesaccess to thescheduleofphysiciansandHouseStaffOfficers toallow forsafeandeffective transitionsofcare. Inaddition,theseschedulesshouldclearlydelineatetheresponsiblephysicianand/orHouseStaffOfficerforagivenpatientatanytime,toensurethatpropercareandoversightisprovidedforeachpatient.
c.TheOfficeofGMEwillmonitortheentryofschedulesintoNew
InnovationstoensurethatHouseStaffOfficerandfacultyschedulesareentered.
d. TheOfficeofGMEwillgrantview-onlyaccessof theseschedules tonecessary parties, such as nurses who are working alongside House Staff
177
Officersincaringforapatient.C.TrainingProgramResponsibilities
a.Eachprogramjusthaveitsownpolicyfortransitionsofcare/handoff.Thesepolicies must address any specialty-specific tasks necessary for a safeandeffectivetransitionofcare.Thesepoliciesshouldaddress,butarenotlimitedto:
i.Theacceptedstandardfortransitionsofcarewithinthedepartmentorprogramii.ExpectationsforfollowingtheTransitionofCarePolicyiii.CourseofActionintheeventthataHouseStaffOfficerviolatesthis
policyiv. Instructions on how the program intends to educate all House Staff
Officersonhowtoperformappropriateandsafetransitionsofcare.v.The required level of supervision for transitionsof care fordifferent
levelsoftraineesand/orpatientcare.
b. Allschedulesandcall-schedulesmustbemadeavailabletonurses,attendings,andotherHouseStaffOfficersthroughNewInnovationsorotherappropriatemethods.c.TheTrainingprogrammustensurethattheschedulesofHouseStaffOfficersminimizesthenumberoftransitionsofpatientstomaintainpatientsafetyandcontinuityofcare,andalsoallowHouseStaffOfficerstocomplywithACGMEandNewYorkStateDutyHourregulations.
V.RelatedPolicies(ifapplicable)A.DutyHourPolicyforHouseStaffOfficersB.AlertnessManagement/FatigueMitigation
178
Book&ConferenceFundNYUSchoolofMedicineIssuingDepartment:GraduateMedicalEducationEffectiveDate:08/09/11ReissueDate:01/01/2016Book and Conference Stipend ReimbursementPolicy
I.PolicyPurposeTheBookandConferenceStipendswereinstitutedtohelpoffsetexpensesincurredduringthetraineesAcademicYear(July1stthruJune30th)byHouseStaffinrelationtopurchaseofmedicalequipmentorConferencepresentation/attendance.II.ApplicabilityofthePolicyHouseStaffOfficerswhoareassignedtoNYUHospitalsCenterpaylineareeligibleforoneorbothofthesestipends.HouseStaffOfficersassignedtoaBellevuepaylineareeligibleforoneorbothofthesestipendsthruCIR.HouseStaffOfficersassignedtoaNYULutheranpaylineareeligibleforNYULutheranstipendsonly.EffectiveJuly1,2008HouseStaffOfficersassignedtoaStatepaylinewillbeeligibleforBookStipendreimbursement.HouseStaffOfficersontheStatelinemustbePGY2orbelowtobeeligibleforthe$600.00reimbursement.Eligibilitybeginswiththedatetrainingbeginsandthestipendamountsarenon-accruable.StipendrequestsforeachacademicyearmustbesubmittedforapprovalbyJune30.HouseStaffOfficersinnon-ACGME,non-AOA,ornon-CPMEprogramsnotfundedbyaHospitalpaylineorwhosesalaryis100%fundedbyagrant,arenoteligibleforthesestipends.III.Definitions
A. ACGME–AccreditationCouncilforGraduateMedicalEducation
B. AOA-AmericanOsteopathicAssociation
C. CPME-CouncilonPodiatricMedicalEducation
179
D. GME–OfficeofGraduateMedicalEducation
E. CIR–CommitteeofInternsandResidents
F. PEP–CIRProfessionalEducationPlan
G. HHC–HealthandHospitalsCorporation
H. SponsoringInstitutions–NYUSchoolofMedicineandNYUHospitalsCenterIV.PolicyNYULANGONEMEDICALCENTERSTIPEND:
A. BookStipend–NYUBookStipendfollowsCIRestablishedguidelinessetforthePEPforeligiblereimbursableexpenses.1. Eligibility – All House Staff Officers assigned to NYU Hospitals Center pay line.HouseStaffassignedtoaStatelinethatarePGY2orbelow.
2. Reimbursement – Up to $600.00 per academic year for qualified academicexpenses:a. MedicalBooks/electronicmedicalbooksb. MedicalAudioorVideoTapesc. MedicalCompactDiscsd. Work-RelatedMedicalEquipment
i. Personal digital assistants (PDAs or "Palm Pilots") are work-relatedmedicalequipmentandreimbursable.
ii. Itemsthatcanbeusedonlyforwork/medicalpurposes,suchasthePocketPDR®,arereimbursable.
iii. Smartphone, BlackBerry, Treo’s and i-Phone that have available medicalsoftwarearereimbursable.
iv. Items, other than PDAs, that can be used generally, that is either forwork/medical purposes, or personal/non-work purposes, such ascomputers,laptops,cameras,ormostsoftware,arenotreimbursable.
e. DuesforMedicalSpecialtySocietiesf. SubscriptionsforMedicalSpecialtyJournalsg. MedicalLicenseApplicationFeesh. MedicalLicenseExaminationFeesi. SpecialtyBoardExaminationFees
180
B. ConferenceStipend–NYU Conference Fund follows CIR established guidelines forHHCConferenceFundforeligiblereimbursableexpenses.1. Eligibility
a. Allresidentstobeusedanytimeduringtheirbasicresidencyprogram.b. ExtraYearChiefResidentswhohavefinishedtheirbasicresidency.c. Fellowsinsubspecialtytrainingprograms.
2. Reimbursementa. $1,500.00maximumbenefitduringbasicresidencyb. $1,500.00maximumeachyearforFellowsorExtraYearChiefs.
NYULUTHERANMEDICALCENTERSTIPEND:
A. Educational Stipend – NYU Lutheran Educational Stipend follows establishedguidelinessetfortheNYULutheranHouseStaffforeligiblereimbursableexpenses.1. Eligibility–AllHouseStaffOfficersassignedtoNYULutheranMedicalCenterpayline.
2. Educational Stipend Reimbursement – Up to $250.00 per academic year forqualifiedacademicexpenses:a. MedicalBooksb. MedicalAudioorVideoTapesc. MedicalCompactDiscsd. Work-RelatedMedicalEquipment
i. Personal digital assistants (PDAs or "Palm Pilots") are work-relatedmedicalequipmentandreimbursable.
ii. Itemsthatcanbeusedonlyforwork/medicalpurposes,suchasthePocketPDR®,arereimbursable.
iii. Smartphone, BlackBerry, Treo’s and i-Phone that have available medicalsoftwarearereimbursable.
iv. Items, other than PDAs, that can be used generally, that is either forwork/medical purposes, or personal/non-work purposes, such ascomputers,laptops,cameras,ormostsoftware,arenotreimbursable.
3. Reimbursementforfinalyearofresidency(forresidencyprogramsoftwoormoreyears)–Upto$1,000forfinalyearinlieuofthe$250describedabovefora board review course approved by their Director. Other expenses such astravel,meals,orlodgingarenottobeincludedinthe$1,000.
B. ConferenceStipend–NYULutheranConferencestipendallowsforupto$1,000pertrainee for eligible reimbursable expenses (available once during training period)towards attendance at a regional or national conference for advanced training orpresentationofresearchprojects.1. Eligibility
181
a. All ACGME,AOA, and CPME residents to be used anytimeduring their basicresidencyprogram.
b. Fellowsinaccreditedsubspecialtytrainingprograms.2. Reimbursement
a. $1,000.00maximumbenefitduringbasicresidencyonlyifpresenting.
BELLEVUEHOSPITALCENTERSTIPENDHouseStaffonBellevueHospitalarepartoftheHHCandareeligiblefortheBookandConferenceFundthroughtheirmembershipwithCIR.V.ProcedureNYULANGONEMEDICALCENTERREIMBURSEMENTPROCESS:
A. NYUHospitalsCenterandStateHospital1. To apply for reimbursement, House Staff Officers should complete the NYU
Hospitals Center Book & Conference Reimbursement Form. This form is to besubmitted to the Program's Residency Coordinator with the correspondingoriginalreceipts.(HouseStaffOfficer,besuretoprovideyourmailingaddressontheform.)
2. As requests are reviewed by the department, the Coordinator thenenters/updatesthedataontheBookStipendTrackingspreadsheetandtheBookStipendSubmissiontemplate.ThecompletedtemplateshouldthenbesubmittedviaemailtotheapplicableGMETrainingProgramSpecialistforreview.Onceitisapproved, the GME Training Program Specialist will submit it to NYU PayrollServicesmailto:[email protected].
3. ConferenceReimbursementrequestsarereviewedbythedepartmentandtheCoordinatorentersthedataontheNYUMedicalCenter-HospitalforJointDiseasesConferenceFeeTravelExpenseReimbursementFormtobesubmittedtoAccountsPayableforpayment.
4. ProgramCoordinatorsmaynot add individuals to theBookorConferencereimbursement roster. Please contact the Office of GME if an individual ismissingfromthereimbursementrosterortocheckeligibilitystatus.
5. HouseStaffOfficersshouldcontacttheProgramCoordinatorwithanyquestions.6. NYUFinanceprocessforreimbursementmustbefollowed:
http://finance.webdev.nyumc.org/policies-and-procedures
182
NYULUTHERANMEDICALCENTERREIMBURSEMENTPROCESS:
A. NYULutheran1. To apply for reimbursement, House Staff Officers should complete the NYU
Lutheran Educational Stipend Reimbursement Form (available on NewInnovations). This form must be submitted to the Program's ResidencyCoordinatorwiththecorrespondingoriginalreceipts.
2. TheCoordinatorobtainsapprovalfromtheProgramDirector(ifapplicable)thenenters/updatesthedataontheBookStipendTrackingspreadsheetandtheBookStipendSubmission template. ACheck request to submit reimbursement to thehouse staff officer is submitted to the GME Office for signatory. Once it isapproved,theCoordinatorwillsubmittheCheckrequesttotheFinance,AccountsPayableforprocessing.
3. RequestsforConferenceReimbursementmusthavepriorapprovalbeforethehousestaffofficerattendsaconference.TheEducationalStipendForm(availableonNewInnovations)mustbecompletedandsignedbytheProgramDirectorpriortoattendance.AllrequestsarereviewedbytheGMEOfficebeforeReimbursementissubmittedtoFinance,AccountsPayableforpayment.
4. HouseStaffOfficersshouldcontacttheProgramCoordinatorwithanyquestions.BELLEVUEHOSPITALCENTERSTIPENDPROCESSProfessionalEducationalPlan(PEP)ThePEPreimbursescostsassociatedwithbooks,boardexams,medicallicensurefees,duessubscriptionjournals,andmobileelectronicmedicaldevices.EffectiveJuly1,2011,themaximumbenefitpayableis$650perplanyear.Anyunusedfundscanberolledovertothenextplanyear,providedyouremainonBellevuepayroll.
TheCIR/SEIUProfessionalEducationPlan(PEP)ReimbursementClaimFormcanbefoundat:http://www.cirseiu.org/pep/
ContinuingLearningProgram(CLP)TheCLP(formerlyknownasConferenceReimbursement),reimbursesResidentsandFellowsamaximumof$1,500.00everythreeyearsbasedsolelyontheirPGYlevel.TheCIR/SEIUContinuingLearningProgram(CLP)ReimbursementClaimFormcanbefoundat:http://www.cirseiu.org/hsclaims/.NOTE:EffectiveJuly1,2014,theConferencereimbursementamount,forfellowsonBellevuepayroll,is$1,500.00maximumfortheentirelengthofthefellowship.ThisdiffersfromthereimbursementforfellowsonNYUMCpayroll.
183
PatientSafety/QualityImprovementResources,Expectations&CurriculumI.ProgramEvaluationCommitteemeetings–aportionofeachmeetingwillbedesignatedtodiscussongoingissueswithpatientsafety.Atthesemeetingswewillidentifyissueswithreportingsystemsaswellasdisseminatenewinformationregardingpatientcommunication,safetyandnewmodulesavailableinthetool-box.Inadditiontogoingovermilestoneevaluations,weusethesemeetingsasopportunitiestodiscussissueswithsupervision,Scopeofpractice,TOCandprofessionalism.Inparticular,wehavehighlightedpotentialareaswhereprofessionalismisinquestionsanddevelopedmethodstoeducateourresidentsontheseissues.Wearealsoassessingourresidentsonthesekeyareasatthesemeetings.II.Allresidents,incollaborationwithoneofourfacultymemberswillcontinuallydevelopaqualityimprovementinstrumentintheformofadatabasethatwillmonitorandtrackpatientmortalityandmorbidity.Theaimistoproducedatathatcanbeusedtoaidesurgicaldecision-makingandimprovepatientcareoutcomes.Residentsareencouragedtoparticipateinadvanceddataanalysistodevelopclinicalresearchprojectsandpublicationsonfindings.Itisourprogramsgoaltonotonlyimprovetheoverallqualityofoursystemsofcarebutindoingsoalsoencourageourresidentstoparticipateinresearchanddatagatheringthatwillcontributetothepromotionofeffectiveandevidencedbasedcare.Inregardstoreducinghealthcaredisparities,analysisofcasenumbersandareasofdeficiencywillassistinidentifyingareasforimprovement.Forexample,wehaverecentlybegunananalysisofsurgicalmorbidityintheelderly.III.Transitionofcareprocess-iscontinuouslybeingreviewed.Chairalsomeetswiththeresidentsduringchairrounds,todiscussongoingissuesonthefloors.IV.QAcommittee-wasestablishedbyourchair.Dr.DonatoPacionewillbespearheading.Theywilloccuronquarterlybasis.GMEandhospitalwideinitiativeswillbediscussed.RepresentationfromtheProgramDirector,ProgramManagerandgoingforwardaPGY4willbeprovided.TheQPSgoalswerediscussedandmethodstodisseminatetoourresidentsdeveloped.Minutesareavailableuponrequest.V.360evaluations-arebeingutilizedasmethodsforcontinuousdevelopment.Eachresidentwillcompletetheseonaquarterlybasisfornoteachotherbutthemselves.Informationfrom360isbeingincorporatedintothemilestonemeetingsandProgramManagerresponsibleforhighlightingareasofdeficiency.
184
VI.Portfolios-willberolledouttoallresidentsinAY2015.Inadditiontoreportingscholarlyactivity,theprogramwillbecollectingthedatafromprojectsforitsowndatabaseofongoingprojectsrelatedtoqualityandsafety.
185
EducationandScholarlyActivitiesforTraineesI.Allresidentswilldemonstrateatleast2publications.ThiscanbeintheformofPeer-reviewedpublications,Abstracts/Presentations/Posters,orBookChapters.Progressonthispolicywillbereviewedatsemi-annualassessments.TheCCC(ClinicalCompetencyCommittee)willalsobereviewingallresidentscholarlyactivity.II.AspartofScholarlyActivityExpectation,allresidentsandfacultymustprovideanupdatedCVwithallscholarlyactivityandappropriatesections.TheNIHformatorNYUformatarehighlyencouraged.ProgrammanagerwillrequestCVonasemi-annualbasisforcomplianceandreportingpurposes.III.GrandRoundPresentations–PresentingatGrandRoundsispartofprofessionaldevelopment.Assuch,asPGY6’sand7’smustpresentatleastonetopicofinteresteachyear.SchedulingofthispresentationmustbecoordinatedwithProgramManager.AllfacultyarealsohighlyencouragedtoparticipateinpresentingatGrandRoundsonayearlybasis.IV.JournalClub–allresidentsareexpectedtoparticipateregularlyinJournalClub.AbstractsandpublicationsaredistributedaweekpriortoJournalClubforreviewbyresidents.ItistheirresponsibilitytoreviewandbepreparedfordiscussionandQandA.FacultyarestronglyencouragedtoattendallJournalClubMeetings.V.CMEofferingsbyDepartment–allresidentsandfacultyareguaranteedregistration,freeofcharge,toanyandallCMEofferingscoordinatedbytheDepartmentofNeurosurgery.ThisincludestheannualNeurosurgerySymposiuminDecemberandGammaKnifecourses.ProgramManagerwilldistributeemailsandschedulesonaregularbasis.VI.ReportingofScholarlyActivityOnceayear,ACGMEwilldistributefacultyandresidentscholarlyactivitytemplates.Programmanagerwillinformfacultyandresidentsofneedtoprovideinformationfortemplate.FacultyandresidentsshouldcompletedtemplateinatimelymanneroratminimumprovideupdatedCV.PMIDsforallpublicationsshouldalsobeincluded.Foranyquestions,pleasecontactprogramadministration.WehaveaddedaresearchprogrammanagerandresearchcoordinatortotheNeurosurgeryDepartmenttoassisttheresidents.
186
EducationandScholarlyActivitiesforFacultyI.ProgramEvaluationCommitteemeetings–aportionofeachmeetingwillbedesignatedtodiscussongoingissueswithpatientsafety.Atthesemeetingswewillidentifyissueswithreportingsystemsaswellasdisseminatenewinformationregardingpatientcommunication,safetyandnewmodulesavailableinthetool-box.Inadditiontogoingovermilestoneevaluations,weusethesemeetingsasopportunitiestodiscussissueswithsupervision,Scopeofpractice,TOCandprofessionalism.Inparticular,wehavehighlightedpotentialareaswhereprofessionalismisinquestionsanddevelopedmethodstoeducateourresidentsontheseissues.Wearealsoassessingourresidentsonthesekeyareasatthesemeetings.II.Allresidents,incollaborationwithoneofourfacultymemberswillcontinuallydevelopaqualityimprovementinstrumentintheformofadatabasethatwillmonitorandtrackpatientmortalityandmorbidity.Theaimistoproducedatathatcanbeusedtoaidesurgicaldecision-makingandimprovepatientcareoutcomes.Residentsareencouragedtoparticipateinadvanceddataanalysistodevelopclinicalresearchprojectsandpublicationsonfindings.Itisourprogramsgoaltonotonlyimprovetheoverallqualityofoursystemsofcarebutindoingsoalsoencourageourresidentstoparticipateinresearchanddatagatheringthatwillcontributetothepromotionofeffectiveandevidencedbasedcare.Inregardstoreducinghealthcaredisparities,analysisofcasenumbersandareasofdeficiencywillassistinidentifyingareasforimprovement.Forexample,wehaverecentlybegunananalysisofsurgicalmorbidityintheelderly.III.Transitionofcareprocess-iscontinuouslybeingreviewed.Chairalsomeetswiththeresidentsduringchairrounds,todiscussongoingissuesonthefloors.IV.QAcommittee-wasestablishedbyourchair.Dr.DonatoPacionewillbespearheading.Theywilloccuronquarterlybasis.GMEandhospitalwideinitiativeswillbediscussed.RepresentationfromthePD,ProgramManager/coordinatorandgoingforwardaPGY4willbeprovided.TheQPSgoalswerediscussedandmethodstodisseminatetoourresidentsdeveloped.Minutesareavailableuponrequest.V.360evaluations-arebeingutilizedasmethodsforcontinuousdevelopment.Eachresidentwillcompletetheseonaquarterlybasisfornoteachotherbutthemselves.Informationfrom360isbeingincorporatedintothemilestonemeetingsandProgramManagerresponsibleforhighlightingareasofdeficiency.
187
VI.Portfolios-willberolledouttoallresidentsinAY2015.Inadditiontoreportingscholarlyactivity,theprogramwillbecollectingthedatafromprojectsforitsowndatabaseofongoingprojectsrelatedtoqualityandsafety.
188
ClinicalCompetencyCommitteeDescription(CCC)
DepartmentofNeurosurgeryClinicalCompetencyCommittee/ProgramEvaluationCommittee
TheClinicalCompetencyCommitteeservesattheinvitationoftheProgramDirectorandformsthehighestdepartmentalauthorityintheevaluationofeachresidentintermsofattainmentofmilestonesforreportingtotheACGME,andmakesrecommendationstotheProgramDirectorforadvancementorremediationordismissal.TheClinicalCompetencyCommitteeconsistsoffacultymembersacrosstrainingsites.MembersareappointedbytheProgramDirectorbasedonprogramrequirementV.A.1.FacultyMembers:Drs.Golfinos,Riina,Frempong,Wisoff,Kondziolka,Sen,Mogilner,Harter,Huang,PacioneandDr.StoneNon-PhysicanMembers:NP/PA,ProgramManagerTheCCCischargedwiththefollowingresponsibilities:
1) Reviewallresidentevaluationssemi-annually(facultyandpeerevaluations,self-assessmentscorereports,scholarlyactivitiesandconsultationswithteachingfaculty,caselogs,pre-andpost-rotationexaminationscores).
2) Milestonesevaluationsofeachresidenta. Reviewallresidentevaluationdatacompletedbyfacultyb. PrepareandensurethereportingofMilestonesevaluationssemi-annually
June/Decc. MakerecommendationstoPDforresidentprogress,includingpromotion,
remediationanddismissal.3) Advisetheprogramdirectorregardingresidentprogress,includingpromotion,
remediation,anddismissal.Theprogramdirectorwillmakethefinaldecisionofeachresident.,
189
ProgramEvaluationCommitteeDescription(PEC)TheroleofthePECmembersistoplan,develop,implementandevaluatetheprogram’seducationalactivities.ThePECmembers’responsibilityistoreviewandtomakerecommendationsforrevisionofthecurriculum,includingthegoalsandobjectivesoftheprogram.ThePECusesACGMEandinternal,facultyandresidentfeedbacktoreviewtheresidencyprogramannually,andaddressareasofnon-compliancetoACGMEstandards.ThePECisalsoresponsibleofrenderingaformal,writtenAnnualProgramEvaluation(APE)andpreparingawrittenplanofaction.ThePECwillmeet,inpersonorvirtuallysemi-annually.TheProgramEvaluationCommitteeconsistsoffacultymembersacrosstrainingsites,andincludesthefollowingmembers:FacultyMembers:Drs.Golfinos,Riina,Frempong,Wisoff,Kondziolka,Sen,Mogilner,Harter,Huang,PacioneandDr.StoneRotatingMembers:PGY7Chiefs,PGY6sandPGY4s–designatedeachyearandProgramManagerThePECwillmonitorandtrack,atminimum,eachofthefollowing,andanythingelsethatmaybespecifictoyourprogramthatisgermanetoprogramqualityand/oroutcomes:
• Residentperformance• Facultydevelopment• Graduateperformance,includingcertificationexaminationscores(ABNS
certification)• Programquality–asjudgedfromtraineeandfacultyevaluationsoftheprogram.• Progressonlastyear’sactionplan(programimprovementplanorPIP)• ReviewallRRCProgramRequirements/Expectations• DiscussallProgramrelatedissuesincludingbutnotlimitedto:Evaluationsand
Process,curriculum,rotations,changestoprogram,interviewprocess,ACGMEaccreditationissues/topics,andinternalGMEandhospitalrequirementsforalltrainees.
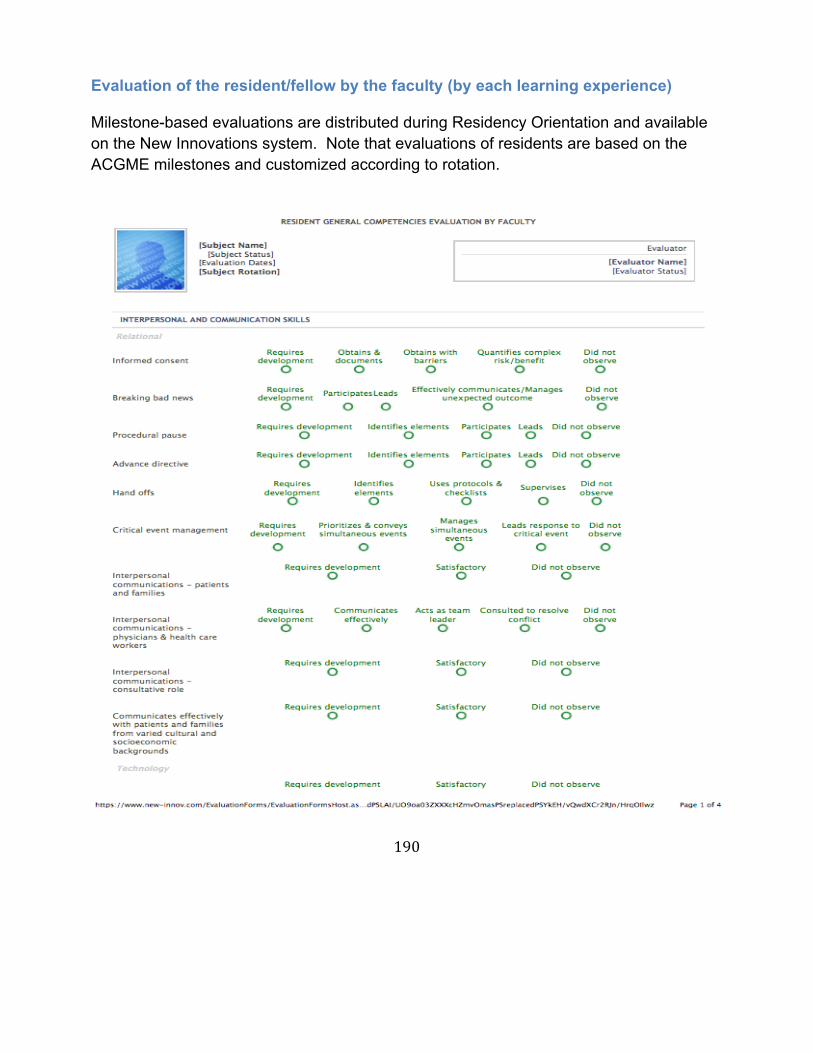
190
Evaluation of the resident/fellow by the faculty (by each learning experience) Milestone-based evaluations are distributed during Residency Orientation and available on the New Innovations system. Note that evaluations of residents are based on the ACGME milestones and customized according to rotation.
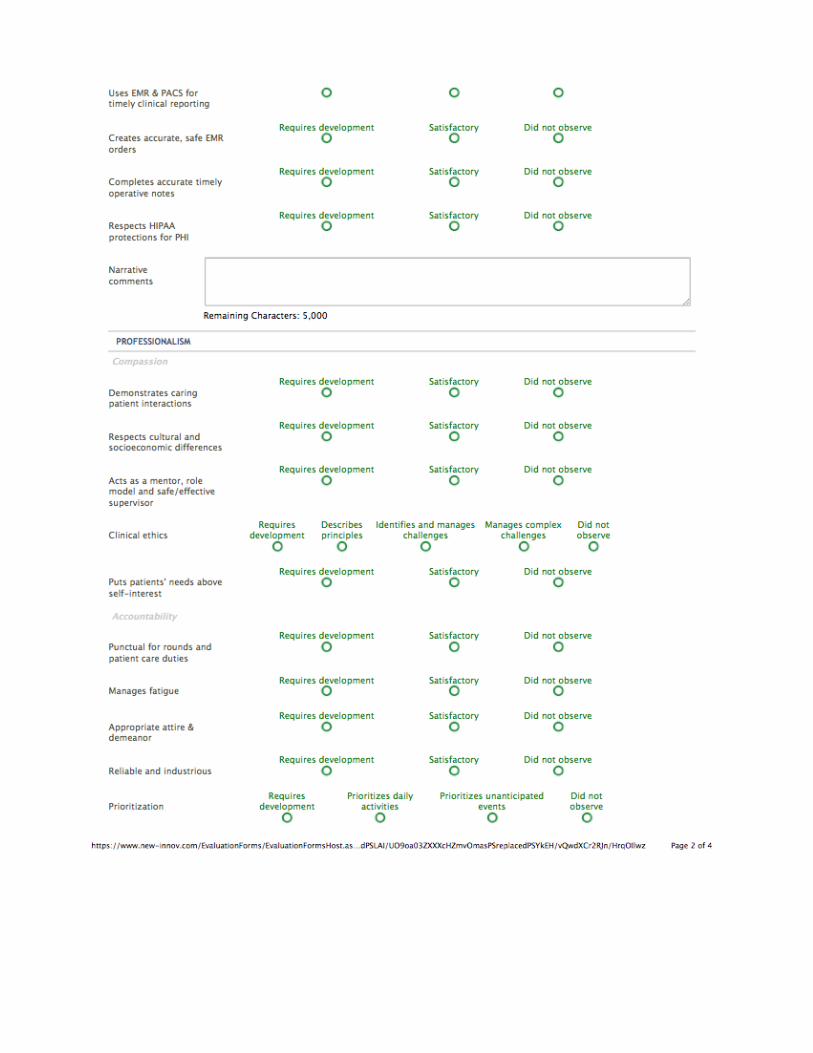
191
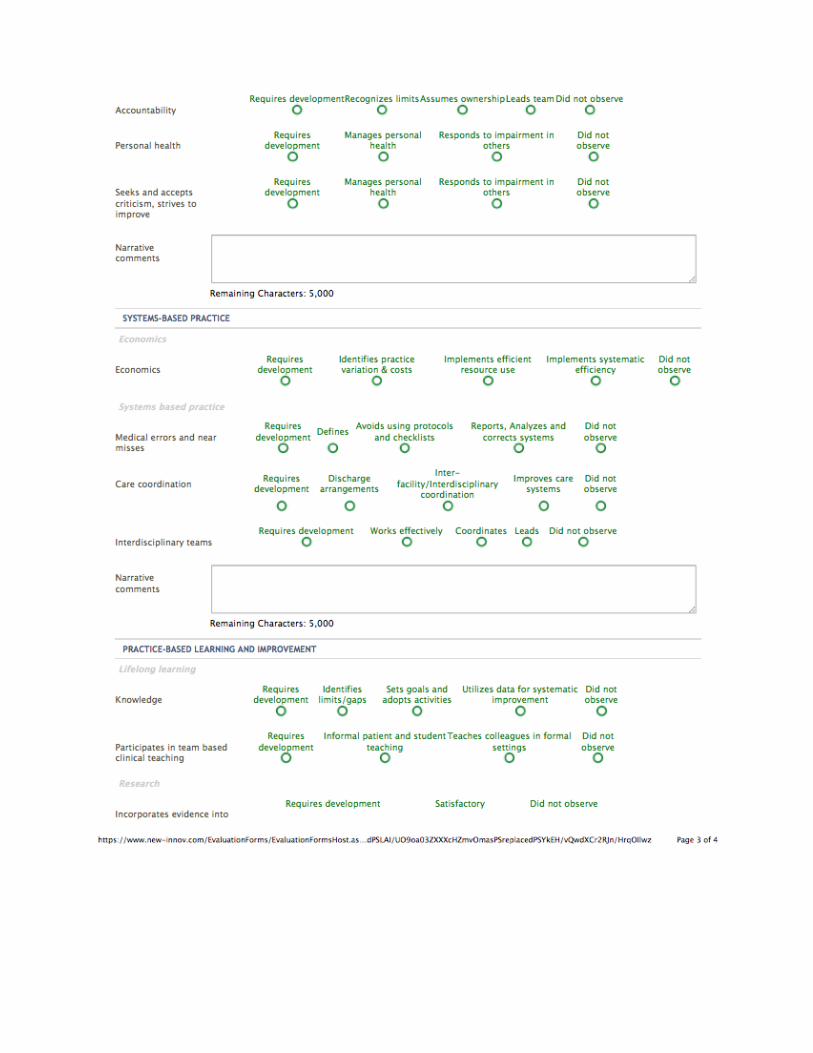
192
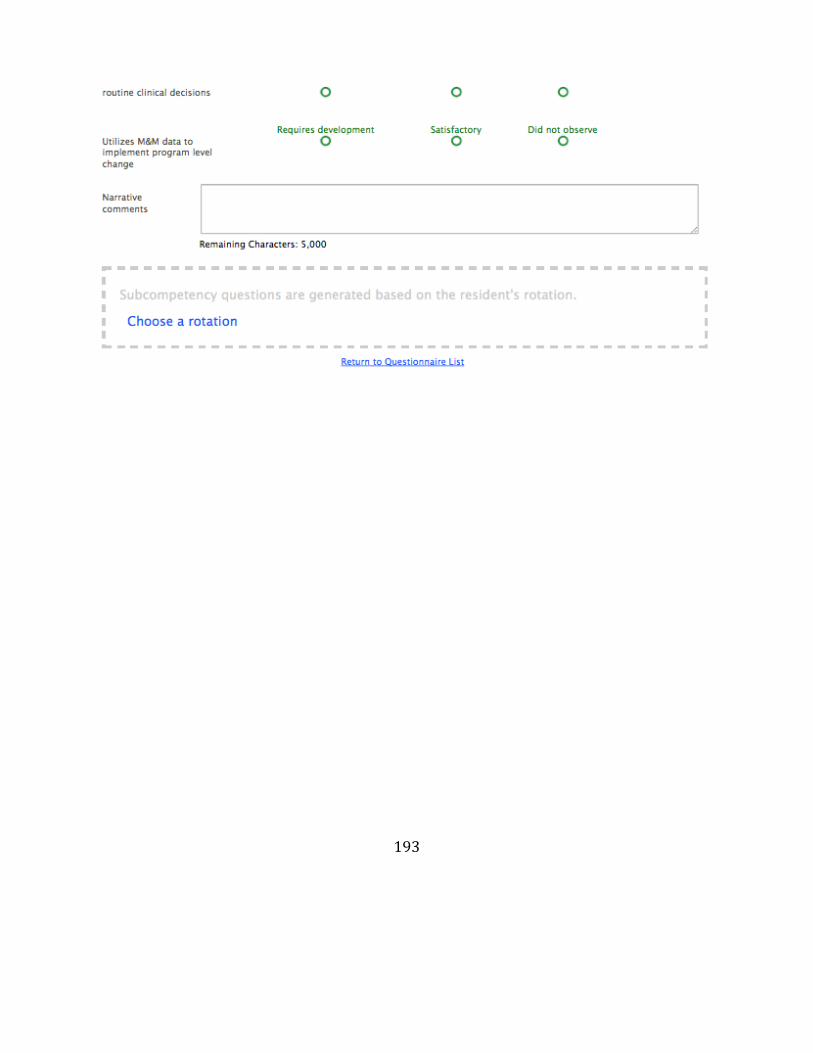
193
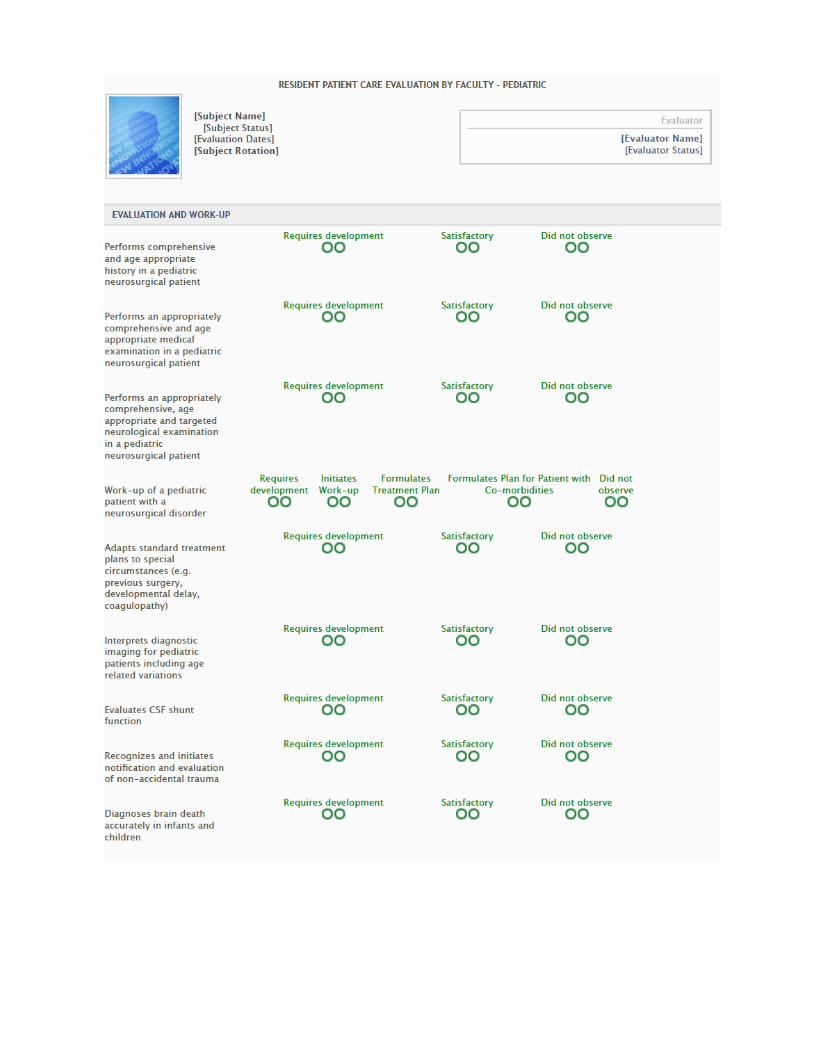
194
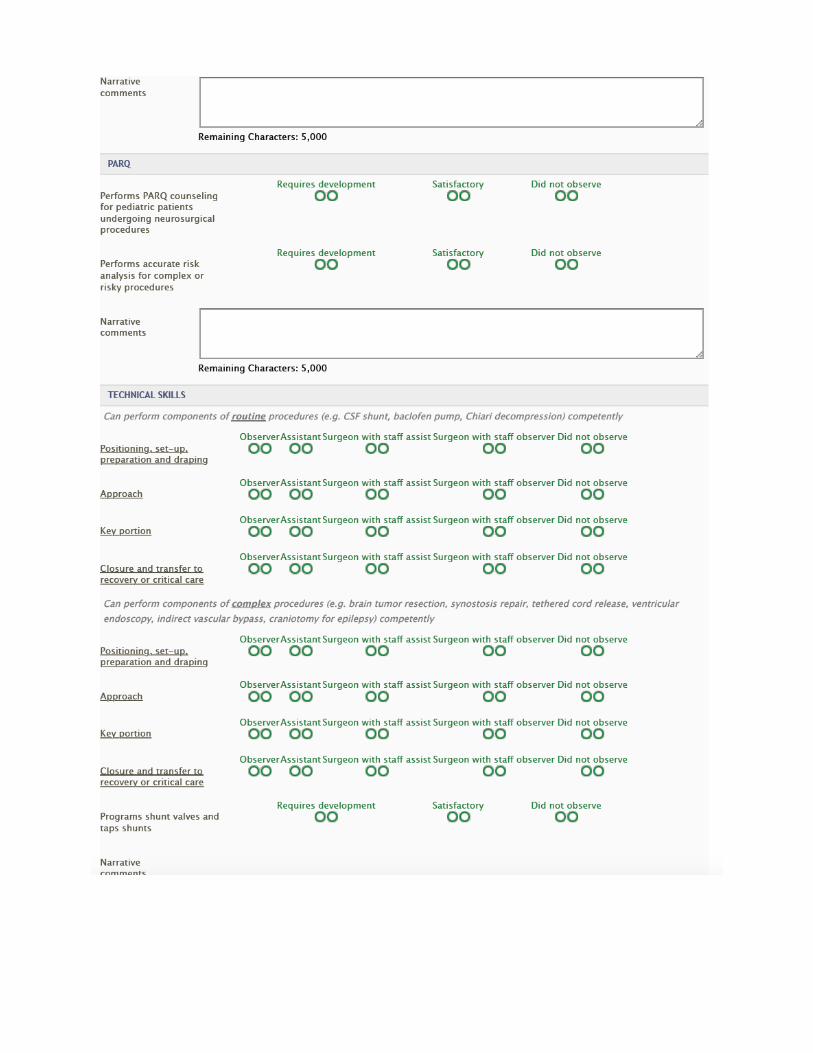
195
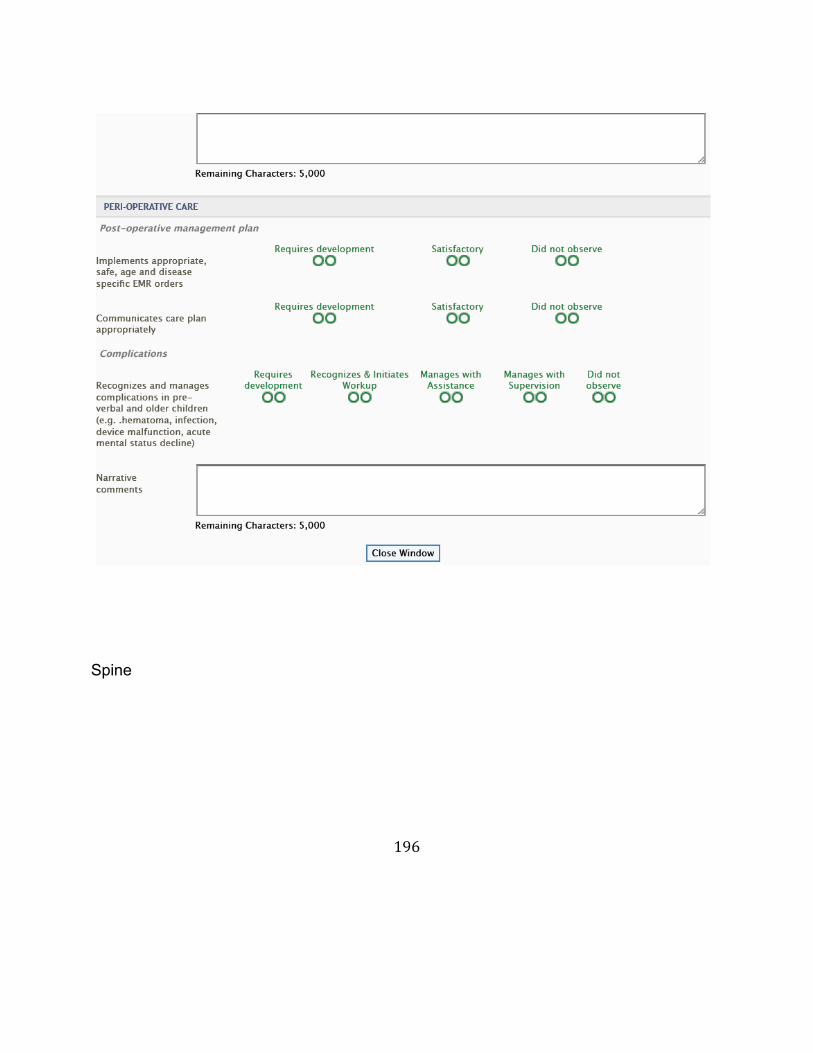
196
Spine
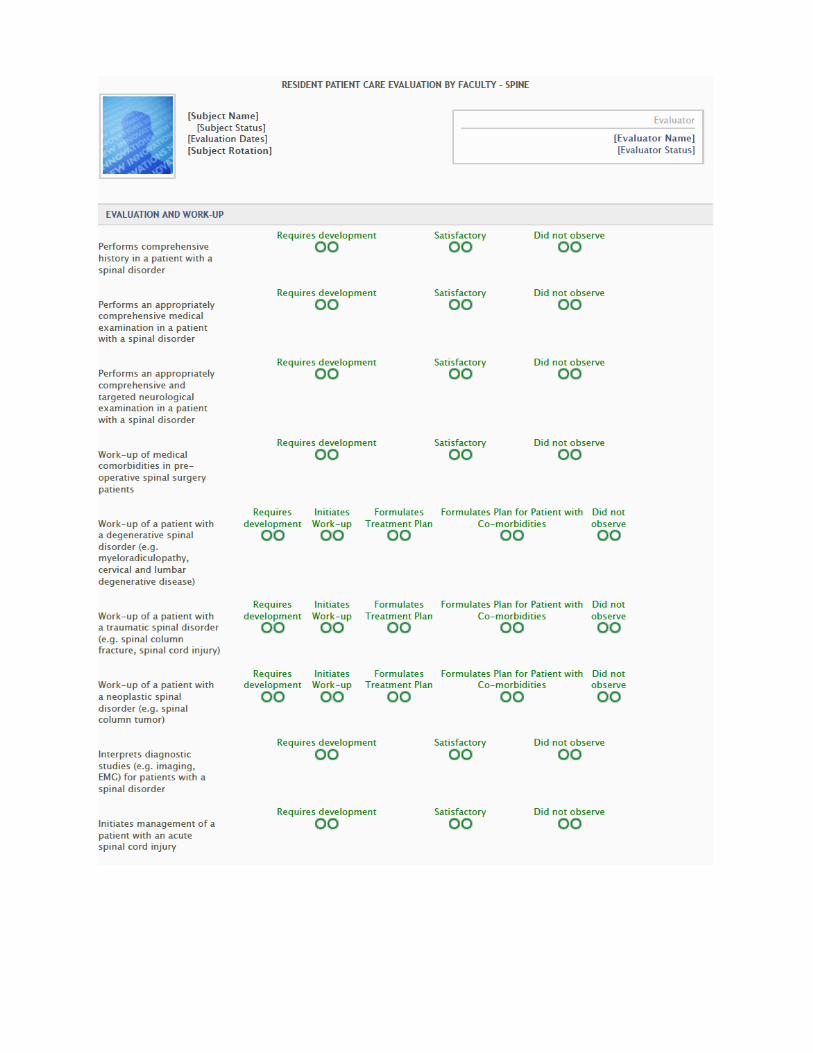
197
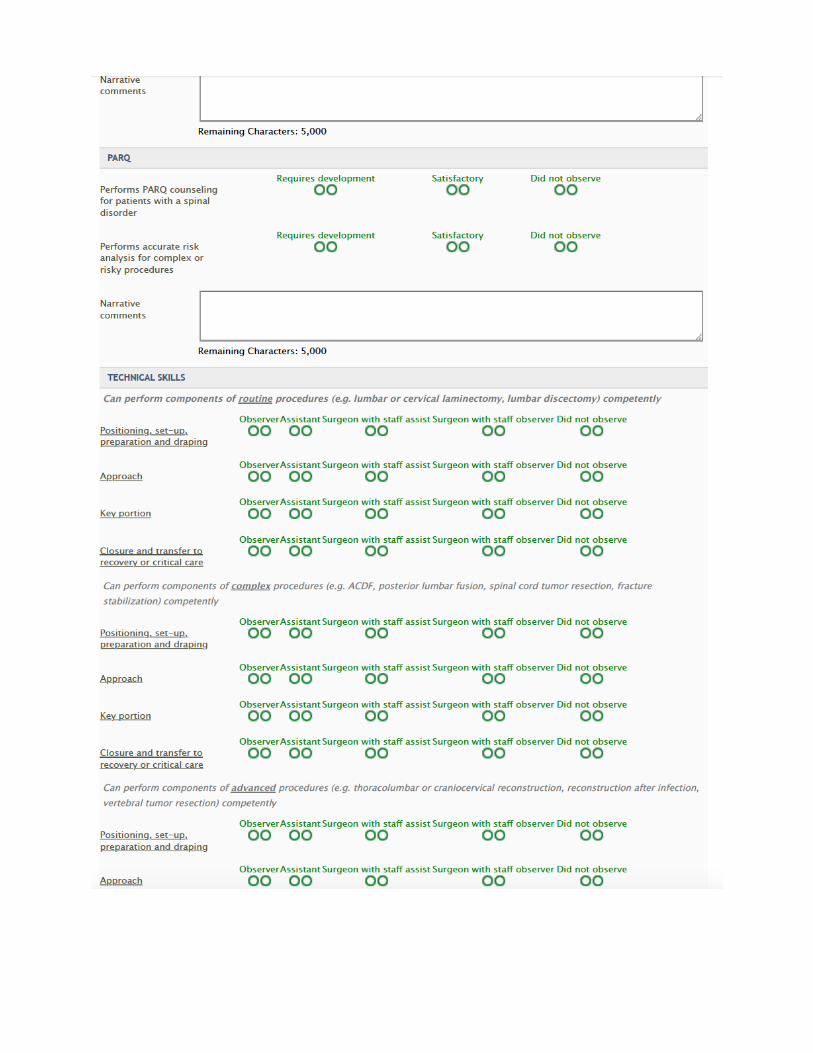
198
199
Tumor
200
201

202
203
Trauma
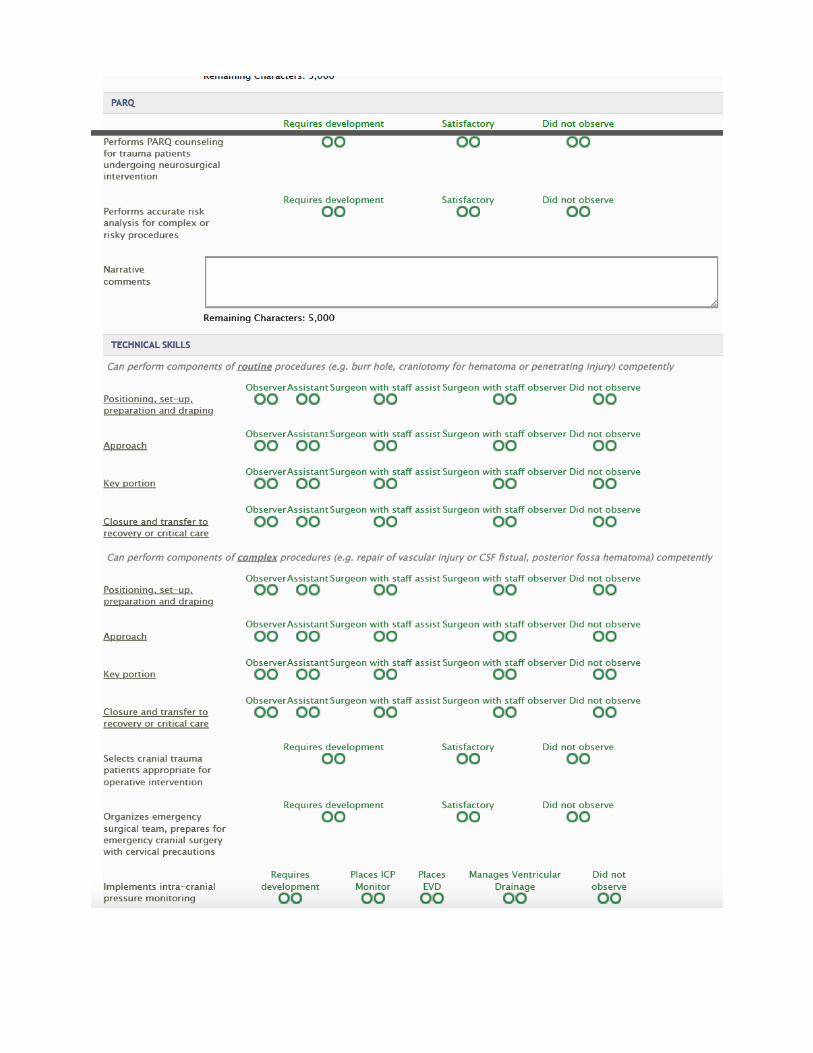
204
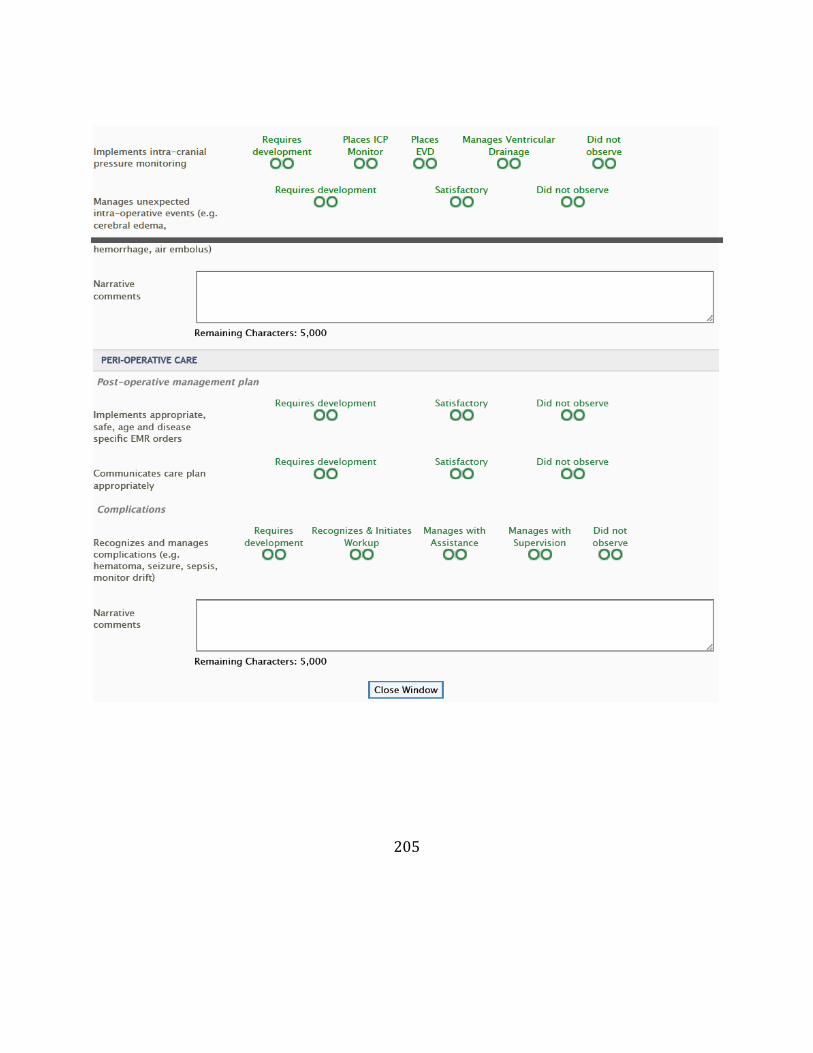
205
206
Evaluationofthefacultybytheresident/fellowFacultyEvaluationAtleastannually,theprogramandresidentsmustevaluatefacultyperformanceasitrelatestotheeducationalprogram.Thisevaluationmustincludeatleastannualwrittenfullyconfidentialevaluationsbytheresidents.EvaluationsarereviewedwiththeFacultyduringtheannualonetoonemeetingswiththefacultyandchair.Theseevaluations:
• Clinicalteachingabilities• Commitmenttotheeducationalprogram• Clinicalknowledge• Professionalism• Scholarlyactivities
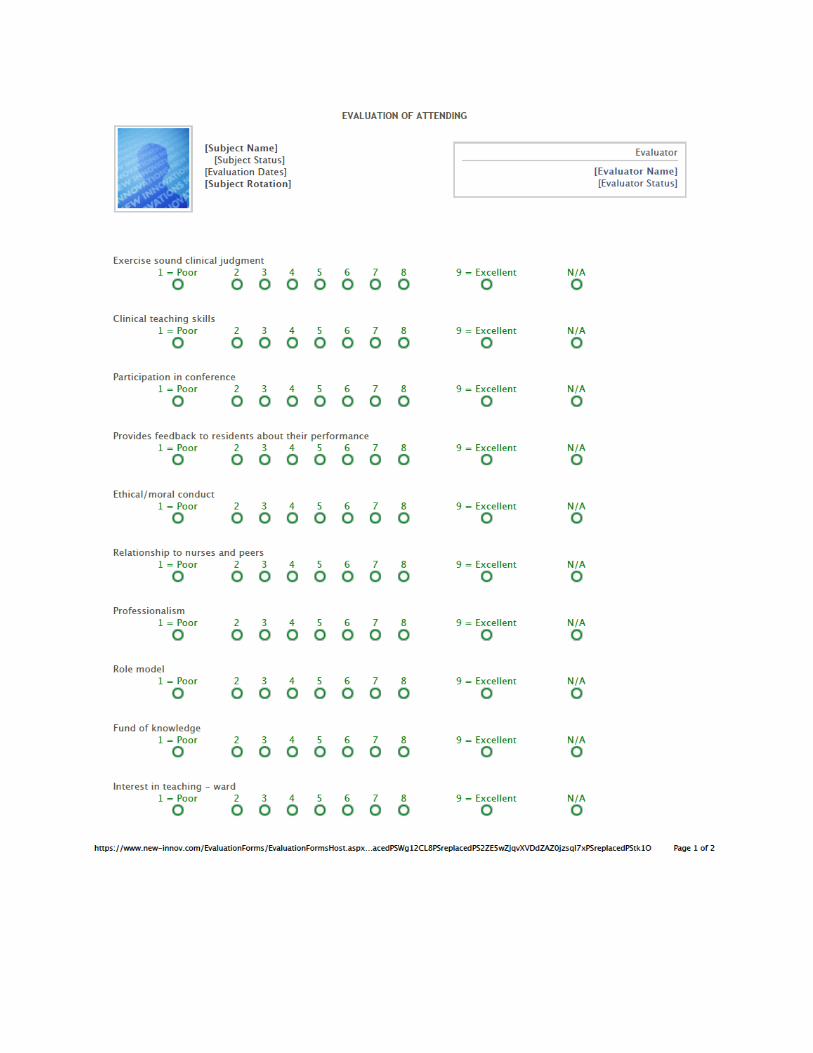
207
208
209
MultipleEvaluators(peers,patient,self,etc)Theseevaluationsarecompletedbyvariousindividuals,otherthanthesupervising/teachingfacultymembers,foraparticularlearningactivity.Certaincompetencieswillbeaddressedthroughmultisourceevaluations.Forexample,InterpersonalandCommunicationSkills(teamwork,managementskill,communication)willbeevaluatedbynurses,technicalstaff,peersandpatients.Typically,MedicalKnowledgeshouldnotbeevaluatedbypeoplewhodonothavetherequisiteexpertise.ExamplesofevaluatorswhoparticipateinMultisourceEvaluations:•Nurses•AlliedHealthProfessionals•TechnicalStaff•AdministrativeandClericalStaff•PatientsandFamilyMember•Peers•Othertraineesandstudents•Selfevaluation
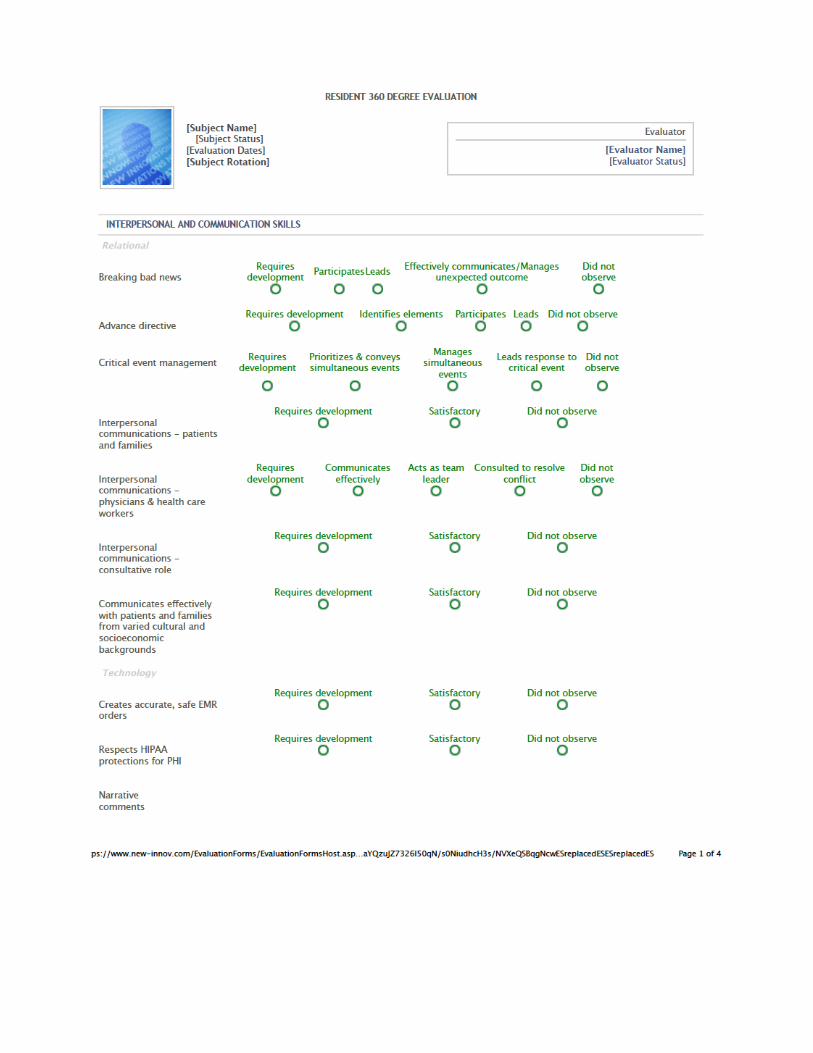
210
211
Semi-AnnualEvaluation(bytheProgramDirector)Insummativeevaluationfindingsandrecommendationsaredesignedtoaccumulateallrelevantassessmentsforago/no-godecision.Inresidentevaluationthesummativeevaluationisusedtodecidewhethertheresidentqualifiestocontinuetothenexttrainingyear.Inprogramevaluationthesummativeevaluationisusedtojudgewhethertheprogrammeetstheacceptedstandardsforthepurposeofcontinuing,restructuringordiscontinuingtheprogram.

212
213
214
Summative Evaluation (by the Program Director) In summative evaluation findings and recommendations are designed to accumulate all relevant assessments for a go/no-go decision. In resident evaluation the summative evaluation is used to decide whether the resident qualifies to continue to the next training year. In program evaluation the summative evaluation is used to judge whether the program meets the accepted standards for the purpose of continuing, restructuring or discontinued the program.
215
Evaluation of the program by the resident/fellow
216
217
218
Evaluation of the program by the faculty Program Curriculum and Improvement Evaluation The program must document a formal evaluation of the training program. The neurosurgery faculty will be asked to evaluate the training program.
219
Examinations,Licensure&CertificateNeurosurgicalResidencyTraining
Allpost-graduatetrainingdescribedbelowmustbeacquiredasaresidentinaneurologicalsurgerytrainingprogramorprogramsaccreditedbytheAccreditationCouncilforGraduateMedicalEducation(ACGME).Itmustbeundertheultimatedirectionandcontroloftheresident’sneurosurgeryProgramDirector.
• ResidentsWhoBeganTrainingbetweenJuly1,2009,andJune30,2013 Seventy-twomonthsofneurosurgicalresidencytraininginACGMEaccredited
programsunderthedirectionofaneurosurgicalProgramDirector.Thismustconsistof:
o 42monthsofcoreclinicalneurosurgery,including12monthsaschiefresident;atleast21monthsmustbespentinoneprogram.
o PGY-1mustincludeaminimumof3monthsoffundamentalclinicalskillstraining(criticalcare,traumaandotherrotationsasdesignatedbytheProgramDirector);itmayincludeupto6monthsofneurosurgerythatwillcounttowardthe42monthsrequired.
o 3monthsofclinicalneurologytakenduringthefirst3yearsoftraining,preferablyduringthePGY-1.
o 24monthsofelectives,i.e.:neuropathology,neuroradiology,research,and/ormoreneurosurgery,possiblyinareasofspecialinterestsuchascomplexspinesurgery,endovascular,orpediatricneurosurgery,and/orclinicalandnon-clinicalneurosciences.
• ResidentsWhoBeganTrainingafterJune30,2013 Eighty-fourmonthsofneurosurgicalresidencytraininginACGMEaccredited
programsunderthedirectionofaneurosurgicalProgramDirector.Thismustconsistof:
• 54monthsofcoreclinicalneurosurgery,includingo 12monthsaschiefresidentduringthelasttwoyearsoftraining
(PGY-6or7);21monthsmustbespentinoneprogram.o 3monthsofbasicneuroscience(e.g.,neurology,neuro-otology,
neuroradiology,neuropathology)takeninthefirst18monthsoftraining.
o 3monthsofcriticalcarerelevanttoneurosurgerypatientstakeninthefirst18monthsofresidency.
o 6monthsofstructurededucationingeneralpatientcare(e.g.:trauma,generalsurgery,orthopedicsurgery,otolaryngology,plasticsurgery,etc.).
220
§ 21monthsmustbespentinoneprogram.o 30monthsofelectives,i.e.:neuropathology,neuroradiology,
research,and/ormoreneurosurgery,possiblyinareasofspecialinterestsuchascomplexspinesurgery,endovascular,orpediatricneurosurgery,and/orclinicalandnon-clinicalneurosciences.
o Outsiderotationsof6to12monthsatanACGMEaccreditedprogrammaybecountedtowardsthecore54monthsofneurosurgerytraining.TheprogramdirectormustrequestcreditfromtheABNSpriortotherotation.
o Credittowardsthe30monthsofelectivetimemayberequestedbyaprogramdirectorforprioreducationalexperiences,suchasaPhDdegreeinarelevantsubject,clinicalrotationsotherthanfellowshipsobtainedatnon-ACGMEaccreditedprograms,andneurosurgicaltrainingcompletedoutsideoftheU.S.,particularlyiftheresidentiscertifiedinthatcountry.WrittenrequestssubmittedbytheprogramdirectortotheABNSmustcontainacompletedescriptionoftheexperienceandjustificationoftherequest.
o TheBoardwillevaluateACGMEcaselogdataasameasureofthebreadthofresidentexperienceatthecompletionofresidencytraining.
Trainingofanytype,includingresearch,doneininstitutionsoutsideoftheparentprogramanditsaffiliatedhospitalswillnotcounttowardmeetingtheserequirementsunlesscreditisrequestedinwritingfromtheBoardprospectivelybytheProgramDirectorandapprovedinwriting.AsofJuly1,2013,rotationsof6to12monthsinotherACGMEaccreditedneurosurgicalprogramsmaybegrantedclinicalneurosurgerycreditthatwillcounttowardtherequired54months;otherwisecreditiselectiveonly.TheABNSmayalsograntelectivecreditfortraininginnon-ACGMEaccreditedU.SorforeigncentersonanindividualbasiswhenundertakenwiththeadviceandapprovaloftheProgramDirector.Approvalfortrainingperiodsoflessthanthreemonthswillnotordinarilybegrantedsincetheyareofquestionableeducationalvalue.
Trainingdevotedtoneuroscienceeducation,criticalcare,orotherdisciplinesrelatedtoneurosurgerymayalsobeacquiredasafulltimeresidentinACGMEaccreditedtrainingprograms(suchasgeneralandorthopedicsurgery)thatareinthesameinstitutionastheresident’sneurosurgeryprogram.ThistrainingdoesnotneedtheBoard’sapprovalaslongasitremainsundertheultimatedirectionandcontroloftheresident’sneurosurgeryProgramDirector.
Uponpetitionfromaresident’sProgramDirector,theBoardmaygrantelectivecreditfortrainingdonebeforeenteringanaccreditedneurosurgeryprogramiftheresidenthad
221
substantiallymorethantheprerequisitetrainingingeneralsurgery,neurology,orthebasicneurologicalsciencesatacceptableinstitutions.IfthetrainingresultedinaPhDinaneurosciencefield,oneyearofelectivecreditwillbegiven.Neurosurgeryresidencytrainingcompletedabroad,particularlyifitconcludedwithcertificationinthatcountry,mayalsomeritretroactiveelectivecreditiftheABNSispetitionedbytheProgramDirector.Creditisnotautomatic.ItmustberequestedbytheProgramDirectorandapprovedinwritingbytheBoard.
Trainingbypreceptorshipdoesnotfulfilltheserequirements.Furthermore,nocreditisgivenfortrainingdonebyfellowsorotherindividualsnotenrolledasresidentstrackingtowardcertificationinACGMEaccreditedneurosurgeryprograms.Residenttrainingcannotbeobtainedduringrepeatedshortintervalsinanumberofinstitutions.Theseprovisionsinnowayalterthebasicminimumrequirements.
LeavingorTransferringfromaResidencyProgramShouldaresidentleaveatrainingprogram,theDirectormustsendalettertotheABNSstatingthecreditfortraininginbothtimeandcategorythathasbeensuccessfullycompleted.Shouldtheindividualenteranewneurosurgeryprogram,thenewProgramDirectormayhonorthatcreditdependingonhisorherdirectappraisaloftheresident’sprofessionalandeducationalprogress.ThatProgramDirectormustthenwritetotheBoardstatinghowmuchcreditwillbeaccepted.
Informationontransferringresidentsishandledinthesamemannerasabove.BoththeoriginalandnewProgramDirectorsmustsubmittraininginformationinwritingtotheABNSprospectively.
PrimaryExamination/InServiceExamTheABNSPrimaryExaminationisanimportantstepinthecertificationprocess.ItisavailabletoallresidentsinACGMEaccreditedneurosurgeryprogramsandisdesignedtoevaluatecandidates’knowledgeandprovidedirectionforcontinuedlearning.TheABNSpreparesthe375questiononlineexaminationwiththeguidanceoftheNationalBoardofMedicalExaminers(NBME).Mostquestionsaremultiplechoicecoveringinformationonthebasicsciences,criticalcare,fundamentalclinicalskills,imaging,neuroanatomy,neurobiology,neurology,neuropharmacology,neurosurgery,pathologyandotherdisciplinesdeemedsuitableandimportant.ItisgiveneachyearinMarchatmostU.S.neurosurgicalresidencies.TheABNSandRRCrequireresidentstopasstheExaminationforcredittowardcertificationbeforecompletingtrainingandpriortobeginningthechiefresidentyear(PGY7).
NeurosurgeonswhocompletedresidencytraininginACGMEaccreditedprogramsmaytakethePrimaryExaminationasoftenastheywish.IndividualswhoenteredCanadianneurosurgeryprogramspriortoJuly16,1997mayalsotakeit.ABNSRulesandRegulationsdonotallowittobeofferedtofellowsormedicalschoolstudents,etc.

222
ChangetopolicyasofOctober2015ABNSonlineexamsarescheduledinMarchofeveryyear.Forallwhowishtotakeexamforcreditornot;theymustnotifyprogramadministrationtocompleteyourregistration.Allresidentswhohavealreadypassedbycomfortablemargincantakeexamforcredit.AsaPGY1itisoptional,howeverstronglyencouragedtotakeifyouplanonstudyingandshouldnotbeusedforpracticealone.IfyouhaveanyquestionsaboutyourrequirementsfortakingthisexampleasespeaktoDr.HarterorDr.Riina.
LicensingAllresidentsmustapplyforlimitedpermitorpermanentNYSlicensepriortotheirPGY6year.CopyoflicenseshouldbeprovidedtoProgramManageandGMEHouseStaffAffairsOffice.USMLEstep3isrequiredforlicensure.
223
HouseStaffWellbeingNYUSchoolofMedicineIssuingDepartment:GraduateMedicalEducationEffectiveDate:05/2008ReissueDate:04/01/2013FitnessforDutyI.PolicyPurposeAllstaffmembers(allNYUMCemployees,includingHouseStaffOfficersandotheremployedmedical staffmembers), areexpected to report towork fit forduty.Individualswho report towork impairedcanunderminetheproductivityof theMedicalCenter’sworkforceandcreateaseriousthreattothemselvesorthewelfareofpatients,staff,andvisitors. TheMedicalCenter,therefore, adopts the following policy andprocedures to ensure that staffmembers are fit forduty.II.Definitions(ifapplicable)
A.FitnessforDutyreferstotheabilityofastaffmembertoperformtheessentialfunctionsofhisorherjobwithoutanimpairmentthatmayposeapotentialrisktopatients,adirectthreattothesafetyoftheindividualstaffmemberortoothers intheworkplace,and/orinterferewiththeperformanceofhisorherduties,withorwithoutareasonableaccommodation. There are primarily threecategories ofimpairment associated withFitnessforDuty:
a.Impairmentassociatedwith theuseor the suspicionofuseofalcoholor illegaldrugs;
b.Impairmentassociatedwithbehaviorthatmayposeadirectthreattotheemployeeortoothersintheworkplace;and
c.Impairment caused by amedical condition, includingmental health,and/ortheuseofmedicationforthatcondition
III.Policy
224
A.SuspectedAlcoholand/orIllegalDrugUse
a.ProceduresDuringRegularBusinessHours forHouseStaffOfficers: If anyHouseStaffOfficersaresuspectedofbeingimpairedwhileatwork,theprogramdirector should contact theNYUOffice ofGME, in accordancewith theCorrectiveActionAndDisciplinaryPolicyForHouseStaffOfficers.TheOfficeof GMEwillreferthe House Staff Officer to the NYUMC Employee HealthService(EHS).TheEHSclinicianshallexaminetheindividualtodetermineifheorsheisworkingundertheinfluenceofalcoholand/oranillegaldrug.Theexammayinclude,butnotnecessarilybelimitedto,toxicologytestingofbloodorotherbodyfluids.HouseStaffOfficerswhorefusetoundergosuchexaminationmaybesuspended and/or dismissedfrom thetrainingprogram in accordance with theCorrectiveActionAndDisciplinaryPolicyForHouseStaffOfficers.
AftertheEHSevaluationtheHouseStaffmemberwillbeplacedonpaidmedicalLeaveofAbsence(“LOA”),inaccordancewiththeCorrectiveActionAndDisciplinaryPolicyForHouseStaffOfficers,pendingtheresultsoftheevaluationforalcoholorsubstanceabuse. Aspartof thisprocess, theHouseStaffOfficerwillbeevaluatedbyaphysiciandesignatedbytheInstitution.AfterproperevaluationandconsultationwiththeHouseStaffmemberandtheOfficeofGME,thedesignatedphysicianmayrefertheindividualtotheCommitteeforPhysicianHealthoftheNewYorkMedicalSociety(CPH)oranothermedicalprovider.TheHouse Staff Officermay be asked to completeconsents for release of relevantinformationtoapplicablepartiessuchasthedesignatedphysician,EHS,andtheOfficeofGME. StaffunwillingtocomplywiththetreatmentrecommendationsofthedesignatedphysicianwillbereportedtotheOfficeofGMEandtheHouseStaff Officerwill be subject to disciplinary action as defined intheCorrectiveActionAndDisciplinaryPolicyForHouseStaffOfficers.
b.ProceduresDuringNon-BusinessHoursForHouseStaffOfficers-IfaHouseStaffOfficerrequiresassessmentduringhourswhenEHSisclosed,he/sheshouldbeaccompaniedbytheirrespectivedepartmentleadershiptotheEmergencyDepartmentofNYUHospitalsCenterorBellevueforanassessment. Refusaltoparticipate in the evaluation for alcohol or substance abusewill be deemed anadmissionofusageandmaysubjecttheindividualtosuspensionand/ordismissal.Iftheindividualisimmediatelyassessedasunabletowork,he/shewillbereleasedfromworkpendingtheresultsoftheevaluation.ThedepartmentleadershipindividualwhoaccompaniedtheHouseStaffOfficertotheERshouldnotifyEHSandOfficeofGMEoftheincidenttoensurepropercollaborationandfollow-uputilizingproceduresasdescribedabove.
225
c.ProceduresDuringRegularBusinessHours ForAllOther Staff -Staffmembers who report to work appearing to be under the influence of alcoholand/orillegaldrugswillnotbeallowedtowork. EmployeeRelationsshouldbeconsultedandtheemployeeimmediatelyreferredtotheEHS.TheEHSclinicianshallevaluatetheindividualtodetermineifheorsheisworkingundertheinfluence ofalcoholand/oran illegal drug. Evaluation may include, but notnecessarilybelimitedto,toxicologytestingofbloodorotherbodyfluids.Refusaltoparticipate inthetoxicologyscreeningwillbedeemedanadmissionofusageandthestaffmemberwillbeimmediatelysuspended,pendingfurtherinvestigation, andwill besubjectadditional disciplinary action up to andincludingtermination.
At the time of the EHS evaluation, the individual will be released fromwork(withoutpay)pendingtheresultsoftheevaluationforalcoholorsubstanceabuse.EHSwillnotifytheappropriatedepartmentleadershipandEmployeeRelationsofthedecisiontoremovetheindividualfromtheworkplace.Aspartofthisprocessandafterproperevaluationandconsultationwith thestaffmember, theClinicalDirectorofEmployeeHealthServicemayrefertheindividualtoanotherprovideror theorganization’s Facultyand Staff Assistance Program (FASAP) provider,whichwillprovideassessmentandreferral for treatmentandcasemanagement.The staffmember may be asked tocomplete consents for release of relevantinformationtoapplicablepartiessuchasEHS,andtheEmployeeRelationsDepartment.Staffunwillingtocomplywiththetreatmentrecommendationswillbereportedandmaybedischargedfromemployment.
d.ProceduresDuringNon-BusinessHoursForAllOtherStaff-Ifastaffmemberrequires assessment during hours when EHS is closed, he/she should beaccompanied by their respective department leadership to the NYU HospitalsCenter Emergency Department for an assessment. Refusal to participate in theevaluationforalcoholorsubstanceabusewillbedeemedanadmissionofusageandthe staff member will be subject to suspension and/or termination. If theindividualisimmediatelyassessedasunabletowork,he/shewillbereleasedfromworkpendingtheresultsoftheevaluation.Thestaffmember’sdepartmentleadershipshouldnotifyEHSandEmployeeRelationsof the incident toensurepropercollaborationandfollow-uputilizingproceduresasdescribedabove.
B.Impairment Associated with Behavior that Poses a Direct Threat to Safety inthe
Workplace
226
a.ProceduresForHouseStaffOfficers -HouseStaffOfficerswhoexhibitinappropriateorunusualbehaviorpresentingadirectthreattothemselvesorothersintheworkplacewillbereferredtothedesignatedphysicianforevaluation.Ifthe designated physician determines that the individual’sbehavior poses adirectthreattohisorherhealthandsafety,ortothehealthandsafetyofothersintheworkplace,he/shemaybereferredtoEHSfortesting,toCPH,ortoanothermedicalproviderforfurtherassessment;suchevaluationswillbecomepartoftheindividual’sconfidentialhealthrecord. TheNYUMedicalCenterSecurityDepartmentshouldbecontactedasnecessaryforassistanceinhandlinganyHouse Staff Officersposing such a threat to healthor safety. For House StaffOfficersexhibitingbehaviorthatisanimminentthreattohealthandsafetyintheworkplace,andifinappropriateorunusualbehavioroccursduringhourswhenthedesignatedphysicianisunavailable,departmentleadershipshallescorttheHouseStaff Officer to theNYUHospitalsCenter orBellevue EmergencyDepartmentforanassessment. If the individual isimmediatelyassessedasunable towork,he/she will be released fromworkpendingthe results of the evaluation.TheHouseStaffOfficer’sdepartmentleadershipshouldalsonotifyEHSandtheOffice of GME of the incident toensure propercollaboration and follow-uputilizingproceduresasdescribedabove.TheNYUMedicalCenterSecurityDepartmentshouldbecontactedasnecessaryforassistanceinhandlinganystaffmembersposingsuchathreattohealthorsafety.
b.Procedures ForAllOther Staff -Staffmemberswho exhibit inappropriate or
unusualbehaviorpresentingadirect threat to themselvesorothers intheworkplacewill be referred to EHS for evaluation.If EHS determines thattheindividual’sbehaviorposesadirectthreattohisorherhealthandsafety,ortothehealthandsafetyofothers intheworkplace,he/sheshallbereferredbyEHStothe FASAP (1-800-833-8707) for further assessment Suchevaluationswillbecome part of the individual’s confidential health record.The NYUMedicalCenter Security Department should be contacted asnecessary for assistance inhandling any staff members posing such a threatto health or safety. For staffexhibitingbehavior that isan imminent threattohealthandsafety in theworkplace, and if inappropriate or unusualbehavior occurs during hours whenEHS isclosed,department leadershipshallescort thestaffmember to theNYUHospitalsCenterEmergencyDepartment foranassessment. If the individual isimmediatelyassessedasunabletowork,he/shewillbereleasedfromworkpendingtheresultsoftheevaluation. Thestaffmember’sdepartmentleadershipshouldnotifyEHSandEmployeeRelationsoftheincidenttoensurepropercollaborationandfollow-uputilizingproceduresasdescribedabove. TheNYUMedical CenterSecurityDepartment should be contacted as necessary forassistancein
227
handlinganystaffmembersposingsuchathreattohealthorsafety.
C.ImpairmentCausedbyaMedicalCondition,IncludingMentalHealth-Astaffmembermaybeaskedtosubmittoamedicalexaminationorsomeotherformofdisability-relatedinquirywhenthedepartmentleadershiphasareasonablebelief,thattheindividual’sability toperformtheessential functionsofhisorher jobis impairedbyamedical condition, includingmentalhealth and/or theuseofmedication for thatcondition. The results of the medical examination and/orpsychiatric evaluation willbecomepartofthestaffmember’sconfidentialhealthrecord.
a.Procedures forHouse StaffOfficers -Department leadershipmustcontacttheOfficeofGMEforguidancepriortomakingadisability-relatedinquiryorrequiringaphysicalexaminationorpsychiatricevaluation. TheOfficeofGMEwillrevieweachrequestforamedicalexaminationortomakeadisability-relatedinquiryona case-by-casebasis. A referral to thedesignatedphysicianorCPHmaybeappropriateforevaluationofHouseStaffOfficers,whomaybeimpairedduetoamentalhealthconditionand/ortheuseofmedicationforthatcondition
b.ProceduresforAllOtherStaff -Department leadershipmustcontact
EmployeeRelationsforguidancepriortomakingadisability-relatedinquiryorrequiringaphysicalexaminationorpsychiatricevaluation. EmployeeRelationswillrevieweachrequestforamedicalexaminationortomakeadisability-relatedinquiryonacase-by-casebasis.AreferraltoFASAP(1-800-833-8707)maybeappropriatefor evaluation of staffmembers, whomay be impaired due to amental healthconditionand/ortheuseofmedicationforthatcondition
D.FitnesstoReturntoWork
a.Procedures forHouseStaffOfficers -CPHor an individual treatingphysicianwilladvisethedesignatedphysicianandtheOfficeofGMEwhentheHouseStaffOfficerbeingmonitoredhasbeendeemedabletoreturntoworkwithorwithoutareasonable accommodation. If accommodation isrequested, theEmployeeRelationsofficeshouldbe involved. The individualwillberequiredtoprovidedocumentation of the clearance to return towork from thetreatingfacility/physicianorCPH. If theHouse StaffOfficerwason atemporaryleaveduetotreatmentforalcoholorillegaldrugabuse,thatindividualwillberequiredtoprovidedocumentationtothedesignatedphysicianshowingeithercompletionof treatment and/or ongoing treatment,
228
depending on thecircumstances of theleave.ThedesignatedphysicianwillreviewandverifythesourceofallfitnessfordutydocumentationsubmittedbytheHouseStaffOfficer. Thedesignatedphysicianwillthenconsultwiththeindividual’sProgramDirectorandtheOfficeofGMEregardingtheindividual’sabilitytoreturntoworktoperformtheessentialfunctionsofhisorherjobwithorwithoutareasonableaccommodation.Forthoseclearancesinvolvingthetreatmentforalcoholordrugabuse,theHouseStaffOfficermayberequiredtosubmittorandomalcoholand/ordrugtoxicologyscreening following theirreturn towork, whichwill be performed at anappropriatefacilitywiththerecommendationofthedesignatedphysician.Inaddition, theindividual’s compliancewith their treatmentprogramwillbemonitoreduntiltreatmentiscompleted
b.Procedures for Other Staff - FASAP or an individual treating physician
willadviseEHSandEmployeeRelationswhenthestaffmemberbeingmonitoredhasbeendeemedabletoreturntoworkwithorwithoutareasonableaccommodation.Ifaccommodation is requested, the Employee Relationsoffice should beinvolved.Theindividualwillberequiredtoprovidedocumentationoftheclearancetoreturntoworkfromthetreatingfacility/physicianorFASAP. Ifthestaffmemberwas on a temporary leavedue to treatment for alcohol or illegaldrugabuse, that individual will berequired to provide documentation to EHSshowingeithercompletionoftreatmentand/orongoing treatment,dependingonthecircumstances of theleave. The EHS clinician will review and verify thesourceofallfitnessfordutydocumentationsubmittedbythestaffmember.TheEHSclinicianwillthenconsultwith the individual’sdepartment leadershipandtheEmployeeRelationsrepresentativeregardingtheindividual’sabilitytoreturnto worktoperform the essential functions of his or her job with or without areasonableaccommodation.
E.AssistanceAgencies:
a.FacultyandStaffAssistanceProgram(FASAP),providedbyCorporateCounselingAssociates1-800-833-8707(24/7).a. CommitteeforPhysicianHealth1-800-338-1833.
229
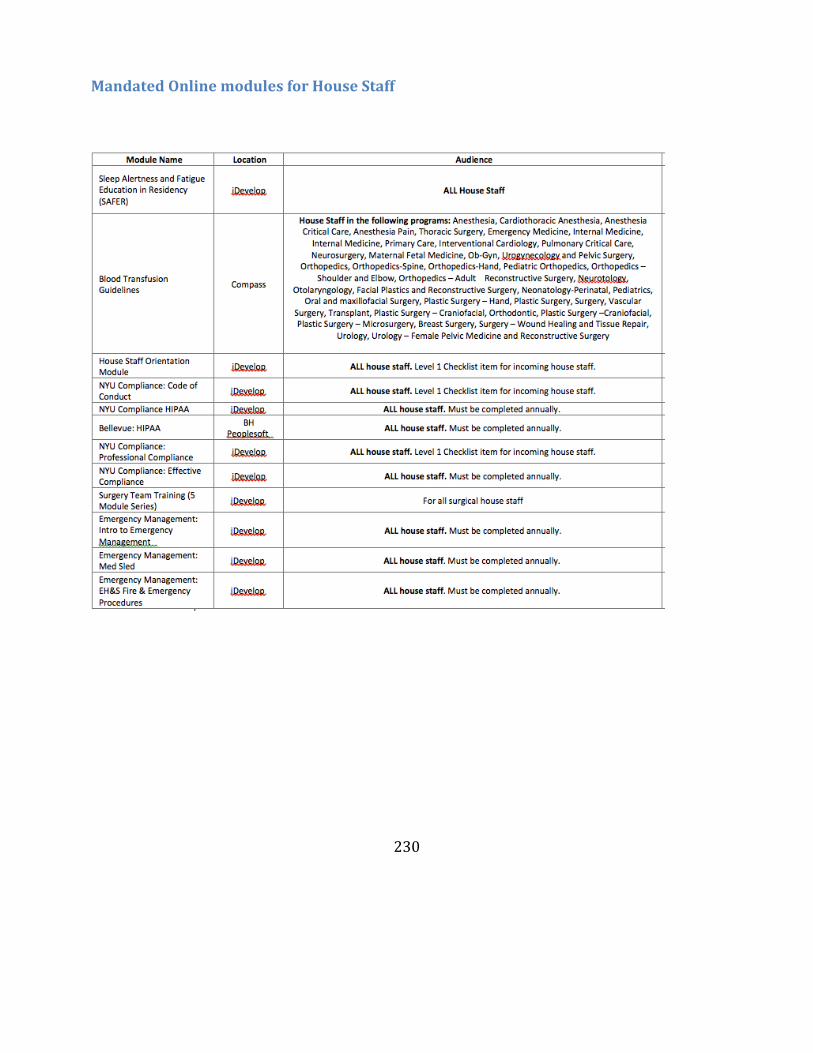
230
MandatedOnlinemodulesforHouseStaff
231
NYULMCMedicalLibraryVisittheNYUMedicalLibraryonatNYULMCunderPopularLinks.http://central.nyumc.org/shared/lib/Pages/Home.aspx
232
OnCallRoomsGENERALINFORMATIONNeurosurgeryOn-CallroomsavailableBellevueHospital–7S33TischHospital–12thFloor,JrOn-callRoomandChiefOn-callroom(keysareavailableintheprogrammanager’sofficeinBH7S4)Apartments1Aand2G(rooms2G2&2G3)areusedfortemporaryovernightlodgingforHouseStaffandPhysicalMedicineandRehabpersonnel.Apartment1Aisanindividualstudio apartment. Apartment2G is a three-bedroomsuite. Eachroomwithinthe2Gapartmentisidentifiedwith“1”,“2”or“3”onthedoor.
Room1A–ForHouseStaffpersonnellodgingONLY.
Room2G-1 --ForPhysicalMedicineandRehabpersonnellodgingONLY.Room2G-2 –ForHouseStaffpersonnellodgingONLY.
Room2G-3–ForHouseStaffpersonnellodgingONLY.
PhysicalMed&Rehabadministrativestaffwillmonitorkey issuance, trackingandcontrol for their personnel using 2G1.Security does not have a role orresponsibilityinthis.Thekeysforrooms1A,and2G-2and2G-3willbedispensedbyGreenbergHallSecuritystaff.KeysaretrackedandmonitoredbytheGraduateMedicalEducational(GME)office.KEYSThereare threerings locatedat theGreenbergSecurityDesk (Post22). Thealuminumplatewillstateeither“APT1A”,“APT2G–2”or“APT2G–3”. For“APT2G–2”and“APT2G–3”,thekeyringwillhavetwokeys.Onekeywillbetoentertheapartment;theotherkeyisfortheroom. Genderwillnotplayaroleinhowthekeysaredistributed.PROCEDURETherewillbealistingofauthorizedhousestaffinabinderattheGBHsecuritydesk,
233
whichisupdatedmonthly.Thekeyswillbeissuedonafirst-come,first-served basis.The intent is for one-nightstays under normal circumstances.Securitywillnotmonitorlengthofstays.DONOTLEAVEANYPATIENTINFORMATIONORPERSONALITEMSBEHINDWHENYOULEAVETHEROOMFORTHENIGHT/DAY.Theprocedureisasfollows:
•A House Staff member will request a key to the apartment fromthesecurityofficerintheGreenbergHallLobby.
•The securityofficerwill inspect themember’svalid IDbadgeandcrossreferenceitagainsttheHouseStafflistprovidedbytheGMEoffice.Thebadgemuststate“HouseStaff”. “VisitingHouseStaff”arenotauthorizedtousetheserooms.
•Oncevalidated,alineentrywillbecompletedintheOn-CallHouseStaffLodgingRecordform;thekeywillthenbeissued.
•Weekdays at noon-time (1200 hrs) Monday-Friday, the GBHsecurityofficerwill place a call to the GME office (212-263-5506)stating thestatusofthetwosetsofkeys. Theofficeisclosedweekends/holidays.
•If a key has not been returned, the GME office will be responsibletocontacttheHouseStaffmember(s)toretrieve/obtainoutstandingkeys.
•IfakeyisnotavailablewhenaHouseStaffmemberdesiresaroom,thesecurityofficerwilladvisetherequestorthattheroom(s)aretaken/notavailable andhave them contact the GME office if there is anurgentneedforuseoftheroom.
•Ifthereareanyproblemsduringtheshift,thesecurityofficerwillcontactasecuritysupervisorat212.263.5120(24hours).
234
CommitteeParticipationforHouseStaffHouseStaffareencouragedtoparticipateinvariouscommittees(listedbelow).HouseStaffLeadershipCommitteeTheHouseStaffLeadershipCommitteehasbeennewlyformedbymergingtheCombinedHouseStaffCommitteeandtheHouseStaffCounciltoserveasaforumforthehousestafftoconsolidateandvoicetheirconcerns.LouisMiller, MDistheFacultyAdvisor. ThecommitteealsoservesanewroleasameetingforhousestafftopresentprogramactivityineachoftheCLERfocusareas.Itisameaningful forumforhousestafftointeractwithoneanotherandhospitalleadershipinastructuredway,andwithinthecontextofNAS/CLER.Themembershaveanimportantroleinprovidingfeedbackfromprogramsintermsofprogress,andreportingproblemsandnewideas.AmemberwillalsoReporttotheMedicalBoardforBHandTH.HouseStaffmembersarepeer---selectedresidentsfromeachcoreprogramwhoarevotedinandappointedbytheChairoftheHouseStaffLeadershipCommittee.AdditionalHouseStaffrepresentativesmayattendcommitteemeetingsasnon---votingmembers;provideinformation,adviceandfeedback.TheCommitteemeetsquarterlywithhospitalleadershipandmembersoftheGMEEC.Newmembersareelectedannually.PleasebeintouchwithyourProgramDirector,Coordinator,orChiefsifyouareinterestedinparticipating!TwocurrentHouseStaffresidentssitontheHouseStaffLeadershipCommittee.HouseStaffPatientSafetyCouncilTheHouseStaffPatientSafetyCouncilattheNYUSchoolofMedicinewasestablishedinJune2012.Dr.KatherineHochman,MDistheCouncil'sfacultyadvisor.TheHouseStaffPatientSafetyCounciliscomprisedofhousestaffwhoarecommittedtoqualityimprovementandpatientsafetythroughout theinstitution.ThehospitaladministrationandGMEOfficeareveryinterestedinhavingresidentsdirectlyengagedinpatientsafetyandqualityimprovementactivities,andareallfullysupportiveofourCouncil.FourexecutiveleadersareelectedbyfellowhousestaffataHSCmeetinginthebeginningoftheyear.Newmembersareelectedannually.PleasebeintouchwithyourProgramDirector,Coordinator,orChiefsifyouareinterestedinjoiningthecouncil!TwocurrentHouseStaffresidentssitontheHouseStaffLeadershipCommittee.HouseStaffWellnessCommittee
235
TheHouseStaffWellnessCommitteehasbeennewlyformed.CarolBernstein,MD(PsychiatryResidencyProgramDirector)istheCouncil’sfacultyadvisor.TheHouseStaffWellnessCommitteeisasubcommitteeoftheGMEC.ItiscomprisedofHouseStaffofficers.ThemissionoftheHouseStaffWellnessCommittee(HSWC)istoprovideastructured,sustainablecommittee,whichwillidentifyandaddressissuesrelatedtothewellnessandmentalhealthneedsofallHouseStaffatNewYorkUniversityLangoneMedicalCenter(NYULMC),BellevueHospitalCenter(BHC),andtheVeteransAffairsNewYorkHarborHealthcareSystem(VA-NY).TheCommitteemeetsthesecondThursdayofeverymonthat6pm.Locationtobedetermined.Newmembersareelectedannually.TwocurrentHouseStaffresidentssitontheHouseStaffLeadershipCommittee.
236
AdditionalInformationIdentificationBadgesThereareatleastthreeIDsthatHouseStaffwillneedandpotentiallymore,dependingonthesitesatwhichyouwillbeworking.Thethreeare:NYULMC,BellevueandtheVA(Manhattan).YourprogramwillhelpyoudetermineifanyadditionalIDbadgesareneeded.NYULMCIDbadgesNYULangoneMedicalCenterpolicyrequiresallemployeestowearanidentificationbadgewhileonMedicalCenterproperty.IdentificationbadgesaredistributedbytheNYULMCSecurityOffice.Location: 550FirstAvenue,Room182 MedicalScienceBuilding(MSB)–followtheyellowpathwayPhone: 212-263-5038BellevueIDbadgesIfyouwillbeworkingatBellevueHospital,youMUSTobtainaBellevueIDbadges.Todoso,youmaygototheBellevueHospitalPoliceOffice.Location: 462FirstAvenue,RoomGD-17 Monday-Friday:7:00am–5:00pm Closed:Noon-1:00pm Phone: 212-562-2345VeteransAffairsMedicalCenter(ManhattanCampus)IDbadgeObtainingofthisIDbadgerequiresthecompletionofappropriatesecurityformswhichvarydependinguponyouraccessrequirements.ThesemayincludeaSpecialAgencyCheck(electronicfingerprintscanning)andNationalAgreementCheck&Inquiry.MCITTelecommunications
237
AsanNYULMCResident/Fellow,youwillbeassignedapersonallong-rangealpha/textpagercapableofbeingactivatedviatelephone,emailorSMStext.YourpersonalpagerwillaccompanyyouthroughoutyourtrainingyearsatNYULMC.IfyouhavequestionsaboutyourpagerpleasecontacttheTelecommunicationsDepartment.Location: GreenbergHall,545FirstAvenue LevelSC-1,Room129Hours: Monday-Friday:9:00am–5:00pmPhone:212-263-1120LinenServicesLongwhitecoatsandscrubsareavailabletoallmembersoftheHouseStaffviamachineslocatedonthefloors.YoucanretrieveyourscrubcodeforthesemachinesattheLinenServicesRoom.YoumustpresentyourNYULMCIDbadgewhenpickinguporexchangingyourlinens.Location: 550FirstAvenue,4thfloor,Room401(acrossfromtheAelevator) Hours: Monday-Friday:6:30am–4:00pm Closed:10:00am–11:30amforinventoryPhone:646-754-6209(outsidehospital) Extension73134(insidehospital)MachineLocations: TischHospital:Floors2,5,8&11 HCC:Floors2&14
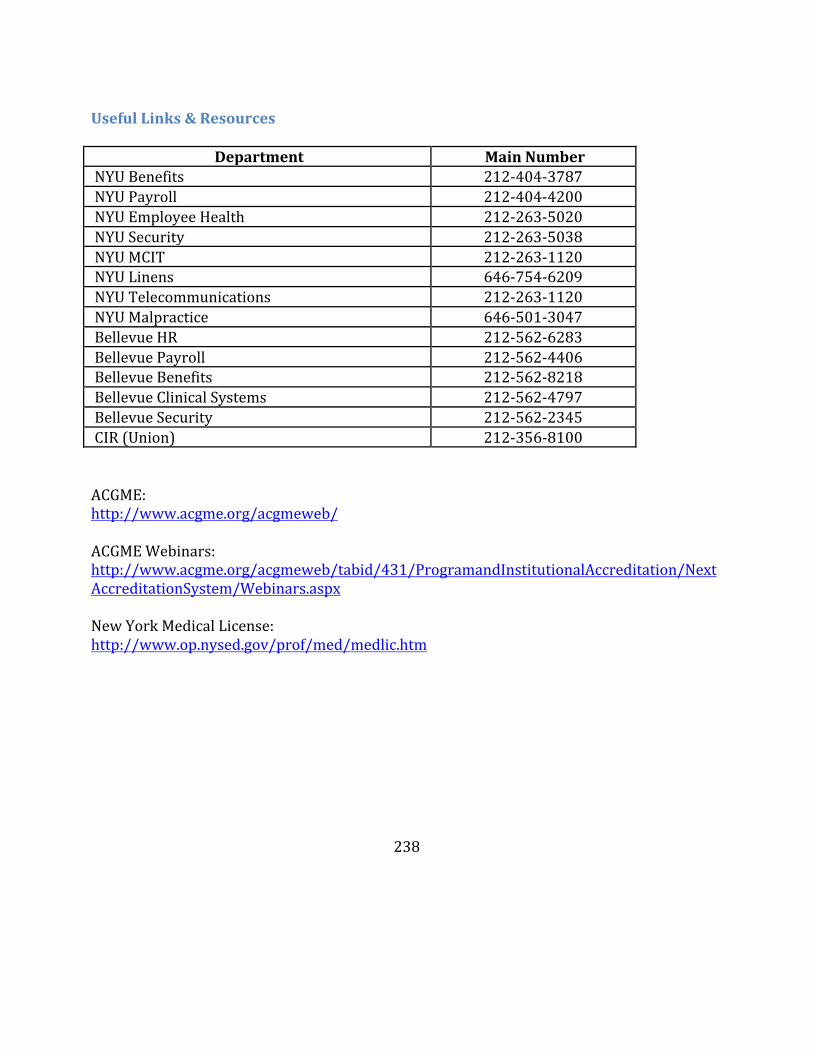
238
UsefulLinks&Resources
Department MainNumberNYUBenefits 212-404-3787NYUPayroll 212-404-4200NYUEmployeeHealth 212-263-5020NYUSecurity 212-263-5038NYUMCIT 212-263-1120NYULinens 646-754-6209NYUTelecommunications 212-263-1120NYUMalpractice 646-501-3047BellevueHR 212-562-6283BellevuePayroll 212-562-4406BellevueBenefits 212-562-8218BellevueClinicalSystems 212-562-4797BellevueSecurity 212-562-2345CIR(Union) 212-356-8100ACGME:http://www.acgme.org/acgmeweb/ACGMEWebinars:http://www.acgme.org/acgmeweb/tabid/431/ProgramandInstitutionalAccreditation/NextAccreditationSystem/Webinars.aspxNewYorkMedicalLicense:http://www.op.nysed.gov/prof/med/medlic.htm